Embed Size (px)
Citation preview
Postgraduate Medical Journal (May 1977) 53, 237-242.
Necrotizing fasciitis
M. A. TEHRANIF.R.C.S.
I. McA. LEDINGHAMM.B., Ch.B.
University Department of Surgery, Western Infirmary, Glasgow
SummaryThe authors' experience of fourteen patients withnecrotizing fasciitis is reviewed. The pathognomonicfeature of this condition is an extensive necrosis ofsubcutaneous tissue caused by a vicious cycle of infec-tion, local ischaemia and reduced host defencemechanisms. The diagnosis can only be confirmed byimmediate exploratory incision.The reported mortality of 30-40%/ reflects the
inadequacy of conservative surgery in the treatment ofthis serious condition. Mortality can be reduced byearly recognition followed by radical excision of thenecrotic fascia and overlying skin. The preservationand subsequent use of the excised skin has the ad-vantage of economy in the use of donor areas andreduction in morbidity. Hyperbaric oxygen therapydoes not halt the spread of the necrotizing process andis not a substitute for radical surgery.
Definition and historical backgroundNecrotizing fasciitis is a relentlessly destructive
bacterial infection characterized by extensive necrosisof the subcutaneous tissues of the abdominal walland, less frequently, the extremities. The condition isfortunately uncommon but is potentially fatal anddemands early recognition in order that treatmentmay be effective. Although the serious nature of thiscondition was recognized as long as 100 years ago(Jones, 1871), confusion in the literature was com-pounded by the multiplicity of descriptive termi-nology and inadequate bacteriological data. Thus thecondition has been referred to as 'hospital gangrene'(Jones, 1871), 'acute infective gangrene' (Fedden,1909), 'necrotizing erysipelas' (Pfanner, 1918),'haemolytic streptococcus gangrene' (Meleney, 1924,1929), and 'suppurative fasciitis' (McCafferty andLyons, 1948).The first large series published in the present
century was that of Meleney who, in 1924, reportedtwenty patients from China. Meleney described thecondition as a rapidly developing gangrene whichoccurred more frequently in males and the extremi-ties were affected in the large majority of cases. He
Correspondence: Dr lain McA. Ledingham, UniversityDepartment of Surgery, Western Infirmary, GlasgowGil 6NT.
stated that 'the infection essentially produces agangrene of the subcutaneous tissues, subsequently itcauses death of a part of the overlying skin'. InMeleney's report, bacterial culture showed that thehaemolytic streptococcus 'was the only organisminvariably present'. Other organisms which wereidentified were fewer in number and none of themappeared regularly enough to be considered as the'causative organism'-hence the term 'haemolyticstreptococcus gangrene'.Wilson (1952) was the first to use the descriptive
term 'necrotizing fasciitis' because of the charac-teristic necrotic fascia and subsequently observednon-specificity of the pathogenic organism involved.Others in later reports (Rea and Wyrick, 1970;Meade and Mueller, 1968; Ledingham and Tehrani,1975) have confirmed the validity of this statementand have continued to use this term in preference toother descriptive names.
BacteriologyPathogenic organisms undoubtedly play a major
role in initiating and spreading the necrotizingprocess. The type of bacteria now encountered,however, seem to differ from those in earlier reports.In Wilson's series of twenty-two patients (Wilson,1952), haemolytic organisms were found in pureculture in 58% of cases studied bacteriologically andwere present along with non-haemolytic bacteria inan additional 26% of the patients. The majority oforganisms (88%) were pathogenic staphylococci.Rea and Wyrick (1970) reported forty-four patientswith necrotizing fasciitis seen during 15 years atParkland Memorial Hospital in Dallas. In thisgroup, haemolytic streptococci and pathogenicstaphylococci together accounted for 89% of thewound infections with enteric Gram-negativeorganisms responsible for the remaining 11%. In arecent report, Wilson and Haltalin (1973) describedeleven children with necrotizing fasciitis. Haemolyticstreptococci were found in 50%/ of cases. The otherorganisms were staphylococci and Pseudomonasaeruginosa. In the report by Ledingham and Tehrani(1975) the predominant organisms in initial woundculture, obtained through fresh incisions in theaffected areas, were coliforms in combination most
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.53.619.237 on 1 May 1977. D
ownloaded from
238 M. A. Tehrani and . McA. Ledingham
frequently with enterococci and streptococci; in onlyone case was the streptococcus of the a-haemolyticvariety. Other organisms included Bacteroides,diphtheroids, Clostridium welchii, Proteus, Staphylo-coccus and Ps. aeruginosa. Since colonizing bacteriarapidly invade the affected area, bacteriologicalcultures, both aerobic and anaerobic must be takenfrom several sites at an early stage in the course of thedisease.
PathogenesisIrrespective of the species of organism involved,
the initial bacterial growth takes place in the sub-cutaneous tissues, i.e. the subcutaneous fat, super-ficial fascia and the superficial layer of the deepfascia, most commonly of the abdominal wall andlower extremities. The initiating injury responsiblefor introduction of the infection may follow minortrauma (abrasions, cuts, bruises, insect bites, minorburns) or surgical incision. At times, no obviouscause is found.
In the series reported by Rea and Wyrick (1970),minor trauma was responsible for 80% of the casesand in eight patients, no history of specific injurycould be obtained. In the present series of fourteenpatients, necrotizing fasciitis developed followingischio-rectal sepsis in six, abdominal surgery in five,and fractured pelvis, diabetic peripheral vasculardisease and repeated supra-pubic aspiration of urineeach in one patient. Similarly in eleven children,reported by Wilson and Haltalin (1973), the conditionoccurred following surgery in five, and traumaticlaceration, varicella, osteomyelitis, abscess of buttockand bone marrow aspiration, each in one patient. Inthe final patient of this series no predisposing con-dition was present.
After the initial bacterial insult, the infectionspreads rapidly along the fascial plane causingmassive necrosis. The presence of ischaemic tissuefurther facilitates spread of the necrotizing process.The skin remains intact initially but later developspatchy necrosis and becomes gangrenous as a resultof thrombotic occlusion of both venules and arte-rioles supplying the skin. Damage to cutaneousnerves causes numbness and subsequent anaesthesiaof the part. Untreated, the affected skin becomesextensively necrotic. At an early stage, histologicalexamination of full thickness skin biopsies reveals noabnormality. The subcutaneous fat and superficialfascia show a continuing non-specific inflammatoryreaction, with fibrinoid arteriolitis and thrombosis ofthe vessels. Organisms may or may not be demon-strated in specially stained preparations.The factors responsible for this alarming spread
are unknown. An anaphylactic reaction similar tothe Schwartzmann or Arthus phenomenon wassuggested by Meleney (1933). McCafferty and
Lyons (1948) postulated activation by streptokinaseor staphylokinase of a serum proteolytic enzyme,present in the inflammatory exudate, causing pro-gressive collagen necrosis.
Haemolytic streptococci are capable of producinghaemolysin, leucocidine, fibrinolysin, erythrogenictoxin and the enzyme hyaluronidase. The filtrate ofpathogenic staphylococci has haemolytic, necroticand coagulating properties (Kellaway, Burnet andWilliams, 1930). Other organisms such as Pseudo-monas are known to produce collagenase with aprimary effect on subcutaneous tissues and fascia(Meade and Mueller, 1968).Another important factor which should be con-
sidered in the pathogenesis of a major infection ofthis sort is reduction in the host defence mechanisms(HDM). Primarily, local reduction in tissue resis-tance is achieved by the action of bacterial toxinsadded to the effect of bacterial kinases. This action isfurther enhanced by the general reduction in HDMoccurring in the postoperative period, or by pre-existing systemic diseases such as diabetes, arterio-sclerosis, agamma- or hypogammaglobulinaemia,rheumatoid arthritis, malnutrition and gastro-intestinal haemorrhage (Table 1).
TABLE 1. Factors involved in the pathogenesis of necro-tizing fasciitis. HDM - host defence mechanisms
Infection(non-specific bacteria)
PostoperativeDiabetic
Collagenase ArteriosclerosisBacterial toxins Agamma/Hypo-Proteolytic enzymes Reduced HDM globulinaemia
>. Rh. arthritisMalnutritionGastrointestinal
Necrosis of the haemorrhagesuperficial fascia
Ischaemia
Rapid spread alongavascular fascial plane+ gross undermining
Secondary gangrene of skin
Abele et al. (1960) reported a case of progressivefatal cutaneous gangrene associated with hypo-gammaglobulinaemia. In Buchanan's patient(Buchanan and Haserick, 1970) there was elevationof serum complement level and a slight increase inIgA, but its significance was unknown. In sixpatients in the present series, hypoalbuminaemia andhypergammaglobulinaemia were found. Clearlymore detailed studies are required to detect thepossibility of specific immunological defects contri-buting to the spread of necrotizing process. Diabetes
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.53.619.237 on 1 May 1977. D
ownloaded from
Necrotizing fasciitis 239
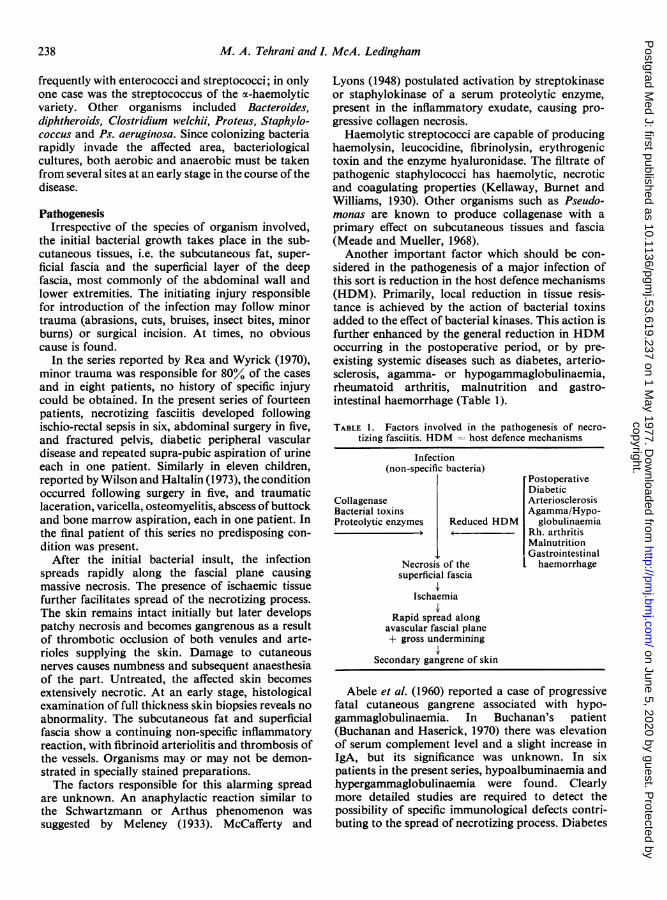
is an important predisposing condition whichreduces the host-defence mechanisms. In Cros-thwait's series (Crosthwait, Crosthwait and Jordan,1964), 50%/ of the deaths occurred in diabeticpatients and in Meade and Mueller's report (1968),neither of the two diabetic patients who developednecrotizing fasciitis, survived. Six cases recentlydescribed by Roberts and Hester (1972) as syner-gistic bacterial gangrene, had most of the features ofnecrotizing fasciitis and all had diabetes and keto-acidosis. Infection, local ischaemia and reduced hostdefence mechanisms combine to form a vicious cyclewhich is responsible for the initiation and spread ofthe lesion (Fig. 1).
Infection
Ischaemia
Reduced hostdefence mechanisms
FIG. 1. Factors involved in initiation and spread ofnecrotizing fasciitis.
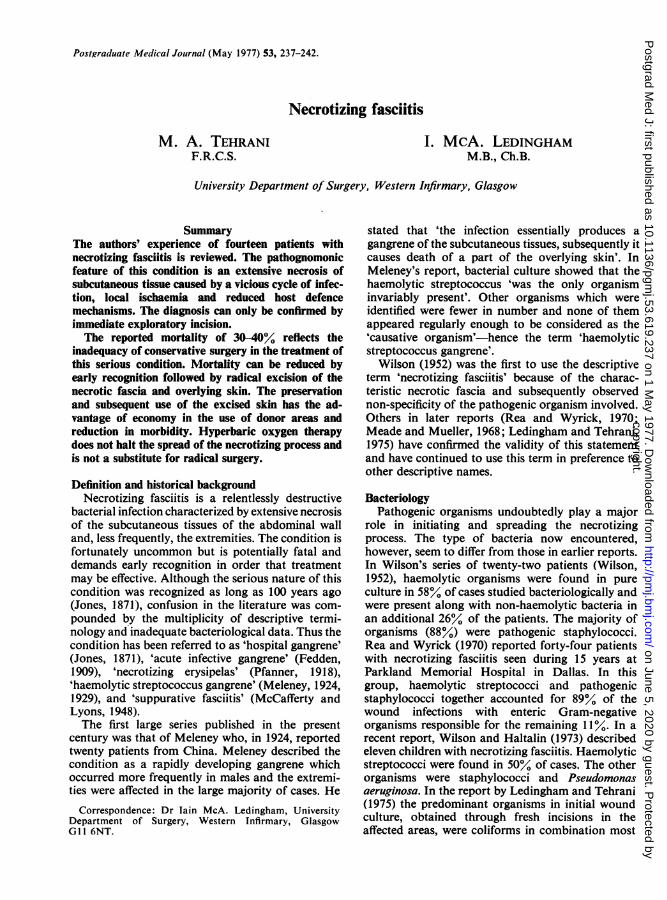
DiagnosisAt an early stage the external appearance of the
skin, in spite of the active underlying necrotizingprocess, is normal (Fig. 2a and b). Later the skinbecomes red, hot, and oedematous, with no clear lineof demarcation. Subsequently, dusky discolorationwith patchy necrosis of the skin occurs and theinvolved part, which is initially painful, becomesnumb. There is usually gross undermining of theskin. Co-incident with these local features of pro-gressive infection, the general condition of thepatient deteriorates. Toxaemia, dehydration andmental apathy ensue. Anaemia is a frequent occur-rence and is due to haemolysis, cutaneous hyper-aemia, loss of blood in extensive subcutaneousspaces and bone marrow depression. Hypoprotein-aemia, hyponatraemia and hypocalcaemia, conse-quent to extensive fat necrosis, also commonly occur.Other systemic manifestations of severe infectionsuch as disseminated intravascular coagulation,respiratory failure and septic shock lead to majorhaemodynamic disturbances. The majority of thepatients in the present series required continuoushaemodynamic monitoring in the Intensive Therapy
(a)
/~:~t4
·iFr:lI,
(b)~a~
FIG. 2. (a) Portion of excised normal skin overlying anarea affected by necrotizing fasciitis.(b) Undersurface of the same portion of skin showingfascial necrosis. By kind permission of the EditorialSecretary and Publisher of British Journal of Surgery.
Unit of the hospital. Death occurs as a result ofsepsis, respiratory or renal failure. Multi-organfailure, therefore, is the terminal event leading todeath in inadequately treated patients.The diagnosis should be established as rapidly as
possible by making small incisions in the affectedpart. The finding of gross undermining of the skinassociated with necrotic subcutaneous tissue ispathognomonic of the condition and calls for urgentappropriate therapeutic measures.The differential diagnosis from gas gangrene and
progressive bacterial gangrene should not prove tobe too difficult. Gas gangrene frequently occurs inassociation with penetrating wounds followingmajor trauma. Invasion of muscles by clostridialorganisms, crepitus and a 'mousy'-smelling dischargeare characteristic. Incision reveals a characteristicbluish appearance of muscle which does not bleed.Progressive bacterial gangrene is a more slowly pro-gressive lesion affecting the total thickness of skin
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.53.619.237 on 1 May 1977. D
ownloaded from
240 M. A. Tehrani and I. McA. Ledingham
but not involving the deep fascia. The condition,essentially a postoperative surgical complication,occurs as a result of the synergistic action of a non-haemolytic microaerophylic streptococcus withsome other organism (Meleney, 1933), althoughseveral other synergistic combinations have beenknown to produce the same lesion (Lyall and Stuart,1948; Webb and Berg, 1966). The lesion typicallyoccurs at the site of the drainage tube or around thelaparotomy wound. The initial cellulitis spreadscircumferentially and its centre becomes necrotic.The gangrenous ulcer may reach tremendous pro-portions. Surrounding the border of the gangrenousarea there is a tender purplish zone which in turn issurrounded by an area of oedematous red andtender skin. There is no undermining of the skin andthe subcutaneous tissues and deep fascia are pri-marily intact. Pus formation is variable. The impor-tance of an underlying systemic disease predisposingto the development of this condition should be bornein mind.
ManagementOnce the diagnosis is established, the aims of treat-
ment are two-fold. Firstly, general treatment andsecondly, local measures to eradicate the source ofinfection.
(I) General treatment consists of the administrationof intravenous fluid, large doses of appropriatesystemic antibiotics and, when necessary, resuscita-tive measures preferably in an Intensive TherapyUnit. The majority of the patients, particularly thosewith extensive trunk or lower limb involvement andthose in whom the diagnosis has been delayed,exhibit features of severe toxaemia and septic shock.The importance of adequate volume replacement,monitored by measurement of central venouspressure and hourly urine output and electrolytebalance cannot be overstressed. Frequent dailybacteriological swabs, taken from the involved areas,and blood cultures should be done to achievemaximum therapeutic benefit from antibiotictherapy. Particular attention should be paid topreventing the respiratory and renal complications socommonly encountered in patients with septic shock.Adequate oxygenation and, at times, assisted venti-lation with frequent blood gas estimation are re-quired. Digitalisation may be necessary to reduce therisk of cardiac complications of septic shock(Ledingham, 1975). Likewise, daily coagulationscreening is desirable for early detection of a con-sumptive coagulopathy. As part of general treatmentin particular when the lower extremities are involved,a defunctioning transverse colostomy is usuallyrequired to prevent contamination of the involvedareas.
(II) Local treatment. The principle of surgical
management as initially outlined by Meleney (1924),and subsequently emphasized by Wilson (1952),Crosthwait et al. (1964), Meade and Mueller (1968)and Rea and Wyrick (1970), consists of multiplelinear incisions over the affected area as far as thesubcutaneous necrosis extends, thus exposing theentire area of necrotizing fasciitis. The extent ofundermining is determined by passing a probe or byfinger dissection. Fasciotomy and debridement iscarried out to the limit of the undermined skin andsubcutaneous tissue until it no longer separates fromthe deep fascia. Meleney (1924) immersed the area inhot water and others used multiple drainage orfrequent daily antibiotic irrigation (Meade andMueller, 1968). The denuded area is grafted withsplit-thickness skin grafts at a later date.Although in some earlier reports, this relatively
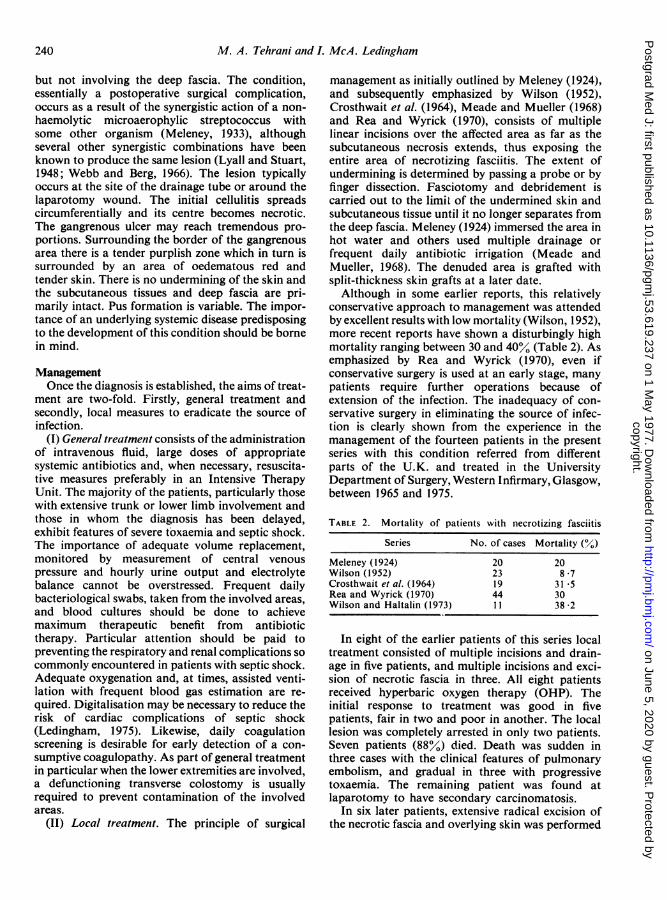
conservative approach to management was attendedby excellent results with low mortality (Wilson, 1952),more recent reports have shown a disturbingly highmortality ranging between 30 and 40% (Table 2). Asemphasized by Rea and Wyrick (1970), even ifconservative surgery is used at an early stage, manypatients require further operations because ofextension of the infection. The inadequacy of con-servative surgery in eliminating the source of infec-tion is clearly shown from the experience in themanagement of the fourteen patients in the presentseries with this condition referred from differentparts of the U.K. and treated in the UniversityDepartment of Surgery, Western Infirmary, Glasgow,between 1965 and 1975.
TABLE 2. Mortality of patients with necrotizing fasciitis
Series No. of cases Mortality (%)
Meleney (1924) 20 20Wilson (1952) 23 8-7Crosthwait et al. (1964) 19 31 -5Rea and Wyrick (1970) 44 30Wilson and Haltalin (1973) 11 38 2
In eight of the earlier patients of this series localtreatment consisted of multiple incisions and drain-age in five patients, and multiple incisions and exci-sion of necrotic fascia in three. All eight patientsreceived hyperbaric oxygen therapy (OHP). Theinitial response to treatment was good in fivepatients, fair in two and poor in another. The locallesion was completely arrested in only two patients.Seven patients (88%) died. Death was sudden inthree cases with the clinical features of pulmonaryembolism, and gradual in three with progressivetoxaemia. The remaining patient was found atlaparotomy to have secondary carcinomatosis.
In six later patients, extensive radical excision ofthe necrotic fascia and overlying skin was performed
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.53.619.237 on 1 May 1977. D
ownloaded from
Necrotizing fasciitis 241
(a)
(b)
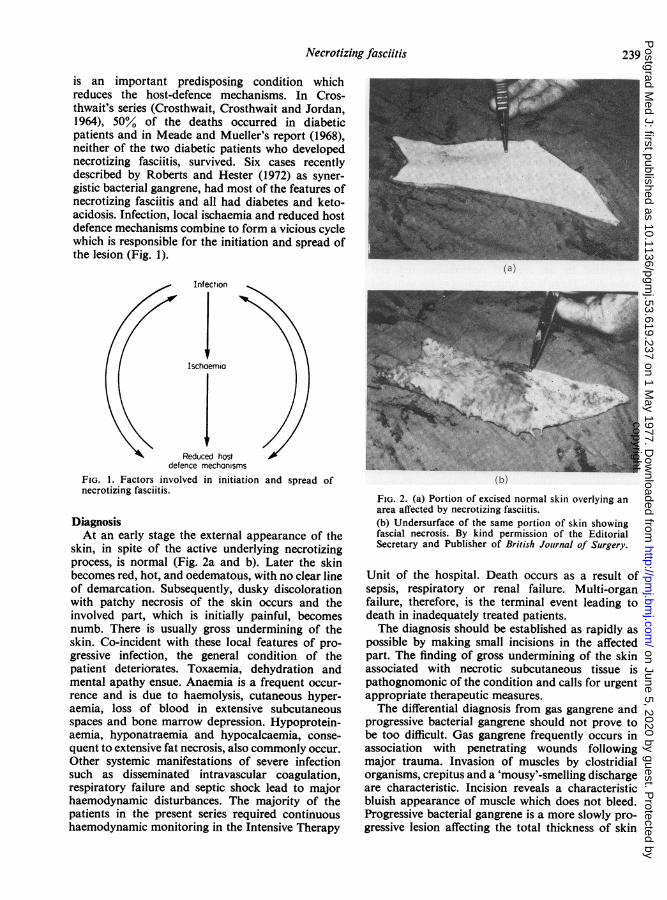
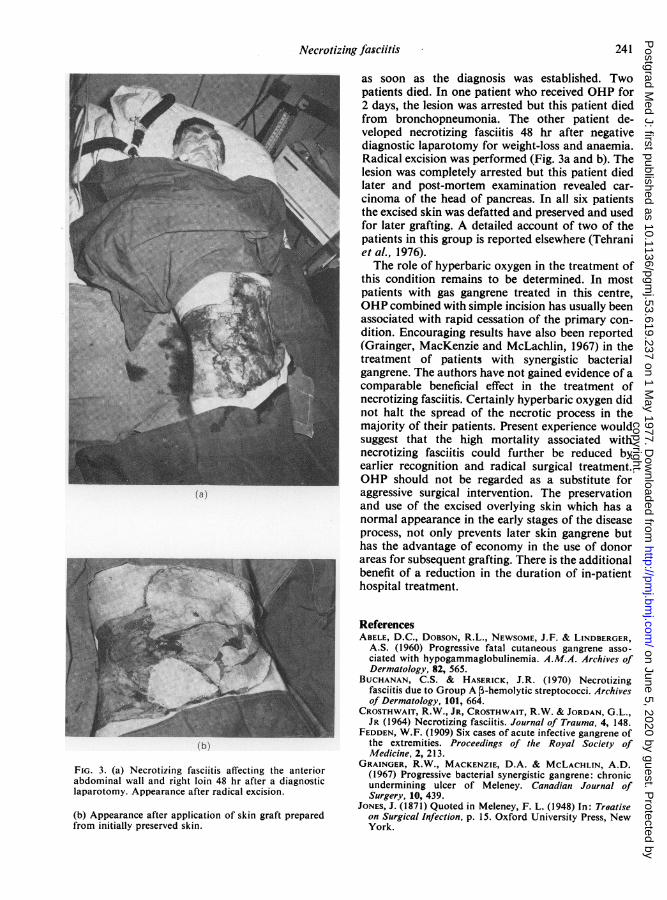
FIG. 3. (a) Necrotizing fasciitis affecting the anteriorabdominal wall and right loin 48 hr after a diagnosticlaparotomy. Appearance after radical excision.
(b) Appearance after application of skin graft preparedfrom initially preserved skin.
as soon as the diagnosis was established. Twopatients died. In one patient who received OHP for2 days, the lesion was arrested but this patient diedfrom bronchopneumonia. The other patient de-veloped necrotizing fasciitis 48 hr after negativediagnostic laparotomy for weight-loss and anaemia.Radical excision was performed (Fig. 3a and b). Thelesion was completely arrested but this patient diedlater and post-mortem examination revealed car-cinoma of the head of pancreas. In all six patientsthe excised skin was defatted and preserved and usedfor later grafting. A detailed account of two of thepatients in this group is reported elsewhere (Tehraniet al., 1976).The role of hyperbaric oxygen in the treatment of
this condition remains to be determined. In mostpatients with gas gangrene treated in this centre,OHP combined with simple incision has usually beenassociated with rapid cessation of the primary con-dition. Encouraging results have also been reported(Grainger, MacKenzie and McLachlin, 1967) in thetreatment of patients with synergistic bacterialgangrene. The authors have not gained evidence of acomparable beneficial effect in the treatment ofnecrotizing fasciitis. Certainly hyperbaric oxygen didnot halt the spread of the necrotic process in themajority of their patients. Present experience wouldsuggest that the high mortality associated withnecrotizing fasciitis could further be reduced byearlier recognition and radical surgical treatment.OHP should not be regarded as a substitute foraggressive surgical intervention. The preservationand use of the excised overlying skin which has anormal appearance in the early stages of the diseaseprocess, not only prevents later skin gangrene buthas the advantage of economy in the use of donorareas for subsequent grafting. There is the additionalbenefit of a reduction in the duration of in-patienthospital treatment.
ReferencesABELE, D.C., DOBSON, R.L., NEWSOME, J.F. & LINDBERGER,
A.S. (1960) Progressive fatal cutaneous gangrene asso-ciated with hypogammaglobulinemia. A.M.A. Archives ofDermatology, 82, 565.
BUCHANAN, C.S. & HASERICK, J.R. (1970) Necrotizingfasciitis due to Group A 3-hemolytic streptococci. Archivesof Dermatology, 101, 664.
CROSTHWAIT, R.W., JR, CROSTHWAIT, R.W. & JORDAN, G.L.,JR (1964) Necrotizing fasciitis. Journal of Trauma, 4, 148.
FEDDEN, W.F. (1909) Six cases of acute infective gangrene ofthe extremities. Proceedings of the Royal Society ofIMedicine, 2, 213.
GRAINGER, R.W., MACKENZIE, D.A. & MCLACHLIN, A.D.(1967) Progressive bacterial synergistic gangrene: chronicundermining ulcer of Meleney. Canadian Journal ofSurgery, 10, 439.
JONES, J. (1871) Quoted in Meleney, F. L. (1948) In: Treatiseon Surgical Infection, p. 15. Oxford University Press, NewYork.
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.53.619.237 on 1 May 1977. D
ownloaded from
242 M. A. Tehrani and I. McA. Ledingham
KELLAWAY, C.H., BURNET, F.M. & WILLIAMS, F.E. (1930)Pharmacological action of exotoxin of staphylococcus.Journal of Pathology and Bacteriology, 33, 889.
LEDINGHAM, I.McA. & TEHRANI, M.A. (1975) Diagnosis,clinical course and treatment of acute dermal gangrene.British Journal of Surgery, 62, 364.
LEDINGHAM, I.McA. (1975) Septic shock. British Journal ofSurgery, 62, 777.
LYALL, A. & STUART, R.D. (1948) Progressive postoperativegangrene of the skin. Observations on aetiology in twocases. Glasgow Medical Journal, 29, 1.
MCCAFFERTY, E.L. & LYONS, C. (1948) Suppurative fasciitisas the essential feature of haemolytic streptococcus gan-grene with notes on fasciotomy and early wound closure astreatment of choice. Surgery, St. Louis, etc., 24, 438.
MEADE, J.W. & MUELLER, C.B. (1968) Necrotizing infectionsof subcutaneous tissues and fascia. Annals of Surgery, 168,274.
MELENEY, F.L. (1924) Hemolytic streptococcus gangrene.Archives of Surgery. Chicago, 9, 317.
MELENEY, F.L. (1929) Hemolytic streptococcus gangrene:importance of early diagnosis and operation. Journal of theAmerican Medical Association, 92, 2009.
MELENEY, F.L. (1933) Differential diagnosis between certaintypes of infectious gangrene of the skin. Surgery, Gyne-cology and Obstetrics, 56, 847.
PFANNER, W. (1918) Zur kenntnis und Behandlung desnekrotisierenden Erysipels. Deutsche Zeitschrift furChirurgie, 144, 108.
REA, W.J. & WYRICK, W.J. (1970) Necrotizing fasciitis.Annals of Surgery, 172, 957.
ROBERTS, D.B. & HESTER, L.L. (1972) Progressive synergisticbacterial gangrene arising from abscesses of the vulva andBartholin's gland duct. American Journal of Obstetrics andGynecology, 114, 285.
TEHRANI, M.A., WEBSTER, M.H.C., ROBINSON, D.W. &LEDINGHAM, I.McA. (1976) Necrotising fasciitis treated byradical excision of the overlying skin. British Journal ofPlastic Surgery, 29, 74.
WEBB, R. & BERG, E. (1966) Symbiotic gangrene due toPseudomonas pyocyanea and E. coli. Australian and NewZealand Journal of Surgery, 36, 159.
WILSON, B. (1952) Necrotizing fasciitis. American Surgeon,18, 416.
WILSON, H.D. & HALTALIN, K. (1973) Acute necrotizingfasciitis in childhood. American Journal of Diseases ofChildren, 125, 591.
copyright. on June 5, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.53.619.237 on 1 May 1977. D
ownloaded from





























