Embed Size (px)
Citation preview

Clinical Radiology (1994) 49, 829-831
Case Report: Humero-spinal Dysostosis M. J. W. SPARKS, P. A. GAINES and R. K. LEVICK
Departments of Radiology, Children's and Royal Hallamshire Hospital, Sheffield
We report a case of humero-spinal dysostosis which is only the fourth reported in the literature. The condition is characterized by distal bifurcation of humeri, elbow joint dislocation, spinal malformation, widened iliac bones and talipes equinovarus. Sparks, M.J.W., Gaines, P.A. & Levick, R.K. (1994). Clinical Radiology 49, 829-831. Case Report: Humero-spinal Dysostosis
CASE REPORT
A male child, now aged 11 years, was born after a normal pregnancy at full term in the breech position. The birth weight was 71b 8oz. There was no family history of congenital abnormali ty.
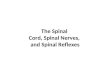
On examination at birth the child was described as healthy and well built. There was right-sided talipes equinovarus and anterior subluxation of the left knee (Fig. 1). Subsequent examination revealed more extensive and widespread abnormalities. In the lumbar spine, the interpedicular distance at L1 was normal for age but the spinal canal narrowed distally (Fig. 2). The vertebrae were morphologically abnormal with tall, narrow bodies (Fig. 3). The pelvis showed broadening of the iliac blades with narrow sciatic notches (Fig. 4). The femoral necks were wide and convex in their upper borders with prominent greater trochanters (Fig. 5). Characteristically the distal humeri were bifid with radiohumeral dislocation on the right side (Fig. 6).
At 4 years of age it was apparent that the thoraco-lumbar develop- ment was disproportionate, with normal thoracic cage development, but with short and undeveloped lumbar spine. As growth continued femoral modelling improved but he later developed bilateral avascular necrosis of the femoral heads by the age of 10 years (Fig. 7).
Apart from his skeletal abnormalities, the child had no cardiac, gastrointestinal or urological problem and remains well.
Koslowski et al. [1] in 1974 and subsequently by Cortina et al. [2] in 1979.
In the cases reported by Koslowski et al. [1] the condition was characterized by bifid distal humeri, sub- luxation of the elbow joints, shortening and hypotubula- tion of the long bones, widening of the iliac bones, talipes equinovarus and coronal clefts in the vertebral bodies. Widening of the interpedicular distance at L1, with narrowing distally of the spinal canal, was also a feature. In addition, both cases suffered cardiac abnormality. Other generalized skeletal disorders are often associated with cardiac abnormalities and these include the Marfan [3], Holt-Oram [4] and Ellis-van Creveld [5] syndromes, but the characteristic feature of humero-spinal dysostosis is the bifid distal humeri not seen in other disorders.
DISCUSSION
Humero-spinal dysostosis was first reported by
Fig. 1 - Left knee showing anterior subluxation of tibia at the knee joint."
Correspondence to: Dr M. J. W. Sparks, Department of Radiology, Children's and Royal Hallamshire Hospital, Glossop Road, Sheffield S10 2JF.
Fig. 2 - Interpedicular distance at L1 17mm at 6 months with progressive narrowing of the spinal canal distally.

830 CLINICAL RADIOLOGY
Fig. 5 - Wide femoral necks with convex upper border and prominent greater trochanter.
Fig. 3 - Abnormal morphology of the vertebral bodies at L4 and L5 which are tall and narrow.
Fig. 4 - lliac blades are broad with narrow, sharply-angled sciatic notches.
(a)
Fig. 6 (a,b) Bifid distal humeri with radio-humeral subluxation.

CASE REPORTS 831
Fig. 6 (b)
Fig. 7 - Changes of bilateral avascular necrosis of the capital femoral epiphysis.
The case repor ted by Cor t ina e t aL [2] showed similar rad iographic appearances with the addi t ion o f subluxa- t ion o f knees. N o significant cardiac or o ther abnormal i ty was found. The corona l clefting in the vertebral bodies was found as a t empora ry feature, regressing in early life. Corona l clefting is a feature seen in some normal chil- dren, d isappear ing in the first few weeks o f life, and is seen in some other skeletal disorders. In puncta te epiphyseal dysplasia, clefts [6,7] may persist for life and in the Wei s senbache r -Zweymul l e r syndrome [8,9] clefts are present at bir th but regress after several weeks.
The case we r epor t has mos t of the features descr ibed in the three previous cases repor ted , bu t wi thou t the corona l cleft ing of the ver tebra l bodies .
Acknowledgement. We would like to thank Mr M. J. Bell, Orthopaedic Department, Royal Hallamshire Hospital, for his help and permission to report this case.
REFERENCES
1 Koslowski KS, Celermajer JM, Tink AR. Humero-spinal dysostosis with congenital heart disease. American Journal of Diseases of Children 1974;127:407-410. Cortina H, Vidal J, Vallcanera A et al. Humero-spinal dysostosis. Paediatric Radiology 1979;8:188-190. Pyeritz R, McCusick V. The Marfan syndrome: diagnosis and management. New England Journal of Medicine 1979;300:772-776. Holt, M, Oram, S. Familial heart defect with skeletal involvement. British Heart Journal 1960;22:236. Ellis R, van Crefeld S. A syndrome characterized by ectodermal dysplasia, polydactyly, chondrodystrophia and congenital morbis cordis. Archives of Disease in Childhood 1940;15:65. Sheffield L, Danks D, Mayne Vet al. Chondrodysplasia punctata - 23 cases of a mild and relatively common variety. Journal of Paediatrics 1976;89(6):916 923. Heselson N, Cremin B, Beighton P. Lethal chondrodysplasia punctata. Clinical Radiology 1978;29:679 684. Cortina H, Aperici R, Beltran J et al. The Weissenbacher- Zweymuller syndrome. Paediatric Radiology 1977;6:109-111. Hailer J, Berdon W, Robinow Met al. The Weissenbacher-Zweymuller syndrome. American Journal of Roentgenology 1975; 125:936.