Embed Size (px)
Citation preview

Case ReportCytomegalovirus Uveitis with Hypopyon MimickingBacterial Endophthalmitis
Atsushi Yoshida Hiroto Obata and Hidetoshi Kawashima
Department of Ophthalmology Jichi Medical University 3311-1 Yakushiji Tochigi Shimotsuke 329-0498 Japan
Correspondence should be addressed to Atsushi Yoshida a-yosidasageocnnejp
Received 2 March 2015 Accepted 24 April 2015
Academic Editor Antonio Ferreras
Copyright copy 2015 Atsushi Yoshida et alThis is an open access article distributed under the Creative CommonsAttribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
We report an 83-year-old immune-competent female with unilateral endophthalmitis extraordinarily caused by cytomegalovirus(CMV) Since she was suspected of suffering possible bacterial endophthalmitis she was referred to our hospital At the first visithypopyon in the anterior chamber and the opacity of vitreous body were observed in the left eye The best-corrected visual acuity(BCVA) of the left eye was counting fingers and the intraocular pressure (IOP) was 20mmHg Bacterial and fungus culture of theaqueous humor revealed no infection However the density of corneal endothelial cell was less than the measurable range andCMV was detected by PCR of the aqueous humor She was immune-competent and the data indicated neither systemic infectionsnor diseases Systemic valganciclovir and corticosteroid were administered After that hypopyon in the anterior chamber and theopacity of vitreous body of the left eye were improved and the BCVA of the left eye was 20200 one year after the first visit Howeverthe inflammation of the anterior chamber recurred accompanied by elevated IOP after the discontinuance of administeringvalganciclovir CMV-induced uveitis accompanied with hypopyon is quite rareTherefore it can be easily misdiagnosed as bacterialendophthalmitis
1 Introduction
Cytomegalovirus (CMV) is a member of the human herpesvirus family It is known that CMV infection induces retinitisanterior uveitis or endothelial keratitis [1ndash6] while endoph-thalmitis is an intraocular inflammation due to variousbacteria and fungi after intraocular surgeries or systemicinfection [7] CMV anterior uveitis and corneal endotheliitisare unilateral recurrent or chronic and steroid-refractorythough CMV retinitis is characterized by slowly spreadingretinal necrosis in patients who have impaired T-cell functionas a result of transplantation acquired immune deficiencysyndrome (AIDS) or immune-suppressive treatment Theclinical presentations of CMV anterior uveitis or cornealendotheliitis are endothelial cell loss local stromal edema ofthe cornea and keratic precipitates sometimes accompaniedby raised IOP [1ndash4] We experienced an immune-competentpatient who developed endophthalmitis with hypopyon dueto cytomegalovirus infection
2 Case Report
An 83-year-old woman was referred to our hospital from alocal ophthalmologist claiming that she developed bacterialendophthalmitis She had suffered reduced visual acuity ofthe left eye two weeks ago She had undergone bilateraltrabeculectomy for primary open angle glaucoma 20 yearsago and bilateral cataract surgery 15 years ago Otherwise shehad had no illness systemically
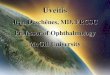
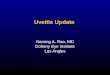
At the first visit hypopyon in the anterior chamber(Figure 1) was observed in the left eye Her best-correctedvisual acuity (BCVA) was 2020 in the right eye and countingfingers in the left eye the intraocular pressures (IOPs) of theright and left eyes were 15mmHg and 20mmHg and thedensities of corneal endothelial cell of the right and left eyeswere 1500 cellsmm2 and 800 cellsmm2 The fundus of theleft eye could not be observed because of the opacity of thevitreous body The image of B-scan ocular ultrasound of theleft eye showed vitreous opacity without retinal detachment
Hindawi Publishing CorporationCase Reports in Ophthalmological MedicineVolume 2015 Article ID 489813 4 pageshttpdxdoiorg1011552015489813
2 Case Reports in Ophthalmological Medicine
Figure 1 Photograph of the anterior segment in the left eye at thefirst visit Hypopyon in the anterior chamber ciliary hyperemia andcorneal epithelium and stoma edema were observed
The systemic data indicated neither systemic infectionsnor diseasesThe body temperature was 362∘C Blood exam-inations revealed that the white blood cell counting was 50 times103 cells120583L CRP was 009mgdL and HIV was negativeMoreover the serous Ig M of varicella zoster virus (VZV)herpes simplex virus (HSV) and CMV were negative ChestX-ray photograph chest computed tomography (CT) andabdomen CT did not show abnormal symptom
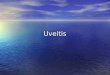
Bacterial and fungus culture and qualitative polymerasechain reaction (PCR) for VZV HSV and CMV were per-formed The aqueous humor (02mL) of the left eye wasdivided into two equal parts One part was used for bacterialand fungus culture and the other for qualitative PCR anal-ysis which was performed by a laboratory company (SRLTokyo Japan) Consequently neither bacterial nor fungusinfections were detected PCR analysis revealed that CMVwas positive while VZV and HSV were negative For sevendays before we received the results of culture and PCRintravenous administration of broad spectrum antibiotics(imipenemcilastatin) at the dose of 10 gday oral adminis-tration of prednisolone at the dose of 20mgday eye drops ofantibiotics (ceftazidime and vancomycin) at hourly intervalsand one intravitreal injection of antibiotics (ceftazidime andvancomycin) at the dose of 20mg and 10mg respectivelyhad been performed However intraocular inflammation didnot improve We were hesitant to apply vitreous surgerysince the IOP was 7mmHg and the density of cornealendothelial cell was less than the measurable range (less than500 cellsmm3) Eventually qualitative PCR of the aqueoushumor revealed that only CMV is present Thus the admin-istering of systemic valganciclovir (1800mgday) in additionto prednisolone (20mgday) was started Ceftazidime andvancomycin were given only as eye drops At the 7th dayafter the beginning of valganciclovir hypopyon in the leftanterior chamber disappeared (Figure 2) However the IOPof the left eye increased at the level of 30mmHg Thereforeacetazolamide was administered additionally At the 2nd
Figure 2 Photograph of the anterior segment of the left eye atthe 7th day after the beginning of valganciclovir Hypopyon inthe anterior chamber ciliary hyperemia and corneal edema haddisappeared It was revealed that intraocular lens was in the lenscapsule bag treated with posterior capsulotomy
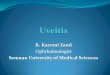
Figure 3 Panorama photograph of the fundus in the left eye at the2nd week after the beginning of valganciclovir Since hypopyon andvitreous opacity had disappeared the fundus of the left eye could beobserved enough No inflammation sign could be observed at thefundus
week after the beginning of valganciclovir the fundus of theleft eye could be observed enough and no inflammation signon the fundus could be observed (Figure 3) Several monthslater the administration of valganciclovir prednisolone andacetazolamide was discontinued Three months after thediscontinuance of valganciclovir anterior uveitis recurredand the IOP of the left eye increased at the level of 30mmHgHowever the recurrence of hypopyon and the opacity ofthe vitreous body were not observed Oral valganciclovir(900mgday) and oral acetazolamide (500mgday) and 01betamethasone as eye drops were readministered Althoughthe IOP of the left eye improved the density of cornealendothelial cell of the left eye could not be measured since itwas too lowThe readministration of valganciclovir had beenmaintained for four months At the time of the discontinu-ance of the administration the BCVA and the IOP of the lefteye were almost 20200 and 20mmHg
Case Reports in Ophthalmological Medicine 3
BCVA
CF
IOP
(mm
Hg)
IOP in the left eyeBCVA of the left eye
302010
ReoccurrenceAd Dis
MonthsSteroid eye drops
IMPPSLVG
ACT
3 w
eeks0 2 4 6 8 10 12 14 16 18 20 22 24
202000202002020
10 g
20mg10
1800mg 900
500mg
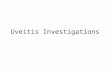
Figure 4 Clinical course of the left eye during two years after the first visit Ad admission dis discharge (998787) recurrence of inflammation ofthe anterior chamber (998771) injection of ceftazidime and vancomycin ( loz) eye drops of ceftazidime and vancomycin IMP imipenemcilastatinPSL prednisolone VG valganciclovir and ACT acetazolamide (mdash) best-corrected visual acuity (BCVA) (- - -) intraocular pressure (IOP)and CF visual acuity of counting fingers
Subsequently the inflammation of the anterior chamberoften recurred accompanied by raised IOP after the discon-tinuance of administering valganciclovir Two years after thefirst visit due to corneal opacity the BCVA of the left eyedecreased to 201000The clinical course of the left eye (visualacuity IOP and treatment) during two years after the first visitis shown in Figure 4 During the observation period we hadperformedneither broad range PCRnormultiplex PCR sincewe could not get patientrsquos consent
3 Discussion
Since this patient had bilateral trabeculectomy for primaryopen angle glaucoma and bilateral cataract surgery shewas speculated to suffer infectious endophthalmitis at thefirst visit However it had been too long an interval sincethose surgeries The conjunctival bleb of the left eye wasflat and nonfunctional and the symptom of blebitis wasnot evident Both systemic and topical antibiotics wereineffective and neither bacterial nor fungus infections couldbe detected in the cultured aqueous humor of the left eyeThesystemic examinations indicated the patient was immune-competent and suffered from neither systemic infectionnor systemic autoimmune disease PCR examinations ofthe anterior humor are useful in differentiating betweenCMV and other herpes viruses and in making a definitediagnosis in anterior uveitis or corneal endotheliitis [8]Since CMV was detected by qualitative PCR of the aqueoushumor of the current patient we changed the therapeuticstrategy to valganciclovir and prednisolone QuantitativePCR (broad range PCR and multiplex PCR) would addto the weight of diagnosis of CMV-induced uveitis if hightiter was demonstrated However quantitative PCR wasnot available The prompt effectiveness of valganciclovirand the recurrence of intraocular inflammation after thediscontinuance of valganciclovir indicated that CMV wasthe cause of the endophthalmitis-like uveitis However as
far as the author searched neither immune-competent CMVanterior uveitis nor corneal endotheliitis accompanied withhypopyon in the anterior chamber was reported in the pastalthough several immunocompromised patients with CMVuveitis accompanied with hypopyon were reported [9ndash11]Consequently the reason why the patient had such severeinflammation as hypopyon was still unclear The vitreousopacity of the left eye might have resulted from posteriorcapsulotomy for after-cataract surgery The inflammation ofthe anterior chamber might have spread into the vitreousbody through the capsulotomy hole
It has been reported that CMV or other herpes virus-induced uveitis was often accompanied with diffuse irisstromal atrophy [5 12 13] As for the current patient atthe first visit the pupillary light reflex in the left eye hadbeen lost perfectly compared with that in the right eyealthough depigmentation of the iris was not clear Thus itwas speculated that peripupillary atrophy caused by CMVinfection had been existing in the left eye for a long time
A small amount of systemic administration of corti-costeroid together with antibiotics is generally effective inthe treatments for bacterial endophthalmitis since severeintraocular infections are accompanied with secondaryinflammation which requires anti-inflammatory treatmentsLikewise we thought it was effective to administer a smallamount of systemic corticosteroid together with anti-CMVagent against severeCMV-induced uveitis accompaniedwithhypopyon in the anterior chamber and the opacity of thevitreous body Thus we continued to administer oral pred-nisolone for the current patient after PCR analysis revealedthat CMV was positive
Treatment strategy for recurrent CMV anterior uveitis(or corneal endotheliitis) has not been enough establishedyet though systemic or intravitreal anti-CMV treatment iseffective for CMV anterior uveitis [13ndash15] More clinicalinvestigations are needed
4 Case Reports in Ophthalmological Medicine
CMV-induced immune-competent anterior uveitisaccompanied with hypopyon is quite rare and might bemisdiagnosed as bacterial endophthalmitis It might recurafter the discontinuance of administering valganciclovir Wereconfirmed that PCR examination of the aqueous humorwas useful in diagnosing and deciding the treatment for suchpatients as in our case
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] A Carmichael ldquoCytomegalovirus and the eyerdquo Eye vol 26 no2 pp 237ndash240 2012
[2] A Radwan J L Metzinger D M Hinkle and C S FosterldquoCytomegalovirus retinitis in immunocompetent patients casereports and literature reviewrdquo Ocular Immunology and Inflam-mation vol 21 no 4 pp 324ndash328 2013
[3] K Toriyama T Suzuki Y Hara and Y Ohashi ldquoCytome-galovirus retinitis aftermultiple ocular surgeries in an immuno-competent patientrdquo Case Reports in Ophthalmology vol 3 no3 pp 356ndash359 2012
[4] M Miyanaga S Sugita N Shimizu et al ldquoA significant asso-ciation of viral loads with corneal endothelial cell damage incytomegalovirus anterior uveitisrdquo British Journal of Ophthal-mology vol 94 no 3 pp 336ndash340 2010
[5] S-P Chee K Bacsal A Jap S-Y Se-Thoe C L Chengand B H Tan ldquoClinical features of cytomegalovirus anterioruveitis in immunocompetent patientsrdquoTheAmerican Journal ofOphthalmology vol 145 no 5 pp 834e1ndash840e1 2008
[6] S-P Chee and A Jap ldquoCytomegalovirus anterior uveitis out-come of treatmentrdquo British Journal of Ophthalmology vol 94no 12 pp 1648ndash1652 2010
[7] M S Kresloff A A Castellarin and M A Zarbin ldquoEndoph-thalmitisrdquo Survey of Ophthalmology vol 43 no 3 pp 193ndash2241998
[8] S Sugita M Ogawa N Shimizu et al ldquoUse of a comprehensivepolymerase chain reaction system for diagnosis of ocularinfectious diseasesrdquo Ophthalmology vol 120 no 9 pp 1761ndash1768 2013
[9] L C Chumbley D M Robertson T F Smith and R JCampbell ldquoAdult cytomegalovirus inclusion retino uveitisrdquoAmerican Journal of Ophthalmology vol 80 no 5 pp 807ndash8161975
[10] J Biswas S Choudhry and S Solomon ldquoImmune recoveryvitritis presenting as panuveitis following therapy with proteaseinhibitorsrdquo Indian Journal of Ophthalmology vol 48 no 4 pp313ndash315 2000
[11] L Figueiredo R Rothwell M Bilhoto R Varandas and SFonseca ldquoImmune recovery uveitis masked as an endogenousendophthalmitis in a patient with active CMV retinitisrdquo CaseReports in Ophthalmological Medicine vol 2013 Article ID462968 4 pages 2013
[12] J HWooWK Lim S LHo and S C Teoh ldquoCharacteristics ofcytomegalovirus uveitis in immunocompetent patientsrdquoOcularImmunology amp Inflammation 2014
[13] L A A van Boxtel A van der Lelij J van der Meer andL I Los ldquoCytomegalovirus as a cause of anterior uveitis in
immunocompetent patientsrdquoOphthalmology vol 114 no 7 pp1358ndash1362 2007
[14] I de Schryver F Rozenberg N Cassoux et al ldquoDiagnosisand treatment of cytomegalovirus iridocyclitis without retinalnecrosisrdquo British Journal of Ophthalmology vol 90 no 7 pp852ndash855 2006
[15] H Mietz S Aisenbrey K U Bartz-Schmidt S Bamborschkeand G K Krieglstein ldquoGanciclovir for the treatment of anterioruveitisrdquo Graefersquos Archive for Clinical and Experimental Ophthal-mology vol 238 no 11 pp 905ndash909 2000
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Ophthalmological Medicine
Figure 1 Photograph of the anterior segment in the left eye at thefirst visit Hypopyon in the anterior chamber ciliary hyperemia andcorneal epithelium and stoma edema were observed
The systemic data indicated neither systemic infectionsnor diseasesThe body temperature was 362∘C Blood exam-inations revealed that the white blood cell counting was 50 times103 cells120583L CRP was 009mgdL and HIV was negativeMoreover the serous Ig M of varicella zoster virus (VZV)herpes simplex virus (HSV) and CMV were negative ChestX-ray photograph chest computed tomography (CT) andabdomen CT did not show abnormal symptom
Bacterial and fungus culture and qualitative polymerasechain reaction (PCR) for VZV HSV and CMV were per-formed The aqueous humor (02mL) of the left eye wasdivided into two equal parts One part was used for bacterialand fungus culture and the other for qualitative PCR anal-ysis which was performed by a laboratory company (SRLTokyo Japan) Consequently neither bacterial nor fungusinfections were detected PCR analysis revealed that CMVwas positive while VZV and HSV were negative For sevendays before we received the results of culture and PCRintravenous administration of broad spectrum antibiotics(imipenemcilastatin) at the dose of 10 gday oral adminis-tration of prednisolone at the dose of 20mgday eye drops ofantibiotics (ceftazidime and vancomycin) at hourly intervalsand one intravitreal injection of antibiotics (ceftazidime andvancomycin) at the dose of 20mg and 10mg respectivelyhad been performed However intraocular inflammation didnot improve We were hesitant to apply vitreous surgerysince the IOP was 7mmHg and the density of cornealendothelial cell was less than the measurable range (less than500 cellsmm3) Eventually qualitative PCR of the aqueoushumor revealed that only CMV is present Thus the admin-istering of systemic valganciclovir (1800mgday) in additionto prednisolone (20mgday) was started Ceftazidime andvancomycin were given only as eye drops At the 7th dayafter the beginning of valganciclovir hypopyon in the leftanterior chamber disappeared (Figure 2) However the IOPof the left eye increased at the level of 30mmHg Thereforeacetazolamide was administered additionally At the 2nd
Figure 2 Photograph of the anterior segment of the left eye atthe 7th day after the beginning of valganciclovir Hypopyon inthe anterior chamber ciliary hyperemia and corneal edema haddisappeared It was revealed that intraocular lens was in the lenscapsule bag treated with posterior capsulotomy
Figure 3 Panorama photograph of the fundus in the left eye at the2nd week after the beginning of valganciclovir Since hypopyon andvitreous opacity had disappeared the fundus of the left eye could beobserved enough No inflammation sign could be observed at thefundus
week after the beginning of valganciclovir the fundus of theleft eye could be observed enough and no inflammation signon the fundus could be observed (Figure 3) Several monthslater the administration of valganciclovir prednisolone andacetazolamide was discontinued Three months after thediscontinuance of valganciclovir anterior uveitis recurredand the IOP of the left eye increased at the level of 30mmHgHowever the recurrence of hypopyon and the opacity ofthe vitreous body were not observed Oral valganciclovir(900mgday) and oral acetazolamide (500mgday) and 01betamethasone as eye drops were readministered Althoughthe IOP of the left eye improved the density of cornealendothelial cell of the left eye could not be measured since itwas too lowThe readministration of valganciclovir had beenmaintained for four months At the time of the discontinu-ance of the administration the BCVA and the IOP of the lefteye were almost 20200 and 20mmHg
Case Reports in Ophthalmological Medicine 3
BCVA
CF
IOP
(mm
Hg)
IOP in the left eyeBCVA of the left eye
302010
ReoccurrenceAd Dis
MonthsSteroid eye drops
IMPPSLVG
ACT
3 w
eeks0 2 4 6 8 10 12 14 16 18 20 22 24
202000202002020
10 g
20mg10
1800mg 900
500mg
Figure 4 Clinical course of the left eye during two years after the first visit Ad admission dis discharge (998787) recurrence of inflammation ofthe anterior chamber (998771) injection of ceftazidime and vancomycin ( loz) eye drops of ceftazidime and vancomycin IMP imipenemcilastatinPSL prednisolone VG valganciclovir and ACT acetazolamide (mdash) best-corrected visual acuity (BCVA) (- - -) intraocular pressure (IOP)and CF visual acuity of counting fingers
Subsequently the inflammation of the anterior chamberoften recurred accompanied by raised IOP after the discon-tinuance of administering valganciclovir Two years after thefirst visit due to corneal opacity the BCVA of the left eyedecreased to 201000The clinical course of the left eye (visualacuity IOP and treatment) during two years after the first visitis shown in Figure 4 During the observation period we hadperformedneither broad range PCRnormultiplex PCR sincewe could not get patientrsquos consent
3 Discussion
Since this patient had bilateral trabeculectomy for primaryopen angle glaucoma and bilateral cataract surgery shewas speculated to suffer infectious endophthalmitis at thefirst visit However it had been too long an interval sincethose surgeries The conjunctival bleb of the left eye wasflat and nonfunctional and the symptom of blebitis wasnot evident Both systemic and topical antibiotics wereineffective and neither bacterial nor fungus infections couldbe detected in the cultured aqueous humor of the left eyeThesystemic examinations indicated the patient was immune-competent and suffered from neither systemic infectionnor systemic autoimmune disease PCR examinations ofthe anterior humor are useful in differentiating betweenCMV and other herpes viruses and in making a definitediagnosis in anterior uveitis or corneal endotheliitis [8]Since CMV was detected by qualitative PCR of the aqueoushumor of the current patient we changed the therapeuticstrategy to valganciclovir and prednisolone QuantitativePCR (broad range PCR and multiplex PCR) would addto the weight of diagnosis of CMV-induced uveitis if hightiter was demonstrated However quantitative PCR wasnot available The prompt effectiveness of valganciclovirand the recurrence of intraocular inflammation after thediscontinuance of valganciclovir indicated that CMV wasthe cause of the endophthalmitis-like uveitis However as
far as the author searched neither immune-competent CMVanterior uveitis nor corneal endotheliitis accompanied withhypopyon in the anterior chamber was reported in the pastalthough several immunocompromised patients with CMVuveitis accompanied with hypopyon were reported [9ndash11]Consequently the reason why the patient had such severeinflammation as hypopyon was still unclear The vitreousopacity of the left eye might have resulted from posteriorcapsulotomy for after-cataract surgery The inflammation ofthe anterior chamber might have spread into the vitreousbody through the capsulotomy hole
It has been reported that CMV or other herpes virus-induced uveitis was often accompanied with diffuse irisstromal atrophy [5 12 13] As for the current patient atthe first visit the pupillary light reflex in the left eye hadbeen lost perfectly compared with that in the right eyealthough depigmentation of the iris was not clear Thus itwas speculated that peripupillary atrophy caused by CMVinfection had been existing in the left eye for a long time
A small amount of systemic administration of corti-costeroid together with antibiotics is generally effective inthe treatments for bacterial endophthalmitis since severeintraocular infections are accompanied with secondaryinflammation which requires anti-inflammatory treatmentsLikewise we thought it was effective to administer a smallamount of systemic corticosteroid together with anti-CMVagent against severeCMV-induced uveitis accompaniedwithhypopyon in the anterior chamber and the opacity of thevitreous body Thus we continued to administer oral pred-nisolone for the current patient after PCR analysis revealedthat CMV was positive
Treatment strategy for recurrent CMV anterior uveitis(or corneal endotheliitis) has not been enough establishedyet though systemic or intravitreal anti-CMV treatment iseffective for CMV anterior uveitis [13ndash15] More clinicalinvestigations are needed
4 Case Reports in Ophthalmological Medicine
CMV-induced immune-competent anterior uveitisaccompanied with hypopyon is quite rare and might bemisdiagnosed as bacterial endophthalmitis It might recurafter the discontinuance of administering valganciclovir Wereconfirmed that PCR examination of the aqueous humorwas useful in diagnosing and deciding the treatment for suchpatients as in our case
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] A Carmichael ldquoCytomegalovirus and the eyerdquo Eye vol 26 no2 pp 237ndash240 2012
[2] A Radwan J L Metzinger D M Hinkle and C S FosterldquoCytomegalovirus retinitis in immunocompetent patients casereports and literature reviewrdquo Ocular Immunology and Inflam-mation vol 21 no 4 pp 324ndash328 2013
[3] K Toriyama T Suzuki Y Hara and Y Ohashi ldquoCytome-galovirus retinitis aftermultiple ocular surgeries in an immuno-competent patientrdquo Case Reports in Ophthalmology vol 3 no3 pp 356ndash359 2012
[4] M Miyanaga S Sugita N Shimizu et al ldquoA significant asso-ciation of viral loads with corneal endothelial cell damage incytomegalovirus anterior uveitisrdquo British Journal of Ophthal-mology vol 94 no 3 pp 336ndash340 2010
[5] S-P Chee K Bacsal A Jap S-Y Se-Thoe C L Chengand B H Tan ldquoClinical features of cytomegalovirus anterioruveitis in immunocompetent patientsrdquoTheAmerican Journal ofOphthalmology vol 145 no 5 pp 834e1ndash840e1 2008
[6] S-P Chee and A Jap ldquoCytomegalovirus anterior uveitis out-come of treatmentrdquo British Journal of Ophthalmology vol 94no 12 pp 1648ndash1652 2010
[7] M S Kresloff A A Castellarin and M A Zarbin ldquoEndoph-thalmitisrdquo Survey of Ophthalmology vol 43 no 3 pp 193ndash2241998
[8] S Sugita M Ogawa N Shimizu et al ldquoUse of a comprehensivepolymerase chain reaction system for diagnosis of ocularinfectious diseasesrdquo Ophthalmology vol 120 no 9 pp 1761ndash1768 2013
[9] L C Chumbley D M Robertson T F Smith and R JCampbell ldquoAdult cytomegalovirus inclusion retino uveitisrdquoAmerican Journal of Ophthalmology vol 80 no 5 pp 807ndash8161975
[10] J Biswas S Choudhry and S Solomon ldquoImmune recoveryvitritis presenting as panuveitis following therapy with proteaseinhibitorsrdquo Indian Journal of Ophthalmology vol 48 no 4 pp313ndash315 2000
[11] L Figueiredo R Rothwell M Bilhoto R Varandas and SFonseca ldquoImmune recovery uveitis masked as an endogenousendophthalmitis in a patient with active CMV retinitisrdquo CaseReports in Ophthalmological Medicine vol 2013 Article ID462968 4 pages 2013
[12] J HWooWK Lim S LHo and S C Teoh ldquoCharacteristics ofcytomegalovirus uveitis in immunocompetent patientsrdquoOcularImmunology amp Inflammation 2014
[13] L A A van Boxtel A van der Lelij J van der Meer andL I Los ldquoCytomegalovirus as a cause of anterior uveitis in
immunocompetent patientsrdquoOphthalmology vol 114 no 7 pp1358ndash1362 2007
[14] I de Schryver F Rozenberg N Cassoux et al ldquoDiagnosisand treatment of cytomegalovirus iridocyclitis without retinalnecrosisrdquo British Journal of Ophthalmology vol 90 no 7 pp852ndash855 2006
[15] H Mietz S Aisenbrey K U Bartz-Schmidt S Bamborschkeand G K Krieglstein ldquoGanciclovir for the treatment of anterioruveitisrdquo Graefersquos Archive for Clinical and Experimental Ophthal-mology vol 238 no 11 pp 905ndash909 2000
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Ophthalmological Medicine 3
BCVA
CF
IOP
(mm
Hg)
IOP in the left eyeBCVA of the left eye
302010
ReoccurrenceAd Dis
MonthsSteroid eye drops
IMPPSLVG
ACT
3 w
eeks0 2 4 6 8 10 12 14 16 18 20 22 24
202000202002020
10 g
20mg10
1800mg 900
500mg
Figure 4 Clinical course of the left eye during two years after the first visit Ad admission dis discharge (998787) recurrence of inflammation ofthe anterior chamber (998771) injection of ceftazidime and vancomycin ( loz) eye drops of ceftazidime and vancomycin IMP imipenemcilastatinPSL prednisolone VG valganciclovir and ACT acetazolamide (mdash) best-corrected visual acuity (BCVA) (- - -) intraocular pressure (IOP)and CF visual acuity of counting fingers
Subsequently the inflammation of the anterior chamberoften recurred accompanied by raised IOP after the discon-tinuance of administering valganciclovir Two years after thefirst visit due to corneal opacity the BCVA of the left eyedecreased to 201000The clinical course of the left eye (visualacuity IOP and treatment) during two years after the first visitis shown in Figure 4 During the observation period we hadperformedneither broad range PCRnormultiplex PCR sincewe could not get patientrsquos consent
3 Discussion
Since this patient had bilateral trabeculectomy for primaryopen angle glaucoma and bilateral cataract surgery shewas speculated to suffer infectious endophthalmitis at thefirst visit However it had been too long an interval sincethose surgeries The conjunctival bleb of the left eye wasflat and nonfunctional and the symptom of blebitis wasnot evident Both systemic and topical antibiotics wereineffective and neither bacterial nor fungus infections couldbe detected in the cultured aqueous humor of the left eyeThesystemic examinations indicated the patient was immune-competent and suffered from neither systemic infectionnor systemic autoimmune disease PCR examinations ofthe anterior humor are useful in differentiating betweenCMV and other herpes viruses and in making a definitediagnosis in anterior uveitis or corneal endotheliitis [8]Since CMV was detected by qualitative PCR of the aqueoushumor of the current patient we changed the therapeuticstrategy to valganciclovir and prednisolone QuantitativePCR (broad range PCR and multiplex PCR) would addto the weight of diagnosis of CMV-induced uveitis if hightiter was demonstrated However quantitative PCR wasnot available The prompt effectiveness of valganciclovirand the recurrence of intraocular inflammation after thediscontinuance of valganciclovir indicated that CMV wasthe cause of the endophthalmitis-like uveitis However as
far as the author searched neither immune-competent CMVanterior uveitis nor corneal endotheliitis accompanied withhypopyon in the anterior chamber was reported in the pastalthough several immunocompromised patients with CMVuveitis accompanied with hypopyon were reported [9ndash11]Consequently the reason why the patient had such severeinflammation as hypopyon was still unclear The vitreousopacity of the left eye might have resulted from posteriorcapsulotomy for after-cataract surgery The inflammation ofthe anterior chamber might have spread into the vitreousbody through the capsulotomy hole
It has been reported that CMV or other herpes virus-induced uveitis was often accompanied with diffuse irisstromal atrophy [5 12 13] As for the current patient atthe first visit the pupillary light reflex in the left eye hadbeen lost perfectly compared with that in the right eyealthough depigmentation of the iris was not clear Thus itwas speculated that peripupillary atrophy caused by CMVinfection had been existing in the left eye for a long time
A small amount of systemic administration of corti-costeroid together with antibiotics is generally effective inthe treatments for bacterial endophthalmitis since severeintraocular infections are accompanied with secondaryinflammation which requires anti-inflammatory treatmentsLikewise we thought it was effective to administer a smallamount of systemic corticosteroid together with anti-CMVagent against severeCMV-induced uveitis accompaniedwithhypopyon in the anterior chamber and the opacity of thevitreous body Thus we continued to administer oral pred-nisolone for the current patient after PCR analysis revealedthat CMV was positive
Treatment strategy for recurrent CMV anterior uveitis(or corneal endotheliitis) has not been enough establishedyet though systemic or intravitreal anti-CMV treatment iseffective for CMV anterior uveitis [13ndash15] More clinicalinvestigations are needed
4 Case Reports in Ophthalmological Medicine
CMV-induced immune-competent anterior uveitisaccompanied with hypopyon is quite rare and might bemisdiagnosed as bacterial endophthalmitis It might recurafter the discontinuance of administering valganciclovir Wereconfirmed that PCR examination of the aqueous humorwas useful in diagnosing and deciding the treatment for suchpatients as in our case
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] A Carmichael ldquoCytomegalovirus and the eyerdquo Eye vol 26 no2 pp 237ndash240 2012
[2] A Radwan J L Metzinger D M Hinkle and C S FosterldquoCytomegalovirus retinitis in immunocompetent patients casereports and literature reviewrdquo Ocular Immunology and Inflam-mation vol 21 no 4 pp 324ndash328 2013
[3] K Toriyama T Suzuki Y Hara and Y Ohashi ldquoCytome-galovirus retinitis aftermultiple ocular surgeries in an immuno-competent patientrdquo Case Reports in Ophthalmology vol 3 no3 pp 356ndash359 2012
[4] M Miyanaga S Sugita N Shimizu et al ldquoA significant asso-ciation of viral loads with corneal endothelial cell damage incytomegalovirus anterior uveitisrdquo British Journal of Ophthal-mology vol 94 no 3 pp 336ndash340 2010
[5] S-P Chee K Bacsal A Jap S-Y Se-Thoe C L Chengand B H Tan ldquoClinical features of cytomegalovirus anterioruveitis in immunocompetent patientsrdquoTheAmerican Journal ofOphthalmology vol 145 no 5 pp 834e1ndash840e1 2008
[6] S-P Chee and A Jap ldquoCytomegalovirus anterior uveitis out-come of treatmentrdquo British Journal of Ophthalmology vol 94no 12 pp 1648ndash1652 2010
[7] M S Kresloff A A Castellarin and M A Zarbin ldquoEndoph-thalmitisrdquo Survey of Ophthalmology vol 43 no 3 pp 193ndash2241998
[8] S Sugita M Ogawa N Shimizu et al ldquoUse of a comprehensivepolymerase chain reaction system for diagnosis of ocularinfectious diseasesrdquo Ophthalmology vol 120 no 9 pp 1761ndash1768 2013
[9] L C Chumbley D M Robertson T F Smith and R JCampbell ldquoAdult cytomegalovirus inclusion retino uveitisrdquoAmerican Journal of Ophthalmology vol 80 no 5 pp 807ndash8161975
[10] J Biswas S Choudhry and S Solomon ldquoImmune recoveryvitritis presenting as panuveitis following therapy with proteaseinhibitorsrdquo Indian Journal of Ophthalmology vol 48 no 4 pp313ndash315 2000
[11] L Figueiredo R Rothwell M Bilhoto R Varandas and SFonseca ldquoImmune recovery uveitis masked as an endogenousendophthalmitis in a patient with active CMV retinitisrdquo CaseReports in Ophthalmological Medicine vol 2013 Article ID462968 4 pages 2013
[12] J HWooWK Lim S LHo and S C Teoh ldquoCharacteristics ofcytomegalovirus uveitis in immunocompetent patientsrdquoOcularImmunology amp Inflammation 2014
[13] L A A van Boxtel A van der Lelij J van der Meer andL I Los ldquoCytomegalovirus as a cause of anterior uveitis in
immunocompetent patientsrdquoOphthalmology vol 114 no 7 pp1358ndash1362 2007
[14] I de Schryver F Rozenberg N Cassoux et al ldquoDiagnosisand treatment of cytomegalovirus iridocyclitis without retinalnecrosisrdquo British Journal of Ophthalmology vol 90 no 7 pp852ndash855 2006
[15] H Mietz S Aisenbrey K U Bartz-Schmidt S Bamborschkeand G K Krieglstein ldquoGanciclovir for the treatment of anterioruveitisrdquo Graefersquos Archive for Clinical and Experimental Ophthal-mology vol 238 no 11 pp 905ndash909 2000
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Ophthalmological Medicine
CMV-induced immune-competent anterior uveitisaccompanied with hypopyon is quite rare and might bemisdiagnosed as bacterial endophthalmitis It might recurafter the discontinuance of administering valganciclovir Wereconfirmed that PCR examination of the aqueous humorwas useful in diagnosing and deciding the treatment for suchpatients as in our case
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] A Carmichael ldquoCytomegalovirus and the eyerdquo Eye vol 26 no2 pp 237ndash240 2012
[2] A Radwan J L Metzinger D M Hinkle and C S FosterldquoCytomegalovirus retinitis in immunocompetent patients casereports and literature reviewrdquo Ocular Immunology and Inflam-mation vol 21 no 4 pp 324ndash328 2013
[3] K Toriyama T Suzuki Y Hara and Y Ohashi ldquoCytome-galovirus retinitis aftermultiple ocular surgeries in an immuno-competent patientrdquo Case Reports in Ophthalmology vol 3 no3 pp 356ndash359 2012
[4] M Miyanaga S Sugita N Shimizu et al ldquoA significant asso-ciation of viral loads with corneal endothelial cell damage incytomegalovirus anterior uveitisrdquo British Journal of Ophthal-mology vol 94 no 3 pp 336ndash340 2010
[5] S-P Chee K Bacsal A Jap S-Y Se-Thoe C L Chengand B H Tan ldquoClinical features of cytomegalovirus anterioruveitis in immunocompetent patientsrdquoTheAmerican Journal ofOphthalmology vol 145 no 5 pp 834e1ndash840e1 2008
[6] S-P Chee and A Jap ldquoCytomegalovirus anterior uveitis out-come of treatmentrdquo British Journal of Ophthalmology vol 94no 12 pp 1648ndash1652 2010
[7] M S Kresloff A A Castellarin and M A Zarbin ldquoEndoph-thalmitisrdquo Survey of Ophthalmology vol 43 no 3 pp 193ndash2241998
[8] S Sugita M Ogawa N Shimizu et al ldquoUse of a comprehensivepolymerase chain reaction system for diagnosis of ocularinfectious diseasesrdquo Ophthalmology vol 120 no 9 pp 1761ndash1768 2013
[9] L C Chumbley D M Robertson T F Smith and R JCampbell ldquoAdult cytomegalovirus inclusion retino uveitisrdquoAmerican Journal of Ophthalmology vol 80 no 5 pp 807ndash8161975
[10] J Biswas S Choudhry and S Solomon ldquoImmune recoveryvitritis presenting as panuveitis following therapy with proteaseinhibitorsrdquo Indian Journal of Ophthalmology vol 48 no 4 pp313ndash315 2000
[11] L Figueiredo R Rothwell M Bilhoto R Varandas and SFonseca ldquoImmune recovery uveitis masked as an endogenousendophthalmitis in a patient with active CMV retinitisrdquo CaseReports in Ophthalmological Medicine vol 2013 Article ID462968 4 pages 2013
[12] J HWooWK Lim S LHo and S C Teoh ldquoCharacteristics ofcytomegalovirus uveitis in immunocompetent patientsrdquoOcularImmunology amp Inflammation 2014
[13] L A A van Boxtel A van der Lelij J van der Meer andL I Los ldquoCytomegalovirus as a cause of anterior uveitis in
immunocompetent patientsrdquoOphthalmology vol 114 no 7 pp1358ndash1362 2007
[14] I de Schryver F Rozenberg N Cassoux et al ldquoDiagnosisand treatment of cytomegalovirus iridocyclitis without retinalnecrosisrdquo British Journal of Ophthalmology vol 90 no 7 pp852ndash855 2006
[15] H Mietz S Aisenbrey K U Bartz-Schmidt S Bamborschkeand G K Krieglstein ldquoGanciclovir for the treatment of anterioruveitisrdquo Graefersquos Archive for Clinical and Experimental Ophthal-mology vol 238 no 11 pp 905ndash909 2000
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom