Embed Size (px)
Citation preview

1
Guillermo E. Umpierrez, MD, FACP, FACE
Professor of Medicine
Director, Grady Hospital Clinical Research Unit
Emory University School of Medicine
Director, Diabetes & Endocrinology Section
Grady Health System
Inpatient Glycemic Control
Case Presentation:
64 y/o male with a 3 cm thyroid nodule, FNA biopsy suspicious for papillary thyroid carcinoma. He has an 12 yr history of T2DM treated with metformin.
In the pre-surgery holding area, his BG is 324 mg/dL, A1C: 9.2%, normal TSH and Free T4.
Given this patient’s history and laboratory values, what is the best treatment option for glycemic management?
1. Hold surgery and reschedule after glycemic control improved
2. Move to ICU/step-down and start continuous IV insulin drip?
3. Cover with sliding-scale insulin and proceed with surgery?
4. Start basal bolus regimen – long + rapid acting analogs?
Distribution of patient-day-weighted mean POC-BG values for ICU
Swanson et al. Endocrine Practice, October 2011
Data from ~12 million BG readings from 653,359 ICU patients - mean POC-BG: 167 mg/dL
Hyperglycemia*: A Common Comorbidity in Medical-Surgical Patients in a Community Hospital
62%
12%
26%
Normoglycemia
Known Diabetes
New Hyperglycemia
Umpierrez G et al, J Clin Endocrinol Metabol 87:978, 2002
n = 2,020
* Hyperglycemia: Fasting BG 126 mg/dl or Random BG 200 mg/dl X 2

2
Diagnosis & recognition of hyperglycemia and diabetes in the hospital setting
Admission
Assess all patients for a history of diabetes
Obtain laboratory BG testing on admission
Umpierrez et al. J Clin Endocrinol Metabol. 97(1):16-38, 2012
BG<140 mg/dl
No POC
BG testing
History of diabetes
BG monitoring
No history of diabetes
Start POC BG
testing x 24-48h
Check A1C
A1C ≥ 6.5%
BG >140 mg/dl
A1C for Diagnosis of Diabetes in the Hospital
HbA1c should be measured in non-diabetic subjects with hyperglycemia (BG>140 mg/dl) and in subjects with diabetes if not done within 2-3 months prior to admission.
In the presence of hyperglycemia, a patient with HbA1c >6.5% can be identified as having diabetes.
Implementation of A1C testing can be useful:
assess glycemic control prior to admission
assist with differentiation of newly diagnosed diabetes from stress hyperglycemia
designing an optimal regimen at the time of discharge
Umpierrez et al, J Clin Endocrinol Metabol, 2012
What is the association between hyperglycemia and
hospital outcomes? 111-145
146-199
200-300
>300
Me
an
BG
(m
g/d
L)
Nondiabetics 153,910
Odd Ratio Odd Ratio
History Diabetes
Diabetics 62,868
No History Diabetes
Falciglia et al, Crit Care Med 2009
216,775 consecutive first admission
177 surgical, medical, cardiac ICUs
73 geographically diverse VAMC
Mortality Risk Greater in Hyperglycemic Patients without History of Diabetes

3
Thirty Day Mortality and Hospital Complications in Diabetic and Non-diabetic subjects Undergoing General Non-Cardiac Surgery
†p = 0.1 * p= 0.001
#p=0.017
†
*
* *
* #
*
%
A Frisch et al. Diabetes Care, May 2010
Adverse Events Stratified by Perioperative Hyperglycemia
BG at any point on the day of surgery, post-op day 1 and 2 N= 11,633, colorectal and bariatric surgery;
29.1% with hyperglycemia
Diabetes No Diabetes
*
*
*
*
§
§ p <0.05 * P <0.01
Known et al. Ann Surg 2013
Proportion of Patients (%)
BG > 180 mg/dl
BG < 180 mg/dl
Hyperglycemia: An Independent Marker of In-Hospital Mortality in Patients with Undiagnosed Diabetes
Total In-patient Mortality
Normoglycemia Known New Diabetes Hyperglycemia
1.7% 3.0%
16.0% *
Mort
alit
y (
%)
* p < 0.01
Umpierrez GE et al, J Clin Endocrinol Metabol 87:978, 2002
What target glucose should we aim in the hospital?

4
Prospective study of 2,467 consecutive diabetics who underwent open heart surgery. DSWI, deep sternal wound infection; SCI, subcutaneous insulin; CII, continuous insulin infusion.
4.0
3.0
2.0
1.0
0.0
DSWI (%)
87 88 89 90 91 92 93 94 95 96 97
Year
Furnary AP, et al. Ann Thorac Surg. 1999;67:352–362.
CII SCI
Portland Diabetes Project: Insulin Infusion Reduces DSWI
SCI Group: Day of surgery: 241 mg/dL
POD #1: 206 mg/dL
CII Group: Day of surgery: 199 mg/dL
POD #1: 176 mg/dL
Intensive Insulin Therapy in SICU: The Leuven Study
N= 1548 pts in a surgical ICU
Conventional IT
• Target BG: 180-200 mg/dL
• Mean daily BG: 153 mg/dL
Intensive IT
• Target BG: 80-110 mg/dL
• Mean daily BG: 103 mg/dL
Van-Den Berge et al, NEJM 345:1359, 2001
Intensive Glucose Management in RCT
Trial
N
Setting
Primary Outcome
ARR
RRR
Odds Ratio (95% CI)
P-value
Van den Berghe 2006
1200 MICU Hospital mortality
2.7% 7.0% 0.94* (0.84-1.06)
N.S.
Glucontrol 2007
1101 ICU ICU mortality
-1.5% -10% 1.10* (0.84-1.44)
N.S.
Ghandi 2007
399 OR Composite 2% 4.3% 1.0* (0.8-1.2)
N.S.
VISEP 2008
537 ICU 28-d mortality
1.3% 5.0% 0.89* (0.58-1.38)
N.S.
De La Rosa 2008
504 SICU
MICU
28-d mortality
-4.2% * -13%* NR N.S.
NICE-SUGAR 2009
6104 ICU 3-mo mortality
-2.6% -10.6 1.14 (1.02-1.28)
< 0.05
*not significant
The NICE-SUGAR Study
Blood Glucose Level,
According to Treatment Group
IIT goal: 81 – 108 mg/dL (mean BG 118 mg/dL)
CIT goal: <180 mg/dL (mean BG 145 mg/dL)
Probability of Survival
90 days: Absolute mortality difference of 2.6% (95% CI, 0.4 to 4.8);
Odds ratio for death with IIT: 1.14 (95% CI, 1.02 to 1.28; p = 0.02).
829
751
RR= 1.14
NICE-SUGAR Trial. N Engl J Med. 360:1283-1297, 2009.

5
Griesdale DE, et al. CMAJ. 2009;180(8):821-827.
Favors IIT Favors Control
Hypoglycemic Events
Intensive Insulin Therapy and Hypoglycemic Events in Critically Ill Patients
No. Events/Total No. Patients
Study IIT Control Risk ratio (95% CI)
Van den Berghe et al 39/765 6/783 6.65 (2.83-15.62)
Henderson et al 7/32 1/35 7.66 (1.00-58.86)
Bland et al 1/5 1/5 1.00 (0.08-11.93)
Van den Berghe et al 111/595 19/605 5.94 (3.70-9.54)
Mitchell et al 5/35 0/35 11.00 (0.63-191.69)
Azevedo et al 27/168 6/169 4.53 (1.92-10.68)
De La Rosa et al 21/254 2/250 10.33 (2.45-43.61)
Devos et al 54/550 15/551 3.61(2.06-6.31)
Oksanen et al 7/39 1/51 9.15 (1.17-71.35)
Brunkhorst et al 42/247 12/290 4.11(2.2-7.63)
Iapichino et al 8/45 3/45 2.67 (0.76-9.41)
Arabi et al 76/266 8/257 9.18 (4.52-18.63)
Mackenzie et al 50/121 9/119 5.46 (2.82-10.60)
NICE-SUGAR 206/3016 15/3014 13.72 (8.15-23.12)
Overall 654/6138 98/6209 5.99 (4.47-8.03)
0.1 1 10
Risk Ratio (95% CI)
Moghissi ES, et al; AACE/ADA Inpatient Glycemic Control Consensus Panel. Endocr Pract. 2009;15(4).
2009 AACE/ADA Recommended Target Glucose Levels in ICU Patients
Recommended 140-180
Acceptable 110-140
Not recommended <110
Not recommended >180
Computerized algorithm (Glucommander) to reduce risk of hypoglycemia and protocol violations
GLUCO-CABG trial - first prospective RCT to determine the optimal BG target during the perioperative period in hyperglycemic subjects who undergo CABG.
100-140 mg/dl
141-180 mg/dl
GLUCO-CABG Trial – RCT to determine the optimal BG target during the peri-operative period (ICU stay, hospital stay, 90 day after
discharge) in hyperglycemic subjects who undergo CABG
NCT 01792830
Gluco-CABG: Methods
Patients with hyperglycemia during surgery, or after surgery were randomized to:
Intensive insulin therapy (100-140 mg/dL) Conservative insulin therapy (141-180 mg/dL)
Computerized algorithm (Glucommander) was used to guide continuous insulin infusion
IV insulin in ICU until patients were able to eat and/or for transfer to non-ICU services
Transition to SQ insulin (target <140 mg/dL) Diabetes → Basal bolus regimen Non-diabetes requiring CII ≥ 2 U/h → Basal bolus regimen
Non-diabetes requiring < 2 U/h → correction doses with SSI
GLUCO-CABG Trial Perioperative Blood Glucose Concentration
Data are means SEM
Intensive (n=151): Target BG 100-140 mg/dl Conservative (n=151): Target BG 141-180 mg/dl
Umpierrez GE, et al. 2014 ADA Scientific Meeting
100
120
140
160
180
200
Admit Rando- mization
OR ICU I.V.
ICU Non- ICU
After Discharge
Glu
cose
, m
g/d
l
* *
p<0.001 p<0.001
Intensive= 130±11 mg/dl (IQR 124-139) Conventional= 159±14 mg/dl (IQR 142-164)
i.v. ICU
Intensive= 132±14 mg/dl (IQR 124-139) Conventional= 154±16 mg/dl (IQR 142-164)
ICU
Intensive
Conservative
6
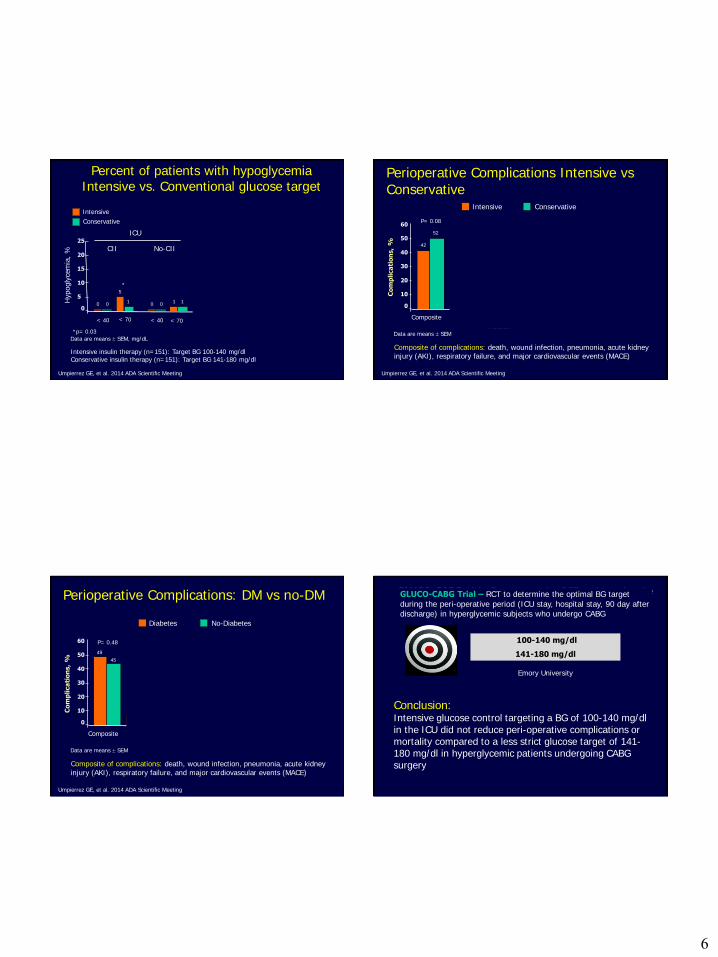
Percent of patients with hypoglycemia Intensive vs. Conventional glucose target
Hypogly
cem
ia,
%
Intensive insulin therapy (n=151): Target BG 100-140 mg/dl Conservative insulin therapy (n=151): Target BG 141-180 mg/dl
Umpierrez GE, et al. 2014 ADA Scientific Meeting
5
10
15
20
25
0
Data are means SEM, mg/dL
Hospital Non-ICU
After Hospital Discharge
< 40
5
1
< 70 < 70
CII No-CII
ICU
< 40
1 1 0 0 0 0
< 40
1 1
< 70
20
23
< 40 < 70
0 0
24
19
Intensive
Conservative
*
*p= 0.03
Perioperative Complications Intensive vs Conservative
Co
mp
lica
tio
ns,
%
Intensive Conservative
Composite of complications: death, wound infection, pneumonia, acute kidney injury (AKI), respiratory failure, and major cardiovascular events (MACE)
Umpierrez GE, et al. 2014 ADA Scientific Meeting
10
20
30
40
50
60
Wound Infection
Pneumonia AKI Composite Death Resp Failure
MACE
0
P= 0.08
42
52
1 3
P= 0.45
2 4
P= 0.62
2 5
P= 0.45
14
19
P= 0.27 P= 0.27 P= 0.27
11
19
34
32
Data are means SEM
Perioperative Complications: DM vs no-DM
Co
mp
lica
tio
ns,
%
Diabetes No-Diabetes
Composite of complications: death, wound infection, pneumonia, acute kidney injury (AKI), respiratory failure, and major cardiovascular events (MACE)
Umpierrez GE, et al. 2014 ADA Scientific Meeting
10
20
30
40
50
60
Wound Infection
Pneumonia AKI Composite Death Resp Failure
MACE
0
P= 0.48
49
45
5
0
P= 0.02
4 1
P= 0.17
4 3
P>0.9
20
12
P= 0.048 P= 0.49 P= 0.53
14 17
39 36
Data are means SEM
*
*
GLUCO-CABG trial - first prospective RCT to determine the optimal BG target during the perioperative period in hyperglycemic subjects who undergo CABG.
100-140 mg/dl
141-180 mg/dl
Emory University
GLUCO-CABG Trial – RCT to determine the optimal BG target
during the peri-operative period (ICU stay, hospital stay, 90 day after discharge) in hyperglycemic subjects who undergo CABG
Conclusion: Intensive glucose control targeting a BG of 100-140 mg/dl in the ICU did not reduce peri-operative complications or mortality compared to a less strict glucose target of 141-180 mg/dl in hyperglycemic patients undergoing CABG surgery

7
How should we manage hyperglycemia in non-ICU settings?
1.ACE/ADA Task Force on Inpatient Diabetes. Diabetes Care. 2006 & 2009 2.Diabetes Care. 2009;31(suppl 1):S1-S110..
Antihyperglycemic Therapy
Insulin
Recommended
OADs
Not Generally Recommended
Recommendations for Managing Patients With Diabetes in the Hospital Setting
Inpatient Management in non-ICU Setting
Sliding Scale Regular Insulin
Basal Bolus Insulin Regimen
In insulin naïve patients with T2DM, does treatment with basal bolus regimen with glargine once daily and glulisine before meals is superior to sliding scale regular insulin?
RABBIT-2D TRIAL: - Research Question:
Umpierrez et al, Diabetes Care 30:2181–2186, 2007
Rabbit 2 Trial: Changes in Glucose Levels With Basal-Bolus vs. Sliding Scale Insulin
Umpierrez GE, et al. Diabetes Care. 2007;30(9):2181-2186.
Days of Therapy
BG
, m
g/d
L
100
120
140
160
180
200
220
240
Admit 1
Sliding-scale
Basal-bolus
bP<.05.
a a a
b b
b b
2 3 4 5 6 7 8 9 10
aP<.05.
• Sliding scale regular insulin (SSRI) was given 4 times daily • Basal-bolus regimen: glargine was given once daily; glulisine was given before meals.
0.4 U/kg/d x BG between 140-200 mg/dL
0.5 U/kg/d x BG between 201-400 mg/dL
Hypoglycemia rate:
Basal Bolus Group:
BG < 60 mg/dL: 3%
BG < 40 mg/dL: none
SSRI:
BG < 60 mg/dL: 3%
BG < 40 mg/dL: none

8
Inpatient Management in non-ICU Setting
Basal Bolus Insulin Regimen
NPH and Regular Insulin-Spilt-
Mixed Regimen
In patients with T2DM on diet, oral agents or insulin treatment, does treatment with basal bolus regimen with detemir once daily and aspart before meals is superior to NPH and Regular split-mixed insulin regimen?
DEAN TRIAL: - Research Question:
Umpierrez et al, J Clin Endocrinol Metab 94: 564–569, 2009
DEAN Trial: Changes in Mean Daily Blood Glucose Concentration
BG
, m
g/d
L
Duration of Therapy, d
Data are means SEM.
Detemir + aspart
NPH + regular
Basal-bolus regimen: detemir was given once daily; aspart was given before meals. NPH/regular regimen: NPH and regular insulin were given twice daily, two thirds in AM, one third in PM.
Umpierrez GE, et al. J Clin Endocrinol Metab. 2009;94(2):564-569.
P=NS
100
120
140
160
180
200
220
240
Pre-Rx
BG
0 1 2 3 4 5 6-10
Does glucose control prevents hospital complications in non-ICU settings?
Inpatient Management
in General Surgery
Sliding Scale
Regular Insulin
Basal Bolus
Insulin Regimen
In patients with T2DM on diet, oral agents or insulin treatment,
does treatment with basal bolus regimen with glargine and glulisine is superior to SSRI?
RABBIT-2 Surgery Trial: - Research Question:
• Differences between groups in mean daily BG
• Composite of hospital complications: wound infection, pneumonia, respiratory failure, acute renal failure, and bacteremia
Umpierrez et al, Diabetes Care 34 (2):1–6, 2011

9
*
*
* *
Mean BG before meals and at bedtime during basal bolus and SSI therapy
Breakfast Lunch Dinner Bedtime
*p<0.001
Glargine+Glulisine
Sliding Scale Insulin
Umpierrez et al, Diabetes Care 34 (2):1–6, 2011
Postoperative Complications
P=0.003
P=NS
P=0.05 P=0.10
P=0.24
Glargine+Glulisine
Sliding Scale Insulin
Umpierrez et al, Diabetes Care 34 (2):1–6, 2011
* Composite of hospital complications: wound infection, pneumonia, respiratory failure, acute renal failure, and bacteremia.
Insulin Treatment in in Non-ICU Setting
Do you need basal bolus in ALL patients? Do you need basal bolus in ALL patients?
T2DM with BG > 140 mg/dl (7.7 mmol/l)
Basal insulin
- Start at 0.2-0.25 U/Kg/day* - Correction doses with rapid
acting insulin AC
- Adjust basal as needed
NPO
Uncertain oral intake Adequate
Oral intake
Basal Bolus
TDD: 0.4-0.5 U/Kg/day -½ basal, ½ bolus
-- adjust as needed
Basal Plus Trial:
Basal + Correction vs. Basal Bolus
Basal plus supplements
Starting glargine*: 0.25
units/kg
Correction with glulisine
for BG >140 mg/dl per
sliding scale
Basal Bolus Regimen
Starting TDD*: 0.5 U/kg
Glargine: 0.25 U/kg
Glulisine: 0.25 U/kg in three equally divided doses (AC)
Correction with glulisine
for BG >140 mg/dl per
sliding scale
* Reduce TDD to 0.15 U/kg in
patients ≥70 yrs and/or serum
creatinine ≥ 2.0 mg/dL
* Reduce TDD to 0.3 U/kg in
patients ≥70 yrs and/or serum
creatinine ≥ 2.0 mg/dL Umpierrez et al, Diabetes Care, 2013

10
Duration of Treatment (days)
0 1 2 3 4 5 6 7 8 9 10
Blo
od G
lucose (
mg/d
L)
120
140
160
180
200
220
240Basal Plus
Basal Bolus
Basal-PLUS vs Basal Bolus: 300 medical & surgical non-ICU patients
Patients treated with diet, oral agents or with low-dose insulin ≤ 0.4 U/Kg/Day
Basal Plus: glargine once daily
0.25 U/kg plus glulisine supplements
Basal Bolus: TDD: 0.5 U/kg/d
Glargine 50% glulisine 50%
Umpierrez et al, Diabetes Care, 2013
Basal-PLUS vs Basal Bolus: Medicine and Surgery Patients
Medicine Surgery
BG AC & HS
Daily BG Daily BG
BG AC & HS
Smiley et al, Diabetes Care, 2013
Can you treat patients with oral agents in the hospital?
Inpatient Management in
non-ICU
Basal Bolus or
Basal Plus Regimens
What about Incretin-Based
Therapy?
Umpierrez et al, Diabetes Care, 2013
DPP-4 Therapy in Hospitalized Patients
Study Type: Multicenter, prospective, open-label
randomized clinical trial
Patient Population: Patients with T2D admitted to general
medicine and surgery services at 3 hospitals: Emory
University, Grady, and University of Michigan
Treatment Groups* Group 1. Sitagliptin once daily (n=30)
Group 2. Sitagliptin plus glargine insulin once daily (n=30)
Group 3. Basal bolus regimen with glargine once daily
and lispro before meals (n=30)
* All groups received supplemental doses of lispro for BG > 140 mg/dl before meals
NCT01378117
Umpierrez et al, Diabetes Care, 2013

11
Randomi-zation
Mean Daily BG During Treatment
Umpierrez et al, Diabetes Care, 2013
Me
an D
aily
Blo
od
Glu
cose
(m
g/d
L)
Randomization Blood Glucose (<180 mg/dl and >180 mg/dl) and Mean Daily Glucose concentration
p= 0.91
p= 0.08
Umpierrez et al, Diabetes Care, 2013
Inpatient Management in
non-ICU
Basal Bolus or
Basal Plus Regimens
Management of Patients With Diabetes a After Hospital Discharge
What Regimen Should We Use at
Hospital Discharge?
Use admission A1C to adjust therapy at discharge
7%
8%
9%
10%
Adjust original therapy, ADD another agent or basal insulin
Return to original therapy
ADD basal insulin therapy
ADD basal or REPLACE with basal/bolus
Umpierrez G et al. Endocrine Society Inpatient Diabetes Guidelines. J Clin Endocrinol Metabol, 2012
Recommendations for Managing Patients With Diabetes After Hospital Discharge
12
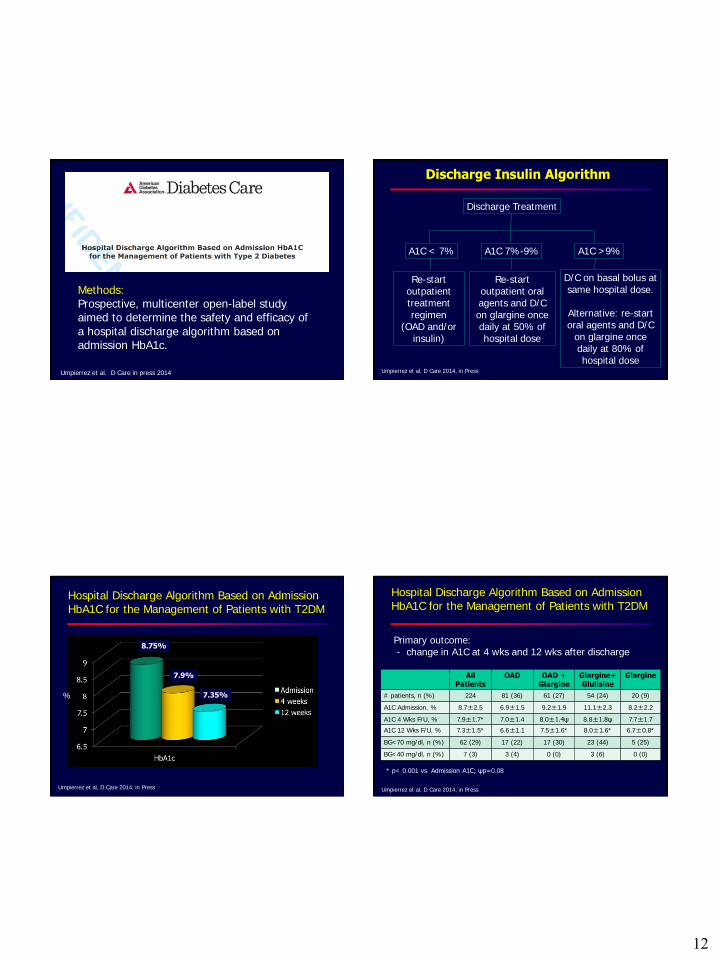
Methods: Prospective, multicenter open-label study aimed to determine the safety and efficacy of a hospital discharge algorithm based on admission HbA1c.
Umpierrez et al. D Care in press 2014
A1C < 7%
Re-start outpatient treatment regimen
(OAD and/or insulin)
A1C 7%-9%
Re-start outpatient oral agents and D/C on glargine once daily at 50% of hospital dose
A1C >9%
D/C on basal bolus at same hospital dose.
Alternative: re-start oral agents and D/C
on glargine once daily at 80% of hospital dose
Discharge Insulin Algorithm
Discharge Treatment
Umpierrez et al, D Care 2014, in Press
Hospital Discharge Algorithm Based on Admission HbA1C for the Management of Patients with T2DM
8.75%
7.9%
7.35% %
Umpierrez et al, D Care 2014, in Press
Hospital Discharge Algorithm Based on Admission HbA1C for the Management of Patients with T2DM
Primary outcome: - change in A1C at 4 wks and 12 wks after discharge
All Patients
OAD OAD + Glargine
Glargine+ Glulisine
Glargine
# patients, n (%) 224 81 (36) 61 (27) 54 (24) 20 (9)
A1C Admission, % 8.7±2.5 6.9±1.5 9.2±1.9 11.1±2.3 8.2±2.2
A1C 4 Wks F/U, % 7.9±1.7* 7.0±1.4 8.0±1.4ψ 8.8±1.8ψ 7.7±1.7
A1C 12 Wks F/U, % 7.3±1.5* 6.6±1.1 7.5±1.6* 8.0±1.6* 6.7±0.8*
BG<70 mg/dl, n (%) 62 (29) 17 (22) 17 (30) 23 (44) 5 (25)
BG<40 mg/dl, n (%) 7 (3) 3 (4) 0 (0) 3 (6) 0 (0)
* p< 0.001 vs. Admission A1C; ψp=0.08
Umpierrez et al, D Care 2014, in Press

13
Management of diabetes in non-critical care setting
So… What really have we learned?
Umpierrez et al. Endocrine Society Annual Meeting, 2014
What Glucose Level Predicts Hospital Complications?
Guillermo E. Umpierrez, MD
Thank you!





















![Glycemic Control-Subcutaneous Regimen Adjustment [1758] · Page 3 of 18 GLYCEMIC CONTROL SUBCUTANEOUS REGIMEN ADJUSTMENT [1758] (11/23/15) PATIENT INFORMATION [ ] Insulin …](https://img.pdfslide.us/doc/110x75/5b5e10097f8b9a415d8bb3a2/glycemic-control-subcutaneous-regimen-adjustment-1758-page-3-of-18-glycemic.jpg)






