Embed Size (px)
Citation preview

Chestclinic
CASE BASED DISCUSSION
A 63-year-old man with a recurrent right-sidedpleural effusionJohn P Corcoran,1 Emma L Culver,2 Ioannis Psallidas,1 Robert J Hallifax,1
Susan J Davies,3 Adrian C Bateman,4 Eleanor Barnes,2,5 Najib M Rahman1,5
1Oxford Centre for RespiratoryMedicine, Oxford UniversityHospitals NHS Trust,Oxford, UK2Translational GastroenterologyUnit, Oxford UniversityHospitals NHS Trust,Oxford, UK3Department of CellularPathology, Oxford UniversityHospitals NHS Trust,Oxford, UK4Department of CellularPathology, University HospitalSouthampton NHS FoundationTrust, Southampton, UK5NIHR Oxford BiomedicalResearch Centre, University ofOxford, Oxford, UK
Correspondence toDr John P Corcoran, OxfordCentre for RespiratoryMedicine, Churchill Hospital,Oxford OX3 7LE, UK;[email protected]
To cite: Corcoran JP,Culver EL, Psallidas I, et al.Thorax Published OnlineFirst: [please include DayMonth Year] doi:10.1136/thoraxjnl-2014-206423
JPC: A 63-year-old Caucasian man was seen inclinic having been referred by his general practi-tioner with a 10 -week history of progressive exer-tional dyspnoea, associated with dry cough andretrosternal discomfort over the preceding fort-night. There was no history of fever, weight loss,anorexia, haemoptysis, dysphagia or other localis-ing systemic symptoms. His past medical historyincluded psoriatic arthropathy, atrial fibrillation,hypertension and gastro-oesophageal reflux; ofnote, there was no recent history of palpitations orworsening peripheral oedema, while his jointdisease remained quiescent. Current medications(all long-standing) included methotrexate, omepra-zole, bisoprolol, aspirin, ramipril and simvastatin.He was a lifelong non-smoker and retired solicitorwith no occupational risk factors for lung disease.On examination he was afebrile with no palpable
lymphadenopathy or clubbing. Cardiovascularexamination demonstrated rate-controlled atrial fib-rillation only; abdominal examination was normal.Respiratory examination revealed dull percussionnote and reduced breath sounds at the right lungbase, with normal resting oxygen saturations. Chestradiograph and thoracic ultrasound confirmed thepresence of a large right-sided pleural effusion.Routine bloods including full blood count, clottingstudies, renal function, liver function and serumcalcium were unremarkable. I performed a diagnosticand therapeutic pleural aspiration, draining 1500 mLof straw-coloured fluid with no complications.Laboratory analysis showed the effusion to be anexudate (protein 46 g/L, lactate dehydrogenase(LDH) 961 IU/L, glucose 0.4 mmol/L); pleural fluidculture and cytology (including flow cytometry) werenegative.NMR: The presence of a cytology-negative
exudative pleural effusion of unknown aetiology ina previously well individual requires urgent furtherinvestigation. The low pleural fluid glucose andhigh LDH may imply infection, although thesefindings are non-specific and can also be seen in thecontext of chronic inflammation or malignancy;furthermore, the clinical history and negativeculture go against an infective cause. The presenceof an inflammatory arthropathy may prompt con-sideration of whether an underlying connectivetissue or autoimmune disease is responsible; metho-trexate is also associated with pleural effusion for-mation. In the first instance, a contrast-enhancedCT scan of the thorax (staging protocol, ideallytaken in the venous phase to allow assessment ofthe pleura) should be performed. Unless this
demonstrates an indisputable cause for the effusionor a more suitable diagnostic route, the patient willneed to have pleural biopsies taken with the aim ofmaking a definite diagnosis—it is worth remember-ing that neither negative pleural fluid cytology noran apparently normal CT scan can definitivelyexclude an underlying pleural malignancy.JPC: The patient’s CT scan revealed a moderate
right-sided pleural effusion that enhanced peripher-ally but also appeared to contain a heterogeneouslyenhancing curvilinear opacity, potentially of vascu-lar origin. Subsequent MRI thorax excluded anoccult ongoing intrapleural bleed. Smooth visceraland parietal pleural thickening was noted, but therewere no features that would be consistent with amalignant process such as nodularity, chest wallinvasion or mediastinal involvement. The lung par-enchyma, mediastinum and upper abdominalorgans appeared otherwise unremarkable.Local anaesthetic thoracoscopy was performed in
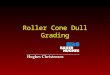
order to obtain pleural tissue for histological ana-lysis. A further 2200 mL of straw-coloured fluidwas drained from the right hemithorax; visualinspection of the pleural cavity identified twomobile mass lesions with an apparently fatty con-sistency adjacent to the diaphragm, alongsidediffuse pleural thickening involving both parietaland visceral (right lower lobe) surfaces (figure 1A,B). Full-thickness pleural biopsies were taken fromthe extensive parietal thickening at multiple sitesusing a two-port technique; biopsies were alsoobtained separately from the two mass lesions. Talcpoudrage was not performed, meaning the patientcould be discharged home the same day after chestradiograph and thoracic ultrasound confirmedre-expansion of the right lung.SJD: Biopsies from the intrathoracic mass lesions
demonstrated fibrin only with some entrappeddegenerate cells of inflammatory origin and periph-eral macrophages; no malignant cells were seen.The pleural biopsies (figure 1C–E) showed featuresconsistent with chronic inflammation and fibrinouspleuritis. In some areas, a single layer of histiocyteswas visible at the surface, but no malignant cellswere identified. The inflammatory change was richin lymphocytes with lymphoid follicle formationfocally and, in addition, a highly prominent popu-lation of plasma cells that stained positive forimmunoglobulin G4 (IgG4). There were no fea-tures of haematological malignancy identified, withkappa and lambda light chain immunohistochemis-try excluding a clonal plasma cell population. Noobliterative phlebitis was observed. These findings
Corcoran JP, et al. Thorax 2015;0:1–4. doi:10.1136/thoraxjnl-2014-206423 1
Chest clinic Thorax Online First, published on January 8, 2015 as 10.1136/thoraxjnl-2014-206423
Copyright Article author (or their employer) 2015. Produced by BMJ Publishing Group Ltd (& BTS) under licence.
on October 4, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thoraxjnl-2014-206423 on 8 January 2015. D
ownloaded from

Chestclinic
raised the possibility of the pleural inflammation and thickeningbeing secondary to IgG4-related disease and prompted referralof the histology for a second expert opinion.
ACB: A review of the pleural tissue received demonstratedfibrous thickening with, in areas, a prominent lymphoplasmacy-tic chronic inflammatory infiltrate. Active myofibroblasts werepresent but storiform pattern fibrosis was not identified.Immunohistochemistry revealed a mean of 73 IgG4-positiveplasma cells per high-power field, with a ratio of IgG4-positiveto IgG-positive plasma cells >40%. While the features were notdiagnostic of IgG4-related disease based on histopathologicalevidence alone, they would be in keeping with ‘probable histo-logical features of IgG4-related disease’ according to the Bostoncriteria.1
JPC: The patient was reviewed in clinic to discuss thepleural biopsy results and plan further investigations. Once
again he reported no recent or previous history of abdominalsymptoms. Serum and urine electrophoresis was normal,while serum IgG4 level was elevated at 2.84 g/L (normalrange 0.1–1.3 g/L). Autoimmune profile including antinuclearantibody, complement and rheumatoid factor was unremark-able; serum amylase was also normal. Chest radiograph andthoracic ultrasound confirmed further recurrence of thepatient’s right pleural effusion, although not to the pointwhereby repeat aspiration for symptomatic benefit wasrequired. Completion imaging with CT scan of the abdomenand pelvis did not demonstrate any further pathologicalabnormality. The patient’s case was subsequently discussedat the regional IgG4-related disease multidisciplinaryteam meeting where in the context of clinical, biochemical,radiological and histological correlation a diagnosis ofIgG4-related pleural disease was agreed.
Figure 1 Images (A) and (B) takenduring local anaesthetic thoracoscopydemonstrate inflammatory pleuritis anddiffuse thickening involving theparietal and visceral surfaces;subsequent pleural biopsiesdemonstrate histological changesconsistent with immunoglobulin G4(IgG4)-related pleural diseaseincluding: (C) and (D) fibrousthickening and prominentlymphoplasmacytic infiltrate (H&E);and (E) strongly positive staining forIgG4-positive plasma cells.
2 Corcoran JP, et al. Thorax 2015;0:1–4. doi:10.1136/thoraxjnl-2014-206423
Chest clinic on O
ctober 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thoraxjnl-2014-206423 on 8 January 2015. Dow
nloaded from

Chestclinic
NMR: Having initially been recognised in association withautoimmune pancreatitis nearly two decades ago, IgG4-relateddisease is now increasingly acknowledged as being a multisystemfibroinflammatory disorder that can affect almost any organsystem including the lungs.2 The most common intrathoracicmanifestation of IgG4-related disease is hilar or mediastinallymphadenopathy, seen in up to 80% of patients. Pulmonaryinvolvement can be extremely variable with features includingsolid nodules or masses, bronchiectasis, bronchovascularinvolvement and interstitial lung disease all described either inisolation or combination. Pleural involvement in the form ofeffusions and/or thickening (with or without underlying lungparenchymal involvement) is also increasingly recognised in theliterature base.3 The key differential diagnosis in this particularcase was a lymphoproliferative disorder; the absence of clonalityon either pleural fluid flow cytometry or pleural biopsy hist-ology was reassuring in this regard, as was the absence oflymphadenopathy on full-body CT imaging.
ACB: Diagnosing IgG4-related disease is frequently challen-ging, with elevated tissue IgG4-positive plasma cell numbershelpful but not specific. Instead, it is necessary to identify char-acteristic histopathological features1 that are usually consistentregardless of the site of disease. The three key histopathologicalfeatures are dense lymphoplasmacytic infiltration, storiformpattern fibrosis and obliterative phlebitis (venulitis), although itis common for not all of these to be present within a tissuesample. However, the level of confidence for a diagnosis ofIgG4-related disease increases if at least two—and ideally allthree—morphological features are present. The diagnosis canthen be further supported by the demonstration of prominentIgG4-positive plasma cells and a ratio of IgG4-positive toIgG-positive plasma cells of >40%. Other features may includethe variable presence of eosinophils within the tissue. As withany diagnosis, the clinical history, serology, radiology and hist-ology should be carefully correlated to ensure consistency acrossthese characteristics.
EB: IgG4 is ordinarily the least abundant subclass of IgG inhealthy individuals and has traditionally been regarded ashaving an anti-inflammatory role, being unique among the sub-classes of IgG in not activating complement or forming immunecomplexes. Nonetheless, it is recognised as being potentiallyinvolved in a number of autoimmune conditions includingforms of pemphigus and membranous glomerulonephritis; andseparate to this it underlies the collection of related disordersthat have now bracketed under the internationally recognisedterm of ‘IgG4-related disease’.4
The pathogenesis of IgG4-related disease is at this point intime poorly understood, perhaps unsurprising since we havelimited understanding of the role IgG4 even plays in normalhealth. Furthermore, it is unclear whether the excessive levelsof IgG4 seen in affected patients are pathogenic and destruc-tive in themselves, or simply an exaggerated response toanother unidentified primary immunological stimulus.Proposed triggers for IgG4-related disease include geneticand human leucocyte antigen-associated susceptibility, auto-immunity, an abnormal allergic response and molecularmimicry by an infective agent. The subsequent developmentof the condition is thought to be driven by an overabundanceof Th2 and regulatory T cells in the affected tissues, a keydistinction from the vast majority of autoimmune conditionswhere the function of regulatory T cells is classically eitherimpaired or downregulated.
Being an only recently described entity, we have limited infor-mation about the epidemiology of IgG4-related disease. In
addition, a lack of awareness of the condition alongside theability of IgG4-related disease to mimic a number of better-known diagnoses (eg, primary sclerosing cholangitis in thebiliary system or sarcoidosis in the lung) means it may havebeen and still remain under-recognised. The data available indi-cate that IgG4-related disease is most frequently seen in malepatients over the age of 50 years2—a striking contrast to mostautoimmune disease that predominates in a young female popu-lation—with autoimmune pancreatitis remaining the best recog-nised and studied presenting feature. Data (unpublished) fromthe Oxford IgG4-related disease patient cohort and that ofothers5 show an increased risk of malignancy both at diagnosisand during follow-up compared with age-matched and sex-matched controls, the reasons for which are not understood atthis point in time. As such, the presence of malignancy inpatients with suspected IgG4-related disease should be activelyexcluded at the time of diagnosis and monitored for during sub-sequent treatment and follow-up.
It is important to recognise that IgG4-related disease shouldbe a diagnosis made through the identification of specific histo-pathological findings placed in an appropriate clinical context.Relying on serum IgG4 alone may result in underdiagnosis sincea number of patients with biopsy-proven IgG4-related diseasewill have normal serum levels; and indeed overdiagnosis asapproximately 5% of healthy controls can have elevated serumIgG4 levels at any point in time. Nonetheless, making thecorrect diagnosis is crucial since IgG4-related disease is typicallysteroid-responsive in the absence of established tissue fibrosiswith symptomatic resolution and improved function of theaffected organ(s). It remains unclear whether early diagnosisand intervention has an impact on long-term outcomes, and thiswill only become apparent over time and with greater clinicalexperience.
Steroid dosing varies according to local practice, but initialtreatment regimens with oral prednisolone of between 30 mgand 1 mg/kg daily are commonly used. Assuming a favourableresponse, this can be gradually weaned over subsequent months.In resistant or relapsing cases, despite steroid therapy additionalimmunomodulatory medications such as rituximab, azathioprineand mycophenolate can be used, although this is not on thebasis of any randomised trial data.
JPC: Our patient was informed of the diagnosis ofIgG4-related pleuritis and started on oral prednisolone at adose of 40 mg daily, weaning gradually according to clinicaland radiological response. He remains well on a low-maintenance dose of prednisolone after 8 months, with near-total resolution of his previously reported respiratory symp-toms. Serum IgG4 levels have returned to within normallimits, while there is evidence of reduction in both pleuralthickening and effusion volume on serial imaging with nofeatures to suggest further organ system involvement by hisIgG4-related disease.
Contributors The article was conceived by JPC, ELC, EB and NMR. JPC and ELCwere responsible for draft preparation and revision. All authors were involved incritical appraisal of each draft and approval of the final submitted manuscript.All authors contributed to the patient’s clinical care. JPC is the lead author of thisarticle; JPC and NMR are responsible for the overall content as guarantors.
Funding IP is the recipient of a European Respiratory Society Fellowship (LTRF2013-1824). EB and NMR are funded by the NIHR Oxford Biomedical Research Centre.
Competing interests None.
Patient consent Obtained.
Ethics approval Informed written consent was obtained from the patient prior tothe production of this article.
Corcoran JP, et al. Thorax 2015;0:1–4. doi:10.1136/thoraxjnl-2014-206423 3
Chest clinic on O
ctober 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thoraxjnl-2014-206423 on 8 January 2015. Dow
nloaded from

Chestclinic
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Deshpande V, Zen Y, Chan JK, et al. Consensus statement on the pathology of
IgG4-related disease. Mod Pathol 2012;25:1181–92.2 Stone JH, Zen Y, Deshpande V. IgG4-related disease. New Engl J Med
2012;366:539–51.
3 Ryu JH, Sekiguchi H, Yi ES. Pulmonary manifestations of immunoglobulin G4-relatedsclerosing disease. Eur Respir J 2012;39:180–6.
4 Stone JH, Khosroshahi A, Deshpande V, et al. Recommendations for thenomenclature of IgG4-related disease and its individual organ system manifestations.Arthritis Rheum 2012;64:3061–7.
5 Shiokawa M, Kodama Y, Yoshimura K, et al. Risk of cancer in patients withautoimmune pancreatitis. Am J Gastroenterol 2013;108:610–17.
4 Corcoran JP, et al. Thorax 2015;0:1–4. doi:10.1136/thoraxjnl-2014-206423
Chest clinic on O
ctober 4, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thoraxjnl-2014-206423 on 8 January 2015. Dow
nloaded from