Embed Size (px)
Citation preview

10/13/2009
1
Difficult Neurology Cases
Dr Jane Evanson FRCR
Dr Chloe Orkin FRCPBarts and the London NHS Trust
Case 1

10/13/2009
2
Case 1
• 26 yr old ♂ schoolteacher
• British bisexual (Moroccan descent)
• HIV diagnosed 2003
• Engaged with services in June 2008
• Lives in Hackney
• No travel history
• Admitted to St Barts via referring hospital
• CD4 175c/mm³, viral load 5 million c/ml
Initial History-June 08
• Fever > 39.5°C every day (1 month)
• Cough (2 weeks)
• Shortness of breath on exertion
• Nightsweats (drenching)
• Loss of weight (10kg over 2 months)
• Headache (occasional)
• Leg swelling
10/13/2009
3
51%
6%
10%
0%
19%
2%
10%
2%
0%
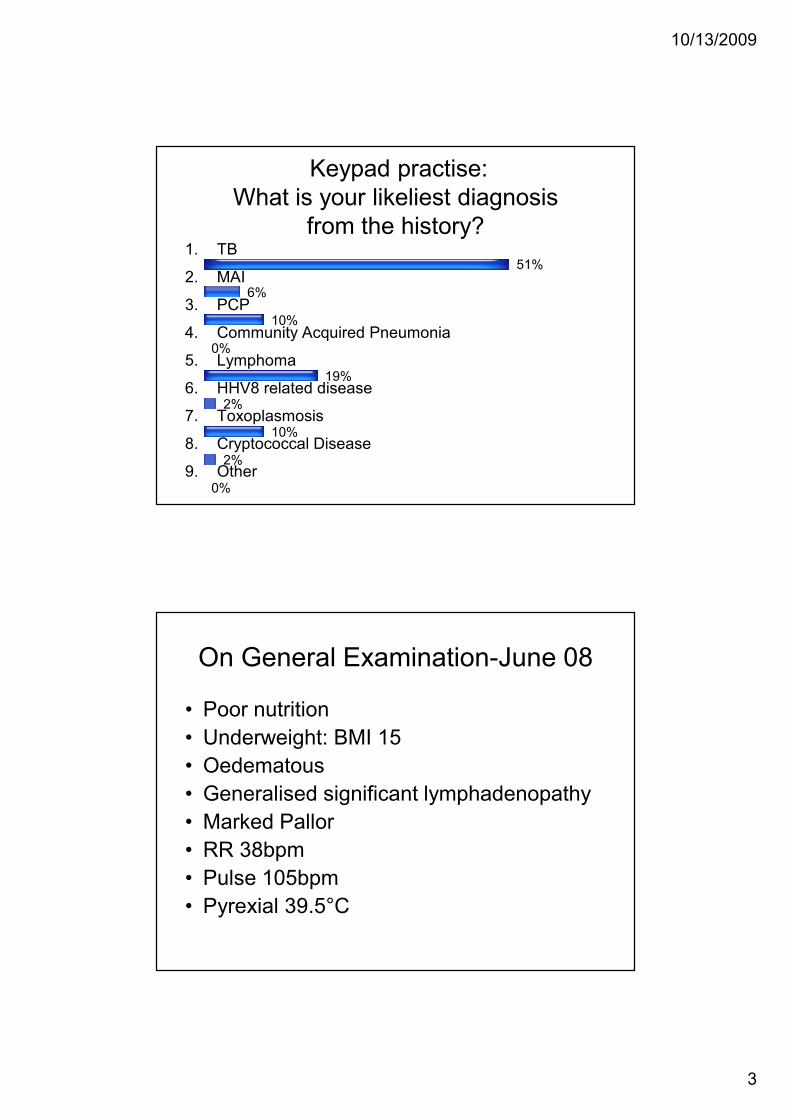
Keypad practise: What is your likeliest diagnosis
from the history?1. TB
2. MAI
3. PCP
4. Community Acquired Pneumonia
5. Lymphoma
6. HHV8 related disease
7. Toxoplasmosis
8. Cryptococcal Disease
9. Other
On General Examination-June 08
• Poor nutrition
• Underweight: BMI 15
• Oedematous
• Generalised significant lymphadenopathy
• Marked Pallor
• RR 38bpm
• Pulse 105bpm
• Pyrexial 39.5°C

10/13/2009
4
Systems Exam Revealed…
• CNS:NAD
• CVS: NAD
• Chest: bilateral crepitations, pleural effusion
• Abdomen: marked hepatosplenomegaly
• Skin: multiple skin lesions
Lab findings:
• Hb: 8.5g/dL
• WCC: 4.2 10/L
• Plt:62 10/L
• Albumin:25g/L
• LDH:364 iu/L
• CRP: 120 mg/L
• HHV8 VL :18,000c/ml
• Pleural fluid: no AFB, plasma cells identified

10/13/2009
5
Want to vote again?
8%
4%
0%
2%
17%
57%
8%
0%
4%
1. TB
2. MAI
3. PCP
4. Community Acquired Pneumonia
5. Lymphoma
6. HHV8 related disease
7. Toxoplasmosis
8. Cryptococcal Disease
9. Other
����

10/13/2009
6
• Diagnosed with
– Multicentric Castleman’s disease on cervical LN biopsy
– Disseminated KS (cutaneous and pulmonary)

10/13/2009
7
Treatment
• Immediate ARV’s: Truvada +EFV
• Rituximab 375mg/kg X 4 weekly cycles
– completed July 08
• Followed by 6 cycles of L-Doxorubicin
– Completed mid November 08
Outcome
• KS: lesions flattened and disappeared• Castleman’s Disease: responded • CD4 325, VL < 40c/ml on Atripla
• Back at work, asymptomatic• Stable until March 09 when he presented with difficulty in mobility
and swelling of his legs.• Indurated violaceous plaques involving his thighs • No ‘B ‘symptoms • No organomegaly. • R pleural effusion unchanged (tap -),Tb blood cultures -, TB Elispot -• Re-referred for urgent chemotherapy for KS

10/13/2009
8
This admission 4/5/9
• Admitted by referring hospital
• Teaching at his school until last week
• 5 day History: – feeling ‘unwell’
– fever
– confusion
– word finding difficulties
– diarrhoea
• CD4 191c/mm³, VL <40 c/ml on Truvada / EFV
• Recent treatment with L-Doxorubicin 2 weeks prior
• Most recent HHV8 VL 5900c/ml (Jan 2009)
10/13/2009
9
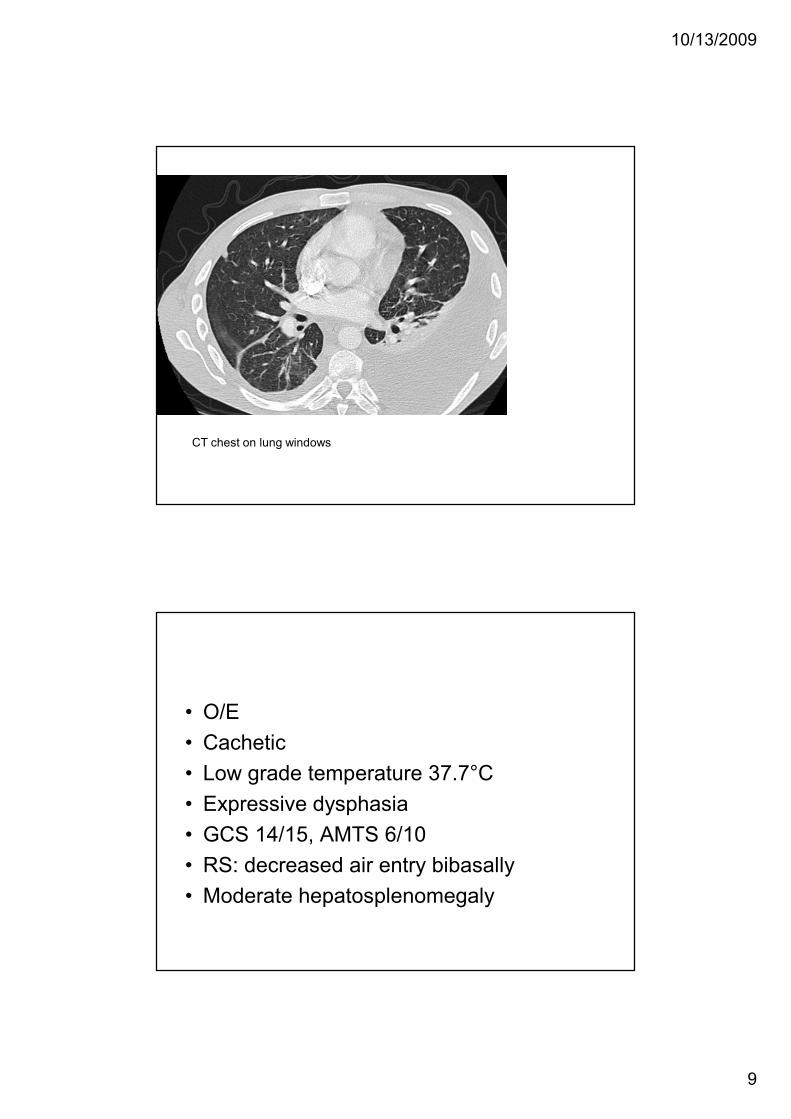
CT chest on lung windows
• O/E
• Cachetic
• Low grade temperature 37.7°C
• Expressive dysphasia
• GCS 14/15, AMTS 6/10
• RS: decreased air entry bibasally
• Moderate hepatosplenomegaly

10/13/2009
10
T2 scans Enhanced T1
Diffusion scan
Results
• Bloods: Hb 11.1, WCC 5.7, Plts 422, normal U&Es and LFTs, CRP 73
• LP:
– Opening Pressure 34cmHg,
– WCC 450 (L 70% N 30%),
– RCC 1840,
– protein 4.1g,
– glucose 1.8, (serum 4.5)
– LDH 137
– no organisms,
– India ink negative, CrAg negative

10/13/2009
11
• Started on
- Ceftriaxone, Metronidazole
- Aciclovir
- Sulphadiazine, Pyrimethamine, Calcium Folinate
• Transferred to Barts 5/5/9
• On arrival GCS 14/15. Able to mobilise and eating and drinking
6/5/9
• GCS dropped to 8/15 (E1M5V2)
• Pinpoint pupils bilaterally
• CT brain

10/13/2009
12
With contrast No contrast
3
12
21
8
9
1. Intracranial haemorrhage
2. Hydrocephalus
3. Thalamic tuberculomas
4. Basal ganglia ischaemia
5. MCA infarcts
What does the CT scan show?More than one answer possible
����
����

10/13/2009
13
Enhanced T1 scansT2 scan
Diffusion scan ADC
9%
6%
32%
15%
38%
What does the MR show?
1. Widespread tuberculomas
2. Deep venous thrombosis
3. Basal ganglia infarction
4. HIV encephalopathy
5. PML
Restricted diffusion-implies cell necrosis
����

10/13/2009
14
• Impression– Toxoplasmosis unlikely– ? Fungal– ? TB (previous Elispot negative in Jan 2009)
• Ceftriaxone/Metronidazole changed to Meropenem
• Quadruple TB therapy started• Liposomal amphotericin started• Aciclovir and Toxoplasmosis treatment
continued• Dexamethasone and Sodium Valproate started
7/5/9
• Reviewed by Oncology
• Clinically GCS fluctuating 8-10/15. Remains febrile
• Aciclovir and Toxoplasmosis treatment stopped
• ?seizure. GCS drops to 4/15
• Intubated and transferred to ITU.

10/13/2009
15
CT body on bony windows
ITU at RLH
• EEG showed no epileptiform activity
• Neurology team reviewed
• Working diagnoses,
- TB meningitis and vasculitis
- Lymphoma
- Disseminated fungal or bacterial infection

10/13/2009
16
Treatment
• Ambisome 200mg
• Rifampicin/ Isoniazid/ Ethambutol/ Pyrizinamide
• Meropenem 2g tds
• Dexamethasone 4mg qds
• Sodium valproate 200mg bd
• Phenytoin 100mg tds
• Truvada/ Efavirenz 800mg
• GCS remains 4
• 18/5/9: Transferred back to FAW. Made not for resuscitation or for escalation of treatment
• 19/5/9: Care of the dying pathway started. Remained on TB therapy and iv fluids
• 25/5/9: RIP

10/13/2009
17
Granuloma
2%
17%
81%
Had he survived… how long would you continue TB treatment for CNS
TB?
1. 6 months
2. 9 months
3. 12 months

10/13/2009
18
Case 2
Case 2
• 21 year old ♀ from Ivory Coast
• English student
• Resident in UK for 2 years-no travel.
• Known Mild Anaemia (β Thalassaemia trait).
• Living with parents.
• Non-smoker/no alcohol /drugs.
• One lifetime sexual partner from Ivory Coast at age 15

10/13/2009
19
History of presenting complaint
• Unwell for 2 months prior to this with productive cough-attended GP 10th June 09.
• GP arranged:– sputum culture (3x AAFB smear neg on 11,12,15 June)
– CXR
• Referred to East London DGH on 23/6/9 OPD
• Admitted from OPD:– left sided weakness
– numbness of left hand
• Bloods showed Na 128, Ur 6.4, Cr 150, Alb 27, CRP 50, Hb 8.4, MCV 65.3, WCC 5.0, N 2.6, L 1.4, Plt 271
• e GFR 49ml/min
• Albumin 22g/L
• Creatinine 120µmol/L
• Urea 7.5mmol/L

10/13/2009
20
PA CXR

10/13/2009
21
T2 scan
Enhanced T1 scan
Diffusion
9%
56%
7%
28%
0%
What does the MR show
1. HIV encephalopathy
2. Ring enhancing lesion(s)
3. RT MCA infarct
4. Bacterial abscess
5. PML
MULTIPLE LESIONS TB/TOXO/LYMPHOMA ?
����

10/13/2009
22
8%
0%
14%
14%
60%
0%
4%
What Treatment Would you start?
1. Toxoplasmosis treatment only
2. TB Treatment only
3. Toxoplasmosis Treatment with steroids
4. TB treatment with steroids
5. Toxoplasmosis Treatment, TB treatment, steroids
6. Aciclovir
7. I would refer for biopsy before treatment
24/6/9 at DGH
• Started 1st line treatment for toxoplasmosis and sodium valproate 200mg bd.
• Remained febrile during admission and complaining of headache.

10/13/2009
23
26/6/9: Transferred from DGH to Barts
• Neuro: Power 4/5 LUL and 3/5 LLL with decreased sensation to light touch, vibration and proprioception.
• Toxoplasma treatment stopped as likely TB.• Started on TB quadruple therapy and dexamethasone
8mg bd. Transfused 2 units blood.• 29/6/9: Bronchoscopy – No AAFB, No PCP, cultures
sent• 30/6/9:Renal USS ‘diffusely enlarged kidneys bilaterally
with decreased corticomedullary differentiation in keeping with HIVAN’.
• Urine PCR >400• 4/7/9 renal r/v: Likely HIVAN. Not for biopsy as yet.
Results:
– CD4 45 cellsmm³, VL 255040c/ml
– Genotype CRF02-AG, fully susceptible
– Toxo serology IGg positive
– TB Elispot negative
– CrAg negative
– Hep B/C negative
– STS negative
– EBV DNA plasma < 250c/ml
10/13/2009
24
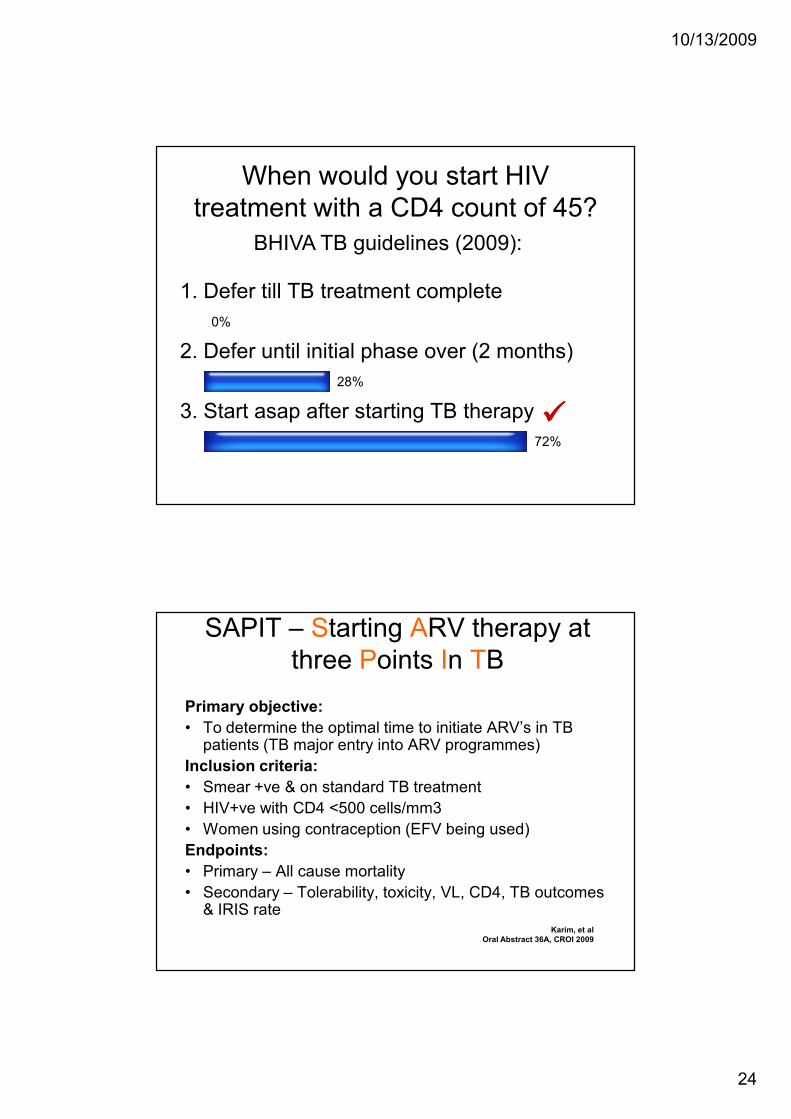
0%
28%
72%
When would you start HIV treatment with a CD4 count of 45?
1. Defer till TB treatment complete
2. Defer until initial phase over (2 months)
3. Start asap after starting TB therapy
BHIVA TB guidelines (2009):
����
SAPIT – Starting ARV therapy at three Points In TB
Primary objective:
• To determine the optimal time to initiate ARV’s in TB patients (TB major entry into ARV programmes)
Inclusion criteria:
• Smear +ve & on standard TB treatment
• HIV+ve with CD4 <500 cells/mm3
• Women using contraception (EFV being used)
Endpoints:
• Primary – All cause mortality
• Secondary – Tolerability, toxicity, VL, CD4, TB outcomes & IRIS rate
Karim, et al
Oral Abstract 36A, CROI 2009

10/13/2009
25
SAPIT study- Mortality rates per CD4 count
Arm CD4 count
<200 cells/mm3 >200 cells/mm3
Integrated arm
•# dead/py (n)
•Mortality rate
23/281 (273)
8.2 (5.2-12.3)
2/185 (156)
1.1 (0.1-3.9)
Sequential arm
•# dead/py (n)
•Mortality rate
21/137 (138)
15.3 (9.57-23.5)
6/86 (75)
7.0 (2.6-15.3)
Hazard ratio
•Cox regression
0.54 (0.34-0.98)
P=0.04
0.16 (0.03-0.79)
P=0.02
Reduction in mortality rates is present in patients with CD4
counts above and below 200 cells/mm3
Karim, et al
Oral Abstract 36A, CROI 2009
Progress
• 13/7/9: Started on Atripla and EFV 200mg (wt 65kg) within 2 weeks of TB therapy
• TDM EFV done at 2 weeks post start
• 14/7/9: Repeat MRI

10/13/2009
26
T2 scan Enhanced T1 scan

10/13/2009
27
Results
• 27/7/9: BAL TB culture positive.
• Rifampicin sensitive.
Case 3

10/13/2009
28
Case 3
• 38 year old heterosexual Brazilian ♂• Dx HIV+ at DGH on 13/03/09 • Presented to Urology with haematuria and back pain• No diarrhoea• No other symptoms• He was found to be anaemic• Referred for CT abdomen which showed no renal lesion and splenomegaly• Referred to haematology • Autoimmune haemolytic anaemia
– Hb 6.6 g/dL– WCC 3.5 109/L– PLT 179 109/L– Reticulocytes:6.8%
• CD4 30c/mm³, VL 89,000c/ml
• CrAg + (1/16)• CSF Crag -, LP otherwise ‘normal’• Hep B vaccinated, Hep C Ab-• STS –• Started on Tvda/Lop/r 20/03/09
Referred to Barts for Investigation and Treatment of Auto-immune Haemolytic
AnaemiaBlood Film: Erythrocyte poikilocytosis with polychromasia++, and
microspherocytes Imp: haemolysis– G6PD :normal– Haemoglobinopathy screen: normal
• BM: Hypercellular marrow with erythroid predominance and megaloblastoid / dyserypoietic features . No morphological evidence of bone marrow sepsis, infiltration or granulomas.
• Required steroids (unresponsive)• Multiple blood transfusions• Full septic workup including TB cultures and CSF analysis which
was unremarkable• LDH: 1704 iU/L• Ongoing back pain

10/13/2009
29
Sag T2 Sag T1
Axial T2
3
5
2
40
20
What does the MR showMore than one answer possible
1. Traumatic fracture of L1
2. Diffuse bone marrow abnormality
3. Cauda equina compression
4. Infiltration of L1
5. Paraspinal soft tissue at L1
TB or Lymphoma can produce paraspinal soft tissue
����
����
����

10/13/2009
30
PET 1
Biopsy

10/13/2009
31
• Commenced high risk DLBCL treatment under the R-CODOX-M and IVAC schedule (due to his stage, LDH and greater >1 extra
nodal site).
• Neurosurgeons lumbar vertebrae unstable Cox Brace for mobilisation
69%
31%
In view of the diagnosis, would you change the HAART-Truvada/Lop/r
to another regime?
1. Yes
2. No
����

10/13/2009
32
61%
9%
28%
0%
2%
What?
1. Kivexa or Truvada +EFV
2. Kivexa or Truvada +Nevirapine
3. Kivexa or Truvada +Raltegravir
4. Truvada or Kivexa +alternative PI/r
5. I would stop HAART during the intensive chemotherapy to avoid additive toxicity
����
ARV switch
• GART: Clade B, wild-type
• Medications on Discharge:– Truvada po od, Efavirenz 600mg po od,
– Co-trimoxazole 960mg po Monday, Wednesday, Friday
– Acyclovir 400mg po bd
– Fluconazole 200mg po od
– Allopurinol 300mg po od
– Azithromycin 1250mg po once a week

10/13/2009
33
PET 2
PET 1

10/13/2009
34
Quick Quiz
T2scan Diffusion scan
Enhanced T1 scan
Quick Quiz 1

10/13/2009
35
What does this show?
Toxoplasmosis
Neurocysticercosis
HIV Dementia
CerebralAbscesses
�
�
�
�
� �� �
55%
19%
0%
26%
T2 scan Enhanced T1 scan
Quick Quiz 2

10/13/2009
36
What does this show?
HIV Dementia
HIVencephalopathy
Ependymitis
Hydrocephalus
�
�
�
�
� �� �
14%
56%
10%
20%
T2 scan Enhanced T1 scan
Quick Quiz 3

10/13/2009
37
What does this show?
Hydrocephalus
PML
Acute demyelinatingencephalomyelitis
�
�
�
�
HIVencephalopathy
� �� �
35%
23%
17%
25%
FLAIR scans
Enhanced T1 scansQuick Quiz 4
Diffusion scan

10/13/2009
38
What does this show?
CVA
Posterior reversibleencephalopathy syndrome
PML
TB
�
�
�
�
� �� �
10%6%
64%
20%
T2 scan Enhanced T1 scan
Diffusion scan Quick Quiz 5

10/13/2009
39
What does this show?
Tuberculoma
Primary CNS lymphoma
Toxoplasmosis
Echinococcosis
�
�
�
�
� �� �
22%
65%
0%
13%
Thanks
•Dr Steve Ellis
•Dr Rasgeshri Dhairywan
•Dr Vanessa Apea
•Dr Hasan Rizvi
•Dr Andy Williams



![CR-1 : @TAWAS B LIB.TAWAS B(SCH 1):PAGE1 TAWASnotebookschematic.org/data/NOTEBOOK/attachments/SC... · resume gp[6] gp[7] gp[8] gp[9] 3.3v 3.3v 3.3v 3.3v gp[23] gp[24] gp[25] gp[26]](https://img.pdfslide.us/doc/110x75/5f812ff679030c23f20de0bd/cr-1-tawas-b-libtawas-bsch-1page1-ta-resume-gp6-gp7-gp8-gp9-33v.jpg)