Embed Size (px)
Citation preview

©2015 MFMER | slide-1
Caring for the Critically Ill Patient with Cerebral Palsy
Hannah Sauer, PharmDPGY1 Pediatric Pharmacy Resident
Mayo Clinic Children’s Center

©2015 MFMER | slide-2
Objectives• Describe challenges in acute medical
management of patients with cerebral palsy (CP)
• List special considerations for drug therapy in patients with CP
• Identify the optimal approach to pain and sedation in patients with CP

©2015 MFMER | slide-3
Objectives• Describe challenges in acute medical
management of patients with cerebral palsy (CP)
• List special considerations for drug therapy in patients with CP
• Identify the optimal approach to pain and sedation in patients with CP

©2015 MFMER | slide-4
Cerebral Palsy (CP)• Occurs in 205 per 1000 live births• Permanent disorder of the development of
movement and posture resulting in activity limitation
• Caused by non-progressive disturbances that occurred in the developing fetal or infant brain
Novak, I. J Child Neurol, 2914; 29(8):1141-1156.

©2015 MFMER | slide-5
Morbidity and Mortality• Most have normal life expectancy
• 5-10% mortality during childhood• Comorbid epilepsy and intellectual disability
predictive of premature death• Deterioration of function occurs due
musculoskeletal impairments• Medical interventions do not improve overall
gross motor function
Taft, LT. Pediatrics in Review, 1995; 16(11):411-418.Novak, I. J Child Neurol, 2914; 29(8):1141-1156.

©2015 MFMER | slide-6
Classification by Severity
I - Indepdently ambulates
II - Indepdently ambulates withlimitations
III - Ambulates with walking aids
IV - Independently mobilizes withpowered mobility
V - Dependent for all mobility

©2015 MFMER | slide-7
Most patients with CP will walk
I - Indepdently ambulates
II - Indepdently ambulates withlimitations
III - Ambulates with walking aids
IV - Independently mobilizes withpowered mobility
V - Dependent for all mobility

©2015 MFMER | slide-8
CP Subtypes
SpasticDyskineticAtaxic

©2015 MFMER | slide-9
ComorbiditiesNeurologic/Psychiatric
• Intellectual disability (50%)• Behavior disorder (25%)• Non-verbal (25%)• Epilepsy (25%)• Bladder incontinence (25%)• Sleep disorder (20%)
Musculoskeletal• Chronic pain (75%)• Hip displacement (33%)
Sensory• Blindness (10%)• Deafness (4%)
Other• Chronic lung disease (33%)• Gastroesophageal reflux• Hyper-salivation

©2015 MFMER | slide-10
“Chronic Critical Illness”• Complex disease state with multiple
comorbidities• Common reasons for ICU admission
• Orthopedic surgeries• Acute infections (pneumonia)• Refractory epilepsy
Novak, I. J Child Neurol, 2914; 29(8):1141-1156.

©2015 MFMER | slide-11
Challenges in Cerebral Palsy
•Pediatric features•Limited literature
• Polypharmacy• Medication
sensitivity?
• Communication barriers
• Emotional burden• Low rates of
confidence• Consult overload
Provider Factors
Patient Factors
Disease Factors
Medication Factors

©2015 MFMER | slide-12
Objectives• Describe challenges in acute medical
management of patients with cerebral palsy (CP)
• List special considerations for drug therapy in patients with CP
• Identify the optimal approach to pain and sedation in patients with CP

©2015 MFMER | slide-13
Common Medications
• Anti-epileptics• Anti-spasticity • Anti-spasmodics• Analgesics• Antacids
• Laxatives• Anti-sialogogues• Prophylactic
antibiotics• Bisphosphonates
Novak, I. J Child Neurol, 2014; 29(8):1141-1156.
Assess for drug interactions.

©2015 MFMER | slide-14
Drug Sensitivity • May be more sensitive to dose changes• Comorbid intellectual disability associated with
idiosyncratic reactions• Increased risk for medication withdrawal?
Nolan, J, et al. Anaesthsia, 2000; 55(32-41).

©2015 MFMER | slide-15
Intrathecal Baclofen Withdrawal• If pump must be removed oral baclofen should
be started 2-3 days beforehand• Monitor for withdrawal
• Tachycardia, labile pressures, hypothermia• Delirium, hallucinations, seizures• Muscle rigidity, paresthesis
• Symptom-directed treatment
Ross, JC, et al. Neurocrit Care, 2011; 14:103-108.

©2015 MFMER | slide-16
Paralytic Agents• Up-regulation of ACh receptors in CP patients
(30%)• Increased risk of hyperkalemia following
succinylcholine?• Increased sensitivity to non-depolarizing
agents?
Prosser, DP and Sharma, N. Anaesthsia, 2010; 10(3):72-76.

©2015 MFMER | slide-17
Paralytic Agents• Up-regulation of ACh receptors in CP patients
(30%)• Increased risk of hyperkalemia following succinylcholine?• Increased sensitivity to non-depolarizing agents?
Clinically… • Succinycholine is not contraindicated• Non-depolarizing agents are less potent and
have shorter duration
Prosser, DP and Sharma, N. Anaesthsia, 2010; 10(3):72-76.

©2015 MFMER | slide-18
Dosing Considerations• Increased body surface area to body weight
ratio (“giant neonates”)• Low body weight relative to non-CP individuals• Poor nutritional status
• Altered absorption• Dehydration and hypovolemia common
• Consider appropriate assessments of renal function
Taft, LT. Pediatrics in Review, 1995; 16(11):411-418.Novak, I. J Child Neurol, 2914; 29(8):1141-1156.

©2015 MFMER | slide-19
ASSESSMENT QUESTION 1Which of the following represents a true statement about critically ill adult patients with CP?
a) Serum creatinine is a reliable indicator of renal function
b) Succinylcholine is an appropriate paralytic agent for rapid sequence intubation
c) Intrathecal baclofen can be safely held for 48 hours
d) Pediatric weight-based dosing should be avoided in anyone over 18 years

©2015 MFMER | slide-20
General Principles of Medication Management• Use appropriate weight-based dosing, even in
adult patients• Keep medication withdrawal on differential• Consider unpredicted responses to medications• Re-start home medications as soon as possible

©2015 MFMER | slide-21
Objectives• Describe challenges in acute medical
management of patients with cerebral palsy (CP)
• List special considerations for drug therapy in patients with CP
• Identify the optimal approach to pain and sedation in patients with CP

©2015 MFMER | slide-22
Audience Poll: True or False“Individuals with cerebral palsy are desensitized to pain and therefore have increased pain tolerance.”
A. TrueB. False

©2015 MFMER | slide-23
Pain in CP• Increased sensitivity to pain stimuli due to
altered excitability in the somatosensory cortex• Heterogeneous pain experiences both inter-
and intra-personally • Typical and atypical physical manifestations• Significant emotional and spiritual burden
Riquelme I, et al. Pain Med, 2011; 12(4):535-545.Warlow and Hain. Children 2018; 5(13).

©2015 MFMER | slide-24
Warlow and Hain. Children 2018; 5(13).
PainMusculoskeletal
Hypertonia
Muscle fatigue, immobility
Constipation
Gastrointestinal dysmotility
Baseline Pain Burden• 75% of patients experience pain at least weekly• 50% have episodes of pain that last >9 hours

©2015 MFMER | slide-25
Post-Operative Pain Management• Post-operative analgesia should be continuous
rather than on demand regimens• Options:
• Continuous intravenous opioids • Intermittent intravenous and oral opioids• Epidural opioids• Epidural opioids + local anesthetic

©2015 MFMER | slide-26
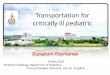
Epidural v. Systemic Analgesia ProtocolsMoore, et al.
Study design Retrospective comparison of post-operative analgesia protocols
Population Pediatric patients with cerebral palsy undergoing selective dorsal rhizotomy
Efficacy Outcomes Difference in age-appropriate pain scale scoreFrequency of severe pain episode (pain ≥5)
Safety Outcomes Treated nausea or pruritisHypoxia, supplemental O2 requirements
Moore, et al. Pediatric Anesthesia, 2013; 23(720-725).

©2015 MFMER | slide-27
Moore, et al. Pediatric Anesthesia, 2013; 23(720-725).
Systemic Protocol
Epidural Protocol
• Continuous infusion fentanyl
• 1 mcg/kg/h x12 hours followed by
• 0.5 mcg/kg/h until noon POD2
• Diazepam 0.1 mg/kg q4h scheduled x6 doses, then q6h x4 doses
• Gabapentin added D2 for kids ≥ 10 years
• Ropivicaine 0.2%/ hydromorphone 2.5 mcg/mL
• Rate of 0.2 mL/kg/h until 6 am POD3
• Ketorolac 0.5 mg/kg q6h (total of 8 doses)
• Methocarbamol 15 mg/kg q8h prn for breakthrough spasm

©2015 MFMER | slide-28
POD1 POD2 POD3
Fentanyl @1 Fentanyl @0.5
Midazolam
Ropivacaine/hydromorphone epidural
Ketorolac
Methocarbamol as needed
Gabapentin if age-appropriate
Study Protocols
Systemic ProtocolEpidural Protocol

©2015 MFMER | slide-29
Patient Characteristics
Epidural (n=31) Systemic (n=41)
Age (years) 6.06 (±3.78) 6.63 (±4.02)
Weight (kg) 21.43 (±9.53) 24.9 (±14.12)
Male 64.5% 61%
Diplegia 93.5% 92.6%
Moore, et al. Pediatric Anesthesia, 2013; 23(720-725).

©2015 MFMER | slide-30
Post-Operative Pain Scores
0
1
2
3
4
5
6EpiduralSystemic
*p<0.05Moore, et al. Pediatric Anesthesia, 2013; 23(720-725).

©2015 MFMER | slide-31
ResultsEpidural (n=31) Systemic (n=41) OR p-value
Episodes of severe pain (POD 0-1)
9.6% 68.3% 20.1 <0.001
Episodes of severe pain (POD 0-1)
5 episodes 74 episodes NR NR
Respiratorydepression 6.5% 41% 10.3 <0.001
POD=post-op dayMoore, et al. Pediatric Anesthesia, 2013; 23(720-725).

©2015 MFMER | slide-32
Epidural v. Systemic Analgesia ProtocolsStudy Conclusions• Multimodal approach to
pain control is ideal
• Epidural may be preferred route of analgesia in post-operative setting
Study Limitations• Study design
• Cause of improved pain control?
• Other medications not reported
• Pain assessment tools
Moore, et al. Pediatric Anesthesia, 2013; 23(720-725).

©2015 MFMER | slide-33
Validated Pain Assessment Tools
Pediatric Pain Profile (PPP)
• Twenty item behavioral scale (4
points each)• Designed for non-verbal children with severe neurological
impairment (SNI)• Highly sensitive and
specific
Face Legs Activity Cry Consolability
(FLACC)• Five item behavior scale (3 points each)• Quick assessment
• Only validated in post-operative settings for
SNI
Non-Communication Children’s Pain
Checklist—Revised • Thirty item behavior scale (4 points each)
• Two hours of observation required
• Highly sensitive and specific
• Weak correlation to parent scores
Warlow and Hain. Children 2018; 5(13).

©2015 MFMER | slide-34
ASSESSMENT QUESTION 2:Which of the following may be a sign of pain in a non-verbal patient with cerebral palsy?a) Flushing and/or pallorb) Tachycardiac) Sudden stillnessd) Self-harme) All of the above

©2015 MFMER | slide-35
Procedural Sedation in CP • Preferred agents
• Historically propofol, benzodiazepines• No sedative agents contraindicated
• Consider co-morbidities• Seizures• Respiratory status
• Optimal doses and general approaches remain controversial…

©2015 MFMER | slide-36
Sedation in Patients with CP• Disability associated with risk for respiratory
depression and delayed awakening• Review of intravenous sedation in patients with
disabilities revealed cerebral palsy:• Independently associated with SpO2 <90%
(OR 1.642, p=0.018)• Not independently associated with delayed
awakening
Yoshikawa, et al. Anesth Prog, 2013; 153-161.

©2015 MFMER | slide-37
General Anesthesia in CP • Patients with cerebral palsy require lower doses
of propofol for anesthesia induction• Target bispectral index (BIS™) 35-45• 3.29 mg/kg versus 3.6 mg/kg (p=0.03)
• Decreased minimum alveolar concentration (MAC) of halothane
• Levels 20% lower compared to healthy controls (p<0.05)
• Delayed emergence? Saricaoglu F, et al. Pediatric Anesthesia, 2005; 15:1048-1052.Frei, FJ, et al. Anaesthesia, 1997; 52(11):1056-1060.

©2015 MFMER | slide-38
Optimal Propofol Dose for MRIKim, et al.
Study PopulationCerebral palsy Age 6 months to 5 yearsScheduled for brain MRI under sedation
Intervention
Propofol started at 2 mg/kg and modified for sequential patients• If unsuccessful, dose increased by 0.5 mg/kg for
next child• If successful, decreased by 0.5 mg/kg for next child
Efficacy OutcomesSuccessful sedation (UMSS* score ≥3 after 1 minute)ED50 and ED95 determined by modified up-and-down method
Kim EJ, et al. Korean J Anesthesiol, 2011; 61(3):216-19.*University of Michigan Sedation Scale

©2015 MFMER | slide-39
Patient CharacteristicsN=20
Age 28.7 months ± 17.8
Weight 10.3 kg ± 4.6
Male 80%
MRI scanning time 26.3 minutes
Co-morbid behavior disturbances 16
On anti-epileptic medications 4
Kim EJ, et al. Korean J Anesthesiol, 2011; 61(3):216-19.

©2015 MFMER | slide-40
Results• Successful completion of all MRI scans
• Ten received 2 mg/kg (50% success)• Five received 1.5 mg/kg (0% success)• Five received 2.5 mg/kg (80% success)
• Desaturation in 5 patients with successful sedation
• Proposed therapeutic index:• ED50 = 2.07 mg/kg (CI 1.69-2.56)• ED95 = 2.69 mg/kg (CI 2.35-5.95)*
• Mean total dose 3.2 mg/kg ± 0.9 mg/kg*Up-down method used
Kim EJ, et al. Korean J Anesthesiol, 2011; 61(3):216-19.

©2015 MFMER | slide-41
Study Summary and Conclusions• Typical starting procedural sedation 1-2 mg/kg• CP alone may not be a compelling indication to
give lower doses of procedural sedation• Lingering questions
• What subgroups of patients are worth exploring?• Is desaturation in 25% of patients significant?• What is the appropriate starting dose of propofol for
procedural sedation?
Kim EJ, et al. Korean J Anesthesiol, 2011; 61(3):216-19.

©2015 MFMER | slide-42
The Bottom Line for Pain and Sedation• Assess and treat anxiety related to disease and
hospitalization• Multimodal approaches to pain are ideal (don’t
forget about baseline pain factors)• Continuous pain control > on demand pain control• Use appropriate pain assessment tools and rely
on caregiver assessments• Start with low end of sedative dose ranges and
titrate slowly

©2015 MFMER | slide-43
ASSESSMENT QUESTION 3:A 24 yoM (30 kg) with cerebral palsy s/p orthopedic surgery is being admitted to your ICU. Which of the following standard post-operative orders is your priority for re-assessment prior to his arrival to the unit?
a) Morphine PCA 2 mg load, followed by (level 1) 1 mg IV every 10 minutes 20 mg LO q4h
b) Ketorolac 15 mg IV q6h x 4 dosesc) Cefazolin 1 g q8h x2 dosesd) Senna 17.2 mg PO QHS

©2015 MFMER | slide-44
Summary• A lack of published experience in managing CP
patients in ICU settings makes it a challenging population
• Patients with CP should be assessed for appropriate weight-based dosing, drug interactions and medication withdrawal
• CP does not permit a “one size fits all” approach to optimal pain and sedation