Embed Size (px)
Citation preview

PEOPLE CARING FOR PEOPLE
carelines
carelines
carelines
carelines
carelines
carelines
carelines+
carelines
carelines
plus
Issue # 7
EBOS HealthcareAged Care Division
Free call: 1800 269 534 Free fax: 1800 810 257
Email: [email protected]
July 2014
Save the environment, sign up to receive this newsletter via email. Visit: www.eboshealthcare.com.au
Products for practice: Moist wound healingPage 10-15
Better oral health in residential aged carePage 9
EBOS NEWS & CONFERENCESPage 16,17
Dysphagia and new FMR solutionsPage 7

2 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 3
To the 7th edition of Carelines!In this issue you will find “Products for Practice’, a brand new section where we talk about a new range of super-absorbent dressings specifically designed for moist would healing. The article includes case studies together with a thorough explanation of what the novel super-absorbent polymer technology (SAP) can do to achieve optimal moisture levels for healing.
We speak with the Head of R&D at Flavour Creations about some innovative ‘real food’ solutions just launched for people with dysphagia and we have an article on the final report from the Australian Government Better Oral Health in Residential Healthcare Project.
As usual we include lots of information on the topics that are relevant to you eg skin care, protection and lifting equipment as well as reviewing some new products that have just been launched at EBOS Aged Care.
We hope you will find Carelines full of interesting information and that you will be able to use some of this content as part of your CPD plan.
A couple of reminders on how to get in touch with us:
• The latest issue of Carelines is available on our corporate website www.eboshealthcare.com.au
• If you want to send us comments or suggestions on what you would like to see next in Carelines just email us at [email protected]
• Our online ordering system www.ebosonline.com.au contains over 10,000 products across all the product categories you need for your Facility. Make sure you visit the website, browse the product range and register to order online. It’s quick and easy!
Cheers,
The Aged Care Team
@ EBOS Healthcare
National Account ManagerDebbie Greenaway0400 424 [email protected]
National Equipment Co-ordinatorDe’Ann Keevers0417 497 [email protected]
Key Account Manager NSWElizabeth Conridge 0419 612 [email protected]
Key Account Manager VICCarolyn Knight 0411 542 [email protected]
Key Account Manager SAJanet Pitts 0416 130 [email protected]
Key Account Manager QLDLarissa Mueller0417 524 [email protected]
Key Account Manager QLDLiz Wiggins0414 486 [email protected]
Key Account Manager WAGlen Charles0408 [email protected]
Asst. to National Acct MgrEmma Belgre02 9502 [email protected]
carelines
carelines
carelines
carelines
carelines
carelines
carelines+
carelines
carelines
plus
CARELINES ISSUE #6
Key Account Manager QLDLarissa Mueller0417 524 [email protected]
Key Account Manager VICCarolyn Knight 0411 542 [email protected]
Key Account Manager QLDLiz Wiggins0414 486 [email protected]
National Account ManagerDebbie Greenaway0400 424 [email protected]
National Equipment Co-ordinator Key Account Manager SAJanet Pitts 0416 130 [email protected]
Key Account Manager WAGlen Charles0408 [email protected]
Our Aged Care Team
page 3Contribute to your CPD with Carelines,EBOS Aged Care Division
page 4 New products at EBOS Aged Care
page 5Gastroenteritis Preparedness Kit from the Outbreak Coordinator’s Handbook
page 6Australian research shows link between anemia & Alzheimer’s disease
page 7Dysphagia and new FMR solutions
page 9Better oral health in residential aged care
page 10Products for practice: Moist wound healing
page 16 Conference and Event News
page 17 In the Spotlight: Emma Belgre
page 18 Skin care - Why is it important to us all?
page 19Case study: Prevention of skin lesions in the sacral region in an incontinent patient
page 22Vernacare introduces new VernaFem in Australia
National Equipment Co-ordinatorDe’Ann Keevers0417 497 [email protected]
Key Account Manager NSWElizabeth Conridge 0419 612 [email protected]
Contribute to your Continuing Professional Development (CPD) with CarelinesThe CPD Registration Standard for Nurses and Midwives sets out a minimum requirement of 20 hours of continuing nursing professional development per year for nurses on the nurses’ register.
One hour of active learning will equal one hour of CPD, and the CPD must be relevant to the nurse’s context of practice. You can read Carelines as self-directed CPD, as a tool to maintain, improve and broaden your knowledge, expertise and competence as a nurse working in Aged Care.
For more information on self-directed CPD, the CPD cycle and how to document your CPD see the Nursing and Midwifery Board of Australia – ‘Continuing professional development registration standard.’
carelines
carelines
carelines
carelines
carelines
carelines
carelines+
carelines
carelines
plus
EBOS – A FRESH, INNOVATIVE PARTNER WITH THE PEOPLE, ORGANISATIONAL STRENGTH, PRODUCTS, SYSTEMS AND COVERAGE TO HELP YOU DELIVER SUPERIOR VALUE TO YOUR RESIDENTS
With the continued expansion of the general aged care sector, aged care providers are faced with the challenge of improving quality of service to residents at an economic scale.
EBOS provides a consistently high standard of service, support and a streamlined ordering process as a single supply partner for your medical consumable and equipment needs.
We have a dedicated Product Catalogue for our Aged Care division, where our customers can easily find all the product categories they need every day for their facilities.
Our customers can then review and order these products online through our fast and easy online ordering system at www.ebosonline.com.au. A simple and efficient way to do all your purchases.
We deliver economies of scale and measurable continuous improvement without compromising best practice.
EBOS is Australasia’s largest and most experienced provider of medical supplies and equipment across the general healthcare market. We are proud to be ‘in-tune’ with the needs of our customers and are committed
to providing the most responsive and professional service levels. With a commitment to sourcing sustainable products and providing first class supply chain solutions, EBOS is an outstanding supply partner for aged care facilities.
EBOS Aged Care delivers a comprehensive support package at facility, procurement and management level. We believe we:
• are capable of demonstrating an efficient track record with a national supply chain solution
• have proven management systems and consistent service standards
• are prepared to develop innovative support platforms that complement your culture and strengths
• offer a competitive price without compromising service or support levels
Most importantly, our people bring a commitment to customers, fresh ideas, integrity and determination that provide the best possible service and supply chain solution.
EBOS Aged Care DivisionPEOPLE CARING FOR PEOPLE
CARELINES ISSUE #7
Asst. to National Acct MgrEmma Belgre02 9502 [email protected]
Our presence is national with warehouses conveniently located in major cities so
we can meet all your product and service requirements efficiently.

4 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 5
CARELINES ISSUE #
No facility or office should be without a quality first aid kit.
Our new First Aid kits contain a comprehensive variety of first aid products to cover general medical applications in a variety of work environments.
The A Kits have been designed for up to 25 people in any work place and the B range for more than 25 people at one time. Both kits are ideally suited for aged care facilities. They are availabe in a wall mountable plastic box or plastic tackle for mobile convenience.
Essential First Aid Kits
CARELINES ISSUE #7
We have just launched a brand new range of woundcare products under our InHealth brand of quality medical consumables.
The InHealth range already features autoclave pouches, ECG electrodes, examination gloves, saline solutions, tourniquets, urine drainage bags and closed system bags.
The new range landed in our warehouses last month, so if you are interested in high quality dressings at low prices, ask our Customer Service or your Key Account Manager about our new InHealth Woundcare range.
EBOS introduces a new range of high quality woundcare dressings and tapes under the INHEALTH value brand.
Product Qty CodeNon Adherent Dressing5x5cm Box/100 19220050
10x10cm Box/100 19220051
7.5x5cm Box/50 19220052
7.5x10cm (Lite)
Box/50 19220053
Adhesive Island Dressing6x7cm Box/50 19220054
10x6cm Box/50 19220055
10x12cm Box/20 19220056
Waterproof Film Dressing6x7cm Box/50 19220057
10x12cm Box/50 19220058
Waterproof Island Film Dressing6x7cm Box/25 19220059
8x10cm Box/25 19220060
Woundcare Range
Product First Aid kit A First Aid kit A First Aid kit B First Aid kit BType Plastic Tackle Steel - Wall mounted Plastic Tackle Steel - Wall mounted
Code AFATACKLE AFKS1405 AFBTACKLE AFKS1404
For more information on any product featured please contact customer service on
1800 269 534
NEW Gastroenteritis Preparedness Kit from the Outbreak Coordinator’s HandbookProducts at EBOS Aged Care
Prevent spreadAdequate supplies of Personal Protective Equipment, including:• Aprons• Gloves • Gowns (BX7000)• Disposable toilet pans (101AA100) • Protective eyewear (CAD1755)• Dust/mist masks (Earloop- GUPM004, N95 Face Mask- SN36361335)• Extra liquid soap and alcohol-based hand gel/rub (DEB6045)
Extra supplies of cleaning equipment, including:• Detergents • Bleach (NB: check expiry date)• Paper towels • Alcohol wipes (min.70%) (901SW225)• Variety of single-use cloths, colour coded for separate tasks• Containers for disposing items, waste bags (GUCW003), separate linen bags (CAMELT)
Resources for the Outbreak Coordinator• Gastro Info Kit • Outbreak Management Plan• State/Territory supplied gastroenteritis resources
Notification details and legislation• GP contact list • List of notifiable parties and relevant contact details • Forms required for notification • Legislation listing notifiable parties for your jurisdiction
Documentation - Templates for recording information, including:• Listing of symptomatic residents or staff - updated daily (e.g. onset time, complications, contacts)• Photocopies of the relevant hand outs from the Gastro Info Kit, including Information and Resource Sheets and poster• Copy of Outbreak Management Plan • Specimen Tracking Form• Details of groups at risk
Collect specimens• Disposable spatulas • Pathology request forms • Specimen jars and labels • Water proof bags• Designated specimen esky
External resourcesIt may be appropriate to store instructions within the Preparedness Kit for the location of certain items that are not suited for storage in the Kit. For example:• Designated specimen refrigerator • Infection control guidelines
This Preparedness Kit should be assembled by the Outbreak Coordinator in preparation for any gastroenteritis outbreaks.The items listed in this Kit will be essential during an outbreak of Gastroenteritis.NB: It is important to monitor the expiry dates of some items.
Extracted from the Gastro-Info - Outbreak Coordinator’s Handbook.For more information please visit www.health.gov.au
For more information on any product featured above please contactcustomer service on 1800 269 534

6 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 7
CARELINES ISSUE #CARELINES ISSUE #7
Australian scientists have discovered a link between Alzheimer’s disease and anemia (lower levels of hemoaglobin in the blood).
In an article published in the journal Molecular Psychiatry (Jan 2014), Professor A. Bush, Dr Faux and their colleagues from the Cooperative Research Centre for Mental Health explain the results of their study conducted on the blood of 1,112 volunteers - some healthy, some with mild cognitive impairment and some with Alzheimer’s desease.
They found that individuals with Alzeheimer’s disease had significantly lower hemoglobin levels, which was a major risk factor for develoing anemia.
The strong association between anemia and Alzheimer’s emerged as the explanation for the treatment resistant anemia, even when controlling all other available explanations for anemia.
This data indicates that Alzheimer is complicated by anemia, which may itself contribute to cognitive decline. The hope is to improve the quality of life for people with Alzheimer’s by finding an effective treatment for the blood disorder to improve cognitive decline.
Australian research shows link between anemia and Alzheimer’s disease
This year, National Palliative Care Week (May 25th to 31st) celebrated the people who work in palliative care and the important role they play in ensuring quality care at the end of life for all.
The theme of the week was ‘Palliative Care is everyone’s business: Lets work together’. After all palliative care IS everyone’s business. To ensure that we all have quality care at the end of life and are able to live and die well we all need to take responsibility for making this happen.
The key messages Palliative Care Australia want all Australians to be aware of are:
• This National Palliative Care Week we’re celebrating the people who work in palliative care and the quality care they provide to people with a life limiting illness, their families
and carers. These people – the nurses, GP’s, specialists, allied health professionals, volunteers and family carers are our unsung heroes supporting Australians through one the most difficult moments in their lives with respect, dignity and care.
• Let’s work together to ensure everyone who needs it receives the best possible palliative care. Everyone has a role to play and we’re asking people to think about what that might be.
• Death is a normal part of life. Like the birth of a child or a hospital emergency, palliative care services are a vital part of Australia’s health system.
• We encourage everyone to think about the care we would want
to receive towards the end of life and to have conversations with those closest to us about these preferences. Decisions such as where we would like to be, the type of care we want, who we would like to see and who can make decisions on our behalf if we’re unable to do so.
• Palliative care is everyone’s business. No matter whether you’re a partner, a parent, a child, a friend, a loved one, or a health professional National Palliative Care Week is a chance to start a conversation on how we would like to spend the end of our lives.
• After all you only die once so you might as well have your say in it.
National Palliative Care Week 2014
Source: http://www.palliativecare.org.
1. Jeremy, why did you decide to direct your product development efforts towards a savoury FMR? The nutrition market is crowded with sweet, generally dairy-based products. Our recently launched FMR Smooth Beef & Red Wine Casserole offers a savoury alternative to the sweet monotony, while providing the nutrients equivalent to one complete meal (850kJ energy, 12g protein, 26 vitamins & minerals) in an innovative 120g serving size. Whilst providing an extremely nutrient dense offering, we haven’t compromised on flavour and use hearty ingredients including beef, vegetables (tomato, carrot, peas and mushrooms), and red wine as the base. This product is Texture C suitable; is very versatile and can be used in a number of serving applications in addition to being a meal on its own e.g. soup, gravy, toast or shepherd’s pie.
2. Is this product also suitable for people with intolerances? (gluten, milk protein/lactose, nuts)FMR Smooth Beef & Red Wine Casserole is free from all major allergens e.g. gluten, nut, lactose, soy.
3. Do you have other FMR products in your range that are lactose free?Several, including our new FMR Apple Berry and the FMR Smooth Fruits which is available in three flavours - Banana & Mango, Pineapple & Coconut and Plum & Apple. Our staple FMR Iced Coffee and FMR Chocolate flavours are also extremely low in lactose (<0.1g).
4. The new casserole comes off the back of the new FMR Apple Berry which was launched in April this year, and the Bite Size Cookies launched in October last year. Can you tell us a bit about these other products you released recently, and how did you come to identify the needs for these innovations?By maximising nutrition per gram, we focus on improving consumer compliance, and ultimately by increasing nutritional density, we are aiming to ensure that the consumer is benefiting from every mouthful consumed.
We also believe in removing the barriers that prevent our clients from enjoying the everyday food and drinks they love. These philosophies, and the feedback received from our close ties with both speech pathologists and dietitians guided our new product development and resulted in the release of several innovative nutritional products in the past year. This includes the release of our FMR Bite Size Cookies, which are available in four sweet and savoury variants: Triple Chocolate, Vanilla Shortbread, Date & Coconut and Three Cheese, along with FMR Apple Berry. The Bite Size Cookies are our most nutritionally dense product to date offering an amazing 4kcal per gram of energy, 12g of protein and 26 vitamins and minerals, all packed into a tiny 50g serve. This product is perfect served as a mid-meal snack at morning or afternoon tea and can also be snacked on throughout the course of the day, to add to the overall nutrition intake. FMR Apple Berry is being well received as a refreshing, great tasting alternative to chocolate and vanilla supplement offerings.
Flavour Creations is committed to creating innovative and nutritional product solutions to assist in the dietary management of dysphagia and malnutrition. This is achieved through an extensive range of ready-to-eat hydration and nutritional supplements designed to support a healthy lifestyle and improve the quality of life of their clients.
Established in 1997, the Brisbane-based company has a long and successful history of developing ‘real food’ solution products that are tasty and nutritionally balanced. Its latest innovation, FMR Smooth Beef & Red Wine Casserole - a complete ready-to-eat meal in a compact 120g serving size has solidified Flavour Creations’ scientific and technological expertise in developing nutritional products that assist in managing a wide variety of health and nutrition challenges.
Flavour Creations’ Head of Research and Development Jeremy Betros is talking with us about their new FMRs.
NEW Smooth Beef & Red Wine Casserole from
Jeremy Betros talks about Flavour Creations NEW FMR savoury solution
Another innovative ‘real food’ solution from Flavour Creations
All queries regarding this tool kit should be addressed to Palliative Care Australia on 02 6232 4433 or by email on [email protected]
Welcome
Palliative Care Australia (PCA) represents the interests and aspirations of all Australians who share the ideal of quality care at the end of life.
Each year, we dedicate a week to raise awareness about palliative care and to spark interest and conversation about palliative care and end of life issues.
In 2014, we would love your support to help raise awareness about how we can all work together to make palliative care everyone’s business.
In this tool kit
The tool kit is intended to provide individuals and organisations with access to materials that can be used when planning and conducting events and activities to support National Palliative Care Week.
In it you will find:
• 2014 National Palliative Care Week theme and key messages • Communication materials you can access • Ideas for holding an event • Tips on engaging your own audiences through traditional and online media • A template media release.
National Palliative Care Week Theme
The theme for National Palliative Care Week 2014 is Palliative care is everyone's business: Let's work together. This year, we're celebrating the people who work in palliative care and the important role they play in ensuring quality care at the end of life for all. Palliative care is an issue that will affect all of us at some point in our lives, whether as a patient, carer, family member, neighbour or friend. We want to educate the community about palliative care and encourage people to think about what their own role may be.
After all, palliative care is everyone’s business. To ensure that we all have quality care at the end of life, and are able to live and die well, we all need to take responsibility for making this happen.
National Palliative Care Week 25- 31 May 2014 COMMUNICATIONS TOOL KIT

8 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 9
CARELINES ISSUE #7
The 2013 survey helped identify attitudes on people aged 50 years and over on how they live and want to be cared for in their last years.
In 2013 COTA (Council of the Ageing) NSW conducted a survey of 1800 people aged 50 years and over with the aim to collect valuable information on their attitude towards some of the main issues important to older people, including how they would like to live and be cared for during their last years.
In NSW it was found that 43% of all adults are now aged 50 years and over and nearly 33% of the total Australian population is comprised of people aged 50 years and over. For this reason it
is very important to understand their needs and to take them into account in the development of future policies and services.
The survey contains 11 sections exploring the current situation of the respondents in terms of employment status, living arrangements, source of income, health and wellbeing, age discrimination (in the workplace or when purchasing products or
services), experience with their GP appointments and hospital care as well as end of life care.
With regards to end of life decisions the survey respondents wanted more control over their end of life period. Nearly 75% of them said they could envisage circumstances where they would contemplate ‘being helped to die’.
This is probably also linked to their perception of current palliative care services; a quarter of the respondents knew someone receiving palliative care and did not feel that it provided enough comfort towards the end of the person’s life.
COTA NSW Survey on Over 50’s
Source: cotansw.com.au
A g e d C a r eC o n s u m a b l e s C a t a l o g u e
E B O S H e a l t h c a r e a r e p r o u d d i s t r i b u t o r s o f t h e f o l l o w i n g b r a n d s :
Have you got a copy of the latest EBOS Aged Care
Consumables Catalogue? Either
call your Key Account Manager or email
[email protected] to receive your copy!
Solving the supply chain
puzzle
Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email Manager or email call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account call your Key Account
Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either Catalogue? Either
to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your [email protected] [email protected] [email protected] to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your [email protected] [email protected] [email protected] to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your [email protected] [email protected] to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your [email protected] [email protected] [email protected] to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your [email protected] [email protected] to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your copy!to receive your [email protected] [email protected] [email protected] to receive your copy!to receive your copy!to receive your copy!to receive your [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected]
Manager or email Manager or email Manager or email [email protected] [email protected]
Manager or email Manager or email [email protected] [email protected] [email protected] [email protected]
Manager or email Manager or email Manager or email [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected]
Manager or email Manager or email Manager or email [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected] [email protected]
Manager or email Manager or email Manager or email [email protected] [email protected]
Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables Consumables EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care EBOS Aged Care copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest copy of the latest
Did you hear about the Final Report from the Australian Government’s Better Oral Health in Residential Aged Care Project?Have you implemented the train the trainer program in your facility?Does your facility have Champion of Oral Care?If you answered no to any of these questions, please keep reading.
In 2009 the Australian Government’s Department of Health and Ageing, under the Encouraging Best Practice in Residential Aged Care Program rolled out The Better Oral Health in Residential Aged Care Program in to Residential Aged Care Facilities across Australia. Each facility was invited to send up to 2 staff members (preferably RN’s) to attend a day of Oral Health training, these staff members returned to their workplace and delivered the training to the remaining staff.
After the program was completed, a report was written regarding the outcomes. The following information was published.
Let’s recap on the main points:
“Key Messages1
A healthy mouth will improve overall health and well being. Six of the Best Ways to maintain a healthy mouth for residents:
1. Brush Morning & Night2. High Fluoride toothpaste on teeth3. Soft toothbrush on gums, tongue & teeth4. Antibacterial Product after Lunch5. Keep the mouth moist6. Cut down on sugar
It takes a team approach to maintain a healthy mouth, with general practitioners, registered nurses, care workers and dental professionals taking responsibility for one or more of the four key processes:
1. Oral Health Assessment2. Oral Health Care Planning3. Daily Oral Hygiene4. Dental Treatment
Key Findings
Oral Health Assessment by non dental professionals does not replace dental examination but can be successfully used by general practitioners (GP’s) and registered nurses (RN’s) to identify residents requiring dental referral.
RN’s can successfully use the oral health assessment tool to inform oral care planning, monitor residents’ oral health and evaluate oral hygiene interventions.
Dentists and other dental professionals can be encouraged to visit residential aged care facilities to deliver dental care if they are supported and have access to portable equipment.
Residents’ oral health status improves rapidly with the implementation of the Better Oral Health in Residential Care Model.
Nursing Care can make a significant difference to all residents’ oral health and improve their quality of life. It is not only about dental treatment, it is about the difference daily oral hygiene activities can make.
A simple toothbrush that can be bent easily is the most economic and effective tool for improving oral health.
The Better Oral Health in Residential Care education and training program can be delivered successfully by non dental health professionals.
An aged care facilities RN is best placed to become the oral health champion and deliver the training to the other staff, following the train the trainer model. 1”
Another pearl of wisdom to emerge from this program is the Seasonal Toothbrush. Replace your resident’s toothbrush with a new colour at the beginning of each new season.
To find out more, the full Better Oral Health in Residential Care Portfolio is still available for download from http://www.health.gov.au/internet/main/publishing.nsf/Content/ageing-better-oral-health.htm
Better Oral Health in Residential Aged Care: The final report
Reference: 1. Anne Fricker & Adrienne Lewis – Better Oral Health in Residential Care Final Report Dec 2009
Small head soft bendable toothbrush range
Mouthwash range
Hamilton dry mouth range
Oraswab mouth swab with sodium bicarbonate
For more information on any product featured please contact customer service on 1800 269 534
www.eboshealthcare.com.au 11
CARELINES ISSUE #
10 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
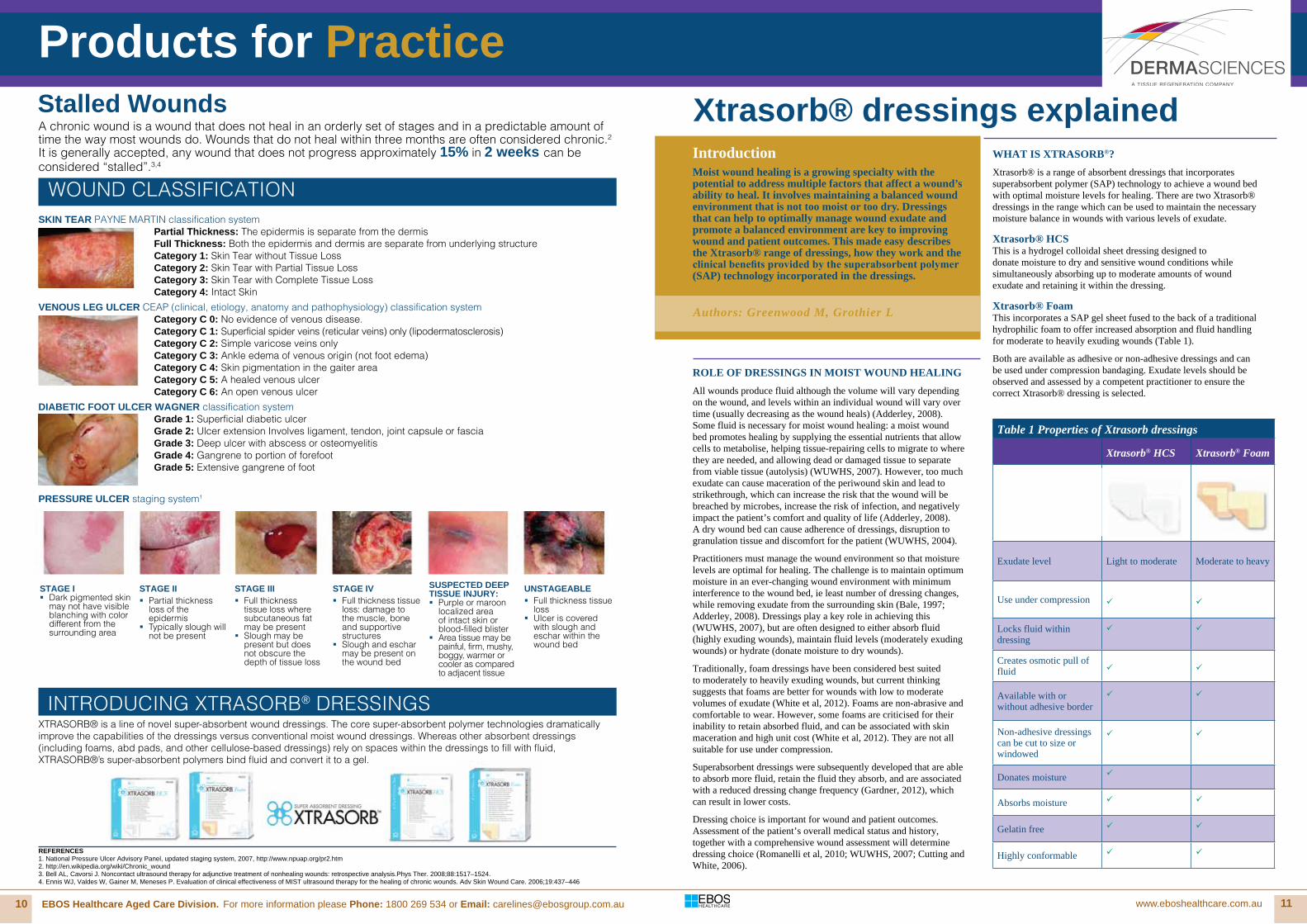
IntroductionMoist wound healing is a growing specialty with the potential to address multiple factors that affect a wound’s ability to heal. It involves maintaining a balanced wound environment that is not too moist or too dry. Dressings that can help to optimally manage wound exudate and promote a balanced environment are key to improving wound and patient outcomes. This made easy describes the Xtrasorb® range of dressings, how they work and the clinical benefits provided by the superabsorbent polymer (SAP) technology incorporated in the dressings.
ROLE OF DRESSINGS IN MOIST WOUND HEALINGAll wounds produce fluid although the volume will vary depending on the wound, and levels within an individual wound will vary over time (usually decreasing as the wound heals) (Adderley, 2008). Some fluid is necessary for moist wound healing: a moist wound bed promotes healing by supplying the essential nutrients that allow cells to metabolise, helping tissue-repairing cells to migrate to where they are needed, and allowing dead or damaged tissue to separate from viable tissue (autolysis) (WUWHS, 2007). However, too much exudate can cause maceration of the periwound skin and lead to strikethrough, which can increase the risk that the wound will be breached by microbes, increase the risk of infection, and negatively impact the patient’s comfort and quality of life (Adderley, 2008). A dry wound bed can cause adherence of dressings, disruption to granulation tissue and discomfort for the patient (WUWHS, 2004).
Practitioners must manage the wound environment so that moisture levels are optimal for healing. The challenge is to maintain optimum moisture in an ever-changing wound environment with minimum interference to the wound bed, ie least number of dressing changes, while removing exudate from the surrounding skin (Bale, 1997; Adderley, 2008). Dressings play a key role in achieving this (WUWHS, 2007), but are often designed to either absorb fluid (highly exuding wounds), maintain fluid levels (moderately exuding wounds) or hydrate (donate moisture to dry wounds).
Traditionally, foam dressings have been considered best suited to moderately to heavily exuding wounds, but current thinking suggests that foams are better for wounds with low to moderate volumes of exudate (White et al, 2012). Foams are non-abrasive and comfortable to wear. However, some foams are criticised for their inability to retain absorbed fluid, and can be associated with skin maceration and high unit cost (White et al, 2012). They are not all suitable for use under compression.
Superabsorbent dressings were subsequently developed that are able to absorb more fluid, retain the fluid they absorb, and are associated with a reduced dressing change frequency (Gardner, 2012), which can result in lower costs.
Dressing choice is important for wound and patient outcomes. Assessment of the patient’s overall medical status and history, together with a comprehensive wound assessment will determine dressing choice (Romanelli et al, 2010; WUWHS, 2007; Cutting and White, 2006).
WHAT IS XTRASORB®?Xtrasorb® is a range of absorbent dressings that incorporates superabsorbent polymer (SAP) technology to achieve a wound bed with optimal moisture levels for healing. There are two Xtrasorb® dressings in the range which can be used to maintain the necessary moisture balance in wounds with various levels of exudate.
Xtrasorb® HCSThis is a hydrogel colloidal sheet dressing designed to donate moisture to dry and sensitive wound conditions while simultaneously absorbing up to moderate amounts of wound exudate and retaining it within the dressing.
Xtrasorb® FoamThis incorporates a SAP gel sheet fused to the back of a traditional hydrophilic foam to offer increased absorption and fluid handling for moderate to heavily exuding wounds (Table 1).
Both are available as adhesive or non-adhesive dressings and can be used under compression bandaging. Exudate levels should be observed and assessed by a competent practitioner to ensure the correct Xtrasorb® dressing is selected.
Table 1 Properties of Xtrasorb dressings
Xtrasorb® HCS Xtrasorb® Foam
Exudate level Light to moderate Moderate to heavy
Use under compression
Locks fluid within dressing
Creates osmotic pull of fluid
Available with or without adhesive border
Non-adhesive dressings can be cut to size or windowed
Donates moisture
Absorbs moisture
Gelatin free
Highly conformable
Authors: Greenwood M, Grothier L
A chronic wound is a wound that does not heal in an orderly set of stages and in a predictable amount of time the way most wounds do. Wounds that do not heal within three months are often considered chronic.2
It is generally accepted, any wound that does not progress approximately 15% in 2 weeks can be considered “stalled”.3,4
REFERENCES1. National Pressure Ulcer Advisory Panel, updated staging system, 2007, http://www.npuap.org/pr2.htm2. http://en.wikipedia.org/wiki/Chronic_wound3. Bell AL, Cavorsi J. Noncontact ultrasound therapy for adjunctive treatment of nonhealing wounds: retrospective analysis.Phys Ther. 2008;88:1517–1524.4. Ennis WJ, Valdes W, Gainer M, Meneses P. Evaluation of clinical effectiveness of MIST ultrasound therapy for the healing of chronic wounds. Adv Skin Wound Care. 2006;19:437–446
SKIN TEAR PAYNE MARTIN classification system Partial Thickness: The epidermis is separate from the dermis Full Thickness: Both the epidermis and dermis are separate from underlying structure Category 1: Skin Tear without Tissue LossCategory 2: Skin Tear with Partial Tissue LossCategory 3: Skin Tear with Complete Tissue LossCategory 4: Intact Skin
VENOUS LEG ULCER CEAP (clinical, etiology, anatomy and pathophysiology) classification system Category C 0: No evidence of venous disease. Category C 1: Superficial spider veins (reticular veins) only (lipodermatosclerosis) Category C 2: Simple varicose veins only Category C 3: Ankle edema of venous origin (not foot edema)Category C 4: Skin pigmentation in the gaiter area Category C 5: A healed venous ulcer Category C 6: An open venous ulcer
DIABETIC FOOT ULCER WAGNER classification system Grade 1: Superficial diabetic ulcer Grade 2: Ulcer extension Involves ligament, tendon, joint capsule or fascia Grade 3: Deep ulcer with abscess or osteomyelitis Grade 4: Gangrene to portion of forefootGrade 5: Extensive gangrene of foot
STAGE I � Dark pigmented skin
may not have visible blanching with color different from the surrounding area
STAGE II � Partial thickness
loss of the epidermis
� Typically slough will not be present
STAGE III � Full thickness
tissue loss where subcutaneous fat may be present
� Slough may be present but does not obscure the depth of tissue loss
STAGE IV � Full thickness tissue
loss: damage to the muscle, bone and supportive structures
� Slough and eschar may be present on the wound bed
SUSPECTED DEEP TISSUE INJURY: � Purple or maroon
localized area of intact skin or blood-filled blister
� Area tissue may be painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue
UNSTAGEABLE � Full thickness tissue
loss � Ulcer is covered
with slough and eschar within the wound bed
WOUND CLASSIFICATION
PRESSURE ULCER staging system1
Xtrasorb® dressings explained
XTRASORB® is a line of novel super-absorbent wound dressings. The core super-absorbent polymer technologies dramatically improve the capabilities of the dressings versus conventional moist wound dressings. Whereas other absorbent dressings (including foams, abd pads, and other cellulose-based dressings) rely on spaces within the dressings to fill with fluid, XTRASORB®’s super-absorbent polymers bind fluid and convert it to a gel.
Stalled Wounds
Products for Practice
INTRODUCING XTRASORB® DRESSINGS

12 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 13
WHAT IS POLYMER TECHNOLOGY? Superabsorbent polymers are compounds that can absorb and retain large volumes of liquid relevant to their mass.
Polymers are classified as non-ionic, without electrical charge (eg polyurethane foam dressings), or ionic polymers, with electrical charge.
Non-ionic polymer chains are linked closely together or coiled and do not have much capacity for absorbing fluid. Dressings containing non-ionic polymers, such as polyurethane foams, are used for wounds with low volumes of exudate (White et al, 2012).
Ionic polymers have negatively charged side arms that repel the linking polymer chains away from each other (Figure 1). The repelling ions cause the ionic polymers to stay spread apart, thus creating more space in the polymer chain and allowing for extremely high absorption rates (Pytlik et al, 2005).
Dressings containing ionic polymers with increased absorption capacity, such as calcium alginate dressings, are suited to use in wounds with moderate to high levels of exudate (Walker and Parsons, 2010). However, these dressings can sometimes lose structural integrity and disintegrate due to the large volumes of liquid absorbed.
Figure 1: An illustration of the structure and form of polymers and their absorbtion capabilities
XTRASORB® AND SAP TECHNOLOGY
Benefits of superabsorbent polymersSuperabsorbent polymers provide considerable benefits in wound dressings through their:• very high absorptive capacity• gel-forming action that retains absorbed fluid within the
structure of the polymer• ability to create an osmotic gradient• ability to sequester and retain potentially harmful exudate
components (Vachon and Yager, 2006; Wiegand et al, 2011)• protease modulating activity resulting from modification of the
wound environment (Tarlton and Munro, 2013).
Xtrasorb® dressings contain cross-linked ionic SAPs that enable them to have enhanced absorptive capabilities and remain intact despite the high volume of fluid uptake (Wiegand et al, 2011). This is in contrast to, for example, alginates, which are ionic polymers but are not cross-linked polymers.
As fluid is absorbed into the material, a gel is formed locking within the dressing the fluid, which contains bacteria, matrix
metalloproteinases (MMPs) and other enzymes (Vachon and Yager, 2006; Wiegand et al, 2011). In chronic wounds, healing may be disrupted by a number of factors including excessive levels of enzymes, such as MMPs (Liu et al, 2009), and/or high levels of bacteria. In this way, the superabsorbent polymer may improve the chronic wound environment by reducing the impediments to healing (Tarlton and Munro, 2013).
Additionally, in vitro studies of Xtrasorb® HCS and Xtrasorb® Foam have shown that the Xtrasorb® polymer sheet technology helps to reduce MMP activity through two mechanisms: by direct absorption of the proteases and by reducing co-factors essential for their function, such as metal ions (Tarlton and Munro, 2013).
WHAT IS XTRASORB® HCS?Xtrasorb® HCS is composed of 45% SAP, 50% hydrogel (a glycerin/water mix) and 5% sodium carboxymethylcellulose (a hydrocolloid component).
It is a versatile dressing designed to help manage varying wound conditions by donating moisture to a dry wound environment while optimally handling the fluid associated with light to moderately exuding wounds.
How does it work?Xtrasorb® HCS is able to absorb up to four times more liquid than other hydrocolloid dressings by taking fluid up vertically into the dressing and preventing sideways or lateral spread of fluid onto the periwound area (data on file). This helps prepare the wound bed by removing excess moisture while devitalised tissue is removed by autolysis, decreasing the risk of periwound maceration (Welber et al, 2012).
This is sometimes a consequence of using hydrogels under compression (see Case Report 1).
Xtrasorb® HCS has a cooling and soothing effect (see Case Report 1) on dry and sensitive skin conditions and on the wound bed. The dressing provides an atraumatic wound contact layer that is highly conformable and non-adherent to wound tissue (see Case Report 1).
In addition, Xtrasorb® HCS is transparent, allowing clinicians to view the wound and identify early signs of infection or cues that the dressing needs changing earlier than planned.
When is Xtrasorb® HCS indicated?Xtrasorb® HCS is indicated for light to moderately exuding wounds including:• pressure ulcers• venous leg ulcers• arterial ulcers• diabetic foot ulcers• postoperative wounds• traumatic wounds• first and second degree burns• donor sites
Contraindications and precautionsXtrasorb® HCS should not be used on heavily bleeding wounds or third degree burns, or in patients with known hypersensitivity to the product itself or to any of its components (including glycerin or sodium carboxymethylcellulose).
How to apply Xtrasorb® HCS• Cleanse the wound and surrounding area according to local
protocol, and ensure the surrounding skin is dry.• Select a dressing of a size that will allow the dressing pad to
completely cover the wound and extend onto healthy skin by approximately 10–15mm.
• Remove a corner of the white plastic liner to expose the tacky portion of the dressing.
• Position the dressing and smooth into place while removing the second portion of the white plastic liner.
• When using the non-adhesive non-bordered version of Xtrasorb® HCS, secure in place with tape or a secondary dressing, eg a conforming bandage.
• When using the adhesive bordered version of Xtrasorb® HCS, peel away the top liner from the dressing once the dressing is in place.
WHAT IS XTRASORB® FOAM?
Xtrasorb® Foam consists of a SAP gel sheet fused to the back of a polyurethane foam wound contact layer for use in moderately to highly exuding wounds. Because of its polymer technology, is able to absorb approximately two to four times more fluid than other foam dressings. It is suitable for use under compression therapy as it absorbs and retains fluid under pressure (data on file).
How does it work?Exudate is absorbed into the polyurethane foam layer and pulled up into the SAP sheet. When the fluid comes into contact with the SAP layer it is drawn by osmosis into the gel sheet where it converts to a gel (Figure 2). The gel holds the exudate and its harmful components securely away from the wound surface and surrounding skin.
When is Xtrasorb® Foam indicated?Xtrasorb® Foam is indicated for moderate to heavily exuding wounds, including:• diabetic foot ulcers• leg ulcers – including venous leg ulcers, arterial ulcers and
ulcers of mixed aetiology• pressure ulcers• first and second degree partial thickness burns• postoperative wounds
• donor sites• traumatic wounds.Figure 2: Structure of Xtrasorb® Foam and mechanism of action
Two to four times more absorption than standard foam dressings• Locks wound fluid away from the wound and surrounding skin• Fewer dressing changes• SAP layer provides additional cushioning and pressure
redistribution
Contraindications and precautionsXtrasorb® Foam should not be used on heavily bleeding wounds or third degree burns, and not with oxidisingagents such as Dakin’s (hypochlorite solution) or hydrogen peroxide. However, it can be used with honey dressings that produce hydrogen peroxide ions (Welber et al, 2012).
A tightly coiled non-ionicpolymer. Eg:• polyurethane foam
Xtrasorb® Foam pulls fluid to the back of the dressing and converts it to a gel, retaining it in a controlled area
Case report 1: Application of Xtrasorb® HCS to a leg ulcer in conjunction with hosiery
Background An 82-year-old gentleman with a four-year history of multiple episodes of leg ulceration and episodes of varicose eczema presented to the tissue viability clinic with a re-ulceration to the left medial malleolus. He had a history of varicose eczema. The open wound, which measured 0.5cm x 0.5cm, was dehydrated and the majority of the wound was covered with superficial devitalised tissue. There was a low level of exudate. The condition of the surrounding skin was poor. Previous treatments had been unsuccessful at removing the hard devitalised tissue and the varicose eczema had caused irritation to the surrounding skin.
Treatment Xtrasorb® HCS was used to rehydrate the tissue. The dressing was changed twice weekly. Inelastic cohesive bandaging was applied and a course of steroid ointment was prescribed for the skin irritation. After 11 days of treatment the dehydrated tissue had reduced significantly and a simple non-adherent dressing was applied. The wound and surrounding skin responded well to Xtrasorb® HCS. At week 11, as the wound was considered well-managed and care could be provided in part by a practice nurse, the patient progressed on to a made-to-measure 40mmHg hosiery kit.
Outcome The wound went on to heal completely within nine weeks of assessment. Tissue viability staff reported that Xtrasorb® HCS was easy to apply and remove, did not adhere to the skin and was conformable to the patient’s limb. The patient reported that he found it extremely comfortable and that the dressing had had a ‘soothing effect’ throughout wearing it. Overall, the dressing was evaluated as a cost-effective clinical solution for autolytically debriding devitalised tissue and preparing the wound bed for healing.
Figure 1: The wound at presentation showing devitalised tissue
Figure 2: The dressing in place enables the wound to be clearly monitored
Figure 3: The wound has reduced in size and the condition of the periwound skin has improved
An ionic polymer expands becausethe negatively charged side armsrepel each other. Eg:
• High absorption - carboxymethylcellulose and calcium alginate
• Very high absorption - polyacrylates
Products for Practice
Xtrasorb® Foam pulls fluid to the back Xtrasorb® Foam pulls fluid to the back of the dressing and converts it to a gel, retaining it in a controlled area

14 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 15
How to apply Xtrasorb® Foam• Cleanse the wound and surrounding area according to local
protocols. As with other polyurethane foam dressings, oxidising solutions should be avoided.
• Select a dressing that will overlap onto healthy tissue by approximately 25mm.
• A secondary film dressing or conforming bandage should be used to secure the dressing in place.
• Before applying the adhesive dressing, remove one half of the white plastic liner to expose the adhesive border. Position the dressing and smooth it into place while removing the second half of the liner. Ensure good contact between the adhesive border and periwound skin by smoothing the edge of the dressing.
• Once the dressing is in place, remove the backing material from the slit in the centre of the top of the dressing.
FREQUENCY OF DRESSING CHANGESThe frequency of dressing change should be guided by the condition of the wound, the patient and the level of exudate. Dressings containing large volumes of fluid can become bulky and cause discomfort to the patient.
As a guide, Xtrasorb® HCS should be replaced after three to seven days. In the case of a moderately exuding wound the dressing may need to be replaced more frequently.
When should Xtrasorb® be discontinued?The dressing can be discontinued once the wound has reached full closure (healed) and/or the key objective for the dressing choice has been achieved, in line with the wound management goals.
Removing Xtrasorb® HCS and FoamNon-adhesive borderless Xtrasorb® dressings Gently lift the corners of the dressing and remove from the wound.
Adhesive bordered Xtrasorb® dressings Loosen the adhesive film border before lifting the dressing away from the wound. Saline or water may be used to irrigate the Xtrasorb® dressings if necessary.
CLINICAL BENEFITS OF XTRASORB® DRESSINGS
Both Xtrasorb® HCS and Xtrasorb® Foam can be used to aid healing in a wide range of wound types. The SAP technology incorporated into the dressing allows for optimal fluid handling and the sequestration of bacteria and harmful components found within wound fluid, helping to keep the wound clear (Wiegand et al, 2011; Turkos and Stallo, 2008). Both dressings incorporate SAP technology that helps to overcome some of the issues faced by patients and clinicians when using other dressings. They can be used as primary or secondary dressings. By converting fluid into a gel Xtrasorb® offers a number of distinct advantages.
Fewer dressing changesXtrasorb® dressings can be left in place for up to seven days depending on the wound exudate levels. The high absorbency of the dressings allows for dressing changes to be less frequent, which offers the potential to reduce overall wound management costs (Stille, 2012; Peters et al, 2007).
Reduced risk of strikethroughThe SAP mechanism of gel formation holds absorbed liquid within the dressing reducing the risk of strikethrough. Because fluid does not need to evaporate from Xtrasorb® dressings like it does in dressings that rely on moisture vapour transmission rate (MVTR) (Peters et al, 2007), a film layer covers the back of the dressings rendering them water resistant. Strip washing is preferred to showering.
Reduced risk of macerationThe high absorbency of the dressings and gel formation, along with lack of lateral wicking (Turkos and Stallo, 2008; Peters, 2007) mean that wound exudate is absorbed into and retained within the dressings. This prevents potentially damaging exudate from coming into contact with periwound skin. A case series examining the use of Xtrasorb® HCS in lower extremity wounds reported a reduction or elimination of maceration in all cases (Welber et al, 2012).
Use under compressionThe gelling action of the SAP in the Xtrasorb® dressings prevents
Case report 2: Application of Xtrasorb® Foam to a skin tear that had failed to progress
Background An 83-year-old male was admitted to hospital after falling down a step at home. He had extremely fragile, tissue-paper skin and had sustained a skin tear on his right forearm near the elbow during the fall. He was admitted to hospital with a fractured pelvis, signs of heart failure and some consolidation to the left lung. Oral antibiotics were commenced. The patient became unwell on the ward and pseudo-obstruction of the bowel was diagnosed. He had a history of diabetes, hypertension, heart disease and chronic obstructive pulmonary disease. The patient was also partially blind, had diverticular disease and prostatic hypertrophy. He was referred to tissue viability because the wound had not improved since admission. The wound measured 8cm x 2.5cm and had moderate levels of haemoserous exudate. Bruising to the surrounding skin was evident. The patient experienced high levels of pain during dressing changes. He described the previous dressing used as ‘uncomfortable to wear’ and difficult to remove from his fragile skin.
Treatment Xtrasorb® Foam adhesive was applied to absorb exudate, prevent maceration and encourage healing. The dressing was changed after two days and then every third day, following reassessment of the wound and exudate levels.
Outcome The wound epithelialised without complications within two weeks, despite the patient’s comorbidities. The tissue viability nurse found the dressing to be conformable and easy to apply. The dressing prevented strikethough and the patient found the dressing extremely comfortable to wear and ‘not too difficult to remove’.
Figure 1: Skin tear on outer elbow, day 1
Figure 2: The wound progressed to healing, day 13
Case report 3: Application of Xtrasorb® Foam to a heavily exuding pressure ulcer
Background A 53-year-old female with a venous leg ulcer and multiple comorbidities, including morbid obesity and chronic venous insufficiency, was being treated in the community. The wound was dressed with thick gauze and absorbent cotton/cellulose pads, and compression therapy was applied. Large amounts of exudate had led to strikethrough, maceration of periwound tissue and excoriation of the surrounding skin. The dressing had required changing daily.Treatment Xtrasorb® Foam adhesive was applied to absorb exudate, prevent maceration and encourage healing. The dressing was changed after two days and then every third day, following reassessment of the wound and exudate levels.
Treatment It was decided to dress the wound with Xtrasorb® Foam, to manage the volume of exudate more effectively. Compression therapy was also continued.
Outcome Dressing changes were reduced from daily to three times a week after 13 days. Strikethrough was eliminated and the dressing held exudate under compression therapy. The patient’s self-image and mobility increased. The maceration and skin excoriation resolved and the wound’s surface area decreased by 52% in 34 days.
Figure 1: Wound on presentation
Figure 2: Wound 34 days later
absorbed fluid from being squeezed out of the dressing when pressure is applied, which may be a benefit over conventional foam dressings that are unable to lock fluid within them under compression. The dressings are therefore suitable for use under compression bandaging or hosiery (Welber et al, 2012).
Additional clinical benefitsXtrasorb® HCS and Xtrasorb® Foam both have high tensile strength which allows the non-adhesive dressings to be cut to size (Stille, 2012) or windows cut into them, and for the dressings to maintain their integrity even when at their full absorptive capacity.
In addition, Xtrasorb® HCS is gelatin free and does not produce the characteristic odour associated with some dressings such as hydrocolloids. It provides a useful alternative for patients who prefer products that do not contain gelatin.
Xtrasorb® HCS and Xtrasorb® Foam have been designed to help clinicians manage the varying levels of moisture present in chronic and healing wounds. The SAP technology incorporated by the dressings enables them to absorb and retain greater levels of fluid without losing structural integrity. Xtrasorb® HCS is able to donate moisture to wounds and maintain optimal fluid levels at the wound bed. Key benefits include protease modulation, reduced incidence of skin maceration and strikethrough, less frequent dressing changes and the ability to use both dressings under compression.
REFERENCES
Adderley U (2008) Wound exudate: what is it and how to manage it. Wounds Essentials 3: 8-13
Bale S (1997) In: A Colour Guide to the Nursing Management of Chronic Wounds (2nd edn). Eds: Morison M et al. Mosby, London
White R, Cutting K (2006) Modern exudate management: a review of wound treatments. http://www.worldwidewounds.com/2006/september/ White/Modern-Exudate-Mgt.html
Dowsett and Newton (2005) Wound bed preparation: TIME in practice. Wounds UK 1(3): 58-70. Available at: www.wounds-uk.com
Gardner S (2012) Managing high exudate wounds. Wounds Essentials 7(1). Available from: www.wounds-uk.com/pdf/content_10474.pdf
Liu Y, Min D, Bolton T, et al (2009) Increased matrix metalloproteinase-9 predicts predicts poor wound healing in diabetic foot ulcers. Diabetes Care 32(1): 117-19
Peters KL, Liguori PA, Bowers JM (2007) An evaluation of a new super- absorbent
foam dressing’s exudate management capabilities. Poster, Symposium on Advanced Wound Care (SAWC), Tampa, FL, USA
Pytlik E, Molino D, Moritz J (2005) Superabsorbent polymers. UB Engineering, University at Buffalo. Available at: http://www.eng.buffalo. edu/courses/ce435/Diapers.html
Romanelli M, Vowden K, Weir D (2010) Exudate Management Made Easy. Wounds International 1(2): Available from http://www. woundsinternational.com
Stille S (2012) A novel approach to the effective management of a non- healing peristomal wound. Poster, Symposium on Advanced Wound Care (SAWC), Atlanta, GA, USA
Tarlton JF, Munro HS (2013) Use of superabsorbent polymer dressings for protease modulation in improved chronic wound care. Wounds 25(2): 51-57
Turkos M, Stallo K (2011) Protease modification by absorbent polymer dressings. Poster presented at: Symposium on Advanced Wound Care (SAWC), Dallas, TX, USA
Turner TD (1979) Hospital usage of absorbent dressings. Pharmaceutical J 222: 421-26
Vachon DJ, Yager DR (2006) Novel sulfonated hydrogel composite with the ability to inhibit proteases and bacterial growth. J Biomed Mater Res A 76(1): 35-43
Walker M, Parsons D (2010) Hydrofibre® technology: its role in wound management. Wounds UK 6(2): 31–38
Welber A, Celestin C, Mehrdad F, et al (2012) The effectiveness of Leptospermum honey and a novel super-absorbent hydrogel-colloidal sheet in managing challenging lower extremity wounds: a case study series. Poster, Wound Ostomy and Continence Nurse (WOCN) Annual Conference, Charlotte, NC, USA
White R, Gardner S, Cutting K, et al (2012) What is the current status of foam dressings? WUK Debate. Wounds UK 8(3): 21-24. Available from: www.wounds-uk.com/pdf/content_10557.pdf
Wiegand C, Abel M, Ruth P, et al (2011) Superabsorbent polymer- containing wound dressings have a beneficial effect on wound healing by reducing PMN elastase concentration and inhibiting microbial growth. J Mater Sci Mater Med 22(11): 2583-90
World Union of Wound Healing Societies (WUWHS) (2007) Wound Exudate and the Role of Dressings, A Consensus Document. London, MEP Ltd. Available from: www.woundsinternational.com
World Union of Wound Healing Societies (WUWHS) (2004) Minimising Pain at Wound Dressing-related Procedures, a Consensus document. London, MEP Ltd. Available from: www.woundsinternational.com
AUTHOR DETAILS
Greenwood M1, Lorraine Grothier2
1. Lead Nurse Tissue Viability, Walsall Healthcare NHS Trust2. Clinical Nurse Specialist Tissue Viability, Central Essex Community Services
Summary
To support your educational needs, Derma Sciences continues to present online educational programs with topics relevent to your wound care management needs.Please visitwww.dermasciences.com.au for current webinars and clinical reviews available.
Products for Practice

16 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 17
CARELINES ISSUE #
COMING UP...
NIMAC Conference, 9-11 July, Gold Coast 2014The Nurses In Management Aged Care (NIMAC) Conference and Trade Exhibition 2014 brings together nurses working in the aged care industry. This annual event provides the opportunity for nurses to gather, network and visit the trade exhibition and speak with sponsors who provide relevant information products and services. The theme for this year’s Conference is ‘We come from the land down under’ The program for 2014 is informative and challenging. It will encourage delegates to develop new visions and strategies for the future. Our EBOS team will be at Booths 36 and 37 so come past and say hi!
ACSA National Conference, 7-10 September, Adelaide 2014 The 2014 Aged and Community Services Australia (ACSA) National Conference program in Adelaide is designed for us all to redefine the experience of ageing in our communities questioning everything about delivery of services and what else is possible. The sector has matured and is ready to work on a new image/pathway for aged care.
Leading Age Services Australia (LASA) National Congress, 20-22 October, Adelaide 2014At LASA Congress 2014 The theme ‘Breakthrough: Motivate Innovate Integrate’ aims to inspire individuals by those who have broken through, learned valuable lessons and trod before. Come ready to be part of the new wave in age services, where our industry develops and leads the conversation; joined by Older Australians in implementation of care and services without compromise. Our EBOS team will be at Booth 81 so come past and say hi!
Information Technology in Aged Care, 22-23 July, Hobart 2014The theme of the conference, Digital Revolution in Seniors Living - assistive technologies: disruptor or enhancer of services? emphasises the importance of information technology in establishing a sustainable, quality focused aged care environment. These critical aged care topics will be discussed from a practical perspective, highlighting the information we need to know how to better manage and design aged care service delivery.
The first few months of 2014 have truly seen our EBOS Aged Care team on their feet, busy networking with key clients on the changing needs of our industry. Don’t forget to look for our EBOS booth at this year’s key events.
Conference and Event News from EBOS
Elizabeth Conridge & Debbie Greenaway, National LASA 2013 Conference, Sydney.
Karen Amosa, Amelia Lea and Emma Belgre supporting Aged Care in Customer Service.
EBOS expands customer service to support local customers
Emma Belgre is our National Aged Care Support for National Account Manager Debbie Greenaway. Emma has been with the Aged Care Division for the past year and a half.
What do you like most about your role working in the Aged Care Industry?There is always so much to learn in Aged Care, getting to know about all the dedicated products and how the industry works really intrigues me. As I didn’t have a lot of industry experience before I started in this role everyday I learn something new, and am now starting to be able to pass this onto our Clients.
My Special Day – 25th October 2013. Last October I married my best friend Adam Belgre at the Novotel in Wollongong. We had a simple ceremony as we just wanted to celebrate with 120 of our closest family and friends.Adam and I have been together now for just over seven years. I was fifteen at the time and still in school when a friend ‘set-us up’. Three weeks after we had met we started ‘dating’; back then this only meant seeing one another once or twice a week (and being a teenager at the time I never thought anything serious would come out of it.)
Five years down the track Adam decided to propose to me on our anniversary- a romantic proposal in front of the restaurants in Darling Harbour! I burst out in tears of joy and Adam had to remind me in the end that I hadn’t really said yes.
Just shy of two years later I finally got to walk down the aisle and meet my now husband at the other end.
Three things of my wedding day I will remember forever:•When I saw Adam at the end of the aisle with tears in his eyes and a tissue in hand to wipe them away. Still to this day he insists that the sun was in his eyes!•Having both my father and step father walk me down the aisle.•The moment Adam and I were pronounced Husband and Wife. This was the happiest moment of my life.The most unusual thing that happened at my wedding. The groomsmen decided to play golf the day before the wedding. It was an overcast day so the boys obviously thought they didn’t have to wear sunscreen. At the wedding the next day all five of them were sunburnt, with the sunglasses tan on their faces and burnt necks. Adam’s brother (best man) was the worst and as he is bald, his head was extremely burnt. He had to keep a tissue on it as his skin had blistered and was weeping the entire day. Our photographer advised us to get some shots without him…If I could do it again, I would…. Put the entire day in slow motion. Everyone says the day goes fast but I never believed them until it was my turn. The day in my eyes was perfect and I would marry Adam again in a heart beat if I could (and didn’t have to pay for it again).
Karen Amosa and Amelia Lea are members of the EBOS Customer Service Team dedicated to our Aged Care Division. Together they support our Aged Care customers and provide a great knowledge of our products and aged care customers’ needs.
Alongside this amazing duo Emma Belgre works closely with Debbie Greenaway, our National Account Manager, providing her with daily support to meet the needs of national key clients. See more about Emma on your right.
Most of our busy Customer Service Team are based in our head office in Sydney, but as EBOS business continues to grow nationally we are focusing on providing more local support to our Clients.
We already have five warehouses in Australia– with Perth being the latest addition to our Sydney, Melbourne, Brisbane and Hobart locations.
We are now growing our Customer Service with more customer support staff based in our State offices in Brisbane, Tasmania and Melbourne- a testament to our growth and future support for the business as a whole.
The latest addition to our local Customer Service staff - Ellyne Winsall, has just joined the Victorian team and we are currently recruiting for our offices in Perth.
Karen, Emma and Amelia
JUST PAST..
Cultural Diversity in Ageing Conference: Shaping Inclusive Services, 12-13 June, Melbourne 2014The Conference provided a forum for service providers to gain insight and inspiration in their pursuit of excellence in meeting the needs of a culturally diverse society. This year’s conference theme ‘Shaping Inclusive Services’ showcased culturally inclusive measures and models designed to ensure quality outcomes for older Australians from culturally and linguistically diverse backgrounds.
International Dementia Conference - Risky business 2, 26 - 27 June, Sydney 2014This conference considered the opportunities and challenges confronting care for people with dementia. It addressed risk from everyone’s point of view; from the risks people with dementia choose to take in their lives, to the challenges of building and delivering services that provide choice and therapeutic benefits, to the legislative and policy context that simultaneously seeks to protect and deny certain freedoms.
CARELINES ISSUE #7

18 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 19
CARELINES ISSUE #
™Trademark of Smith & Nephew SN11438 (06/2014)
SECURA™ Cleanser and Extra Protective Cream Z30 Case Study Prevention of skin lesions in the sacral region in an incontinent patientIliana Pérez, Manuel Rodríguez, Jesús Vallejo, Mª del Mar Valverde, NursesResidencia de Mayores “José Matía Calvo” (Cádiz)Antonio Blanco del Valle. Nurse.Clinical department. Wound treatment section, Smith & Nephew, Spain
IntroductionIncontinence may lead to the development of skin lesions in the sacral region. If left untreated there is a high risk that these lesions may develop into pressure ulcers. This is because irritation caused by urine, faeces as well as mechanical damage that can be caused by using soap and water and rubbing the area dry may lead to a break down in skin integrity.
PatientA 92-year-old woman with mixed incontinence, using incontinence pads 24 hours a day. The patient was totally dependent on care staff for her personal hygiene.
TreatmentAt the start of treatment the sacral region showed signs of dermatitis and erythema. Following each incontinence episode the affected area was cleaned with SECURA Cleanser. SECURA Extra Protective Cream Z30 was also applied to help protect the skin. This was applied once a day.
ResultsWithin eleven days the condition of the skin improved with no signs of erythema or dermatitis, which were present at the start of treatment.As the treatment progressed the patient’s quality of life significantly improved as she experienced less discomfort due to skin irritation.
ConclusionsThis study shows that SECURA Cleanser and Extra Protective Cream Z30 were an effective way of helping to maintain skin integrity in an incontinent patient.
Start of treatment
End of treatment
Always read the label and use only as directed. If symptoms persist, consult your healthcare professional.
CARELINES ISSUE #6
™Trademark of Smith & Nephew SN11469 (06/14)
SECURA™ provides a simple 3-part process for good skin care management:
1. Cleanse 2. Protect 3. Moisturise
The SECURA™ difference.
Skin is our natural first line of defence against bacteria. Keeping skin intact is essential to reduce the human and economic cost of wounds. Broken skin causes discomfort and is often painful, reduces mobility and can affect how that individual feels about life – a significant human cost. Additionally, the associated economic costs for the individual and the medical facility treating them can be significant, especially if it develops into something more complex, such as an infection. By keeping skin intact through good skin care management, we can all assist in the reduction of the human and economic cost associated with further complications.
Healthy intact skin maintains a naturally acidic pH (4.5-5.5) providing an unfavourable environment for bacterial growth. Appropriate skin care helps avoid skin breakdown and infection and may reduce the incidence of skin tears, the development of pressure injuries from the effects of friction, and protection from the damaging effects of incontinence and wound exudate.
Age and altered mobility as well as nutritional status and altered consciousness also contribute to skin breakdown.
The Effects of Moisture on the SkinExcess moisture comes from perspiration (e.g. under breasts skin folds and tummy aprons), urine, faeces, wound exudate and saliva. Prolonged exposure on intact skin can alter the natural pH of the skin and affect the protective barrier, making it vulnerable to breakdown and infection and weakening its ability to withstand friction and shear.
Frequent washing of the skin can strip off its natural oils that keep it soft and hydrated, and denude its outer layer, the stratum corneum. This can result in incontinence
associated dermatitis (IAD) and possible infection. Areas most at risk are the perineum, the thighs and between the buttocks.
Skin HygieneThe main approach to protecting the skin and avoiding skin breakdown is appropriate washing and drying and the use of barrier treatments. This can be a three step approach of cleanse, protect and moisturise.
Why Cleanse?Washing with conventional soap and water may damage the skin by interfering with several of its protective mechanisms. Whilst this approach may be suitable for protecting the skin from occasional incontinence or faecal soiling, it exposes the skin to several potentially damaging factors. Soap is highly alkaline and continued use can disrupt the skin’s natural protective acidic conditions, and alter the delicate balance of the skin’s normal flora. Soap residue on the skin is common, even after rinsing. Scrubbing the skin is abrasive and can remove the stratum corneum. More effective alternatives to soaps are pH neutral cleansers such as the no-rinse SECURA◊ Cleanser which surfactants in the formula lift body waste away from the skin without harsh scrubbing.
Why Protect and Moisturise?Intact skin that is supple and moisturised is stronger and better able to resist skin breakdown and infection. Moisture barriers (e.g. creams and lotions) and films may help shield the skin from exposure to irritants such as urine, faeces and excess moisture, as they are designed to seal out wetness from unwanted moisture and may help prevent water loss and improve skin hydration. They can provide relief to irritated and sensitive skin. Zinc and dimethicone based barrier creams are thicker in texture
Skin care – Why is it so important to us all?and leave a protective barrier from incontinence episodes. SECURA◊ Barrier Cream D and Protective Cream Z10 help avoid skin problems associated with incontinence by sealing out wetness and reducing exposure to urine and faeces, while SECURA◊ Extra Protective Cream Z30 is a more durable and long lasting protectant, providing a high level of protection for patients with denuded skin.
Moisturising creams and lotions protect and reduce the effects of dry skin, a known risk factor for skin tears. Recent research carried out by the Wound Management Innovation CRC has shown that twice daily application of
a moisturiser can reduce the number of skin tears by 50% in older people1. SECURA◊ Moisturizing Cream and Lotion are gentle to sensitive skin, absorb quickly and help restore moisture to the skin.
Broken skin can be uncomfortable and painful. Keeping skin intact through good skin care management, can assist in the reduction of the human and economic cost associated with skin complications.Reference: 1. Wound Management Innovation CRC. Media Release. 2013. http://www.woundcrc.com/index.php?option=com_content&view=article&id=73%3Awound-crc-research-delivers-a-50-reduction-in-skin-tears&catid=7&Itemid=6 Accessed on 27 May 2014
™Trademark of Smith & Nephew SN11438 (06/2014)
SECURA™ Cleanser and Extra Protective Cream Z30 Case Study Prevention of skin lesions in the sacral region in an incontinent patientIliana Pérez, Manuel Rodríguez, Jesús Vallejo, Mª del Mar Valverde, NursesResidencia de Mayores “José Matía Calvo” (Cádiz)Antonio Blanco del Valle. Nurse.Clinical department. Wound treatment section, Smith & Nephew, Spain
IntroductionIncontinence may lead to the development of skin lesions in the sacral region. If left untreated there is a high risk that these lesions may develop into pressure ulcers. This is because irritation caused by urine, faeces as well as mechanical damage that can be caused by using soap and water and rubbing the area dry may lead to a break down in skin integrity.
PatientA 92-year-old woman with mixed incontinence, using incontinence pads 24 hours a day. The patient was totally dependent on care staff for her personal hygiene.
TreatmentAt the start of treatment the sacral region showed signs of dermatitis and erythema. Following each incontinence episode the affected area was cleaned with SECURA Cleanser. SECURA Extra Protective Cream Z30 was also applied to help protect the skin. This was applied once a day.
ResultsWithin eleven days the condition of the skin improved with no signs of erythema or dermatitis, which were present at the start of treatment.As the treatment progressed the patient’s quality of life significantly improved as she experienced less discomfort due to skin irritation.
ConclusionsThis study shows that SECURA Cleanser and Extra Protective Cream Z30 were an effective way of helping to maintain skin integrity in an incontinent patient.
Start of treatment
End of treatment
Always read the label and use only as directed. If symptoms persist, consult your healthcare professional. ◊Trademark of Smith & Nephew SN11438 (06/2014)
™Trademark of Smith & Nephew SN11438 (06/2014)
SECURA™ Cleanser and Extra Protective Cream Z30 Case Study Prevention of skin lesions in the sacral region in an incontinent patientIliana Pérez, Manuel Rodríguez, Jesús Vallejo, Mª del Mar Valverde, NursesResidencia de Mayores “José Matía Calvo” (Cádiz)Antonio Blanco del Valle. Nurse.Clinical department. Wound treatment section, Smith & Nephew, Spain
IntroductionIncontinence may lead to the development of skin lesions in the sacral region. If left untreated there is a high risk that these lesions may develop into pressure ulcers. This is because irritation caused by urine, faeces as well as mechanical damage that can be caused by using soap and water and rubbing the area dry may lead to a break down in skin integrity.
PatientA 92-year-old woman with mixed incontinence, using incontinence pads 24 hours a day. The patient was totally dependent on care staff for her personal hygiene.
TreatmentAt the start of treatment the sacral region showed signs of dermatitis and erythema. Following each incontinence episode the affected area was cleaned with SECURA Cleanser. SECURA Extra Protective Cream Z30 was also applied to help protect the skin. This was applied once a day.
ResultsWithin eleven days the condition of the skin improved with no signs of erythema or dermatitis, which were present at the start of treatment.As the treatment progressed the patient’s quality of life significantly improved as she experienced less discomfort due to skin irritation.
ConclusionsThis study shows that SECURA Cleanser and Extra Protective Cream Z30 were an effective way of helping to maintain skin integrity in an incontinent patient.
Start of treatment
End of treatment
Always read the label and use only as directed. If symptoms persist, consult your healthcare professional.
™Trademark of Smith & Nephew SN11469 (06/14)
1. Cleanse
2. Protect
3. Moisturise
SECURA™ is formulated with high-quality ingredients that make the difference between basic care and proactive prevention. The user-friendly, colour-coded packaging reflects the 3-part, preventive skin care system. SECURA™ products are formulated with high-quality ingredients that define the standard of care for prevention.
SECURA™ provides a simple 3-part process for good skin care management:
1. Cleanse 2. Protect 3. Moisturise
The SECURA™ difference.
Simple skin care management with SECURA™Easy. Effective. Economical.
SN11469 - Secura Ad_EBOS.indd 1 6/23/2014 12:39:52 PM
™Trademark of Smith & Nephew SN11438 (06/2014)
SECURA™ Cleanser and Extra Protective Cream Z30 Case Study Prevention of skin lesions in the sacral region in an incontinent patientIliana Pérez, Manuel Rodríguez, Jesús Vallejo, Mª del Mar Valverde, NursesResidencia de Mayores “José Matía Calvo” (Cádiz)Antonio Blanco del Valle. Nurse.Clinical department. Wound treatment section, Smith & Nephew, Spain
IntroductionIncontinence may lead to the development of skin lesions in the sacral region. If left untreated there is a high risk that these lesions may develop into pressure ulcers. This is because irritation caused by urine, faeces as well as mechanical damage that can be caused by using soap and water and rubbing the area dry may lead to a break down in skin integrity.
PatientA 92-year-old woman with mixed incontinence, using incontinence pads 24 hours a day. The patient was totally dependent on care staff for her personal hygiene.
TreatmentAt the start of treatment the sacral region showed signs of dermatitis and erythema. Following each incontinence episode the affected area was cleaned with SECURA Cleanser. SECURA Extra Protective Cream Z30 was also applied to help protect the skin. This was applied once a day.
ResultsWithin eleven days the condition of the skin improved with no signs of erythema or dermatitis, which were present at the start of treatment.As the treatment progressed the patient’s quality of life significantly improved as she experienced less discomfort due to skin irritation.
ConclusionsThis study shows that SECURA Cleanser and Extra Protective Cream Z30 were an effective way of helping to maintain skin integrity in an incontinent patient.
Start of treatment
End of treatment
Always read the label and use only as directed. If symptoms persist, consult your healthcare professional.
CARELINES ISSUE #7

20 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] www.eboshealthcare.com.au 21
CARELINES ISSUE #
20 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
For information on the NEW Allegro Concepts Lifting Equipment and all EBOS Healthcare Patient Care Equipment please contact:
De’Ann Keevers on 0417 497 694 or [email protected]
CARELINES ISSUE #7
SALSA 200Compact Active Standing Aid
ALTO Lift ™ 200Heavy Duty Patient Lifting Hoist
Standard Yoke 4 Point Yoke Tri Hook Yoke
Pivot Frame Powere3d Pivot Frame Weight Scale
Multiple Grip Position Adjustable Kneepad Removable Footplate
Tempo Handle Kit Custom Sitting Sling Knob Kit for Custom Sitting Sling
NEW Products at EBOS Aged Care

www.eboshealthcare.com.au 23
CARELINES ISSUE #
22 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
Vernacare introduces new VernaFem in Australia
SECTION SECTION SUB HEAD
See below to requestfree samples or trials
T he UK manufactured product is made from clean over-issued newspaper and is disposed of in an environmentally friendly
manner by using pulp disposal units, also manufactured by Vernacare. By using this hygienic disposal method, hospitals can also improve their environmental performance since, after use, the urinals disintegrate into minute fragments that wash away down the drains using a cold water process.
VernaFem improves patient experience at UK South Tees Hospital UK South Tees Hospitals NHS Foundation Trust has introduced Vernacare’s new VernaFem female urinal to a number of acute wards at its James Cook University Hospital as part of its commitment to compassionate patient care. The VernaFem product provides greater independence and comfort for bed-bound female patients at the Middlesbrough hospital, helping to preserve their dignity. Angela Milbourne, Clinical Matron, Acute Medicine for South Tees Hospitals NHS Foundation Trust, said: “The product is making a big di�erence to some of our patients. Even in instances where sta� assistance is required to help place the urinal, it is more comfortable than being rolled onto a bed pan and it is also far less labour intensive. Two to four nurses can be required for other methods of continence care, whereas a maximum of one nurse is needed when using the female urinal.” Vernacare’s unique patient toileting solution is helping hospitals and aged care facilities to improve the culture of compassionate care. Using the product can be liberating for those females who are unable to
»For more information or to register for free samples or a trial of the new VernaFem, please email [email protected] or contact EBOS Customer Service at 1800 269 534
Free Call: 1800 269 534 Free Fax: 1800 810 257Email: [email protected] www.eboshealthcare.com.au
For more information or to register for free samples or a trial:
New VernaFemSingle-use pulp Female Urinal• DisposablepulpVernaFem,idealfortoiletingfemalepatientsinbed
• Aless-invasiveandmoredignifiedalternativetocatheterisationorincontinencepads
• Singleusesolution–reducestheriskofcrossinfectionandreducesnursesworkload
• Maceratableandbiodegradable
NEW
Ergonomicdesignhelpspromoteself-toileting
Curvededgesalloweasierpatientpositioning
Wideopeningincreasespatient
confidence
Uniquedesignretainscapacityandminimisesriskof
spillage
VernaFem-FullPageAd.indd 1 1/05/14 9:38 AM
Medical Product manufacturer Vernacare UK has just launched VernaFem, a new award winning pulp female urinal – designed and developed in partnership with the UK NHS Trusts. The VernaFem robust form includes a wide base to increase stability and capacity, combined with a wide opening to reduce spillage. Its curved design moulds to the female body for ease and comfort in a range of positions - from lying down to sitting.
get out of bed to use a commode or toilet, helping increase their confidence and self-esteem. The product broadens the traditional continence care options, such as catheters, bedpans and pads, providing a cost e�ective alternative. As a single-use pulp product it is a safe and hygienic method that can reduce the risk and cost associated with healthcare acquired infections. EBOS Healthcare, who have exclusive distribution of the Vernacare system of disposable pulp products and macerators for Australia, will be introducing the new VernaFem in May.
THE AUSTRALIAN HOSPITAL + HEALTHCARE BULLETIN WINTER 2014 hospitalhealth.com.au1
CARELINES ISSUE #6
Vernacare introduces new VernaFem in Australia
SECTION SECTION SUB HEAD
See below to requestfree samples or trials
T he UK manufactured product is made from clean over-issued newspaper and is disposed of in an environmentally friendly
manner by using pulp disposal units, also manufactured by Vernacare. By using this hygienic disposal method, hospitals can also improve their environmental performance since, after use, the urinals disintegrate into minute fragments that wash away down the drains using a cold water process.
VernaFem improves patient experience at UK South Tees Hospital UK South Tees Hospitals NHS Foundation Trust has introduced Vernacare’s new VernaFem female urinal to a number of acute wards at its James Cook University Hospital as part of its commitment to compassionate patient care. The VernaFem product provides greater independence and comfort for bed-bound female patients at the Middlesbrough hospital, helping to preserve their dignity. Angela Milbourne, Clinical Matron, Acute Medicine for South Tees Hospitals NHS Foundation Trust, said: “The product is making a big di�erence to some of our patients. Even in instances where sta� assistance is required to help place the urinal, it is more comfortable than being rolled onto a bed pan and it is also far less labour intensive. Two to four nurses can be required for other methods of continence care, whereas a maximum of one nurse is needed when using the female urinal.” Vernacare’s unique patient toileting solution is helping hospitals and aged care facilities to improve the culture of compassionate care. Using the product can be liberating for those females who are unable to
»For more information or to register for free samples or a trial of the new VernaFem, please email [email protected] or contact EBOS Customer Service at 1800 269 534
Free Call: 1800 269 534 Free Fax: 1800 810 257Email: [email protected] www.eboshealthcare.com.au
For more information or to register for free samples or a trial:
New VernaFemSingle-use pulp Female Urinal• DisposablepulpVernaFem,idealfortoiletingfemalepatientsinbed
• Aless-invasiveandmoredignifiedalternativetocatheterisationorincontinencepads
• Singleusesolution–reducestheriskofcrossinfectionandreducesnursesworkload
• Maceratableandbiodegradable
NEW
Ergonomicdesignhelpspromoteself-toileting
Curvededgesalloweasierpatientpositioning
Wideopeningincreasespatient
confidence
Uniquedesignretainscapacityandminimisesriskof
spillage
VernaFem-FullPageAd.indd 1 1/05/14 9:38 AM
Medical Product manufacturer Vernacare UK has just launched VernaFem, a new award winning pulp female urinal – designed and developed in partnership with the UK NHS Trusts. The VernaFem robust form includes a wide base to increase stability and capacity, combined with a wide opening to reduce spillage. Its curved design moulds to the female body for ease and comfort in a range of positions - from lying down to sitting.
get out of bed to use a commode or toilet, helping increase their confidence and self-esteem. The product broadens the traditional continence care options, such as catheters, bedpans and pads, providing a cost e�ective alternative. As a single-use pulp product it is a safe and hygienic method that can reduce the risk and cost associated with healthcare acquired infections. EBOS Healthcare, who have exclusive distribution of the Vernacare system of disposable pulp products and macerators for Australia, will be introducing the new VernaFem in May.
THE AUSTRALIAN HOSPITAL + HEALTHCARE BULLETIN WINTER 2014 hospitalhealth.com.au1 • Free Call 1800 269 534 • Free Fax 1800 810 257• Email [email protected]
For more information:
The Vernacare Disposable System. Advancing infection prevention in healthcare facilities around the world.
The Vernacare pulp range is designed to help protect the nurse and patient from the risk of infection, the comprehensive range of
pulp receptacles are manufactured in the UK and carry the B.S.I Kitemark to guarantee effective liquid retention and maceration. The
Vortex macerator disposes of four single-use bedpans or urine bottles every 2 minutes, with no waiting around to unload processed
bedpans, no unhygienic stacking of soiled receptacles, and no cross contamination from inadequately cleaned bedpans. The Vortex
saves approx 60% water and 97% electricity compared to traditional pan washers.
TA K E I T F O R A S P I N P U L P A N D P U L P S U P P O R T R A N G E
ernacare has led the way in modern, hygienic and cost effective human waste management for more than four decades.
NEW NEW NEWNEW
24 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected] 24 EBOS Healthcare Aged Care Division. For more information please Phone: 1800 269 534 or Email: [email protected]
We hope you enjoyed this issue!
Visit: www.eboshealthcare.com.au
to receive this newsletter via email
Just click on the subscribe button.
carelines
carelines
carelines
carelines
carelines
carelines
carelines+
carelines
carelines
plus
Carelines is an EBOS initiative designed to support
the ongoing education and development of our
valued customers and their staff. Each edition
explores a wide range of topics relevant to the
aged care sector such as advanced wound
care, incontinence, infection prevention, nutrition
and oral care. Our objective is to continue
the support of people caring for people.