Embed Size (px)
Citation preview

CARE TRANSITIONS TASKFORCE – IMPROVEMENT WORK AT SFGH Larissa Thomas, MD | Michelle Schneidermann, MD | Karishma Oza, MPH
SFGH Division of Hospital Medicine

Outline
Background on care transitions Dashboard data Care Transitions Taskforce Work
Taskforce structure Inpatient work High risk work Outpatient work

What leads to problem transitions?
Discharge process Discharged quicker and sicker? Ineffective communication between sending and receiving
providers? Insufficient coordination and community referrals?
Patient factors: self-management skills/health literacy, confidence, what to watch for (“red flags”)
Medications: too many, inadequate access, or unclear instructions
Lack of access: to timely follow-up and/or advice line

SFGH Care Transitions Taskforce: Vision

SFGH Care Transitions Taskforce
Aim statement: Reduce all-cause 30 day readmissions for patients
discharged from San Francisco General Hospital by 15 percent from a baseline of 12.3 percent to 10.4 percent by December 2014.
Through: Coordination along care continuum
Promotion of best practice standards
Identification and referral of high risk patients
Provision of timely performance feedback

30-Day Readmission Rate: SFGH
12.49% 12.65%
12.88%
14.49%
13.02%
13.55% 13.46%
12.25%
11.00%
11.50%
12.00%
12.50%
13.00%
13.50%
14.00%
14.50%
15.00%
2012-1 2012-2 2012-3 2012-4 2013-1 2013-2 2013-3 2013-4 Quarter
Care Transitions dashboard draft | Karishma Oza, Michelle Schneidermann, MD & Larissa Thomas, MD | Mar. 2014 Source: LCR

30-Day CMS Readmission Rate for Core Measures
19.1% 20.5%
27.7% 27.0% 32.5%
37.9%
32.7% 33.6%
20.0%
15.6%
19.5%
24.0%
0%
5%
10%
15%
20%
25%
30%
35%
40%
2011Q2-2012Q1 2011Q4-2012Q3 2012Q2-2013Q1 2012Q3-2013Q2
Pneumonia CHF MI n=47
n=15
n=5
n=8
n=23
n=48 n=45
n=20
n=12
REGION 2011-Q2-2012Q1 2011Q4-2012Q3 2012Q2-2013Q1 2012Q3-2013Q2
Pneumonia 19.0% 18.7% 17.2% 17.4%
CHF 25.1% 26.7% 25.1% 25.0%
MI 20.3% 23.4% 22.9% 22.8%
CALIFORNIA
Pneumonia 18.6% 18.5% 18.3% 18.1%
CHF 26.4% 26.5% 26.2% 26.0%
MI 20.6% 20.1% 19.9% 19.9%
n=41
n=13
n=7
Source: CMS/Quality Net

30-Day Readmission Rate by Service
0%
5%
10%
15%
20%
25%
30%
35%
CAR FPR GYN MED NEU NSU NUR OBS OPH ORT OSU OTO PED PSU TRA URO
Service
2013-1 2013-2 2013-3
2013 median rate for all services: 7% (Q1), 9% (Q2), 8% (Q3)
Service 2013-1 2013-2 2013-3
CAR 39 42 49
FPR 29 42 65
GYN 4 3 1
MED 124 166 174
NEU 6 11 3
NSU 10 16 13
NUR 24 20 24
OBS 5 3 6
OPH 1 0 0
ORT 9 19 21
OSU 1 1 1
OTO 2 0 1
PED 13 9 8
PSU 3 4 4
TRA 20 30 45
URO 3 7 4
# of Readmissions by Service:
Source: LCR

30-Day Readmission Rate by Unit
Increased for 5A, 5D Stayed relatively the same for 4B, 5C Declined for 4D, 6A
11% 10%
14%
11%
13%
7% 8%
10%
13% 14% 15%
7%
11%
9%
15% 14%
16%
4%
0% 2% 4% 6% 8%
10% 12% 14% 16% 18%
4B 4D 5A 5C 5D 6A Unit
2013-1 2013-2 2013-3
Care Transitions dashboard draft | Karishma Oza, Michelle Schneidermann, MD & Larissa Thomas, MD | Mar. 2014 Source: LCR

30-Day Readmission Rate for Top 5 Index DRG Associated with Readmission
Index DRG 2013-1 2013-2 2013-3 Average
CHF NOS 22% 20% 39% 27%
PNEUMONIA ORGANISM NOS 15% 14% 17% 15%
ABDOMINAL PAIN-SITE NOS 11% 24% 20% 18%
ALCOHOL WITHDRAWAL 15% 21% 20% 19%
SHORTNESS OF BREATH 17% 13% 21% 17%
Care Transitions dashboard draft | Karishma Oza, Michelle Schneidermann, MD & Larissa Thomas, MD | Mar. 2014 Source: LCR

30-Day Readmission Rate: Homeless Patients
21%
17% 18% 16%
17% 18%
14% 16%
0%
5%
10%
15%
20%
25%
2012-1 2012-2 2012-3 2012-4 2013-1 2013-2 2013-3 2013-4
2012-13 readmit rate
• Steady decline since Q12012 • 2012-2013 average rate: 17%
Care Transitions dashboard draft | Karishma Oza, Michelle Schneidermann, MD & Larissa Thomas, MD |Mar. 2014 Source: LCR

Cardiology: LOS & Readmit Rate
4.6 4.3 3.4 4.0 3.6
4.5 3.8
3.0 3.2 3.4 3.9 3.6 2.8
6.8 5.7 6.3 6.3 6.5
5.4 5.2 4.4
6.5
4.5 4.7 5.5
4.3
10.9%
13.5%
11.5%
13.5% 12.5%
17.5% 16.0%
11.6% 13.1% 12.8%
17.9%
15.2%
15.8%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
0.0
5.0
10.0
15.0
20.0
25.0
Perc
enta
ge
Avg
LO
S (D
ays)
All Patients Readmitted Patients Readmit Rate
Care Transitions dashboard draft | Karishma Oza, Michelle Schneidermann, MD & Larissa Thomas, MD | Mar. 2014 Source: LCR

Proportion of SFGH Pts Attending PCH FU Appt Within 7 and 14 Days (2013 Average)
14-day FU appt rates approx. double 7-day rates
12% 11%
22%
13%
25%
16%
24%
18%
9% 10%
30%
12% 17%
23% 19%
47%
27%
47%
34%
42%
33%
17%
25%
57%
37% 34%
0%
10%
20%
30%
40%
50%
60%
7 Days 14 Days
Care Transitions dashboard draft | Karishma Oza, Michelle Schneidermann, MD & Larissa Thomas, MD | Mar. 2014 Source: LCR

Care Transitions Taskforce: Work to Date
INPATIENT improvement work Partnering with IT to build Standard d/c summary template within the EMR ePDP and d/c instructions within the EMR
Development of medical student and housestaff curricula on care transitions resources and best practices National best practice standards for all patients Red flag identification for high risk patients
In process: Requirement to complete d/c summary on day of d/c Standardization for PCP communication

asdfgghjjk asdfvb
CURRENTLY: medicine dept has excellent d/c summary template based on best practices. Problems: not user friendly, can choose whether or not to complete as prompted, not used by services other than medicine.
GOAL: build standardized template based on consensus guidelines directly into EMR. Benefits: User friendly, required by all services, force function to promote completeness.



Care Transitions Taskforce: Work to Date
HIGH RISK PATIENTS improvement work Risk prediction tools Developed a modified BOOST 7P’s tool Partnering w/IS to build LACE index into EMR
SFGH Transitional Care RN program Extending length of intervention Adding a CHF focus Adding a pharmacist to the team Piloting Meducation software
Partnering w/SF Community Care Transitions Program

BOOST at SFGH
Psychological Disease Principal Diagnoses OR Prior
Hospitalization in the last 6 months Polypharmacy and Problem
Medications Insufficient Patient Support Need for Palliative care Polysubstance abuse Placement


SFGH Transitional Care Nursing Program
What: RN-based intervention to prevent readmissions for high risk
patients Who qualifies:
>55 yrs old w/core measure diagnoses or referral from inpatient providers
Intervention: During hospitalization: coaching/motivational interviewing,
expanded med rec, and care plan. Additional teaching and pharmacy intervention for CHF.
Post-discharge phone calls: within 48 hours and then weekly phone calls for 30 days.
Care coordination with outpatient & community-based providers Warm-line

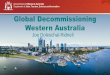
SFGH Transitional Care RN Program: Patient Characteristics
18%
73%
7% 2% Language
Chinese English Spanish Other
62%
38%
Gender
Male Female
Variable Values
Number of patients* 1419
Age, in years (average) 60
Male (%) 62%
Female (%) 38%
LANGUAGE:
Chinese (n, %) 259 (18%)
English (n, %) 1033 (73%)
Spanish (n, %) 104 (7%)
Other (n, %) 23 (2%)
*Between Oct 2012 and Oct 2013 Source: TCN Database

126
135 137
109
137
126
98
136
SFGH Transitional Care RN Readmission Rates & Timeline
18%
10% 9%
6%
11%
8%
5%
8%
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
Mar-13 Apr-13 May-13 Jun-13 Jul-13 Aug-13 Sept-13 Oct-13
Perc
enta
ge CCTP partnership started
CHF booklet implemented
Pharmacy pilot started
TAACT Collaborative
Source: TCN Database
Inclusion criteria & recruitment protocol implemented

SF Community Care Transitions Project
ACA initiative: CMS pays CBOs to do transitions work 9 hospitals and 8 CBOs in partnership with DAAS
Target: Medicare FFS beneficiaries Intervention: Social workers provide coaching, care
coordination, and service package: 14 d. home delivered meals Up to 6 hrs/day homecare 2 roundtrip visits to clinic appointments Linkage to case management as needed after 45 days

Care Transitions Taskforce: Work to Date
OUTPATIENT improvement work Taking Accountability for Ambulatory Care Transitions
(TAACT) collaborative Primary care-based pilot utilizing complex care management
teams to do transitions work Admission list developed with IT, sortable by clinic and
PCP (lives in EMR) Primary care integration working group to focus on
standards: Scheduling post-discharge follow-up appointment Content& documentation of post-discharge follow-up appts Use of non-physician personnel to provide post-discharge f/u

Admission List, Sortable by PCC or PCP
26

Care Transitions Taskforce: Next Steps
Data dashboard: Generate & present reports Look at specific high risk populations – homeless & marginally housed,
patients w/substance use disorders, hot-spotters Chart reviews & deeper dives of readmitted patients
High risk patients: Finalize & validate risk prediction tool Work with pharmacy leadership to expand resources for patients
with polypharmacy or high risk medications Work w/cardiology and administration to improve outpatient care of
complex HF patients Partner with DPH Primary Care Integration Group and
Transitions Dept. to scale up outpatient interventions Standardize follow-up of pending studies, explore options for a
post-discharge “warm line”