Embed Size (px)
Citation preview

Alfa D’Amato, Deputy Director, ABF TaskforceSusan Dunn, Manager, ABF Workstreams, ABF Taskforce
ABF TASKFORCEEmergency Department
Funding Model
ABF Taskforce

NHRA 2011 ObjectivesObjectives of the National Health Reforms – Broader than ABF
• Share the future cost of growth in the efficient price and service provision equally between the State and Commonwealth
• Establish a national consistent approach to activity based funding for public hospitals, with the provision for block funding smaller rural hospitals where required
• Ensure strong national standards to improve clinical safety and quality in hospitals and health care settings
• Enhance transparency on the performance of hospital and health care services.

National Health Reform Agreement Implementation of a nationally consistent Activity based funding
system for:
– admitted acute services, emergency department services and non-admitted patient services from July 2012
– mental health and sub and non-acute services from July 2013; and
Teaching Training and Research no later than 30 June 2018
Commonwealth will fund 45% of efficient growth from July 2014, increasing to 50% from July 2017.
Block Funded hospitals: Commonwealth will fund 45% of growth in efficient cost from July 2014, increasing to 50% from July 2017.

LHDs/SHNs
Australian Commission on Safety and Quality in
Health Care
National Health Performance
Authority
Independent Hospital Pricing
AuthorityNational Funding
Body
Ministry of Health
Data Provision by Health Departments Data Provision by Health Departments
National Minimum Data Set Reporting
Performance KPIse.g. Emergency
e.g. Elective Surgery
Patient Level Cost & Activity Data
Activity Targetse.g. Admitted Acute
e.g. Emergency
National Health Reform Act (NHRA)
National Minimum Data Set Reporting
Performance KPIse.g. Emergencye.g. Elective Surgery
Patient Level Cost & Activity Data
Activity Targetse.g. Admitted Acutee.g. Emergency

Independent Hospital Pricing Authority - IHPA An independent statutory authority established under
Commonwealth legislation (Dec 2011) as part of the National Health Reform Agreement (NHRA) reached by the Council of Australian Governments (COAG) in August 2011
Set in scope services, national efficient price (NEP $4808), set national efficient cost (NEC), set general guidelines
Guidelines may change in the future
May do audit in the future – therefore, need to be able to prove the source of data in WebNAP ie 150 Respiratory OOS in WebNAP corresponds to 150 OOS in IPM

State Accountability
System manager for the public hospital system
Negotiates with LHDs/SHNs about service volumes (targets) and locations to be delivered
Determines state funding contribution and total funding to each LHD/SHN. State price = $4471
Bears residual risk and meet costs of service delivery State remains majority funder of health services until 2063
when Commonwealth share finally reaches 50%BUT Role of the Independent Administrator may effect payments Local decision making - LHDs/SHNs responsible for allocation
of budgets to hospitals under Service Agreements

National Efficient Price (NEP)Interpreting the NEP
The NEP, as calculated by the IHPA, is based on the average cost of providing acute admitted services across Australia, but also applies to emergency and non-admitted services.
All cost weights are expressed as a single unit of measure being the National Weighted Activity Unit (NWAU). It provides a scale that identifies the relative measure of resource use of each public hospital service.

NEP Adjustments Indigenous - A patient based adjustment of 5%
LocationA patient based adjustment with three levels:
Outer regional 8.7%Remote 15.3%Very remote 19.4%
Calculation of Price$ (2012/13) = NEP x NWAU(12)NWAU(12) = URG_PriceWeight * (1+Aindig + Alocation))

Emergency Departments Classification System

Emergency Classification(1)Urgency Disposition Groups Classified to UDGs - Urgency Disposition Groups
– Classification developed by Dr George Jelinek (FACEM) in 1992 using WA hospitals data
– ED Role delineation 1 – 3A
– eg Batemans Bay, Sydney/Sydney Eye, Singleton
Requires correct classification of:
– Triage Category
– Disposition (mode of separation)
9

Emergency Classification (2)Urgency Related Groups Groups to URGs -
– Initially developed by Dr George Jelinek (FACEM) based on UDGs
– ED Role delineation 3B – 6
– eg Westmead, Prince Alfred, Liverpool
Requires correct classification of:
– Triage Category
– ED principal diagnosis
– groups to 27 Major Diagnostic Blocks
– Disposition (mode of separation)10

Urgency Disposition Groups
admitted non-admitted dead on arrival(URG 38)
did not wait(URG 73)
MDB 2A(URG 1)
MDB 3O(URG 2)
MDB 2B(URG 3)
MDB 1A/1B(URG 4)
MDB 3B(URG 5)
MDB 3A(URG 6)
MDB Other(URG 7)
triage 1 triage 2 triage 3 triage 4 triage 5
Emergency Department Classification System
Urgency Related Groups

URG Components
–Triage Category
–Disposition (mode of separation)
–ED principal diagnosis
URG 3 Admitted Triage 1 - Injury

URG Components:TriageDefinition:
Classification according to urgency of need for medical and nursing care, using the Australian Triage Scale.
Valid Triage Codes
– 1 Emergency Presentation
– 2 Emergency
– 3 Urgent
– 4 Semi urgent
– 5 Non urgent

URG Components:Disposition
Disposition Classes
• The URG classification system consists of 4 disposition classes that include:
– Non-admitted
– Admitted
– Dead on arrival
– Did not wait
Assignment to disposition class is dependent on ED Mode of Separation value
Code Domain Description

URG Components:DispositionCode ED Mode of Separation (disposition) Disposition
01 Admitted: To Ward/inpatient unit, not a Critical Care Ward Admitted
02 Admitted & discharged as inpatient within ED Non admitted
03 Admitted: Died in ED Died in ED
04 Departed: Treatment completed Non admitted
05 Departed: Transferred to another hospital without first being admitted to the hospital from which transferred
Transfer presentation
06 Departed: Did not wait Did not wait
07 Departed: Left at own risk Non admitted
08 Dead on Arrival Dead on Arrival
09 Departed: for other Clinical Service Location Non admitted
10 Admitted: To Critical Care Admitted
11 Admitted: Via Operating Suite Admitted
12 Admitted: Transferred to another hospital Transfer presentation
13 Admitted: Left at own risk Admitted
99 Registered in Error
Code Domain Description

URG Components:ED Diagnosis
•Diagnosis code maps to Major Diagnostic group•Acute bronchitis, unspecified
3B Respiratory system illness•Stroke, not specified as haemorrhage or infarction
3E Neurological illness•No diagnosis code = Moves to a UDG code

1A Poisoning, comatose1B Poisoning, conscious1C Drug reaction1D Alcohol/drug abuse and alcohol/drug induced mental disorders2A Injury, multiple sites2B Injury, single site2BA Injury, single site *minor (subset of MDB 2B)3A Circulatory system illness3B Respiratory system illness3C Digestive system illness3D Urological illness3E Neurological illness
Major Diagnostic Blocks

Recording Diagnosis 2012-13
Non-admitted patient
ED component
Time of arrival at ED Time of departure from ED
Applicable period of reported ED diagnosisED diagnosis assigned
URG Components:ED Diagnosis

Recording Diagnosis – 2012-13
Admitted to ward patient
ED component Ward component
Time of arrival at ED Time of departure from ED to ward
Applicable period of reported ED diagnosisED diagnosis assigned
Time of departureFrom hospital
Applicable period of reported principal diagnosis
Principal diagnosis assigned
URG Components:ED Diagnosis
URG/UDG AR-DRG

URG classification: Diagnosis code = SeizureURG classification can be any of these depending on the Triage category and the disposition (ED Separation mode)
Each of these URG codes will have a separate funding amount attached to it based on the National Weighted Activity Unit value.

Example of URG Funding Scenario 1 Major Trauma patient (non-aboriginal from a remote area) is brought in
via ambulance to a regional emergency department, & triaged as a category 1. Patient is stabilised, and a decision to transfer is made. Patient is subsequently transferred to a major tertiary major trauma centre. On discharge, patient ED principal diagnosis recorded as Traumatic subdural haemorrhage
Key data items:
Triage 1ED Mode of separation: Departed: Transferred to another hospital without first
being admitted to the hospital from which transferred (Non Admitted)Diagnosis –Traumatic subdural haemorrhage (MDB 2A) Injury, multiple
sitesAssigned -URG Group 39 Non Admitted Triage 1 – All MDB groupsATSI –No
Very Remote –Yes (19.4%)

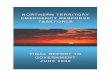
URG Funding Scenario 1 (cont)Price:
NWAU(12) = URG_39 PriceWeight * (1+Aindig + Alocation))
= 0.2203 * (1 + 0 + 0.194)
= 0.2630382
$ (2012/13) = State price x NWAU(12)
= $4,471 x 0.2630382
= $1,176.04

0
200
400
600
800
1000
1200
1400
1600
2011-12 Emergency URG 39 Non-Admitted Triage 1 - All MDB GroupsAverage Cost - Peer Groups A1 to C1 - Draft
Average Cost of URG 39 per ED Presentation

Example of URG Funding Scenario 2
Major Trauma patient (non-aboriginal from a remote area) from a regional emergency department is received at a major trauma centre. Patient is brought into the ED, triaged a category 1, assessed , CT scan is ordered, reviewed and a decision is made to transfer the patient to theatre. Patient is subsequently transferred to a ward. On ED discharge, patient ED principal diagnosis recorded as Traumatic subdural haemorrhage (S065).
Key data items:
Triage 1
ED Mode of separation 11 Admitted: Via Operating Suite (admitted)
Diagnosis Traumatic subdural haemorrhage (MDB 2A) Injury, multiple sites
Assigned - URG 3 Admitted Triage 1 -Injury
ATSI – No
Very Remote – Yes (19.4%)

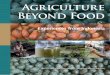
URG Funding Scenario 2 (cont)Price:
NWAU(12) = URG 3_PriceWeight * (1+Aindig + Alocation))
= 0.3313 * (1 + 0 + 0.194)
= 0.3955722
$ (2012/13) = State price x NWAU(12)
= $4,471 x 0.3955722
= $1,768.60

Average Cost of URG 3 per ED Presentation
0
500
1,000
1,500
2,000
2,500
3,000
3,500
2011-12 Emergency URG 3 Admitted Triage 1 - InjuryAverage Cost - Peer Groups A1 to C1 - Draft

Further ABF Information
Resource kit available: http://internal.health.nsw.gov.au/communications/funding_reform/resources.html
Email: [email protected]