Embed Size (px)
Citation preview
1
Care Transitionsto reduce 30-day readmissions
OneCity Health Care Model Webinar
March 28, 2016
2
“A standard set of roles, responsibilities, resources, and relationships for organizations within the PPS, designed to accomplish a specific project.”
Detailed implementation plans require an understanding of the local environment, and are being developed in conjunction with partners.
What is a care model?
3
October-December 2014
o Project-specific workgroup was created under leadership of subject matter experts to complete the NYS DOH DSRIP application. The application included description of the intervention that responded to the NYS DOH’s project requirements.
January-June 2015
o Clinical expertise group with broad range of backgrounds met in February and in April 2015 to review application, submit updates required by the NYS DOH, and determine implementation steps for basic implementation planning.
July 2015- January 2016
o OneCity Health finalized details for the State Implementation Plan (SIP).
o Care Transtions Care Model developed based on State requirements, national guidelines, literature review of evidence-based standards, and input from clinical expertise group and subject experts.
o Care Transitions Care Model was completed and presented to the OneCity Health Care Models Committee on January 7, 2106. The Care Models Committee represents a range of partner types and professional backgrounds, and members were nominated through a formal application process. The care model was recommended by the Care Models Committee and subsequently approved by the OneCity Health Executive Committee.
Development of Care Models
4
• By the end of the meeting today we will:
o Describe the core components of the Care Transitions project
o Understand the roles of transition management teams
o Understand the role of the acute care facilities in Care Transitions
o Understand how Care Transitions can help to link patients to community-based resources
Agenda for today’s webinar
5
• To provide a 30-day supported transition period for patients who are being discharged from the hospital and are at high risk of readmission
• Transitions management includes:
Assessing the patient in the hospital and developing a care plan prior to discharge
Addressing modifiable risk factors for readmission
Bridging the patient to resources in the community setting
Care Transitions Objectives
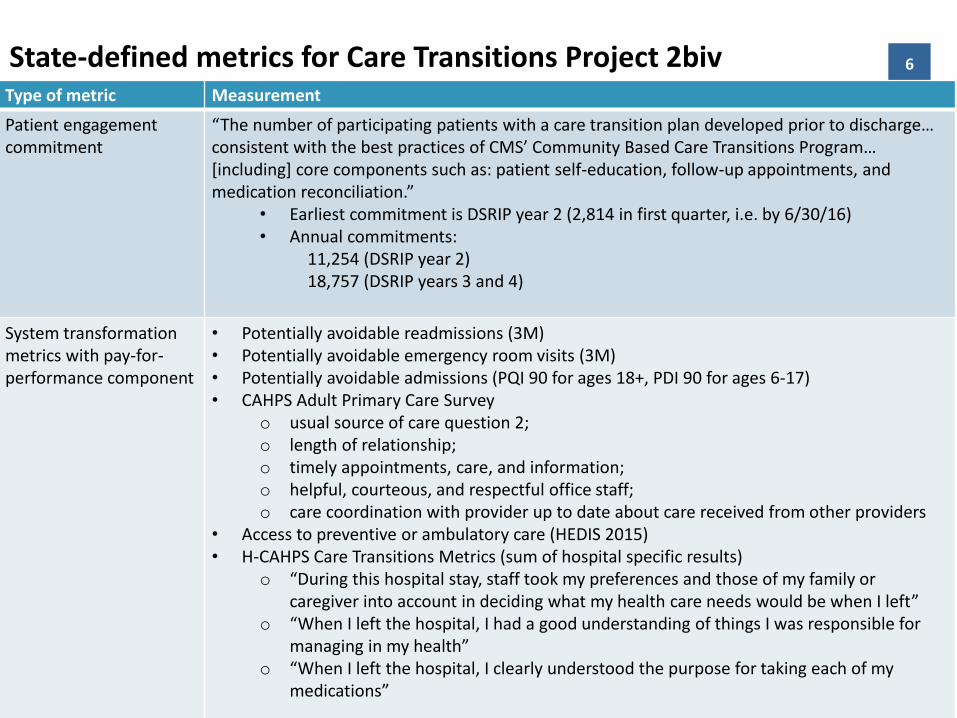
6State-defined metrics for Care Transitions Project 2bivType of metric Measurement
Patient engagement commitment
“The number of participating patients with a care transition plan developed prior to discharge… consistent with the best practices of CMS’ Community Based Care Transitions Program… [including] core components such as: patient self-education, follow-up appointments, and medication reconciliation.”
• Earliest commitment is DSRIP year 2 (2,814 in first quarter, i.e. by 6/30/16)• Annual commitments:
11,254 (DSRIP year 2)18,757 (DSRIP years 3 and 4)
System transformation metrics with pay-for-performance component
• Potentially avoidable readmissions (3M)• Potentially avoidable emergency room visits (3M)• Potentially avoidable admissions (PQI 90 for ages 18+, PDI 90 for ages 6-17)• CAHPS Adult Primary Care Survey
o usual source of care question 2; o length of relationship; o timely appointments, care, and information; o helpful, courteous, and respectful office staff; o care coordination with provider up to date about care received from other providers
• Access to preventive or ambulatory care (HEDIS 2015)• H-CAHPS Care Transitions Metrics (sum of hospital specific results)
o “During this hospital stay, staff took my preferences and those of my family or caregiver into account in deciding what my health care needs would be when I left”
o “When I left the hospital, I had a good understanding of things I was responsible for managing in my health”
o “When I left the hospital, I clearly understood the purpose for taking each of my medications”
7Core Components of Care Transitions Intervention
• Identifying patients at high risk of readmission early in the hospital stay. o Focus on potentially preventable readmissions
• Transitions management for patients identified as at high risk of readmission.o A dedicated transitions management team will visit referred
patients in the hospital and continue follow-up until 30 days after discharge
• Leveraging the OneCity Health partner network to address actionable risk factors.o The transition management team will link patients to resources
that meet their needs.
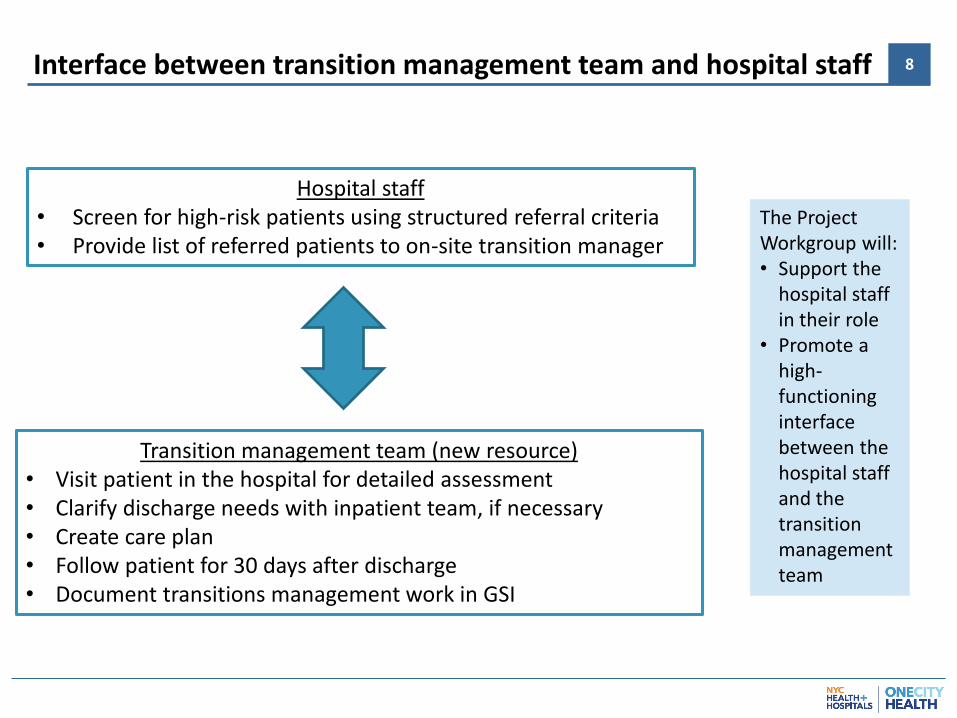
8Interface between transition management team and hospital staff
Hospital staff• Screen for high-risk patients using structured referral criteria• Provide list of referred patients to on-site transition manager
Transition management team (new resource)• Visit patient in the hospital for detailed assessment• Clarify discharge needs with inpatient team, if necessary• Create care plan • Follow patient for 30 days after discharge• Document transitions management work in GSI
The Project Workgroup will:• Support the
hospital staff in their role
• Promote a high-functioning interface between the hospital staff and the transition management team
9Hospital staff will identify and refer high-risk patients
• OneCity Health initial working estimate is that 15-20% of patients discharged from the hospital will receive transitions management services
• Patients are eligible for this program regardless of insurance status
• Review of patient lists for referrals should become standard work on inpatient units.
This may be best done during multidisciplinary team rounds as different disciplines will have key perspectives on readmissions risk.
• Identifying and referring patients will be the major new work for this project, from the perspective of inpatient clinical teams
10Referral criteria
Prior hospitalization in last 90 days
Behavioral health condition that interferes with self-care
Social support insufficient to meet follow-up needs, or high caregiver stress
Significant recent decline in ADL
High risk of medical decompensation in absence of close short-term follow-up
• These referral criteria were drafted based on literature review and expert workgroups. • The purpose of these referral criteria is to structure how inpatient teams think about
referrals to transition management. • Patients with any of these criteria should be considered for referral to the transition
management team.
11Considerations in identifying and referring patients
• The Project Workgroup and the transition management team will collaborate to obtain the appropriate number and quality of referrals Identify opportunities to provide education and ‘marketing’ of transition
management services Identify processes that support teams in identifying high-risk patients, e.g. use
daily census report during the rounds to mark candidates and provide it to care transitions team
Identify how teams can consistently communicate referrals to the transition management team (e.g. designate a point person on the unit to collect and communicate referrals; set up communication via phone, secure email, etc.)
Promote strong working relationships between inpatient staff and their transition management teams, e.g. invite transitions managers to routine rounds
• The referring team does not need to research the patient’s other care management options in order to refer the patient. The transitions management team will undertake the work of assessing and
coordinating with patients’ other care management resources.
12Will data-driven algorithms be used to identify high-risk patients?
• Risk stratification algorithms can use information from databases, such as billing or EMR data, to identify patients at higher risk of readmission and automatically ‘refer’ them to transitions managers
• For the Phase 1 implementation period, OneCity Health will not be providing a risk stratification algorithm
• The option of data-based risk algorithms is being actively explored by OneCity Health for later phases of the project.
• Issues that need to be considered include: Technical issues in linking Quadramed data to risk algorithms
Limited data quality in the absence of payer data
Prominent risk factors for readmission include factors (like social stress and functional decline) are not well represented in our databases
• If data-based algorithms are incorporated later in later phases of the project, they will supplement (not replace) referrals from hospital staff
13
• The transition management teams will be funded by OneCityHealth and matched to acute care facilities
• Transition management teams will include:o A clinically licensed professional as team leader
o Care coordinators working under the team leader’s supervision
o Additional resources assisting the transition management team, such as pharmacist or other supportive clinical backgrounds
• The tasks of the transition management team will be standardized across OneCity Health hospitals
• Transition managers will document their work in GSIo Clinical staff will not be required to use GSI
Transition management team: roles and activities
14
Visit referred patients in hospital for initial assessment
Identify and coordinate with other care management services available to the patient
Assist in medication reconciliation
Provide self-management support
Link to community-based resources as neededo E.g. home services, social services, caregiver support
Ensure ability to obtain medications, DME, and supplies as prescribed
Assist in follow-up with primary care physician and other key providers
Call patient after discharge within 24-48 hours
Provide phone calls and home visits as needed for 30 days after discharge
Enter data, create care plan, and track in GSI
The intensity and type of transition management services will be determined by the transition management team, based on patient assessment.
Key tasks of transition management teams
15Each Facility will have a Project Workgroup
• The Workgroup will play an essential role in the success of this project
• Creating highly functional interfaces between different teams and settings is the key to a high-functioning integrated delivery system
• Workgroup tasks include Educate hospital staff about transitions management program
Imbed referral processes in routine hospital staff work
Help transition management team to integrate into hospital setting
Help to understand existing care management resources at the facility and create high-functioning interfaces with transition management teams
Arrange for contact person that transition managers can call with questions that arise after patients are discharged
Provide feedback to OneCity Health on how to improve program
• Workgroups will include representative(s) of the transition management team as well as hospital personnel
16Integrating care management resources
• Patients may be enrolled in or eligible for any of a variety of care management resources that vary between them specific roles and abilities
• As part of standard work, the transition management team will identify and coordinate with patients’ existing care management resources
Patients with ongoing care management services that include transition management
the OneCity Health transition manager will not enroll the patient, so as to avoid redundancy
Patients with ongoing care management services that cannot provide intensified transition management services
the OneCity Health transition manager will support the patient’s care managers during the transition period, in coordination with them
Patients without care management
the OneCity Health transition manager will manage the transition period, assess for ongoing care management needs beyond 30 days, and refer as needed
17Care Transitions links patients to the broader PPS network
• Transitions management intervention starts in the hospital, but focuses on the 30 days after discharge.
• This presents an opportunity to leverage and strengthen the PPS partner network
o Strengthen communication with primary care and other continuity providers
o Screen and refer patients for community-based programso E.g.: palliative care
o E.g.: nutritional therapy
o Develop a more sophisticated understanding of patients’ modifiable risk factors for readmissiono Understand the type and frequency of community-based needs for
patients discharged from OneCity Health acute care facilities
o Identify related strengths and gaps in our PPS network
18
• Questions?
• To contact our team, please email [email protected], with the title “Care Transitions”





























