Embed Size (px)
Citation preview

Care Coordination and Chronic Management: A Specialist’s View Karen E. Joynt, MD, MPH Harvard Medical School and Harvard School of Public Health Staff Cardiologist, Boston VA Medical Center June 6, 2014

Disclosures • I am a specialist

Outline • Why and When Specialists?
• Why Not Specialists?
• How Specialists? • Challenges to meaningful co-management
• Communication • Electronic Health Records
• Conclusions and Recommendations

Why Specialists?
0
5
10
15
20
25
30
35
40
45
50
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Perc
ent o
f Pop
ulat
ion
18–44, 2 or 3
45–64, 2 or 3
≥65, 2 or 3
18–44, 4 or more
45–64, 4 or more
≥65, 4 or more
• High prevalence of multimorbidity
Ward and Schiller, Prev Chron Dis 2013

Why Specialists? • Increasing prevalence of complex disease
Go et al, Circulation 2014

Why Specialists? • More familiarity may mean better care
• Lower mortality rates • Higher use of evidence-based therapies • Heart Failure, Heart Attack, Stroke • Less evidence in outpatient setting
• Higher “quality” care but similar outcomes
• Despite a higher burden of disease in specialist-managed patients
Ansari et al, JACC 2003; Go et al, AJM 1999; Joynt et al, Circ HF 2013; Mitchell et al, Stroke 1996

Why Specialists, Continued
5.5% 7.5%
25.9%
8.6% 10.9%
31.3%
11.0% 13.5%
36.3%
10.9% 12.4%
37.1%
0%
5%
10%
15%
20%
25%
30%
35%
40%
In-Hospital Mortality 30-Day Mortality One-Year Mortality
Mor
talit
y Ra
te fo
r Hea
rt F
ailu
re
Cardiologists General Internists Family Practitioners Other Physicians
Jong et al, Circulation 2003
• Lower mortality for heart failure patients

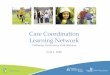
Why Specialists, Continued
16.1%
55.9%
23.3%
50.9%
25.3%
47.4%
19.4%
48.7%
0%
10%
20%
30%
40%
50%
60%
90-Day Mortality Discharge Home
Mor
talit
y Ra
te fo
r Hea
rt F
ailu
re
Neurologists General Internists Family Practitioners Combination
Mitchell et al, Stroke 1996
• Lower mortality for stroke patients

When Specialists?
14%
23% 25%
40%
16%
24%
30%
45%
15%
36% 34%
49%
18%
30% 34%
51%
0%
10%
20%
30%
40%
50%
60%
Low risk: <75 y, Charlson<2
Medium risk: <75 y, Charlson ≥2
High risk: ≥75 y, Charlson <2
Very high risk: ≥75 y, Charlson ≥2
One
Yea
r Mor
talit
y
Cardiologists General Internists Family Practitioners Other Physicians
Jong et al, Circulation 2003
• Greatest benefit is in highest-risk patients

Why Not Specialists?
$12,095
$8,414 $7,536
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
Cost of HF HospitalizationCardiologists General Internists Family Practitioners
Joynt et al, Circulation HF 2013; Mitchell et al, Stroke 1996
• Higher costs with more specialists/capita • Higher costs for HF and stroke
$7,218
$5,972 $5,096
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
Cost of Stroke HospitalizationNeurologists General Internists Family Practitioners

How Specialists? • Gatekeeping
• Prevent specialty visits at all costs
• Consultation • Obtain limited specialist input
• Shared management • Co-manage multiple conditions, share ideas
• Specialist management • Assume all aspects of care for patient

How Specialists? • Gatekeeping
• Healthy outpatient with occasional needs
• Consultation • Patient with complex organ-system disease
• Shared management • Patient with multiple chronic conditions
• Specialist management • Patient with rare needs (ESRD, VADs, TxP)

Barriers: Communication • The typical primary care physician has 229
(interquartile range, 125 to 340) other physicians working in 117 (interquartile range, 66 to 175) practices with which care must be coordinated, equivalent to an additional 99 physicians and 53 practices for every 100 Medicare beneficiaries managed by the primary care physician.
Pham et al, Annals 2009

Barriers: Communication
Primary Care
Physician
Specialist Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Pham et al, NEJM 2010

Electronic Health Records
Hsiao et al, Health Affairs 2013

EHRs: Specialty Care
Patel et al, JGIM 2013

Patient
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Primary Care
What is the Right Model?
Pham et al, NEJM 2010
• Care coordinator linked directly to patient

Patient
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Primary Care
What is the Right Model?
Pham et al, NEJM 2010
Care Coordinator
• Care coordinator linked directly to patient

Primary Care
Specialist
Specialist
Specialist
Specialist Specialist
Specialist
Specialist
What is the Right Model?
Pham et al, NEJM 2010
• Care coordinator centered with PCP

Primary Care
Specialist
Specialist
Specialist
Specialist Specialist
Specialist
Specialist
What is the Right Model?
Pham et al, NEJM 2010
Care Coordinator
• Care coordinator centered with PCP

Primary Care
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Primary Care
What is the Right Model?
Pham et al, NEJM 2010
• Care coordinators linked to specialists

Primary Care
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Primary Care
What is the Right Model?
Pham et al, NEJM 2010
Care Coordinator
• Care coordinators linked to specialists

Primary Care
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Specialist
Primary Care
What is the Right Model?
Pham et al, NEJM 2010
Care Coordinator
• Care coordinators linked to specialists
Care Coordinator

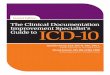
What is the Right Model?
Pham et al, NEJM 2010
• Care coordinators part of group practices
Medicare Patient
Primary care
physician Specialist
Specialist
Specialist
Specialist Primary
care physician
Specialist
Specialist
Specialist

What is the Right Model?
Pham et al, NEJM 2010
• Care coordinators part of group practices
Medicare Patient
Primary care
physician Specialist
Specialist
Specialist
Specialist Primary
care physician
Specialist
Specialist
Specialist Care
Coordinator

What is the Right Model?
Pham et al, NEJM 2010
• Care coordinators part of group practices
Medicare Patient
Primary care
physician Specialist
Specialist
Specialist
Specialist Primary
care physician
Specialist
Specialist
Specialist Care
Coordinator

Conclusions • The prevalence of complex patients is high
and rising • Specialists are an important part of the
health care team • Can improve outcomes for selected patients
• We don’t know how care should be shared • Likely many models, depending on needs
• Major barriers are communication and lack of “tradition” and clear roles

Recommendations • A team needs to form around the patient
• Best centered with lead decisionmaker
• We need shared information • Electronic health records, personal records
• More evidence should be generated • How should we organize the system? • Local laboratories • Learning health care systems