Embed Size (px)
Citation preview

Cardiovascular risk A key long-term comorbidity for HIV+
Dr Graeme Moyle
Chelsea and Westminster Hospital
London, United Kingdom

1999-2000 2001-2 2003-4 2005-6 2007-8 2009-11
Smith CJ et al. Lancet 2014
ICD-10 (until 2004)
CoDe (from 2004 on)
Age-standardised incidence rates (D:A:D Study)
All-cause (both AIDS and non-AIDS) mortality has
decreased with cART

SCOPE cohort: subclinical atherosclerosis in HIV
Hsue PY et al, AIDS 2009
mean
intima-media
thickness
mm

HIV is associated with a relative increase
in cardiovascular events
Age Group
Inci
de
nce
Rat
e o
f A
MI p
er
1,0
00
p
ers
on
ye
ars
PLHIV HIV-negative
Drozd et.al. 2017 JAIDS

“U-shaped” relationship between BMI and poor outcomes in PLHIV
Achhra et.al. 2018 JAIDS

SMART Study Group. N Eng J Med. 2006;355: 2283-2296.
No. at Risk
Treatment
Interruption 2720 2070 1663 1292 1041 867 693 543 443 375 273 157
Continuous Treatment
2752 2077 1692 1307 1070 899 713 563 462 380 282 165
44 40 36 32 28 24 20 16 12 8 4 0 0.00
0.05
0.10
0.15
0.20
Major Cardiovascular, Renal, or Hepatic Disease
Hazard ratio, 1.78; 95% CI, 1.1-2.5; P=0.009
Cu
mu
lati
ve
Pro
bab
ilit
y o
f E
ve
nt
Months
Treatment
Interruption
Continuous Treatment
N=5472 HIV-infected patients with a CD4+ cell count >350mm3
Endpoint Hazard Ratio
(95%CI)* P Value
Death, any cause 1.8 (1.2-2.9) 0.007
Major cardiovascular, renal or hepatic disease
1.7 (1.1-2.5) 0.009
Fatal or non-fatal CVD
1.6 (1.0-2.5) 0.05
*Treatment Interruption vs. Continuous Treatment
SMART Study: HIV Viremia Can Contribute to CV Risk

Lundgren J, et al; 8th IAS, Vancouver, Canada, July 19-22, 2015; Abst. MOSY0301.

Higher impact of smoking than that of HIV infection
in mortality of HIV-infected Persons
Helleberg M et al. Clin Infect Dis 2014
Pro
port
ion s
urv
ivin
g

Cardiovascular risk: calculation
Framingham risk score
AHA/ACC pooled cohort equations CV risk
calculator (PCE)
Friis-Moller et al, Eur J Prev Cardiol 2016
DAD model
includes age, gender, BP, smoking, FH, DM, TC, HDL,
CD4, cumulative exposure to PIs and NRTIs, current
use of ABC
predicted risk more accurately than Framingham

Non-modifiable risk factors common to CKD and CVD
1. Booth GL, et al. Lancet 2006;368:29–36; 2. Mocroft A, et al. AIDS 2010;24:1667–78; 3. Hunt SC, et al. Am J Prev Med 2003;24:136–42;
4. NICE CKD Guidelines 2008. http://www.nice.org.uk/nicemedia/pdf/CG073NICEGuideline.pdf; 5. NICE CVD Guidelines 2010. http://www.nice.org.uk/nicemedia/live/13024/49273/49273.pdf
Non-modifiable risk factors CKD CVD
Advancing age1,2 + +
Gender1,2 + (female) + (male)
Family history3,4 + +
Ethnicity4,5 + (Black/Asian) + (Asian)

Major modifiable risk factors CKD CVD
Diabetes1,2 + +
Hypertension1,2 + +
Dyslipidaemia/abnormal lipids1,3 + +
Smoking1,4 + +
HIV disease5–7 + +
Metabolic syndrome8,9 + +
Hepatitis C virus infection2,10 + +
Obesity1,11 + +
Many modifiable risk factors are common to CKD and CVD
1. NICE CVD Guidelines 2010. Available at http://www.nice.org.uk/nicemedia/live/13024/49273/49273.pdf; 2. Mocroft A, et al. AIDS 2010;24:1667–78; 3. CKD in Adults: UK Guidelines http://www.renal.org/CKDguide/full/UKCKDfull.pdf;
4. NICE CKD Guidelines http://www.nice.org.uk/nicemedia/pdf/CG073NICEGuideline.pdf; 5. SMART Study Group. N Eng J Med 2006;355:2283–96; 6. Klein D, et al. CROI. 2011;Abstract 810;
7. Campbell LJ, et al. HIV Med 2009;10:329–36; 8. WHO CVD Guidelines. http://www.who.int/cardiovascular_diseases/guidelines/Full%20text.pdf; 9. Royal College of Physicians CKD Guidelines. http://www.nice.org.uk/nicemedia/live/12069/42116/42116.pdf;
10. Butt AA, et al. Clin Infect Dis 2009;49:225–32; 11. Ix JH & Sharma KJ. Am Soc Nephrol 2010;21:406–12

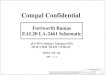
NA-ACCORD:
Contributions to MI Risk in HIV+ Subjects
Althoff K, et al. 24th CROI; Seattle, WA; February 13-16, 2017. Abst. 130.
Population attributable fractions have been adjusted for all the risk factors in the figure, as well as age, sex, race, HIV transmission risk, diabetes, and stage 4 chronic kidney disease.
Population attributable fractions and 95% confidence intervals for traditional and HIV-related factors, and hepatitis C virus infection, NA-ACCORD (1 Jan 2000 – 31 Dec 2013)
38% 41% 43%
2% 3%
10% 6%
2% 8%
0%
80%
Po
pu
lati
on
att
rib
uta
ble
tr
ac
tio
n (
PA
F)

Source: Haffner SM et al. NEJM 1998;339:229–234
Patients with DM but no CHD experience a similar rate of MI as patients
without DM but with CHD
Eve
nts
*/
10
0 p
ers
on
-ye
ars
Prior CHD
45 DM
No DM
No prior CHD
50
40
30
20
10
0
19 20
3.5
*Fatal or non-fatal MI
CHD=Coronary heart disease, DM=Diabetes mellitus, MI=Myocardial infarction
East-West Study
Diabetes Mellitus: Risk of Myocardial Infarction

CV Risk Modification in HIV
Petoumenos K for D:A:D . 20th CROI 2013.
Reduce TC 1 mmol/L
Stop smoking
CVD hazard in D:A:D*
Reduce sysBP 10 mmHg
*relative to 40 y.o. HIV+ male

NNT to Harm with MI: ABC in D:A:D
Risk Underlying 5
year risk (%) 5 year NNH
Underlying 10
year risk (%) 10 year NNH
Low (40 yo
non-smoker
with good
lipids and BP
0.1 1111 0.3 370
Smoker 0.4 277 1.5 92
Smoker and
DM 1.1 101 3.1 35
Smoker and
raised lipids 3.1 35 7.5 14
Previous CVD 5 22 10 14
Kowalska JD, et al . HIV Med. 2010 Mar;11(3):200-8. NNT, number needed to harm; MI, myocardial infarction; ABC, abacavir;
DM, diabetes mellitus; CVD, cardiovascular disease

Impact on CV risk of selected interventions
Intervention Type
HIV+ Patient Base Case Profile: 50 years
old, Male, On Abacavir, Smoker, w/
Hypertension, w/ Hyperlipidemia
1
Abacavir substitution with an alternative
antiviral without association to higher MI
rate [1][2][3]
2 Prescribing anti-hyperlipidemia
medication [4][8]
3 Prescribing anti-hypertensive medication
[4][7][8]
4
Counseling including standard treatment
for smoking cessation such as nicotine
patch and varenicline [4][5][6]
Hsue P, et al 692

D:A:D:
Cumulative Exposure to DRV/r Increase MI Risk
Ryom L, et al. 24th CROI; Seattle, WA; February 13-16, 2017. Abst. 128LB.
*Adjusted for gender, race, HIV exposure group, enrolment cohort, baseline date, prior CVD, nadir CD4 count, current CD4 count**, dyslipdaemia**, BMI**, diabetes**, eGFR**, age (all as fixed variates at baseline), HBV, HCV, smoking, family history of CVD, VL., hypertension, AIDS, cumulative exposure to darunavir/r, atazanavir/r, lopinavir/r & indinavir & recent exposure to abacavir (≤6 months) (all as time-updated variables).
**Factors considered to potentially lie on the causal pathway between PI/r exposure and CVD and values hence fixed at baseline.
Unadjusted CVD rate ratios per 5 years additional exposure: ATV/r 1.25 [1.10-1.43] and DRV/r 1.93 [1.63-2.28]
Adjusted* CVD rate ratios per 5 years additional exposure: ATV/r 1.03 [0.90-1.18] and DRV/r 1.59 [1.33-1.91]
Cumulative Years of Drug Exposure
Events
0 0-1 1-2 2-3 3-4 4-5 5-6 >6 0 0-1 1-2 2-3 3-4 4-5 5-6 >6
824 75 49 41 26 46 34 62 909 52 51 44 39 17 18 27
ATV/r DRV/r
20.0-
15.0-
10.0-
5.0-
4.0-
3.0-
2.0-
1.0-

ART classes and dyslipidaemia
NRTIs
TDF preferred (switching to TAF reduces lipid effect)
ABC associated with MI risk
NNRTIs
RPV, DOR preferred over EFV
PIs
ATV preferred even when boosted over LPV/rr
DRV/r associated with MI risk
InSTIs
Lipid neutral but no CV risk. Weight gain risk?

NEAT 022: Switch from PI/r- to DTG-based Regimen in Subjects with
Elevated CV Risk
Gatell J, et al. IAS 2017. Abstract 2461
• NEAT 022: randomised, open-label non-inferiority trial over 96 weeks in treatment-experienced
patients, designed to investigate lipid parameters in subjects with elevated CV risk*
– Changes in plasma lipids from BL to Week 48 were primary (TC) and secondary (other lipids) endpoints
– Co-primary endpoint: % of patients free of therapeutic failure at Week 48, in the ITT population
-8,7 -11,3
-18,4
-7,7
1,1
-7,0
0,7 0,5 4,2 2,0 2,5
0,4
-25,
-20,
-15,
-10,
-5,
0,
5,
TC Non-HDL-C
TG LDL-C HDL-C TC/HDLratio
p<0.001 p<0.001
p<0.001
p<0.001
p<0.001
P=0.286
• TC and other lipid
fractions (except HDL-
C) improved
significantly (p<0.001)
from BL with DTG.
• Virologic suppression
was maintained after
switch to DTG
Switching from a PI/r-based regimen to a DTG-based regimen improved
lipid profile versus continuing a P-based regimen in virologically
suppressed patients with elevated CV risk*
–7.0 –7.7 –8.7
–
11.3
–18.4
–5
–10
–5
–5
–15
Me
an
ch
an
ge
fro
m B
L t
o W
ee
k 4
8
(mm
ol/
L)
–20
–25
DTG† (n=205)
PI/r† (n=210)

Atorvastatin vs Pbo for Non-Ca++ Coronary Plaques
40 HIV-infected pts with subclinical coronary atherosclerosis and low density lipoprotein (LDL) cholesterol <130mg/dL
Coronary atherosclerotic plaque as assessed by coronary computed tomography angiography
Statin therapy was well-tolerated, with low incidence of clinical adverse events or laboratory abnormalities
-67,5
-45,
-22,5
0,
22,5
45,
NCPlaque % LDL-c mg/dl Lpa ng/dl
Changes in Non-Calcified Plaque and Key Lipids
Atorvastatin Placebo
Lo J, et al. 22nd CROI; Seattle, WA; February 23-26, 2015. Abst. 136.
p =.009 p =.0001 p =.0005

Beware of Drug Interactions
Boosters and statins esp simva-, fluva-statin
DRV induction and Atorva- and Rosuva-
Boosters and Ca Channel blockers e.g. amlodepine, diltiazem
Inducers (EFV>NVP) and statins, Ca Channels
DTG and metformin (+75%)

REPRIEVE: trial design (n=6500) http://reprievetrial.org/overview/
Screening and consent (asymptomatic HIV-infected persons with no history of CVD)
Randomisation
Mechanistic study primary (coronary plaque, vascular inflammation,
or immune activation)
Secondary end points (individual components of primary end point; all-cause death; incidence or progression
of non-calcified plaque; high-risk plaque; inflammatory, immunologic or metabolic biomarkers; predictors of statin effect; and non-AIDS-related comorbidities)
Composite primary end point (CVD-related death, myocardial infarction, unstable angina,
stroke, and arterial revascularization)
Placebo Pitavastatin 4mg daily

Management principles in HIV-infected persons
Same risk reduction strategies as general population
aspirin (?), statin, BP control, management of DM
Screen for DM and dyslipidaemia at baseline and every 3
to 6 and 6 to 12 months respectively
Use InSTI and avoid ABC in treatment naïve with
increased cardiovascular risk
Switch PI to InSTI has modest benefit on dyslipidaemia in
treatment experienced
atorvastatin, pitavastatin and rosuvastatin are statins of
choice for dyslipidaemia on ART