Embed Size (px)
Citation preview
Cardiovascular Roundtable
The New Economics of
Cardiovascular Services
17th Annual Topics in Cardiovascular Care
February 6, 2015
Brian Contos
Executive Director
The Advisory Board Company
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Road Map
2
3
1
2
CV Strategic Priorities Under the New Economics
• Finance Strategy: Avoidable Costs
• Clinical Strategy: Complex Care Management
• Service Strategy: Patient Experience
• Market Strategy: Patient Access
Discussion and Q&A
Cardiovascular Payment Policy Updates
• Inpatient
• Outpatient
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
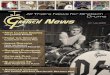
Defining Commonly Used Acronyms
3
Acronym Description
CMS Centers for Medicare and Medicaid Services: Federal agency
administering Medicare and Medicaid services; annual policy-setting
process for hospital, physician and other provider payment
MedPAC Medicare Payment Advisory Commission: Independent federal body
advising Congress on issues affecting administration of Medicare
Services; often influences CMS policy
ACA Affordable Care Act: Signed into law in 2010; includes provisions to
expand coverage and increase the quality and affordability of care;
impacts several aspects of hospital reimbursement policy
MS-DRG/DRG Medicare severity diagnosis related group: system to classify inpatients,
used to determine hospital payment
APC Ambulatory payment classification: system to classify hospital
outpatients, used to determine hospital payment
CPT/HCPCS Current procedural terminology/Healthcare common procedure coding
system: system to classify patient services, used for hospital outpatient
services and physician services, used to determine physician payment
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
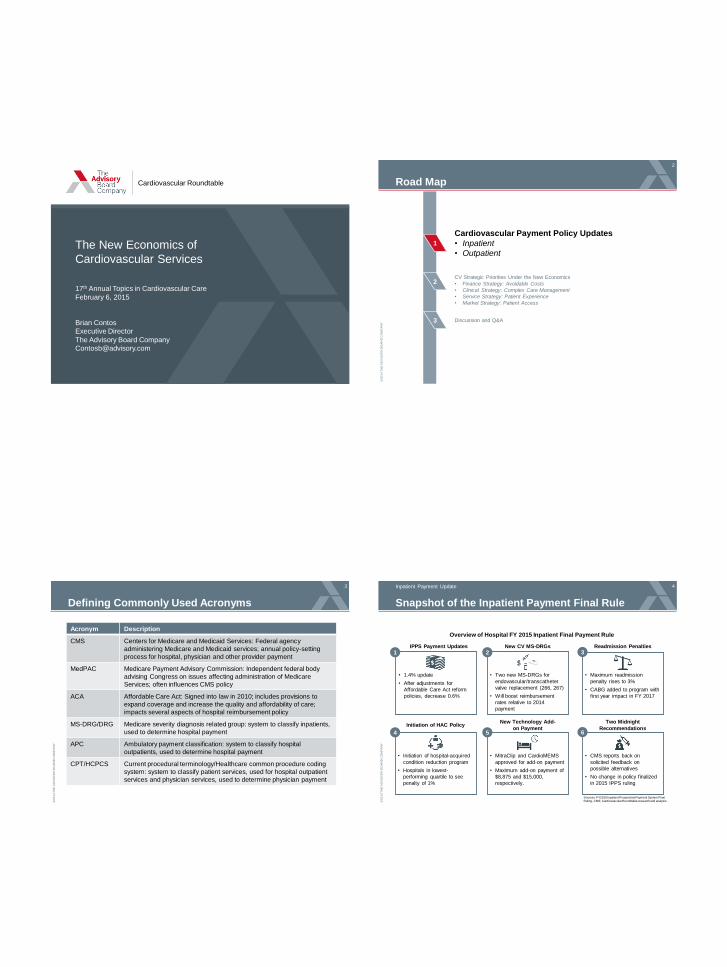
Snapshot of the Inpatient Payment Final Rule
4
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
Inpatient Payment Update
z 1
z 2
z 3
z 4
z 5
z 6
IPPS Payment Updates Readmission Penalties
Initiation of HAC Policy New Technology Add-
on Payment
• Maximum readmission
penalty rises to 3%
• CABG added to program with
first year impact in FY 2017
• Initiation of hospital-acquired
condition reduction program
• Hospitals in lowest-
performing quartile to see
penalty of 1%
• MitraClip and CardioMEMS
approved for add-on payment
• Maximum add-on payment of
$8,875 and $15,000,
respectively.
New CV MS-DRGs
• Two new MS-DRGs for
endovascular/transcatheter
valve replacement (266, 267)
• Will boost reimbursement
rates relative to 2014
payment
Two Midnight
Recommendations
• CMS reports back on
solicited feedback on
possible alternatives
• No change in policy finalized
in 2015 IPPS ruling
• 1.4% update
• After adjustments for
Affordable Care Act reform
policies, decrease 0.6%
Overview of Hospital FY 2015 Inpatient Final Payment Rule
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
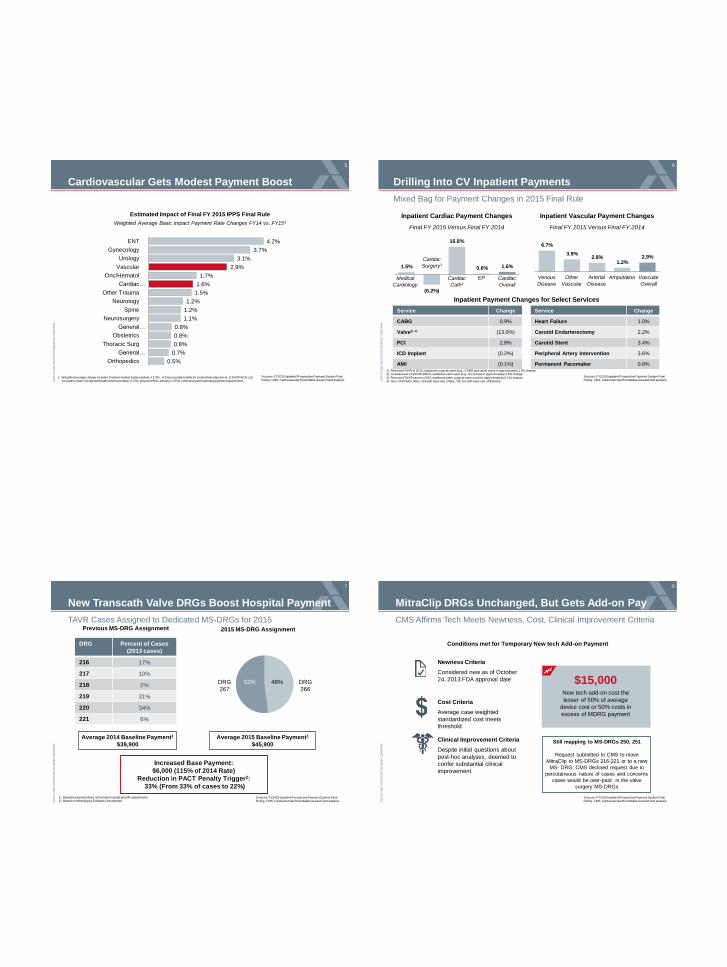
Cardiovascular Gets Modest Payment Boost
5
Estimated Impact of Final FY 2015 IPPS Final Rule
Weighted Average Basic Impact Payment Rate Changes FY14 vs. FY151
1. Weighted average change Includes: finalized market basket update (+2.9%, -0.5% proposed multifactor productivity adjustment,-0.2% PPACA cut), excludes impact of proposed readmissions penalty (-0.2%), proposed HAC penalty (-0.3%), other proposed operating payment adjustments
0.5%
0.7%
0.8%
0.8%
0.8%
1.1%
1.2%
1.2%
1.5%
1.6%
1.7%
2.9%
3.1%
3.7%
4.2%
Orthopedics
General…
Thoracic Surg
Obstetrics
General…
Neurosurgery
Spine
Neurology
Other Trauma
Cardiac…
Onc/Hematol
Vascular
Urology
Gynecology
ENT
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis. ©
20
14 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Drilling Into CV Inpatient Payments
6
Mixed Bag for Payment Changes in 2015 Final Rule
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
Service Change
CABG 0.9%
Valve3, 4 (13.0%)
PCI 2.8%
ICD Implant (0.2%)
AMI (0.1%)
Service Change
Heart Failure 1.0%
Carotid Endarterectomy 2.2%
Carotid Stent 3.4%
Peripheral Artery Intervention 3.6%
Permanent Pacemaker 0.8%
Inpatient Payment Changes for Select Services
1.5%
(6.2%)
16.8%
0.6% 1.6%
Inpatient Cardiac Payment Changes
Final FY 2015 Versus Final FY 2014
Cardiac
Surgery1
Cardiac
Cath2
EP Medical
Cardiology
Cardiac
Overall
6.7%
3.9% 2.8%
1.2% 2.9%
Amputation Other
Vascular
Arterial
Disease
Venous
Disease
Inpatient Vascular Payment Changes
Final FY 2015 Versus Final FY 2014
Vascular
Overall
1) Removed TAVR in 2015; traditional surgical cases (e.g., CABG and valve) result in approximately 1.0% change. 2) Includes new TAVR MS-DRGs; traditional cath cases (e.g., PCI) result in approximately 2.8% change.
3) Removed TAVR cases in 2015; traditional valve surgical cases result in approximately (0.1%) change. 4) New TAVR MS-DRGs: 266 with base rate of $52,743; 267 with base rate of $39,602.
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
New Transcath Valve DRGs Boost Hospital Payment
7
TAVR Cases Assigned to Dedicated MS-DRGs for 2015
1) Baseline payment does not include hospital-specific adjustments. 2) Based on Modeling by Edwards Lifesciences.
Previous MS-DRG Assignment
DRG Percent of Cases
(2013 cases)
216 17%
217 10%
218 2%
219 31%
220 34%
221 6%
52% 48% DRG
266
DRG
267
Increased Base Payment:
$6,000 (115% of 2014 Rate)
Reduction in PACT Penalty Trigger2:
33% (From 33% of cases to 22%)
Average 2014 Baseline Payment1
$39,900
Average 2015 Baseline Payment1
$45,900
2015 MS-DRG Assignment
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis. ©
20
14 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
MitraClip DRGs Unchanged, But Gets Add-on Pay
8
CMS Affirms Tech Meets Newness, Cost, Clinical Improvement Criteria
Conditions met for Temporary New tech Add-on Payment
Cost Criteria
Average case weighted
standardized cost meets
threshold
Newness Criteria
Considered new as of October
24, 2013 FDA approval date
Clinical Improvement Criteria
Despite initial questions about
post-hoc analyses, deemed to
confer substantial clinical
improvement
New tech add-on cost the
lesser of 50% of average
device cost or 50% costs in
excess of MDRG payment
$15,000
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
Still mapping to MS-DRGs 250, 251
Request submitted to CMS to move
MitraClip to MS-DRGs 216-221 or to a new
MS- DRG; CMS declined request due to
percutaneous nature of cases and concerns
cases would be over-paid in the valve
surgery MS-DRGs
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
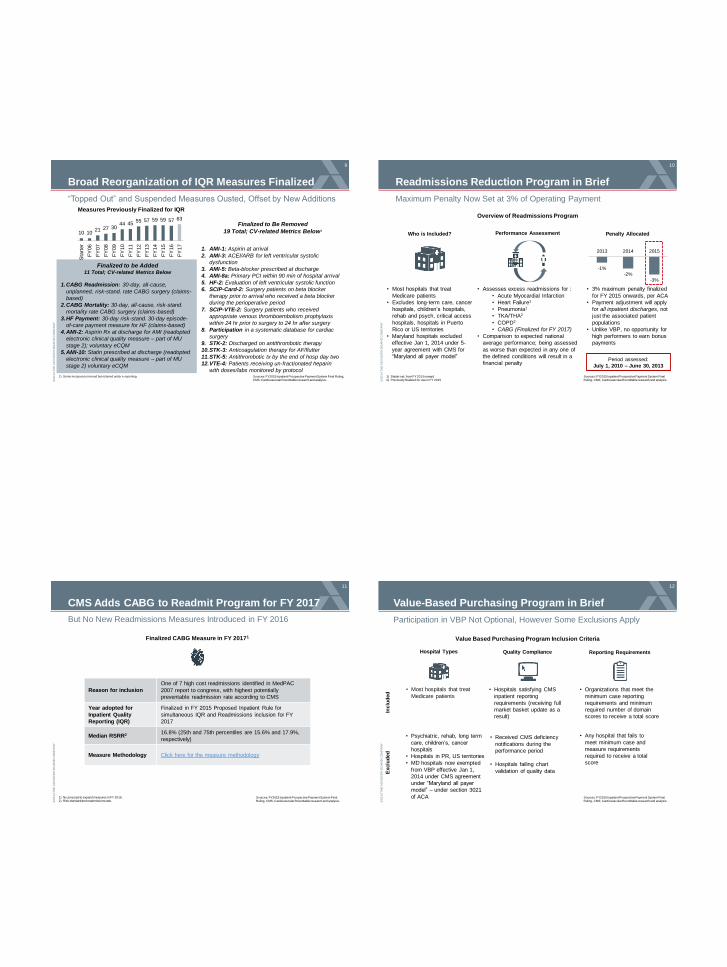
10 10 21 27 30
44 45 55 57 59 59 57 63
Sta
rter
FY
06
FY
07
FY
08
FY
09
FY
10
FY
11
FY
12
FY
13
FY
14
FY
15
FY
16
FY
17
9
“Topped Out” and Suspended Measures Ousted, Offset by New Additions
1.CABG Readmission: 30-day, all-cause,
unplanned, risk-stand. rate CABG surgery (claims-
based)
2.CABG Mortality: 30-day, all-cause, risk-stand.
mortality rate CABG surgery (claims-based)
3.HF Payment: 30-day risk-stand. 30-day episode-
of-care payment measure for HF (claims-based)
4.AMI-2: Aspirin Rx at discharge for AMI (readopted
electronic clinical quality measure – part of MU
stage 2); voluntary eCQM
5.AMI-10: Statin prescribed at discharge (readopted
electronic clinical quality measure – part of MU
stage 2) voluntary eCQM
Finalized to be Added 11 Total; CV-related Metrics Below
Finalized to Be Removed
19 Total; CV-related Metrics Below1
Measures Previously Finalized for IQR
1. AMI-1: Aspirin at arrival
2. AMI-3: ACEI/ARB for left ventricular systolic
dysfunction
3. AMI-5: Beta-blocker prescribed at discharge
4. AMI-8a: Primary PCI within 90 min of hospital arrival
5. HF-2: Evaluation of left ventricular systolic function
6. SCIP-Card-2: Surgery patients on beta blocker
therapy prior to arrival who received a beta blocker
during the perioperative period
7. SCIP-VTE-2: Surgery patients who received
appropriate venous thromboembolism prophylaxis
within 24 hr prior to surgery to 24 hr after surgery
8. Participation in a systematic database for cardiac
surgery
9. STK-2: Discharged on antithrombotic therapy
10.STK-3: Anticoagulation therapy for AF/flutter
11.STK-5: Antithrombotic tx by the end of hosp day two
12.VTE-4: Patients receiving un-fractionated heparin
with doses/labs monitored by protocol Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
Broad Reorganization of IQR Measures Finalized
1) Some measures removed but retained under e-reporting. ©
20
14 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Readmissions Reduction Program in Brief
10
Maximum Penalty Now Set at 3% of Operating Payment
Who is Included? Performance Assessment Penalty Allocated
• Most hospitals that treat
Medicare patients
• Excludes long-term care, cancer
hospitals, children’s hospitals,
rehab and psych, critical access
hospitals, hospitals in Puerto
Rico or US territories
• Maryland hospitals excluded
effective Jan 1, 2014 under 5-
year agreement with CMS for
“Maryland all payer model”
• Assesses excess readmissions for :
• Acute Myocardial Infarction
• Heart Failure1
• Pneumonia1
• TKA/THA2
• COPD2
• CABG (Finalized for FY 2017)
• Comparison to expected national
average performance; being assessed
as worse than expected in any one of
the defined conditions will result in a
financial penalty
• 3% maximum penalty finalized
for FY 2015 onwards, per ACA
• Payment adjustment will apply
for all inpatient discharges, not
just the associated patient
populations
• Unlike VBP, no opportunity for
high performers to earn bonus
payments
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
Overview of Readmissions Program
1) Starter set, from FY 2013 onward 2) Previously finalized for use in FY 2015
-1%
-2%
-3%
2013 2014 2015
Period assessed:
July 1, 2010 – June 30, 2013
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
CMS Adds CABG to Readmit Program for FY 2017
11
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
1) No proposal to expand measures in FY 2016. 2) Risk standardized readmissions ratio.
Reason for inclusion
One of 7 high cost readmissions identified in MedPAC
2007 report to congress, with highest potentially
preventable readmission rate according to CMS
Year adopted for
Inpatient Quality
Reporting (IQR)
Finalized in FY 2015 Proposed Inpatient Rule for
simultaneous IQR and Readmissions inclusion for FY
2017
Median RSRR2 16.8% (25th and 75th percentiles are 15.6% and 17.9%,
respectively)
Measure Methodology Click here for the measure methodology
But No New Readmissions Measures Introduced in FY 2016
Finalized CABG Measure in FY 20171
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Value-Based Purchasing Program in Brief
12
Participation in VBP Not Optional, However Some Exclusions Apply
Value Based Purchasing Program Inclusion Criteria
• Most hospitals that treat
Medicare patients
• Hospitals satisfying CMS
inpatient reporting
requirements (receiving full
market basket update as a
result)
Hospital Types Quality Compliance
• Organizations that meet the
minimum case reporting
requirements and minimum
required number of domain
scores to receive a total score
Reporting Requirements
Inclu
ded
E
xclu
ded
• Psychiatric, rehab, long term
care, children’s, cancer
hospitals
• Hospitals in PR, US territories
• MD hospitals now exempted
from VBP effective Jan 1,
2014 under CMS agreement
under “Maryland all payer
model” – under section 3021
of ACA
• Any hospital that fails to
meet minimum case and
measure requirements
required to receive a total
score
• Received CMS deficiency
notifications during the
performance period
• Hospitals failing chart
validation of quality data
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
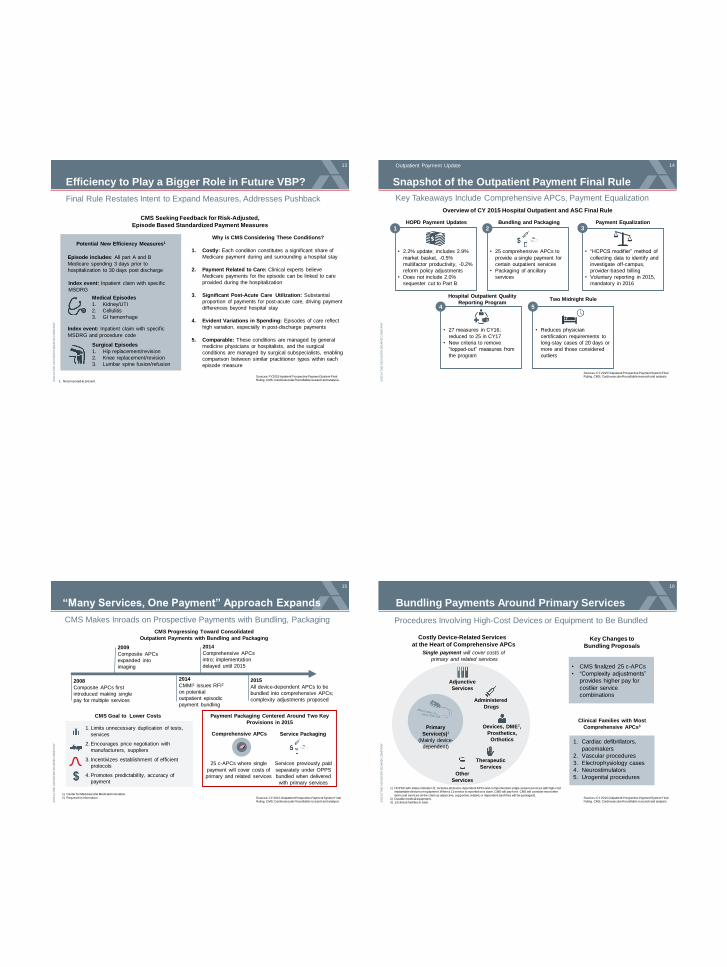
Efficiency to Play a Bigger Role in Future VBP?
13
1. Not proposed at present.
CMS Seeking Feedback for Risk-Adjusted,
Episode Based Standardized Payment Measures
Medical Episodes
1. Kidney/UTI
2. Cellulitis
3. GI hemorrhage
Surgical Episodes
1. Hip replacement/revision
2. Knee replacement/revision
3. Lumbar spine fusion/refusion
Potential New Efficiency Measures1
Index event: Inpatient claim with specific
MSDRG and procedure code
Why is CMS Considering These Conditions?
1. Costly: Each condition constitutes a significant share of
Medicare payment during and surrounding a hospital stay
2. Payment Related to Care: Clinical experts believe
Medicare payments for the episode can be linked to care
provided during the hospitalization
3. Significant Post-Acute Care Utilization: Substantial
proportion of payments for post-acute care, driving payment
differences beyond hospital stay
4. Evident Variations in Spending: Episodes of care reflect
high variation, especially in post-discharge payments
5. Comparable: These conditions are managed by general
medicine physicians or hospitalists, and the surgical
conditions are managed by surgical subspecialists, enabling
comparison between similar practitioner types within each
episode measure
Final Rule Restates Intent to Expand Measures, Addresses Pushback
Index event: Inpatient claim with specific
MSDRG
Episode includes: All part A and B
Medicare spending 3 days prior to
hospitalization to 30 days post discharge
Sources: FY2015 Inpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis. ©
20
14 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
14
Overview of CY 2015 Hospital Outpatient and ASC Final Rule
Snapshot of the Outpatient Payment Final Rule
z
• 2.2% update; includes 2.9%
market basket, -0.5%
multifactor productivity, -0.2%
reform policy adjustments
• Does not include 2.0%
sequester cut to Part B
1 z
2 z
3
z 4
z 5
HOPD Payment Updates Payment Equalization
Hospital Outpatient Quality
Reporting Program Two Midnight Rule
• “HCPCS modifier” method of
collecting data to identify and
investigate off-campus,
provider-based billing
• Voluntary reporting in 2015,
mandatory in 2016
• 27 measures in CY16;
reduced to 25 in CY17
• New criteria to remove
“topped-out” measures from
the program
• Reduces physician
certification requirements to
long-stay cases of 20 days or
more and those considered
outliers
Bundling and Packaging
• 25 comprehensive APCs to
provide a single payment for
certain outpatient services
• Packaging of ancillary
services
Key Takeaways Include Comprehensive APCs, Payment Equalization
Outpatient Payment Update
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
“Many Services, One Payment” Approach Expands
CMS Makes Inroads on Prospective Payments with Bundling, Packaging
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
1) Center for Medicare and Medicaid Innovation.
2) Request for information.
2008
Composite APCs first
introduced making single
pay for multiple services
2009
Composite APCs
expanded into
imaging
2014
Comprehensive APCs
intro; implementation
delayed until 2015
2015
All device-dependent APCs to be
bundled into comprehensive APCs;
complexity adjustments proposed
CMS Progressing Toward Consolidated
Outpatient Payments with Bundling and Packaging
Payment Packaging Centered Around Two Key
Provisions in 2015
CMS Goal to Lower Costs
25 c-APCs where single
payment will cover costs of
primary and related services
Comprehensive APCs
Services previously paid
separately under OPPS
bundled when delivered
with primary services
Service Packaging 1. Limits unnecessary duplication of tests,
services
2. Encourages price negotiation with
manufacturers, suppliers
3. Incentivizes establishment of efficient
protocols
4. Promotes predictability, accuracy of
payment
15
2014
CMMI1 issues RFI2
on potential
outpatient episodic
payment bundling
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Bundling Payments Around Primary Services
Procedures Involving High-Cost Devices or Equipment to Be Bundled
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
1) HCPSC with status indicator J1; includes all device-dependent APCs and comprehensive single-session services with high-cost implantable devices or equipment. When a J1 service is reported on a claim, CMS will pay for it. CMS will consider most other
items and services on the claim as adjunctive, supportive, related, or dependent (and they will be packaged). 2) Durable medical equipment. 3) 13 clinical families in total.
• CMS finalized 25 c-APCs
• “Complexity adjustments”
provides higher pay for
costlier service
combinations
Adjunctive
Services
Therapeutic
Services
Other
Services
Administered
Drugs
Primary
Service(s)1
(Mainly device-
dependent)
Costly Device-Related Services
at the Heart of Comprehensive APCs
Single payment will cover costs of
primary and related services
16
1. Cardiac defibrillators,
pacemakers
2. Vascular procedures
3. Electrophysiology cases
4. Neurostimulators
5. Urogenital procedures
Clinical Families with Most
Comprehensive APCs3 Devices, DME2,
Prosthetics,
Orthotics
Key Changes to
Bundling Proposals
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
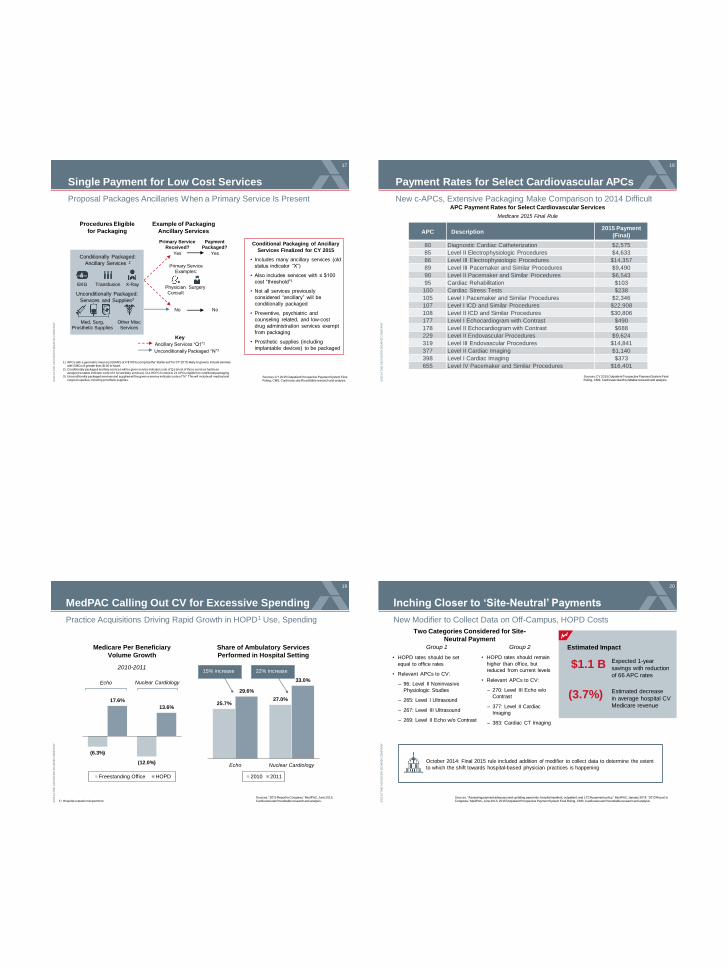
Single Payment for Low Cost Services
Proposal Packages Ancillaries When a Primary Service Is Present
Conditional Packaging of Ancillary
Services Finalized for CY 2015
• Includes many ancillary services (old
status indicator “X”)
• Also includes services with ≤ $100
cost “threshold”1
• Not all services previously
considered “ancillary” will be
conditionally packaged
• Preventive, psychiatric and
counseling related, and low-cost
drug administration services exempt
from packaging
• Prosthetic supplies (including
implantable devices) to be packaged
Example of Packaging
Ancillary Services
Procedures Eligible
for Packaging
Payment Packaged?
Primary Service Examples:
Conditionally Packaged:
Ancillary Services 2
1) APCs with a geometric mean cost (GMC) of ≤ $100 to comprise the “starter set” for CY 2015; likely to grow to include services with GMCs of greater than $100 in future.
2) Conditionally packaged ancillary services will be given service indicator code of Q1 (most of these services had been assigned a status indicator code of X for ancillary services). 511 HCPCS codes in 21 APCs eligible for conditional packaging.
3) Unconditionally packaged services and supplies will be given a service indicator code of “N.” This will include all medical and surgical supplies, including prosthetic supplies.
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
17
EKG Transfusion X-Ray
Unconditionally Packaged:
Services and Supplies3
Primary Service Received?
Yes
No
Physician Consult
Surgery
Yes
No
Med, Surg, Prosthetic Supplies
Other Misc Services
Ancillary Services “Q1”2
Unconditionally Packaged “N”3
Key
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Payment Rates for Select Cardiovascular APCs
18
New c-APCs, Extensive Packaging Make Comparison to 2014 Difficult
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
APC Payment Rates for Select Cardiovascular Services
Medicare 2015 Final Rule
APC Description 2015 Payment
(Final)
80 Diagnostic Cardiac Catheterization $2,575
85 Level II Electrophysiologic Procedures $4,633
86 Level III Electrophysiologic Procedures $14,357
89 Level III Pacemaker and Similar Procedures $9,490
90 Level II Pacemaker and Similar Procedures $6,543
95 Cardiac Rehabilitation $103
100 Cardiac Stress Tests $238
105 Level I Pacemaker and Similar Procedures $2,346
107 Level I ICD and Similar Procedures $22,908
108 Level II ICD and Similar Procedures $30,806
177 Level I Echocardiogram with Contrast $490
178 Level II Echocardiogram with Contrast $688
229 Level II Endovascular Procedures $9,624
319 Level III Endovascular Procedures $14,841
377 Level II Cardiac Imaging $1,140
398 Level I Cardiac Imaging $373
655 Level IV Pacemaker and Similar Procedures $16,401
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
MedPAC Calling Out CV for Excessive Spending
19
Practice Acquisitions Driving Rapid Growth in HOPD1 Use, Spending
Sources: “2013 Report to Congress,” MedPAC, June 2013; Cardiovascular Roundtable research and analysis. 1) Hospital outpatient department.
Medicare Per Beneficiary
Volume Growth
(6.3%)
(12.0%)
17.6%
13.6%
Freestanding Office HOPD
Echo Nuclear Cardiology
2010-2011
Share of Ambulatory Services
Performed in Hospital Setting
15% increase
25.7% 27.0%
29.6%
33.0%
Echo Nuclear Cardiology
2010 2011
22% increase
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Inching Closer to ‘Site-Neutral’ Payments
20
New Modifier to Collect Data on Off-Campus, HOPD Costs
Sources: “Assessing payment adequacy and updating payments: hospital inpatient, outpatient, and LTCH payment policy,” MedPAC, January 2014; “2013 Report to Congress,” MedPAC, June 2013; 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis
Two Categories Considered for Site-
Neutral Payment
Group 1 Group 2
• HOPD rates should be set
equal to office rates
• Relevant APCs to CV:
– 96: Level II Noninvasive
Physiologic Studies
– 265: Level I Ultrasound
– 267: Level III Ultrasound
– 269: Level II Echo w/o Contrast
Estimated Impact
$1.1 B Expected 1-year
savings with reduction
of 66 APC rates
(3.7%) Estimated decrease
in average hospital CV
Medicare revenue
• HOPD rates should remain
higher than office, but
reduced from current levels
• Relevant APCs to CV:
– 270: Level III Echo w/o
Contrast
– 377: Level II Cardiac
Imaging
– 383: Cardiac CT Imaging
October 2014: Final 2015 rule included addition of modifier to collect data to determine the extent
to which the shift towards hospital-based physician practices is happening
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
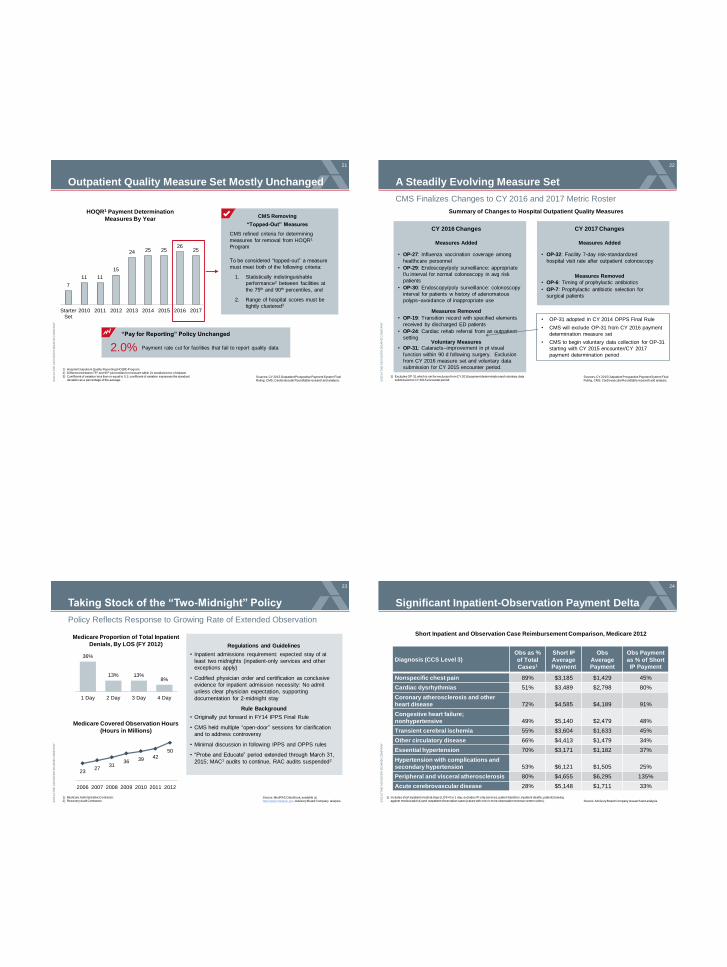
Outpatient Quality Measure Set Mostly Unchanged
21
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
7
11 11
15
24 25 25 26
25
StarterSet
2010 2011 2012 2013 2014 2015 2016 2017
HOQR1 Payment Determination
Measures By Year
1) Hospital Outpatient Quality Reporting (HOQR) Program. 2) Difference between 75th and 90th percentiles for measure within 2x standard error of dataset.
3) Coefficient of variation less than or equal to 0.1; coefficient of variation expresses the standard deviation as a percentage of the average.
CMS Removing
“Topped-Out” Measures
CMS refined criteria for determining
measures for removal from HOQR1
Program
To be considered “topped-out” a measure
must meet both of the following criteria:
1. Statistically indistinguishable
performance2 between facilities at
the 75th and 90th percentiles, and
2. Range of hospital scores must be
tightly clustered3
Payment rate cut for facilities that fail to report quality data 2.0%
“Pay for Reporting” Policy Unchanged
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
A Steadily Evolving Measure Set
22
CMS Finalizes Changes to CY 2016 and 2017 Metric Roster
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
Measures Added
• OP-27: Influenza vaccination coverage among
healthcare personnel
• OP-29: Endoscopy/poly surveillance: appropriate
f/u interval for normal colonoscopy in avg risk
patients
• OP-30: Endoscopy/poly surveillance: colonoscopy
interval for patients w history of adenomatous
polyps–avoidance of inappropriate use
Measures Removed
• OP-19: Transition record with specified elements
received by discharged ED patients
• OP-24: Cardiac rehab referral from an outpatient
setting Voluntary Measures
• OP-31: Cataracts–improvement in pt visual
function within 90 d following surgery. Exclusion
from CY 2016 measure set and voluntary data
submission for CY 2015 encounter period.
Measures Added
• OP-32: Facility 7-day risk-standardized
hospital visit rate after outpatient colonoscopy
Measures Removed
• OP-6: Timing of prophylactic antibiotics
• OP-7: Prophylactic antibiotic selection for
surgical patients
CY 2016 Changes CY 2017 Changes
• OP-31 adopted in CY 2014 OPPS Final Rule
• CMS will exclude OP-31 from CY 2016 payment
determination measure set
• CMS to begin voluntary data collection for OP-31
starting with CY 2015 encounter/CY 2017
payment determination period
1) Excludes OP-31 which is set for exclusion from CY 2016 payment determination and voluntary data submission for CY 2015 encounter period.
Summary of Changes to Hospital Outpatient Quality Measures
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Source: MedPAC Data Book, available at: http://www.medpac.gov; Advisory Board Company analysis.
36%
13% 13% 8%
1 Day 2 Day 3 Day 4 Day
Medicare Proportion of Total Inpatient
Denials, By LOS (FY 2012)
23 27
31 36 39 42
50
2006 2007 2008 2009 2010 2011 2012
Medicare Covered Observation Hours
(Hours in Millions)
Regulations and Guidelines
• Inpatient admissions requirement: expected stay of at
least two midnights (inpatient-only services and other
exceptions apply)
• Codified physician order and certification as conclusive
evidence for inpatient admission necessity: No admit
unless clear physician expectation, supporting
documentation for 2-midnight stay
Rule Background
• Originally put forward in FY14 IPPS Final Rule
• CMS held multiple “open-door” sessions for clarification
and to address controversy
• Minimal discussion in following IPPS and OPPS rules
• “Probe and Educate” period extended through March 31,
2015; MAC1 audits to continue, RAC audits suspended2
Taking Stock of the “Two-Midnight” Policy
Policy Reflects Response to Growing Rate of Extended Observation
23
1) Medicare Administrative Contractor. 2) Recovery Audit Contractor. ©
20
14 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Significant Inpatient-Observation Payment Delta
24
Source: Advisory Board Company research and analysis.
1) Includes short inpatient medical stays (LOS=0 or 1 day; excludes IP-only services, patient transfers, inpatient deaths, patients leaving against medical advice) and outpatient observation cases (cases with one or more observation revenue center codes).
Short Inpatient and Observation Case Reimbursement Comparison, Medicare 2012
Diagnosis (CCS Level 3) Obs as %
of Total
Cases1
Short IP
Average Payment
Obs
Average Payment
Obs Payment
as % of Short IP Payment
Nonspecific chest pain 89% $3,185 $1,429 45%
Cardiac dysrhythmias 51% $3,489 $2,798 80%
Coronary atherosclerosis and other
heart disease 72% $4,585 $4,189 91%
Congestive heart failure;
nonhypertensive 49% $5,140 $2,479 48%
Transient cerebral ischemia 55% $3,604 $1,633 45%
Other circulatory disease 66% $4,413 $1,479 34%
Essential hypertension 70% $3,171 $1,182 37%
Hypertension with complications and
secondary hypertension 53% $6,121 $1,505 25%
Peripheral and visceral atherosclerosis 80% $4,655 $6,295 135%
Acute cerebrovascular disease 28% $5,148 $1,711 33%

©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Has the Policy Worked?
Preliminary Reports, Anecdotal Evidence, Indicate Mixed Results
Source: MedPAC Comment Letter, accessed at: http://www.medpac.gov/documents/06132014_MedPAC_FY15_IPPS_comment.pdf;
Advisory Board Company interviews and analysis.
Category Before Two Midnight After Two Midnight1
Observation
Utilization
Growth in observation use,
significant volume of long stay
observation cases
Due to caution, accelerated observation
use reported by some facilities;
complaints that regulation does not
consider obs. workflow or infrastructure
Admissions
Clarity
Ambiguity regarding what
constitutes an appropriate
inpatient stay
Continued ambiguity as cases with
similar diagnosis and duration may be
considered differently depending on
admission time
Beneficiary
Liability
Observation proliferation
entails greater out-of-pocket
costs, ineligibility for SNF
coverage
Where greater observation volumes
have occurred, liability situation similar;
some recent movement on SNF
coverage issue2
Admissions Policy Issues Prior to and Post Two Midnight Rule Implementation
25
1) Two Midnight Rule “Probe and Educate” period currently extended through March 31, 2015. Although no RAC
audits are currently occurring, MAC audits of inpatient stays shorter than two midnights are ongoing. 2) CMS has recently exempted Medicare beneficiaries at some hospitals from the existing three-day stay SNF
qualification rule, though it has not been broadly instituted. For more information please see this posting: http://www.advisory.com/daily-briefing/2014/07/28/at-some-hospitals-medicare-is-ditching-an-observation-penalty. ©
20
14 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
CMS Loosens the Reins on Certification
Proposed Requirements Would Limit Physician Certification to Outliers
Sources: CY 2015 Outpatient Prospective Payment System Final Ruling, CMS; Cardiovascular Roundtable research and analysis.
Key Certification Proposals
• Physician certification a contentious
requirement of the two midnight rule
• CMS removing the requirement for
physician certification except in long-stay or
outlier case
• Certification for long-stay cases should be
furnished no later than the 20th day of the
stay
• Admission order and progress notes should
contain information to support medical
necessity even without the formal
certification requirement
Documentation Elements When
Certification Is Required
Reasons for continued
hospitalization
Special or unusual
services required for
outlier case
Estimated time
remaining on patient
stay
Plans for post hospital
care
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Road Map
2
3
1
27
CV Strategic Priorities Under the New Economics
• Finance Strategy: Avoidable Costs
• Clinical Strategy: Complex Care Management
• Service Strategy: Patient Experience
• Market Strategy: Patient Access
Discussion and Q&A
Cardiovascular Payment Policy Updates
• Inpatient
• Outpatient
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Framework for Assessing Avoidable Costs
28
Weighing the Options to Inflect CV Costs
Source: Cardiovascular Roundtable research and analysis.
Finance Strategy: Avoidable Costs
Three Methodologies to Identify High Spending Populations
Highest-Cost
Patients
Utilization
Variability
Avoidable Cost
Benchmarks
Population
• Costliness analysis to identify
high users of care
• Enables targeting individuals
for care management
• Often used as a proxy for
avoidability
• Identifies broad cost drivers
for a population
• Compares actual costs
against well-managed
populations
• Allows targeted management
of populations, conditions
based on feasibility
Individual
Most Specific Least Specific Avoidable Cost Specificity
Scope
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
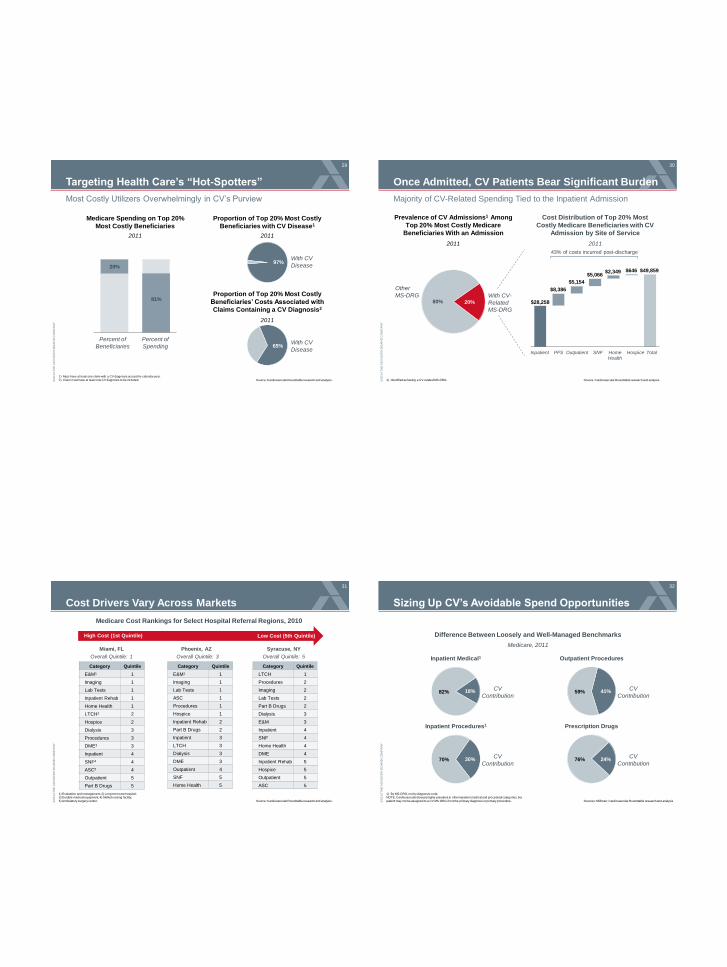
Targeting Health Care’s “Hot-Spotters”
29
Most Costly Utilizers Overwhelmingly in CV’s Purview
Source: Cardiovascular Roundtable research and analysis.
1) Must have at least one claim with a CV diagnosis across the calendar year. 2) Claim must have at least one CV diagnosis to be included.
20%
81%
Medicare Spending on Top 20%
Most Costly Beneficiaries
2011
Percent of
Beneficiaries
Percent of
Spending
Proportion of Top 20% Most Costly
Beneficiaries with CV Disease1
97% With CV
Disease
Proportion of Top 20% Most Costly
Beneficiaries’ Costs Associated with
Claims Containing a CV Diagnosis2
65%
2011
2011
With CV
Disease
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Once Admitted, CV Patients Bear Significant Burden
30
Majority of CV-Related Spending Tied to the Inpatient Admission
Source: Cardiovascular Roundtable research and analysis. 1) Identified as having a CV-related MS-DRG.
Prevalence of CV Admissions1 Among
Top 20% Most Costly Medicare
Beneficiaries With an Admission
2011
20% 80% With CV-
Related
MS-DRG
Other
MS-DRG
Cost Distribution of Top 20% Most
Costly Medicare Beneficiaries with CV
Admission by Site of Service
2011
Inpatient PFS Outpatient Home Health
Hospice Total SNF
43% of costs incurred post-discharge
$28,258
$8,386
$5,154
$5,066 $2,349 $646 $49,859
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Cost Drivers Vary Across Markets
31
Source: Cardiovascular Roundtable research and analysis.
1) Evaluation and management; 2) Long-term care hospital; 3) Durable medical equipment; 4) Skilled nursing facility;
5) Ambulatory surgery center.
Category Quintile
E&M1 1
Imaging 1
Lab Tests 1
Inpatient Rehab 1
Home Health 1
LTCH2 2
Hospice 2
Dialysis 3
Procedures 3
DME3 3
Inpatient 4
SNF4 4
ASC5 4
Outpatient 5
Part B Drugs 5
Category Quintile
E&M1 1
Imaging 1
Lab Tests 1
ASC 1
Procedures 1
Hospice 1
Inpatient Rehab 2
Part B Drugs 2
Inpatient 3
LTCH 3
Dialysis 3
DME 3
Outpatient 4
SNF 5
Home Health 5
Category Quintile
LTCH 1
Procedures 2
Imaging 2
Lab Tests 2
Part B Drugs 2
Dialysis 3
E&M 3
Inpatient 4
SNF 4
Home Health 4
DME 4
Inpatient Rehab 5
Hospice 5
Outpatient 5
ASC 5
Miami, FL Phoenix, AZ Syracuse, NY
Medicare Cost Rankings for Select Hospital Referral Regions, 2010
High Cost (1st Quintile) Low Cost (5th Quintile)
Overall Quintile: 1 Overall Quintile: 3 Overall Quintile: 5
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Sizing Up CV’s Avoidable Spend Opportunities
32
Sources: Milliman; Cardiovascular Roundtable research and analysis
1) By MS-DRG, not by diagnosis code. NOTE: Cardiovascular disease highly prevalent in other inpatient medical and procedural categories, but
patient may not be assigned to a CV MS-DRG if not the primary diagnosis or primary procedure.
18% 82%
Difference Between Loosely and Well-Managed Benchmarks
Medicare, 2011
Inpatient Medical1
CV
Contribution
30% 70%
Inpatient Procedures1
CV
Contribution
41% 59%
Outpatient Procedures
CV
Contribution
24% 76%
Prescription Drugs
CV
Contribution
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
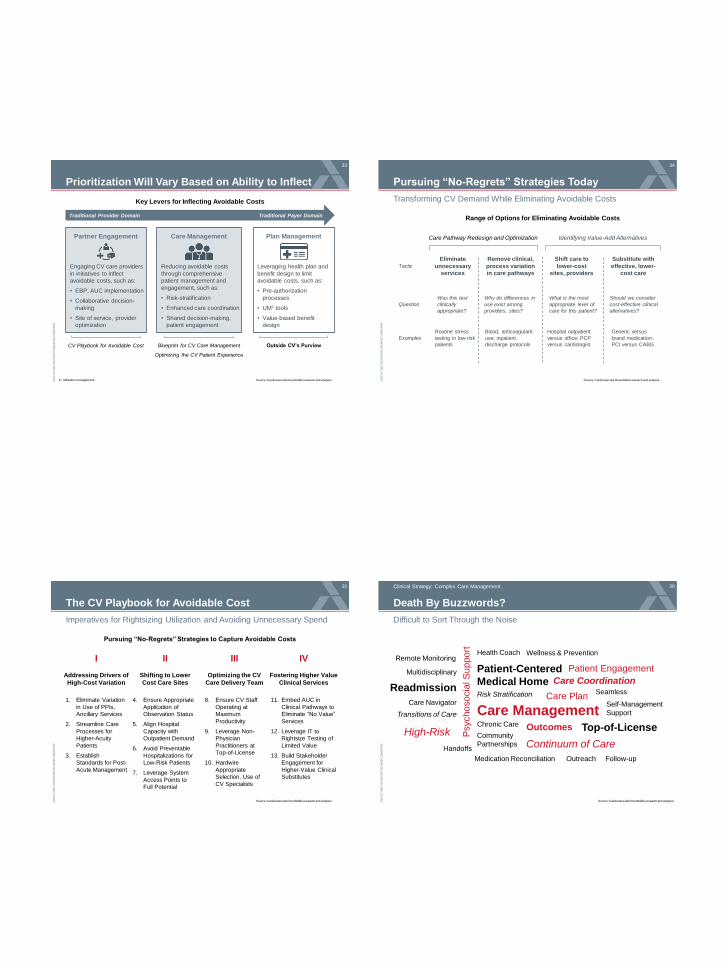
Prioritization Will Vary Based on Ability to Inflect
33
Source: Cardiovascular Roundtable research and analysis. 1) Utilization management.
Care Management
Reducing avoidable costs
through comprehensive
patient management and
engagement, such as:
• Risk-stratification
• Enhanced care coordination
• Shared decision-making,
patient engagement
Plan Management
Leveraging health plan and
benefit design to limit
avoidable costs, such as:
• Pre-authorization
processes
• UM1 tools
• Value-based benefit
design
Partner Engagement
Engaging CV care providers
in initiatives to inflect
avoidable costs, such as:
• EBP, AUC implementation
• Collaborative decision-
making
• Site of service, provider
optimization
Traditional Provider Domain Traditional Payer Domain
CV Playbook for Avoidable Cost Blueprint for CV Care Management
Optimizing the CV Patient Experience
Outside CV’s Purview
Key Levers for Inflecting Avoidable Costs
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Pursuing “No-Regrets” Strategies Today
34
Transforming CV Demand While Eliminating Avoidable Costs
Source: Cardiovascular Roundtable research and analysis.
Range of Options for Eliminating Avoidable Costs
Care Pathway Redesign and Optimization Identifying Value-Add Alternatives
Shift care to
lower-cost
sites, providers
What is the most
appropriate level of
care for this patient?
Hospital outpatient
versus office; PCP
versus cardiologist
Substitute with
effective, lower-
cost care
Should we consider
cost-effective clinical
alternatives?
Generic versus
brand medication;
PCI versus CABG
Eliminate
unnecessary
services
Was this test
clinically
appropriate?
Routine stress
testing in low-risk
patients
Remove clinical,
process variation
in care pathways
Blood, anticoagulant
use; inpatient
discharge protocols
Why do differences in
use exist among
providers, sites?
Tactic
Question
Examples
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
The CV Playbook for Avoidable Cost
35
Imperatives for Rightsizing Utilization and Avoiding Unnecessary Spend
Source: Cardiovascular Roundtable research and analysis.
Pursuing “No-Regrets” Strategies to Capture Avoidable Costs
1. Eliminate Variation
in Use of PPIs,
Ancillary Services
2. Streamline Care
Processes for
Higher-Acuity
Patients
3. Establish
Standards for Post-
Acute Management
Addressing Drivers of
High-Cost Variation
I
4. Ensure Appropriate
Application of
Observation Status
5. Align Hospital
Capacity with
Outpatient Demand
6. Avoid Preventable
Hospitalizations for
Low-Risk Patients
7. Leverage System
Access Points to
Full Potential
Shifting to Lower
Cost Care Sites
II
8. Ensure CV Staff
Operating at
Maximum
Productivity
9. Leverage Non-
Physician
Practitioners at
Top-of-License
10. Hardwire
Appropriate
Selection, Use of
CV Specialists
Optimizing the CV
Care Delivery Team
III
11. Embed AUC in
Clinical Pathways to
Eliminate “No Value”
Services
12. Leverage IT to
Rightsize Testing of
Limited Value
13. Build Stakeholder
Engagement for
Higher-Value Clinical
Substitutes
Fostering Higher Value
Clinical Services
IV
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Death By Buzzwords?
36
Difficult to Sort Through the Noise
Clinical Strategy: Complex Care Management
Readmission
High-Risk
Care Management
Patient-Centered
Medical Home Risk Stratification
Chronic Care
Care Plan Self-Management
Support
Psych
oso
cia
l S
up
po
rt
Community
Partnerships Continuum of Care
Care Navigator
Transitions of Care
Outcomes
Medication Reconciliation
Multidisciplinary
Remote Monitoring
Patient Engagement
Wellness & Prevention Health Coach
Seamless
Handoffs
Top-of-License
Care Coordination
Outreach Follow-up
Source: Cardiovascular Roundtable research and analysis.
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
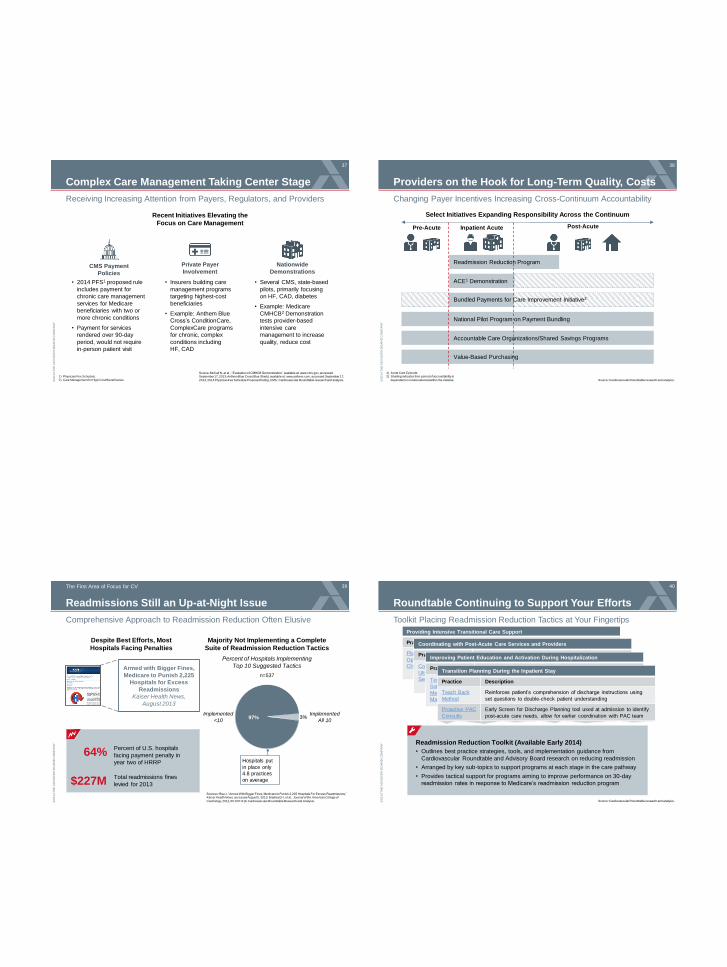
Complex Care Management Taking Center Stage
37
Receiving Increasing Attention from Payers, Regulators, and Providers
Source: McCall N, et al., “Evaluation of CMHCB Demonstration,” available at: www.cms.gov, accessed September 17, 2013; Anthem Blue Cross Blue Shield, available at: www.anthem.com, accessed September 17,
2013; 2014 Physician Fee Schedule Proposed Ruling, CMS; Cardiovascular Roundtable research and analysis.
1) Physician Fee Schedule. 2) Care Management for High-Cost Beneficiaries.
• 2014 PFS1 proposed rule
includes payment for
chronic care management
services for Medicare
beneficiaries with two or
more chronic conditions
• Payment for services
rendered over 90-day
period, would not require
in-person patient visit
CMS Payment
Policies
• Insurers building care
management programs
targeting highest-cost
beneficiaries
• Example: Anthem Blue
Cross’s ConditionCare,
ComplexCare programs
for chronic, complex
conditions including
HF, CAD
Private Payer
Involvement
• Several CMS, state-based
pilots, primarily focusing
on HF, CAD, diabetes
• Example: Medicare
CMHCB2 Demonstration
tests provider-based
intensive care
management to increase
quality, reduce cost
Nationwide
Demonstrations
Recent Initiatives Elevating the
Focus on Care Management
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Providers on the Hook for Long-Term Quality, Costs
38
Changing Payer Incentives Increasing Cross-Continuum Accountability
Source: Cardiovascular Roundtable research and analysis.
1) Acute Care Episode. 2) Shading indicates time period of accountability is
dependent on model selected within the initiative.
Pre-Acute Inpatient Acute Post-Acute
ACE1 Demonstration
Select Initiatives Expanding Responsibility Across the Continuum
Bundled Payments for Care Improvement Initiative2
Readmission Reduction Program
National Pilot Program on Payment Bundling
Value-Based Purchasing
Accountable Care Organizations/Shared Savings Programs
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Despite Best Efforts, Most
Hospitals Facing Penalties
Readmissions Still an Up-at-Night Issue
39
Comprehensive Approach to Readmission Reduction Often Elusive
Sources: Rau J, “Armed With Bigger Fines, Medicare to Punish 2,225 Hospitals For Excess Readmissions,” Kaiser Health News, accessed August 5, 2013; Bradley EH, et al., Journal of the American College of
Cardiology, 2012, 60: 607-614; Cardiovascular Roundtable Research and Analysis.
The First Area of Focus for CV
64% Percent of U.S. hospitals
facing payment penalty in
year two of HRRP
$227M Total readmissions fines
levied for 2013
3% 97%
Majority Not Implementing a Complete
Suite of Readmission Reduction Tactics
Percent of Hospitals Implementing
Top 10 Suggested Tactics
Implemented
All 10
Implemented
<10
Armed with Bigger Fines,
Medicare to Punish 2,225
Hospitals for Excess
Readmissions
Kaiser Health News,
August 2013
Hospitals put
in place only
4.8 practices
on average
n=537
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Toolkit Placing Readmission Reduction Tactics at Your Fingertips
Providing Intensive Transitional Care Support
Practice Description
Planning and
Operating a HF
Clinic
Roundtable Continuing to Support Your Efforts
40
Source: Cardiovascular Roundtable research and analysis.
Readmission Reduction Toolkit (Available Early 2014)
• Outlines best practice strategies, tools, and implementation guidance from
Cardiovascular Roundtable and Advisory Board research on reducing readmission
• Arranged by key sub-topics to support programs at each stage in the care pathway
• Provides tactical support for programs aiming to improve performance on 30-day
readmission rates in response to Medicare’s readmission reduction program
Coordinating with Post-Acute Care Services and Providers
Practice Description
Co-branded
Ultrafiltration
Services at PACs
Hospital partners with PAC nursing facility to provide co-
branded ultrafiltration services on site at the PAC; aim is to
reduce HF readmissions from the PAC, streamline care,
communication between the settings
Improving Patient Education and Activation During Hospitalization
Practice Description
Technology
Solutions for
Medication
Management
Transition Planning During the Inpatient Stay
Practice Description
Teach Back
Method
Reinforces patient’s comprehension of discharge instructions using
set questions to double-check patient understanding
Proactive PAC
Consults
Early Screen for Discharge Planning tool used at admission to identify
post-acute care needs, allow for earlier coordination with PAC team
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
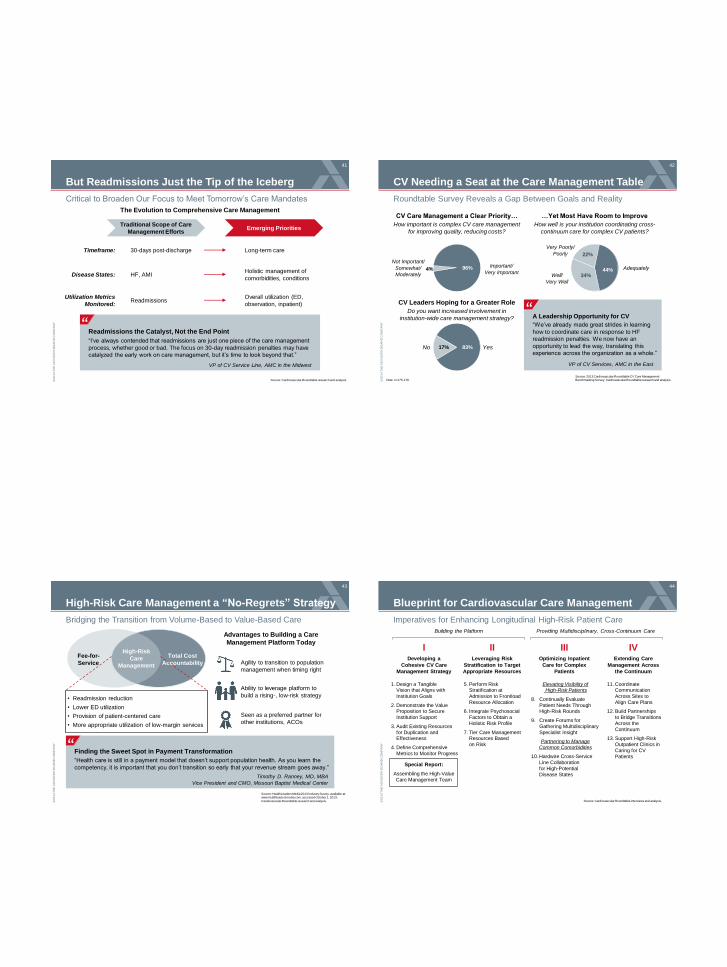
But Readmissions Just the Tip of the Iceberg
41
Critical to Broaden Our Focus to Meet Tomorrow’s Care Mandates
Source: Cardiovascular Roundtable research and analysis.
The Evolution to Comprehensive Care Management
Readmissions the Catalyst, Not the End Point
“I’ve always contended that readmissions are just one piece of the care management
process, whether good or bad. The focus on 30-day readmission penalties may have
catalyzed the early work on care management, but it’s time to look beyond that.”
VP of CV Service Line, AMC in the Midwest
”
Emerging Priorities Traditional Scope of Care
Management Efforts
Timeframe:
Disease States:
Utilization Metrics
Monitored:
30-days post-discharge Long-term care
HF, AMI Holistic management of
comorbidities, conditions
Readmissions Overall utilization (ED,
observation, inpatient)
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
CV Needing a Seat at the Care Management Table
42
Roundtable Survey Reveals a Gap Between Goals and Reality
Source: 2013 Cardiovascular Roundtable CV Care Management Benchmarking Survey; Cardiovascular Roundtable research and analysis. Note: n=175-179.
CV Care Management a Clear Priority…
How important is complex CV care management
for improving quality, reducing costs?
…Yet Most Have Room to Improve
How well is your institution coordinating cross-
continuum care for complex CV patients?
CV Leaders Hoping for a Greater Role
Do you want increased involvement in
institution-wide care management strategy? A Leadership Opportunity for CV
VP of CV Services, AMC in the East
”
22%
44% 34%
83% Yes
Very Poorly/
Poorly
Important/
Very Important 96%
“We’ve already made great strides in learning
how to coordinate care in response to HF
readmission penalties. We now have an
opportunity to lead the way, translating this
experience across the organization as a whole.”
Adequately
Well/
Very Well
17%
4%
Not Important/
Somewhat/
Moderately
No
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
High-Risk Care Management a “No-Regrets” Strategy
43
Bridging the Transition from Volume-Based to Value-Based Care
Source: HealthLeaders Media 2013 Industry Survey, available at: www.healthleadersmedia.com, accessed October 1, 2013;
Cardiovascular Roundtable research and analysis.
• Readmission reduction
• Lower ED utilization
• Provision of patient-centered care
• More appropriate utilization of low-margin services
Fee-for-
Service
High-Risk
Care
Management
Total Cost
Accountability Agility to transition to population
management when timing right
Ability to leverage platform to
build a rising-, low-risk strategy
Seen as a preferred partner for
other institutions, ACOs
Finding the Sweet Spot in Payment Transformation
“Health care is still in a payment model that doesn’t support population health. As you learn the
competency, it is important that you don’t transition so early that your revenue stream goes away.”
Timothy D. Ranney, MD, MBA
Vice President and CMO, Missouri Baptist Medical Center
”
Advantages to Building a Care
Management Platform Today
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Blueprint for Cardiovascular Care Management
44
Imperatives for Enhancing Longitudinal High-Risk Patient Care
Source: Cardiovascular Roundtable interviews and analysis.
Building the Platform Providing Multidisciplinary, Cross-Continuum Care
I II III IV Developing a
Cohesive CV Care
Management Strategy
Leveraging Risk
Stratification to Target
Appropriate Resources
Special Report:
Assembling the High-Value
Care Management Team
Optimizing Inpatient
Care for Complex
Patients
Extending Care
Management Across
the Continuum
1. Design a Tangible Vision that Aligns with
Institution Goals
2. Demonstrate the Value Proposition to Secure
Institution Support
3. Audit Existing Resources
for Duplication and Effectiveness
4. Define Comprehensive
Metrics to Monitor Progress
5. Perform Risk Stratification at
Admission to Frontload
Resource Allocation
6. Integrate Psychosocial
Factors to Obtain a
Holistic Risk Profile
7. Tier Care Management Resources Based
on Risk
Elevating Visibility of High-Risk Patients
8. Continually Evaluate
Patient Needs Through High-Risk Rounds
9. Create Forums for
Gathering Multidisciplinary
Specialist Insight
Partnering to Manage
Common Comorbidities
10. Hardwire Cross-Service
Line Collaboration
for High-Potential
Disease States
11. Coordinate Communication
Across Sites to
Align Care Plans
12. Build Partnerships
to Bridge Transitions
Across the
Continuum
13. Support High-Risk
Outpatient Clinics in
Caring for CV
Patients
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
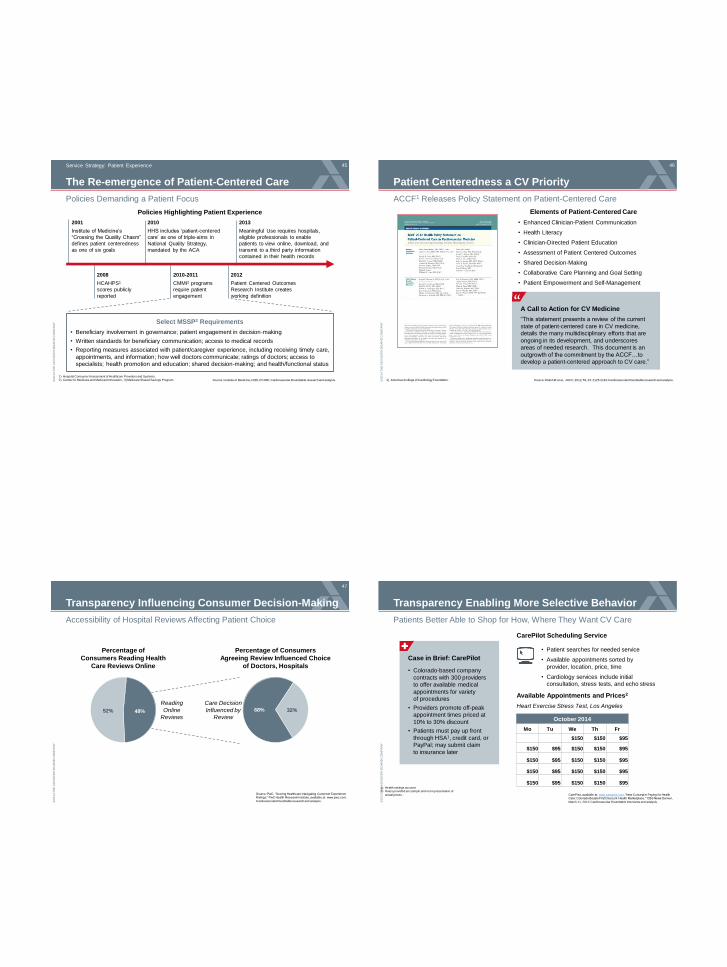
The Re-emergence of Patient-Centered Care
45
Policies Demanding a Patient Focus
Source: Institute of Medicine; CMS; PCORI; Cardiovascular Roundtable research and analysis.
Service Strategy: Patient Experience
1) Hospital Consumer Assessment of Healthcare Providers and Systems. 2) Center for Medicare and Medicaid Innovation.; 3) Medicare Shared Savings Program.
2001
Institute of Medicine’s
“Crossing the Quality Chasm”
defines patient centeredness
as one of six goals
2010
HHS includes ‘patient-centered
care’ as one of triple-aims in
National Quality Strategy,
mandated by the ACA
2013
Meaningful Use requires hospitals,
eligible professionals to enable
patients to view online, download, and
transmit to a third party information
contained in their health records
2010-2011
CMMI2 programs
require patient
engagement
Policies Highlighting Patient Experience
Select MSSP3 Requirements
• Beneficiary involvement in governance; patient engagement in decision-making
• Written standards for beneficiary communication; access to medical records
• Reporting measures associated with patient/caregiver experience, including receiving timely care,
appointments, and information; how well doctors communicate; ratings of doctors; access to
specialists; health promotion and education; shared decision-making; and health/functional status
2008
HCAHPS1
scores publicly
reported
2012
Patient Centered Outcomes
Research Institute creates
working definition
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Patient Centeredness a CV Priority
46
ACCF1 Releases Policy Statement on Patient-Centered Care
Source: Walsh M et al., JACC, 2012, 59, 23: 2125-2143; Cardiovascular Roundtable research and analysis. 1) American College of Cardiology Foundation.
A Call to Action for CV Medicine
“This statement presents a review of the current
state of patient-centered care in CV medicine,
details the many multidisciplinary efforts that are
ongoing in its development, and underscores
areas of needed research. This document is an
outgrowth of the commitment by the ACCF…to
develop a patient-centered approach to CV care.”
”
• Enhanced Clinician-Patient Communication
• Health Literacy
• Clinician-Directed Patient Education
• Assessment of Patient Centered Outcomes
• Shared Decision-Making
• Collaborative Care Planning and Goal Setting
• Patient Empowerment and Self-Management
Elements of Patient-Centered Care
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Transparency Influencing Consumer Decision-Making
47
Accessibility of Hospital Reviews Affecting Patient Choice
Source: PwC, “Scoring Healthcare: Navigating Customer Experience Ratings;” PwC Health Research Institute, available at: www.pwc.com;
Cardiovascular Roundtable research and analysis.
Percentage of Consumers
Agreeing Review Influenced Choice
of Doctors, Hospitals
48% 52% 68% 32%
Percentage of
Consumers Reading Health
Care Reviews Online
Reading
Online
Reviews
Care Decision
Influenced by
Review
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Patients Better Able to Shop for How, Where They Want CV Care
CarePilot, available at: www.carepilot.com, “New Concept in Paying for Health Care: Colorado Boasts First Discount ‘Health Marketplace,’” CBS News Denver,
March 11, 2012; Cardiovascular Roundtable interviews and analysis.
1) Health savings account. 2) Rates provided are sample and not representative of
actual prices.
Transparency Enabling More Selective Behavior
October 2014
Mo Tu We Th Fr
$150 $150 $95
$150 $95 $150 $150 $95
$150 $95 $150 $150 $95
$150 $95 $150 $150 $95
$150 $95 $150 $150 $95
Case in Brief: CarePilot
• Colorado-based company
contracts with 300 providers
to offer available medical
appointments for variety
of procedures
• Providers promote off-peak
appointment times priced at
10% to 30% discount
• Patients must pay up front
through HSA1, credit card, or
PayPal; may submit claim
to insurance later
• Patient searches for needed service
• Available appointments sorted by
provider, location, price, time
• Cardiology services include initial
consultation, stress tests, and echo stress
CarePilot Scheduling Service
Available Appointments and Prices2
Heart Exercise Stress Test, Los Angeles
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
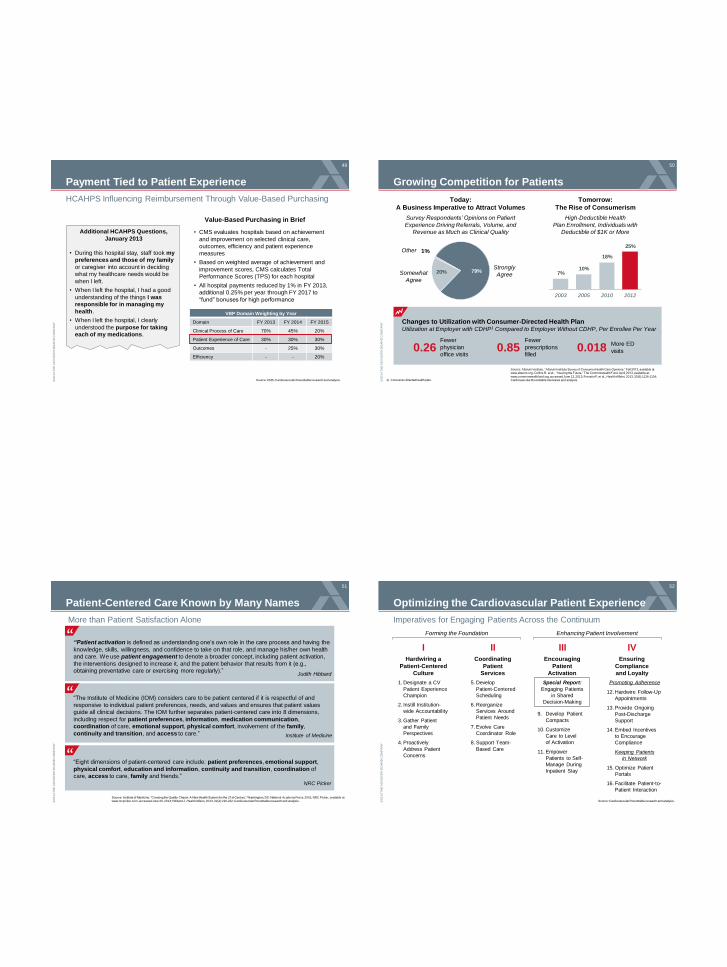
Payment Tied to Patient Experience
49
HCAHPS Influencing Reimbursement Through Value-Based Purchasing
Source: CMS; Cardiovascular Roundtable research and analysis.
Additional HCAHPS Questions,
January 2013
• During this hospital stay, staff took my
preferences and those of my family
or caregiver into account in deciding
what my healthcare needs would be
when I left.
• When I left the hospital, I had a good
understanding of the things I was
responsible for in managing my
health.
• When I left the hospital, I clearly
understood the purpose for taking
each of my medications.
VBP Domain Weighting by Year
Domain FY 2013 FY 2014 FY 2015
Clinical Process of Care 70% 45% 20%
Patient Experience of Care 30% 30% 30%
Outcomes - 25% 30%
Efficiency - - 20%
• CMS evaluates hospitals based on achievement
and improvement on selected clinical care,
outcomes, efficiency and patient experience
measures
• Based on weighted average of achievement and
improvement scores, CMS calculates Total
Performance Scores (TPS) for each hospital
• All hospital payments reduced by 1% in FY 2013,
additional 0.25% per year through FY 2017 to
“fund” bonuses for high performance
Value-Based Purchasing in Brief
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Growing Competition for Patients
50
Source: Altarum Institute, “Altarum Institute Survey of Consumer Health Care Opinions,” Fall 2012, available at: www.altarum.org; Collins R, et al., “Insuring the Future,” The Commonwealth Fund, April 2013, available at:
www.commonwealthfund.org, accessed June 12, 2013; Fronstin P, et al., Health Affairs, 2013, 32(6):1126-1134; Cardiovascular Roundtable interviews and analysis. 1) Consumer-directed health plan.
Today:
A Business Imperative to Attract Volumes
Tomorrow:
The Rise of Consumerism
Survey Respondents’ Opinions on Patient
Experience Driving Referrals, Volume, and
Revenue as Much as Clinical Quality
79% 20%
1%
Strongly
Agree Somewhat
Agree
High-Deductible Health
Plan Enrollment, Individuals with
Deductible of $1K or More
7% 10%
18%
25%
2003 2005 2010 2012
Other
Changes to Utilization with Consumer-Directed Health Plan Utilization at Employer with CDHP1 Compared to Employer Without CDHP, Per Enrollee Per Year
0.26 Fewer
physician
office visits 0.85 0.018
Fewer
prescriptions
filled
More ED
visits
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Patient-Centered Care Known by Many Names
51
More than Patient Satisfaction Alone
Source: Institute of Medicine. “Crossing the Quality Chasm: A New Health System for the 21st Century.” Washington, DC: National Academy Press, 2001; NRC Picker, available at: www.nrcpicker.com, accessed June 30, 2013; Hibbard J, Health Affairs, 2013, 32(2):216-222; Cardiovascular Roundtable research and analysis.
“Patient activation is defined as understanding one’s own role in the care process and having the
knowledge, skills, willingness, and confidence to take on that role, and manage his/her own health
and care. We use patient engagement to denote a broader concept, including patient activation,
the interventions designed to increase it, and the patient behavior that results from it (e.g.,
obtaining preventative care or exercising more regularly).” Judith Hibbard
“The Institute of Medicine (IOM) considers care to be patient centered if it is respectful of and
responsive to individual patient preferences, needs, and values and ensures that patient values
guide all clinical decisions. The IOM further separates patient-centered care into 8 dimensions,
including respect for patient preferences, information, medication communication,
coordination of care, emotional support, physical comfort, involvement of the family,
continuity and transition, and access to care.” Institute of Medicine
“Eight dimensions of patient-centered care include: patient preferences, emotional support,
physical comfort, education and information, continuity and transition, coordination of
care, access to care, family and friends.”
NRC Picker
”
”
”
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Optimizing the Cardiovascular Patient Experience
52
Imperatives for Engaging Patients Across the Continuum
Source: Cardiovascular Roundtable research and analysis.
I II III IV Hardwiring a
Patient-Centered
Culture
Coordinating
Patient
Services
Special Report:
Engaging Patients
in Shared
Decision-Making
Encouraging
Patient
Activation
Ensuring
Compliance
and Loyalty
1. Designate a CV
Patient Experience
Champion
2. Instill Institution-
wide Accountability
3. Gather Patient
and Family
Perspectives
4. Proactively
Address Patient
Concerns
5. Develop
Patient-Centered
Scheduling
6. Reorganize
Services Around
Patient Needs
7. Evolve Care
Coordinator Role
8. Support Team-
Based Care
9. Develop Patient
Compacts
10. Customize
Care to Level
of Activation
11. Empower
Patients to Self-
Manage During
Inpatient Stay
Forming the Foundation Enhancing Patient Involvement
Promoting Adherence
12. Hardwire Follow-Up
Appointments
13. Provide Ongoing
Post-Discharge
Support
14. Embed Incentives
to Encourage
Compliance
Keeping Patients
in Network
15. Optimize Patient
Portals
16. Facilitate Patient-to-
Patient Interaction
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
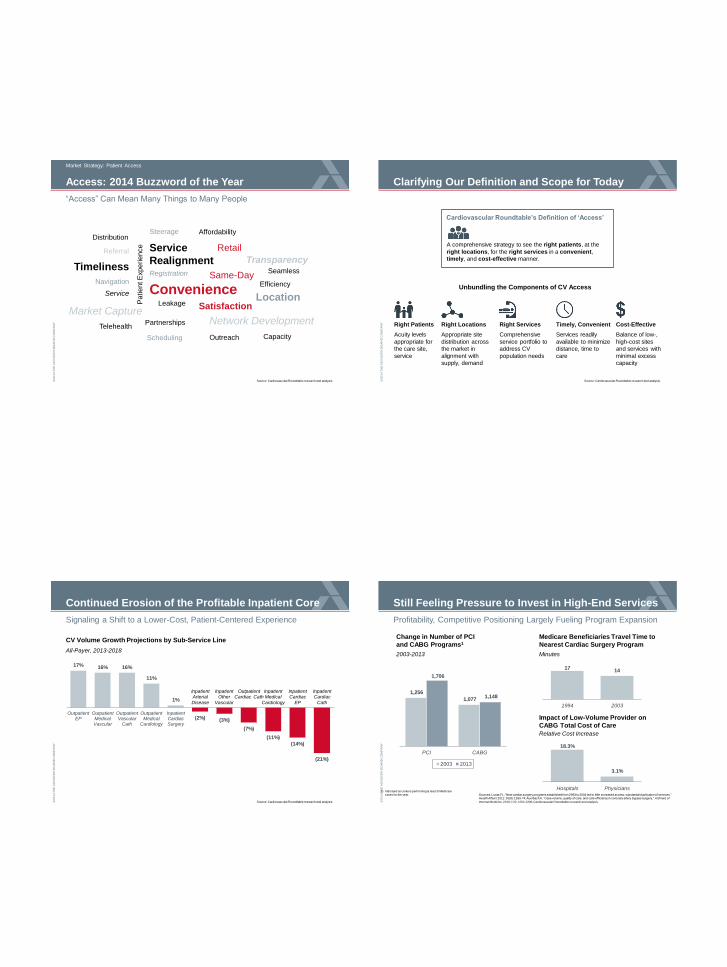
“Access” Can Mean Many Things to Many People
Market Strategy: Patient Access
Access: 2014 Buzzword of the Year
Source: Cardiovascular Roundtable research and analysis.
Timeliness
Market Capture
Convenience
Service
Realignment Registration
Leakage
Same-Day Efficiency
Partnerships Network Development
Navigation
Service
Satisfaction
Scheduling
Referral
Distribution
Retail
Affordability Steerage
Seamless
Telehealth
Location
Transparency
Outreach Capacity
Pa
tie
nt E
xp
erie
nce
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Source: Cardiovascular Roundtable research and analysis.
Clarifying Our Definition and Scope for Today
Cardiovascular Roundtable’s Definition of ‘Access’
A comprehensive strategy to see the right patients, at the
right locations, for the right services in a convenient,
timely, and cost-effective manner.
Unbundling the Components of CV Access
Right Patients
Acuity levels
appropriate for
the care site,
service
Right Locations
Appropriate site
distribution across
the market in
alignment with
supply, demand
Right Services
Comprehensive
service portfolio to
address CV
population needs
Timely, Convenient
Services readily
available to minimize
distance, time to
care
Cost-Effective
Balance of low-,
high-cost sites
and services with
minimal excess
capacity
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Signaling a Shift to a Lower-Cost, Patient-Centered Experience
Continued Erosion of the Profitable Inpatient Core
17% 16% 16%
11%
1%
(2%) (3%)
(7%)
(11%)
(14%)
(21%)
OutpatientEP
OutpatientMedicalVascular
OutpatientVascular
Cath
OutpatientMedical
Cardiology
InpatientCardiacSurgery
CV Volume Growth Projections by Sub-Service Line
All-Payer, 2013-2018
Inpatient Arterial
Disease
Inpatient Other
Vascular
Outpatient Cardiac Cath
Inpatient Medical
Cardiology
Inpatient Cardiac
EP
Inpatient Cardiac
Cath
Source: Cardiovascular Roundtable research and analysis. ©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Profitability, Competitive Positioning Largely Fueling Program Expansion
Sources: Lucas FL, “New cardiac surgery programs established from 2993 to 2004 led to little increased access, substantial duplication of services,” Health Affairs 2011: 30(8): 1569-74; Auerbach A, “Case volume, quality of care, and care efficiency in coronary artery bypass surgery,” Archives of
Internal Medicine, 2010; 170: 1202-1208; Cardiovascular Roundtable research and analysis.
Still Feeling Pressure to Invest in High-End Services
Change in Number of PCI
and CABG Programs1
2003-2013
1,256
1,077
1,706
1,148
PCI CABG
2003 2013
Medicare Beneficiaries Travel Time to
Nearest Cardiac Surgery Program
17 14
1994 2003
Impact of Low-Volume Provider on
CABG Total Cost of Care
18.3%
3.1%
Hospitals Physicians
Minutes
Relative Cost Increase
1) Indicated as centers performing at least 5 Medicare cases for the year.
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
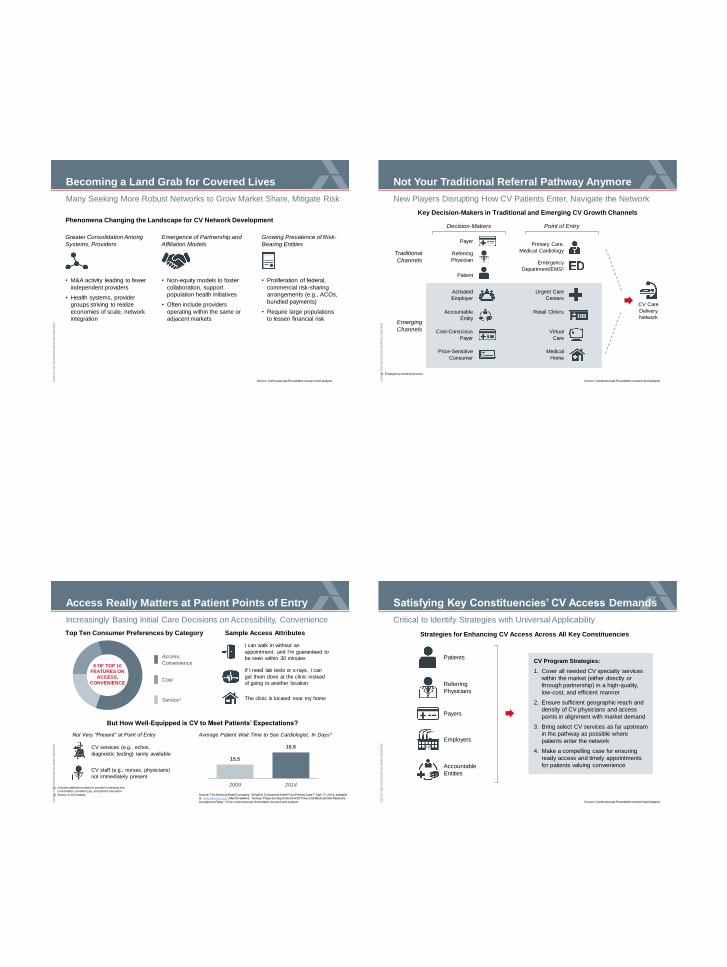
Many Seeking More Robust Networks to Grow Market Share, Mitigate Risk
Source: Cardiovascular Roundtable research and analysis.
Becoming a Land Grab for Covered Lives
Phenomena Changing the Landscape for CV Network Development
Greater Consolidation Among
Systems, Providers
Emergence of Partnership and
Affiliation Models
Growing Prevalence of Risk-
Bearing Entities
• M&A activity leading to fewer
independent providers
• Health systems, provider
groups striving to realize
economies of scale, network
integration
• Non-equity models to foster
collaboration, support
population health initiatives
• Often include providers
operating within the same or
adjacent markets
• Proliferation of federal,
commercial risk-sharing
arrangements (e.g., ACOs,
bundled payments)
• Require large populations
to lessen financial risk
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
New Players Disrupting How CV Patients Enter, Navigate the Network
Source: Cardiovascular Roundtable research and analysis.
Not Your Traditional Referral Pathway Anymore
Traditional
Channels
Key Decision-Makers in Traditional and Emerging CV Growth Channels
Payer
Emerging
Channels
Patient
Decision-Makers
Emergency
Department/EMS1
Point of Entry
Primary Care,
Medical Cardiology
Retail Clinics
Urgent Care
Centers
Virtual
Care
Price-Sensitive
Consumer
Activated
Employer
Medical
Home
Accountable
Entity
Cost-Conscious
Payer
CV Care
Delivery
Network
1) Emergency medical services.
Referring
Physician
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Increasingly Basing Initial Care Decisions on Accessibility, Convenience
Source: The Advisory Board Company, “What Do Consumers Want From Primary Care?” April 17, 2014, available at: www.advisory.com; Merritt Hawkins, “Survey: Physician Appointment Wait Times and Medicaid and Medicare
Acceptance Rates,” 2014; Cardiovascular Roundtable research and analysis.
1) Includes attributes related to provider continuity and coordination, provider type, and patient education.
2) Survey of 15 markets.
Access Really Matters at Patient Points of Entry
Cost
Service1
Access,
Convenience
Top Ten Consumer Preferences by Category
6 OF TOP 10 FEATURES ON
ACCESS,
CONVENIENCE
I can walk in without an
appointment, and I’m guaranteed to
be seen within 30 minutes
If I need lab tests or x-rays, I can
get them done at the clinic instead
of going to another location
The clinic is located near my home
Sample Access Attributes
But How Well-Equipped is CV to Meet Patients’ Expectations?
Not Very “Present” at Point of Entry Average Patient Wait Time to See Cardiologist, In Days2
CV services (e.g., echos,
diagnostic testing) rarely available
CV staff (e.g., nurses, physicians)
not immediately present
15.5
16.8
2009 2014
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Critical to Identify Strategies with Universal Applicability
Source: Cardiovascular Roundtable research and analysis.
Satisfying Key Constituencies’ CV Access Demands
CV Program Strategies:
1. Cover all needed CV specialty services
within the market (either directly or
through partnership) in a high-quality,
low-cost, and efficient manner
2. Ensure sufficient geographic reach and
density of CV physicians and access
points in alignment with market demand
3. Bring select CV services as far upstream
in the pathway as possible where
patients enter the network
4. Make a compelling case for ensuring
ready access and timely appointments
for patients valuing convenience
Strategies for Enhancing CV Access Across All Key Constituencies
Patients
Referring
Physicians
Payers
Employers
Accountable
Entities
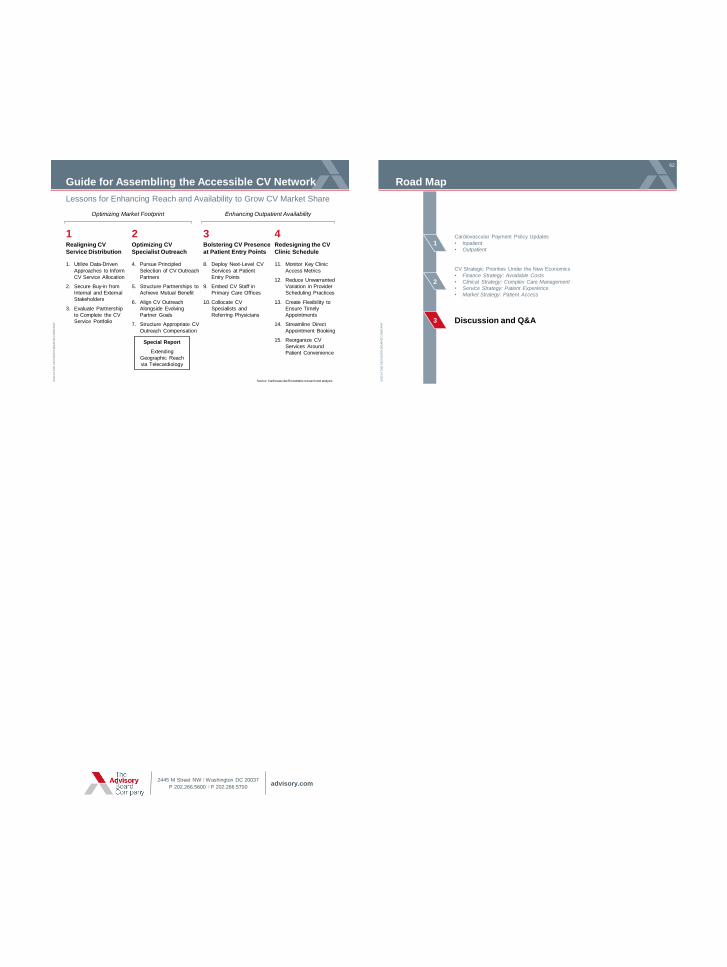
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Guide for Assembling the Accessible CV Network
1. Utilize Data-Driven
Approaches to Inform
CV Service Allocation
2. Secure Buy-in from
Internal and External
Stakeholders
3. Evaluate Partnership
to Complete the CV
Service Portfolio
1 Realigning CV
Service Distribution
4. Pursue Principled
Selection of CV Outreach
Partners
5. Structure Partnerships to
Achieve Mutual Benefit
6. Align CV Outreach
Alongside Evolving
Partner Goals
7. Structure Appropriate CV
Outreach Compensation
2 Optimizing CV
Specialist Outreach
8. Deploy Next-Level CV
Services at Patient
Entry Points
9. Embed CV Staff in
Primary Care Offices
10. Collocate CV
Specialists and
Referring Physicians
3 Bolstering CV Presence
at Patient Entry Points
11. Monitor Key Clinic
Access Metrics
12. Reduce Unwarranted
Variation in Provider
Scheduling Practices
13. Create Flexibility to
Ensure Timely
Appointments
14. Streamline Direct
Appointment Booking
15. Reorganize CV
Services Around
Patient Convenience
4 Redesigning the CV
Clinic Schedule
Source: Cardiovascular Roundtable research and analysis.
Optimizing Market Footprint Enhancing Outpatient Availability
Special Report
Extending
Geographic Reach
via Telecardiology
Lessons for Enhancing Reach and Availability to Grow CV Market Share
©2
01
4 T
HE
AD
VIS
OR
Y B
OA
RD
CO
MP
AN
Y
Road Map
2
3
1
62
CV Strategic Priorities Under the New Economics
• Finance Strategy: Avoidable Costs
• Clinical Strategy: Complex Care Management
• Service Strategy: Patient Experience
• Market Strategy: Patient Access
Discussion and Q&A
Cardiovascular Payment Policy Updates
• Inpatient
• Outpatient
2445 M Street NW I Washington DC 20037
P 202.266.5600 I F 202.266.5700 advisory.com