Embed Size (px)
DESCRIPTION
great source to make ur knowledge bout cardiology
Citation preview
CARDIOMYOPATHY
1
Definition
• Disorders of the cardiac muscle of unknown aetiology
• “A primary disorder of the heart muscle that causes abnormal myocardial performance and is not the result of disease or dysfunction of other cardiac structures … myocardial infarction, systemic hypertension, valvular stenosis or regurgitation”
2
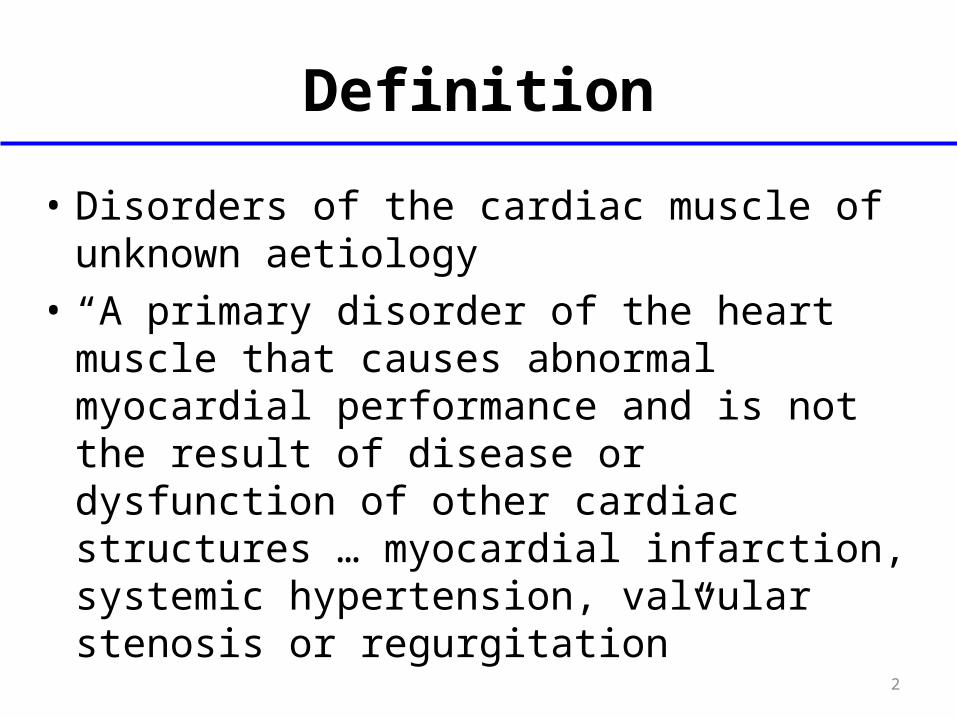
Classifications
Braunwald 8th ed, 2008.3
Functional Classification• Dilatated (congestive, DCM, IDC)
– ventricular enlargement and syst dysfunction
• Hypertrophic (IHSS, HCM, HOCM)– inappropriate myocardial hypertrophy
in the absence of HTN or aortic stenosis
• Restrictive (infiltrative)– abnormal filling and diastolic function
4
IDIOPATHIC DILATED CARDIOMYPATHYEPIDEMIOLOGY
• ANNUAL INCIDENCE 5-8/100,000
• PREVELANCE 36/ 100,000
• INCREASED RISK ASSOCIATED WITH:– MALE GENDER– BLACK RACE– HYPERTENSION– CHRONIC BETA-AGONIST USE
5
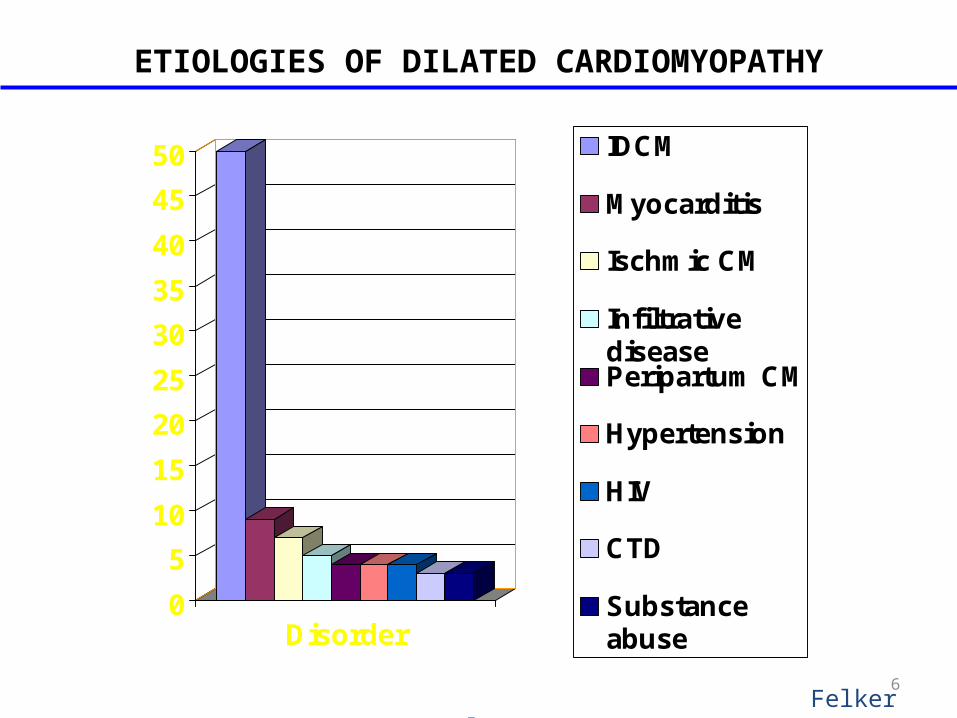
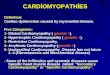
ETIOLOGIES OF DILATED CARDIOMYOPATHY
0
5
10
15
20
25
30
35
40
45
50
Disorder
IDCM
Myocarditis
Ischmic CM
InfiltrativediseasePeripartum CM
Hypertension
HIV
CTD
Substanceabuse
Felker et al NEJM 20006
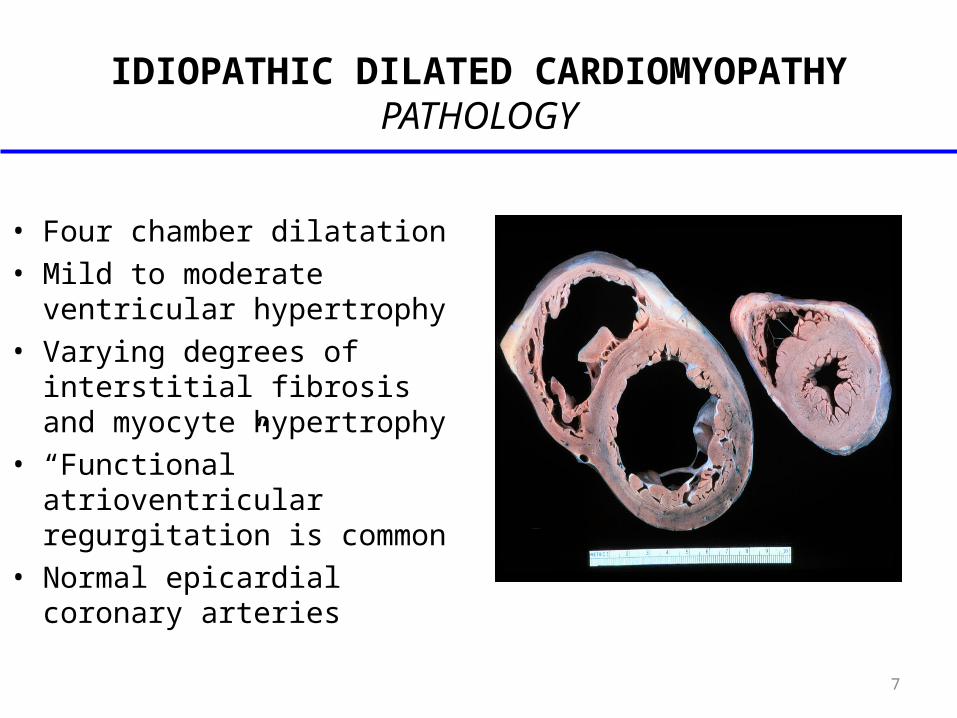
IDIOPATHIC DILATED CARDIOMYOPATHYPATHOLOGY
• Four chamber dilatation• Mild to moderate ventricular
hypertrophy• Varying degrees of interstitial
fibrosis and myocyte hypertrophy
• “Functional” atrioventricular regurgitation is common
• Normal epicardial coronary arteries
7
IDIOPATHIC DILATED CARDIOMYOPATHYPATHOGENESIS
• Familial/genetic factors• Viral myocarditis and cytotoxic insults• Immunologic abnormalities• Beta-receptor auto-antibodies
– Abnormal T-cell function
• Metabolic, energetic, and contractile abnormalities– Ca2+-ATPase– Myofibrillar ATPase– Creatine Kinase
8
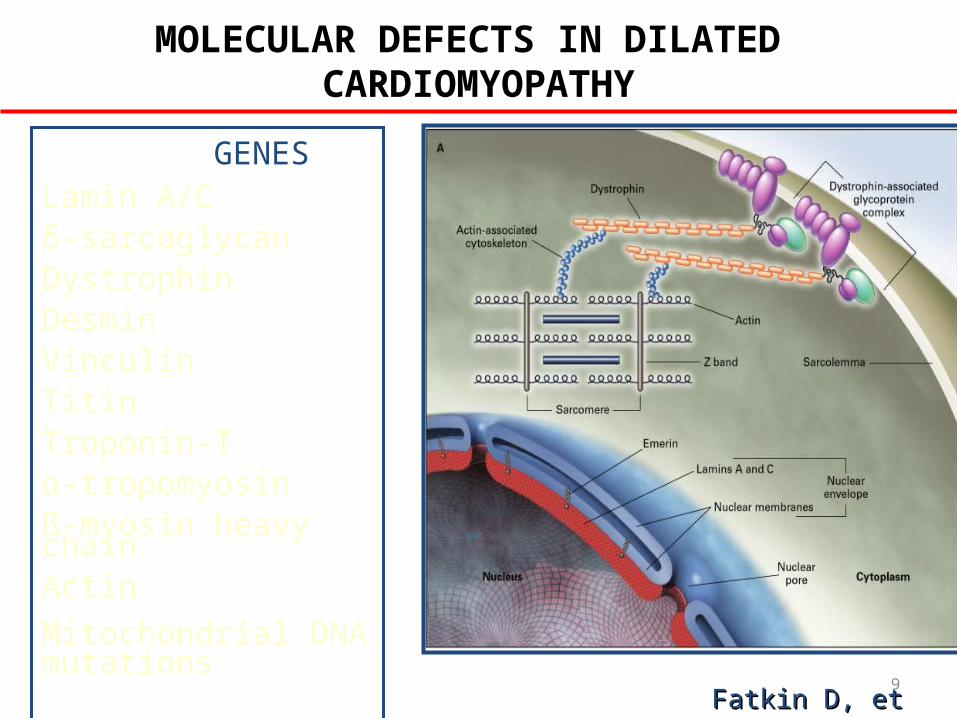
MOLECULAR DEFECTS IN DILATED CARDIOMYOPATHY
Fatkin D, et al. NEJM 1999;341Fatkin D, et al. NEJM 1999;341
GENESLamin A/Cδ-sarcoglycanDystrophinDesminVinculinTitinTroponin-Tα-tropomyosinß-myosin heavy chainActin
Mitochondrial DNA mutations
9
IDIOPATHIC DILATED CARDIOMYPATHYCLINICAL PRESENTATIONS
• Heart failure symptoms 75%-85%• Anginal chest pain 8%-20%
• Emboli (systemic or pulmonary) 1%-4%• Syncope <1%• Sudden cardiac death <1%
10
IDIOPATHIC DILATED CARDIOMYPATHYCARDIAC IMAGING
• CXR : enlargement of cardiac silhoutte• ECG : evidence of old MCI, conduction abnormalities e.g
LBBB, LV hypertrophy, AF or VT• 24-hour ambulatory ECG (Holter)
– lightheadedness, palpitation, syncope
• Two-dimensional echocardiogram or Radionuclide ventriculography to assess : LV ejection fraction, end-diastolic volume, diastolic function
• Cardiac catheterization– age >40, ischemic history, high risk profile, abnormal ECG
11
IDCM:PROGNOSTIC FEATURES
• VENTRICULOGRAPHIC FINDINGS– Degree of impairment in LVEF– Extent of left ventricular enlargement– Coexistent right ventricular dysfunction– Ventricular mass/volume ratio– Global wall motion abnormalities– Left ventricular sphericity
• CLINICAL FINDINGS– Favorable prognosis: NYHA < IV, younger age, female
sex
– Poor prognosis: Syncope, persistent S3 gallop, right-sided heart failure, AV or bundle branch block, hyponatremia, troponin elevation, increased BNP, maximum oxygen uptake < 12 mg/kg/min
12
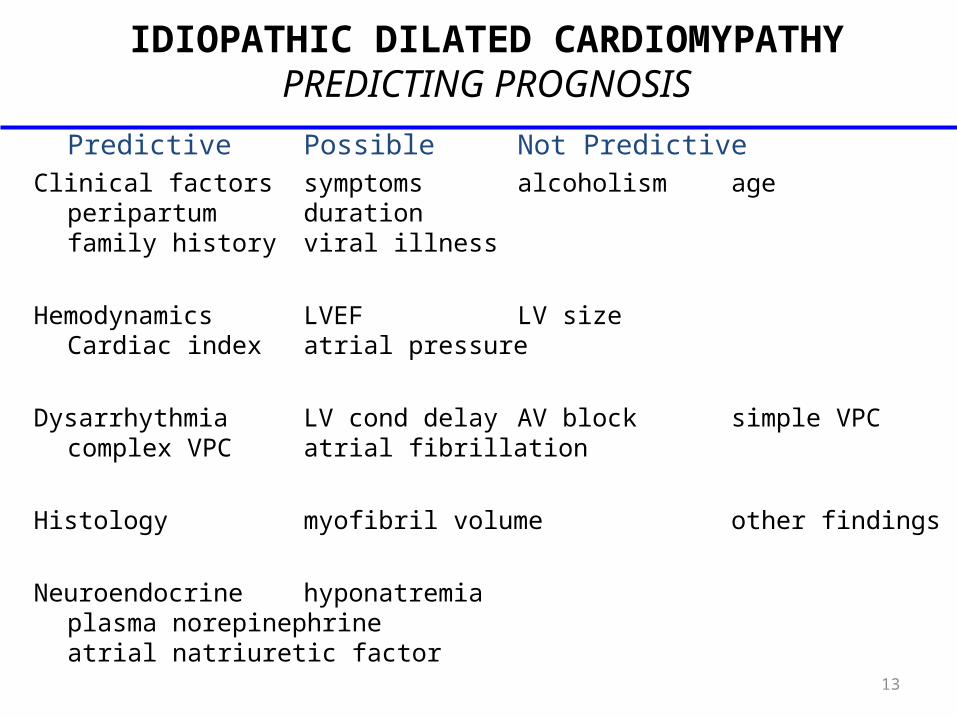
IDIOPATHIC DILATED CARDIOMYPATHYPREDICTING PROGNOSIS
Predictive Possible Not PredictiveClinical factors symptoms alcoholism age
peripartum durationfamily history viral illness
Hemodynamics LVEF LV sizeCardiac index atrial pressure
Dysarrhythmia LV cond delay AV block simple VPCcomplex VPC atrial fibrillation
Histology myofibril volume other findings
Neuroendocrine hyponatremiaplasma norepinephrineatrial natriuretic factor 13
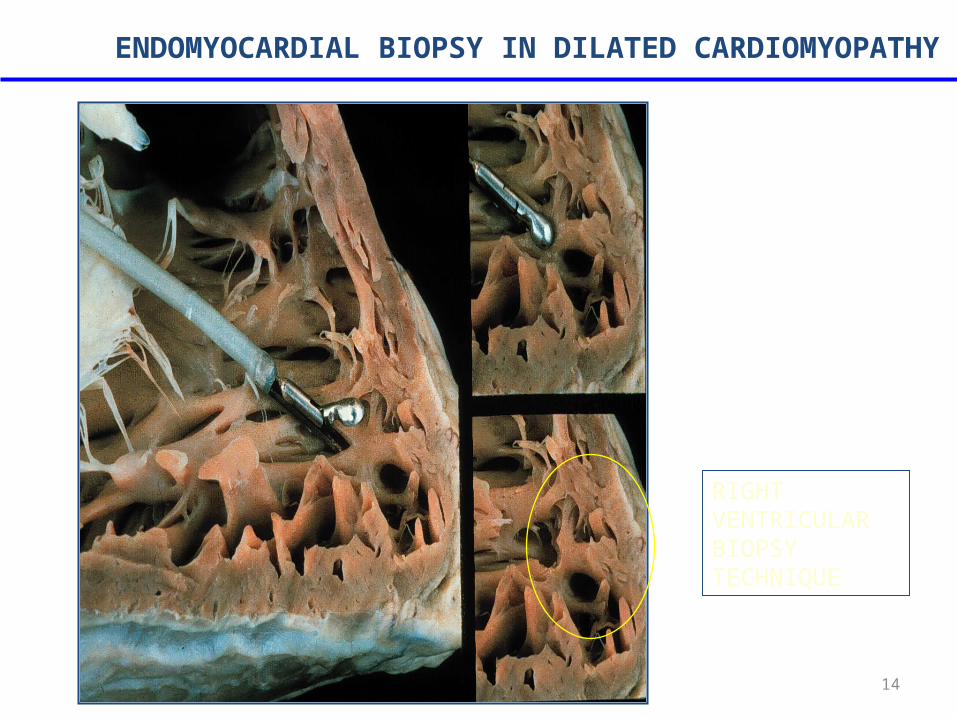
RIGHT VENTRICULAR BIOPSY TECHNIQUE
ENDOMYOCARDIAL BIOPSY IN DILATED CARDIOMYOPATHY
14
INDICATIONS FOR ENDOMYOCARDIAL BIOPSY
• Acute dilated cardiomyopathy with refractory heart failure symptoms
• Rapidly progressive ventricular dysfunction in an unexplained cardiomyopathy of recent onset
• New onset cardiomyopathy with recurrent ventricular tachycardia or high grade heart block
• Heart failure in the setting of fever, rash, and peripheral eosinophilia
• Dilated cardiomyopathy in setting of systemic diseases known to affect the myocardium (systemic lupus erythematosus, polymyositis, sarcoidosis)
Wu LA, et al. Mayo Clin Proc 2001;76:1030-815
IDIOPATHIC DILATED CARDIOMYOPATHYMANAGEMENT
• Limit activity based on functional status• salt restriction of a 2-g Na+ (5g NaCl) diet• fluid restriction for significant low Na+• initiate medical therapy
– ACE inhibitors, diuretics– digoxin, carvedilol– hydralazine / nitrate combination
16
IDIOPATHIC DILATED CARDIOMYOPATHYMANAGEMENT
• consider adding ß-blocking agents if symptoms persists
• anticoagulation for EF <30%, history of thromboemoli, presence of mural thrombi
• intravenous dopamine, dobutamine and/or phosphodiesterase inhibitors
• cardiac transplantation
17
HYPERTROPHIC CARDIOMYOPATHY
• First described by the French and Germans around 1900
• uncommon with occurrence of 0.02 to 0.2%• a hypertrophied and non-dilated left ventricle in
the absence of another disease
• small LV cavity, asymmetrical septal hypertrophy (ASH), systolic anterior motion of the mitral valve leaflet (SAM)
18
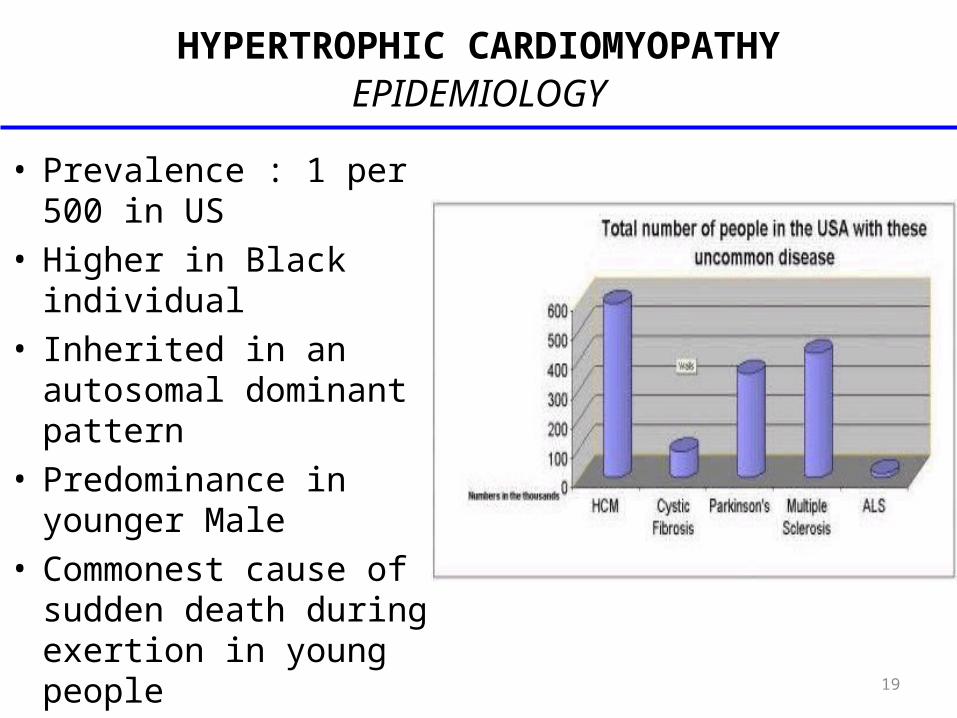
HYPERTROPHIC CARDIOMYOPATHY EPIDEMIOLOGY
• Prevalence : 1 per 500 in US
• Higher in Black individual• Inherited in an
autosomal dominant pattern
• Predominance in younger Male
• Commonest cause of sudden death during exertion in young people
19
HYPERTROPHIC CARDIOMYOPATHY PATHOGENESIS
• Misconception that outflow tract obstruction• Impaired ventricular compliance as
consequence of inappropriate myocardial hypertrophy
20
HYPERTROPHIC CARDIOMYOPATHY PATOPHYSIOLOGY
• Systole– dynamic outflow tract gradient
• Diastole– impaired diastolic filling, filling pressure
• Myocardial ischemia– muscle mass, filling pressure, O2 demand– vasodilator reserve, capillary density– abnormal intramural coronary arteries– systolic compression of arteries
21
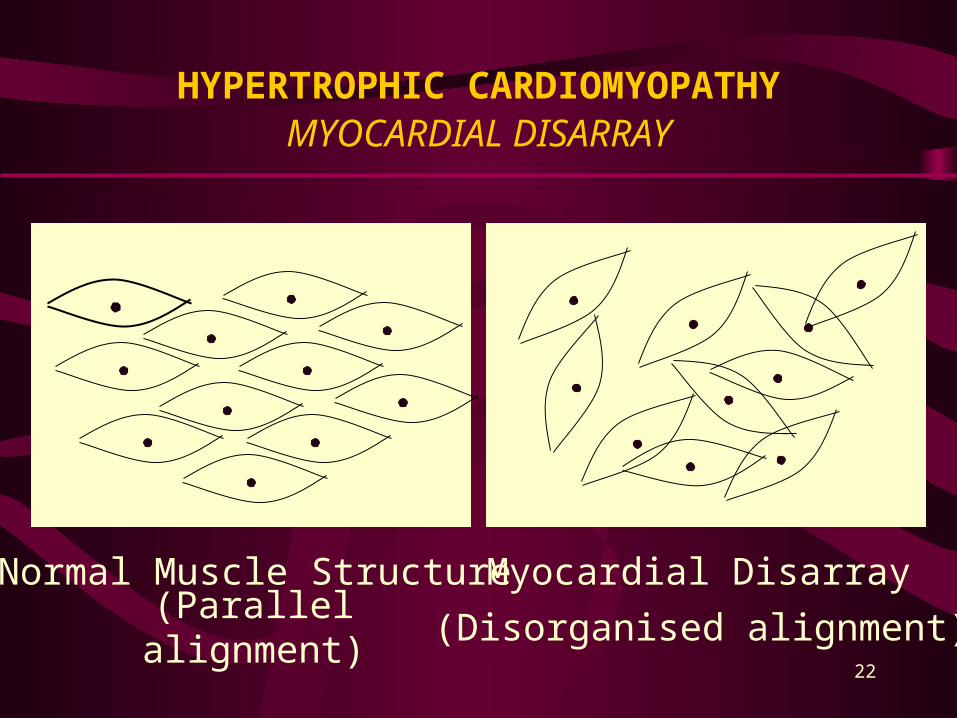
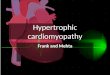
HYPERTROPHIC CARDIOMYOPATHY MYOCARDIAL DISARRAY
Normal Muscle Structure Myocardial Disarray
(Parallel alignment) (Disorganised alignment)22
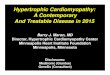
HYPERTROPHIC CARDIOMYOPATHY TYPES
• HCM or HOCM• Asymmetric septal (ASH) - without obstruction• Asymmetric septal (ASH) - with obstruction• Symmetric hypertrophy - concentric• Apical hypertrophy
23
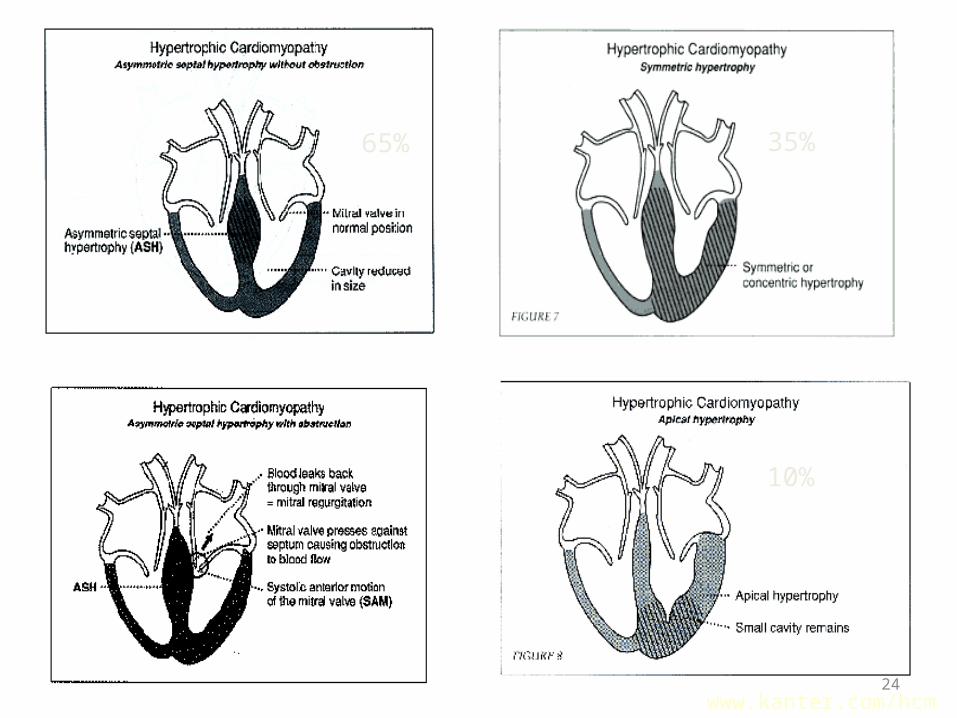
65% 35%
10%
www.kanter.com/hcm24
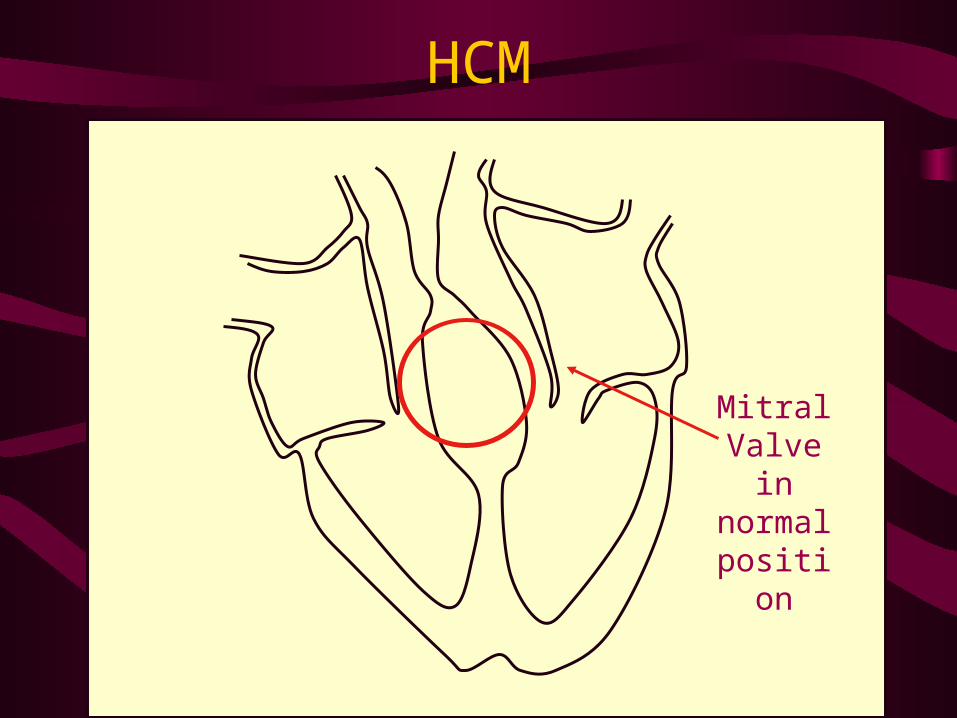
HCM
Mitral Valve in normal position
25
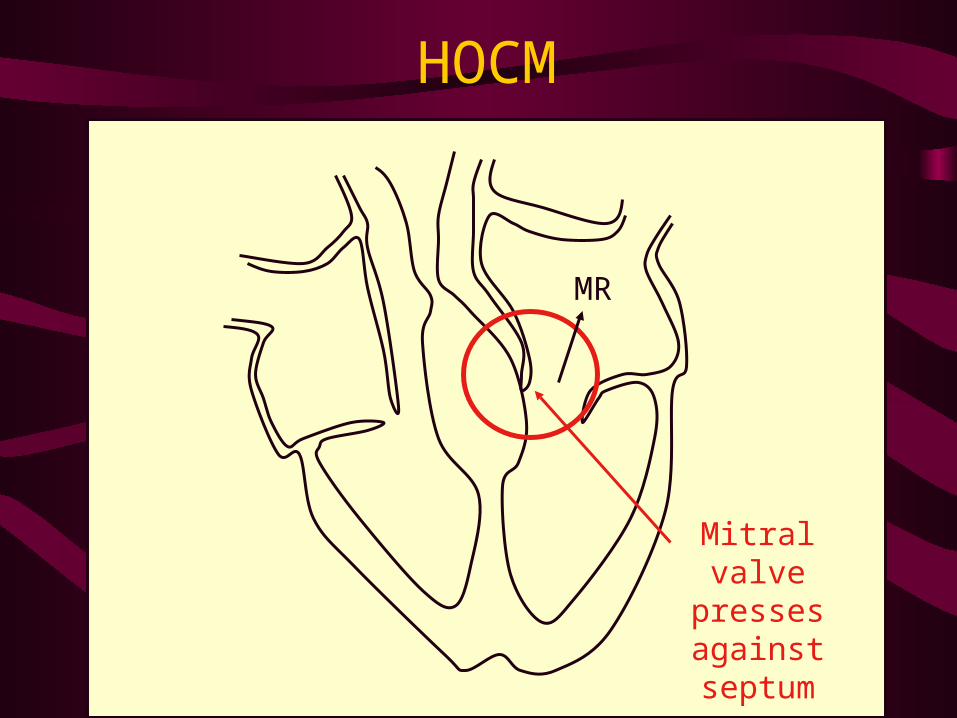
HOCM
Mitral valve presses against septum
MR
26
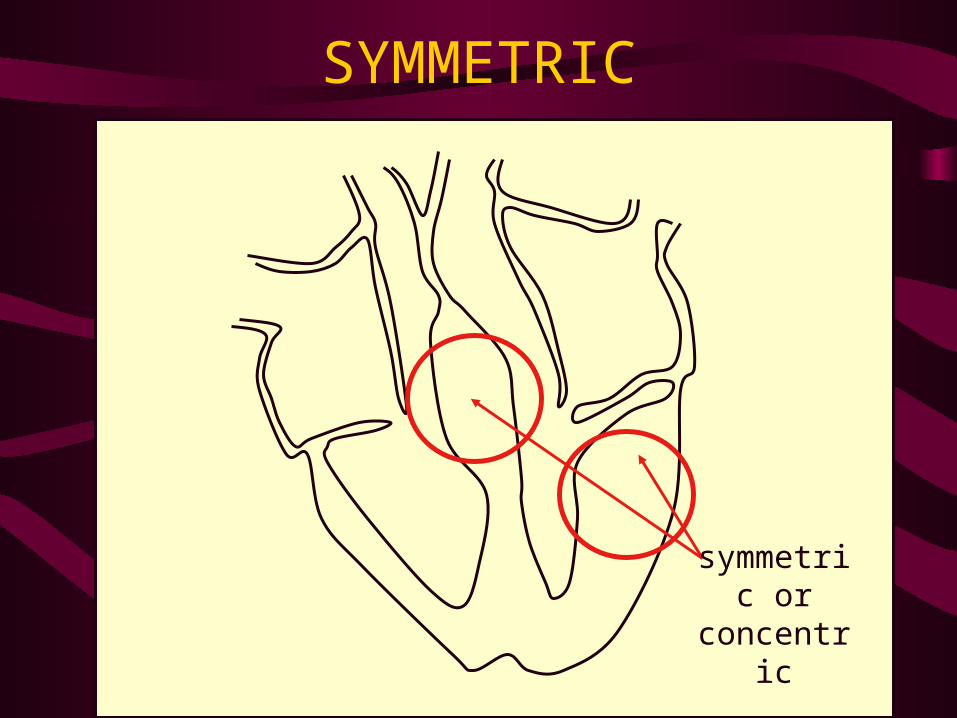
SYMMETRIC
symmetric or
concentric27
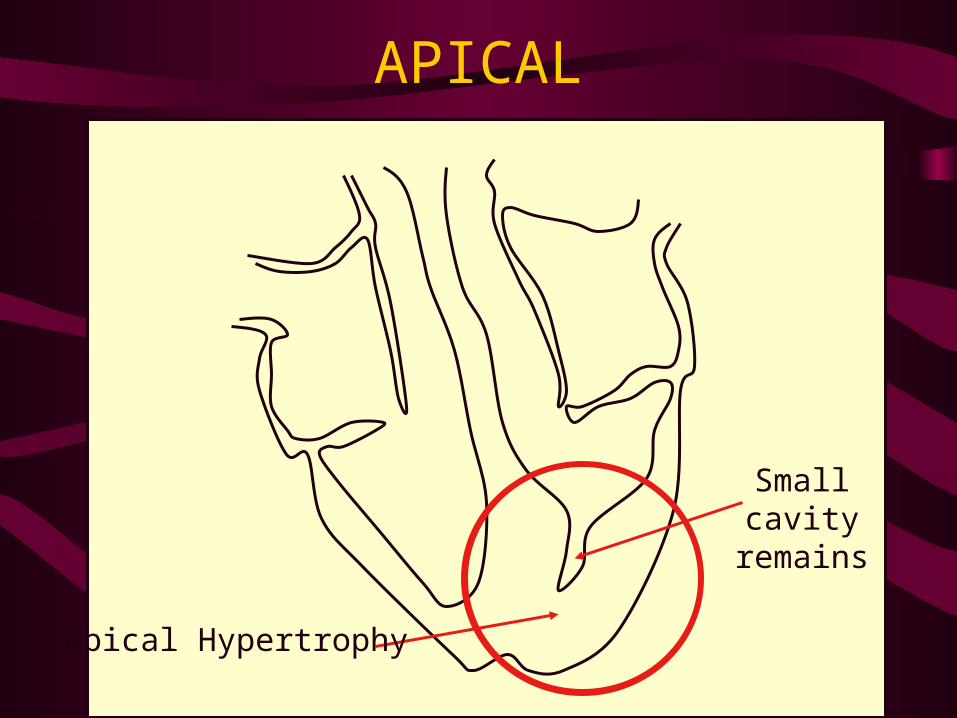
APICAL
Small cavity
remains
Apical Hypertrophy28
HYPERTROPHIC CARDIOMYOPATHY CLINICAL PRESENTATIONS
• Some patients asymptomatic• Symptomatic
– dyspnea in 90%– angina pectoris in 75%– fatigue, pre-syncope, syncope
risk of SCD in children and adolescents– palpitation, PND, CHF, dizziness less frequent
• Costello syndrome• ECG : giant negative T waves in the precordial leads• Spade like appearence
29
HYPERTROPHIC CARDIOMYOPATHY PHYSICAL EXAMINATIONS
• Carotid impulse• Prominent a waves of JV pulse• Outflow murmur• Mitral regurgitation• Atrial fibrilation• Embolic phenomena• Heart Failure symptoms
30
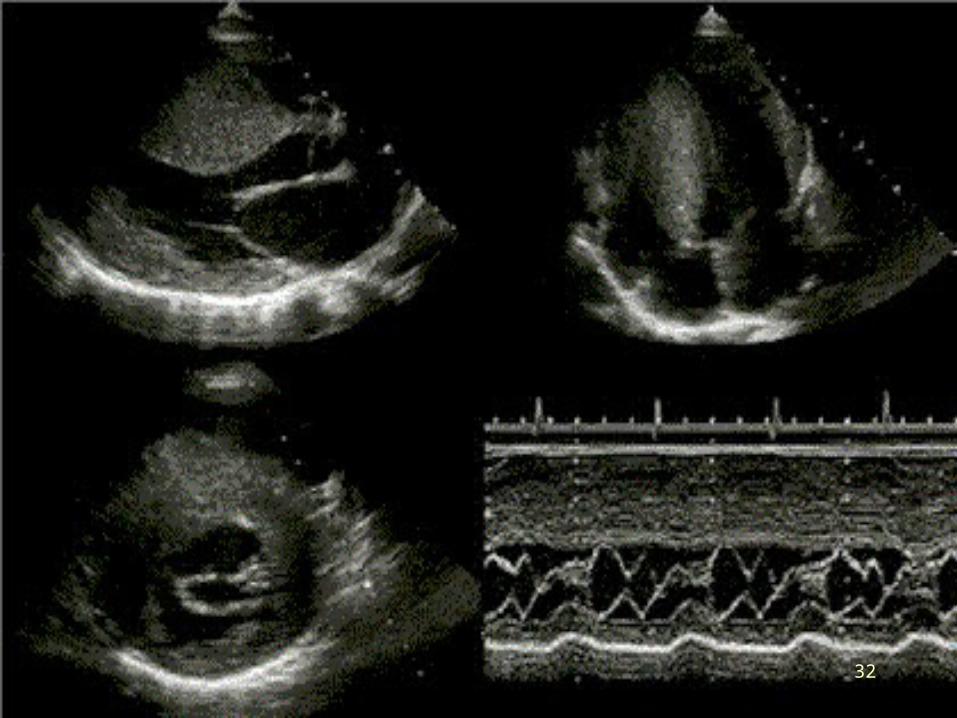
HYPERTROPHIC CARDIOMYOPATHY DIAGNOSTIC APPROACH
ECG :• Abnormalities of ST segment and T waves• LVH• QRS complex tallest at mid precordial leads
Echo :• Concentric caused by pressure overload e.g. AS• Eccentric caused by volume overload e.g MR, AR• Septal thickening wall• Mitral valve anterior leafleat may be enlarged• MR
31
32
HYPERTROPHIC CARDIOMYOPATHY DIFFERENTIAL DIANOSIS
• Left Ventricular hypertrophy• Outflow obstruction secondary to valvular
heart disease e.g AS, coarctation of aorta and infiltrative disorder of myocardium
• Pattern hypertrophy in hypertension is concentric meanwhile in HCM is distinctive
33
HCM vs Aortic Stenosis
HCM Fixed Obstruction
carotid pulse spike and dome parvus et tardusmurmur radiate to carotids
valsalva, standing squatting, handgrip passive leg elevation
systolic thrill 4th left interspace 2nd right interspacesystolic click absent present
34
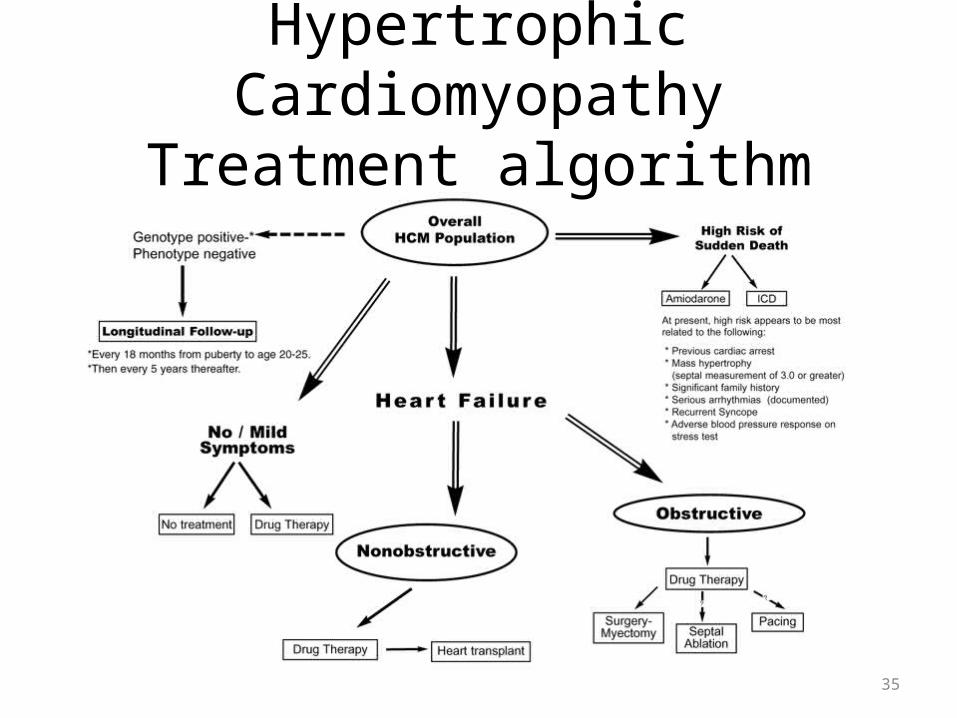
Hypertrophic CardiomyopathyTreatment algorithm
35
HYPERTROPHIC CARDIOMYOPATHY MANAGEMENT
Medical management:• B-blockers• CCB, verapamil• Disopyramide in decreasing outflow gradient• Endocarditis prophylaxisPermanent PacingI C D Alcohol ablation of the septum• Injected 1-4 ml absolute alcohol into the septal
perforator branch of LAD
36
HYPERTROPHIC CARDIOMYOPATHY MANAGEMENT
Surgical therapy• Subaortic ventricular myotomy• Resection myocardium from proximal septum to
beyond mitral leafleatAdvantage :• Low mortality• Reduced symptoms• Improved functional capacityHeart transplantation
37
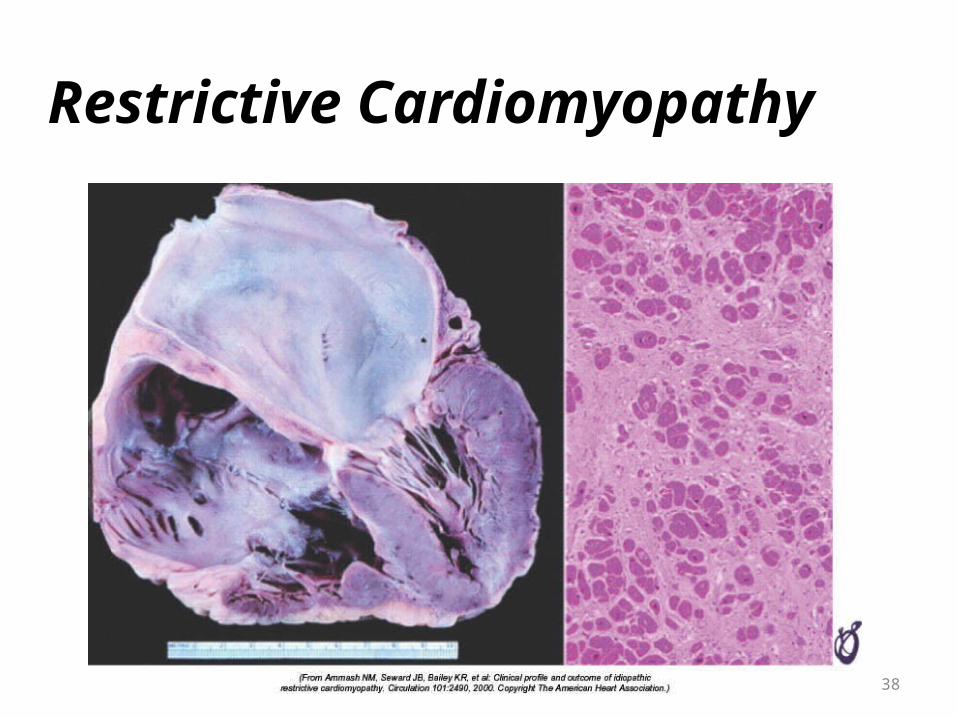
Restrictive Cardiomyopathy
38
RESTRICTIVE CARDIOMYOPATHY
• Hallmark: abnormal diastolic function• rigid ventricular wall with impaired
ventricular filling• importance lies in its differentiation from
operable constrictive pericarditis • Characteristics by : Abnormal compliance of
the left ventricle and short relaxation time
39
RESTRICTIVE CARDIOMYOPATHY ETIOLOGY
•Non infiltrative cause Associated with patchy endomyocardial fibrosis, increased cardiac mass and enlarged atria•Infiltrative cause
Amyloidisis, primary caused by the deposition of amyloid protein. Secondary caused by production nonimunoglobulin protein and termed AA
•Sarcoidosis•Endomyocardial fibrosis
40
RESTRICTIVE CARDIOMYOPATHY EXCLUSION “GUIDELINES”
• LV end-diastolic dimensions 7 cm• Myocardial wall thickness 1.7 cm• LV end-diastolic volume 150 mL/m2• LV ejection fraction < 20%
41
RESTRICTIVE CARDIOMYOPATHY CLASSIFICATION
• Idiopathic• Myocardial
1. Noninfiltrative– Idiopathic– Scleroderma
2. Infiltrative– Amyloid– Sarcoid– Gaucher disease– Hurler disease
3. Storage Disease– Hemochromatosis– Fabry disease– Glycogen storage
• Endomyocardial– endomyocardial fibrosis– Hyperesinophilic synd– Carcinoid– metastatic malignancies– radiation, anthracycline
42
RESTRICTIVE CARDIOMYOPATHY CLINICAL PRESENTATIONS
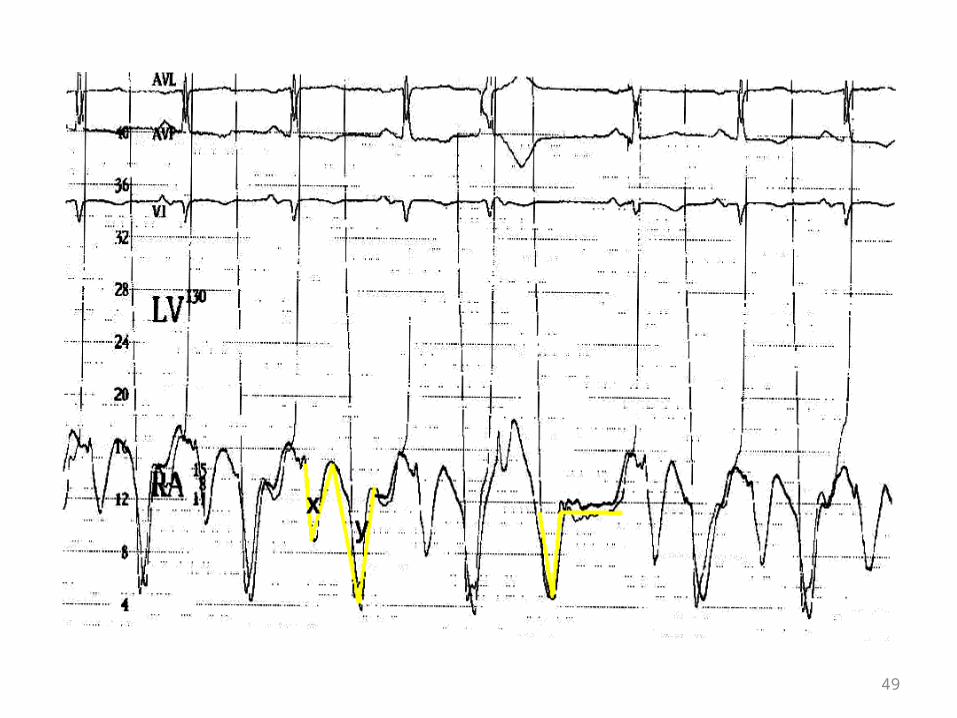
• Symptoms of right and left heart failure• Angina if CAD involve• Jugular Venous Pulse
– prominent x and y descents• Echo-Doppler
– abnormal mitral inflow pattern– prominent E wave (rapid diastolic filling)– reduced deceleration time ( LA pressure)
43
RESTRICTIVE CARDIOMYOPATHY DIAGNOSTIC APPROACH
ECG :• Low voltage• Poor R wave progression• Pseudoinfarction pattern in the inferior leads• P pulmonal If pulmonary hipertension present• Atrial arrhythmia esp fibrillation• Sick sinus syndrome is common• Ventricular Tachiarrhytmia
44
RESTRICTIVE CARDIOMYOPATHY DIAGNOSTIC APPROACH
Chest X-ray• Normal CTR and enlarged atria• Enlarged right ventricle may be seen if pulmonary
hypertension presentEcho• Severe biatrial enlargement• Thickened LV wallsCardiac nuclear imagingCT scan and MRICardiac catheterization and endomyocardial biopsy
45
• No satisfactory medical therapy• Drug therapy must be used with caution
– diuretics for extremely high filling prssures– vasodilators may decrease filling pressure– ? Calcium channel blockers to improve diastolic
compliance– digitalis and other inotropic agents are not
indicated
RESTRICTIVE CARDIOMYOPATHY MANAGEMENT
46
RESTRICTIVE CARDIOMYOPATHY DIFFERENTIAL DIAGNOSIS
• Constrictive pericarditis• Chronic RV infarction• RV dysfunction from RV pressure or RV
volume overload• Instrinsic RV myocardial disease• Tricuspid valve disease
47
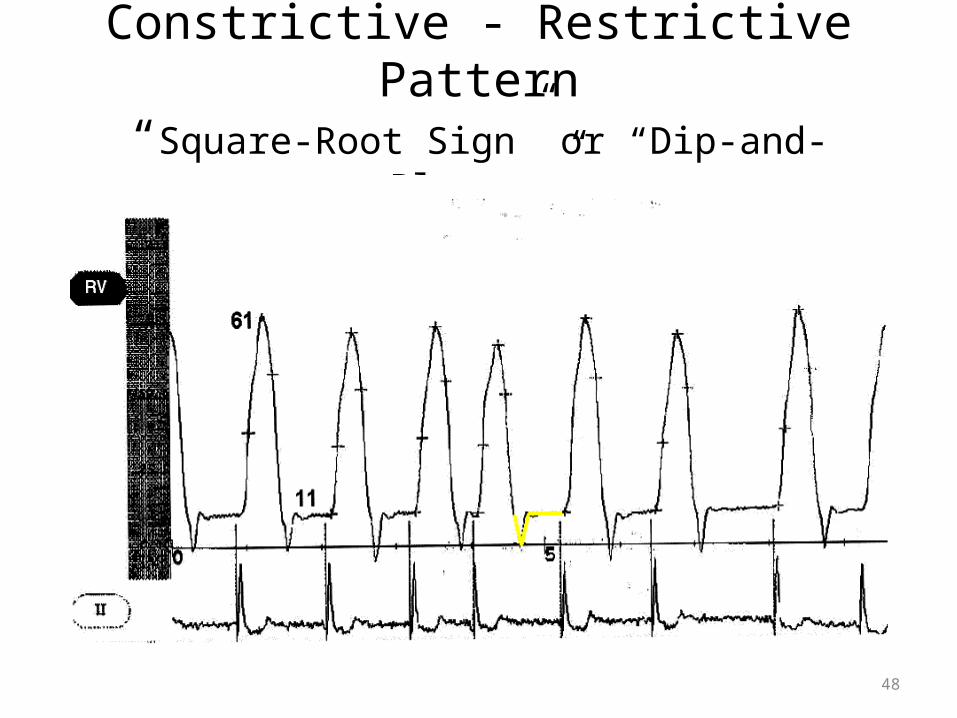
Constrictive - Restrictive Pattern“Square-Root Sign” or “Dip-and-Plateau”
48
49
RESTRICTIVE CARDIOMYOPATHY Restriction vs Constriction
History provide can important clues• Constrictive pericarditis
– history of TB, trauma, pericarditis, sollagen vascular disorders
• Restrictive cardiomyopathy– amyloidosis, hemochromatosis
• Mixed– mediastinal radiation, cardiac surgery
50
MYOCARDITIS
• Inflammation of myocardium• Can be result of systemic disorder or
infectious agent• Viral-Coxsackie B, echovirus, influenza,
parainfluenza, Epstein-Bar, and HIV• Bacterial-C. Diptheria, N. meningitidis, M.
pneumonia, and beta-hemolytic strep• Frequently accompanied with pericarditis
51
MYOCARDITISClinical Presentations
• Fever, tachycardia out of proportion to fever, myalgias, headache,rigors
• Chest pain due to coexisting pericarditis• Pericardial friction rub• Severe cases may have CHF symptoms
52
MYOCARDITISCLINICAL PRESENTATIONS
• EKG-nonspecific changes, av block, prolonged QRS suration, or ST elevation(with pericarditis)
• CXR-Normal• Cardiac Enzymes- may be elevated• Differentail-ischemia or infarct, valvular
disease, and sepsis
53
MYOCARDITIS
MANAGEMENT • Supportive care• Blood cultures• Antibiotics for bacterial cause• Watch for signs of progressive heart failure
54
Pericardial disease
55
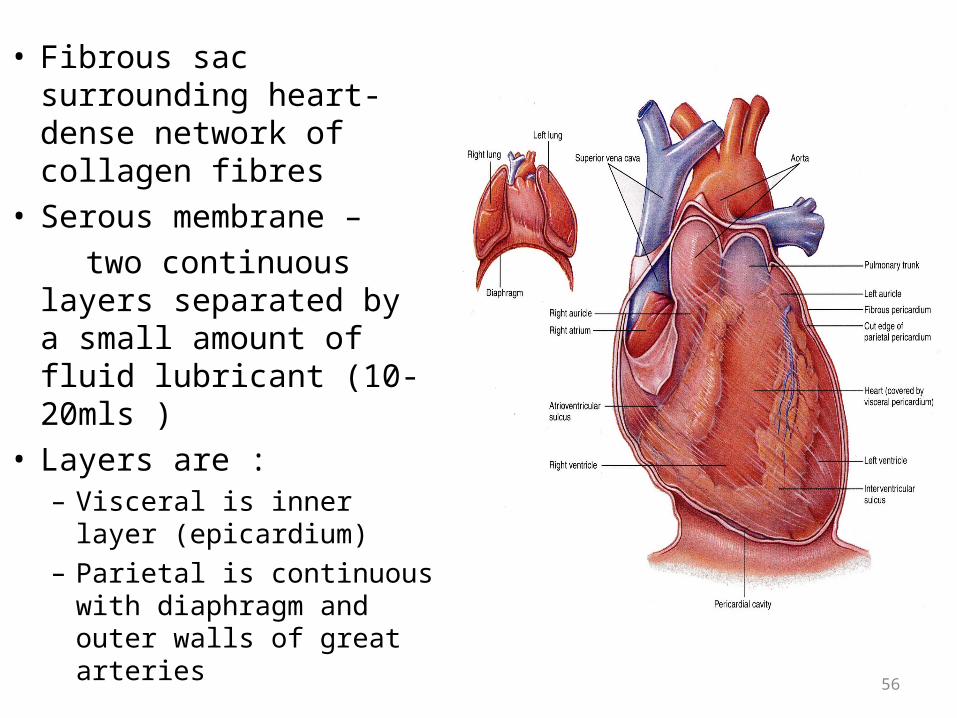
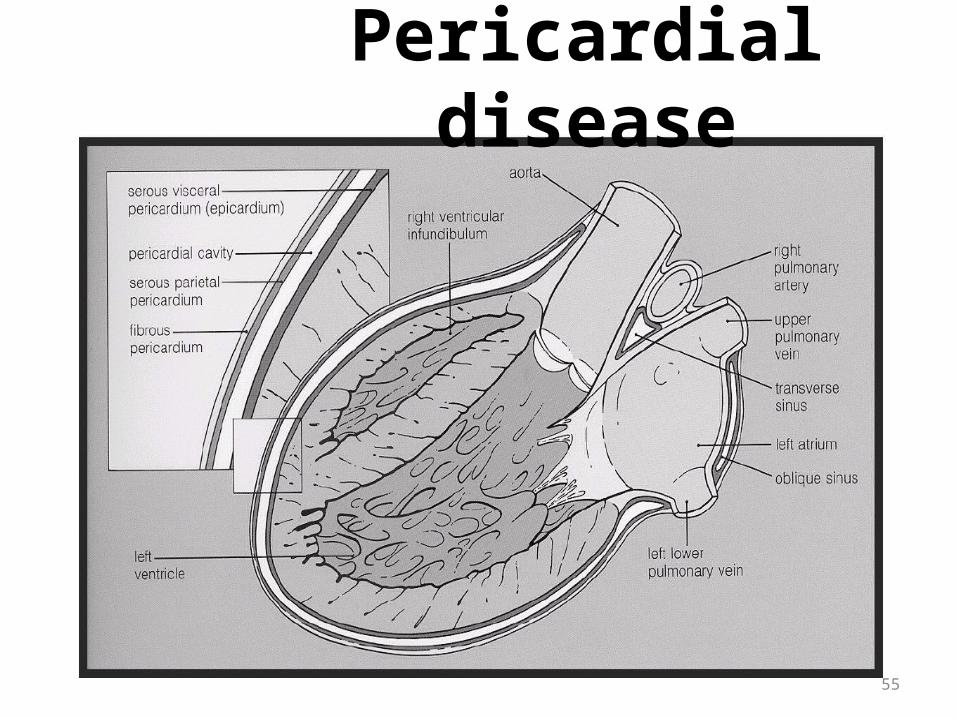
• Fibrous sac surrounding heart-dense network of collagen fibres
• Serous membrane – two continuous layers
separated by a small amount of fluid lubricant (10-20mls )
• Layers are :– Visceral is inner layer
(epicardium)– Parietal is continuous with
diaphragm and outer walls of great arteries
56
ACUTE PERICARDITIS
• Loose visceral pericardium and dense parietal pericardium surround heart
• Pericardial space may contain up to 50ml normally
• Etiologies of acute pericarditis-viral, bacterial, fungal, malignancy, drugs, radiation, connective tissue disorder, uremia, myxedema, post-MI, or idiopathic
57
ACUTE PERICARDITIS ETIOLOGY
Idiopathic – 86%• Infective (viral or bacterial) – 7%• Following a myocardial infarction or cardiac surgery
(Dressler’s syndrome)• Radiation therapy• Neoplastic disease (commonly lung or breast) – 6%• Connective tissue disease
Figures from Permanyer-Miralda et al 198558
ACUTE PERICARDITIS CLINICAL PRESENTATIONS
• Retrosternal chest pain – sharp or stabbing pain worse on insp and lying flat
• Friction rub (high pitched scratching noise)
• Raised jugular venous pressure
59
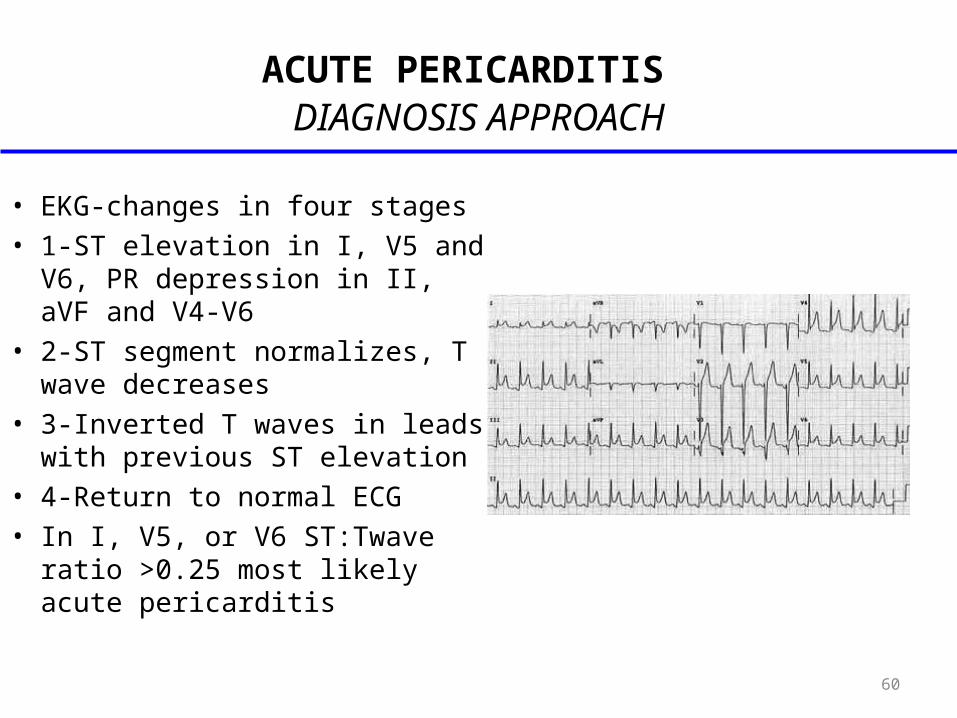
ACUTE PERICARDITIS DIAGNOSIS APPROACH
• EKG-changes in four stages• 1-ST elevation in I, V5 and V6, PR
depression in II, aVF and V4-V6• 2-ST segment normalizes, T wave
decreases• 3-Inverted T waves in leads with
previous ST elevation• 4-Return to normal ECG• In I, V5, or V6 ST:Twave ratio
>0.25 most likely acute pericarditis
60
ACUTE PERICARDITIS DIAGNOSIS APPROACH
• Chest Xray-normal and can help r/o other disease
• Other tests of value-CBC, bun and cr, streptococcal serology, viral serologies, antinuclear/anti-DNA abs, thyroid function, ESR, Cardiac Enzymes
61
ACUTE PERICARDITIS MANAGEMENT
• Search for the underlying disease• No good evidence from randomised controlled trials• Patients require bed rest• NSAID (aspirin, indomethacin) are generally accepted
as effective for relieving symptoms of chest pain• NSAID ketorolac tromethamine rapid results• Colchicine may be a useful adjunct in those who do
not respond to NSAIDs alone
62
ACUTE PERICARDITIS PROGNOSIS
• Pericarditis is usually a benign disorder• Diagnosis relates to underlying cause• But any cause can lead to an effusion and
tamponade which can lead to death• Pericarditis can also progress to pericardial
constriction and heart failure
63
CONSTRICTIVE PERICARDITIS
• Occurs when fibrous thickening and loss of elasticity interfere with diastolic filling
• Cardiac trauma, pericardiotomy, intrapericardial hemmorhage, fungal or bacterial pericarditis, uremic pericarditis are most common causes
64
CONSTRICTIVE PERICARDITIS CLINICAL PRESENTATIONS
• Sx’s gradually develop-mimics restrictive CM- CHF, DOE, and decreased exercise tolerance
• Chest pain, orthopnea and pnd are uncommon
• Exam-Pedal edema, hepatomegaly, ascites, jvd, and Kussmaul’s sign.
• Pericardial “knock”-early diastolic sound may be heard at apex
65
CONSTRICTIVE PERICARDITIS DIAGNOSIS APPROACH
• EKG-not very helpful-may show low voltage QRS and inverted T waves
• CXR-pericardial calcifications seen in 50% on lateral view(not diagnostic)
• ECHO, CT, MRI are diagnostic
66
CONSTRICTIVE PERICARDITIS DIFFERENTIAL DIAGNOSIS
• Consider acute pericarditis, myocarditis, exacerbation of chronic ventricular dysfunction, or systemic process resulting in decreased cardiac performance(sepsis)
67
CONSTRICTIVE PERICARDITIS MANAGEMENT
• Supportive care• Symptomatic patients require admission and
pericardiectomy
68
PERICARDIAL EFFUSION
• Major causes are post cardiac surgery and • Neoplastic disease• Gradual accumulation of fluid (chronic) permits
progressive stretching of pericardium• Patient may develop a substantial fluid without
significant increase in intrapericardial pressure
69
PERICARDIAL EFFUSION PATOPHYSIOLOGY
• Significantly increased intrapericardial pressure impedes diastolic filling of the ventricles
• Therefore in order for the ventricles to fill the end-diastolic pressure must exceed the pericardial pressure
• Global effusion – pericardial pressure is equal around heart
• Therefore both ventricles have to increase EDP to same amount for ventricles to fill
70
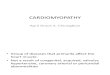
PERICARDIAL EFFUSION DIAGNOSTIC APPROACH
• Clinical examination – SOB, orthopnoea, tachycardia (varying degrees)
• Auscultation – may have muffled heart sounds• ECG may show low amplitude QRS complexes and
alternating axis• CXR – globular appearance to heart and therefore
increased cardiothoracic ratio• Echo – size of effusion and haemodynamic effect of it
71
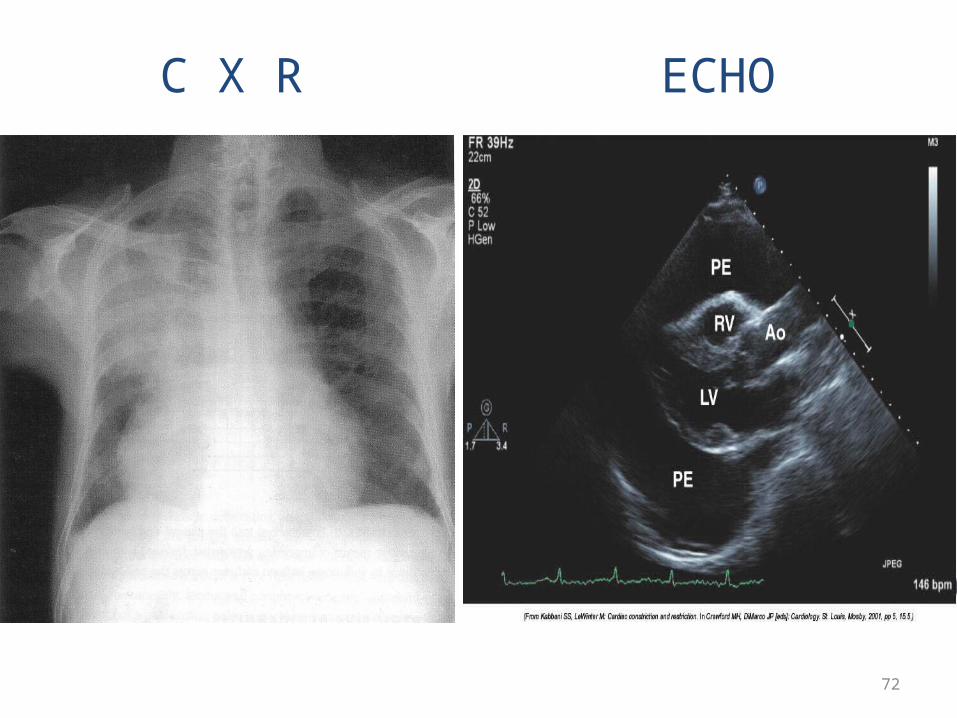
C X R ECHO
72
PERICARDIAL EFFUSION TREATMENT
• Depends on the cause and nature• If acute the cause is treated and the patient
monitored• If persistent problem or life threatening more
dramatic action is called for
73
CARDIAC TAMPONADE
• Occurs when the fluid accumulation around the heart impairs filling to such an extent that there is haemodynamic compromise.
• It is a medical emergency and must be treated promptly.
• Risk of death depends upon speed of diagnosis, treatment and underlying cause of the tamponade.
74
CARDIAC TAMPONADE CLINICAL PRESENTATIONS
• Dyspnea and decreased exercise tolerance-wt loss, pedal edema, ascites
• Tachycardia, Narrow pulse pressure• Pulsus paradoxus• JVD, Muffled heart sounds, Hypotension
75
CARDIAC TAMPONADE DIAGNOSTIC APPROACH
• EKG-low voltage QRS with ST elevation and PR depression possible
• Electrical Alternans-classic finding—P and R wave beat to beat variability
• CXR-+/- enlarged cardiac silhoutte “globular heart”• ECHO :
- Size and location of effusion- Any evidence of diastolic collapse- ‘Swinging’ of the heart- Decrease of insp. flow across MV
76
CARDIAC TAMPONADE DIAGNOSTIC APPROACH
• IV Fluid Bolus-improves RV filling and improves hemodynamics
• Pericardiocentesis-therapeutic and diagnostic
• Admission to ICU or monitored setting
77