Embed Size (px)
Citation preview
CARDIOMYOPATHIES
Dr. M. A. Sofi MD; FRCP (London); FRCPEdin;
FRCSEdin

• 1980 World Health Organization (WHO) defined cardiomyopathy as "heart muscle diseases of unknown cause" to distinguish cardiomyopathy from cardiac dysfunction due to known cardiovascular entities such as hypertension, ischemic heart disease, or valvular disease
• 1995 As a result, the WHO/International Society and Federation of Cardiology (ISFC) set a Task Force on the Definition and Classification of the Cardiomyopathies
Cardiomyopathies

CardiomyopathyWHO Classification1. Dilated (DCM)
• Enlarged • Systolic
dysfunction2. Hypertrophic (HCM)
• Thickened• Diastolic
dysfunction3. Restrictive (RCM)
• Diastolic dysfunction
3. Arrhythmogenic RV Cardiomyopathy/Dysplasia (AVRCD/D)• Fibrofatty
replacement 4. Unclassified
• Fibroelastosis• LV no compaction
• Ischemic
• Valvular• Hypertensive• Familial • Idiopathic • InflammatoryInfectious• Viral – picornovirus, Cox B, CMV,
HIV• Ricketsial - Lyme Disease• Parasitic - Chagas’ Disease,
ToxoplasmosisToxic• Alcohol, Anthracyclins
(adriamycin), Cocaine, heavy metals
Infiltrative• Hemochromatosis , Amylodosis
Non-infectious• Collagen Disease
(SLE, RA)• PeripartumMetabolic•Endocrine –thyroid dz, pheochromocytoma, DM, acromegaly, Nutritional• Thiamine, selenium,
carnitine Neuromuscular (Duchene dystrophy,
Myotonic dystrophy
DCM: Etiology
Cardiomyopathy associated with collagen-vascular disease
• Several collagen-vascular diseases have been implicated in the development of cardiomyopathies. These include the following:
• Rheumatoid arthritis • Systemic lupus erythematosus • Progressive systemic sclerosis • Polymyositis • HLA-B12–associated cardiac
disease • Diagnosis is based on
identification of the underlying disease in conjunction with appropriate clinical findings of heart failure.
Granulomatous cardiomyopathy (sarcoidosis)
• End myocardial biopsy may be helpful especially in sarcoidosis in which the myocardium may be involved.
• Involvement may be patchy, resulting in a negative biopsy finding.
• The diagnosis can also be made if some other tissue diagnosis is possible or available in conjunction with the appropriate clinical picture for heart failure.
• Cardiac involvement in sarcoidosis reportedly occurs in approximately 20% of cases.
DCM: Etiologies

• DCM is characterized by dilatation and impaired contraction of one or both ventricles.
• Affected patients have impaired systolic function and clinical presentation is usually with features. of heart failure
• When the presenting manifestations include conduction abnormalities, atrial and/or ventricular arrhythmias, and sudden death, then an arrhythmogenic cardiomyopathy caused by mutations in desmosomal, ion channel, and the lamin gene should be considered
Dilated Cardiomyopathy
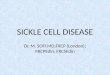
This plain frontal radiograph of the chest demonstrates marked enlargement of the cardiac silhouette compatible with a dilated cardiomyopathy..
Dilated cardiomyopathy chest radiograph
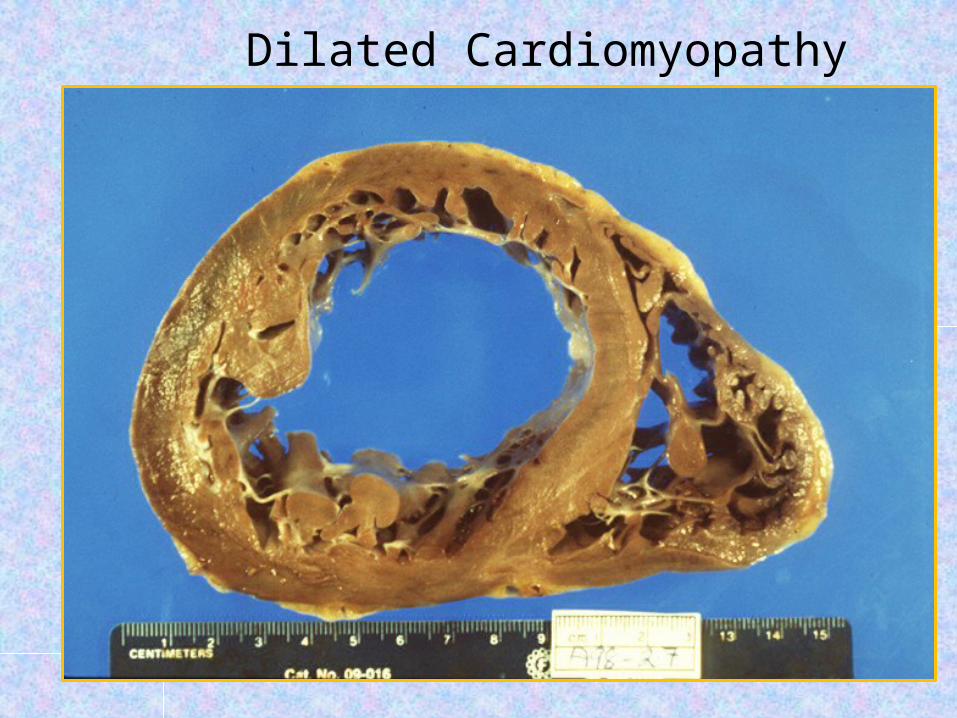
Dilated Cardiomyopathy

• The most distinctive (2D) dimensional echocardiographic findings in a DCM are:
• Left ventricular spherical dilatation
• Normal or reduced wall thickness,
• Poor systolic wall thickening, and/or reduced inward endocardial systolic motion and image.
• All of the systolic indices are reduced, including left ventricular fractional shortening, fractional area change, and ejection fraction.
• Four chamber cardiac enlargement is often present .
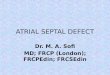
DILATED CARDIOMYOPATHY: ECHOCARIOGRAPHIC FINDINGS
4 chamber view of 2D echocardiogram:Panel A – Normal heart Panel B - Cardiomyopathy The heart is more spherical than its normal counterpart; the developing of a spherical configuration is fairly typical of cardiomyopathy.
Left ventricle in cardiomyopathy

Alcoholic cardiomyopathy• Chronic use• Reversible with abstinence• Mechanism?:–Myocyte cell death and fibrosis–Directly inhibits:• mitochondrial oxidative phosphorylation•Fatty acid oxidation
DCM: Toxic

Familial Cardiomyopathy
• Familial DCM is diagnosed in patients with idiopathic cardiomyopathy who have 2 or more first- or second-degree relatives with the same disease (without defined etiology).
• 30% of ‘idiopathic’• Inheritance patterns– Autosommal dom/rec, x-linked, mitochondrial
• Associated phenotypes:– Skeletal muscle abn, neurologic, auditory
• Mechanism:– Abnormalities in:• Energy production• Contractile force generation
– Specific genes coding for:• Myosin, actin, dystophin…
DCM: Inherited

Peripartum cardiomyopathy (PPCM, also called pregnancy-associated cardiomyopathy) is a rare cause of heart failure (HF) that affects women late in pregnancy or in the early puerperium
• Presentation of PPCM is variable and similar to that in other forms of systolic HF due to cardiomyopathy .
• Patients most commonly complain of dyspnea; other frequent symptoms include cough, orthopnea, paroxysmal nocturnal dyspnea, pedal edema, and hemoptysis.
Diagnosis (PPCM) is based upon three clinical criteria:
• Development of heart failure (HF) toward the end of pregnancy or in the months following delivery
• Absence of another identifiable cause of HF
• left ventricular (LV) systolic dysfunction with an LV ejection fraction (LVEF) generally <45 percent
DCM: Peripartum
• Fatigue• Dyspnea on
exertion• Shortness of breath• Orthopnea,
paroxysmal nocturnal dyspnea
• Increasing edema, weight, or abdominal girth
On physical examination, look for signs of heart failure and volume overload. Assess vital signs with specific attention to the following:• Tachypnea• Tachycardia• Hypertension
Dilated cardiomyopathy: Signs & Symptoms

Other pertinent findings are determined by the level of cardiac compensation or de-compensation • Signs of hypoxia (e.g.,
cyanosis, clubbing)• Jugular venous
distension (JVD)• Pulmonary edema
(crackles and/or wheezes)
• S3 gallop
• Enlarged liver• Peripheral edema
Look for the following on examination of the neck:• Jugular venous
distention (as an estimate of central venous pressure)
• Hepatojugular reflux• a wave• Large cv wave
(observed with tricuspid regurgitation)
• Goiter
Dilated cardiomyopathy: Signs & Symptoms

Findings on examination of the heart may include the following:• Cardiomegaly
(broad and displaced point of maximal impulse, right ventricular heave)
• Murmurs (with appropriate maneuvers)
• S2 at the base (paradoxical splitting, prominent P2),
• S3, and S4
• Tachycardia• Irregularly
irregular rhythm• Gallops
Dilated Cardiomyopathy: Signs & Symptoms
The workup in a patient with suspected cardiomyopathy may include the following:• Complete blood
count• Metabolic panel• Thyroid function tests• Cardiac biomarkers
• B-type natriuretic peptide assay
• Chest radiography• Echocardiography• Cardiac magnetic
resonance imaging (MRI)
• Electrocardiography (ECG)
DCM: Laboratory work up
Drug classes used include the following:• Angiotensin-
converting enzyme (ACE) inhibitors
• Angiotensin II receptor blockers (ARBs)
• Beta-blockers• Aldosterone
antagonists
• Cardiac glycosides• Diuretics• Vasodilators• Antiarrhythmics• Human B-type
natriuretic peptide• Inotropic agents• Anticoagulants may
be used in selected patients.
Management:Treatment of dilated cardiomyopathy is essentially the same as treatment of chronic heart failure (CHF).

• Left ventricular assist devices• Cardiac resynchronization
therapy (biventricular pacing)• Automatic implantable
cardioverter-defibrillators• Ventricular restoration surgery• Heart transplantation
Treatment:Surgical options for patients with disease refractory to medical therapy include the following

• Hypertrophic cardiomyopathy (HCM) is a genetic disorder that has a variable presentation and carries a high incidence of sudden death.
• Its hallmark is myocardial hypertrophy that is inappropriate and often asymmetrical and that occurs in the absence of an obvious inciting hypertrophic stimulus.
Signs and symptoms• Signs and symptoms of HCM
can include the following:• Sudden cardiac death (the
most devastating presenting manifestation)
• Dyspnea (the most common presenting symptom)
Signs and symptoms
• Angina• Palpitations• Orthopnea and
paroxysmal nocturnal dyspnea (early signs of congestive heart failure [CHF])
• CHF (relatively uncommon but sometimes seen)
• Dizziness
Hypertrophic Cardiomyopathy
Physical findings may include the following:• Double apical impulse or
triple apical impulse (less common)
• Normal first heart sound; second heart sound usually is normally split but is paradoxically split in some patients with severe outflow gradients; S3 gallop is common in children but signifies decompensated CHF in adults; S4 is frequently heard
• Jugular venous pulse revealing a prominent a wave
• Double carotid arterial pulse
• Apical precordial impulse that is displaced laterally and usually is abnormally forceful and enlarged
• Systolic ejection crescendo-decrescendo murmur
• Holosystolic murmur at the apex and axilla of mitral regurgitation
• Diastolic decrescendo murmur of aortic regurgitation (10% of patients)
Hypertrophic Cardiomyopathy

Signs and symptoms• Signs and symptoms
of HCM can include the following:
• Sudden cardiac death (the most devastating presenting manifestation)
• Dyspnea (the most common presenting symptom)
• Syncope • Angina• Palpitations• Orthopnea and
paroxysmal nocturnal dyspnea (early signs of congestive heart failure [CHF]
• CHF (relatively uncommon but sometimes seen)
• Dizziness
Hypertrophic Cardiomyopathy

Physical findings may include the following:• Double apical impulse or
triple apical impulse (less common)
• Normal first heart sound; second heart sound usually is normally split but is paradoxically split in some patients with severe outflow gradients; S3 gallop is common in children but signifies decompensated CHF in adults; S4 is frequently heard
• Jugular venous pulse revealing a prominent a wave
• Double carotid arterial pulse
• Apical precordial impulse that is displaced laterally and usually is abnormally forceful and enlarged
• Systolic ejection crescendo-decrescendo murmur
• Holosystolic murmur at the apex and axilla of mitral regurgitation
• Diastolic decrescendo murmur of aortic regurgitation (10% of patients)
Hypertrophic Cardiomyopathy

Hypertrophic Cardiomyopathy

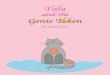
No specific laboratory blood tests are required in the workup. Genetic testing is not yet widely available but is becoming increasingly so.• Two-dimensional (2-D)
echocardiography is diagnostic for HCM. Findings may be summarized as follows:
• Abnormal systolic anterior leaflet motion of the mitral valve
• Left ventricular hypertrophy (LVH)
• Left atrial enlargement• Small ventricular
chamber size• Septal hypertrophy
with septal-to-free wall ratio greater than 1.4:1
• Mitral valve prolapse and mitral regurgitation
• Decreased midaortic flow
• Partial systolic closure of the aortic valve in midsystole
Hypertrophic Cardiomyopathy: Diagnosis
Other imaging modalities that may be useful include the following:• Chest radiography• Radionuclide imaging• Cardiac MRI: Particularly
useful when echocardiography is questionable, particularly with apical hypertrophy
Cardiac catheterization (to determine the degree of outflow obstruction, cardiac hemodynamics, the anatomy and diastolic characteristics of the left ventricle, and the coronary anatomy)
Electrocardiographic findings:• ST-T wave abnormalities
and LVH• Axis deviation (right or
left)• Conduction
abnormalities (P-R prolongation, bundle-branch block)
• Sinus bradycardia with ectopic atrial rhythm
• Atrial enlargement• Abnormal and prominent
Q wave in the anterior precordial and lateral limb leads, short P-R interval with QRS suggestive of preexcitation, atrial fibrillation (poor prognostic sign), and a P-wave abnormality (all uncommon)
Hypertrophic Cardiomyopathy: Diagnosis
Pharmacologic therapy for HCM may include the following:• Beta blockers• Calcium channel
blockers• Diltiazem,
amiodarone, and disopyramide (rarely)
• Antitussives to prevent coughing
The following caveats are warranted:• Avoid inotropic
drugs if possible• Avoid nitrates and
sympathomimetic amines, except in concomitant coronary artery disease
• Avoid digitalis• Use diuretics with
caution
HCM: Management

Surgical and catheter-based therapeutic options include the following:• Left ventricular
myomectomy• Mitral valve
replacement• Permanent pacemaker
implantation• Catheter septal ablation• Placement of an
implantable cardioverter defibrillator
ComplicationsComplications of HCM may include the following:• Congestive heart failure• Ventricular and
supraventricular arrhythmias
• Infective mitral endocarditis
• Atrial fibrillation with mural thrombus formation
• Sudden death
HOCM: Management

Restrictive cardiomyopathy (RCM)
• The World Health Organization (WHO) defines RCM as a myocardial disease characterized by restrictive filling and reduced diastolic volume of either or both ventricles with normal or near-normal systolic function and wall thickness.
• Increased interstitial fibrosis may be present.• This disease may be idiopathic or associated with
other diseases (e.g., amyloidosis and endomyocardial disease with or without hypereosinophilia).
• The course of RCM varies, depending on the pathology and treatment, but is often unsatisfactory.
Restrictive cardiomyopathy (RCM)
• The importance of an accurate diagnosis of RCM is to distinguish this condition from constrictive pericarditis, a clinically and hemodynamically similar entity.
• It also presents with restrictive physiology but is frequently curable by surgical intervention.
• This distinction is difficult to make but crucial because the treatment options and prognoses for the 2 conditions differ drastically.
• Echocardiography and cardiac magnetic resonance imaging have been reported to be comparable in their ability to differentiate RCM from constrictive pericarditis.
• Idiopathic RCM may be caused by EMF or by Loeffler eosinophilic endomyocardial disease.

Secondary Restrictive cardiomyopathy(RCM)
Secondary restrictive cardiomyopathy may be caused by:• Hemochromatosis• Amyloidosis (the most common cause of
RCM in the United States)• Sarcoidosis• Progressive systemic sclerosis (scleroderma)• Carcinoid heart disease• Glycogen storage disease of the heart• Radiation• Metastatic malignancy• Anthracycline toxicity

Secondary Restrictive cardiomyopathy(RCM)
Treatment:• Restrictive cardiomyopathy (RCM) has no specific
treatment.• Therapies directed at individual causes of RCM have been
proven to be effective. • Examples of this include corticosteroids for sarcoidosis
and Loeffler endocarditis, • Endocardiectomy for endomyocardial fibrosis and
Loeffler endocarditis, • Phlebotomy and chelation for hemochromatosis• Chemotherapy for amyloidosis. • The mainstays of medical treatment include diuretics,
vasodilators, and angiotensin-converting enzyme inhibitors (ACEs) as indicated, as well as anticoagulation (if not contraindicated).[14]
• In selected patients, permanent pacing, LVAD therapy, and transplantation (heart or heart-liver) may be considered.