Embed Size (px)
Citation preview

Cardiology: preoperative assessment and investigation
10 March 2016 John Chambers
Prof Clinical Cardiology 20
16 POPS

Risk of myocardial infarction or death at 30 days
• 2.5% in major surgery • 6.2% vascular surgery (NB higher if troponin screening)
Mangano Anesthesiology 1998; 88: 561-4; Mangano NEJM 1995; 333: 1750-6
2016
POPS

Risk of myocardial infarction or death at 30 days
• 2.5% in major surgery • 6.2% vascular surgery (NB higher if troponin screening) • Mechanism plaque rupture in 50% • Noninvasive testing limited: medical therapy
effective
Mangano Anesthesiology 1998; 88: 561-4; Mangano NEJM 1995; 333: 1750-6
2016
POPS

Triage of presurgical assessment
• Emergency - Clinical assessment • Semi-emergency – Cardiac investigation:
– Unstable or severe angina – Decompensated heart failure – Significant arrhythmia – Severe aortic or mitral stenosis
Kristensen. Europ Heart J 2014; 35: 2383-243. Fleisher. Circulation 2007; 116: e418-e500 and Fleisher JACC 2014;64:e77-e137.
2016
POPS

Screening in stable patients with non-emergency surgery
Risk score
Type of surgery Functional capacity 2016
POPS

Revised cardiac index risk score
• CAD Distant myocardial infarct; positive exercise test; current angina; use of nitrates; Q waves
• CCF History of CCF or pulmonary oedema; S3 and rales; chest X-ray evidence • CVA History of CVA or TIA
• Diabetes On insulin • CRF Creatinine > 160 micromol/L
• Age > 70
Lee. Circulation 1999; 100: 1043-9; Boersma Am J Med 2005; 118: 1134-41
2016
POPS

Estimated energy requirements
• Eat, dress, use lavatory • Walk inside the house • Light work like dusting/washing dishes • Climb 2 flights of stairs/hill • Walk on level ground at 4.0 mph • Run for a bus • Scrub floors/move furniture • Golf, bowling, doubles tennis • Swimming, singles tennis
1 MET
4 METs
> 10 METs Reilly. Arch Intern Med 1999; 159: 2185-92
7 METs
2016
POPS

Classification of surgical risk (30 day MCI and death)
Risk Types of surgery High (>5%) Vascular – aortic & peripheral, liver resection, duodeno-
pancreatic, oesophagectomy, perforated bowel, adrenal resection, total cystectomy, pneumonectomy, lung or liver transplant
Intermed (1-5%)
Abdominal (including laparoscopic), symptomatic carotid, peripheral artery PCI, endovascular aneurysm repair, head and neck, hip and spine, pulmonary, major urological or gynaecological, renal transplant, non-major intrathoracic
Low (<1%) Orthopaedic (knee), minor urological (TURP), carotid (asymptomatic), breast, dental, eye, minor gynae, plastic
Fleisher. Circulation 2007; 116: e418-e500 Kristensen. Europ Heart J 2014; 35: 2383-243
2016
POPS

Are routine tests needed?
12 lead ECG • Known CAD or structural disease except
having low-risk surgery • Consider if high-risk surgery Echo for LV systolic function • Breathless or known heart failure
Fleischer. JACC 2014; 64:e77-e137 20
16 POPS

Approach to valve disease
• No problem: – All mild lesions and mod MR or AR plus – No symptoms plus – Normal LV
• All else needs cardiac referral: – Symptoms often only revealed by exercise testing – Severe MS may decompensate even if asymptomatic – Beware moderate AS 20
16 POPS

Management of aortic stenosis
Kristensen. EHJ 2014; 35: 2383-243 20
16 POPS

Aortic and mitral regurgitation
• Even if severe well if compensated: – No symptoms and – LVEF > 50% for AR and > 60% for MR
2016
POPS

Functional cardiac testing • Only if testing will change management
– Intervention usually increases risk – Medical therapy effective
Kristen. Europ Heart J 2014; 35: 2383-243 Fleisher JACC 2014; 64: e77-e137
2016
POPS

Functional cardiac testing • Only if testing will change management
– Intervention usually increases risk – Medical therapy effective
• Indicated (class I) if high risk surgery plus – ≥2 risk factors and – Poor or unknown functional capacity
Kristen. Europ Heart J 2014; 35: 2383-243
Fleisher JACC 2014; 64: e77-e137 20
16 POPS

Functional cardiac testing • Only if testing will change management
– Intervention usually increases risk – Medical therapy effective
• Indicated (class I) if high risk surgery plus – ≥2 risk factors and – Poor or unknown functional capacity
• Consider (IIa) if high/intermed risk plus – ≥1 risk factors and – Poor functional capacity (<4 Mets)
Kristen. Europ Heart J 2014; 35: 2383-243 Fleisher JACC 2014; 64: e77-e137
2016
POPS

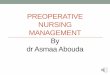
Coronary Artery Revascularization Prophylaxis trial before vascular surgery
McFalls. NEJM 2004; 351: 2795-2804 2016
POPS

Beta-blocker vs revascularisation
• Status of beta-blockade questioned because of: – DECREASE family flaws – POISE trial unrepresentative methodology*
• Imbalanced meta-analysis (Bouri Heart 2014;100:456) • Newspaper scare stories
*POISE: 100 mg metoprolol 2-4 hrs before and 6 hrs after and 200 mg 18 hrs CVS 5.8% vs 6.9%; deaths 3.1% vs 2.3%; stroke 1.0% vs 0.5% 20
16 POPS

Propensity matched effect of beta-blockers
Deaths RR Total group 0.73 2 Risk factors 0.63 3 Risk factors 0.54 4 Risk factors 0.40 Nonfatal MCI 0.67
VA medical centres Database 75,610 matched No effect in the vascular subgroup No increase in stroke
London. JAMA 2013;309:1704-13 20
16 POPS

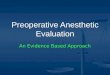
Effect of heart rate control
Feringa. Circulation 2006; 114: I-344-9 2016
POPS

When to start oral beta-blockade
• Continue if already indicated (class I) • Positive functional test (IIb) • High risk surgery and ≥ 2 risk factor (IIb)
– Start beta-blocker early ?≥30 days (certainly >1 week)
– Long-acting and beta1 selective e.g. atenolol or bisoprolol. Start low and titrate up.
– Titrate dose to heart rate 60-65 – Avoid hypotension
London. JAMA 2013;309:1704-13 Fleischmann JACC 2009; 54: 2102-28 Fleisher JACC 2014;64:e77-e137 Lindenauer NEJM 2005;353:349-61
2016
POPS

Statins and aspirin • Avoid interruption
– RR of events 3 for aspirin and 4.6 for statins
• Start statin > 2 weeks before vasc surgery • Stopping antiplatelets requires discussion • After coronary stent wait:
– Balloon alone 14 days – Bare metal stent 30 days (ideally 3 months) – Drug eluting ideally 12 mths (6 mths for new)
Kristensen. Eur Heart J 2014; 35: 2383-243 Burger. J Intern Med 2005; 257: 399-414 Durazzo. J Vasc Surg 2004; 39: 967-75 La Manach. Anesh Analg 2007; 104: 1326-33
2016
POPS

Key points
• Intervention for valve or coronary disease usually only when needed anyway
• Functional testing in: – High-risk surgery, ≥ 2 risk factors and poor (<4 Mets) or
unknown exercise capacity (I) – High or intermed risk, ≥ 1 risk factor and poor capacity (IIa)
• Main protection beta-blocker, aspirin and statin
– Avoid interruption 20
16 POPS

www.researchechocardiography.com 2016
POPS