Embed Size (px)
Citation preview
Cardiology: preoperative assessment and investigation
18 March 2011
John Chambers
Risk of myocardial infarction or death at 30 days
• 2.5% in major surgery
• 6.2% vascular surgery
(NB higher if troponin screening)
Mangano Anesthesiology 1998; 88: 561-4; Mangano NEJM 1995; 333: 1750-6

Risk of myocardial infarction or death at 30 days
• 2.5% in major surgery
• 6.2% vascular surgery
(NB higher if troponin screening)
• Mechanism plaque rupture in 50%
• Noninvasive testing limited: medical therapy effective
Mangano Anesthesiology 1998; 88: 561-4; Mangano NEJM 1995; 333: 1750-6

Deaths from aortic stenosis after non-cardiac surgery in the UK
• 10% of postoperative deaths sampled
• Aortic stenosis in 22
• 2 diagnosed at postmortem; in the rest often no echo or invasive monitoring
• Suggests one death from AS p.a. per hospital
National Confidential Enquiry into Perioperative Deaths 2001
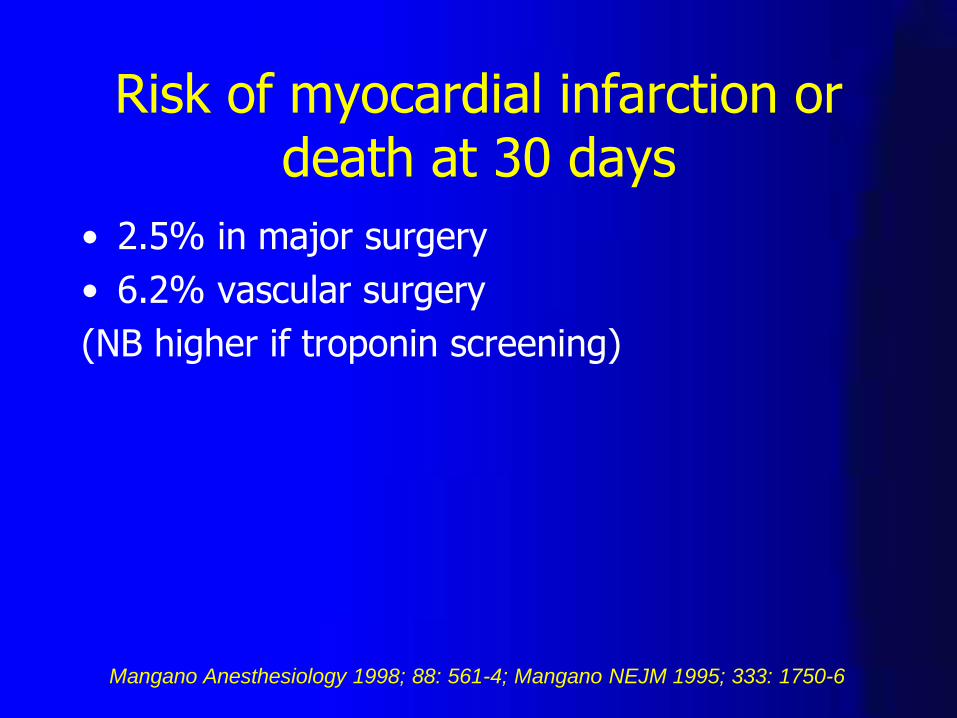
1 year mortality with preop stress testing
Revised cardiac risk index score* Hazard ratio
0 1.35
1-2 0.92
3-6 0.80
Wijeysundera. BMJ 2010; 340: 252
Lee. Circulation 1999; 100; 1043-9
Boersma. Am J Med 2005; 118:1134-41
*IHD, CCF, IDD, CRF, CVA, high-risk surgery
Triage of presurgical assessment
• Emergency - Clinical assessment
• Semi-emergency – Cardiac investigation:
– Unstable or severe angina
– Decompensated heart failure
– Significant arrhythmia
– Severe aortic or mitral stenosis
Screening in stable patients with non-emergency surgery
Risk score
Type of surgery Functional capacity
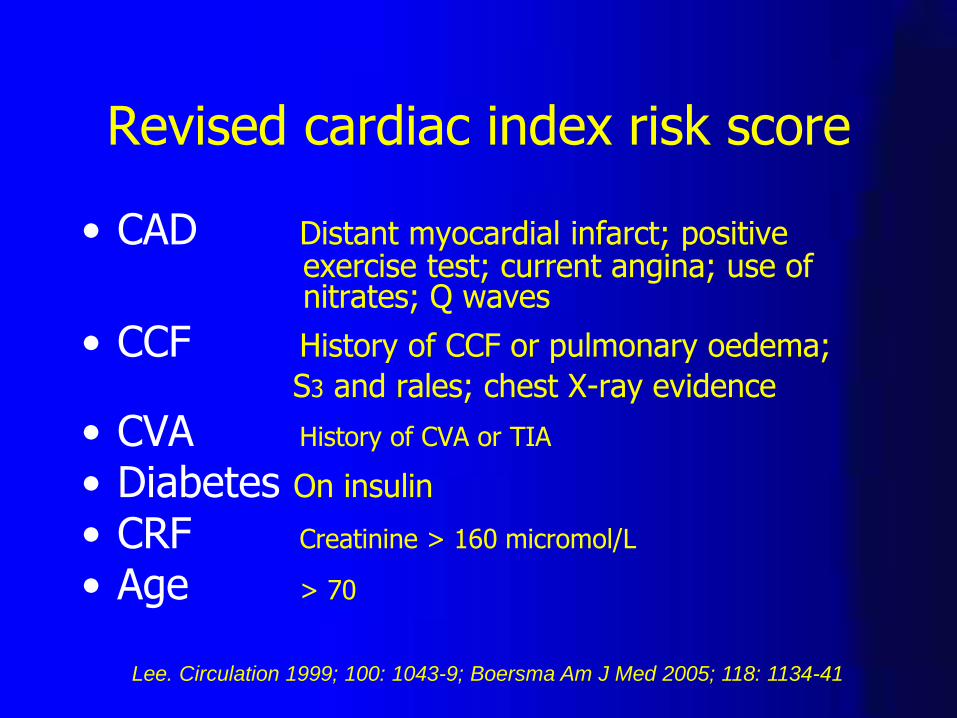
Revised cardiac index risk score
• CAD Distant myocardial infarct; positive exercise test; current angina; use of nitrates; Q waves
• CCF History of CCF or pulmonary oedema;
S3 and rales; chest X-ray evidence
• CVA History of CVA or TIA
• Diabetes On insulin
• CRF Creatinine > 160 micromol/L
• Age > 70
Lee. Circulation 1999; 100: 1043-9; Boersma Am J Med 2005; 118: 1134-41

Estimated energy requirements
• Eat, dress, use lavatory
• Walk inside the house
• Light work like dusting/washing dishes
• Climb 2 flights of stairs/hill
• Walk on level ground at 4.0 mph
• Run for a bus
• Scrub floors/move furniture
• Golf, bowling, doubles tennis
• Swimming, singles tennis
1 MET
4 METs
> 10 METs
Reilly. Arch Intern Med 1999; 159: 2185-92
7 METs

Grades of surgical risk MCI and death
Classification Types of surgery
High Vascular – aortic & peripheral
Intermediate – High Abdominal (including laparoscopic), carotid, peripheral artery PCI, endovascular aneurysm repair, head and neck, neurological, hip and spine, pulmonary, renal/liver transplant, major urological
Intermediate – Low Orthopaedic (knee), minor urological
Low Breast, dental, endocrine, eye, gynaecology, plastic
Boersma. Am J Med. 2005; 118: 1134-41
Fleisher. Circulation 2007; 116: e418-e500
Poldermans. Europ Heart J 2009; 30: 2769-2812

When to do an ECG
Recommendation Class
Risk factors + intermed/high risk surgery I
Risk factors and low risk surgery IIa
No risk factors + intermed/high risk surgery IIb (IIa*)
No risk factors + low risk surgery III
Poldermans. Europ Heart J 2009; 30: 2769-2812
*Fleisher. Circulation 2007; 116: e418-e500
Holter for syncope, presyncope, palpitation
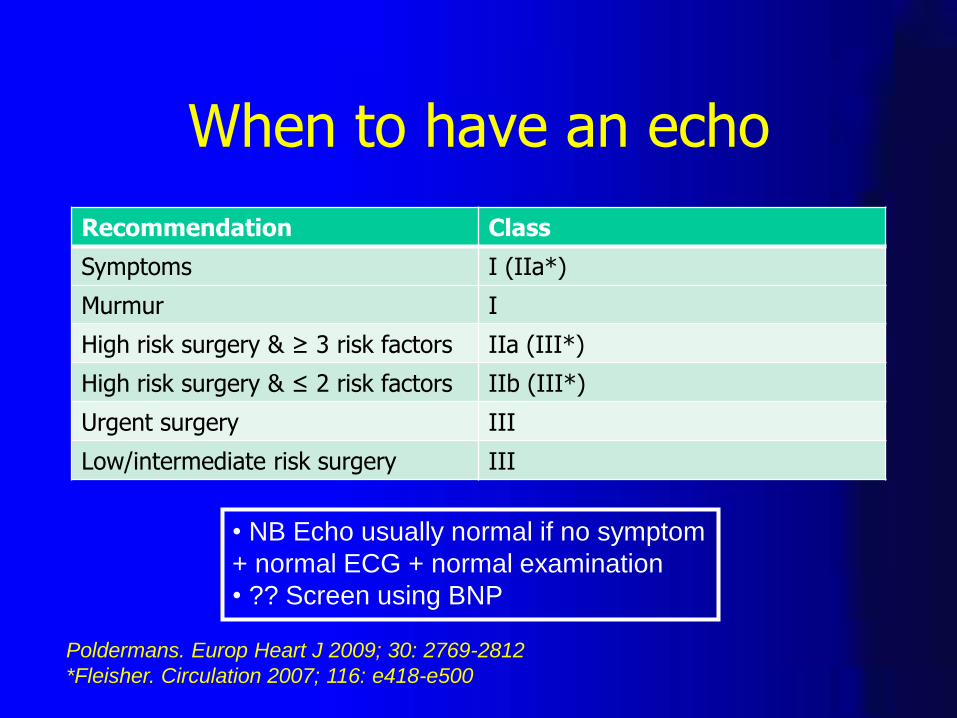
When to have an echo
Recommendation Class
Symptoms I (IIa*)
Murmur I
High risk surgery & ≥ 3 risk factors IIa (III*)
High risk surgery & ≤ 2 risk factors IIb (III*)
Urgent surgery III
Low/intermediate risk surgery III
Poldermans. Europ Heart J 2009; 30: 2769-2812
*Fleisher. Circulation 2007; 116: e418-e500
• NB Echo usually normal if no symptom
+ normal ECG + normal examination
• ?? Screen using BNP
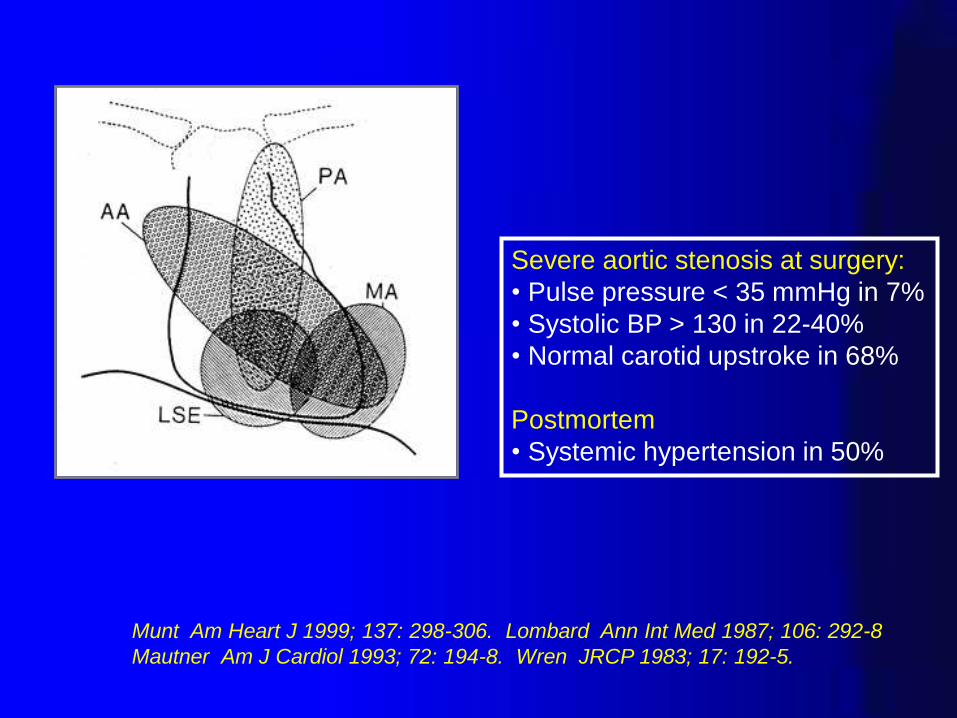
Severe aortic stenosis at surgery:
• Pulse pressure < 35 mmHg in 7%
• Systolic BP > 130 in 22-40%
• Normal carotid upstroke in 68%
Postmortem
• Systemic hypertension in 50%
Munt Am Heart J 1999; 137: 298-306. Lombard Ann Int Med 1987; 106: 292-8
Mautner Am J Cardiol 1993; 72: 194-8. Wren JRCP 1983; 17: 192-5.
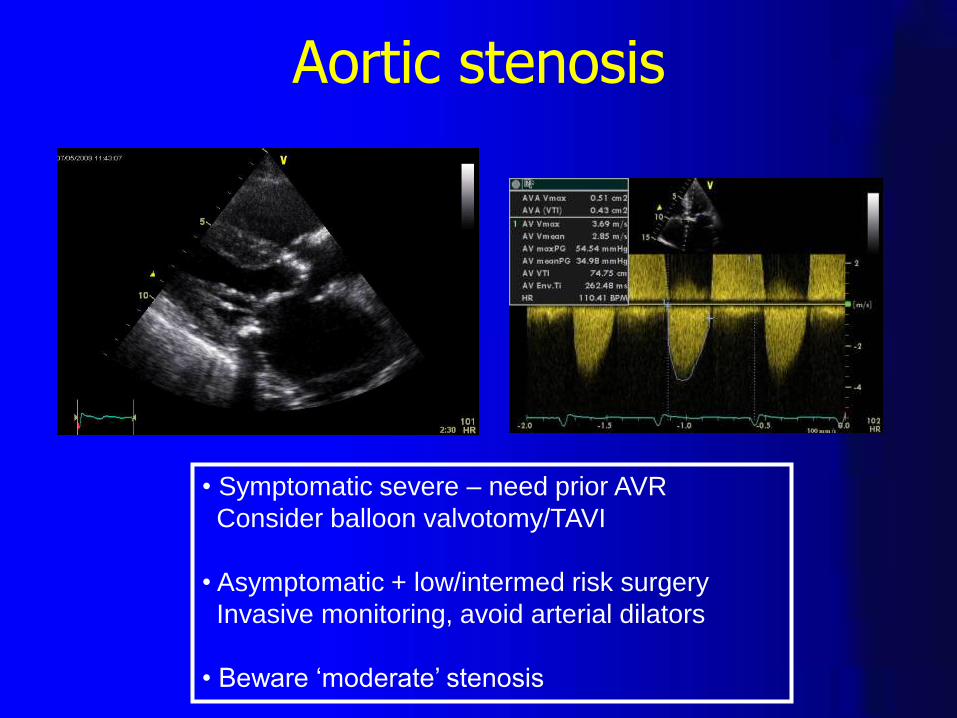
• Symptomatic severe – need prior AVR
Consider balloon valvotomy/TAVI
• Asymptomatic + low/intermed risk surgery
Invasive monitoring, avoid arterial dilators
• Beware ‘moderate’ stenosis
Aortic stenosis
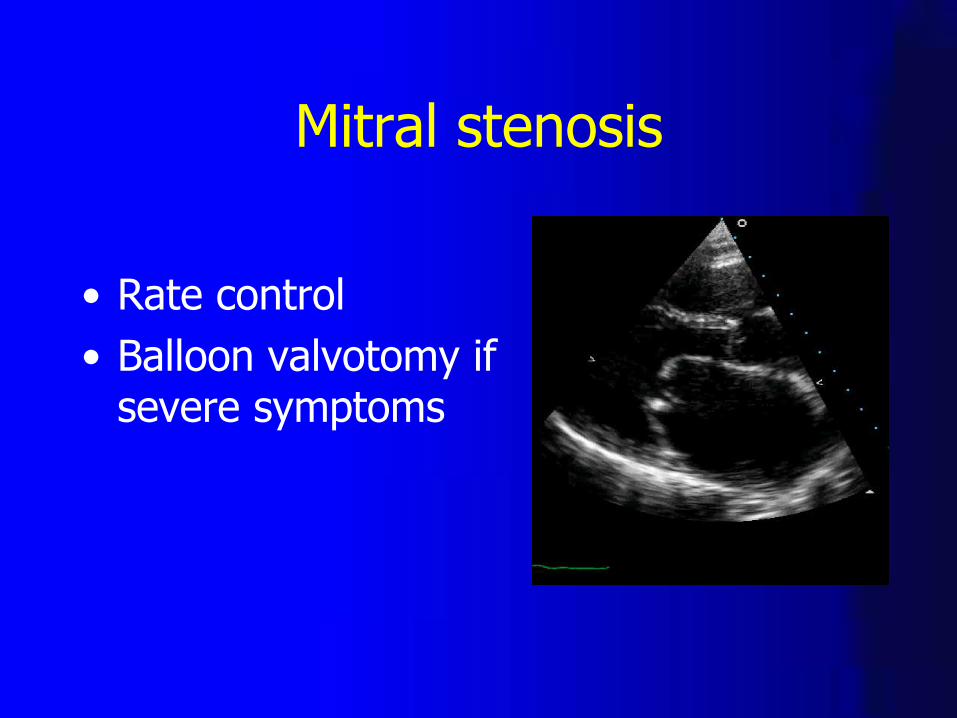
Mitral stenosis
• Rate control
• Balloon valvotomy if severe symptoms
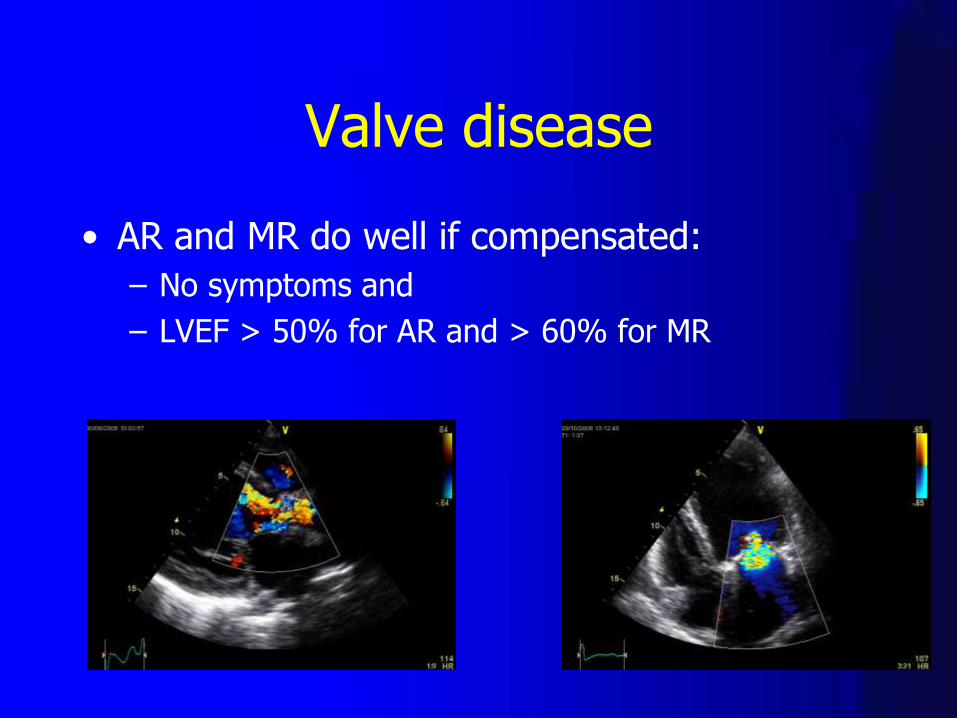
Valve disease
• AR and MR do well if compensated:
– No symptoms and
– LVEF > 50% for AR and > 60% for MR
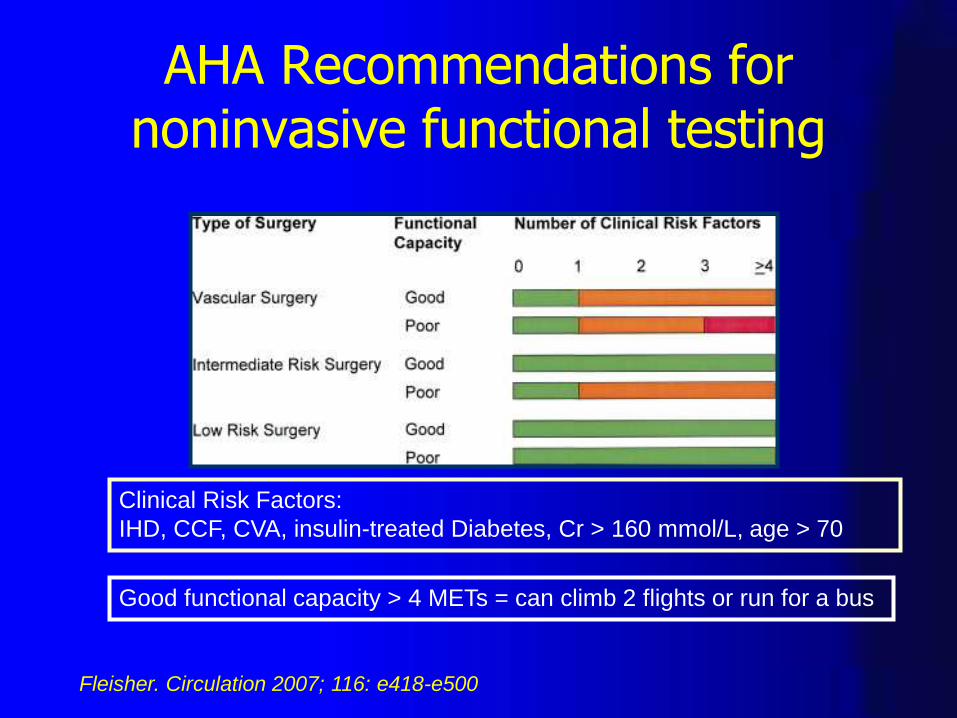
AHA Recommendations for noninvasive functional testing
Clinical Risk Factors:
IHD, CCF, CVA, insulin-treated Diabetes, Cr > 160 mmol/L, age > 70
Good functional capacity > 4 METs = can climb 2 flights or run for a bus
Fleisher. Circulation 2007; 116: e418-e500
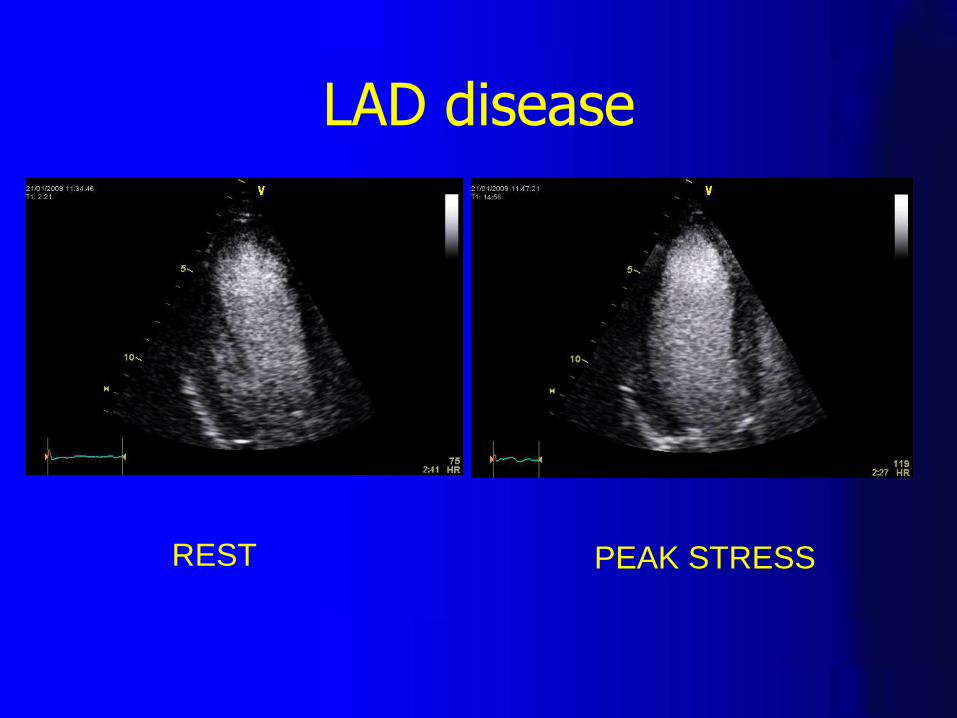
LAD disease
REST PEAK STRESS

Coronary angiography
Recommendation Class
Acute coronary syndrome I
Angina unresponsive to medical therapy I
Stable & intermediate/high-risk surgery IIb
Stable & low risk surgery III
Poldermans. Europ Heart J 2009; 30: 2769-2812
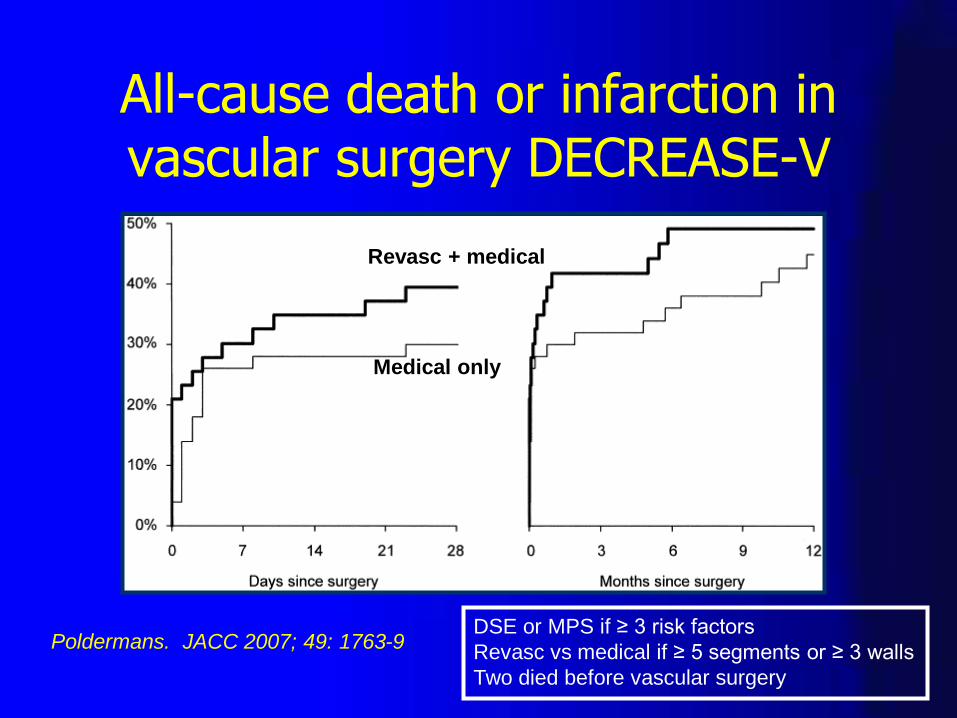
All-cause death or infarction in vascular surgery DECREASE-V
Poldermans. JACC 2007; 49: 1763-9
Revasc + medical
Medical only
DSE or MPS if ≥ 3 risk factors
Revasc vs medical if ≥ 5 segments or ≥ 3 walls
Two died before vascular surgery
Intermediate risk patients having major vascular surgery
• Relative risk 1 or 2. n = 770
• 30 day outcome 2.3% with testing and 1.8% without testing
• Extensive ischaemia in 34 of 386 outcome 25% with revasc and 9.1% without
• Outcome related to heart rate < 65
Poldermans. JACC 2006; 48: 964-9
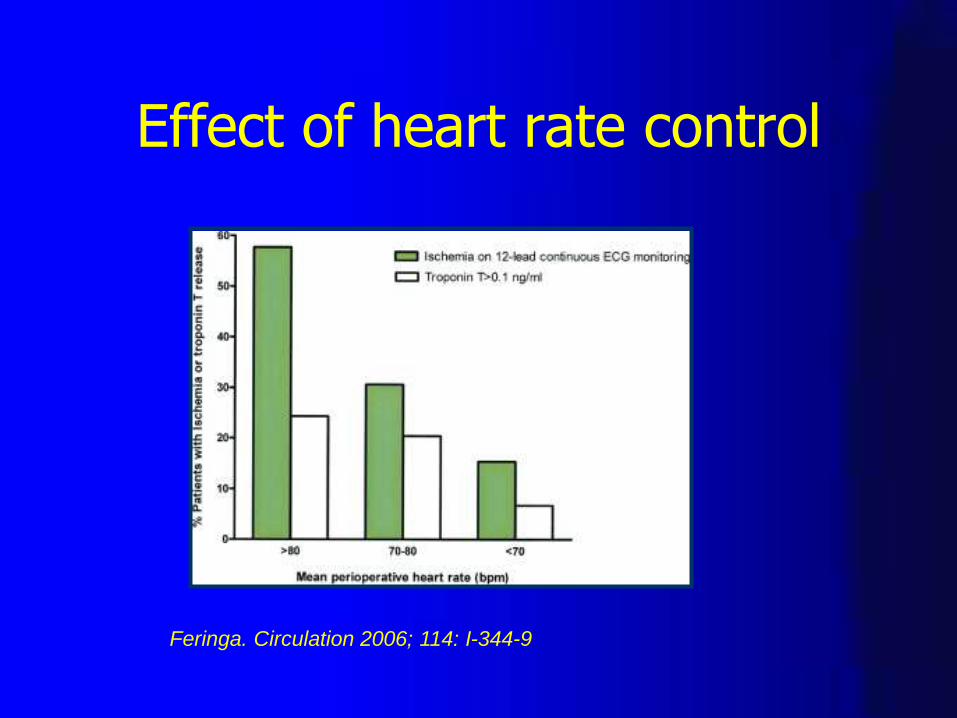
Effect of heart rate control
Feringa. Circulation 2006; 114: I-344-9
When to start oral beta-blockade
• Known CAD including positive functional test
• Vascular surgery or intermediate risk surgery and ≥ 1 risk factor
• Start beta-blocker early > 1 month
• Long-acting
• Titrate dose to heart rate 60-65
• Avoid hypotension (POISE)
Poldermans DECREASE 1. NEJM 1999; 341: 1789-94.
Devereaux. POISE. Lancet 2008; 371: 1839-47
Fleisher JACC 2006; 47: 2343-55
Key points
• Investigate and treat unstable angina, decompensated HF, arrhythmia, valve disease
• Consider investigation before high risk vascular surgery with > 1 risk factor esp if poor exertion
• Main protection medical therapy beta-blocker, aspirin and statin
• For the others investigation has no effect and delays surgery
www.researchechocardiography.com
Statins and aspirin
Statins
• Beneficial effect in all major non-cardiac surgery as well as vascular
• Avoid interruption (RR 4.6)
Aspirin
• Avoid interruption (RR 3)
Biondi-Zoccai. Europ Heart J 2006; 27: 2667-74
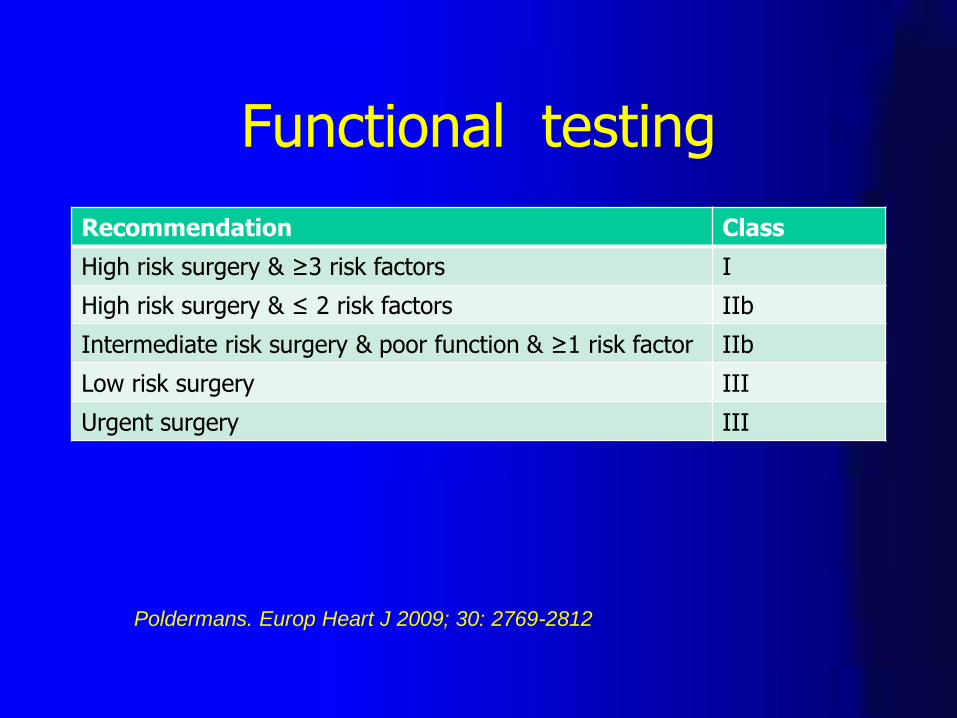
Functional testing
Recommendation Class
High risk surgery & ≥3 risk factors I
High risk surgery & ≤ 2 risk factors IIb
Intermediate risk surgery & poor function & ≥1 risk factor IIb
Low risk surgery III
Urgent surgery III
Poldermans. Europ Heart J 2009; 30: 2769-2812
Cardiac investigation before extracardiac surgery
• Aims: – To improve outcome after non-cardiac surgery
– Change operation e.g. conservative procedure, cancel operation
– Change management e.g. temporary pacing
– Screen for cardiac disease affecting long-term survival
• Avoid: – Investigation leading to poorer outcomes
– Delaying life-saving surgery

NatCEPOD 2001
• ‘Any asymptomatic murmur may indicate significant disease’
• ‘Whenever possible the anaesthetist of a patient with aortic stenosis should obtain a preoperative echocardiogram’
Problems after revascularisation
• Delay of index surgery
• Risks of cardiac surgery/PCI
• Need for clopidogrel after stenting
– 30 days bare metal
– One year drug-eluting
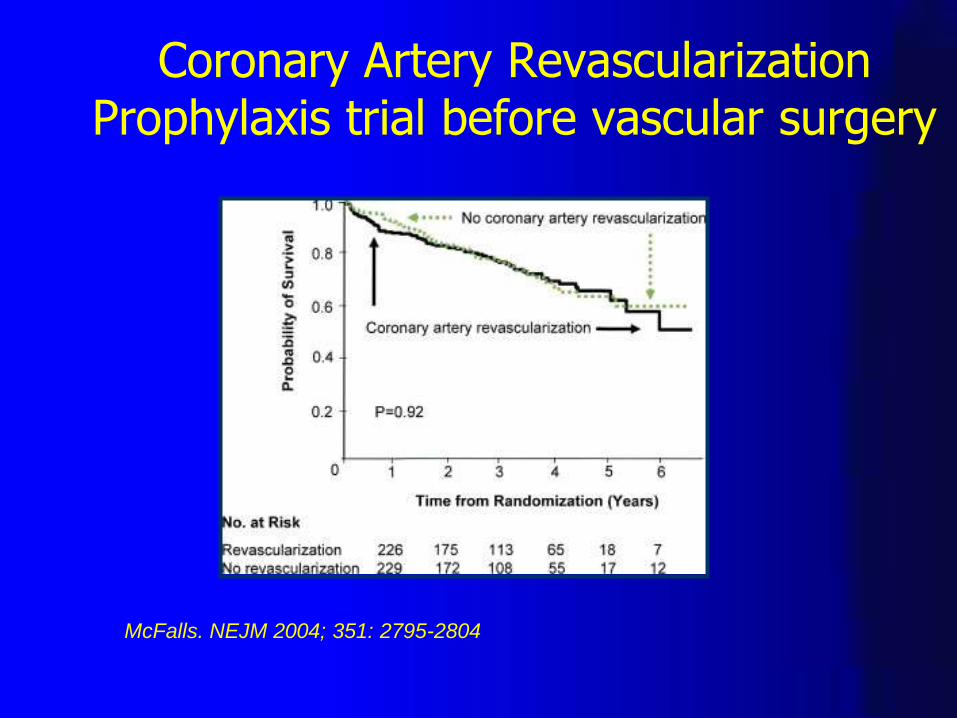
Coronary Artery Revascularization Prophylaxis trial before vascular surgery
McFalls. NEJM 2004; 351: 2795-2804

Performance of revised cardiac risk index score
Revised risk score
Number at risk Death (%) OR
≥ 3 969 3.6 11
2 3,380 1.7 5
1 28,892 0.7 2
0 75,352 0.3 1
Boersma. Am J Med. 2005; 118: 1134-41
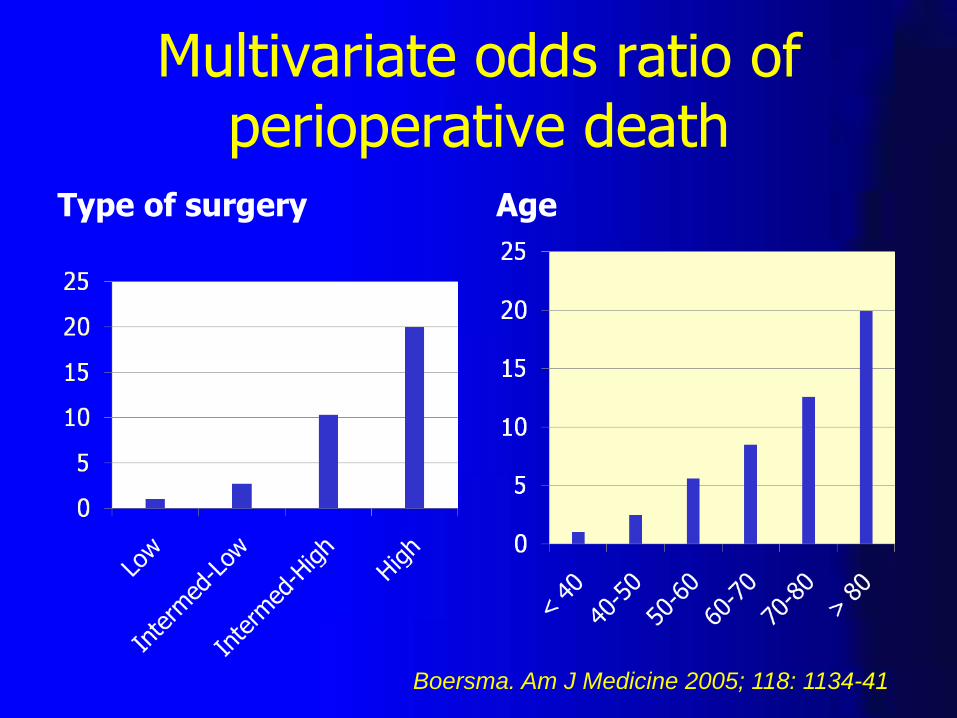
Multivariate odds ratio of perioperative death
Type of surgery Age
Boersma. Am J Medicine 2005; 118: 1134-41
Whom to investigate
• Severe CAD
• Decompensated CCF arrythmia
• Murmur
• Vascular surgery with CAD or risk factors
• Intermediate risk surgery with poor activity and risk factors

Prevalence of valve disease
Three population studies n = 11,911
Ethnically diverse
Nkomo. Lancet 2006; 368: 1005-11
Community study n=16,501 Clinically indicated echoes in Olmsted County (90% white)
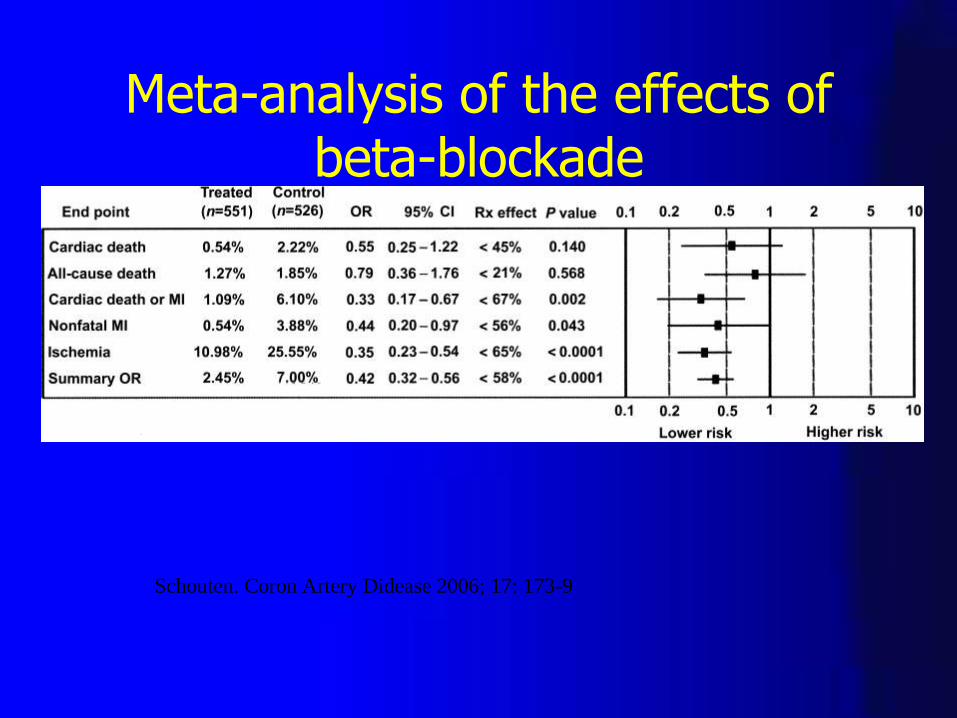
Meta-analysis of the effects of beta-blockade
Schouten. Coron Artery Didease 2006; 17: 173-9