Embed Size (px)
Citation preview

Cardiology Newsletter Volume 8 No 1April 2017
Sponsored in the interests of continuing medical education by:
CPD Accredited
• CommotioCordis:Anunder-appreciatedcauseofsuddencardiacdeathinyoungathletes
• TheclinicalvalueoftheCoronaryArteryCalcificationScore• Theroleofheartrateinthemanagementofheartfailure• Antiphospholypidsyndrome:Importantdiagnosisbutoften
missed

CARVEDILOL:
- is indicated twice daily for mild to moderate stable symptomatic congestive heart failure
- is indicated once daily for essential mild to moderate hypertension
- has a positive effect on metabolic parameters.1
RESTORE cardiac function
Carvetrend 6,25 mg. Each tablet contains 6,25 mg carvedilol. Reg. No.: RSA S3 A37/7.1.3/0276. NAM NS2 08/7.1.3/0105. BOT S2 BOT1101790. Carvetrend 12,5 mg. Each tablet contains 12,5 mg carvedilol. Reg. No.: RSA S3 A37/7.1.3/0277. NAM NS2 08/7.1.3/0104. BOT S2 BOT1101791. Carvetrend 25 mg. Each tablet contains 25 mg carvedilol. Reg. No.: RSA S3 A37/7.1.3/0278. NAM NS2 08/7.1.3/0103. BOT S2 BOT1101792. For full prescribing information, refer to the package insert approved by the Medicines Control Council, 16 September 2004. 1) Panagiotis C Stafylas, Pantelis A Sarafi dis. Carvedilol in hypertension treatment. Vascular Health and Risk Management 2008;4(1):23-30. CDD199/04/2016.
C A R V E D I L O L 6,25 mg 12,5 mg 25 mg
ß
For further product information contact PHARMA DYNAMICS P O Box 30958 Tokai Cape Town 7966 Tel 021 707 7000 Fax 021 701 5898 Email [email protected] CUSTOMER CARE LINE 0860 PHARMA (742 762) www.pharmadynamics.co.za
A Lupin Group Company
CDD199/04/2016_A4_FINAL_6May2016.indd 1 2016/05/05 12:42 PM

Page 3 Volume 8 No 1 April 2017
Editorial
Dr Adrian HorakCardiologist
Vincent Pallotti Hospital, Pinelands, Cape Town
hen we were u n d e r g r a d u a t e s studying medicine we were required to absorb and learn
enormous amounts of information, facts and even techniques.
Having graduated, it is no longer re-garded as adequate for us as medical practitioners to merely diagnose and treat disease correctly and expertly. We frequently need to consider many other issues which may affect decisions we make and the treatment we deliver. Financial considerations, ethical dilem-mas, emotional factors, availability of re-sources and the sometimes unintended consequences of our treatment are some of the many factors which demand our attention. Thus, when presented with new facts or new ideas, we need to as-similate these into our existing pool of knowledge and consider the wider im-plications as to how this will affect our responses, our treatment of and the wellbeing of our patients. We need to consider the Big Picture. In this, the first issue of Heart Matters in 2017, we present four interesting and diverse articles. Two of these deal with common but important problems which confront us on a daily basis, whilst the other two address far more rare condi-tions. All four however have the poten-tial to raise issues which extend beyond the mere scope of the conditions they address.
Sudden death in young athletes is a tragic and unfortunately not too rare an occur-rence. Fortunately, we have now identi-
fied many conditions which predispose to this tragic occurrence. Hypertrophic cardiomyopathy, arrhythmogenic right ventricular dysplasia, congenital long QT syndrome, anomalous coronary artery syndromes and polymorphic ventricular tachycardia can now be screened for and identified. But therein lies the problem. Finding a condition in a young profes-sional athlete may mean the end of his or her career. We need to be aware of this, and fully inform the individual of the potential consequences of any “routine screening” procedures before they are done. This is not standard practice with many professional sports organisations.
Dr Gavin Shang addresses a rare cause of death in young athletes. Commotio Cordis cannot be predicted. It is an ac-
Seeing the BIG picture
cident. But it CAN be treated, provided that a defibrillator (AED) is available im-mediately. And what about all the multi-tude of aging “athletes” and others taking part in physical activities at sports clubs and gyms etc. who are at risk of cardio-vascular events. It would seem appro-priate for all such facilities to at the very least have an AED available and to have trained personnel present. Again, this bare minimum safety measure seems to be sorely lacking at many venues.
On another track, it seems almost in-comprehensible to me that there can still be a “Statin Debate”. Statins are life-saving and life-changing drugs. This has been proven in randomised trials in more than 350,000 patients. How can there be doubt about their ef-ficacy and benefit? Although effective in all grade of risk, the greatest abso-lute reduction on events occurs when high risk individuals are treated. Per-haps it is their use in low risk popula-tions where the benefits are less well perceived, that has made them vulner-able to criticism by sceptics. Stratify-ing cardiovascular risk in our patients to identify high risk individuals who would most benefit from treatment would therefore seem to be appropri-ate although we should recognise that even low risk individuals do derive some benefit from statins (as shown in the Hope 3 study).
Dr Joe Mckibbin discusses value of the Coronary Artery Calcification Score (CAC) in risk stratification of our pa-tients. The CAC will allow us to specifi-cally target high risk individuals for ag-gressive management of their risk and
The CAC will allow us to specifically target high risk individuals for aggressive management of their risk and indeed may even identify patients at high risk who were initially thought to be at low risk. It therefore seems to be a valuable investigation which will improve our care of patients. As with any new procedure, it must be used judiciously.
DisclaimerThe content contained in this publication contains medical or health sciences information and is intended for professional use within the medical field. No suggested test or procedure should be carried out unless, in the reader’s judgement, its risk is justified. Because of rapid advances in the medical sciences, we recommend that the independent verification of diagnoses and drug dosages should be made. Discussions views, and recommendations as to medical procedures, products, choice of drugs, and drug dosages are the views of the authors. The views expressed by the editor or authors in this newsletter do not necessarily reflect those of the sponsors or publishers. The sponsors, publishers and editor will not be liable for any damages or injuries of any kind arising from the use or misuse of information provided in this publication and do not support the use of products for off label indications.
If you have any suggestions or topics you would like to see published or have articles and/or
case studies for publishing, please email us at: [email protected].
Production Editors: Ann Lake, Helen Gonçalves Design: Jane Gouveia
Enquiries: Ann Lake Publications 011 802 8847 Email: [email protected]

Volume 8 No 1 April 2017 Page 4
indeed may even identify patients at high risk who were initially thought to be at low risk. It therefore seems to be a valuable investigation which will im-prove our care of patients. As with any new procedure, it must be used judi-ciously. The CAC correlates with plaque burden and therefore with risk of ad-verse events in the future. It stratifies risk. It does not correlate with percent-age stenosis in arteries. It should not be used to try to diagnose whether a chest pain syndrome is angina or not. It also should not be used in individuals who have already been identified as being at high risk. This would be an inappro-priate use of resources. Used correctly however, the CAC adds great value to our practice.
Risk factors and markers of risk are dis-tinctly different. For example, elevated homocystein levels correlate well with increased cardiac risk. However, lower-ing the levels with therapy does not low-er this risk. (Hope 2 and Norvit studies). Homocysteine is thus a marker of risk, not a risk factor. In his article, Dr Jens Hitzeroth makes a good case for us to regard elevated heart rate as a risk fac-tor rather than merely a marker of poor outcomes in patients with heart failure. Lowering heart rate is beneficial in these patients. This is therefore an added tar-get for our focus in treating patients with heart failure.
Finally, the article on Antiphospholip-id Syndrome by Dr Roos, Dr Hobson and Dr Lubbe focuses our attention on
thromboembolic disease. The diagnosis of thromboembolism, particularly pul-monary embolism, is probably the most frequently missed diagnosis in medical practice. We should always be vigilant for this condition, bearing in mind that even young patients with no obvious risk factors may have conditions (such as the Antiphospholipid Syndrome) which may render them vulnerable to thromboem-bolic disease. This article also emphasis-es to need to identify underlying condi-tions responsible for the problem.
We hope you enjoy reading this edi-tion of Heart Matters, that it adds value to your practice and importantly that it stimulates you, raises issues for discus-sion and debate and prompts us to see the “Big Picture”.
Thankyoutooureditors
On behalf of our sponsor, Pharma Dynamics and ourselves as publishers, we would like to take this opportunity to thank Dr Mike Bennett for his hard work, dedication and expert guidance in producing an informative and up-to-date Heart Matters newsletter. We were privileged and honoured to work with him over the past few years and although passing the editorship to the capable guidance of Dr Adrian Horak, we look forward to input in the future as an occasional contributing author. Thank you Dr Horak for agreeing to take over the editorship and welcome to the Heart Matters Team! We have enjoyed working with you on this first issue and look forward to producing many more informative and interesting issues for our readers.
Ann Lake Publications

Page 5 Volume 8 No 1 April 2017
Dr Gavin Shang MBBCH (WITS) MPHIL SPORTS MED (UCT/SSISA)Sports Physician
Johannesburg
Commotio Cordis: An under-appreciated cause of sudden cardiac death in young athletes
ommotio cordis is a cardiac phenomenon that is a rare cause of sudden death in young athletes. It is primarily an arrhythmic event that re-
quires the synchronisation of certain pathophysiological variables that oc-curs when mechanical energy is trans-ferred from a blunt, non-penetrating force to a distinct area of the praecor-dium at a critical period during the cardiac cycle. This disturbs the electri-cal stability of an otherwise healthy myocardium, resulting in an acute ven-tricular fibrillation (VF) that requires rapid defibrillation.1,57,59
EpidemiologyCommotio cordis is considered as a diagnosis of exclusion; as structural or primary electric cardiac abnormalities are more often associated with unexpected sudden cardiac death (SCD) in young athletes during sports participation.1, 4, 5, 38
Hypertrophic cardiomyopathy (HOCM), arrhythmogenic right ventricular cardi-omyopathy, congenital prolongation of the QTc interval, polymorphic ventricu-lar tachycardia, anomalous coronary artery syndromes, myocardial infarc-tion in childhood and viral myocarditis, account for the majority of these SCDs in young athletes in these unfortunate instances.1,4,5,38
The United States Commotio Cordis Registry (established in 1996) has improved our understanding of its prevalence with 10-20 new cases reported per year and more than 220 cases recorded over the past 15 years.1-4,6,15,35,59
The worldwide incidence of commotio cordis is also probably more common due to poor recognition and under-reporting of past occurrences1 and is now recognised as one of the more frequent causes of SCD (up to 20%)4,46,47 in young athletes after HCOM and congenital coronary artery anomalies.4,5
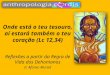
PresentationThis Registry has shown that commotio cordis occurs primarily in young, healthy and active individuals most frequently between 10 – 18 years of age (average age of 15). 95% of affected individuals were male (suspected due to the higher percentage of males involved in impact type sports), participating in a diverse spectrum of competitive (50% of episodes) or recreational (25% of episodes) sporting activities e.g. baseball, softball, ice hockey, American football, lacrosse, polo, soccer, boxing, cricket, rugby, martial arts, skiing and even basketball.1,35,59
Typically, the individual is hit in the chest (with or without chest protection) usually by a pitched, thrown or batted dense projectile at high or low velocity (58% of occurrences) or by the force of bodily contact (42% of occurrences) with the majority of cases collapsing immediately.1,38,59
10-20% of reported cases have displayed a period of purposeful activity, movement or behaviour (e.g. taking a few steps and continuing to walk or run, opening his or her eyes, or even speaking) prior to collapse,1 suggesting a brief period of individual tolerance to the ventricular arrhythmia (ventricular tachycardia (VT) or VF).1 Following collapse, patients are unresponsive, apneic and pulseless. Localised oval or circular contusions or abrasions at the site of impact are noted in one-third of patients.2,3
Laboratory findings Post mortems have shown a notable absence of congenital and acquired structural entities that are known to predispose young athletes to SCD. Cardiac enzymes are within normal hematological reference ranges with no evidence of myocardial necrosis, toxicology screenings have been uni-versally negative, and there has been no evidence of infarction, infection or inflammation histologically.34, 38
Cardiac weight, wall thickness and chamber dimensions were normal as
were the coronary arteries with no evi-dence of damage or thrombosis. There have been no reports of active or healed myocarditis or arrhythmogenic right ventricular cardiomyopathy. A few isolated reports of traumatic haemor-rhage in the left ventricular wall, arte-riovenous node and specialised con-duction system have been noted but the significance of these rare occurrences has yet to be determined in an isolated setting of commotion cordis.38
The absence of any structural cardiac in-jury, haemothorax, haemopericardium, external myocardial contusion and no underlying fracture(s) to the sternum or ribs, distinguishes commotio cordis from contusio cordis1,38, where high im-pact trauma results in morbidity and mortality due to direct trauma to myo-cardial tissue and the overlying thorax.
The most common ECG finding finding (in both non-survivors and survivors) has been found to be VF and asystole. This has been demonstrated repeat-edly in anaesthetised animal test sub-jects.8,9,11-13,15-17,19-24,34,38 Some studies have shown ST-segment elevation in precordial leads V1-V3. However, the significance of this remains unclear as myocardial ischaemia has yet to be demonstrated in anaesthetised animal models or human autopsies.8,9,11-13, 15-
17,19-24,34,38
DeterminantsPrecise synchronisation of certain vari-ables during the smallest of windows of vulnerability, helps to explain why com-motio cordis is such a rare event. 8,9,11-
13,15-17,19-24,34,38,59
Three primary variables have been identified:7-13
1. A relatively low-energy impact precisely over the centre of the left ventricle.15,27
Impacts over other precordial sites resulted in VF less often and impacts that did not overlie the heart failed to produce VF or any other ECG abnormalities.

Volume 8 No 1 April 2017 Page 6
Non-sustained polymorphic VTs, ST segment elevation, transient complete heart block, left bundle branch block and left ventricular wall motion abnormalities have transiently occurred in the absence of VF following impacts over the whole cardiac silhouette in these animal studies.7-12,15-24
2. The electro-physiologic events, following impact, were determined to be critically dependent on the precise timing of the impact during the repolarisation stage of the cardiac cycle (a narrow 10-40ms portion of the ascending phase just before the T wave peak).15,34,38,59
The morphology appears initially uneven and undulating, described as either a polymorphic ventricular tachycardia (PVT) or Torsade de Pointes.59 While PVTs are typically observed at first, they will progress into VF if sustained for over 10 beats. Outside this time frame, VF was rarely seen.59
The probability of precise timing of an impact to cause commotio cordis is about 4% in a cardiac cycle of 500ms (heart rate of 120b/min).38 It has been suggested that exercise induced hypoxia and acceleration of the cardiac conductive system also allows for the heart to be more susceptible to stretch induced VF.38
In vivo studies suggest that follow-ing high-speed impact with a dense projectile to the chest, a rapid rise in left ventricular pressure (250 – 450mmHg)1,9,16,19,24 causes stretch-related activation of normally inac-tive mechano-sensitive ion channels (particularly ATP dependant K+ channels) via mechano-electric coupling and inward current for-mation.8,9,11,16,20,21,34,59 These cellular mechanisms augment non-uniform myocardial activation and cause premature ventricular depolarisa-tions that are the final triggers of VF in commotio cordis.1,34
Coronary artery vasospasm1,6 exces-sive autonomic vagal reflex1,6 varying degrees of myocardial contusion12 and prolonged QRS and QTc dura-tions (resting ECGs in animal sub-jects)15 may have a pathophysiologic role in commotio cordis but these have yet to be confirmed.
3. A narrow and compliant chest wall. The predisposition of com-motio cordis in the younger popula-tion may be directly related to their physical characteristics.24,25 A rela-tively underdeveloped chest cage with immature intercostal muscula-ture may be less capable of blunting the arrhythmogenic consequences of precordial forces.2,3 Adults gain a measure of protection from a fully developed and mature chest cage, which may help to explain the low incidence of commotio cordis in sports such as boxing or martial arts in older age groups.
4. Other factors that have been shown to increase the risk of commotio cordis include the size, shape and density of the object, where solid, hard, small and spherical projectiles have been shown to be directly related to VF.15,18,59
Anaesthetised animal subjects have shown a bell-shaped curve relationship between ball strike velocity and the induction of VF, with the highest incidences occurring at 64km/h (70% of strikes).1-3,19 Between 80 and 112 km/h (50–70 mph) the likelihood of VF decreased and the likelihood of cardiac rupture was shown to increase.59
PreventionPublic education on the importance of avoiding and preventing precordial blows, safety interventions to make impacts less forceful and improved
Typically, the individual is hit in the chest (with or without chest protection) usually by a pitched, thrown or batted dense projectile at high or low velocity (58% of occurrences) or by the force of bodily contact (42% of occurrences) with the majority of cases collapsing immediately.
Copyright: https://www.123rf.com/profile_stefanholm'>stefanholm / 123RF Stock Photo

Page 7 Volume 8 No 1 April 2017
automated external defibrillator (AED) availability, represent the most important primary and secondary intervention strategies that have been instituted to date, as pre-participation screening in young athletes for this presentation of SCD is simply not possible at present.
Enforced rule changes and technique correction for avoiding precordial impacts have been incorporated into many sports in the United States (e.g. teaching batters to turn away from errant baseball pitches, avoidance of the chest to block a ball or puck in lacrosse or ice hockey).25,26
The use of more suitable materials for various age group sports has been de-bated e.g. softer-than-standard safety baseballs1 were proposed at the 36th Bethesda Conference on Eligibility Rec-ommendations for Competitive Ath-letes with Cardiovascular Abnormali-ties for recreational and Little League baseball.18,36 The softer projectiles are presumed to be safer as their propen-sity to collapse would allow for greater dissipation of energy on impact.
Equipment design of various chest guards, have come under much investi-gation and scrutiny.10,25,27-29,58 Chest pro-tectors are designed more for greater movement and performance and not specifically with commotio cordis in mind. The use of inadequate materials for padding against blunt bodily trauma has been proven to be easily penetrable by projectiles and does not dissipate forces adequately enough. This has been documented for 32% of commo-tio cordis victims in American football, baseball, lacrosse and hockey.2,7,10,28,30 Newer chest wall protectors have shown linear correlations between ex-perimental combinations of novel ma-terials and an improved ability to dis-sipate forces. However, these are still being studied and are not as yet com-mercially available.58
The most important therapeutic measure is the increased availability
and familiarity of AEDs at all youth sporting events and recreational settings.1,31,47 As emergency services in most settings cannot possibly be expected to arrive on scene within the necessary time period (5 minutes) of a cardiac arrest, the expanded availability and use of AEDs even by persons with minimal training, may save a life by recognising and automatically terminating a fatal arrhythmia.3,26,32,33,47
ManagementCommotio cordis is managed as with any cardiopulmonary emergency as- sociated with a non-perfusing cardiac rhythm. The critical determinant of survival being the time to defibrilla-tion. CPR should be commenced until defibrillation is available. The updat-ed 2015 American Heart Association (AHA) Guidelines for Cardiopulmonary Resuscitation and Emergency Cardio-vascular Care, recommend immediate implementation of cardiopulmonary resuscitation (CPR) emphasising chest compressions after the emergency re-
sponse system is activated (C-A-B rath-er than A-B-C to reduce any delay to the first compression).60
Compression to ventilation ratio of 30:2 or initial external chest compression only CPR (no ventilation) at a compression rate of at least 100-120 per minute are recommended for adults and children above 1 year until modalities for defibrillation are available.47,60
The success rate of chest compression only CPR has been found to be at least similar to that of traditional compres-sion-ventilation CPR.47-53,60 It should only be considered in circumstances where rescuers are unwilling or unable to ventilate (e.g. infectious concerns)47,60 as many arrests in children will be hy-poxic in origin and ventilations are cru-cial for survival in these instances.57,60
Performing CPR while the AED or de-fibrillator is readied for use is strongly recommended57,60 as a shorter time in-terval between the last chest compres-sion and the first shock correlates di-rectly with the success of defibrillation. Chest compressions should resume im-mediately after a shock and should con-tinue for 2 minutes before a rhythm or pulse check is conducted.
High quality CPR, early recognition of a shockable rhythm and prompt defibrillation with an AED are the key interventions that have helped increase out of hospital survival rates of cardiac arrest subjects.57,60
A controversial issue that is still debated is the use of the precordial thump during resuscitative efforts. There are no prospective studies that have evaluated its efficacy in resuscitation attempts and recent studies have also shown the precordial thump to be ineffective in terminating VF.38-45 A single, immediate precordial thump may be considered after a witnessed cardiac arrest if a defibrillator is not present, but it should not delay prompt defibrillation if available.
Public education on the importance of avoiding and preventing precordial blows, safety interventions to make impacts less forceful and improved automated external defibrillator (AED) availability, represent the most important primary and secondary intervention strategies that have been instituted to date, as pre-participation screening in young athletes for this presentation of SCD is simply not possible at present.

Volume 8 No 1 April 2017 Page 8
Survival after a commotio cordis event is still the exception, as the severity of the injury is often underestimated and the aggressive activation of the chain of survival (early CPR, early defibrillation, followed by advanced life support measures) is therefore delayed.1-4,6 The duration and intensity of exercise prior to a commotio cordis arrest may allow for higher than normal endogenous catecholamine levels and a decreased systemic vascular resistance, which may also play a role in limiting the success rate of resuscitation.
Time to defibrillation is the single most important determinant of survival in cardiac arrest, as VF generally evolves into asystole within a matter of minutes.56 The probability of a successful defibrillation declines 7-10% per minute for every minute that defibrillation is delayed without CPR and 3-4% per minute with bystander CPR.1,37,56 Following induction of VF in anaesthetised animal subjects via blunt chest trauma, defibrillation after 1, 2, 4 and 6 minutes, showed survival rates of 100%, 92%, 46% and 25% respectively.17,56,59
Survival rates were only 3% if resuscitation efforts were delayed longer than 3 minutes and overall, survival trends following exercise-related sudden cardiac arrest from all causes in young athletes continues to be disappointing.1,37,56 According to the United States Commotio Cordis Registry,1-4 present survival rates for commotio cordis remain between 24-35%; which represents a low percentage given the absence of any structural cardiac abnormalities in these cases.
Patients with return of spontaneous circulation should be transferred to the nearest appropriate facility capable of providing post resuscitation care and ventilatory support.57 A complete cardiac evaluation, including a 12-lead ECG, ambulatory Holter monitoring, stress ECG and echocardiography, is advised for all survivors.
Echocardiography in survivors, has mostly shown normal anatomy and functioning post event. There has been no evidence of HOCM, anomalous coronary artery syndromes or aortic root dissection. Cardiac valves have also been shown to be normal in anatomy and functioning. There have been documented isolated incidences in some survivors of mildly diminished global left ventricular systolic function or limited areas of hypokinesis. However, these were all of short duration and resolved spontaneously with a few days.37,38
Rare chronic manifestations beyond this acute phase following blunt chest trauma have been reported weeks to months after a reported incident.59 These have been attributed to mono-morphic ventricular tachycardia (VT) and/or ventricular premature depo-larisations (VPDs) associated with in-homogeneous ventricular wall scarring and remodeling.59 These areas are char-acterised by zones of slow conduction due to non-uniform anisotropy, result-ing in fixed and/or functional regions of electrical conduction block.59 The management of these infrequent cases has included a combination of anti-ar-rhythmic medications and/or epicar-dial radio-frequency ablation.59
Eligibility for return to competitive sporting activity should be based on sound clinical judgment for that specific
individual. There is, at present, no evi-dence to suggest that survivors of com-motio cordis have a greater risk for any future arrhythmic events and accord-ingly, survivors cannot be disqualified from competitive action solely on the basis of a previous occurrence.1
ConclusionGeneral awareness of commotio cordis and all other possible causes of SCD in young athletes should be regularly updated.
As many of these tragic events cannot be completely prevented, accessible AEDs or field-side defibrillators, continued CPR training and updated emergency action plans, remain as some of the most important forms of management that are available for all causes of cardiac arrest in young athletes.47,59,60
Most schools and recreational sporting venues are unfortunately not equipped with even a single AED on their entire premises. If an AED is present, the location, availability, accessibility and proper use of the device also needs to be known. Emergency medical services and the presence of a defibrillator are usually present at organised events, but only if they have been part of the school’s medical preparation plan and if they are affordable for those few hours.
All sporting venues for practices and matches should have access to an AED, as delays in rapid defibrillation have been noted in this review and even though these sudden cardiac events are rare, by combining continued education with the abovementioned strategies and efforts, safer environments for all young individuals participating in sporting activities can be provided.
References available on request.
Eligibility for return to competitive sporting activity should be based on sound clinical judgment for that specific individual. There is, at present, no evidence to suggest that survivors of commotio cordis have a greater risk for any future arrhythmic events.

Page 9 Volume 8 No 1 April 2017
Dr Joe McKibbinCardiologist
Sunninghill Hospital, Johannesburg
The clinical value of the Coronary Artery Calcification Score
he Coronary Artery Calcifica-tion (CAC) Score which cor-relates closely with plaque burden, is now recognised to be the best predictor for fu-
ture coronary events. Glagov in 1987 demonstrated the positive remodelling of the coronary artery and compensato-ry enlargement due to atherosclerosis. Intravascular Ultrasound Studies (IVUS) have confirmed that the atheromatous plaques can spread around long seg-ments of the coronary arteries before luminal stenosis becomes evident. Plaque burden (quantity of atheroma) is the most important predictor of cardio-vascular events and is more predictive than severity of coronary stenosis (Schmermund et al 1997, Story et al, 2003). Nissen S et al followed 1039 pa-tients for 2 years following IVUS studies and correlated cardiac event rates with plaque burden and found each standard deviation increase in baseline burden was associated with a 28% increase in cardiac events. Therefore quantification of atherosclerotic burden is essential for accurate risk stratification.
What is the CAC Score? Since atheroma is an inflammatory process it attracts calcium and therefore the greater the plaque burden the greater will be the calcium volume. Coronary calcium is part of the development of atherosclerosis; it occurs exclusively in atherosclerotic arteries and is absent in the normal vessel wall. Coronary calcification is therefore pathognomonic of atherosclerosis (Budoff et al 2006). The close correlation between the extent of CAC and plaque burden has been confirmed both by histopathology and by IVUS studies (Mintz et al 1997, Baumgart 1998). Atheroma cannot be measured non-invasively but measurement of calcium in the coronary arteries has become very accurate with Computed Tomography (CT) scanning. The amount of calcium measured is proportional to the amount of atheroma; therefore the greater the CAC score the greater the plaque burden. Total CAC score represents an anatomic measurement of overall coronary plaque
burden. The measurement of calcium is expressed as the Agatston score. The score is calculated using a weighted value assigned to the highest density of calcification in a given coronary artery. The density is measured in Hounsfield units. This weighted score is then multiplied by the area (in square millimetres) of the coronary calcification. The calcium score of every calcification in each coronary artery for all of the tomographic slices is then summed up to give the total CAC score.
Utility of the CAC Score Coronary calcification therefore is a marker of atherosclerosis that can be accurately quantified and is proportional to the extent and severity of atherosclerotic disease. However, the CAC score does not necessarily reflect the severity of coronary stenosis and has low specificity for obstructive coronary disease. The main value of the CAC score is therefore not for diagnosis of coronary obstruction but for predicting future risk. It is a good predictor of coronary events and will identify the pool of patients from whom 95% of myocardial infarction (MI) and Acute Coronary Syndrome will emerge. On the other hand, the CAC score does have a very high negative predictive value i.e. zero calcification means very low probability of obstructive coronary disease. Two studies have shown coronary disease prevalence of 2-4% when the CAC is zero. Therefore CAC scoring does have a limited role in the diagnosis of coronary obstructive disease as demonstrated by the U.K. National Institute for Health and Care Excellence (NICE) guidelines in patients with recent onset chest pain where CAC scoring is recommended when the estimated probability of coronary disease is low (10-29%).
The conventional method for estimating multi-factorial absolute risk is performed with screening tools such as the Framingham Risk Score (FRS). But this method has limitations particularly in younger subjects less than 55 years because it is strongly weighted for age. Whereas those that are high risk
(>20% ten year risk) require aggressive preventive therapy (particularly statins). The majority of cardiovascular events occur in individuals at intermediate risk (10-20% ten year risk). Numerous long term studies have demonstrated that CAC score is a stronger independent predictor of future events than the sum of all the conventional risk factors combined and it outperforms FRS in predicting cardiovascular events. FRS predicts risk in large populations but has limited predictive value for an individual asymptomatic patient.
In the Heinz Nixdorf study, Erbel et al. demonstrated the superiority of CAC scoring over FRS when they followed, for five years, subjects with an Intermediate FRS (10-20% 10 year risk) in whom the CAC had been measured. Patients with scores below 100, had a low probability of event rates. But those patients with CAC scores greater than 400 demonstrated an event rate at five years of much greater than 10%. 75% were re-classified - 60% were re-classified as low risk and 14% re-classified as high risk. Hecht has shown that 67% of subjects that fall into the intermediate risk category can be re-classified as low risk or high risk based on the CAC score and even 45% of subjects classified as high risk can be re-classified as low or intermediate risk.
Akosah et al looked at 222 younger pa-tients (men <55, women <65) admit-ted with an MI and calculated FRS to determine how many would be classi-fied as high risk. They found that in men, only 25% were classified in this category (>20% risk) and in women only 18%. This illustrates that FRS underestimates the risk for disease in young adults and the majority would be denied statin therapy using this method, whereas if CAC scoring had been performed the majority would have been identified as being at risk and therefore treated with statins.
Grading of coronary atherosclerosis, based on the CAC score is generally classified as follows: No evidence of CAD:

Volume 8 No 1 April 2017 Page 10
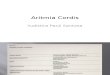
0 calcium score, minimal: 1-10, mild: 11-100, moderate: 101-400 and severe: >400. The above figure (M J Budoff) with mortality as the outcome, demonstrates the value of this measurement in 25000 subjects followed for 12 years.
The negative predictive value of CAC scoring is very evident from this graph. It is readily apparent that a CAC score of zero carries a 12 year risk of death from a cardiac event of almost zero. This has been confirmed recently by another group who showed that if the CAC score is zero and there are no other major risk factors, the mortality out to 15 years is extremely low. Even subjects over 75 years with a zero CAC score have been shown to have a 5.6 year survival of 98%. This has important practical implications since if no calcium is present then there is no atheroma present and treatment with a statin is not necessary. But as the CAC score increases there is a progressive increase in mortality. The exact level at which treatment with a statin is required depends on other variable factors but anyone with demonstrable calcium should be considered for statin therapy, and definitely all subjects with a score of greater than 400 should be treated. The BioMed study from UCLA followed 5600 subjects classified as low risk for 20 years. Mortality data was presented on no-, low-, moderate-, and high-calcium scores. With an average follow-up period of 10 years, even patients with low calcium scores (1–99) were 50% more likely to die than patients with a CAC score of zero. Moderate scores (100–399) were associated with an 80% greater likelihood of dying, and
high scores (above 400) were associated with a three-times-greater risk of dying as compared with patients with zero calcium. These patients had zero to one risk factor, including diabetes, hypertension, current smoking, or family history. Ten percent of these “low-risk” patients had a severe burden of coronary artery calcium of greater than 400.
CAC scoring has been shown to outperform Carotid Intima Media Thickness and hsCRP (high sensitive C-reactive protein) in predicting future cardiac events. The South Bay Heart Watch was the first study to compare the prognostic ability of CAC and hsCRP. This study followed out to 7 years showed that CAC was incremental in predicting cardiac risk with increasing scores while hsCRP failed to add independent prognostic value. Several other studies have confirmed this finding.
Many clinicians base their decision to treat patients with a statin on the cholesterol level alone but this is known to be a very poor predictor of future outcome in an individual (especially LDL, unless elevated above 4.7 mmol/l). And there is no correlation between LDL levels and amount of plaque. CAC scoring is a far better and validated method to make decisions on the need for statin therapy.
Uncertainty remains regarding the use of CAC in young patients less than 40 years. Young patients are likely to be categorised as low cardiovascular risk based on traditional cardiovascular risk factors, because the FRS heavily weights chronological age. Coronary plaque
is less likely to be calcified in young individuals. Although there have been a few studies such as one by Taylor et al. which assessed the predictive value of CAC in 1634 asymptomatic 40–50-year-old men and found that that CAC was independently predictive of CHD in those with an FRS more than 5%.
Two important issues with CAC scoring are cost and radiationThe average cost in South Africa for CAC screening is R4000.00. But cost issues may be outweighed by benefit. If subjects who are at high risk of MI and death because of a high CAC score are detected and treated early, later costs can be obviated. Conversely, those with zero calcification can avoid life-long treatment.
Radiation is an issue, and therefore routine population screening is not justifiable, nor is it for low risk individuals. However, with the latest software the radiation for CAC measurement has been reduced to 0.5 millisieverts (mSv). (Compare that to a mammogram which is 3 mSv! And how many women volunteer for this test annually?)
Who should be screened? Both the American Heart Association (AHA) and the European Society of Cardiology have suggested that it is reasonable to perform CAC testing in intermediate risk patients (10–20% 10-year risk), with the AHA extending this recommendation to low-intermediate risk patients (6–10% 10-year risk).
ConclusionCAC screening is by far the best way to predict the risk of future cardiac events. This is the best method to identify those at highest risk of having an MI. It does not make sense to put everyone with a slightly elevated cholesterol on to a statin, but rather perform this test and treat those with evidence of coronary atherosclerosis. David May stated: “Calcium scores are better predictors than routine exercise evaluation,” and Hecht stated, “If you’ve thought about doing a stress test on someone with no symptoms, do a calcium score first. There is no such thing as a false-positive calcium score. It is 100% accurate for coronary atherosclerosis.”
M Budoff. Ten year follow up for all cause mortality. Patients with scores >1000 had a 26% mortality rate, multiples higher than patients without coronary calcification.
Cumulati
veSurvival
TimetoFollow-up(Years)

Page 11 Volume 8 No 1 April 2017
Dr Jens HitzerothCardiologist
Vincent Pallotti Hospital, Pinelands, Cape Town
The role of heart rate in the management of heart failure
eart failure is a common condition, which most clinicians have to deal with on a daily basis. The prevalence of heart failure in
the adult population is reported to be 1 – 2% and the lifetime risk of heart failure at age 55 years is 28 – 33%.1
Significant progress has been made in the management of patients with heart failure with a reduced ejection fraction (HFrEF) over the last 20 years, and outcomes have improved accordingly. Despite improved heart failure treatment with contemporary medical therapy and device implantation, the prognosis of patients with HFrEF has remained poor. On average, 20% of patients will die within 1 year from diagnosis and the 5 year mortality is consistently reported to be about 50%.2
Apart from highlighting the clear need for new, improved remedies for HFrEF, this also emphasises the importance of optimal usage of currently available therapies.
Various studies have confirmed the adverse prognostic impact of a high resting heart rate in patients with heart failure and recent studies seem to suggest that it may indeed be a modifiable risk factor. Heart rate lowering as a target in heart failure management may therefore be an attractive strategy to achieve better outcomes in our heart failure patients.
Resting heart rate and life expectancyIt is not infrequent that one encounters the somewhat frivolous notion that humans have a predetermined amount of heart beats and death ensues when this total has been reached. The logical conclusion of this theory is of course that a higher heart rate will invariably result in a lower life expectancy.
Surprisingly, there is an element of truth in this surmise. In mammals, the number of heart beats per lifetime is remarkably constant and animals with the shortest life span have a correspondingly higher
resting heart rate, whereas those with the highest life expectancy have the lowest heart rates.3 So far there have not been any conclusive studies to show that purely lowering resting heart rate results in prolongation of life in humans.
In the general population a high resting heart rate is associated with a poorer outcome. In the Framingham Study the risk of cardiovascular disease, cardiovascular mortality and maybe somewhat unexpectedly all-cause mortality increased progressively with an increasing resting heart rate. Multiple studies have confirmed these data.4
In the context of cardiovascular disease, an elevated resting heart rate is strongly associated with mortality in various illnesses, including hypertension, diabetes, HFrEF and after myocardial infarction. It has been shown that in particular in the setting after myocardial infarction as well as LV dysfunction resting heart rate is an independent predictor of mortality.5 It has, however, not been possible to distinguish whether an elevated heart rate is merely a marker for increased risk of dying or whether it truly represents a modifiable risk factor that contributes to poor outcomes in patients with LV dysfunction.
Heart rate and heart failureIn patients with heart failure a major pathophysiological phenomenon is the increase in sympathetic activity while vagal tone is reduced, which results in an increased heart rate. Whilst beneficial in the short term, to maintain cardiac output, this autonomic imbalance ultimately leads to worsening cardiac function, in part as a consequence of a higher resting heart rate.
The elevated heart rate has various pathophysiological consequences. Oxygen consumption is increased with chronic ischaemia, calcium handling is abnormal, there is downregulation of beta-1 receptors, and depletion of myocardial energy stores.
The concept of a high heart rate, resulting in worsening left ventricular function is most dramatically illustrated by the entity described as a tachycardia induced cardiomyopathy (TIC). This cardiomyopathy is caused by various tachyarrhythmias (atrial fibrillation/flutter, incessant supraventricular tachycardia, ventrntricular tachycardia) and is often reversible once the heart rhythm has been treated and heart rate has normalised.6
There is therefore a good pathophysi-ological basis for heart failure therapies that specifically reduce heart rate.
Therapeutically reducing heart rate It is interesting to note that one of the first agents to be used in the treatment of HFrEF and one to this day not infrequently prescribed therapy in heart failure patients – digoxin – enhances vagal tone and to some extent reduces heart rate. It has a narrow therapeutic index and its toxicity has probably offset potential heart failure7 benefits but in the only randomised trial of digoxin to date, digoxin compared to placebo did lower the risk of hospital admissions for heart failure.
Beta-blockers were first studied in patients with cardiomyopathy in the 1970s.8 Although they now form an in-tegral part of heart failure management, their exact mechanism for improved survival is still uncertain. It has been demonstrated that in patients with HFrEF treated with bisoprolol the asso-ciated heart rate reduction as opposed to blood pressure reduction is related to longer survival.9 This would suggest that the heart rate lowering effects of beta-blockers may well be in part di-rectly responsible for the improved out-comes in patients with HFrEF.
This finding has been consistent in other trials. In an analysis of the COMET trial which compared metroprolol and carvedilol in patients with HFrEF, heart rate reduction was an independent predictor of mortality.10

Volume 8 No 1 April 2017 Page 12
Additionally, a meta-analysis was published in 2008, which encompassed most of the landmark beta-blocker trials in HFrEF. These have indicated that a major contributor to the benefits of beta-blocker therapy in patients with heart failure with poor LV function may be the heart rate lowering effect of these agents.11
Interestingly, yet another meta-analysis, that looked at beta-blocker dose, heart rate reduction and death showed that the magnitude of the heart rate reduction achieved was associated with the survival benefit of beta-blockers, whereas, surprisingly the beta-blocker dose of the beta-blocker was not.12
Lastly, a small study done in patients with permanent pacemakers with LV dysfunction on beta-blockers, randomised these to be paced at a rate of 60 beats per minute compared to a rate of 80 beats per minute. This showed a greater decline in left ventricular function in the group of patients that was paced at the higher rate despite similar beta-blocker uptake in both study arms.13 Although the study is not conclusive, the result further supports the notion that heart rate plays a direct role in the pathophysiology of heart failure.
The data seem to suggest then, that the mechanism of the survival benefit of beta-blocker is largely related to their heart rate lowering effect.
Yet further evidence to support the notion that heart rate is not merely a marker of risk in patients with heart failure but actually is a modifiable risk factor, comes from the recent SHIFT trial.
In the SHIFT trial ivabradine was compared to placebo in an HFrEF population on standard background medical therapy. Ivabradine is a specific heart rate lowering agent. It slows down the sinus rate by inhibiting the If channel without any significant other physiological effects. The SHIFT trial then lends itself to evaluating the effect
of heart reduction on heart failure outcome. The placebo group had an average heart rate of 75 bpm compared to the treatment group’s average heart rate of 67 bpm. Although the trial did not show a statistically significant reduction in cardiovascular mortality, it did show a reduction in both hospital admissions for worsening heart failure (hazard ratio 0.74) as well as the risk of death from heart failure (hazard ratio 0.74).14
Subsequent analyses of the SHIFT trial population confirmed that the risk of the primary endpoint (cardiovascular death or hospital admission for worsening heart failure) increased by 16% for every 5 bpm increase in heart rate.15 It has additionally been shown that heart rate reduction in patients with heart failure resulted in improved quality of life scores.16
Heart rate therefore is an important parameter to be measured in patients with HFrEF. If it is elevated, heart failure therapy should probably be escalated to achieve lower heart rate. There is unfor-tunately little data to guide us as to what target heart should be lowered to, to op-timally benefit our patients. There is also no data available to guide us as to what agents should be used to achieve this.
The latest European Society of Cardiology Guidelines for heart failure management recommend ivabradine in patients with HFrEF whose heart rate remains above 70 beats per minute, despite treatment with maximally tolerated evidence-based dosages of beta-blockers, ACE-inhibitors (or angiotensin receptor blockers) and mineralocorticoid receptor antagonists. (Class IIb recommendation).1
ConclusionHeart rate is strongly associated with the risk of mortality in both the general population as well as in patients with cardiovascular disease, including patients who have HFrEF.
Although the pathophysiology of HFrEF is complex, sympathetic activation is a major part of the disease process. It is
very likely that the associated elevated heart rate is a significant contributor to worsening heart failure.
Current data confirms that an elevated resting heart rate is associated with a poorer prognosis. It furthermore suggests that heart rate is a modifiable risk factor and should be a target for therapy in patients with heart failure.
It should be emphasised that this must not be at the expense of treating the patient with existing, proven therapy and every effort should be made to treat the patient with at least an ACE-inhibitor or ARB (or if available an angiotensin receptor neprilysin inhibitor), MRA and beta-blocker titrated to target dosage as evaluated in clinical trials.
References1. Ponikowski P, Voors AA, Anker SD,
Bueno H, Cleland JGF, Coats AJS, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2016;37(27):2129–2194.
2. Gerber Y, Weston S a, Redfield MM, Chamberlain AM, Manemann SM, Jiang R, et al. A contemporary appraisal of the heart failure epidemic in olmsted county, Minnesota, 2000 to 2010. JAMA Intern Med. 2015;175(6):996–1004.
3. Levine HJ. Rest heart rate and life expectancy. J Am Coll Cardiol. 1997;30(4):1104–6.
4. Cook S, Togni M, Schaub MC, Wenaweser P, Hess OM. High heart rate: A cardiovascular risk factor? Eur Heart J. 2006;27(20):2387–93.
5. Fosbøl EL, Seibæk M, Brendorp B, Moller DV, Thune JJ, Gislason GH, et al. Long-term prognostic importance of resting heart rate in patients with left ventricular dysfunction in connection with either heart failure or myocardial infarction: The DIAMOND study. Int J Cardiol. 2010;140(3):279–86.
References 6-16 available on request.

Page 13 Volume 8 No 1 April 2017
Dr B Hobson MBChB MMed (Fam), Dr JS Roos MBChB MMed (Int), Dr F Lubbe MBChB MMed (Neurol) FC (neuro)Medi-Clinic Vergelegen, Somerset West, Western Cape
Antiphospholypid syndrome: Important diagnosis but often missed
ntiphospholipid antibody syndrome (APS) is defined as an acquired autoim-mune disorder resulting in a hypercoagulable state
caused by anti-phospholipid antibod-ies.1,2,3 It is a multidisciplinary disorder of concern for general practitioners, physicians, cardiologists, neurologists and gynecologists. It affects about 50-100000 people, mostly young and mid-dle aged females.
Anti-phospholipid syndrome arises from an abnormal acquired immune response towards normal tissues in the body, affecting the coagulation system.1,4 This autoimmune response provokes the making of antibodies, a protein that is responsible for defending the body against infections, which mistakingly then attacks phospholipids and cause damage to cells. Phospholipids are fat cells found in all living cells and cell membranes.4 The damaged cells provoke clotting, resulting in thrombosis (arteries, venous and microvascular) and/or pregnancy complications.1,2,3
ClinicalAntiphospholipid antibody syndrome is either primary or secondary.
Primary APS occurs in the absence of any related autoimmune disease. These patients don't have any clinical or labo-ratory evidence of any other causative disease. Primary APS rarely progresses to Systemic Lupus Erythematosis (SLE). Secondary APS occurs in the presence of other autoimmune diseases, mainly SLE (10%). Occasionally other auto-immune conditions, infections, drugs and malignancies are associated.2 Very rarely diffuse microvascular thrombosis, Catastrophic APS, leads to acute multi-organ failure and possibly death.1,2 A percentage of the population will have anti-phospholipid antibodies when test-ed randomly. The incidental finding of a single antibody (either anti-cardiolipin, B2-glycoprotein or anti-prothrombin) is not associated with increased risk of thrombosis.
Venous thrombosis occurs most commonly as deep vein thrombosis (DVT) in the legs or a pulmonary embolism. Arterial thrombosis mostly commonly affects the cerebral vascular system, resulting in a transient ischaemic attack (TIA) or stroke. Myocardial infarcts are less common. Microvascular involvement presents as multi-organ disease. Pregnancy complications often presents as multiple miscarriages in the first trimester or late pregnancy fetal loss.1,2
DiagnosisAPS is diagnosed in patients with venous, arterial, microvascular thrombosis or pregnancy complications, failure who has persistent anti-phospholipid antibodies.1,2
Laboratory finding consist of three groups of antibody detection. • Plasma anti-cardiolipin antibodies • enzyme-linked immunosorbent as-
say (ELISA) detecting plasma B2-glycoprotein antibodies
• Anti-prothrombin antibodies. Car-diolipin antibody detection is most specific. Any of these antibodies found on two or more occasions, at least 12 weeks apart, together with one or more clinical finding is diag-nostic of APS.
Some people have anti-phospholipid antibodies but never develop anti-phospholipid antibody syndrome.
APS does not have a cure. Early diag-nosis and preventative anticoagulation treatment, decreases the risk of associ-ated complications.1,2
TreatmentIt is not recommended to initiate primary thromboprophylaxis in the general population with incidentally detected anti-phospholipid antibodies.1,2
Patients with unprovoked venous throm-bosis (DVT or pulmonary embolism) and positive anti-phospholipid antibody tests, should be treated with warfarin as the
risk of recurrence is high. Patients with provoked venous thrombosis are treated for three months and re-evaluated. Pa-tients with a history of stroke and a single positive anti-phospholipid antibody test should be treated with either warfarin or aspirin. There is no evidence to show that warfarin is superior to anti-platelet therapy in these patients. Young patients (<50 years) with a history of stroke and a single positive anti-phospholipid anti-body test should be treated with warfa-rin, as recurrence is very high. Women with recurrent pregnancy loss and posi-tive anti-phospholipid antibodies should be treated with low dose aspirin and low molecular weight heparin (LMWH). Pregnant women with a history of pre-eclampsia or fetal growth restriction and positive anti-phospholipid antibodies should be treated with aspirin.1
Management of other risk factor such as hypercholesterolemia, diabetes and hypertension is part of the overall treatment of APS patients.
Currently there is no place for NOAC in treating APS, but it may become part of the management in future.
Case studiesPresenting three case studies.
Case 1A 48 year old female patient presented to various doctors complaining of episodes of weakness on the left, a noticeable change in speech and off balance gait. These symptoms did not last long. She is known with hypertension, hyperlipidemia and epilepsy. There was no history of recent seizures. In light of her epilepsy, her symptoms were attributed to seizures.
She then presented at MediClinic casualty with an acute stroke causing left hemiparesis, dysarthria and ataxia (NIHS score of 7). She presented outside the window period of standard stroke TPA therapy. From her previous history it was deduced that she most likely suffered TIA's rather than seizures.

Volume 8 No 1 April 2017 Page 14
Laboratory findings showed a strongly positive cardiolipin antibody IgM test, a high total cholesterol of 6.6 with a high low density cholesterol (LDL) of 3.9. Other strongly associated anti-phospholipid syndrome autoimmune disease tests and the hereditary thrombolitic profile was negative. There was no history of pregnancy complications.
On admission her blood pressure was stable. Neurologically she had a left hemiparesis, ataxia and dysarthria. The only other clinical finding was a soft systolic murmur over the mitral valve area of non-significance was audible.
Cardiac Echo only showed mild mitral valve regurgitation. Carotid Intimal Thickness (IMT) was within normal limits.
Electro Cardiogram was normal (ECG).Holter study was normal.
MRI showed numerous subcortical white matter disease, microvascular disease and fronto-temporal brain atrophy.
The patient was referred to a local neurologist and discharged on her chronic epilepsy medication, Prexum Plus, statins and warfarin therapy. Follow up showed that the patient was doing well with most of the stroke symptoms having resolved. No seizures were reported.
Case 2A 22 year old female patient presented at casualty with a history of symptoms suggestive of possible previous TIAs, now with an acute stroke, causing right sided weakness involving the arm, leg and face, dysarthria and dysphasia (NHIS score 8).
Laboratory findings showed a strongly positive cardiolipin antibody IgM and IgG, Anti-B2-glycoprotein IgG and IgM anti-bodies test. The ANF and anti-DNA auto-antibody screen was significantly positive. Cholesterol study and lipopro-tein A was normal. Hereditary throm-bolitic profile was negative.
On admission her blood pressure was stable. A soft systolic murmur over the mitral valve area of non-significance was audible.
Trans-esophageal Echo (TOE) only showed mild mitral regurgitation. There was no evidence of a PFO or ASD. IMT was within normal limits.
Perfusion MRI showed large acute ischemic infarcts in the Insula, left frontal and temporal lobes and three smaller infarcted areas in the left posterior parietal lobe. There was occlusion of one of the three branches of the second segment of the left middle cerebral artery, without dissection.
ECG was normal.
Holter study was normal.
Diagnosis was Ischemic stroke with APS and a positive lupus anti-coagulant. Currently the patient did not have any SLE symptoms, but she was warned to observe for clinical symptoms in future.
The patient was discharged on warfarin therapy. Follow up showed significant improvement in symptoms.
Case 3A 58 year old female patient presented at casualty with a history of 3 episodes of left sided arm and leg weakness. Each episode lasted about 20 minutes.
Inbetween she was completely normal. Her speech or vision was never affected.
Previous medical history was glaucoma, post-menopause and hypertension.
ECG was normal.
Holter study was normal.
TEE excluded PFO. Carotid intimal thickness (IMT) was normal. Carotid dopplers showed plaque formation without flow obstruction.
Laboratory findings showed a strongly positive Cardiolipin antibody IgM, Anti-B2-glycoprotein IgM anti-bodies test. Hereditary thrombolitic profile, ANF and anti-DNA auto-antibody screen was negative. Total Cholesterol (5.6) and LDL (4.1) increased. Lipoprotein small A was normal.
Perfusion MRI showed a small granuloma in the left fronto-parietal cortex. In the right Sylvian fissure a small aneurysm was suspected, which would be followed up.
The diagnosis was symptomatic stroke with anti-phospholipid syndrome. She was discharged on statins and warfarin therapy. Follow up showed that the patient was doing well with most of the stroke symptoms having resolved.
References1. Guidelines on the investigation...BJH2. h t t p s : / / w w w. n h l b i . n i h . g o v /
antiphospholipid3. https://en.wikipedia.org/wiki/
Antiphospholipid_syndrome4. https://en.wikipedia.org/wiki/
Autoimmune_disease

For further product information contact PHARMA DYNAMICS P O Box 30958 Tokai Cape Town 7966 Tel 021 707 7000 Fax 021 701 5898 Email [email protected] CUSTOMER CARE LINE 0860 PHARMA (742 762) www.pharmadynamics.co.zaPearinda 4. Each tablet contains 4 mg perindopril tert-butylamine. Reg. No.: RSA S3 A41/7.1.3/0649. NAM NS2 10/7.1.3/0476. Pearinda 8. Each tablet contains 8 mg perindopril tert-butylamine. Reg. No.: RSA S3 A41/7.1.3/0650. NAM NS2 10/7.1.3/0477. For full prescribing information, refer to the package insert approved by the Medicines Control Council, April 2009. Pearinda Plus 4. Each tablet contains 4 mg perindopril tert-butylamine and 1,25 mg indapamide. Reg. No.: RSA S3 A41/7.1.3/0633. NAM NS2 10/7.1.3/0611. For full prescribing information, refer to the package insert approved by the Medicines Control Council, April 2010. 1) The EUROPA study Investigators. “Effi cacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomized, double-blind, placebo-controlled, multicentre trial (the EUROPA study)”. The Lancet 2003;362:782-788. 2) The PREAMI study Investigators. “Effects of angiotensin-converting enzyme inhibition with perindopril on left ventricular remodelling and clinical outcome. Results of the randomized perindopril and remodelling in elderly with acute myocardial infarction (PREAMI) study”. Arch Intern Med 2006;166:659-666. 3) PROGRESS Collaborative Group. “Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack”. The Lancet 2001;358:1033-41. 4) Guerin AP, et al. “Impact of Aortic Stiffness Attenuation on Survival of Patients in End-Stage Renal Failure”. Circulation 2001;103;987-992. 5) Department of Health website http//www.doh.gov.za – Accessed on 29/03/2016. PAF291/04/2016.
Perindopril has proven outcomes in:• Coronary Artery Disease1
• Acute Myocardial Infarction2
• Stroke3
• End-stage Renal Failure4
Need endurancewhen treating CVS disease?
the affordable5 endurance ACE-inhibitor
A Lupin Group Company
PAF291/04/2016_A4_FINAL_6May2016.indd 1 2016/05/11 11:06 AM

Sponsored in the interests of continuing medical education by:
CPD Accredited
For further product information contact PHARMA DYNAMICS P O Box 30958 Tokai Cape Town 7966 Tel 021 707 7000Fax 021 701 5898 Email [email protected] CUSTOMER CARE LINE 0860 PHARMA (742 762) www.pharmadynamics.co.za
Prescribe a Pharma Dynamics product.
It’s a smart call.
CALCIUM CHANNEL BLOCKERS
enap enalapril maleate
5 mg, 10 mg,20 mg
Pearindaperindopril tert-
butylamine4 mg, 8 mg
ACE INHIBITORS
ß BLOCKERS
bilocorbisoprolol fumarate
5 mg, 10 mg
Pharma Dynamics
clopidogrel75 mg
ANTIPLATELET
nifedipine30 mg, 60 mg
THIAZIDE-LIKE DIURETIC
SR 1,5 mg
STATINS
atorvastatin10 mg, 20 mg,40 mg, 80 mg
simvastatin10 mg, 20 mg,
40 mg
ACE / DIURETIC
perindopril tert-butylamine /indapamide
4 mg / 1,25 mg
Pearinda
ANGIOTENSIN II RECEPTOR BLOCKERS
doxazosin 4 mg
α BLOCKER PDE5 INHIBITOR
sildenafi l50 mg, 100 mg
ARB / DIURETIC
SULPHONYLUREA
SR 30 mg
bisoprolol fumarate / HCTZ2,5 mg / 6,25 mg5 mg / 6,25 mg10 mg / 6,25 mg
ß BLOCKER /DIURETIC
carvedilol6,25 mg, 12,5 mg,
25 mg
amlodipine5 mg, 10 mg
irbesartan150 mg, 300 mg
losatan potassium50 mg, 100 mg
losatan potassium / HCTZ50 mg / 12,5 mg100 mg / 25 mg
valsartan / HCTZ80 mg / 12,5 mg160 mg / 12,5 mg160 mg / 25 mg
telmisartan40 mg, 80 mg
Amloc 5 mg. Each tablet contains amlodipine maleate equivalent to 5 mg amlodipine. S3 A38/7.1/0183. NAM NS2 06/7.1/0011. Amloc 10 mg. Each tablet contains amlodipine maleate equivalent to 10 mg amlodipine. S3 A38/7.1/0147. NAM NS2 06/7.1/0012. Bilocor 5. Each tablet contains 5 mg bisoprolol fumarate. S3 A38/5.2/0053. NAM NS2 06/5.2/0061. Bilocor 10. Each tablet contains 10 mg bisoprolol fumarate. S3 A38/5.2/0051. NAM NS2 06/5.2/0062. Bilocor Co 2,5/6,25. Each tablet contains 2,5 mg bisoprolol fumarate and 6,25 mg hydrochlorothiazide. S3 A44/7.1.3/1010. NAM NS2 13/7.1.3/0260. Bilocor Co 5/6,25. Each tablet contains 5 mg bisoprolol fumarate and 6,25 mg hydrochlorothiazide. S3 A44/7.1.3/1011. NAM NS2 13/7.1.3/0261. Bilocor Co 10/6,25. Each tablet contains 10 mg bisoprolol fumarate and 6,25 mg hydrochlorothiazide. S3 A44/7.1.3/1012. NAM NS2 13/7.1.3/0262. Carvetrend 6,25 mg. Each tablet contains 6,25 mg carvedilol. S3 A37/7.1.3/0276. NAM NS2 08/7.1.3/0105. Carvetrend 12,5 mg. Each tablet contains 12,5 mg carvedilol. S3 A37/7.1.3/0277. NAM NS2 08/7.1.3/0104. Carvetrend 25 mg. Each tablet contains 25 mg carvedilol. S3 A37/7.1.3/0278. NAM NS2 08/7.1.3/0103. Carzin XL. Each tablet contains 4 mg doxazosin. S3 A41/7.1/0557. NAM NS2 10/34/0376. Pharma Dynamics Clopidogrel 75 mg. Each tablet contains 75 mg clopidogrel. S3 A42/8.2/0128. NAM NS2 10/7.1/0377. Dynafi l 50 mg. Each tablet contains 50 mg sildenafi l. S4 A42/7.1.5/1071. NAM NS2 13/7.1.5/0086. Dynafi l 100 mg. Each tablet contains 100 mg sildenafi l. S4 A42/7.1.5/1072. NAM NS2 13/7.1.5/0087. Dyna Gliclazide SR 30 mg. Each tablet contains 30 mg gliclazide. S3 A42/21.2/0249. NAM NS2 12/21.2/0110. Dyna Indapamide SR. Each tablet contains 1,5 mg indapamide. S3 A42/7.1/0790. NAM NS2 12/7.1/0138. Dynarb 150 mg. Each tablet contains 150 mg irbesartan. S3 A43/7.1.3/0720. NAM NS2 12/7.1.3/0223. Dynarb 300 mg. Each tablet contains 300 mg irbesartan. S3 A43/7.1.3/0721. NAM NS2 12/7.1.3/0224. Dynator 10 mg. Each tablet contains 10 mg atorvastatin. S4 A43/7.5/0167. NAM NS2 13/7.5/0111. Dynator 20 mg. Each tablet contains 20 mg atorvastatin. S4 A43/7.5/0168. NAM NS2 13/7.5/0112. Dynator 40 mg. Each tablet contains 40 mg atorvastatin. S4 A43/7.5/0169. NAM NS2 13/7.5/0113. Dynator 80 mg. Each tablet contains 80 mg atorvastatin. S4 A43/7.5/0170. NAM NS2 13/7.5/0114. Dynaval Co 80/12,5 mg. Each tablet contains 80 mg valsartan and 12,5 mg hydrochlorothiazide. S3 A44/7.1.3/0018. NAM NS2 14/7.1.3/0061. Dynaval Co 160/12,5 mg. Each tablet contains 160 mg valsartan and 12,5 mg hydrochlorothiazide. S3 A44/7.1.3/0019. NAM NS2 14/7.1.3/0062. Dynaval Co 160/25 mg. Each tablet contains 160 mg valsartan and 25 mg hydrochlorothiazide. S3 A44/7.1.3/0020. NAM NS2 14/7.1.3/0063. Enap 5 mg. Each tablet contains 5 mg enalapril maleate. S3 A34/7.1.3/0085. NAM NS2 04/7.1.3/1138. Enap 10 mg. Each tablet contains 10 mg enalapril maleate. S3 A34/7.1.3/0086. NAM NS2 04/7.1.3/1137. Enap 20 mg. Each tablet contains 20 mg enalapril maleate. S3 A34/7.1.3/0087. NAM NS2 04/7.1.3/1136. Fedaloc 30 mg SR. Each tablet contains 30 mg nifedipine. S3 A37/7.1/0302. NAM NS2 10/7.1/0033. Fedaloc 60 mg SR. Each tablet contains 60 mg nifedipine. S3 A37/7.1/0303. NAM NS2 10/7.1/0034. Pearinda 4. Each tablet contains 4 mg perindopril tert-butylamine. S3 A41/7.1.3/0649. NAM NS2 10/7.1.3/0476. Pearinda 8. Each tablet contains 8 mg perindopril tert-butylamine. S3 A41/7.1.3/0650. NAM NS2 10/7.1.3/0477. Pearinda Plus 4. Each tablet contains 4 mg perindopril tert-butylamine and 1,25 mg indapamide. S3 A41/7.1.3/0633. NAM NS2 10/7.1.3/0611. Simvacor 10 mg. Each tablet contains 10 mg simvastatin. S4 A35/7.5/0237. NAM NS2 04/7.5/1660. Simvacor 20 mg. Each tablet contains 20 mg simvastatin. S4 A35/7.5/0238. NAM NS2 04/7.5/1659. Simvacor 40 mg. Each tablet contains 40 mg simvastatin. S4 A39/7.5/0132. NAM NS2 07/7.5/0166. Tesar 40 mg. Each tablet contains telmisartan 40 mg. S3 A45/7.1.3/0978. NAM NS2 17/7.1.3/0023. Tesar 80 mg. Each tablet contains telmisartan 80 mg. S3 A45/7.1.3/0979. NAM NS2 17/7.1.3/0024. Zartan 50 mg. Each tablet contains 50 mg losartan potassium. S3 A41/7.1.3/0287. NAM NS2 08/7.1.3/0067. Zartan 100 mg. Each tablet contains 100 mg losartan potassium. S3 A41/7.1.3/0289. NAM NS2 08/7.1.3/0086. Zartan Co 50/12,5. Each tablet contains 50 mg losartan potassium and 12,5 mg hydrochlorothiazide. S3 A42/7.1.3/1068. NAM NS2 12/7.1.3/0070. Zartan Co 100/25. Each tablet contains 100 mg losartan potassium and 25 mg hydrochlorothiazide. S3 A42/7.1.3/1069. NAM NS2 12/7.1.3/0071. For full prescribing information, refer to the package insert approved by the Medicines Control Council.1) IMS Data December 2016. CVSG366/04/2017.
CVSLARGEST
COMPANYIN SA1
CVSG366/04/2017_A4_8Mrch2017.indd 1 2017/03/13 9:20 AM