Embed Size (px)
Citation preview

J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 5 , N O . 2 2 , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 5 . 0 4 . 0 2 4
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
Cardio-Pulmonary-Renal Interactions
A Multidisciplinary ApproachFaeq Husain-Syed, MD,*y Peter A. McCullough, MD, MPH,zx Horst-Walter Birk, MD,y Matthias Renker, MD,kAlessandra Brocca, MSC,* Werner Seeger, MD,y Claudio Ronco, MD*
ABSTRACT
Fro
Me
Gie
He
Div
rec
tha
Lis
Ma
Over the past decade, science has greatly advanced our understanding of interdependent feedback mechanisms
involving the heart, lung, and kidney. Organ injury is the consequence of maladaptive neurohormonal activation,
oxidative stress, abnormal immune cell signaling, and a host of other mechanisms that precipitate adverse
functional and structural changes. The presentation of interorgan crosstalk may include an acute, chronic, or acute
on chronic timeframe. We review the current, state-of-the-art understanding of cardio-pulmonary-renal interac-
tions and their related pathophysiology, perpetuating nature, and cycles of increased susceptibility and reciprocal
progression. To this end, we present a multidisciplinary approach to frame the diverse spectrum of published
observations on the topic. Assessment of organ functional reserve and use of biomarkers are valuable clinical
strategies to screen and detect disease, assist in diagnosis, assess prognosis, and predict recovery or progression
to chronic disease. (J Am Coll Cardiol 2015;65:2433–48) © 2015 by the American College of Cardiology
Foundation.
T he concept of organ crosstalk refers to thecomplex biological communication andfeedback between different organs, medi-
ated via mechanical, soluble, and cellular mecha-nisms. Although crosstalk is essential to maintainbody homeostasis, pathological states in 1 or moreorgans can lead to functional and structuraldysfunction in other organs. The classification ofcardiorenal syndromes has been expanded into 5subtypes. Types 1 and 2 involve acute and chroniccardiovascular disease scenarios leading to acutekidney injury (AKI) or accelerated chronic kidneydisease (CKD). Types 3 and 4 describe AKI andCKD, respectively, leading primarily to heart fai-lure (HF), although it is possible that acute coro-nary syndromes, stroke, and arrhythmias could be
m the *International Renal Research Institute of Vicenza, San Bortolo
dicine II, University Clinic Giessen and Marburg Lung Center, Member
ssen, Giessen, Germany; zBaylor University Medical Center, Baylor Heart a
art and Vascular Hospital, Dallas, Texas; xThe Heart Hospital, Plano, T
ision of Cardiology and Angiology, University Clinic Giessen and Marburg
eived honoraria from GE, Fresenius Medical Care, Baxter, Asahi, Otsuka,
t they have no relationships relevant to the contents of this paper to dis
ten to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Vale
nuscript received March 24, 2015; revised manuscript received April 18, 2
cardiovascular disease outcomes in these forms ofCRS. Finally, CRS type 5 describes a systemic insultto both the heart and the kidneys, such as sepsis,where both organs are injured simultaneously inpersons with previously normal heart and kidneyfunction at baseline. Pulmonary-renal syndromesrepresent heterogeneous clinical entities, describedby a combination of diffuse alveolar hemorrhageon the basis of pulmonary capillaritis in conjunctionwith glomerulonephritis as well as acute respiratorydistress syndrome (ARDS) associated with AKI in theabsence of hematuria. Hepatorenal syndrome caninvolve the development of functional cardiopulmo-nary changes and AKI in patients with advancedliver failure (acute or chronic) and is beyond thescope of this review.
Hospital, Vicenza, Italy; yDepartment of Internal
of the German Center for Lung Research—Campus
nd Vascular Institute, Baylor Jack and Jane Hamilton
exas; and the kDepartment of Internal Medicine I,
—Campus Giessen, Giessen, Germany. Dr. Ronco has
Astute, and Toray. All other authors have reported
close.
ntin Fuster.
015, accepted April 20, 2015.

ABBR EV I A T I ON S
AND ACRONYMS
AKI = acute kidney injury
ARDS = acute respiratory
distress syndrome
BNP = B-type natriuretic
peptide
CKD = chronic kidney disease
CPRI = cardio-pulmonary-renal
interactions
FGF = fibroblast growth factor
GFR = glomerular filtration
rate
HF = heart failure
LV = left ventricular
PH = pulmonary hypertension
Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2434
CARDIO-PULMONARY-RENAL
INTERACTIONS: NEED FOR
DEFINITION OF A SYNDROME?
With growing knowledge of interdependentfeedback mechanisms involved in the heart,lung, and kidney crosstalk, the descriptiveclassification of a syndrome can represent aframework for exploring epidemiology,pathophysiology, detection, and manage-ment. Because of the complicated courses ofhospitalization and the high mortality ofpatients with involvement of all 3 organs,an integrative approach is needed. Thesequence of organ involvement can varydepending on the acuity and nature of theunderlying disorder. Many patients with
disorders of 1 organ (e.g., CKD) die of complications ofthe other (e.g., HF) before the first organ’s failurereaches its fullest extent, or the dysfunction of everyorgan may develop slowly until a “collapse” isreached and full-blown decompensation occurs. Thatis, each dysfunctional organ has the ability to initiateand perpetuate mutual injury through hemodynamic,neurohormonal, and cell signaling feedback mecha-nisms, while multiple episodes of acute (on chronic)decompensation may lead to reciprocal end-organdisease progression (Central Illustration). Given themultitude of contributing factors and the timesequence of events in cardio-pulmonary-renal in-teractions (CPRI), it is challenging to identify theunderlying pathophysiological mechanisms anddevelop a strategy for diagnostic and therapeuticintervention. This review summarizes recent ad-vances in our understanding of CPRI.
LUNG IN ORGAN CROSSTALK:
THE PULMONOLOGIST’S VIEW
Open to environmental influence, the lung is a highlyimmunologic organ, representing a gateway to theenvironment. The lung has critical pathophysiolog-ical connections to the failing heart and kidney(Figure 1A).
LUNG INJURY, ABNORMAL CELL SIGNALING, AND
OXIDATIVE STRESS. The lung conducts gas exchangevia 3 mechanisms: ventilation, diffusion, and perfu-sion. Any imbalance can cause respiratory distur-bance, which can be compensated to a certain degreeby hyperventilation, greater oxygen extraction fromblood by the tissues, and increased cardiac output,depending on the organ’s functional reserve. In bothnoncardiogenic and cardiogenic pulmonary edema,fluid accumulation in the fissure and alveolar spaces
can be seen as a result of increased pulmonarycapillary permeability, elevated intravascular hydro-static pressure, low colloid osmotic pressure, andinsufficient lymphatic drainage (1). Changes to thealveolar-capillary barrier can induce an inflammatorycascade and oxidative stress of the pulmonarymicrocirculation, which results in cycles of alveolarwall injury predisposing and/or aggravating lunginjury (Figure 1B) (2). Invasive and noninvasive mea-surements include analysis of pulmonary edemafluid, exhaled breath condensate (pH, arachidonicacid derivatives), proinflammatory cytokines (inter-leukin [IL]-1b, -2, -6, -8, -12, and -17; interferongamma; and tumor necrosis factor [TNF]-a), anti-inflammatory cytokines (IL-4, -5, -10, and -13 andTGF-b), and chemokines (IL-8, monocyte chemo-attractant protein-1, and macrophage inflammatoryprotein-1b), reactive oxygen and nitrogen species,and exhaled nitric oxide (3,4). The concept of sub-clinical lung injury (e.g., due to previous smoking)takes into account that even asymptomatic eventscan lead to increased future susceptibility to respi-ratory failure events, and new diagnostic techniquesmay provide early detection (5,6).
Circulating factors have been implicated in thepathogenesis of pulmonary inflammation followingrenal and hepatic ischemia/reperfusion injury in an-imal models and humans (7-9). In ischemic AKI,experimental studies demonstrate increased pulmo-nary vascular permeability, cellular apoptosis, alve-olar hemorrhage, and leukocyte trafficking due to theproduction and/or decreased clearance of mediatorsof lung injury (2). Intraluminal neutrophils contributethrough phagocytosis and release of mediators,including reactive oxygen species and proteases, andactivation of dendritic cells, augmenting the immuneresponse. Pro-inflammatory cytokines produced byrenal tubular cells as well as white blood cells includeTNF-a and IL-1b and -6. Conversely, there are coun-terbalancing cell signaling peptides, including theanti-inflammatory IL-10, which has been shown toreduce lung injury in experimental models (2).Delayed recovery of kidney function may impair res-olution of lung inflammation post-AKI (10). Thealtered mechanisms for water transport in pulmonaryedema are described in detail in the “Uremic Lung”section.MECHANICAL VENTILATION AND ARDS. Mechanicalventilation increases intrathoracic pressure and pro-duces adverse hemodynamic effects that are oppo-site to normal spontaneous ventilation. Mechanicalventilation compresses pulmonary vasculature, whichmay result in increased right ventricular afterload anddiminished cardiac output, leading to hypotension

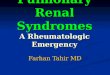
CENTRAL ILLUSTRATION Cardio-Pulmonary-Renal Interactions
Husain-Syed, F. et al. J Am Coll Cardiol. 2015; 65(22):2433–48.
Multiple dependent inflammatory pathways promote injury and elevate the risk for chronic disease of the heart, lung, and kidney, including increased
expression of soluble pro-inflammatory mediators, innate and adaptive immunity, physiological derangements, and cellular apoptosis. The figure illustrates
the cellular and molecular crosstalk and potential biomarkers in acute and chronic cardio-pulmonary-renal interactions. BNP ¼ B-type natriuretic peptide;
ENaC ¼ epithelial sodium channel; FGF ¼ fibroblast growth factor; GST ¼ glutathione S-transferase; hs-cTnT ¼ high-sensitivity cardiac troponin T; ICAM ¼intercellular adhesion molecule; IGFBP ¼ insulin-like growth factor binding protein; IL ¼ interleukin; KIM ¼ kidney injury molecule; L-FABP ¼ L-type fatty
acid binding protein; NAG ¼ N-acetyl-b-D-glucosaminidase; NGAL ¼ neutrophil gelatinase-associated lipocalin; NKCC1 ¼ sodium-potassium chloride
cotransporter 1; TIMP ¼ tissue inhibitor of metalloproteinase; TGF ¼ transforming growth factor; TNF ¼ tumor necrosis factor.
J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5 Husain-Syed et al.J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8 Cardio-Pulmonary-Renal Interactions
2435
and fluid-responsive shock; this scenario is commonlyseen in the initial post-intubated period when venti-lation is initiated. Similarly, decreased venous returnand/or diminished diaphragmatic and abdominal wallcompliance can compromise renal blood flow (11).Importantly, increased intra-abdominal pressure maycontribute to reduced ventilatory volumes, impairedthroughput of blood through the kidneys, and
impaired venous return to the right heart, resultingin CPRI.
The severest form of lung injury is ARDS. Its defi-nition includes the onset of lung failure within 1 weekof the onset of illness, and it is characterized byhypoxemia in the presence of bilateral infiltrates onthe chest x-ray that cannot be explained by HF orfluid overload. Whereas resolution of cardiogenic

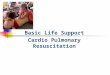
FIGURE 1 The Lung in Cardio-Pulmonary-Renal Interactions
Chronic
Recovery/Non-recovery
Recovery/Non-recoveryChronic HF
CKDESRD
Acute
Chronic Acute
Utilization RFR
Pulmonary embolismPneumonia
ARDSventilation
TraumaToxic agents
Obstructive/Restrictive lung diseaseEmphysemaCystic fibrosisPH
Subclinical AKI
Subclinicalmyocardial injuryAcute HF
Activated neutrophils
Local dentritic cells
Macrophages
Type II cell
klotho (-)
Necrotic or apoptotictype I cell
Inactivatedsurfactant
Hyaline membrane
Edema fluid
Fibrin
Type I cell
Alveolar cells
Surfactant layer
AKIInflammation/ApoptosisEndothelial dysfunction
PEEPBlood gas disturbance
venous congestion
Subclinicalinflammation/ApoptosisEndothelial dysfunctionChronic blood gas disturbanceChronic venous congestion
Acute Chronic
Acute
Glomerular/Interstitialdamage
Sclerosis/Fibrosis
Chronic
Acute Chronic
Ischemic insultArrhythmiaAcute HF
Increased ischemic riskLV hypertrophyRV/LV dyfunction
Pro-fibrotic Anti-fibroticTGF-βIL-1, IL-6, TNF-α
IL-33
Soluble ST2Galectin-3
Anti-inflammatoryCytotoxic
Pro-inflammatoryIL-10
IL-1, IL-6, TNF-α
ROS
acute chronic
Apoptosis, necrosis
Klotho (-)
Alveolar wallthickening
ECM
MyofibroblastFibroblast
Fibrosis
RAAS (-)
B
A
The primary involvement and acuity of organ failure leads to pathophysiological interactions and contributing factors in organ crosstalk. (A) The vicious circle of kidney
and heart injury, reserve capacity and chronic organ failure, and its clinical features. (B) The cellular pattern of lung injury, repair, and fibrosis. Klotho may be an
intermediate mediator that attenuates acute and chronic injury in all 3 organs. AKI ¼ acute kidney injury; ARDS ¼ acute respiratory distress syndrome; CKD ¼ chronic
kidney disease; ECM ¼ extracellular matrix; ESRD ¼ end stage renal disease; HF ¼ heart failure; IL ¼ interleukin; LV ¼ left ventricular; PEEP ¼ positive end-expiratory
pressure; PH ¼ pulmonary hypertension; RAAS ¼ renin-angiotensin-aldosterone system; RFR ¼ renal functional reserve; ROS ¼ reactive oxygen species; RV ¼ right
ventricular; TGF ¼ transforming growth factor; TNF ¼ tumor necrosis factor.
Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2436
pulmonary edema can be rapid, the rate of edemaresolution in most patients with ARDS is markedlyimpaired (1). The role of the alveolar-capillary barrieris very important in ARDS and governs both therapidity of onset and the delayed clearance of alve-olar fluid. ARDS is a major cause of mortality associ-ated with appreciable morbidity, and AKI as anadditional risk factor often develops as a componentof a multiorgan system dysfunction. Even thoughARDS mortality is currently declining (25% to 40%),AKI combined with ARDS increases mortality to 50%to 80% and negatively affects clinical outcomes, ris-ing with AKI severity (12). ARDS is a breakdown ofnormal lung architecture, loss of functioning lung
units, and development of a high-permeability pul-monary edema, all of which result in clinically-stiff,noncompliant, and heterogeneous lungs. Oftenrequiring mechanical ventilation, it can itself in-duce and/or exacerbate lung injury contributing todistant organ effects and deleterious outcomes(2). Mechanistically speaking, pathophysiologicalchanges occur from the direct effect of high pressureon the lung: barotrauma, from the damage caused bylung overdistension; volutrauma, from the shearstress of repetitive opening and closing of alveoli; andatelectotrauma, from the generation of cytokinesand an inflammatory cascade, resulting in bio-trauma. Here, lung-protective ventilation strategies

J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5 Husain-Syed et al.J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8 Cardio-Pulmonary-Renal Interactions
2437
not only improve mortality from ARDS, but alsolead to improved distant organ function, suggestingthe presence of iatrogenic trauma as a result ofhigh volume ventilation that can further triggerhemodynamic, neurohormonal, and cell signalingpathophysiological mechanisms (including right ven-tricular stress with progressive pulmonary hyper-tension [PH]) (10,13). In addition, fluid overload andvenous congestion is an independent predictor ofincreased mortality in AKI that is thought to furthercontribute to respiratory complications (14). Here, thegoal of optimal fluid management for recovery of bothorgans is an area of active study (10). Furthermore,the role of inhaled nitric oxide for alleviation ofARDS and altering renal function has to be defined,including its anti-inflammatory properties (15). Sev-eral favorable effects are known, although trialsand meta-analyses have failed to demonstrate itsbeneficial use in ARDS (16). Inhaled nitric oxide cau-ses selective vasodilation of pulmonary vessels inventilated areas without affecting systemic bloodpressure and cardiac output, improves ventilation-perfusion mismatch, and is a valuable option toreduce PH in susceptible patients (17). In addition,nitric oxide exerts positive effects in acute hyperoxiclung injury models by diminishing inflammation andby protecting both endothelium and alveolar epithe-lium from oxidative injury (18).
Outside of the setting of ARDS, there is convincingevidence that pro-inflammatory effects of mechanicalventilation can be a source of AKI. In lung-injuriousventilator strategies, animal models demonstratethe production of a variety of inflammatory cytokines(e.g., IL-8 and monocyte chemotactic protein-1),expression of nitric oxide synthase (shown to exertcytotoxic effects), induction of renal epithelial cellapoptosis, and dysregulation of renal vascularresponse (19). Injurious mechanical ventilation in-duces myocardial inflammation, including theup-regulation of pro-inflammatory myocardial cy-clooxygenases and expression of IL-8, whereaslung-protective strategies ameliorate myocardialinflammation (20).PULMONARY VASCULAR REMODELING AND FIBROSIS.
Patients with chronic respiratory disease often havemultiple comorbidities such as concomitant cardio-vascular disease, hypertension, and a decline inrenal function (21). The diseases’ natural courseand severity, as well as quality of life, are diverse,depending on pathology in the respiratory systemand on other organ dysfunction. Comorbidities arefrequently the reason for hospitalization and haveled to a common view that chronic respiratory disor-ders contribute to both airway and systemic
inflammation affecting distant organs (22). Poly-pharmacy is frequent in these cohorts, and impairedrenal clearance of drugs could increase the risk ofadverse reactions. Pulmonary congestion in chronicHF can initiate lung structural remodeling by prolif-eration of fibroblasts with fibrosis and extracellularmatrix deposition, resulting in thickening of thealveolar wall (Figure 1B) (23). Similar mechanisms areassumed in CKD, in addition to uremia-relateddysfunction of the pulmonary microcirculation (24).Although the resultant reduction in vascular perme-ability is initially protective against pulmonaryedema and can be seen as a restorative mechanism,the process can cause a restrictive, poorly compliantlung with impaired gas exchange, and reduced exer-cise capacity. The lung diffusion capacity for carbonmonoxide is one of the most clinically-valuable teststo assess the alveolar-capillary membrane. In acutedecompensated HF, it can be normal or elevated dueto an increased alveolar capillary blood volume,whereas the previously-mentioned mechanisms canlead to its impairment in chronic HF (25). In CKD, amarked decrease in diffusion capacity for carbonmonoxide correlates with the severity of renalimpairment after correcting the effects of renal ane-mia (26). The multifunctional protein Klotho regu-lates phosphate/calcium metabolism and is identifiedas an important molecule in the aging processes. Itscytoprotective role is currently investigated in CKDand cardiac remodeling, and Klotho appears as 1 ofseveral unifying mechanisms in the CPRI. Animalstudies emphasize its antioxidative (27) and anti-fibrotic (28) capacity by suppressing vascular endo-thelial growth factor and the pro-fibrotic TGF-b1/Smad 3 expression in pulmonary epithelia.
Chronic hypoxia and vascular remodeling isassumed to be responsible for resultant secondary andin some cases fixed pre-capillary PH, which is an in-dependent predictor of mortality (29). The transitionfrom a primary vasoconstrictive to a vasoproliferativeprocess is the hallmark of fixed PH. This histopatho-logical pattern is defined by “hypertrophy of themedial layer of the vessel wall, hyperplasia of theintimal layer, proliferation of the adventitial layer,and/or plexiform lesions” (29). The natural course ofPH is generally progressive, with osteoblastic trans-formation of vascular smooth muscle cells and depo-sition of hydroxyapatite crystals in the interstitium.As a result, pulmonary vascular stiffness markedlyincreases. In this scenario, a selective pulmonaryvasoactive therapy can potentially worsen a patient’scondition by causing increased venous engorgementand a shift of the interventricular septum, thusinducing left ventricular (LV) failure with pulmonary

Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2438
edema (30). PH has been reported in >60% of patientswith HF with reduced ejection fraction, >80% of pa-tients with HF with preserved ejection fraction, and in78% of patients prior to mitral valve surgery (31).
First established in 1998, the clinical classificationof PH has become more granular over time, and in2013, chronic renal failure was added as a risk factor(29). The prevalence of PH and concomitant CKDincreases with declining renal function, and in currentunderstanding, kidney function may itself have aneffect on pulmonary vascular remodeling in a predis-posed patient, analogous to connective tissue disease,human immunodeficiency virus, or portal hyper-tension (32). Pathophysiological features includeendothelial dysfunction, decreased bioavailability ofnitric oxide, increased levels of endothelin-1, fluidoverload, and shunting via arteriovenous fistulae (32).
BLOOD GAS DISTURBANCES. Maintenance of normalgas exchange is not achieved in patients with chronicunderlying pulmonary disease and in severely ill pa-tients; hypoxemia and/or hypercapnia develops withrelative degrees of renal acid/base compensation.Reflecting alveolar ventilation in most cases, acuteand chronic changes in carbon dioxide tension elicitrenal adaptive buffering mechanisms. In pulmonarydiseases, vasodilator properties of hypercapnia leadto a decrease in systemic vascular resistance andblood pressure with consequent neurohormonalactivation, retention of salt and water, and reductionin renal blood flow and glomerular filtration rate(GFR); cardiac output is not reduced, and renal bloodflow and GFR increase when hypercapnia improves(21,33). Supported by recent findings, the relativecontribution of blood gas disturbances may be crucialin CPRI and its prognosis. The targeted long-term useof noninvasive ventilation (biphasic positive airwaypressure) for reduction of hypercapnia in stablechronic obstructive pulmonary disease patientssignificantly improves survival (34). Likewise, formsof assistance in ventilation for obstructive and centralsleep apnea effect improvements in renal blood flowand glomerular filtration (35). Short-term noninvasiveventilation reduces albuminuria, high-sensitivity C-reactive protein levels, and urinary norepinephrineexcretion in HF patients (36). On the contrary,permissive hypercapnia in acute respiratory disordersmay be beneficial in diminishing lung inflammationand lung/kidney cell apoptosis (37).
HEART IN ORGAN CROSSTALK:
THE CARDIOLOGIST’S VIEW
Cardiovascular diseases remain the major cause forhospitalization, disability, and mortality worldwide.
Among those, HF is a pivotal and progressive condi-tion that leads to a cascade sequence of interorgancrosstalk, including lung and kidney (Figure 2A). HFcomprises different scenarios, depending on acuityand origin (38). Most frequently, acute decom-pensated HF develops in the presence of an under-lying chronic HF, although in 15% to 30% of all causesit may present as new onset HF.
Distant organ damage is often proportional toduration of HF and represents a daily multidisci-plinary challenge. Recently, a TNM–like method wasproposed for HF staging, which includes the charac-terization “H” for heart, “L” for lung, and “M” formalfunction of other organs including the kidney(39). Most distant organ malfunctions (e.g., liver,kidney, or bowel) are the result of right-sided HF andacute on chronic venous congestion (40). Addition-ally, AKI occurs in 25% to 33% of acute decom-pensated HF, which is an independent risk factor forprolonged hospitalization, need for renal replace-ment therapies, readmission, increased stroke risk,and mortality (41). In 60% of cases of acutelydecompensated HF, AKI can be seen as an exacerba-tion of previously-diagnosed CKD, whereas in chronicHF, CKD has been reported as a comorbidity in 26% to63% (42).CARDIAC INJURY, ABNORMAL CELL SIGNALING,
AND OXIDATIVE STRESS. Analogous to the lung,cardiomyocytes show the ability to promote distantorgan damage (e.g., AKI), following ischemic andmechanical injury via innate immune system res-ponse, neurohormonal signaling, and possibly, byrelease of metabolic products (e.g., catalytic iron)(41). IL-1 and TNF-a induce expression of ICAM-1, anintercellular adhesion molecule promoting diape-desis of leukocytes into interstitium, therebydepressing LV function by presumably inducing car-diomyocyte hypoxia and apoptosis (Figure 2B) (43). Inresponse to biomechanical strain, ST2 acts as a decoyfor IL-33 on its receptors in resident satellite cells andcardiomyocytes. Additionally, in response to stimu-lation by aldosterone and other factors, macrophagessecrete galectin-3, which is a powerful stimulus forfibroblasts to proliferate and produce increasedinterstitial collagen. In concomitant AKI, renaltubular cells can further contribute to the circulatinglevels of inflammatory cytokines. The important roleof these cells in the handling of inflammatory medi-ators and resulting efflux into systemic circulation isdiscussed in the section “Acute Kidney Injury,Abnormal Cell Signaling, and Oxidative Stress” (44).Oxidative stress has been implicated as the finalcommon pathway of injury in various pathologicalsystems that are prevalent in cardiac, pulmonary, and

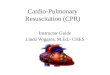
FIGURE 2 The Heart in Cardio-Pulmonary-Renal Interactions
ChronicA
BActivated neutrophils
Local dentritic cells
Macrophages
acute
Apoptosis, necrosis
chronic
Fibrosis
Recovery/Non-recovery
Recovery/Non-recovery
Subclinical lunginjuryLung injuryChronic lung failure
CKDESRD
Acute
Acute
Acute
Impaired gas exchangePulmonary congestionLow compliancePrecapillary PH
Impaired gas exchangeLung edemaPostcapillary PH
Adhesive Pro-fibrotic Anti-fibroticTGF-β
Cytotoxic
Pro-inflammatory
ICAM-1
IL-1, IL-6, IL-8, TNF-α
IL-1, IL-6, TNF-αIL-33
ECM
MyofibroblastFibroblast
Soluble ST2Galectin-3
ROS
Glomerular/Interstitial damage
Sclerosis/Fibrosis
Chronic
Chronic
Acute Chronic
Cardiomyocytes
Acute ChronicUtilization RFRSubclinical AKIAKI
Klotho (-) Klotho (-)FGF23 (+)
RAAS (-)
MyocarditisIschemic heart diseaseHypertensive heartdiseaseCardiomyopathy
Acute myocardialinfarction
ArrhythmiaHypertensive emergency
Cardiac surgeryPericardial tamponade
Toxic agents
Inflammation/ApoptosisEndothelial dysfunctionSympathetic activation
Low cardiac outputVenous congestion
Subclinicalinflammation/ApoptosisEndothelial dysfunctionIncreased RVR/PVRChronic hypoperfusionChronic venous congestion
(A) The vicious circle of heart and lung injury, reserve capacity, and chronic organ failure, and its clinical features. (B) The cellular pattern of renal injury, repair, and
fibrosis. FGF23 may contribute to cardiac remodeling in concert with Klotho deficiency. FGF ¼ fibroblast growth factor; ICAM ¼ intercellular adhesion molecule;
IGFBP ¼ insulin-like growth factor binding protein; PVR ¼ pulmonary vascular resistance; RVR ¼ renal vascular resistance; other abbreviations as in Figure 1.
J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5 Husain-Syed et al.J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8 Cardio-Pulmonary-Renal Interactions
2439
renal disorders (1,44). Accumulation of oxidative-damage products and failure to adapt to reactive ox-ygen species stress may result in an immune systemactivation and a proinflammatory and/or profibroticmilieu to generate functional and structural abnor-malities, and consequently evoke cell death.RIGHT VENTRICULAR STRESS ANDVENOUS CONGESTION.
Pulmonary vascular resistance is in constant inter-play with right ventricular function. In the normalstate, the right ventricle is a thin-walled, compliant,low-pressure chamber that pumps the same strokevolume as the left ventricle, but with z25% of the
stroke work due to the typically low resistance of thepulmonary vasculature (45). In PH, the stressed hearttries to balance pre-load and afterload to accommo-date increased pulmonary vascular resistance.Resultant neurohormonal activation (endothelin,arginine vasopressin) leads to water and salt reten-tion, worsening venous congestion, and furtherreduced cardiac output (46).
In HF, renal failure has traditionally been thoughtto be caused by renal hypoperfusion due to low-output failure. However, most hospitalizations foracute decompensated HF occur because of symptoms

Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2440
of pulmonary and systemic venous congestion ratherthan poor perfusion (47). As 85% of the total bloodvolume is located in the venous side of circulation, anexpansion in total blood volume may occur withoutchanges in the arterial circulation (46). However, adysfunctional left ventricle is prone to afterload var-iations, and therefore, increased systemic bloodpressure can cause pulmonary congestion, irre-spective of the intravascular volume. As reviewedearlier, the pulmonary sequelae extend beyond sim-ply lung edema and congestive pneumonia. Hydro-static effects can induce lung injury and barrierdysfunction, initiating a cascade of local and systemicorgan injury, whereby pulmonary vascular remodel-ing results from chronic affection. Recurrent decom-pensation can account for the vulnerability of HFpatients. Additionally, venous congestion may in-crease gut endotoxin absorption contributing to theharmful environment, although activation of venousendothelium itself is a stimulus for release of in-flammatory mediators (48). As with the heart, thesurrogate central venous pressure is 1 of the mostimportant hemodynamic determinants for worseningrenal function and is independently associated withhigher mortality (47). On the basis of animal models,venous congestion is likely to decrease renal perfu-sion pressure through an increase in back pressureand formation of renal edema, although the renal“intracapsular tamponade” may aggravate backpressure (49). Venous congestion represents a part ofa cascade with stepwise development of fluid over-load, deteriorating LV dysfunction, pulmonarycongestion, secondary fixed pre-capillary PH, rightventricular overload and enlargement with tricuspidincompetence, and interference with LV filling. Theadditional resultant central venous pressure rise istransmitted to the kidney and leads to a positivefeedback loop evolving toward refractory congestiveHF. Those patients are at high risk and have a narrowwindow for fluid management of venous congestion;extremes in either parameter can be associated withworsened renal and right ventricular function.CARDIAC REMODELING AND FIBROSIS. HF repre-sents a heterogeneous group of syndromes leadingto structural (hypertrophy, fibrosis, and/or ventricu-lar dilation) and functional alterations (myocardialstiffness and incomplete relaxation of contractileunits) (50). Here, sequence of abnormal gene ex-pression, cell signaling, and oxidative stress due touncontrolled hypertension, diabetes mellitus, andother factors are a common link that is responsiblefor exuberant repair (fibrosis) pathways (Figure 2B)(41). The transformation predisposes the heart tobecome more vulnerable to re-entrant arrhythmias
and pump failure. Accumulation of cardiac fibrosismay be the mechanism by which age contributes asa determinant of HF in the community (51).
At a cellular level, angiotensin and aldosteroneare major stimuli for galectin-3 secretion with acti-vation of oxidant stress signaling pathways thatdecrease levels of bioavailable nitric oxide, increaseinflammation and TGF-b, and promote fibroblastproliferation, migration, extracellular matrix remod-eling, and deposition of pro-collagen (52,53). Fibrosisin the myocardium, lung, and kidney strongly sug-gests that neurohormonal translation to cell signalsis part of the pathogenesis and progression ofdisease. The mammalian fibroblast growth factor(FGF) family plays a crucial role via distinct actionmechanisms among cardiomyokines and representsa promising novel endeavor. FGF2 and FGF23 pro-mote cardiac hypertrophy and fibrosis by activatingmitogen-activated protein kinases signaling andcirculating (a)-Klotho-independent calcineurin/nu-clear factor of activated T cells signaling, respec-tively. FGF2 significantly induces TGF-b1 that actsdownstream of angiotensin II and promotes cardiacremodeling (54). The bone-derived hormone FGF23regulates phosphate in association with parathyroidhormone and vitamin D in coordination with itscoreceptor Klotho, whereas CKD progression resultsin elevated serum levels of FGF23 (55). In con-trast, FGF16 and FGF21 seem to prevent cardiacremodeling (54). In vitro, Klotho inhibits TGF-b1–,angiotensin II–, or high phosphate-induced fibrosis(56) and confers resistance to oxidative stress andendothelial dysfunction (57). In experimental mo-dels, intravenous delivery of a-Klotho can amelioratecardiac hypertrophy, independent of FGF23 andphosphate levels (55). However, the mechanism ofa-Klotho–independent FGF23 signaling in the heartremains unclear (54). Whether modulation of thiscomplex system would improve cardiac outcomein such a high-risk population awaits furtherinvestigation.
LV remodeling is associated with increased inter-stitial matrix, decreased capillary density, acceleratedapoptosis, chamber dilation, and dyssynchrony,leading to pump failure and sudden death (58).HF with preserved systolic function remains anelusive condition associated with concentric LV hy-pertrophy and impairment of diastolic LV function.It accounts for more than one-half of hospitaliza-tions for HF and has no agreed-upon definitions fordetection or management (59). Activation of the renin-angiotensin-aldosterone system is 1 potential unifyingelement in diastolic HF and CPRI, and the poten-tial efficacy and antifibrotic role of mineralocorticoid

J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5 Husain-Syed et al.J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8 Cardio-Pulmonary-Renal Interactions
2441
receptor antagonists in cardiac, pulmonary, andrenal disease merits further investigation in clinicaltrials (52).
KIDNEY IN ORGAN CROSSTALK:
THE NEPHROLOGIST’S VIEW
The kidney is the window to neurohumoral andimmunological diseases and plays a key role inclearance, fluid, electrolyte, and acid-base homeo-stasis in mammalian physiology. AKI remains 1 of themost complex clinical challenges and is associatedwith excess morbidity and mortality, especially incritically ill patients (44). Regardless of the cause,cardiac and/or pulmonary symptoms are the leadingclinical manifestation (Figure 3A). Current definitionsof AKI are commonly linked to creatinine rise andurinary output, are insensitive to the severity of renalinjury, and can lead to delayed diagnosis and under-estimation of the degree of tubular damage. Theconcept of subclinical AKI emphasizes that even pa-tients who do not fulfill current consensus criteria forAKI are still likely to have acute tubular damage thatmay expose them to an increased susceptibility tofuture injury and elevated risk for subsequent CKDdevelopment (60), providing a significant impulse forthe initiation of organ crosstalk with the heart andlung. The recent KDIGO clinical practice guidelineproposed a new conceptual model, called acute kid-ney disease, to emphasize the need to follow patientswho survived AKI episodes. Here, assessment of renalfunctional reserve seems to be a promising tool topredict kidney recovery versus early function decline(61). Despite medical advances and the widespreadavailability of renal replacement therapy, the mor-tality rate of severe AKI has not declined in recentdecades, reaching 50%, and therapy is limited (62).Early and increased renal replacement therapy doesnot appear to improve outcome. Much of the mor-tality risk is thought to be the consequence of com-plex interactions between the actual insult, activationof inflammation, and distant organ effects. To reducethe systemic inflammatory response, especially incombination with AKI, recent efforts are being madeto use renal replacement therapy as a means toreduce cytokines.
AKI, ABNORMAL CELL SIGNALING, AND OXIDATIVE
STRESS. The renal tubular epithelium is funda-mental in the regulation of inflammatory processesand is immunologically active (44,62). During AKI, itrepresents a major site of cell injury and death,catalyzing circulating mediators in local and sys-temic inflammation/oxidative stress by different
mechanisms including epigenetic processes(Figure 3B). In animal models, the kidney respondswith an expression of IL-1b, vascular cell adhesionmolecule-1, and TGF-b consistent with renal cell in-filtrates and, in advanced stages, perivascular, peri-glomerular, and peritubular fibrosis with increasedmarkers of collagen formation (63). Here, innate andadaptive, cellular, and humoral immune systemscontribute to AKI, which are presumably involved inrepair process as well (62). However, a detailed dis-cussion of immunomodulation is beyond the scopeof this review. Recently, many efforts have beenmade to dissect the mechanisms of ischemic pre-conditioning as a powerful intervention to protectthe heart, lung, and kidney from injury (64,65).Endothelial cells, cardiomyocytes, and vascularsmooth muscle cells have all been shown to altercellular processes as a result of repeated episodes ofnonlethal hypoxia. Thus, these changes may some-day be mimicked by drugs or other interventions toimprove cell survival during ischemic episodes. AKIcan clearly lead to CKD. The incidence of tubu-lointerstitial fibrosis has the best correlation withCKD development (66). Interestingly, Klotho ismainly expressed in renal distal convoluted tubules(56). Thus, renal tubular cells and renal fibroblastsmay be the primary cell types in the progressivedevelopment of CKD contributing to the progressivenature of cardiovascular and pulmonary diseases.
UREMIC LUNG. Chronic uremia affects the lungs andresults in the characteristic central butterfly appear-ance that contrasts with the translucent periphery inanteroposterior x-rays of the lung. In 1951, Bass et al.(67) reported its association with cardiac hypertrophyand LV failure in advanced kidney failure. Uremiaresults in a decrease in diffusion capacity for carbonmonoxide (26), small airway dysfunction (68), andimpaired peak oxygen consumption (69). The uremicmilieu presumably contributes to the development oflung injury and dysfunction, which can be reversedby renal transplantation (9,70). With the introductionof dialysis, the classic presentation of uremic lung inthe absence of volume overload has become lesscommon. Still, its pathophysiologic principles areoperative in CPRI.
At a cellular level, mechanisms for impaired reso-lution of pulmonary edema in acute lung injury (1),in cardiogenic pulmonary edema (71), and in re-sponse to AKI (9) have been identified demonstratingreduced expression of epithelial sodium channel,sodium-potassium ATPase, and aquaporin 5. Epithe-lial sodium channel-inhibition (e.g., with amiloride)can alter alveolar fluid clearance, promoting reversed

FIGURE 3 The Kidney in Cardio-Pulmonary-Renal Interactions
Chronic
Recovery/Non-recovery
Recovery/Non-recovery
Chronic HF
Chronic lung failure
Acute
Chronic Acute ChronicAcute
ChronicAcute
Acute HF
Lung injury
Glomerular/Interstitialdisease
Acute tubular necrosisAcute pyelonephritis
Acute urinary obstructionHypovolemia
Hypertensive nephropathyIschemic nephropathyChronic
Chronic obstructivenephropathy
glomerular/Interstitialdisease
Activated neutrophils AdhesiveVCAM-1
ROSCytotoxic
Pro-inflammatory
Local dentritic cells
Macrophages
Renal tubular cells
Subclinicalmyocardial injury
Subclinical lunginjury
IL-1, IL-6, TNF-α
Inflammation/ApoptosisEndothelial dysfunction
Electrolyte/Acid base disorderUremic solute retention
Sympathetic/RAAS activation
Subclinicalinflammation/ApoptosisEndothelial dysfunctionAnemiaBone mineral disorderElectrolyte/Acid base disorderUremic solute retentionSympathetic/RAAS activation
Acute
A
B
Chronic
Impaired gas exchange
PH
Ischemic insultArrhythmiaAcute HF
Increased ischemic riskLV hypertrophyRV/LV dysfunctionUremic cardiomyopathy
PHUremic lung
Impaired gas exchangeLung edema Pulmonary congestion
Pro-fibroticTGF-βIL-1, IL-6, TNF-αSoluble ST2Galectin-3
Anti-fibroticIL-33
acute
Apoptosis, necrosis Fibrosis
chronic
ECM
MyofibroblastFibroblast
Klotho (-) Klotho (-)RAAS (-)
(A) The vicious circle of heart and lung injury, reserve capacity, and chronic organ failure, and its clinical features. (B) The cellular pattern of renal injury, repair, and
fibrosis. Activation of RAAS may contribute to renal fibrosis by diminishing the cytoprotective effects of Klotho. HF ¼ heart failure; LV ¼ left ventricular; RV ¼ right
ventricular; VCAM ¼ vascular cell adhesion molecule; other abbreviations as in Figure 1.
Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2442
transepithelial ion transport with active augmenta-tion of pulmonary edema. In animal model, inhibitionof either the apical cystic fibrosis transmembraneconductance regulator or sodium-potassium-chloridecotransporter 1 (e.g., with furosemide) can preventactive alveolar fluid secretion (71).UREMIC CARDIOMYOPATHY. CKD accelerates coro-nary artery atherosclerosis by several mechanisms,notably hypertension, dyslipidemia, and abnormalcalcium/phosphorus metabolism, associated with vas-cular remodeling and development of noncompliant
vessels. Still, these mechanisms cannot accountfor cardiovascular risk, as reflected in high rates ofsudden cardiac death, HF, sustained arrhythmias, andmyocardial infarction (72). Uremic cardiomyopathydefines the structural and electrophysiological remod-eling of the heart, characterized by biventricularhypertrophy, systolic and diastolic dysfunction, capil-lary rarefication, cardiac fibrosis, and an enhancedsusceptibility to further injury (73). Involvement ofthe fibrotic pericardium is classically manifestedas acute on chronic uremic pericarditis with sterile

J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5 Husain-Syed et al.J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8 Cardio-Pulmonary-Renal Interactions
2443
effusion, and is a less common complication since theintroduction of dialysis. Contrarily, reversal of renaldysfunction (e.g., after renal transplantation) canimprove cardiac function (74). Uremic cardiomyopathymay represent the advanced alteration of cardiacremodeling described earlier and FGF23 excess/Klothodeficiency might make a considerable contribution inCKD patients (56).
In type 3 cardiorenal syndrome, AKI can lead tocardiac dysfunction by fluid overload, electrolyte andacid-base shift, and renin-angiotensin-aldosteronesystem or central nervous system activation. Analo-gous to the lung, AKI induces endothelial cellactivation, leukocyte trafficking, and myocardial in-filtration (the role of ICAM-1 was reviewed earlier),and pro-apoptotic cascades, resulting in myocardialdamage and long-term dysfunction (44). Followingcardiac ischemia, ventricular fibrillation appearsmuch more frequent in the setting of AKI (75).Impaired cardiac function alters the interdependencyof the cardiopulmonary circuit. Pulmonary conges-tion, in combination with AKI-induced compromiseof tubular epithelial ion pumps, may act syner-gistically to further compromise cardiopulmonaryfunction.
CKD AND FIBROSIS. The high prevalence and burdenof CKD is well established and can represent theorigin and/or continuum of chronic cardiopulmo-nary disorders. The concept of subclinical AKI wasdiscussed, and early pathological changes can occurwithout apparent clinical presentation due to thehigh renal adaptability, but they still depict a slowlyprogressing degenerative process that is both localand systemic. Once the adaptive threshold is reached,the progression to CKD is fast. It is generally acceptedthat all primary causes of CKD share a commonpathogenic pathway of progressive renal injury dueto the destructive consequences of fibrosis. As fi-brosis increases, the nephron that normally has apotent regenerative capacity loses this ability, leadingto apoptosis. Proteinuria is a surrogate marker ofCKD progression and reflects endothelial dysfunc-tion. Even a modest increase in albuminuria is asso-ciated with chronic pulmonary disorders (76), rightventricular/LV remodeling, and adverse cardiovas-cular outcomes (77), although by the time proteinuriamanifests, renal structural damage has alreadyoccurred. Here, clinical and emerging biomarkers(e.g., galectin-3) have been identified (78). Still, it isimportant to underscore that most CKD patients willnever reach the point of needing renal replacementtherapy. They are more likely to die prematurely dueto accelerated cardiovascular diseases.
ORGAN FUNCTIONAL RESERVE
Given the multitude of contributing factors andthe time sequence of events in CPRI, it is chal-lenging to predict early functional and/or structuralchanges. The normal heart, lung, and kidney permita degree of physiological reserve that can maintainnormal organ function for any given insult. Thefunctional reserve of an organ can be defined as thedifference between the minimum baseline functionand the maximum attainable function in responseto a physiological or pathological stimulus. Yet, themutual dependence of the organs is not defined.In daily routine, assessment of cardiac and pulmo-nary functional reserve is a valuable parameter todefine status, recovery, and prognosis toward theorgan’s response to an acute event or chronicdisease. Care and attention is needed in chronicdisorders, because these patients are more proneto develop injury, decreasing the remaining func-tional mass. Thus, patients with “acute on chronic”organ injury are at the highest risk. Genetic dispo-sition and environment influence the individualcourse, while the organ functional reserve declineswith age as a consequence of physiological aging.Frequent physical activity can develop and maintaincardiopulmonary reserve best reflected by peak ox-ygen consumption, but no factors have been iden-tified that can lead to increased renal functionalreserve.
CARDIAC FUNCTIONAL RESERVE. Cardiac func-tional reserve is the ability of the myocardium toaugment its cardiac output and tissue delivery ofoxygen during stress. The spectrum of myocardialdysfunction may range from diastolic dysfunction inthe early stage to overt systolic dysfunction. Bothlimit exercise tolerance before resulting in symptomsat rest, normally manifested by exertional dyspneaand impaired oxygen kinetic during exercise. LVdiastolic reserve is the ability of the LV filling pres-sures to remain normal during stress, whereas insystolic dysfunction, stress can reveal both LV andright ventricular impaired contractile reserve (e.g., tounmask subclinical ischemia or PH) (79,80). However,the presence and extent of coronary artery disease,ischemic burden, old myocardial infarction, andmedication (e.g., diminished chronotropic reservewith beta-blockers) are all factors determiningassessment (79). Probably the best measure of cardiacfunctional reserve is the peak oxygen consumptionmeasured during maximal exercise and expressed asml/kg/min. This variable has been shown to be pre-dictive of survival in the general population and in

Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2444
those with myocardial infarction, HF, and virtually allother chronic conditions.
PULMONARY FUNCTIONAL RESERVE. Pulmonaryfunctional reserve is the ability of the lung toaugment its respiratory minute volume during stress.Its measurement is complex and includes severalvariables for determination whether exercise capacityis reduced (mostly the case) or a reduced ventilatorycapacity limits exercise. The breathing reserve,expressed as the difference between the maximalvoluntary ventilation and the maximum exerciseventilation, and respiratory frequency representvaluable criteria for maximal pulmonary exertion(81). As with cardiac functional reserve, the peak ox-ygen consumption can be thought of as an objectivesurrogate of cardiorespiratory endurance and aerobicfitness, because it reflects both pulmonary capabil-ities for ventilation and gas exchange as well as car-diac output and tissue perfusion (82).
RENAL FUNCTIONAL RESERVE. The concept of renalfunctional reserve represents the capacity of intactnephron mass to increase GFR in response to stressand stands for the difference between peak “stress”GFR induced by protein load (oral or intravenous)and the baseline GFR (61). In physiological (e.g.,pregnancy or solitary kidney) or pathological hy-perfiltration (e.g., diabetes mellitus or nephroticsyndrome), renal functional reserve allows for an in-crease in GFR by recruitment of dormant nephrons,replacing the lost function and maintaining the wholeorgan GFR. Renal functional reserve may represent afuture tool to exploit renal filtration capacity, evenwhen subclinical damage is present and creatinine isstill normal, whereas a reduction of renal functionalreserve may represent the equivalent of renal frailtyor susceptibility to insults.
BIOMARKERS
Inflammation is classically defined by 4 elements:immune cells (typically granulocytes), antibodies,cell signals (cytokines, interleukins, and so on), andcomplement. In the absence of infection, acute organinjury in the lungs, heart, and kidneys has very littleinvolvement by granulocytes, antibodies, or comple-ment. Thus, inflammation, despite its popularity as aterm, may not be optimal to describe the primary roleof abnormal cell signaling in the pathogenesis ofCPRI. Novel biomarkers extend the spectrum to pre-vention, early diagnostic evaluation, treatment, andcourse of the disorder (Central Illustration). However,the relative paucity of biomarkers that link a cardio-pulmonary-renal interaction should be emphasizedas an area that needs further study. In the following
text, we review a select group of currently-established and promising future biomarkers in CPRI.
HIGH-SENSITIVITY CARDIAC TROPONIN. High-sensitivitytroponin I and T have been introduced as biomarkersof myocardial injury detectable at a much earlierstage compared with prior troponin assays. In stablePH, chronic obstructive pulmonary disease, and CKD,elevated levels may indicate subclinical myocardialinjury that subsequently contributes to HF (83,84).Knowledge of its determinants in CPRI may guidefurther research and help to stratify patients at earlycardiovascular risk.
B-TYPE NATRIURETIC PEPTIDE AND N-TERMINAL
PRO–B-TYPE NATRIURETIC PEPTIDE. B-type natri-uretic peptide (BNP) and its inactive cleavage proteinN-terminal pro–B-type natriuretic peptide (NT-proBNP) are markers of cardiac stretch from increasedwall tension, and are established diagnostic, prog-nostic, and management tools for acutely decom-pensated HF, chronic HF, and acute coronarysyndromes (85). BNP is also prognostic for PH, prob-ably due to increased right ventricular wall tensionand up-regulation of the pre-proBNP gene (86). Ele-vations in BNP in the setting of acutely decom-pensated HF and acute coronary syndromes isassociated with an increased risk of AKI (38,85).Patients with CKD have higher levels of BNP than age-and sex-matched patients with normal renal func-tion, and this probably represents both increasedcardiac production of BNP due to subclinical pressureoverload, volume overload, and cardiomyopathy aswell as decreased renal clearance, more notably withNT-proBNP than BNP (38).
SOLUBLE SUPPRESSOR OF TUMORIGENICITY 2. Sol-uble suppressor of tumorigenicity 2 (ST2) is a circu-lating inhibitor of the IL-33 receptor and counteractsthe antifibrotic effects of IL-33 (87). Soluble ST2 hasreceived major attention as it may have an importantrole in the development of fibrosis and/or as abiomarker of disease severity, although it lacks organspecificity. Higher concentrations are associated withworse outcome in ARDS and PH (88,89). Soluble ST2has prognostic value in risk stratification for HF, andpresumably CKD, and is not adversely influenced byage and impaired renal function (90).
GALECTIN-3. Galectin-3 is a b-galactoside–bindinglectin with putative roles in immunomodulation,transformation, and aldosterone-induced fibro-genesis. In the heart, galectin-3 is implicated in thepathogenesis of fibrosis but is also increased withnormal aging and renal impairment (53). Galectin-3levels have prognostic value in patients with HF, in-dependent of etiology and HF typology, and provide

J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5 Husain-Syed et al.J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8 Cardio-Pulmonary-Renal Interactions
2445
an additive value to natriuretic peptide measure-ments. Galectin-3 has been shown to promote TGF-b–mediated activation of fibroblasts in the lung (91) andkidney (78). Complementary prospective studies areneeded to assess whether galectin-3 may be used topredict which patient with cardiac, pulmonary, andrenal involvement may benefit from antifibroticagents.
RENAL CELL CYCLE ARREST MARKERS. In thesetting of cellular injury, 1 of the earliest processes tobe affected is the cell cycle, which is down-regulatedto preserve cellular energetics and metabolic func-tions in the setting of hypoxia or other insults. Boththe proximal and distal renal tubular cells releasetissue inhibitor of metalloproteinase (TIMP)-2 andinsulin-like growth factor binding protein (IGFBP)-7,which are measured in the urine and appear topredict a reduction in renal filtration function at $12h after serious illness (92). The multiplication of the2 concentrations yields a renal risk score, with ascore >0.3 U having a high negative predictive valueand a score >1.2 a strong positive predictive value inAKI. The relationship of these cell-cycle arrestmakers in the urine, which have been recentlybecome available as a commercialized, in-vitrodiagnostic test, and other manifestations of CPRIhave not been explored.
NEUTROPHIL GELATINASE-ASSOCIATED LIPOCALIN. Neu-trophil gelatinase associated lipocalin (NGAL) isexpressed in the distal tubules and collecting duct,seems to be 1 of the earliest renal markers of ischemicor nephrotoxic injury, and is detected in blood andurine soon after AKI (93). Moreover, NGAL has beenimplicated in the induction of cardiomyocytesapoptosis and is highly expressed in failing myocar-dium (65). Plasma NGAL has been associated withadverse cardiovascular outcomes or death and is astrong predictor of all-cause mortality in acutedecompensated HF, suggesting that renal damage hasa role in determining the prognosis of HF patients.However, peak 24-h urinary NGAL seems to predictbest the 30-day mortality and dialysis in intensivecare patients, compared with plasma NGAL and cys-tatin C (93). In small studies, plasma and urinarylevels of NGAL do not correlate with PH (94). Yet, itsrole in acute decompensated right ventricular failureis not defined. Plasma, but not urinary NGAL, in-creases markedly with GFR reduction and can possiblygenerate a high number of false positive diagnosesof AKI in stable CKD patients. Both plasma andurine NGAL are commercially available assays for AKI.
L-TYPE FATTY ACID BINDING PROTEIN. In thesetting of AKI, renal tubular cells release L-type fatty
acid binding protein (L-FABP) into the urine. L-FABPis a housekeeping protein that moves rapidly out ofthe cytosol through the apical membrane of tubularepithelial cells and has been shown to be an earlymarker of AKI (95). It can be readily measured and isa commercialized urine test for AKI. Its relation-ships to other manifestations of CPRI have not beendetermined.
KIDNEY INJURY MOLECULE-1. Kidney injury molecule(KIM)-1 is a transmembrane tubular protein solelyexpressed in response to ischemic or nephrotoxicinsults to proximal renal tubular cells, and has beenproposed as an early marker of AKI as well asimportant in the transition from AKI to CKD (96).KIM-1 is measurable in blood and urine and ispredictive of AKI in patients undergoing coronaryangiography and in HF (95). Conversely, higherlevels are associated with incident HF risk (97).There are no data describing the use of KIM-1 inpulmonary disorders.
USE OF BIOMARKERS IN COMBINATION. The AcuteDialysis Quality Initiative panel has recommendedthe use of both functional (creatinine, cystatin C)filtration markers as well as renal tubular injurymarkers (TIMP-2, IGFBP-7, NGAL, L-FABP, KIM-1,IL-18, and so on) to both screen and detect AKI aswell as to aid in the prognosis for important out-comes, including the need for dialysis and mortality(98). This has been well supported by recent pub-lished data in several settings including patients un-dergoing cardiac surgery (99).
CONCLUSIONS
We have summarized current concepts in the patho-genesis of CPRI including abnormalities, cardiopul-monary and systemic hemodynamics, neurohormonalactivation, abnormal cell signaling, and tissue fi-brosis. A sustained injury to the alveolar-capillarybarrier can initiate lung structural and vascularremodeling, leading to chronic lung disease and pul-monary hypertension. Cardiac injury represents theorigin of cascading deleterious events that may leadto myocardial remodeling with fibrosis and heartfailure. Acute kidney injury might occur as a resultof abnormal immune cell signaling of the injuredtubular epithelial cells, whereas recurrent AKI leadsto an elevated risk for subsequent CKD development.Much is yet to be learned about the time sequence oforgan injury and damage and what, if any, are the keymodifiable mediators in the propagation of organdysfunction. Multiple disciplines working togetherhold the hope of future interventions that can lead to

Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2446
improved survival in the critically ill patient withevidence of cardiac, pulmonary, and renal failure.
ACKNOWLEDGMENTS The authors thankDrs. FernandoE. Núñez Gomez, Daniel Murillo Brambila, AashishSharma, Renhua Lu, and Carla Estremadoyro for theirdevoted help in the development of the manuscript.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Faeq Husain-Syed, Department of Nephrology, Dial-ysis and Renal Transplantation, International RenalResearch Institute of Vicenza, San Bortolo Hospital,Via Rodolfi, 37, Vicenza 36100, Veneto, Italy. E-mail:[email protected].
RE F E RENCE S
1. Matthay MA. Resolution of pulmonary edema.Thirty years of progress. Am J Respir Crit Care Med2014;189:1301–8.
2. Grams ME, Rabb H. The distant organ effects ofacute kidney injury. Kidney Int 2012;81:942–8.
3. De Pasquale CG, Arnolda LF, Doyle IR, Grant RL,Aylward PE, Bersten AD. Prolonged alveolocapil-lary barrier damage after acute cardiogenic pul-monary edema. Crit Care Med 2003;31:1060–7.
4. Pappas LK, Giannopoulos G, Loukides S, et al.Exhaled breath condensate in acute and chronicheart failure: new insights into the role of lunginjury and barrier dysfunction. Am J Respir CritCare Med 2014;190:342–5.
5. Johansson SL, Tan Q, Holst R, et al. Surfactantprotein D is a candidate biomarker for subclinicaltobacco smoke-induced lung damage. Am JPhysiol Lung Cell Mol Physiol 2014;306:L887–95.
6. Kuo SJ, Yang KT, Chen DR. Objective andnoninvasive detection of sub-clinical lung injury inbreast cancer patients after radiotherapy. Eur JSurg Oncol 2005;31:954–7.
7. Weber GF, Swirski FK. Immunopathogenesis ofabdominal sepsis. Langenbecks Arch Surg 2014;399:1–9.
8. Nastos C, Kalimeris K, Papoutsidakis N, et al.Global consequences of liver ischemia/reperfusioninjury. Oxid Med Cell Longev 2014;2014:906965.
9. Li X, Hassoun HT, Santora R, Rabb H. Organcrosstalk: the role of the kidney. Curr Opin CritCare 2009;15:481–7.
10. Andres-Hernando A, Altmann C, Bhargava R,et al. Prolonged acute kidney injury exacerbateslung inflammation at 7 days post-acute kidneyinjury. Physiol Rep 2014;2:e12084.
11. Mohmand H, Goldfarb S. Renal dysfunctionassociated with intra-abdominal hypertension andthe abdominal compartment syndrome. J Am SocNephrol 2011;22:615–21.
12. Soto GJ, Frank AJ, Christiani DC, Gong MN.Body mass index and acute kidney injury in theacute respiratory distress syndrome. Crit Care Med2012;40:2601–8.
13. Ranieri VM, Giunta F, Suter PM, Slutsky AS.Mechanical ventilation as a mediator of multi-system organ failure in acute respiratory distresssyndrome. JAMA 2000;284:43–4.
14. Payen D, de Pont AC, Sakr Y, Spies C,Reinhart K, Vincent JL, for the Sepsis Occurrencein Acutely Ill Patients (SOAP) Investigators.A positive fluid balance is associated with a worseoutcome in patients with acute renal failure. CritCare 2008;12:R74.
15. Wraight WM, Young JD. Renal effects ofinhaled nitric oxide in humans. Br J Anaesth 2001;86:267–9.
16. Dzierba AL, Abel EE, Buckley MS, Lat I.A review of inhaled nitric oxide and aerosolizedepoprostenol in acute lung injury or acute respi-ratory distress syndrome. Pharmacotherapy 2014;34:279–90.
17. Rossaint R, Lewandowski K, Zapol WM. Ourpaper 20 years later: inhaled nitric oxide for theacute respiratory distress syndrome—discovery,current understanding, and focused targets offuture applications. Int Care Med 2014;40:1649–58.
18. ter Horst SA, Walther FJ, Poorthuis BJ,Hiemstra PS, Wagenaar GT. Inhaled nitric oxideattenuates pulmonary inflammation and fibrindeposition and prolongs survival in neonatalhyperoxic lung injury. Am J Physiol Lung Cell MolPhysiol 2007;293:L35–44.
19. Koyner JL, Murray PT. Mechanical ventilationand the kidney. Blood Purif 2010;29:52–68.
20. Smeding L, Kuiper JW, Plotz FB, Kneyber MC,Groeneveld AJ. Aggravation of myocardialdysfunction by injurious mechanical ventilation inLPS-induced pneumonia in rats. Respir Res 2013;14:92.
21. Hemlin M, Ljungman S, Carlson J, et al. Theeffects of hypoxia and hypercapnia on renal andheart function, haemodynamics and plasma hor-mone levels in stable COPD patients. Clin Respir J2007;1:80–90.
22. Kaysoydu E, Arslan S, Yildiz G, Candan F.Factors related to microalbuminuria in patientswith chronic obstructive pulmonary disease. AdvClin Exp Med 2014;23:749–55.
23. Azarbar S, Dupuis J. Lung capillary injury andrepair in left heart disease: a new target fortherapy? Clinical Sci (Lond) 2014;127:65–76.
24. Ewert R, Opitz C, Wensel R, Dandel M,Mutze S, Reinke P. Abnormalities of pulmonarydiffusion capacity in long-term survivors afterkidney transplantation. Chest 2002;122:639–44.
25. Schaufelberger M. Pulmonary diffusion ca-pacity as prognostic marker in chronic heart fail-ure. Eur Heart J 2002;23:429–31.
26. Moinard J, Guenard H. Membrane diffusion ofthe lungs in patients with chronic renal failure. EurRespir J 1993;6:225–30.
27. Ravikumar P, Ye J, Zhang J, et al. Alpha-Klothoprotects against oxidative damage in pulmonaryepithelia. Am J Physiol Lung Cell Mol Physiol2014;307:L566–75.
28. Shin IS, Shin HK, Kim JC, Lee MY. Role ofKlotho, an antiaging protein, in pulmonary fibrosis.Arch Toxicol 2015;89:785–95.
29. Simonneau G, Gatzoulis MA, Adatia I, et al.Updated clinical classification of pulmonary hy-pertension. J Am Coll Cardiol 2013;62:D34–41.
30. Guazzi M, Borlaug BA. Pulmonary hyperten-sion due to left heart disease. Circulation 2012;126:975–90.
31. Walls MC, Cimino N, Bolling SF, Bach DS.Persistent pulmonary hypertension after mitralvalve surgery: does surgical procedure affectoutcome? J Heart Valve Dis 2008;17:1–9,discussion 9.
32. Pabst S, Hammerstingl C, Hundt F, et al. Pul-monary hypertension in patients with chronickidney disease on dialysis and without dialysis:results of the PEPPER-study. PloS one 2012;7:e35310.
33. Anand IS, Chandrashekhar Y, Ferrari R, et al.Pathogenesis of congestive state in chronicobstructive pulmonary disease. Studies of bodywater and sodium, renal function, hemodynamics,and plasma hormones during edema and afterrecovery. Circulation 1992;86:12–21.
34. Kohnlein T, Windisch W, Kohler D, et al. Non-invasive positive pressure ventilation for thetreatment of severe stable chronic obstructivepulmonary disease: a prospective, multicentre,randomised, controlled clinical trial. Lancet RespirMed 2014;2:698–705.
35. Nicholl DD, Hanly PJ, Poulin MJ, et al. Evalu-ation of continuous positive airway pressuretherapy on renin-angiotensin system activity inobstructive sleep apnea. Am J Respir Crit Care Med2014;190:572–80.
36. Tamura Y, Koyama T, Watanabe H, Hosoya T,Ito H. Beneficial effects of adaptive servo-ventilation therapy on albuminuria in patientswith heart failure. J Cardiol 2015;65:412–7.
37. Nardelli LM, Rzezinski A, Silva JD, et al. Effectsof acute hypercapnia with and without acidosis onlung inflammation and apoptosis in experimentalacute lung injury. Respir Physiol Neurobiol 2014;205C:1–6.
38. Ronco C, McCullough P, Anker SD, et al.Cardio-renal syndromes: report from the con-sensus conference of the acute dialysis qualityinitiative. Eur Heart J 2010;31:703–11.
39. Fedele F, Gatto MC, D’Ambrosi A, Mancone M.TNM-like classification: a new proposed methodfor heart failure staging. Scientific World Journal2013:175925.

J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5 Husain-Syed et al.J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8 Cardio-Pulmonary-Renal Interactions
2447
40. Salamon JN, Kelesidis I, Msaouel P, et al.Outcomes in World Health Organization Group IIpulmonary hypertension: mortality and read-mission trends with systolic and preserved ejectionfraction-induced pulmonary hypertension. J CardFail 2014;20:467–75.
41. Ronco C, Cicoira M, McCullough PA. Car-diorenal syndrome type 1: pathophysiologicalcrosstalk leading to combined heart and kidneydysfunction in the setting of acutely decom-pensated heart failure. J Am Coll Cardiol 2012;60:1031–42.
42. Cruz DN, Bagshaw SM. Heart-kidney interac-tion: epidemiology of cardiorenal syndromes. Int JNephrol 2010;2011:351291.
43. Wrigley BJ, Shantsila E, Tapp LD, Lip GY.Increased expression of cell adhesion moleculereceptors on monocyte subsets in ischaemic heartfailure. Thromb Haemost 2013;110:92–100.
44. Virzi G, Day S, de Cal M, Vescovo G, Ronco C.Heart-kidney crosstalk and role of humoralsignaling in critical illness. Crit Care 2014;18:201.
45. Voelkel NF, Quaife RA, Leinwand LA, et al.Right ventricular function and failure: report of aNational Heart, Lung, and Blood Institute WorkingGroup on Cellular and Molecular Mechanisms ofRight Heart Failure. Circulation 2006;114:1883–91.
46. Chaney E, Shaw A. Pathophysiology of fluidretention in heart failure. Contrib Nephrol 2010;164:46–53.
47. Dupont M, Mullens W, Tang WH. Impact ofsystemic venous congestion in heart failure. CurrHeart Fail Rep 2011;8:233–41.
48. Colombo PC, Onat D, Sabbah HN. Acute heartfailure as “acute endothelitis”—interaction of fluidoverload and endothelial dysfunction. Eur J HeartFail 2008;10:170–5.
49. Bellomo R, Prowle JR, Echeverri JE. Diuretictherapy in fluid-overloaded and heart failure pa-tients. Contrib Nephrol 2010;164:153–63.
50. Paulus WJ, Tschöpe C. A novel paradigm forheart failure with preserved ejection fraction:comorbidities drive myocardial dysfunction andremodeling through coronary microvascularendothelial inflammation. J Am Coll Cardiol 2013;62:263–71.
51. Dutta D, Calvani R, Bernabei R,Leeuwenburgh C, Marzetti E. Contribution ofimpaired mitochondrial autophagy to cardiacaging: mechanisms and therapeutic opportunities.Circ Res 2012;110:1125–38.
52. Maron BA, Leopold JA. The role of the renin-angiotensin-aldosterone system in the pathobi-ology of pulmonary arterial hypertension (2013Grover Conference series). Pulm Circ 2014;4:200–10.
53. Calvier L, Martinez-Martinez E, Miana M, et al.The impact of galectin-3 inhibition onaldosterone-induced cardiac and renal injuries.J Am Coll Cardiol HF 2015;3:59–67.
54. Itoh N, Ohta H. Pathophysiological roles ofFGF signaling in the heart. Front Physiol 2013;4:247.
55. Xie J, Yoon J, An SW, Kuro-O M, Huang CL.Soluble Klotho protects against uremic cardiomy-opathy independently of fibroblast growth factor
23 and phosphate. J Am Soc Nephrol 2015;26:1150–60.
56. Hu MC, Shi M, Cho HJ, et al. Klotho andphosphate are modulators of pathologic uremiccardiac remodeling. J Am Soc Nephrol 2014 Oct 17[E-pub ahead of print].
57. Oh HJ, Nam BY, Lee MJ, et al. Decreasedcirculating Klotho levels in patients undergoingdialysis and relationship to oxidative stress andinflammation. Perit Dial Int 2015;35:43–51.
58. Sobanski P, Jaarsma T, Krajnik M. End-of-lifematters in chronic heart failure patients. Curr OpinSupport Palliat Care 2014;8:364–70.
59. Vasan RS, Larson MG, Benjamin EJ, Evans JC,Reiss CK, Levy D. Congestive heart failure in sub-jects with normal versus reduced left ventricularejection fraction: prevalence and mortality in apopulation-based cohort. J Am Coll Cardiol 1999;33:1948–55.
60. Haase M, Kellum JA, Ronco C. SubclinicalAKI—an emerging syndrome with important con-sequences. Nat Rev Nephrol 2012;8:735–9.
61. Sharma A, Mucino MJ, Ronco C. Renal func-tional reserve and renal recovery after acute kid-ney injury. Nephron Clin Pract 2014;127:94–100.
62. Rabb H. The promise of immune cell therapyfor acute kidney injury. J Clin Invest 2012;122:3852–4.
63. Cruz DN, Schmidt-Ott KM, Vescovo G, et al.Pathophysiology of cardiorenal syndrome type2 in stable chronic heart failure: workgroupstatements from the eleventh consensus confer-ence of the Acute Dialysis Quality Initiative (ADQI).Contrib Nephrol 2013;182:117–36.
64. Alreja G, Bugano D, Lotfi A. Effect of remoteischemic preconditioning on myocardial and renalinjury: meta-analysis of randomized controlledtrials. J Invasive Cardiol 2012;24:42–8.
65. Wang Z, Ji Y, Wang S, Wang R, et al. Protectiveeffect of intestinal ischemic preconditioning onischemia reperfusion-caused lung injury in rats.Inflammation 2015;38:424–32.
66. Rodriguez-Iturbe B, Johnson RJ, Herrera-Acosta J. Tubulointerstitial damage and progres-sion of renal failure. Kidney Int Suppl 2005:S82–6.
67. Bass HE, Greenberg D, Singer E, Miller MA.Pulmonary changes in uremia. Bull N Y Acad Med1951;27:397.
68. Tkácová R, Tkác I, Podracký J, Moscovic P,Roland R, Hildebrand T. Spirometric alterations inpatients with reduced renal function. Wien KlinWochenschr 1993;105:21–4.
69. Bonzel KE, Wildi B, Weiss M, Schärer K. Spi-roergometric performance of children and ado-lescents with chronic renal failure. Pediatr Nephrol1991;5:22–8.
70. Guleria S, Agarwal RK, Guleria R, Bhowmik D,Agarwal SK, Tiwari SC. The effect of renal trans-plantation on pulmonary function and respiratorymuscle strength in patients with end-stage renaldisease. Transplant Proc 2005;37:664–5.
71. Solymosi EA, Kaestle-Gembardt SM, Vadasz I,et al. Chloride transport-driven alveolar fluidsecretion is a major contributor to cardiogenic
lung edema. Proc Natl Acad Sci U S A 2013;110:E2308–16.
72. Whitman IR, Feldman HI, Deo R. CKD andsudden cardiac death: epidemiology, mechanisms,and therapeutic approaches. J Am Soc Nephrol2012;23:1929–39.
73. Gross ML, Ritz E. Hypertrophy and fibrosis inthe cardiomyopathy of uremia–beyond coronaryheart disease. Semin Dial 2008;21:308–18.
74. Wali RK, Wang GS, Gottlieb SS, et al. Effect ofkidney transplantation on left ventricular systolicdysfunction and congestive heart failure in pa-tients with end-stage renal disease. J Am CollCardiol 2005;45:1051–60.
75. Grasic Kuhar C, Budihna MV, Pleskovic RZ.Mibefradil is more effective than verapamil forrestoring post-ischemic function of isolated heartsof guinea pigs with acute renal failure. Eur JPharmacol 2004;488:137–46.
76. Romundstad S, Naustdal T, Romundstad PR,Sorger H, Langhammer A. COPD and micro-albuminuria: a 12-year follow-up study. Eur RespirJ 2014;43:1042–50.
77. Katz DH, Burns JA, Aguilar FG, Beussink L,Shah SJ. Albuminuria is independently associatedwith cardiac remodeling, abnormal right and leftventricular function, and worse outcomes in heartfailure with preserved ejection fraction. J Am CollCardiol HF 2014;2:586–96.
78. Drechsler C, Delgado G, Wanner C, et al.Galectin-3, renal function, and clinical outcomes:results from the LURIC and 4D studies. J Am SocNephrol 2015 Jan 7 [E-pub ahead of print].
79. Ramahi TM, Longo MD, Cadariu AR, et al. Leftventricular inotropic reserve and right ventricularfunction predict increase of left ventricular ejec-tion fraction after beta-blocker therapy in non-ischemic cardiomyopathy. J Am Coll Cardiol 2001;37:818–24.
80. Sharma T, Lau EM, Choudhary P, et al.Dobutamine stress for evaluation of right ven-tricular reserve in pulmonary arterial hyperten-sion. Eur Respir J 2015;45:700–8.
81. Vainshelboim B, Fox BD, Saute M, et al. Limi-tations in exercise and functional capacity in long-term postpneumonectomy patients. J CardiopulmRehabil Prev 2015;35:56–64.
82. Saltin B, Calbet JA. Point: in health and in anormoxic environment, VO2 max is limited pri-marily by cardiac output and locomotor muscleblood flow. J Appl Physiol 2006;100:744–5.
83. Bansal N, Hyre Anderson A, Yang W, et al.High-sensitivity troponin T and N-terminal pro-B-type natriuretic peptide (NT-proBNP) and risk ofincident heart failure in patients with CKD: TheChronic Renal Insufficiency Cohort (CRIC) study.J Am Soc Nephrol 2015;26:946–56.
84. Hattori K, Ishii T, Motegi T, Kusunoki Y,Gemma A, Kida K. Relationship between serumcardiac troponin T level and cardiopulmonaryfunction in stable chronic obstructive pulmonarydisease. Int J Chron Obstruct Pulmon Dis 2015;10:309–20.
85. Oremus M, McKelvie R, Don-Wauchope A,et al. A systematic review of BNP and NT-proBNP

Husain-Syed et al. J A C C V O L . 6 5 , N O . 2 2 , 2 0 1 5
Cardio-Pulmonary-Renal Interactions J U N E 9 , 2 0 1 5 : 2 4 3 3 – 4 8
2448
in the management of heart failure: overview andmethods. Heart Fail Rev 2014;19:413–9.
86. Goto K, Arai M, Watanabe A, Hasegawa A,Nakano A, Kurabayashi M. Utility of echocardiogra-phy versusBNP level for the prediction of pulmonaryarterial pressure in patients with pulmonary arterialhypertension. Int Heart J 2010;51:343–7.
87. Bayes-Genis A, Zhang Y, Ky B. ST2 and patientprognosis in chronic heart failure. Am J Cardiol2015;115 Suppl 7:64B–9.
88. Bajwa EK, Volk JA, Christiani DC, et al. Prog-nostic and diagnostic value of plasma solublesuppression of tumorigenicity-2 concentrations inacute respiratory distress syndrome. Crit Care Med2013;41:2521–31.
89. Zheng YG, Yang T, He JG, et al. Plasma solubleST2 levels correlate with disease severity andpredict clinical worsening in patients with pulmo-nary arterial hypertension. Clin Cardiol 2014;37:365–70.
90. Bao YS, Na SP, Zhang P, et al. Characterizationof interleukin-33 and soluble ST2 in serum andtheir association with disease severity in patientswith chronic kidney disease. J Clin Immunol 2012;32:587–94.
91. Mackinnon AC, Gibbons MA, Farnworth SL,et al. Regulation of transforming growth factor-beta1-driven lung fibrosis by galectin-3. Am JRespir Crit Care Med 2012;185:537–46.
92. Hoste EA, McCullough PA, Kashani K, et al.Derivation and validation of cutoffs for clinical useof cell cycle arrest biomarkers. Nephrol DialTransplant 2014;29:2054–61.
93. Ralib A, Pickering JW, Shaw GM, Than MP,George PM, Endre ZH. The clinical utility windowfor acute kidney injury biomarkers in the criticallyill. Crit Care 2014;18:601.
94. Kaiser R, Seiler S, Held M, Bals R, Wilkens H.Prognostic impact of renal function in precapillarypulmonary hypertension. J Intern Med 2014;275:116–26.
95. Torregrosa I, Montoliu C, Urios A, et al. UrinaryKIM-1, NGAL and L-FABP for the diagnosis of AKIin patients with acute coronary syndrome or heartfailure undergoing coronary angiography. HeartVessels 2014 Jul 3 [E-pub ahead of print].
96. Ko GJ, Grigoryev DN, Linfert D, et al. Tran-scriptional analysis of kidneys during repair fromAKI reveals possible roles for NGAL and KIM-1 as
biomarkers of AKI-to-CKD transition. Am J PhysiolRenal Physiol 2010;298:F1472–83.
97. Driver TH, Katz R, Ix JH, et al. Urinary kidneyinjury molecule 1 (KIM-1) and interleukin 18 (IL-18)as risk markers for heart failure in older adults: theHealth, Aging, and Body Composition (HealthABC) Study. Am J Kidney Dis 2014;64:49–56.
98. McCullough PA, Bouchard J, Waikar SS, et al.Implementation of novel biomarkers in the diag-nosis, prognosis, and management of acute kid-ney injury: executive summary from the tenthconsensus conference of the Acute DialysisQuality Initiative (ADQI). Contrib Nephrol 2013;182:5–12.
99. Basu RK, Wong HR, Krawczeski CD, et al.Combining functional and tubular damage bio-markers improves diagnostic precision for acutekidney injury after cardiac surgery. J Am CollCardiol 2014;64:2753–62.
KEY WORDS acute kidney injury, acuterespiratory distress syndrome, cardiorenalsyndromes, chronic kidney disease, heartfailure, pulmonary hypertension