Embed Size (px)
Citation preview

J. clin. Path. (1966), 19, 220
Changes in serum enzyme levels accompanyingcardiac surgery with extracorporeal circulation
NORA WELBOURN', D. G. MELROSE, AND D. W. MOSS2
From the Nuffield Unit of Clinical Physiology, Departments of Surgery andChemical Pathology, Postgraduate Medical School, London
SYNOPSIS Serum lactic dehydrogenase, alpha-hydroxy-butyrate dehydrogenase, iso-citric dehydro-genase, and glutamic oxaloacetic transaminase activities were measured daily for two weeks post-operatively in the serum of 22 patients undergoing cardiac surgery with extracorporeal circulation.The length of perfusion was found to be a major factor affecting the extent of increased post-
operative enzyme activities. Significantly higher levels were demonstrated in patients perfused for overone hour compared with those perfused for under one hour. Hepatocellular damage, age, and type ofoperation were not considered to be major factors in determining the extent of this increased activity.A considerable increase in enzyme activity was found to occur during perfusion when the dilution
introduced by mixing the patient's circulation with the priming fluid of the heart-lung machine was
taken into account. This dilution, when accounted for, increased the observed enzyme activity by30 to 50 %.
The association of raised serum enzyme levels withdamage to heart muscle, e.g., myocardial infarction,is well documented. However, in patients undergoingcardiac surgery with extracorporeal circulationfurther study appeared to be necessary to elucidatethe role extracorporeal circulation played in therelease of these enzymes. Most workers have concen-trated on changes in serum glutamic oxaloacetictransaminase (GOT), although some have includedother enzymes such as lactic dehydrogenase (LDH)and glutamic pyruvic transaminase (GPT). It hasbeen shown that GOT increases after most surgicaloperations (Nickell and Allbritten, 1957; Lawrenceand Schulkins, 1956; Craver, Johnson, and Beal,1957; Person and Judge, 1958; Ticktin, Ostrow, andEvans, 1956; Di Carlo and Parisi, 1958; Candura andMinardi, 1957) but that this rise seldom exceeds30 international units (i.u.) per litre. The greatestincreases of GOT occurred after heart operations,especially after cardiovascular surgery with extra-corporeal circulation (Baer and Blount, 1960;Snyder, Barnard, Varco, and Lillehei, 1958; Werle,Trautschold, Gorriz, and Zill, 1961; Quinn, Sirak,'Correspondence to: Nora Welbourn, Nuffield Unit of ClinicalPhysiology, Dept. of Surgery, Postgraduate Medical School, DucaneRoad, London, W.12."Present address: Department of Clinical Chemistry, Royal Infirmary,Edinburgh, 3.Received for publication 27 October 1965.
Shabanah, and Frajola, 1960; Py6rala, Gordin,Kontinnen, and Telivuo, 1963).There is a wide divergence of opinion concerning
the reasons for these post-operative increases.Fraser, Rossall, Black, and Dvorkin (1962) andQuinn et al. (1960) suggest that the release ofenzymeis due to surgical procedures which produce directheart trauma. They show significantly higher GOTlevels in cases having ventriculotomy than thosewithout. Walker and Morgan (1964) and Baer andBlount (1960) were unable to confirm this conclusion.Snyder et al. (1958) suggest that hepatic changesoccurring during perfusion are the major sources ofincreased levels of GOT, but Walker and Morgan(1964), Baer and Blount (1960), and Norberg andSenning (1959) failed to verify this finding. It hadgenerally been assumed that increased serum enzymeactivity was due to the release of enzymes fromnecrotic cells and, in particular, organs, until Haussand Gerlach in 1958 advanced the concept of theacute syndrome. This proposed that GOT elevationwas due to the complex response of the wholeorganism rather than a local factor.
These conflicting results have led us to re-examinethe problem and to broaden the study to includeLDH, GPT, hydroxybutyrate dehydrogenase (HBD),and isocitric dehydrogenase (ICD). Hydroxy-butyrate dehydrogenase activity is associated mainly
220

Changes in serum enzyme levels accompanying cardiac surgery with extracorporeal circulation 221
with the electrophoretically faster-moving fractionsof LDH which occur predominantly in the myo-cardium (Rosalki and Wilkinson, 1960). Thisenzyme can be measured in the serum by a spectro-photometric method developed by Elliott andWilkinson (1962). It has been shown to be a sensitiveindex of myocardial infarction (Elliott and Wilkin-son, 1961; Elliott, Jepson, and Wilkinson, 1962;Hansson, Johansson, and Sievers, 1962; Konttinen,1961; Konttinen and Halonen, 1963; Pagliaro andNotarbartolo, 1961) but at no time has it beenfound to rise in the serum without a concomitantincrease in LDH (Wieme, 1962; Jontz, Bounous,Heimburger, Su, Teramoto, Shumacker, and Onnis,1960; Rosalki and Wilkinson, 1960). Isocitricdehydrogenase is generally considered to reflecthepatic damage since a sharp increase in the serumactivity follows liver cell damage, while normal valuesare obtained with myocardial infarction (White,1958; Sterkel, Spencer, Wolfson, and Williams-Ashman, 1958; Sampson, 1958). However, Strand-jord, Thomas, and White (1959) were able todemonstrate a transiently raised level of ICD duringthe first 24 hours after experimental myocardialinfarction in dogs, thus showing that the damagedmyocardium does release ICD. Its rapid disappear-ance from the circulation may account for failure todemonstrate increased levels following myocardialinfarction.
METHODS
The patients studied were divided into two main groups.In the first group serum LDH, HBD, ICD, GOT, andGPT activities were measured in 22 patients pre-operatively, immediately post-operatively, and thereafterdaily, when possible, for two weeks to ascertain thegeneral enzyme pattern following surgery. The patients inthis group were further subdivided and the resultsanalysed with respect to the following factors: age, typeof operation, and length of perfusion.
In group II the variations in serum LDH, HBD, ICD,and GOT were followed intensively throughout the per-fusion and immediate post-perfusion period in 12patients. In order to assess the actual amount of enzymereleased from the patient during perfusion it was neces-sary to take into account the dilution which occurredwhen the patient's blood was mixed with the primingvolume in the heart-lung machine. This dilution varieswith the patient's blood volume as the volume necessaryto prime the oxygenator remains fairly constant.The observed enzyme activity was corrected so as to
reflect more accurately the true enzyme activity of thepatient using the equationx =
(observed enzyme activity _ (enzyme activity in pumpx total circulating volume) x pump volume)
patient's blood volumewhen x =- the corrected enzyme activity.
All enzyme levels are expressed in i.u./litre and theblood volume is measured in litres.
This group was further subdivided in an attempt to seewhether it was possible to detect increased serum enzymeactivity during the perfusion period which could beattributed to myocardial damage. In order to do this,blood was simultaneously withdrawn from the coronarysinus, inferior vena cava, and oxygenator at the beginningand end of perfusion.The operations were performed under mild hypo-
thermia, and cardiopulmonary bypass was carried outusing the Melrose-N.E.P. disc oxygenator (Melrose,1961). The composition of the pump fluid generally con-sisted of 120 to 150 ml. of 42% sodium bicarbonate,2 5 to 3 litres of whole blood, and 15 ml. per kilogrambody weight of Rheomacrodex (Long, Sanchez, Varco,and Lillihei, 1961). The perfusion rate was maintain-ed at 2-4 litres per sq. metre of body surface area perminute.
DETERMINATION OF ENZYME ACTIVITY Lactic dehydro-genase, HBD, ICD, GOT, and GPT were determined bythe spectrophotometric methods described by Sigmausing Sigma reagents. The results are expressed in inter-national units (i.u.) per litre as recommended by theJoint Sub-Commission on Clinical Enzyme Units (Kingand Campbell, 1961) which defines 1 i.u. as the trans-formation of I ,umole of substrate per minute. Allmeasurements were corrected to 25°C.
All the peak post-operative enzyme values expressed inthis paper represent the highest level obtained within 72hours after perfusion. This was necessary, even thoughthe peak levels of GOT and ICD occurred within thefirst 24 to 48 hours, as the peak LDH and HBD activitiesoften came within the 48- to 72-hour period.
COLLECTION OF BLOOD SPECIMENS All blood was with-drawn from the patient by venepuncture except duringperfusion when samples were taken directly from theheart-lung machine. The serum was separated immediatelyand stored at 4°C. All the estimations (with the exceptionof ICD which was measured within 24 hours) were com-pleted in one week, during which time the results werereproducible within + 1 %. Visibly haemolysed specimenswere discarded since red blood cells contain appreciableamounts of LDH, HBD, ICD, and GOT, although Baerand Blount (1960) demonstrated that 80 to 100 mg. per100 ml. of free haemoglobin did not significantly alterserum GOT levels. The special inferior vena cava andcoronary sinus samples were taken by the surgeon at theoperating table. The coronary sinus blood was taken bydirect sampling from the right atrium immediately afterthe inferior and superior venae cavae had been snared andthe systemic blood diverted, then just before the snareswere released at the end of perfusion.
In one particular patient the hepatic veins did not jointhe inferior vena cava but entered the right atrium as aseparate vessel. The hepatic vein was cannulated andsamples withdrawn from it were compared with sampleswhich had been drawn simultaneously from the coronarysinus.

Nora Welbourn, D. G. Melrose, and D. W. Moss
TABLE IRELEVANT DATA AND PEAK POST-OPERATIVE ENZYME LEVELS OF THE 22 PATIENTS STUDIED IN GROUP I
Sex Age Length of Lowest LDHPerfusion Temperature (75-240)(min.) (°C.) on Bypass
HBD ICD GOT(60-120) (08-44) (4-20)
Obstructive cardiomyopathy MaleSubaortic stenosis MaleInfundibular stenosis MaleMitral incompetence MaleMitral incompetence FemaleAortic incompetence MaleMitral incompetence MaleVentricular septal defect MaleVentricular septal defect FemaleTetralogy of Fallot FemaleAtrioventricular canal MaleTetralogy of Fallot FemaleTetralogy of Fallot MaleVentricular septal defect FemaleAtrial septal defect MaleAtrial septal defect andpulmonary valvotomy MaleVentricular septal defect FemaleVentricular septal defect MaleAtrial septal defect MaleTraumatic ventricular septal defectand aneurysm of left ventricle MaleAtrial septal defect MaleVentricular septal defect Male
RESULTS
GROUP I The distribution of the patients in thisgroup according to age, sex, type of operation,length of perfusion, and peak post-operative enzymeactivity is shown in Table I.The GPT results showed no consistent variations
and as no significant conclusions could be drawnfrom them they are only shown in Table I and notdiscussed further.
LDONIUIL700r
6004
soo
400
0
0
I
0
3001-
#00LU./L
l.D.L700r
0
6001
500S-
8
v0r
0
0
0
4ooI
300-
2001
700
0
0
12.0
11.0
10.0
9.0
5.0
70
5.0
50
4.0
0
0
0
-0D-
8
8
/CO0
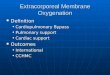
Effect of age Patients of 14 years of age andabove were considered as adults. The scatter andmean of peak post-operative enzyme levels for bothadults and children are shown in Figure 1. There isconsiderable overlapping in the individual peakpost-operative levels of LDH, HBD, ICD, andGOT between children and adults but the main peaklevels of all four enzymes are slightly higher inchildren.
Type of operation In considering the effects of
GOT
'Ora
1201_
0
-3I0-
I
l00 _0
CD
8
-a-Q
oo
60 F
40
20
a1
--U- 0
0
S0
- 8
FIG. 1. Peak post-operative enzymelevels. Mean values shown byhorizontal lines; normal rangeshaded.
I 0 Adults
222
Diagnosis GPT(2-5-18)
434457231848457i51054
1012615
151046
15
103917
7661821331641763546162647177798939
30374041
445355
252727272724271924212320232231
34242634
243126
178433420523617292525565630275414517689505351
250229
263
250262262
131294502322508371345313565266268537490178245
132248246234
164199183
467 1724.95-96-17.51238262675.4526-936
243.75-03.5
4.33 146
66368058133536710911664797811010772
44406155
425539
23617
3322
1215261629
811
91410
7
I * Children |
- V..
I

Changes in serum enzyme levels accompanying cardiac surgery with extracorporeal circulation 223
lOH /15UNITS ENZYME UNITS
(IU/LI0
00
00
-I 0
-- O0
0
500
400pI
30J
200
g00
el
00
0
12.0
11.0
10.0
9.0
8.0
7.0
5.0
5.0
0
0
a0
o_ 0
*
/CD GOT
LU.L
1201
1001-00(9
0
_ 0
.-150
60
0
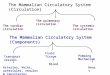
* FIG. 2. Peak post-operative* enzyme levels in patients under-
going cardiac surgery withventriculotomy (0) and withoutventriculotomy (0). Mean
* 8 values shown by horizontal lines:SP normal ranges shaded.
40 [ :
1.0go
surgical trauma the patients were subdividedaccording to those having ventriculotomy (10patients) and those not having ventriculotomy(12 patients). The patients having ventriculotomyincluded the following cases: ventricular septaldefect (7 cases), tetralogy of Fallot (3), subaorticstenosis (1), obstructive cardiomyopathy (1), andthose without ventriculotomy included atrial septaldefect (4), mitral incompetence (3), aortic incompet-ence (1), infundibular stenosis (1), and atrioventricu-lar canal (1). In Fig. 2 the scatter and mean peakpost-operative levels between the two groups areindicated. These results indicate that incision of theright ventricle alone cannot account for the main
20
0
increases observed following perfusion as there areno significant differences between the two groups.
Length of perfusion The patients were thensubdivided according to the length of perfusion withthe division arbitrarily chosen as one hour. Group Aconsists of the 14 cases perfused for over one hourand group B of the eight perfused for under one hour.In Fig. 3 each patient's daily enzyme level is indicatedas well as the mean daily levels for groups A and B.From examining these results it can be seen thatalthough the pre-operative levels are equal for bothA and B, there are significant differences betweentheir post-operative levels. The average peak levelsof LDH, HBD, and GOT are approximately twice
TABLE IIMEAN PEAK POST-OPERATIVE ENZYME LEVELS BETWEEN CHILDREN AND ADULTS PERFUSED FOR UNDER AND OVER ONE HOUR
Division by Age (adults over 14 yr.and children under 14 yr.)
No. ofCases
Average Peak Serum Enzyme Levels
LDH HBD ICD GOT(75-240) (60-120) (0-8-4-4) (4-20)
A (perfused for over one hour) Children 7 514 373 6-6 95Adults 8 427 335 5-3 65
B (perfused for under one hour) Children 3 256 202 4-0 49Adults 5 258 189 3-4 53
TABLE IIIMEAN PEAK POST-OPERATIVE ENZYME LEVELS BETWEEN PATIENTS WITH AND WITHOUT VENTRICULOTOMY
PERFUSED FOR UNDER AND OVER ONE HOUR
Group Type of Operation No. of Average Peak Serum Enzyme LevelsCases
LDH HBD ICD GOT(75-240) (60-120) (0-8-4 4) (4-20)
A (perfused for over one hour) VentriculotomyNo ventriculotomy
B (perfused for under one hour) VentriculotomyNo ventriculotomy
6 5478 4254 2254 251
389348196212
5.95 84-14-1
97654546
Group
o 1o

Nora Welbourn, D. G. Melrose, and D. W. Moss
as high in A, and, with the exception of two cases,only those patients perfused for over one hour havepeak ICD levels outside the normal limit.
Since perfusion time is clearly an important factoraffecting post-operative enzyme levels, groups Aand B were examined separately to consider whetherage or ventriculotomy affected the results when thissource of variation was eliminated. From theresults (Tables II and III) it is obvious that neitherfactor plays a determining role in affecting the meanpeak enzyme levels in the group perfused for underone hour, but in the group perfused for over one hourthe peak levels of LDH, HBD, and GOT are slightlyhigher in children and patients having ventriculo-tomy.
GROUP II In this part of the study an attempt wasmade to determine the actual amount of enzymereleased from the patient during perfusion. Thisassessment was necessary to determine the dilution
which occurred when the patient's blood was mixedwith the priming fluid of the heart-lung machine.As care was taken to choose patients having little
or no visible haemolysis, the increased enzymeactivity in the oxygenator after perfusion (Table IV)cannot be attributed to haemolysis and thereforemust represent cellular enzymes which have beenreleased from the patient during perfusion.By substituting the volumes given in Table V in
the formula (described under methods) correctionswere calculated for 12 patients. The observed andcorrected values for five patients are shown. inFigures 4-8. From examining these results it can beseen that without correction the enzyme activitiesdetermined in the first sample taken after just goingon perfusion are actually lower than the pre-perfusion levels in most cases, whereas if correctedthere is an immediate increase. It is also apparentthat without correction the serum enzyme activitydetermined immediately after perfusion is often only
,LE IVAVERAGE SERUM ENZYME LEVELS PRESENT IN THE HEART-LUNG MACHINE BEFORE AND AFTER PERFUSION
No. of Cases Serum Enzyme Levels in the Average Oxygenator Serum Enzyme LevelsHeart-lung Machine
LDH HBD ICD GOT(75-240) (60-120) (0-8-4 4) (4-20)
15 Before perfusion 157 80 0 3 10After perfusion 276 153 2-5 29
TABLE VRELEVANT DATA FOR PATIENTS IN GROUP II FROM WHICH THE DILUTION FACTOR WAS CALCULATED
FOR CORRECTED AND UNCORRECTED ENZYME LEVELS SHOWN IN FIGURES 4 TO 8Case No. Age and Sex Diagnosis Length of Patient's Oxygenator
Perfusion Blood Volume Volume(min.) (1.) (1.
1 44 Male Subaortic stenosis 60 3-6 4-852 58 Male Aortic valve replacement 132 4-54 4-53 39 Male Aortic valve replacement 80 5-06 4-44 53 Male Aortic valve replacement 93 5-12 4-755 13 Female Fallot's tetralogy 83 3-3 3-45
TABLE VICase Age and Diagnosis Perfusion Blood Specimen LDH HBD ICD GOTNo. Sex Time
(min.) 1 2 1 2 1 2 1 2
5 13 Female Fallot's tetralogy
6 29 Male Ventricular septal defect
7 15 Female Ventricular septal defect
8 14 Female Ventricular septal defect
9 10 Male Ventricular septal defect
Coronary sinus83 Inferior vena cava
OxygenatorCoronary sinus
83 Inferior vena cavaOxygenatorCoronary sinus
39 Inferior vena cavaOxygenatorCoronary sinus
47 Inferior vena cavaOxygenatorCoronary sinus
55 Inferior vena cavaOxygenator
224
305309300230175180319329300320278260285295280
382369320290247190279309280369369310310275285
668468136105110123175140868275115110100
16913810315114211517816114012410790147130118
1-10-650-6013121-11-1111*01-11-31*01-91 41-3
2-22-217112-11-11-51*91-22-1191*52-73.52-4
3330282220161514201515252120
848970343328181615302320412724

L ON0 0
0
D00
50 oo o 0 0
100
0 elvl
o FIG. 3. Pre- and post-operative enzyme levels0 in 22 patients perfusedfor more than one houi
O 0 and less than one hour (0). Mean values in e,8 group are connected: 0 0, 0 ---- 0.
se8° < 4XX Normal ranges hatched.
80 0~~~~~~~~~~~~~~~~~
0~~~~~
70 /
70~~~~~~~
50~~~~~~~~~~~~
t~~~~0 E E l S . pp~~~~~0
Pre- Post 7 2 3 5 5 7 5 9 la 77 72 13 14 Post operationpelzmP0 D~~~~~~AYS FIG. 3A.
S 8 oo~~~~ 0
w 9 ~~~~~0000 0
450 o 0 o o0o 0 0
4*7 0~~~00~~~~~~~~~~~
250 o~~~o 0
200~~~~~2 * 8°a
3eek~~~ ~ ~ ~ ~ ~ ~ ~~ -*.°o .o.
100oo
29 S 0~~~~~~~~~~~~
50~~~~~~~~~~~~~~~~~~~0~~~~~~~~~~~~~~
o I I . . . . . . . . . . .Pr- lSt 2 4 5 5 7 la70 11 12 13 14
PAafusi paAusion nAVlfuR.
r (0)ach
UA T J ri". JD-

226 Nora Welbourn, D. G. Melrose, and D. W. Moss
'CO
0
0
0 0 8 00 0
9 0~~~~~0
in ~~0
PMe- Pest 1 2 3 4 5 6 7peTsbon perfusion GA YS
60r0
8o o
0
0
00
0
00
0 0
0
0
0
0
00
0
0
0 0
o~~~~
h e-A t 1 2 3 4 5 11 12 13
-Pwfnm 7AYS FIG. 3D.
0
FIG. 3c.

Changes in serum enzyme levels accompanying cardiac surgery with extracorporeal circulation 227
CASE 1 CASE 7
[ Corrected Enzywe Value*e1 OberdIed
10.0
9.0
'U
7.0
i Si
~.
3.020
1.0
Ic,
-
N-inI.lLllaflt00 1 MSiOD
for
V
I~°° ICorreted Enzyim ValueIL*- I Obserwed is go
I Ir517.10 12.X0 1.X 2.00 1 3.x
Post pelewon4.X 5.00 6.0
FIG. 4B.
without correction for priming volume of oxygenator.
slightly increased above the pre-operative level,whereas when the dilution is corrected for, theseresults become significantly raised by 30 to 50%.
In Table VI, the results are shown of the studywhich attempted to see if myocardial damage couldbe reflected in the serum enzyme activity of bloodtaken from the coronary sinus as opposed to eitherthe inferior vena cava or the oxygenator. Only withHBD are there any consistent differences betweenthe coronary sinus and inferior vena cava samples.All five patients have higher HBD activity in thecoronary sinus sample at the end of perfusion.
In the one case in which the hepatic vein enteredthe right atrium directly, the post-operative ICDlevels exceeded normal, and therefore if the liverwere the main source of ICD one would expect toobserve a higher enzyme activity in the specimen
from the hepatic vein. In actual fact the ICD activitywas higher in the coronary sinus samples.One significant point to emerge from this particu-
lar study is that in most cases the enzyme activitiesat the end of perfusion were higher in the samplesfrom the patient than from the oxygenator. Thisindicates that the main increase in enzyme activityis due to the release of cellular enzymes from thepatient's tissues and thus emphasizes the importanceof considering the dilution factor when assessingdamage to the patient during perfusion.
DISCUSSION
The results in group I show that the length ofperfusion plays a major role in determining theamount of increased enzyme activity following
Lo#
FIG. 4A.
FIGS. 4-8. Enzyme levels during perfusion, with andNormal ranges hatched.
, ,,~~~~~~~~~~~~~.,,,W-0.#L
11
I

228 Nora Welbourn, D. G. Melrose, and D. W. Moss
CASE 2Corrected Enzyme Value
121 Observed 72
Perfusion
S#t1132'1 1132'1
700~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~7
5~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~69
40 3920
1999 00 700 70 720 00 2000400 SIN9I9W .9970799 .779799 7.99 29 399 499
Hours pmam.m Nours pm
CASE 3
[-] Corrected Enzyme Value
L I [Observed osfs
7MF k Perfusion f,80I.U/I
FIG. 5.
6oT
FIG. 6.

Changes in serum enzyme levels accompanying cardiac surgery with extracorporeal circulation 229
CASE 4
Corrected Enzyme Value|Ii- i|Observed -- "
_°~ ~~~~B"I.0/1I.U/l~~/B
I.U/l25
1)n_
GOT
'u
10 \ \ Perfusion \(93')
5
_ _ __ _
Pre-perfusion
cardiac surgery with perfusion, the mean post-operative peak levels of LDH, HBD, ICD, andGOT being significantly higher in the group perfusedfor over one hour. An effect due to age or ventriculo-tomy could be established only in the group perfusedfor over one hour. The mean peak levels of LDH,HBD, and GOT were then seen to be slightly higherin cases having ventriculotomy, and although bothadults and children had higher enzyme activitieswhen perfused for over an hour, the levels forchildren were increased above the normal limits byapproximately 30% more than those for adults.
Hepatocellular damage was not considered to be amajor source of increased enzyme activity, and the
increased ICD activity could not be attributed solelyto liver damage, as was shown by the one case inwhich there was abnormality of the hepatic veins.Campbell and Moss (1962) have shown that in theheart the predominating fraction of ICD is extremelylabile whereas that of liver ICD is more stable; thiscould account for the difficulty in demonstratingincreased ICD activity following myocardial infarc-tion. In all our cases perfusion was carried out undermild hypothermia, so that ICD being released fromthe myocardium during perfusion would be morelikely to be detected.The results in group I demonstrate the importance
of the duration of the perfusion period in influencing
1. U/II CO
Post perfusion HG. 7.

Nora Welbourn, D. G. Melrose, and D. W. Moss
CASE 5
Corrected Enzyme Value[*--- 1 Observed 'a II
.UIL
7.0605.0
4.03.02.07.0
0.0
7.7
LON
I CD
* Perfusion
(831
GOf
f/
A ,r' E~~~~~Prepefuio 'As pefso
the post-perfusion serum enzyme levels; therefore,in group II this period was studied in greater detail.The activities of all the enzymes studied increasedduring perfusion, and when corrected for dilution themajority of them exceeded the normal limits by theend of perfusion. Dilution by the oxygenator primingvolume conceals this rapid rise in enzyme levelstaking place during perfusion; the corrected levelsare some 30 to 50% higher than the measuredvalues, and emphasize the importance of perfusionas the factor which causes enzyme release from thetissues.When the enzyme activity remaining in the
oxygenator after perfusion was compared with the
pre-perfusion level, a marked increase was observed.Undoubtedly some of this came from haemolysisproduced by the pump, but by choosing cases tofollow with little or no haemolysis at the end ofperfusion, this factor could be ignored, and the in-creased enzyme activity in the oxygenator at the endof perfusion could be attributed mainly to release ofenzymes from the patient's tissues. When bleeding isextensive in the immediate post-perfusion period it isextremely difficult to assess the actual increases inenzyme activity in the patient as the blood volume iskept constant by replacement of losses with wholeblood or plasma; thus, blood with elevated enzymeactivity is being replaced by blood with a low
FIG. 8.
230
I

Changes in serum enzyme levels accompanying cardiac surgery with extracorporeal circulation 231
enzyme activity. The amount of enzyme activity lostcannot be accurately accounted for because the bloodlost is removed by high-pressure suction whichhaemolyses it severely.The results of other workers in this field are
extremely diverse. Quinn et al. (1960), Snyder et al.(1958), and Fraser et al. (1962) demonstrated higherpeak GOT levels in cases with ventriculotomy.Norberg and Senning (1959) noted increases of HBDas well as of GOT following ventriculotomy. Ingroup I of this study, although the highest singleHBD, LDH, and GOT levels occurred in patientswith a ventricular incision, no correlation could bedrawn in general between the mean peak enzymelevels and the degree of surgical trauma. This iscorroborated by Baer and Blount (1960), whoanalysed their results statistically and could show no
significant differences between Fallot operations,ventricular septal defects approached via theventricle, and ventricular septal defects with an
atrio-ventriculoris communis defect approached viathe auricle. Walker and Morgan (1964) also wereunable to demonstrate significant differences in thepeak GOT levels between cases with and withoutventriculotomy. If an increase in GOT were relatedto the extent of surgical trauma then one wouldexpect to demonstrate higher GOT levels withthoracotomies than with laparotomies. Neither ourresults nor those of Pyorala et al. (1963), Quinn et al.
(1960), and Werle et al. (1961) showed a differencebetween them.Nyhus (1958) states that in his experiments the
isolated liver tolerated perfusion poorly, developingsevere oedema. Snyder et al. (1958) suggest thatextracorporeal circulation might subject the liver toreduced oxygenation, or cause sufficient congestionto produce permeability changes in the cell membraneand allow enzymes to leak out. If this were a majorsource of increased enzymes, GPT would be expectedto increase. We could not demonstrate significantchanges in GPT, in agreement with the experienceof Walker and Morgan (1964), Baer and Blount(1960), Pyorala et al. (1963), and Norberg andSenning (1959). The last authors also measuredserum ornithine carbamyl transferase, which is amore sensitive index of liver damage than thetransaminases, and were unable to demonstratesignificant changes in its activity post-operatively.Bang, Iversen, Jagt, and Tobiassen (1959) showedthat GOT increases could come from centrilobularnecrosis following acute heart failure superimposedupon chronic heart failure, but Baer and Blount(1960) were unable to show histological evidence ofcentrilobular necrosis in the livers of patients whodied in the immediate post-operative period. Theysuggest that the chemical changes may precede the
anatomical changes and agree with the concept of'acute syndrome' as put forward by Hauss andGerlach (1958), which regards the release of enzymeas due to an overall response of the organism ratherthan to a single factor. Pyorala et al. (1963) andWerle et al. (1961) also support this idea.
Baer and Blount (1960) observed a positivecorrelation between the post-operative enzyme levelsand the duration of cardiopulmonary bypass. Theyfound that the GOT levels were significantly higherin cases perfused for over 40 minutes. Fraser et al.(1962) and Pyorala et al. (1963) were able to correlatepost-operative enzyme activity with the length ofperfusion only in cases having ventriculotomy.Snyder et al. (1958), Quinn et al. (1960), and Werle etal. (1961) suggest that no correlation exists betweenthe post-operative enzyme levels and the durationof cardiopulmonary bypass. The failure of otherworkers to demonstrate such a correlation could beaccounted for by the fact that the few investigatorswho studied the perfusion period did not considerthe dilution from the priming fluid of the heart-lungmachine to be relevant.
Other factors have been considered as possiblecauses for increasing enzyme activities. Lawrenceand Schulkins (1956) found that the type of anaes-thetic did not influence the post-operative GOTlevels following surgical operations; March, Green-berg, and Rinehart (1954) demonstrated thathaemolysis increased the enzyme levels; Crafoord,Norberg, and Senning (1957) found that, withseven to 59 minutes on bypass, the haemolysis valuesdid not exceed 15 to 55 mg. haemoglobin/100 ml. ofplasma, while Baer and Blount (1960) showed that80 to 100 mg. per 100 ml. of free haemoglobin inhaemolysed samples did not significantly alter GOTlevels. Fraser et al. (1962) found that the post-operative GOT levels in children were considerablyhigher than in adults. Werle et al. (1961) were unableto correlate the increased enzyme activity with any ofthe following factors: type of operation, length ofperfusion, hypothermia, type of anaesthetic, or age.When these results are considered together it
appears that the increased enzyme activities follow-ing cardiac surgery with extracorporeal circulationreflect the response of the whole organism to theperfusion. Increased activities do occur when cardiacsurgery is performed without perfusion but to alesser extent. The difference is even more impressiveif corrections are applied for the dilution from thepriming fluid of the heart-lung machine. The raisedenzyme activity probably results from an increasedpermeability of cellular membranes, thus allowingthe intracellular contents to enter the circulation.These changes could result from any of the following:variation in pH, lowered substrate levels, decreased

Nora Welbourn, D. G. Melrose, and D. W. Moss
oxidative phosphorylation, anoxia occurring fromdecreased peripheral circulation and exclusion ofcertain vessels due to the reversed blood flow duringperfusion, and collapse of small vessels fromhypothermia.
In assessing our results we feel that although therelease of cellular enzymes cannot be attributed to asingle source a large proportion of them are comingfrom myocardial tissue. This can be seen fromexamining the HBD results for the patients perfusedfor over one hour in group I (Fig. 3). The mean levelof HBD was still raised above normal after twoweeks whereas the other three enzymes studied weregenerally within normal limits after one week. As in-creased HBD activity is indicative of myocardialdamage, this can be taken as a sign that the heart isnot fully recovered and is still releasing enzymes intothe circulation from damaged cells.
REFERENCES
Baer, H., and Blount, S. G., Jr. (1960). The response of the serumglutamic oxaloacetic transaminase to open-heart operations.Amer. Heart J., 60, 867.
Bang, N. U., Iversen, K., Jagt, T., and Tobiassen, G. (1959). Serumglutamic-oxaloacetic transaminase activity as an index ofcentrilobular liver cell necrosis in cardiac and circulatoryfailure. Acta med. scand., 164, 385.
Campbell, D. M., and Moss, D. W. (1962). Some properties of humanisocitric dehydrogenase isoenzymes. Proc. Ass. clin. Biochem.,2, 10.
Candura, F., and Minardi, C. (1957). Sul comportamento delatransaminasi gluttammico-ossalacetica sierica in pazientisottoposti a interventi chirurgici e in soggetti traumatizzati.Minerva chir., 12, 1077.
Crafoord, C., Norberg, B., and Senning, A. (1957). Clinical studies inextracorporeal circulation with a heart-lung machine. Actachir. scand., 112, 220.
Craver, W. L., Johnson, G., Jr., and Beal, J. M. (1957). Alterationsin serum glutamic-oxaloacetic transaminase activity followingoperations. Surg. Forum, 8, 77.
Di Carlo, G., and Parisi, A. (1958). Modificazioni dell'attivita trans-aminascia nel decorso post-operatorio e suo significato.Rif. med., 71, 1275.
Elliott, B. A., and Wilkinson, J. H. (1961). Serum 'alpha-hydroxy-butyric dehydrogenase' in myocardial infarction and liverdisease. Lancet, 1, 698.
(1962). The relative efficiencies of some serum-enzymetests in the diagnosis of myocardial infarction. Ibid., 2, 71.
, Jepson, E. M., and Wilkinson, J. H. (1962). Serum alpha-hydroxybutyrate dehydrogenase-a new test with improvedspecificity for myocardial lesions. Clin. Sci., 23, 305.
Fraser, R. S., Rossall, R. E., Black, W., and Dvorkin, J. (1962).Serum transaminase response to cardiac surgery using cardio-pulmonary bypass. J. thorac. cardiovasc. Surg., 43, 810.
Hauss, W., and Gerlach, U., and Schurmeyer, E. (1958). O0ber diePathogenese und die Klinische Bedeutung der Hyperferment-minie. Dtsch. med. Wschr., 83, 1310.
Hansson, A., Johansson, B., and Sievers, J. (1962). Serum 'alpha-hydroxybutyric dehydrogenase' in myocardial infarction andin liver disease. Lancet, 1, 167.
Jontz, J., Bounous, G., Heimburger, I., Su, C. S., Teramoto, S.,Shumacker, H. B., Jr., and Onnis, M. (1960). Renal and portalblood flow under normothermic and hypothermic conditionsduring extracorporeal circulation. J. thorac. cardiovasc. Surg.,39, 781.
King, E. J., and Campbell, D. M. (1961). International enzyme units:an attempt at international agreement. Clin. chim. Acta, 6, 301.
Konttinen, A. (1961). Alpha-hydroxybutyric dehydrogenase in thedetection of myocardial infarction. Lancet, 2, 556.
, and Halonen, P. I. (1963). Serum creatine phosphokinase andalpha-hydroxybutyric dehydrogenase activities compared withGOT and LDH in myocardial infarction. Cardiologia (Basel),43, 56.
Lawrence, S. H., and Schulkins, T. H. (1956). Serum transaminaselevels following prolonged surgical anaesthesia. Anesthesiology,17, 531.
Long, D. M., Jr., Sanchez, L., Varco, R. L., and Lillihei, C. W.(1961). The use of low molecular weight dextran and serumalbumin as plasma expanders in extracorporeal circulation.Surgery, 50, 12.
March, M. E., Greenberg, L. D., and Rinehart, J. F. (1954). Trans-aminase activity of blood hemolysates. Fed. Proc., 13, 467.
Melrose, D. G. (1961). Types of heart-lung machines used in extra-corporeal circulation. Postgrad. med. J., 37, 639.
Nickell, W. K., and Allbritten, F. F., Jr. (1957). Serum transaminasecontent related to tissue injury. Surgery, 42, 240.
Norberg, B., and Senning, A. (1959). A study of serum enzymesduring and after surgery with the Crafoord-Senning heart-lungmachine. Acta chir. scand., suppl., 245, 275.
Nyhus, L. (1958). Quoted in Extracorporeal Circulation, edited byJ. G. Allen, p. 226. Thomas, Springfield, III.
Pagliaro, L., and Notarbartolo, A. (1961). Alpha-hydroxybutyricdehydrogenase in the detection of myocardial infarction.Lancet, 2, 1261.
Person, D. A., and Judge, R. D. (1958). Effect of operation on trans-aminase levels. Arch. Surg., 77, 892.
Py6rAi, K., Gordin, R., Kontinnen, A., and Telivuo, L. (1963).Serum enzymes after cardiac surgery. Acta med. scand., 174,361.
Quinn, J. W., Sirak, H. D., Shabanah, E. H., and Frajola, W. J.(1960). Transaminase values following open-heart surgery.Ann. Surg., 152, 45.
Rosalki, S. B., and Wilkinson, J. H. (1960). Reduction of alpha-ketobutyrate by human serum. Nature (Lond.), 188, 1110.
Sampson, J. J. (1958). Serum transaminase and other enzymes inacute myocardial infarction. Progr. cardiovasc. Dis., 1, 187.
Snyder, D. D., Barnard, C. N., Varco, R. L., and Lillehei, C. W.(1958). Serum transaminase patterns following intracardiacsurgery. Surgery, 44, 1083.
Sterkel, R. L., Spencer, J. A., Wolfson, S. K., Jr., and Williams-Ashman, H. G. (1958). Serum isocitric dehydrogenase activitywith particular reference to liver disease. J. Lab. clin. Med.,52, 176.
Strandjord, P. E., Thomas, K. E., and White, L. P. (1959). Studies onisocitric and lactic dehydrogenase in experimental myocardialinfarction. J. clin. Invest., 38, 2111.
Ticktin, H. E., Ostrow, B. H., and Evans, J. M. (1956). Serumglutamic oxaloacetic transaminase in trauma. Clin. Res. Proc.,4, 102.
Walker, W. F., and Morgan, H. G. (1964). Plasma-transaminaselevels in cardiac surgery with extracorporeal circulation.Lancet, 1, 683.
Werle, E., Trautschold, I., Gorriz, A., and Zill, R. (1961). OJber dasVerhalten der AktivitLt von Serum-Glutamat-Oxalacetat-Transaminase, Glutamat-Pyruvat-Transaminase und Milchs-Luredehydrogenase nach herzchirurgischen Eingriffen. Clin.chim. Acta, 6, 99.
White, L. P. (1958). Some enigmas in the comparison of multipleserum enzyme levels. Ann. N. Y. Acad. Sci., 75, 349.
Wieme, R. J. (1962). cx-Hydroxybutyric dehydrogenase in the diagnosisof myocardial infarction. Lancet, 2, 304.
232