Embed Size (px)
DESCRIPTION
cardiac surgery
Citation preview

Cardiovascular surgery is surgery on the heart or great vessels. Generally speaking, September 9th 1896 is regarded as the day on which heart surgery was founded: on this day, L. Rehn successfully closed a heart stab wound by means of a direct suture. Since then, the fascination for the heart has determined surgeons to develop this field. The thrill of feeling the beating heart in one’s hand is incomparable to any other sensation. A cardiac surgeon needs to be both powerful and meticulous because the heart is one nature’s greatest inventions and it deserves one’s utmost attention.
Anatomy review
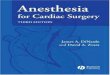
The heart is a hollow muscular organ of a conical form; it lies between the lungs in the middle mediastinum and is enclosed in the pericardium (Fig. 1). It is placed obliquely in the chest behind the body of the sternum and
adjoining parts of the rib cartilages, and projects farther into the left than into the right half of the thoracic cavity.
The heart is subdivided by septa into right and left halves, and a constriction subdivides each half of the organ into two cavities, the upper cavity being called the atrium, the lower the ventricle.
On its superior end, the base of the heart is attached to the aorta, pulmonary arteries and veins, and the vena cava. The inferior tip of the heart, known as the apex, rests just superior to the diaphragm. The base of the heart is located along the body’s midline with the apex pointing toward the left side. Because the heart points to the left, about 2/3 of the heart’s mass is found on the left side of the body and the other 1/3 is on the right.
PericardiumThe heart sits within a fluid-filled cavity called the pericardial cavity. The walls and lining of the pericardial cavity are a special membrane known as the pericardium. Pericardium is a type of serous membrane that produces serous fluid to lubricate the heart and prevent friction between the ever beating heart and its surrounding organs. Besides lubrication, the pericardium serves to hold the heart in position and maintain a hollow space for the heart to expand into when it is full. The pericardium has 2 layers—a visceral layer that covers the outside of the heart and a parietal layer that forms a sac around the outside of the pericardial cavity.
Structure of the Heart WallThe heart wall is made of 3 layers: epicardium, myocardium and endocardium.
Epicardium. The epicardium is the outermost layer of the heart wall and is just another name for the visceral layer of the pericardium. Thus, the epicardium is a thin layer of serous membrane that helps to lubricate and protect the outside of the heart.
Myocardium. The myocardium is the muscular middle layer of the heart wall that contains the cardiac muscle tissue. Myocardium makes up the majority of the thickness and mass of the heart wall and is the part of the heart responsible for pumping blood.

Endocardium. Endocardium is the simple squamous endothelium layer that lines the inside of the heart. The endocardium is very smooth and is responsible for keeping blood from sticking to the inside of the heart and forming potentially deadly blood clots.
Chambers of the HeartThe heart contains 4 chambers: the right atrium, left atrium, right ventricle, and left ventricle. The atria are smaller than the ventricles and have thinner, less muscular walls than the ventricles. The atria act as receiving chambers for blood, so they are connected to the veins that carry blood to the heart. The ventricles are the larger, stronger pumping chambers that send blood out of the heart. The ventricles are connected to the arteries that carry blood away from the heart.
The chambers on the right side of the heart are smaller and have less myocardium in their heart wall when compared to the left side of the heart. This difference in size between the sides of the heart is related to their functions and the size of the 2 circulatory loops. The right side of the heart maintains pulmonary circulation to the nearby lungs while the left side of the heart pumps blood all the way to the extremities of the body in the systemic circulatory loop.
Valves of the HeartThe heart functions by pumping blood both to the lungs and to the systems of the body. To prevent blood from flowing backwards or “regurgitating” back into the heart, a system of one-way valves are present in the heart. The heart valves can be broken down into two types: atrioventricular and semilunar valves.
Atrioventricular valves. The atrioventricular (AV) valves are located in the middle of the heart between the atria and ventricles and only allow blood to flow from the atria into the ventricles. The AV valve on the right side of the heart is called the tricuspid valve because it is made of three cusps (flaps) that separate to allow blood to pass through and connect to block regurgitation of blood. The AV valve on the left side of the heart is called the mitral valve or the bicuspid valve because it has two cusps. The AV valves are attached on
the ventricular side to tough strings called chordae tendineae. The chordae tendineae pull on the AV valves to keep them from folding backwards and allowing blood to regurgitate past them. During the contraction of the ventricles, the AV valves look like domed parachutes with the chordae tendineae acting as the ropes holding the parachutes taut.
Semilunar valves. The semilunar valves, so named for the crescent moon shape of their cusps, are located between the ventricles and the arteries that carry blood away from the heart. The semilunar valve on the right side of the heart is the pulmonary valve, so named because it prevents the backflow of blood from the pulmonary trunk into the right ventricle. The semilunar valve on the left side of the heart is theaortic valve, named for the fact that it prevents the aorta from regurgitating blood back into the left ventricle. The semilunar valves are smaller than the AV valves and do not have chordae tendineae to hold them in place. Instead, the cusps of the semilunar valves are cup shaped to catch regurgitating blood and use the blood’s pressure to snap shut.
Pathology
1. Aortic valve replacement
Aortic stenosis Calcific aortic stenosis and congenital bicuspid aortic valve stenosis account for the overwhelming majority of aortic stenosis cases, followed by less common conditions, such as rheumatic aortic stenosis and congenital aortic stenosis. Echocardiography allows assessment of the valve anatomy as well as of chamber size and ventricular function.

Aortic regurgitationAortic regurgitation can occur because of leaflet pathology or aortic root disease. As an isolated lesion,
aortic regurgitation usually occurs because of a congenital bicuspid aortic valve, often resulting from leaflet prolapse. Infective endocarditis involving the aortic valve may result in aortic regurgitation because of loss of
coaptation, leaflet retraction, or perforation.
Aortic valve replacement is a procedure in which a patient's failing aortic valve is replaced with an artificial heart valve or a bioprostheses (aortic valves processed from pigs -porcine- or cows -bovine-). Aortic valve replacement is most frequently done through a median sternotomy, meaning the incision is made by cutting through the sternum. Once the pericardium has been opened, the patient is put on a cardiopulmonary bypass machine.
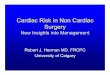
Fig. 2. Intraoperative aspect of the native aortic valve
(IBCV collection)
Once the patient is on bypass, a cut is made in the aorta and a crossclamp applied. The surgeon then removes the patient's diseased aortic valve and a mechanical or tissue valve is put in its place. Once the valve is in place and the aorta has been closed, the patient is taken off the heart-lung machine. Transesophageal echocardiogram (TEE, an ultra-sound of the heart done through the esophagus) can be used to verify that the new valve is functioning properly. Pacing wires are usually put in place, so that the heart can be manually paced should any complications arise after surgery. Drainage tubes are also inserted to drain fluids from the chest and pericardium following surgery. These are usually removed within 36 hours while the pacing wires are generally left in place until right before the patient is discharged from the hospital.
2. Coronary artery bypass surgery
Surgical anatomy of the coronary arteries
The Latin term corona, or crown, aptly describes coronary arteries that supply cardiac parenchyma with nutrient blood flow. Coronary arteries (most often 2) are normally the only vessels arising immediately above the free margin of aortic valve from the ascending aorta. The name and nature of a coronary artery or branch is defined by that vessel's distal vascularization pattern or territory, rather than by its origin. The dominance of the coronary circulation (right versus left) usually refers to the artery from which the posterior descending artery originates, not the absolute mass of myocardium perfused by the left or right coronary artery. Right dominance occurs in 85 to 90% of normal individuals. Left dominance occurs slightly more frequently in males than in females.
Coronary artery bypass surgery, also known as coronary artery bypass graft (CABG, pronounced "cabbage") surgery is a surgical procedure consisting of either diverting the left internal thoracic artery (left internal mammary artery or "LIMA") to the left anterior descending (LAD) branch of the left main coronary artery; or a harvested great saphenous vein of the leg, attaching the proximal end to the aorta or one of its major branches, and the distal end to immediately beyond a partially obstructed coronary artery (the "target vessel") - usually a 50% to 99% obstruction. The purpose is to restore normal blood flow to that partially obstructed coronary artery.
The chest is opened via a median sternotomy.The bypass grafts are harvested – frequent vessels are the internal thoracic arteries, radial arteries or saphenous veins. When harvesting is done, the patient is given heparin to inhibit blood clotting. In the case of "on-pump" surgery, the surgeon sutures cannulae into the heart and instructs the perfusionist to start cardiopulmonary bypass (CPB). Once CPB is established, there are two technical approaches: either the surgeon places the aortic cross-clamp across the aorta and instructs the perfusionist to

deliver cardioplegiawith a cooled potassium mixture to stop the heart and slow its metabolism or performing bypasses on beating state (on-pump beating).One end of each vein graft is sewn on to the coronary arteries
beyond the obstruction and the other end is attached to the aorta or one of its branches. For the internal thoracic artery, the artery is severed and the proximal intact artery is sewn to the LAD beyond the obstruction. Aside the latter classical approach, there are emerging techniques for construction of composite grafts as to avoiding connecting grafts on the ascending aorta (Un-Aortic) in view of decreasing neurologic complications.The heart is restarted; or in "off-pump" surgery, the stabilizing devices are removed. In cases where the aorta is partially occluded by a C-shaped clamp, the heart is restarted and suturing of the grafts to the aorta is done in this partially occluded section of the aorta while the heart is beating.Protamine is given to reverse the effects of heparin. Chest tubes are placed in the mediastinal and pleural space to drain blood from around the heart and lungs. The sternum is wired together and the incisions are
sutured closed.
Mitral valve repair and replacement
Mitral valve replacement is a cardiac surgical procedure in which a patient’s diseased mitral valve is replaced by either a mechanical or bioprosthetic valve.
There are two primary types of artificial mitral valves: mechanical valves and bioprosthetic tissue (biological) valves. The mechanical valves are made from metal and pyrolytic carbon, and can last a lifetime. Patients with mechanical valves must take blood-thinning medications to prevent clotting. Bioprosthetic valves are made from animal tissues. Use of these biological valves allows patients to avoid blood thinners. However, the bioprosthetic valves may only last 10 to 15 years.[6] The choice of which valve type to use depends upon the patient's age, medical condition, preferences with medication, and lifestyle.
Repair Strategy
After the analysis of the valve is carried out, a detailed reparative strategy can be deduced from the pathologic analysis.
In a broad generalization, degenerative disease of the mitral valve creates what amounts to a posterior mitral valve leaflet that is too large, with or without flail segments, in an annulus that is functionally too small for the anterior leaflet. In degenerative disease, most commonly the posterior leaflet is usually pathologic while the anterior leaflet usually is not. The first principle of the repair is to reduce or obliterate the enlarged posterior segments and to reduce the overall height of the posterior leaflet to prevent systolic anterior motion (SAM) of the anterior leaflet. If the height of the posterior leaflet is too high, it will push the anterior leaflet into the LVOT and create SAM. In general, the height of the posterior leaflet should be no more than 1 to 1.5 cm in average-sized patients once the repair is complete. The second principle is that a remodeling annuloplasty ring is essential for all repairs. The annulus, after many years of regurgitation, is often deformed and in myxomatous disease, it is floppy and dilated. The best approach to conceptualize the floppy and dilated annulus in myxomatous disease is to consider it functionally too small for the anterior leaflet. Advantages of Mitral Valve Repair to Replacement
Mitral valve repair is the best option for nearly all patients with a leaking (regurgitant) mitral valve and for many with a narrowed (stenotic) mitral valve.
Compared to valve replacement, mitral valve repair provides better long-term survival, better preservation of heart function, lower risk of complications, and usually eliminates the need for long-term use of anticoagulants.Mitral Valve Repair Surgery — Surgical Techniques Problems with the posterior leaflet are generally corrected by a small resection of the abnormal portion of the valve. Anterior leaflet dysfunction is managed by creation of new chords or chordal transfer. Anterior leaflet repair techniques are technically challenging, requiring a skilled and experienced surgical team to achieve the best result. All repairs include an annuloplasty, which is a complete or partial ring placed around the circumference (rim) of the valve.

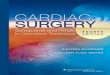
Mitral Valve Posterior Leaflet Prolapse — Valve Repair Surgery
During mitral valve repair heart surgery, triangular resection is the technique used most frequently for posterior leaflet prolapse.
Ruptured chords at free edge of posterior leaflet. Region to be resected is indicated.
Abnormal segment has been removed. Leaflet edges are sewn together.
Annuloplasty completes the repair.
Mitral Valve Anterior Leaflet Prolapse — Valve Repair SurgeryWhen there is mitral valve prolapse of the anterior leaflet, repair is more complex and requires greater
surgical expertise. To correct anterior leaflet prolapse caused by a ruptured or elongated chord, we usually create new chords out of Goretex. These Goretex chords generally last forever. A second technique used for correction of anterior leaflet prolapse is chordal transfer, which involves transfer of chords from another part of the valve to the area with abnormal chords. Both techniques provide excellent long-term results for patients.
Chordal Transfer to Treat Anterior Leaflet Prolapse
Chordal transfer to correct anterior leaflet prolapse.
Posterior leaflet chordae are transferred to the unsupported free edge of the anterior leaflet. The posterior leaflet is then repaired. A cloth annuloplasty band completes the repair.
Cardiopulmonary bypass Cardiopulmonary bypass (CPB) is a technique that temporarily takes over the function of the heart and
lungs during surgery, maintaining the circulation of blood and the oxygen content of the body. Typically, blood is gravity drained from the heart and lungs to a reservoir via venous cannulation and tubing, and returned oxygenated to the cannulated arterial system by utilizing a pump and artificial lung (oxygenator or gas-exchanger). The CPB pump itself is often referred to as a heart-lung machine or "the pump". Cardiopulmonary bypass pumps are operated by perfusionists in association with surgeons who connect the pump to the patient's body and with an anesthesiologist. CPB is a form of extracorporeal circulation.
TechniqueTraditionally, CPB is conducted with the heart approached through a median sternotomy, which
provides excellent exposure for venous and arterial cannulation. Approaching the heart through a right or left thoracotomy, a limited sternotomy (limited to upper portion or lower portion), or initiating CPB before exposing

the heart presents special cannulation problems. These alternative approaches may be used to avoid sternotomy due to previous sternotomy, especially if complicated by prior infection or aneurysms of the ascending aorta or right ventricle and to avoid patent coronary grafts that might pass beneath the sternum (e.g., right internal mammary artery to left coronary circulation). Alternative approaches also may be appropriate for focused access to specific coronary arteries (e.g., right or circumflex), for surgery involving the descending aorta, or when circulatory support is required before entering the chest (e.g., severe cardiac failure or problems encountered
during attempted reentry). These alternative approaches are also being used for minimal access or so-called minimally invasive cardiac surgery.
Partial cardiopulmonary bypassThis technique is used to facilitate descending
aortic surgery. The major issue is how to obtain systemic venous drainage. Several options are available: through the pulmonary artery with the cannula tip left in the main pulmonary artery or threaded retrograde into the right ventricle, through the right ventricular outflow tract, directly into the RA through the right atrial appendage or via the femoral vein. The problem with the latter is achieving adequate
venous drainage through long small catheters, but this is usually solved by use of thin-walled cannulas threaded up into the RA with proper positioning facilitated by TEE. Augmented venous return can be used if gravity drainage is inadequate. Direct cannulation of the RA is quite difficult with risk of compression of the heart, tearing of the atrium, and bleeding. Cannulation of the pulmonary artery is somewhat easier.
The extracorporeal circuit resembles that previously described for full CPB and includes a pump, reservoir, oxygenator, heat exchanger, and bubble trap. It is important to remember that the left ventricle is still the source of blood supply to the upper part of the body, and the heart and the patient's own lungs are providing gas exchange for that blood. Thus, the principles of relative flows to the lower part of the body and the upper part of the body described under partial left heart bypass apply. Furthermore, the adequacy of gas exchange of blood going to the upper body must be assessed separately (from samples drawn from the radial or brachial artery) from that coming out of the oxygenator and going to the lower body.
Full cardiopulmonary bypassThe only difference from what has just been discussed is that virtually all systemic venous return must
be drained from the right heart, which accentuates the demand on venous cannulation and drainage. The CPB circuit supplies all systemic flow and gas exchange. Ascending aortic cross-clamping and administration of antegrade cardioplegia can be problematic. Sasaguri described a special double-lumen balloon catheter that is inserted through the left ventricular apex into the ascending aorta with TEE guidance for occlusion of the ascending aorta and administration of cardioplegic solution during thoracic aortic surgery via a left thoracotomy.