Embed Size (px)
Citation preview
Cardiac Protectionacross the cardiac continuum
Dong-Ju Choi, MD, PhDCollege of MedicineSeoul National University

• t-PA•Cathepsin G•Tonin
Angiotensinogen
A IRenin
A IIA II
CAGECathepsin GChymase
• Antiproliferation• NO Release• Differentiation• Vasodilation
• Hypertrophy/proliferation• Vasoconstriction• Aldosterone release• Antidiuretic hormone release
AT1 receptor AT2 receptor
ACEI site of action
ACE
Degradation products
↑ Bradykinin
↑ Nitric oxide (NO)
Renin Angiotensin Cascade
de Gasparo M, et al. Hypertension. Pathophysiology, Diagnosis, and Management. 2nd ed. New York, NY: Raven Press; 1995:1695–1720. Dzau VJ. J Hypertens. 1989;7:933-936.

Pathophysiologic Effects of Angiotensin II
Burnier M, Brunner HR. Lancet. 2000;355:637–645.
AngiotensinAngiotensin IIII
Abnormalvasoconstriction
Activate SNS
↑Aldosterone
↑Vasopressin
↑Collagen
↑Contractility
↑PAI-1/thrombosis
Platelet aggregation
Superoxideproduction
↑Endothelin
Vascular smooth muscle growth
Myocyte growth

Adverse Effects of RAS on CV System
Vascular change1. Vascular remodeling2. Endothelial dysfunction3. Inflammation
Myocardial damage1. Myocyte sequestration2. Myocyte isolation

Increase BP
Ang II

Vascular Remodeling

AngII-induced InflammationThe inflammatory response by AngII:
1) Increase in vascular permeability,
2) Infiltration of leukocytes, and
3) Tissue remodeling.

Myocardial Damage by RAS
1. Myocyte sequestration• Hypertrophy• Apoptosis• Necrosis
2. Myocyte isolation• Interstitial fibrosis • Conduction disturbance

Blocking RAS is critical to prevent
1. Vascular change (Vascular remodeling, endothelial dysfunction and inflammation)
and
2. Myocardial damage(Myocyte sequestration and myocyte isolation)

The Cardiovascular Continuum:
Risk Factors:
Vascular Dysfunction
Vascular Disease
Tissue Injury
Target OrganDysfunction
End-stageOrgan Failure
Death
Oxidative Stress/EndothelialDysfunction
Target OrganDamageTissue Loss
ANGIOTENSIN II
AtherosclerosisHypertrophy
CAD
MyocardialInfarction
PathologicalRemodeling
Ventricular Enlargement
Heart Failure
Mechanisms and Mediators

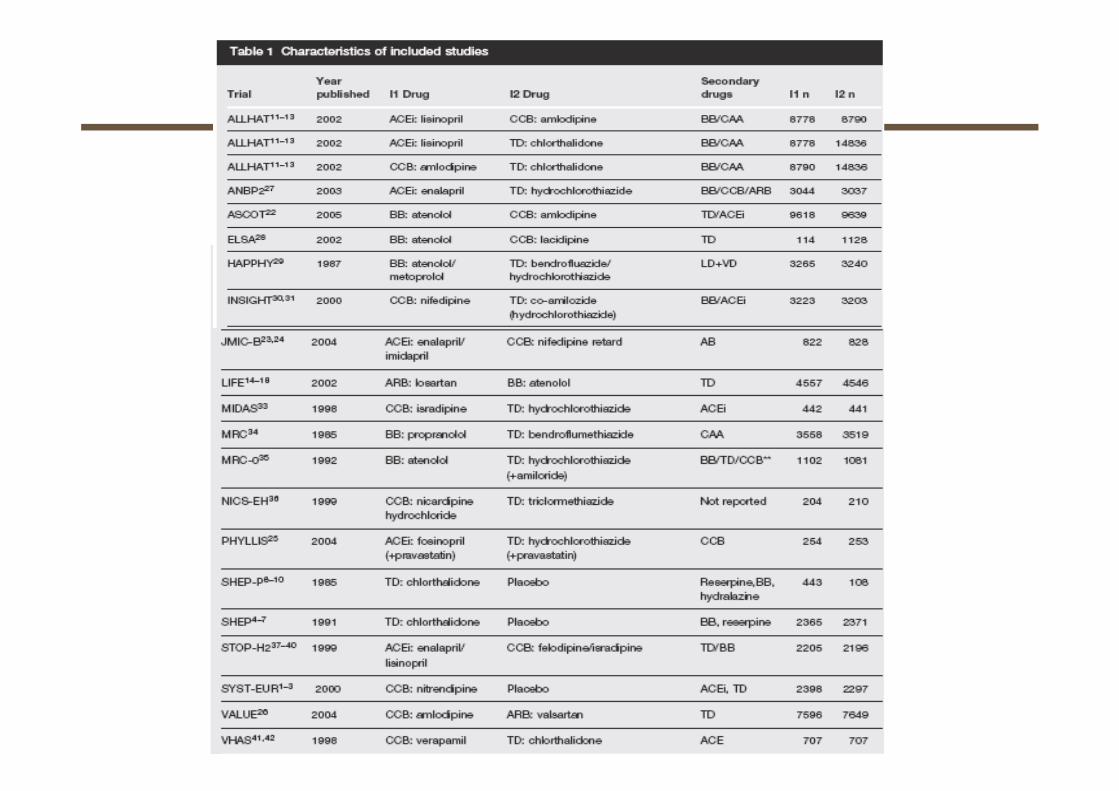
Clinical Trials with ACE inhibitors
Risk Factors:DiabetesHypertensionHyperlipdemia Death
AtherosclerosisHypertrophy
CAD
MyocardialInfarction
PathologicalRemodeling
VentricularEnlargement
Heart FailureHypertension
CAPPP, ALLHAT
DM
ABCD, REIN, AASK
Vascular and CAD
HOPE, QUIET,
EUROPA, PEACE
MI
CONSENSUS,
ISIS-4, GISSI-3
SMILE, SAVE
AIRE, TRACE
HF
SOLVD
V-HeFT II
SAVE,
ATLAS

Clinical Trials with ARB
Risk Factors:DiabetesHypertensionHyperlipdemia Death
AtherosclerosisHypertrophy
CAD, Nephropathy
MyocardialInfarction
PathologicalRemodeling
VentricularEnlargement
Heart FailureHypertension
SCOPE,
VALUE,
TROPHY, LIFE
DM/Renal
RENAAL, IDNT
IRMAII, ARVAL
ABCD-2V,
NAVIGATOR
Post-MI
VALIANT,
OPTIMAL
VAL-PREST
HF
ELITE I&II
Val-HeFT
CHARM

Amlodipine-based
(n=163)
DIOVAN-based
(n=166)
Amlodipine-based
(n=163)
DIOVAN-based
(n=166)
–6.5–6.0
–33.4 –33.5Mea
n ch
ange
in B
P (m
mH
g)
NS
NS
0
–5
–10
–15
–20
–25
–30
–35
Patients were randomised to DIOVAN 80 mg or amlodipine 5 mg
After 8 weeks, patients with SBP ≥140 mmHg were titrated to DIOVAN 160 mg/d or amlodipine 10 mg
After an additional 8 weeks, HCTZ 12.5 mg was added to treatment in patients with SBP ≥140 mmHg
DBPSBP
Randomised, double-blind, titration to effect study of patients (aged 60–80 years) with ISH: 24 weeks’ treatment
Val-Syst: Valsartan in Isolated SystolicHypertension (ISH);Per protocol population data shown; NS = not significant Clin Ther 2003;25:2765–80
Val-Syst Trial:Powerful Double-digit BP Reductions with Valsartan-based Therapy in Patients with ISH Aged 60–80

Time Course of Morning BP Changes Mediated by ARBs
Day
SBP
(mm
Hg)
–7 0 7 14 21 28
165
155
145
135
Valsartan 40–80 mg (n=18)Telmisartan 10–40 mg (n=18)
Losartan 25–100 mg (n=18)Candesartan 2–12 mg (n=18)
Start of treatment
Morning home BP
Patients with essential hypertension: 4 weeks’ treatment
Clin Exp Hypertens 2005;27:477–89

The role of arterial stiffness as the major cause of cardio-vascular risk can be seen in recent outcome data.
Pulse Wave Velocity
aortic pulse wave velocity on entry was used to stratify arterial stiffness in a cohort of ESRD patients into tertiles
1st tertile has almost normal results; 3rd tertile has 6x risk of “all cause’ mortality
The role of arterial stiffnessThe role of arterial stiffness
Clin Exp Hypertens. 2004 Oct-Nov;26(7-8):689-99

Reduces Arterial Stiffness
Am J Hypertens 2004;17:1050–5
Bra
chia
l–an
kle
PWV*
(cm
/sec
)
–195
–69
Nifedipine 20 mg (n=20) Diovan 80 mg (n=21)
p=0.02
0
–50
–100
–150
–200
–250
Randomised study of patients with hypertension: 3 months’ treatment
*Brachial-ankle pulse wave velocity (PWV), a measure for systemic arterialstiffness

Reduces Arterial Stiffness
†Augmentation index (AIx), a measure of arterial function*p<0.01 vs HCTZ and vs placebo
Randomised, double-blind, parallel-group design study of patients with essential hypertension: 6 weeks’ treatment
J Hypertens 2002;20:2423–8
• Diovan improves arterial compliance in patients with hypertension
• Effects are independent of BP reduction (BP reductions similar for Diovan and HCTZ)
–21.7*(n=20)
–3.2(n=20)
–0.3(n=20)
Cha
nge
inA
Ix†
from
bas
elin
e
Diovan 80 mg HCTZ 25 mg Placebo0
–10
–20
–30
–40

DETECTIV : Valsartan Increases Small Artery Elasticity in Asymptomatic Risk Patients with High CV Risk
Results from a 12-month study in 76 asymptomatic patients# with RDS ≥6 and controlled BP and cholesterol levels (DETECTIV study)
6 months 12 months
Cha
nge
in R
DS
from
bas
elin
e
-4
-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
44%reduction*
-2.2
-3.1
-3.9-3.6-3.6
#Individuals completing the study with or without antihypertensive or lipid lowering medications, BP <140/90 mmHg; *p<0.000; RDS=Rasmussen Disease ScoreDuprez et al.
DIOVAN 160 mg od for 12 monthsDIOVAN 160 mg od for 6 monthsPlacebo
6 months 12 monthsCha
nge
in s
mal
l art
ery
elas
ticity
from
bas
elin
e (m
L/m
mH
g x1
00)
0
0.5
1
1.5
2
2.5
3
3.577%
increase*
0.55
1.51
2.39
3.24
JACC 2007;50:published online

DIOVAN 160 mg(n=836)
Co-DIOVAN160/12.5 mg(n=832) Co-DIOVAN 320/12.5 mg
(n=808)
DIOVAN 320 mg(n=807)
Week 0Visit 1
(randomisation)
Week 2Visit 2
Week 6Visit 3
Week 12Visit 4
(End of study)
DIOVAN 320 mg (plus optional HCTZ 12.5 mg)
Co-DIOVAN 320/12.5mg (or optional Co-DIOVAN 320/25mg)
Screening
0–7 days
Val-MARC: Managing BP Aggressively and Evaluating Reductions in hsCRP
Multicentre, open-label, randomised, parallel-group study of patients with Stage II hypertension
Objectives, to determine: • If BP reduction with DIOVAN/Co-DIOVAN is effective at reducing hsCRP levels• If there is a difference between moderate and aggressive BP reduction in terms of hsCRP change
Primary endpoints:• Change in SBP from baseline to Week 6 with DIOVAN vs Co-DIOVAN• Change in hsCRP from baseline to Week 6 with DIOVAN vs Co-DIOVAN• Change in hsCRP from baseline to Week 12 in the overall group
Hypertension 2006;48:73-79

Val-MARC : DIOVAN Reduces hsCRP Levels Independent of Blood Pressure Reduction
Results from a 6-week study* in 1,615 patients with stage II HTN#
(Val-MARC study)C
hang
e in
hsC
RP
plas
ma
leve
l (%
)fr
om b
asel
ine
to 6
wee
ks*
DIOVAN 160 - 320 mg od
(n=807, median change -0.12)
Co-DIOVAN 160/12.5 - 320/12.5 mg od
(n=808, median change +0.05)
#SBP ≥160 mmHg or DBP ≥100 mmHg, patients completing the study; *Study duration 12 weeks, after 6 weeks of treatment, HCTZ 12.5 mg/day allowed at discretion in both groups to reach BP <140/90 mmHg); p<0.001 for DIOVAN vs. Co-DIOVAN Ridker et al.
-8.9%
4.4%
-10
-8
-6
-4
-2
0
2
4
6
Hypertension 2006;48:73-79

Month –0.5 0 1 2 3 4 6 * 72
Amlo 10 mg +HCTZ 25 mg
Amlo 5 mg
Amlo 10 mg +HCTZ 12.5 mg
Amlo 10 mg
DIOVAN 80 mg
DIOVAN 160 mg
Co-DIOVAN 160/12.5 mg
Co-DIOVAN 160/25 mg
Amlodipine-based regimen
DIOVAN 160 mg +HCTZ 25 mg + ‘Free’ add-on
Amlo 10 mg +HCTZ 25 mg + ‘Free’ add-on
DIOVAN-based regimen
ScreeningRandomisation End of treatment adjustment period
Rolloverfromprevious therapy(92%)
*Patient visits every 6 months forMonths 6–72; Amlo = amlodipine
VALUE: Elective Titration to Target BP(<140/90 mmHg)
Lancet 2004;363:2022–31
Patients aged ≥50 years, with treated or untreated hypertensionand at high risk of CV events

Number at risk
Amlodipine 7,596 7,469 7,424 7,267 7,117 6,7726,955 6,576 5,959 3,725 1,4746,391
DIOVAN 7,649 7,459 7,407 7,250 7,085 6,7326,906 6,536 5,911 3,765 1,4746,349
Time (months)0 6 12 18 24 30 36 42 48 54 60 66
Prop
ortio
n of
pat
ient
s w
ith
first
eve
nt (%
)DIOVAN-based regimenAmlodipine-based regimen
HR=1.03; 95% CI=0.94–1.14; p=0.49
14
12
10
8
6
4
2
0
VALUE: Rate of Cardiac Events Did not Differ Between the Vasarta and Amlodipine Groups
Lancet 2004;363:2022–31

LIFE :The Losartan Intervention For Endpoint Reduction in Hypertension Study
* Titration encouraged if SiDBP >90 mmHg or SiSBP >140 mmHg but was mandatory if SiBP >160 / 95 mmHg**Other antihypertensives excluding ACEIs, A II antagonists, beta blockers
Day −14
Day−7
Day1
Mth1
Mth2
Mth4
Mth6
Yr1
Yr1.5
Yr2
Yr2.5
Yr3
Yr3.5
Yr4
Yr5
* Titration to target blood pressure: <140 / 90 mmHg
Placebo Losartan 50 mg
Atenolol 50 mg
Losartan 50 mg + HCTZ 12.5 mg*
Losartan 100 mg + HCTZ 12.5 mg*
Losartan 100 mg + HCTZ 12.5- 25 mg + others**
Atenolol 50 mg + HCTZ 12.5 mg*
Atenolol 100 mg + HCTZ 12.5 mg*
Atenolol 100 mg + HCTZ 12.5- 25mg + others**
Lancet 2002;359;995-1003-1010
Patients aged ≥55 years, with treated or untreated hypertensionand at high risk of CV events

LIFE : BP reductions
Time (months)
Lancet 2002;359;995-1003-1010
Systolic
Diastolic
Mean arterialmm
Hg
180
160
140
120
100
40
80
60
423624 3012 1860 48 54
AtenololLosartan

Endp
oint
Rat
e
LIFE : Primary Composite Endpoint
0 180 360 540 720 900 1080 1260 1440 1620 1800 1980Study Day0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0.16
Intention-to-Treat
Losartan
Atenolol
Study Month 0 6 12 18 24 30 36 42 48 54 60 66Losartan (n) 4605 4524 4460 4392 4312 4247 4189 4110 4045 3895 1888 901Atenolol (n) 4588 4494 4414 4349 4289 4205 4135 4066 3992 3821 1854 876
Adjusted Risk Reduction 13·0%, p=0·021Unadjusted Risk Reduction 14·6%, p=0·009
Lancet 2002;359;995-1003-1010

Atrial fibrillation accounts for 1/3 of all patientsdischarges with arrhythmia as principal diagnosis
2% VF
J Am Coll Cardiol. 1992;19(3):41A.
34% Atrial
Fibrillation
18% Unspecified
6% PSVT
6% PVCs
4%Atrial
Flutter
9% SSS
8%Conduction Disease
3% SCD10% VT

Relative Risk of Stroke and Mortality in Patients with AF vs. without AF
Lancet 1987;1:526Am Heart J 1983;106:389 Am J Med 1995;98:476
0
2
4
6
8
Whitehall
Framingham(no Heart Disease)
Framingham (overall)
Manitoba
Whitehall
Regional Heart Study
Framingham
Stroke MortalityR
ela
tive R
isk (
tim
es)
Stroke rate in Non-Rheumatic HD with AF : ↑5% / year
(Patients without AF)

VALUE - AF :Reduces the risk of new onset AF by 16%
J Hypertens 2008, 26:403–411
•DIOVAN significantly reduces the risk of new-onset AF by 16% compared with amlodipine
•DIOVAN significantly reduces the risk of persistent AF by 32% compared with amlodipine

VALIANT: Study Design and Inclusion Criteria
Primary endpoint: All-cause mortalitySecondary endpoints: CV morbidity and mortalityOther endpoints: Safety and tolerability
Captopril 50 mg tid(n=4,909)
DIOVAN 160 mg bid(n=4,909)
Captopril 50 mg tid + DIOVAN 80 mg bid
(n=4,885)
0.5–10 days after acute MI – SAVE, AIRE or TRACE eligible(either clinical/radiological signs of HF or LVSD)
Major exclusion criteria
– Serum creatinine >2.5 mg/dL
– DBP <100 mmHg
– Prior intolerance of an ARB or ACE-IDouble-blind active-controlled, stepwise titration
Median duration: 24.7 monthsEvent-driven
Am Heart J 2000;140:727–50N Engl J Med 2003;349:1893–906

VALIANT: Risk of Mortality is Similarly Reduced with Valsartan and Captopril
N Engl J Med 2003;349:1893–906
0.30
Prob
abili
ty o
f dea
th
from
any
cau
se
0
0.05
0.10
0.15
0.20
0.25
0 6 12 18 24 30 36Time (months)
DIOVAN vs captopril: HR=1.00; p=0.98
Captopril 50 mg tid* (n=4,909)DIOVAN 160 mg bid* (n=4,909) DIOVAN 80 mg bid + captopril 50 mg tid* (n=4,885) *titration to target dose
DIOVAN + captopril vs captopril: HR=0.98; p=0.73
Patients with acute MI complicated by either HF or LVSD
Captopril 4,909 4,428 4,241 4,018 2,635 1,432 364 Diovan 4,909 4,464 4,272 4,007 2,648 1,437 357 Diovan + captopril
4,885 4,414 4,265 3,994 2,648 1,435 382
LVSD = left ventricular systolic dysfunctionHF = heart failure

OPTIMAAL(Optimal Trial in Myocardial Infarction with the Angiotensin II Antagonist Losartan)
Lancet 2002;360:752–60
50 years of age AMI-patients with heart failure or anterior Q-wave AMI
31,738 assessed
26,261 excluded
5,477 randomised
2,744 Losartan
2,733 Captopril
2,744 analysed 2,733 analysed
459 discont’d 424 discont’d

25
20
15
10
5
0
Endp
oint
rate
(%)
0 6 12 18 24 30 36
Losartan (n= 2,744)Captopril (n=2,733)
Relative risk 1.13 (85% CI 0.99–1.28) p=0.069
OPTIMAAL: No Difference in Mortality Risk Between Losartan and Captopril
Months
Lancet 2002;360:752–60

Val-HeFT (The Valsartan in Heart Failure Trial )
5,010 patients with HF ≥18 years; EF <40%; NYHA II–IV; LVIDd >2.9 cm/m2
ACE-I (93%), diuretics (86%),digoxin (67%), beta-blockers (36%)
DIOVAN 40 mg bid titrated to 160 mg bid
Two primary endpoints: 1) Mortality 2) Combined endpoint of mortality and morbidity
Randomised to
Receiving standard therapy
Placebo
EF = ejection fractionNYHA = New York Heart Association LVIDd = left-ventricular internaldiastolic diameter N Engl J Med 2001;345:1667–75

Val-HeFT: Improves CV Outcomes* in CHF
Time (months)
100
95
90
85
80
75
70
65
0
Even
t-fre
e pr
obab
ility
(%)
DIOVAN‡ (n=2,511)
Placebo (n=2,499)
13.2%risk
reduction†
*Combined 1° endpoint: all-cause mortality, cardiac arrest with resuscitation, hospitalization for worsening HF, or therapy with intravenous inotropes or vasodilators; †p=0.009 vs. placebo; 1° endpoint of mortality was not significantly different between valsartan and placebo; ‡DIOVAN regimen started at 40 mg bid after placebo run-in, doubled every 2 weeks to target 160 mg bidCohn et al.
0 3 6 9 12 15 18 21 24 27
Results from a 23-month mean follow-up study in 5,010 patients with CHF on standard therapy (Val-HeFT study)
RR=0.87; 97.5% CI: 0.77-0.97
N Engl J Med 2001;345:1667-1675

≥ 60 yrs; NYHA II - IV; EF ≤ 40 %ACEI naive or < 7 days in 3 months prior to entry
Standard Rx ( ± Dig / Diuretics ), ß - blocker stratification
Captopril50 mg 3 times daily
n = 1574
Losartan50 mg daily
n = 1578
Event DrivenTargeting 510 deaths
estimate 2 yrsmedian follow-up 555 days
Primary Endpoint : All-cause MortalitySecondary Endpoint : Sudden cardiac death and/or Resuscitated ArrestOther : All-cause Mortality / Hospitalizations
Safety and Tolerability
ELITE II :Evaluation of Losartan in the Elderly Study
Lancet 2000;355:1582–87
Randomised trial of losartan versus captoprilin patients over 65 with heart failure

1.0
0.8
0.6
0.4
0.2
00 100 200 300 400 500 600 700
Follow-up (days)
Even
t-fre
e pr
obab
ility
Losartan (n=1578)Captopril (n=1574)
p=0.18
ELITE II:
Lancet 2000;355:1582–87
Risk of All-cause Mortality or Hospital Admission is Similarly Reduced with Losartan and Captopril

JIKEI HEART : Valsartan-based Therapy Improved Outcomes in Japanese Patients with HT and/or Coronary Heart Disease and/or HF
Run-in
Conventional treatment (non-ARB)
Conventional treatment (non-ARB) + non-ARB
+ non-ARB
+ non-ARB
+ valsartan 40–80 mg daily
+ valsartan40–160 mg daily
+ non-ARBtreatmentValsartan-based therapy group
(n=1541)
Non-ARB treatment arm(n=1540)
Randomisation 0
Titration 8–12
Titration 12–16
End of study(median follow-up
was 3.1 years)
–4
Weeks
Mochizuki et al. Lancet 2007;369:1431–9

40*
Stroke/TIA
JIKEI HEART R
isk
redu
ctio
n (%
) 65*
Hospitalisation for angina
47*
Hospitalisation for HF
39*
CV mortality and morbidity†
0
20
40
60
80TIA = transient ischemic attack*With DIOVAN-based therapy comparedwith non-ARB therapy; †primary endpoint Lancet 2007;369:1431–9
p=0.0002 p=0.0280p=0.0293
p=0.0001

0
10,000
20,000
30,000
40,000
50,000
60,000VALUE1
VALIANT2
NAVIGATOR3
Val-HeFT4
JIKEI HEART5,6
KYOTO HEART*7
Num
ber o
f pat
ient
s
DIOVAN Telmisartan Losartan Candesartan Irbesartan Olmesartan Eprosartan
50,345
29,400
22,99119,768
1,000 1,405
CHARM14
SCOPE15
SCAST*16
CASE-J17
I-Preserve18
IDNT19
ACTIVE*20
SUPPORT*21
MOSES22
1Julius et al. Lancet 2004;363:2022–31; 2Pfeffer et al. NEJM 2003;349:1893–906; 3www.novartis.com; 4Cohn et al. NEJM 2001;345:1667–75; 5Mochizuki et al. J Hypertens 2006;24(Suppl. 4):S31; 6Mochizuki et al. Cardiovasc Drugs Ther 2004;18:305–9; 7http://clinicaltrials.gov (NCT00149227) 8www.ontarget-micardis.com; 9Dahlof et al. Lancet 2002;359:955–1003; 10Dickstein et al. Lancet 2002;360:752–60; 11Pitt et al. Lancet 2000;355:1582–7; 12Brenner et al. NEJM 2001;345:861–9; 13http://clinicaltrials.gov (NCT00090259) 14www.atacand.com; 15Papademetriou et al. J Am Coll Cardiol 2004;44:1175–80; 16http://clinicaltrials.gov (NCT00120003); 17Ogihara J Hypertens 2006;24(Suppl. 4):S30; 18Carson et al. J Card Fail 2005;11:576–85; 19Lewis et al. NEJM 2001;345:851–60; 20http://clinicaltrials.gov (NCT00249795); 21http://clinicaltrials.gov (NCT00417222); 22Schrader et al. Stroke 2005;36:1218–26*Expected enrolment
ONTARGET8
TRANSEND8
LIFE9
OPTIMAAL10
ELITE II11
RENAAL12
NCT00090259*13
14,815
Mortality and Morbidity Endpoint Trials with ARB




Summary:To protect and improve vascular and cardiac structure/function• understanding the effects of angiotensin II is an important issue
in HT.
Blocking the negative effects of angiotensin II at the AT1 receptor• improves endothelial function,• improves inflammation,• reduces oxidative stress• improves left ventricular remodeling and function
ARB has proven clinical benefits from HT to HF patients in the spectrum of CV continuum.
ARB provides proven cardioprotective benefits.