Embed Size (px)
Citation preview
Yaisipw5
FPwo(G
2
Journal of the American College of Cardiology Vol. 55, No. 25, 2010© 2010 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00P
Postural Orthostatic Tachycardia Syndrome
Cardiac Origins of the PosturalOrthostatic Tachycardia Syndrome
Qi Fu, MD, PHD,*† Tiffany B. VanGundy, MS,* M. Melyn Galbreath, PHD,*†Shigeki Shibata, MD, PHD,*† Manish Jain, MD,*† Jeffrey L. Hastings, MD,*†Paul S. Bhella, MD,*† Benjamin D. Levine, MD*†
Dallas, Texas
Objectives The purpose of this study was to test the hypothesis that a small heart coupled with reduced blood volume contrib-utes to the postural orthostatic tachycardia syndrome (POTS) and that exercise training improves this syndrome.
Background Patients with POTS have marked increases in heart rate during orthostasis. However, the underlying mecha-nisms are unknown and the effective therapy is uncertain.
Methods Twenty-seven POTS patients underwent autonomic function tests, cardiac magnetic resonance imaging, andblood volume measurements. Twenty-five of them participated in a 3-month specially designed exercise trainingprogram with 19 completing the program; these patients were re-evaluated after training. Results were com-pared with those of 16 healthy controls.
Results Upright heart rate and total peripheral resistance were greater, whereas stroke volume and cardiac output weresmaller in patients than in controls. Baroreflex function was similar between groups. Left ventricular mass (me-dian [25th, 75th percentiles], 1.26 g/kg [1.12, 1.37 g/kg] vs. 1.45 g/kg [1.34, 1.57 g/kg]; p � 0.01) and bloodvolume (60 ml/kg [54, 64 ml/kg] vs. 71 ml/kg [65, 78 ml/kg]; p � 0.01) were smaller in patients than in con-trols. Exercise training increased left ventricular mass and blood volume by approximately 12% and approxi-mately 7% and decreased upright heart rate by 9 beats/min [1, 17 beats/min]. Ten of 19 patients no longermet POTS criteria after training, whereas patient quality of life assessed by the 36-item Short-Form Health Sur-vey was improved in all patients after training.
Conclusions Autonomic function was intact in POTS patients. The marked tachycardia during orthostasis was attributable toa small heart coupled with reduced blood volume. Exercise training improved or even cured this syndrome inmost patients. It seems reasonable to offer POTS a new name based on its underlying pathophysiology, the“Grinch syndrome,” because in this famous children’s book by Dr. Seuss, the main character had a heart thatwas “two sizes too small.” (J Am Coll Cardiol 2010;55:2858–68) © 2010 by the American College ofCardiology Foundation
ublished by Elsevier Inc. doi:10.1016/j.jacc.2010.02.043
paaee
dwsaiatci
oung women are more susceptible to orthostatic intoler-nce than similarly aged men (1–3), and this sex differences more dramatic in the postural orthostatic tachycardiayndrome (POTS) (also called chronic orthostatic intolerance),n which patients are unable to stand or remain upright forrolonged periods because of intolerable light headedness,eakness, and near syncope. This disorder affects more than00,000 Americans (3), the vast majority of whom are
rom the *Institute for Exercise and Environmental Medicine, Texas Healthresbyterian Hospital Dallas, Dallas, Texas; and †The University of Texas South-estern Medical Center at Dallas, Dallas, Texas. Supported by the National Institutesf Health (K23 grant HL075283); the National Space Biomedical Research Institutegrant CA00701); and the Clinical and Translational Research Center (formerly theeneral Clinical Research Center; grant RR00633).
wManuscript received November 3, 2009; revised manuscript received January 6,
010, accepted February 1, 2010.
re-menopausal women. Severely affected patients are un-ble to work, to attend school, or to participate in recre-tional activities, resulting in substantial morbidity. How-ver, the underlying mechanisms remain unknown and theffective therapy is uncertain.
Sex differences in orthostatic tolerance become moreramatic after spaceflight or a period of bed rest (4,5), inhich deconditioning occurs. Numerous studies have
hown that real or simulated microgravity exposure can elicitPOTS-like syndrome even in healthy, fit individuals. The
nduced tachycardia during orthostasis has been found to bessociated with reduced stroke volume, which is attributableo cardiac atrophy and hypovolemia (6,7). Indeed, withhest roentgenographic and echocardiographic techniques,t was observed that the heart was much smaller in patients
ith chronic fatigue syndrome, a condition with substantial
oips(PdH
epshicscvhcpowbit
M
ScFEcitmcpstedeb(c�oohwitba
cvb
fAascasrstaslwwtim
ectwsasHScnnriaatttbabitd
S
(tpes
2859JACC Vol. 55, No. 25, 2010 Fu et al.June 22, 2010:2858–68 Exercise Training in POTS
verlap with POTS, than in healthy controls (8). Decreasesn blood volume also have been reported in many POTSatients (9,10). In addition, most of these patients haveignificant limitations to even low-intensity physical activity11–13). Based on these observations, we speculated thatOTS per se may be a consequence or signature ofeconditioning, namely, cardiac atrophy and hypovolemia.owever, this speculation needs to be verified.Clarifying the pathophysiologic features of POTS is
ssential for determining optimal evidence-based therapy,articularly because many of these patients have disablingide effects with drug treatment. One nondrug therapy thatas shown some promise is exercise training. For example,
ncreased orthostatic tolerance after mild to moderate exer-ise training was reported in patients with unexplainedyncope or orthostatic hypotension (14,15). Physical exer-ise training has been shown to increase plasma and bloodolume (16). However, its effect on orthostatic tolerance inealthy individuals is controversial (17–19). Whether exer-ise training can be regarded as an effective therapy foratients with POTS needs to be determined. The primarybjective of this study was to test the hypothesis that POTSould be attributable to a small heart coupled with reducedlood volume (i.e., deconditioning) and that exercise train-ng could improve or even cure this syndrome by targetinghe underlying pathophysiology.
ethods
tudy population. The patient population consisted of 54onsecutive patients referred to our tertiary Autonomicunction Clinic between December 2004 and April 2008.ight patients declined to participate immediately after we
ontacted them because they were not interested in partic-pating in research. Forty-six patients were screened; 18 ofhem declined because they were not willing to be withoutedications for several months and to undergo all the
omprehensive assessments before treatment. Twenty-eightatients (27 women, 1 man) eventually were enrolled in thetudy. The severity of POTS was not different betweenhose who declined participation and those who werenrolled in the study. Among these 28 patients, 1 wasiagnosed with Ehlers Danlos syndrome after baselinevaluations and thereafter was excluded from the study,ecause this syndrome may affect cardiac size and function20). All patients met the inclusion without exclusionriteria for POTS (12) and had a heart rate (HR) rise of30 beats/min or a rate that exceeded 120 beats/min that
ccurred after 10 min of standing without any evidence ofrthostatic hypotension (9). Approximately 55% of themad mild POTS (i.e., an increase in HR �35 beats/min),hereas 45% had moderate to severe POTS (i.e., an
ncrease in HR �35 beats/min). Most patients had beenreated at some point with standard medications such aseta-blockers, volume expanders, and alpha1-adrenergic
gonists. Patients had stopped taking medications that dould affect the autonomic ner-ous system 2 weeks or moreefore screening and testing.Healthy controls were recruited
rom the Dallas-Fort Worth area.pproved flyers were posted in an
dvertisement format in locationsuch as local recreational centers,hurches, grocery stores, colleges,nd shopping centers. Potentialubjects were asked to contact ourecruiting staff to inquire about thetudy. Our experienced recruiting nurse performed initialelephone screening. If they did not have any exclusion criteriand seemed to have a sincere interest after explanation of thetudy purpose and requirements, they were invited to ouraboratory for a formal screening. Sixteen healthy controls (15omen, 1 man) eventually were enrolled. Matching of groupsas used in this study with the goal for the patient group and
he control group to be comparable with regard to demograph-cs and confounders; the groups had approximately the same
ean age, sex, height, weight, and body mass index.All participants were nonsmokers. None was an
ndurance-trained athlete (19,21). All were screened with aareful medical history, physical examination, 12-lead elec-rocardiogram, and a 10-min stand test. All participantsere informed of the purpose and procedures used in the
tudy and gave their written informed consent to a protocolpproved by the Institutional Review Boards of the Univer-ity of Texas Southwestern Medical Center and Texasealth Presbyterian Hospital Dallas.
tudy design. BASELINE ASSESSMENTS. All participantsompleted baseline evaluations, which included: 1) auto-omic function tests and blood volume measurements; 2)eurohumoral regulation during 2-h standing (data to beeported elsewhere); and 3) cardiac magnetic resonancemaging (MRI) assessments. Ten female POTS patientsnd 11 healthy women who had normal menstrual cyclesnd were not taking or had not been taking oral contracep-ives for 6 months or more were studied twice, once duringhe early follicular phase (when both estrogen and proges-erone are low) and once during the mid-luteal phase (whenoth sex hormones are high), with the order counterbal-nced. Patients then were assigned randomly to a beta-locker versus placebo drug intervention trial before partic-pation in exercise training (22). For the sake of simplicity,he beta-blocker trial and the effect of the menstrual cycleata will be reported separately.
HORT-TERM EXERCISE TRAINING. Twenty-five patients24 women, 1 man) participated in an optimized exerciseraining program for 3 months with 19 completing therogram, and these patients were evaluated again afterxercise training during the mid-luteal phase of the men-trual cycle. Because of the complexity of the overall study
Abbreviationsand Acronyms
BP � blood pressure
HR � heart rate
MRI � magnetic resonanceimaging
MSNA � musclesympathetic nerve activity
POTS � postural orthostatictachycardia syndrome
esign, we only report here data
obtained from baseline
aPAw1wdop
mccparpar6wstpt6
Flr(ws(1ts2ptwtcCstlraast2bwu
taweEtesdsmt
peImmbcstssaentwtrWsmiidcsqHDcmianiwarphq
2860 Fu et al. JACC Vol. 55, No. 25, 2010Exercise Training in POTS June 22, 2010:2858–68
ssessments in all participants and after exercise training inOTS patients in this paper.utonomic function tests. All participants were providedith an isocaloric constant diet consisting of 200 mEq sodium,00 mEq potassium, and 1,000 mg calcium, and fluid intakeas ad libitum 2 days before testing. Women were testeduring the mid-luteal phase (i.e., 19 to 22 days after the onsetf menstruation) of their menstrual cycles. They took aregnancy test and showed negative results on the testing day.The experiments were performed in the morning 2 h orore after a light breakfast, and 48 h or more after the last
affeinated or alcoholic beverage in a quiet, environmentallyontrolled laboratory with an ambient temperature of ap-roximately 25°C. An intravenous catheter was inserted inton antecubital vein of the nondominant arm, and a smallecording electrode was placed in the peroneal nerve at theopliteal fossa for obtaining muscle sympathetic nervectivity (MSNA) signals (23). After 30 min or more of quietest in the supine position, baseline data were collected formin. After that, a Valsalva maneuver (40 mm Hg, 20 s)as performed, followed by a cold pressor test for 2 min and
tatic handgrip sustained to fatigue at 40% maximal volun-ary contraction force (dominant arm), with 2 min ofost-exercise circulatory arrest. After a sufficient recovery,he subject was tilted passively to 30° upright for 6 min and0° upright for 45 min or until pre-syncope.HR (electrocardiogram), blood pressure (BP) (Portapres,
inapres Medical Systems BV, Amsterdam, the Nether-ands), MSNA (microneurography) (23), and respiratoryate (nasal cannula) were recorded continuously. Arm BPSunTech, Jiangsu Province, People’s Republic of China)as measured intermittently for the calculation of steady-
tate hemodynamics. Cardiac output (acetylene rebreathing)24) was measured supine, at the end of 30° tilt, and after 5,0, 20, 30, and 40 min of 60° tilt. Both stroke volume andotal peripheral resistance were calculated (1,25). Bloodamples were obtained in the supine position and after 5 and0 min of 60° tilt. The subject was returned to the supineosition for recovery either after completing 45 min ofilting or the development of pre-syncope. Blood volumeas measured by a modified carbon monoxide rebreathing
echnique (26,27), with a typical error (expressed as coeffi-ient of variation) of 4% to 5% in our laboratory.ardiac MRI. Cardiac MRI was acquired by a 1.5-T MRI
canner. After completing the standard imaging protocol forhe assessment of mass and volume (28), gradient echo, cineong- and short-axis MRI sequences with a temporalesolution of approximately 42 ms, a repetition time ofpproximately 4 ms, an echo time of approximately 2 ms,nd a flip angle of 55° were obtained. The heart wasectioned in 6-mm slices with a gap of 4 mm spanning fromhe apex to the base, and the image resolution was 256 �56 with a 330-mm field of view. One observer who waslinded to the study read the MRI results. Short-axis slicesere used for left ventricular volume and mass calculations
sing the MRI Analytical Software System (MEDIS, Leiden, ahe Netherlands). The typical error of the intraoperator vari-bility of the manual planning of cardiac MRI in our laboratoryas 1.6% for left ventricular mass and 1.3% for left ventricular
nd-diastolic volume assessments.xercise training. A modified Astrand-Saltin incremental
readmill protocol was used to determine each patient’s peakxercise capacity before training. Based on the maximalteady-state HR and resting HR, 3 training zones wereetermined (i.e., recovery, base pace, and maximal steadytate). To quantify the training stimulus, we used theethod of Banister et al. (29) for the calculation of the
raining impulse.Most of the training sessions, particularly during the early
hases, were prescribed as base training, with the target HRquivalent to approximately 75% to 85% of maximal.nitially, patients trained 2 to 4 times per week for 30 to 45in/session by using a recumbent bike, rowing, or swim-ing. The use of only semirecumbent exercise at the
eginning was a critical strategy, allowing patients to exer-ise while avoiding the upright posture that elicits theirymptoms. As the patients became relatively fit, the dura-ion of the base training sessions was prolonged, andubsequently sessions of increased intensity (i.e., maximalteady state) were added first once and then twice per week,nd were always followed by recovery sessions. Uprightxercise was added gradually as tolerated, although usuallyot until the second or third month. By the end of theraining, patients were exercising 5 to 6 h per week, and theyere encouraged to use an upright bike, to walk on the
readmill, or to jog. In addition to the endurance training,esistance training such as weight lifting was also used.
eight lifting started from once weekly, 15 to 20 min/ession and gradually increased to twice weekly, 30 to 40in/session. Additionally, patients were encouraged to
ncrease their daily salt intake to 6 to 8 g/day and waterntake to 3 to 4 l/day and to elevate the head of the beduring sleeping at night. Patients were encouraged toontinue to train at the same level indefinitely after thetudy so as to maintain their fitness and heart health. Patientuality of life was assessed using the 36-item Short-Formealth Survey (30) before and after training.ata analysis. Sympathetic bursts were identified by a
omputer program (31) and then were confirmed by aicroneurographer. The integrated neurogram was normal-
zed by assigning a value of 100 to the largest amplitude ofburst during baseline. All bursts for that trial were then
ormalized against that value (32). Burst areas of thentegrated neurogram and systolic and diastolic pressuresere measured simultaneously on a beat-to-beat basis. Total
ctivity of the burst was defined as the burst area of theectified and integrated neurogram. The number of burstser minute (burst frequency), the number of bursts per 100eart beats (burst incidence), and total activity were used asuantitative indexes.Sympathetic baroreflex sensitivity was assessed by relating
ll sympathetic bursts occurring during the 20-s straining
pdwwphilcaw1mpdfS7auSnrSmmrtiIHpcbaScwSs
R
PtasmbbotpPc
A30ifTSidBpoptP(tg
V
adtb[mCpmm[bumrs
S
V
2861JACC Vol. 55, No. 25, 2010 Fu et al.June 22, 2010:2858–68 Exercise Training in POTS
eriod of the Valsalva maneuver to the maximum fall ofiastolic pressure (33), and cardiovagal baroreflex sensitivityas assessed during early phase II and phase IV (34). Dataere averaged for 1 min at baseline and during the coldressor test. Data were averaged for 1 min of the initialandgrip, the last 30 s of handgrip before fatigue, the
ntermediate period after the initial 1 min and before theast 30 s of handgrip, and for each 1 min of post-exerciseirculatory arrest. During 30° upright tilt, data were aver-ged from the second to the fifth min. During 60° tilt, dataere averaged from the second to the fifth min, seventh to0th min, 17th to 20th min, 26th to 29th min, 36th to 39thin, and 42nd to 45th min. Because some subjects had
re-syncope during tilting and the tilt test was terminated atifferent time points, we used the last stable data carryorward method for imputing missing values (35).tatistical analysis. Data are expressed as median [25th,5th percentiles]. Physical characteristics, baseline variables,nd baroreflex sensitivity between groups were comparedsing the nonparametric Mann-Whitney rank-sum test.ympathetic and cardiovascular responses during the auto-omic function tests were analyzed using the Friedmanepeated measures analysis of variance on ranks, and thetudent-Newman-Keuls method was used post hoc forultiple comparisons within groups. A 2-way repeatedeasures analysis of variance was used to verify whether
esponses to various interventions during autonomic func-ion tests were different between groups, and the interactionn the model was used for comparisons of group responses.n the case of a significant difference between groups, theolm-Sidak method was used post hoc for multiple com-
arisons. Survival analysis with the log-rank test was used toompare time without pre-syncope during 45-min 60° tiltetween groups. Effects of training on hemodynamic vari-bles, blood volume, cardiac size and mass, and 36-itemhort-Form Health Survey scores were analyzed using Wil-oxon signed-rank tests. All statistical analyses were performedith a personal computer-based analysis program (Sigma Stat,PSS, Inc., Chicago, Illinois). A p value �0.05 was consideredtatistically significant.
esults
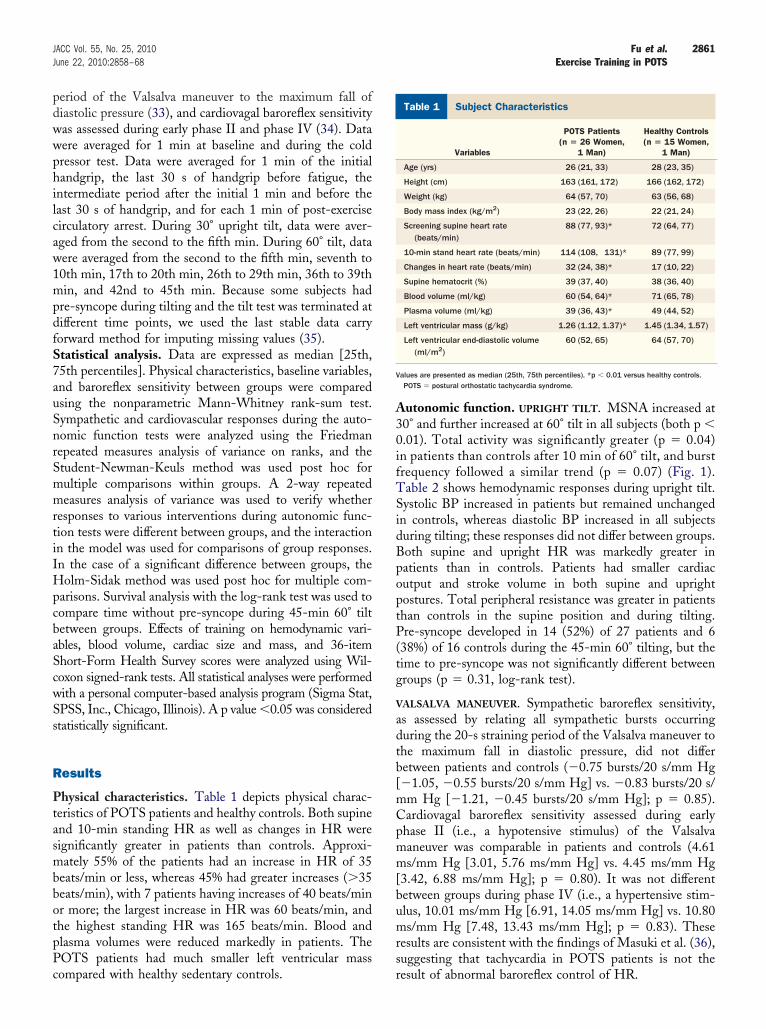
hysical characteristics. Table 1 depicts physical charac-eristics of POTS patients and healthy controls. Both supinend 10-min standing HR as well as changes in HR wereignificantly greater in patients than controls. Approxi-ately 55% of the patients had an increase in HR of 35
eats/min or less, whereas 45% had greater increases (�35eats/min), with 7 patients having increases of 40 beats/minr more; the largest increase in HR was 60 beats/min, andhe highest standing HR was 165 beats/min. Blood andlasma volumes were reduced markedly in patients. TheOTS patients had much smaller left ventricular mass
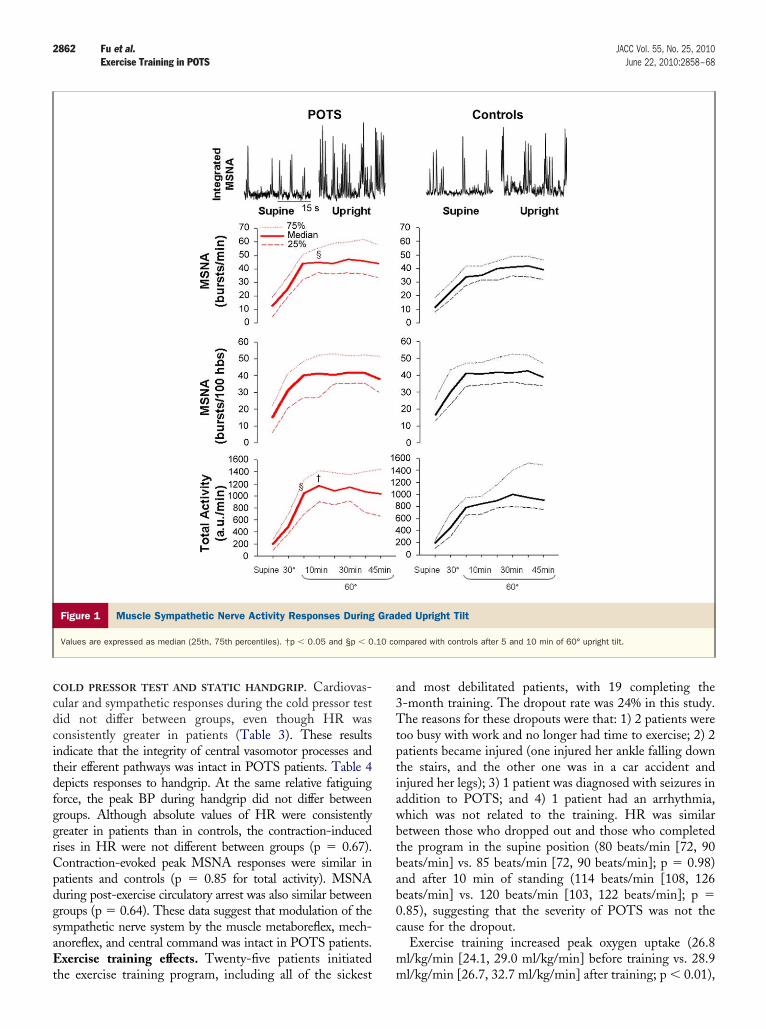
ompared with healthy sedentary controls. rutonomic function. UPRIGHT TILT. MSNA increased at0° and further increased at 60° tilt in all subjects (both p �.01). Total activity was significantly greater (p � 0.04)n patients than controls after 10 min of 60° tilt, and burstrequency followed a similar trend (p � 0.07) (Fig. 1).able 2 shows hemodynamic responses during upright tilt.ystolic BP increased in patients but remained unchanged
n controls, whereas diastolic BP increased in all subjectsuring tilting; these responses did not differ between groups.oth supine and upright HR was markedly greater inatients than in controls. Patients had smaller cardiacutput and stroke volume in both supine and uprightostures. Total peripheral resistance was greater in patientshan controls in the supine position and during tilting.re-syncope developed in 14 (52%) of 27 patients and 6
38%) of 16 controls during the 45-min 60° tilting, but theime to pre-syncope was not significantly different betweenroups (p � 0.31, log-rank test).
ALSALVA MANEUVER. Sympathetic baroreflex sensitivity,s assessed by relating all sympathetic bursts occurringuring the 20-s straining period of the Valsalva maneuver tohe maximum fall in diastolic pressure, did not differetween patients and controls (�0.75 bursts/20 s/mm Hg�1.05, �0.55 bursts/20 s/mm Hg] vs. �0.83 bursts/20 s/m Hg [�1.21, �0.45 bursts/20 s/mm Hg]; p � 0.85).ardiovagal baroreflex sensitivity assessed during earlyhase II (i.e., a hypotensive stimulus) of the Valsalvaaneuver was comparable in patients and controls (4.61s/mm Hg [3.01, 5.76 ms/mm Hg] vs. 4.45 ms/mm Hg
3.42, 6.88 ms/mm Hg]; p � 0.80). It was not differentetween groups during phase IV (i.e., a hypertensive stim-lus, 10.01 ms/mm Hg [6.91, 14.05 ms/mm Hg] vs. 10.80s/mm Hg [7.48, 13.43 ms/mm Hg]; p � 0.83). These
esults are consistent with the findings of Masuki et al. (36),uggesting that tachycardia in POTS patients is not the
ubject CharacteristicsTable 1 Subject Characteristics
Variables
POTS Patients(n � 26 Women,
1 Man)
Healthy Controls(n � 15 Women,
1 Man)
Age (yrs) 26 (21, 33) 28 (23, 35)
Height (cm) 163 (161, 172) 166 (162, 172)
Weight (kg) 64 (57, 70) 63 (56, 68)
Body mass index (kg/m2) 23 (22, 26) 22 (21, 24)
Screening supine heart rate(beats/min)
88 (77, 93)* 72 (64, 77)
10-min stand heart rate (beats/min) 114 (108, 131)* 89 (77, 99)
Changes in heart rate (beats/min) 32 (24, 38)* 17 (10, 22)
Supine hematocrit (%) 39 (37, 40) 38 (36, 40)
Blood volume (ml/kg) 60 (54, 64)* 71 (65, 78)
Plasma volume (ml/kg) 39 (36, 43)* 49 (44, 52)
Left ventricular mass (g/kg) 1.26 (1.12, 1.37)* 1.45 (1.34, 1.57)
Left ventricular end-diastolic volume(ml/m2)
60 (52, 65) 64 (57, 70)
alues are presented as median (25th, 75th percentiles). *p � 0.01 versus healthy controls.POTS � postural orthostatic tachycardia syndrome.
esult of abnormal baroreflex control of HR.
C
cdcitdfggrCpdgsaEt
a3Ttptiawbtbab0c
m
2862 Fu et al. JACC Vol. 55, No. 25, 2010Exercise Training in POTS June 22, 2010:2858–68
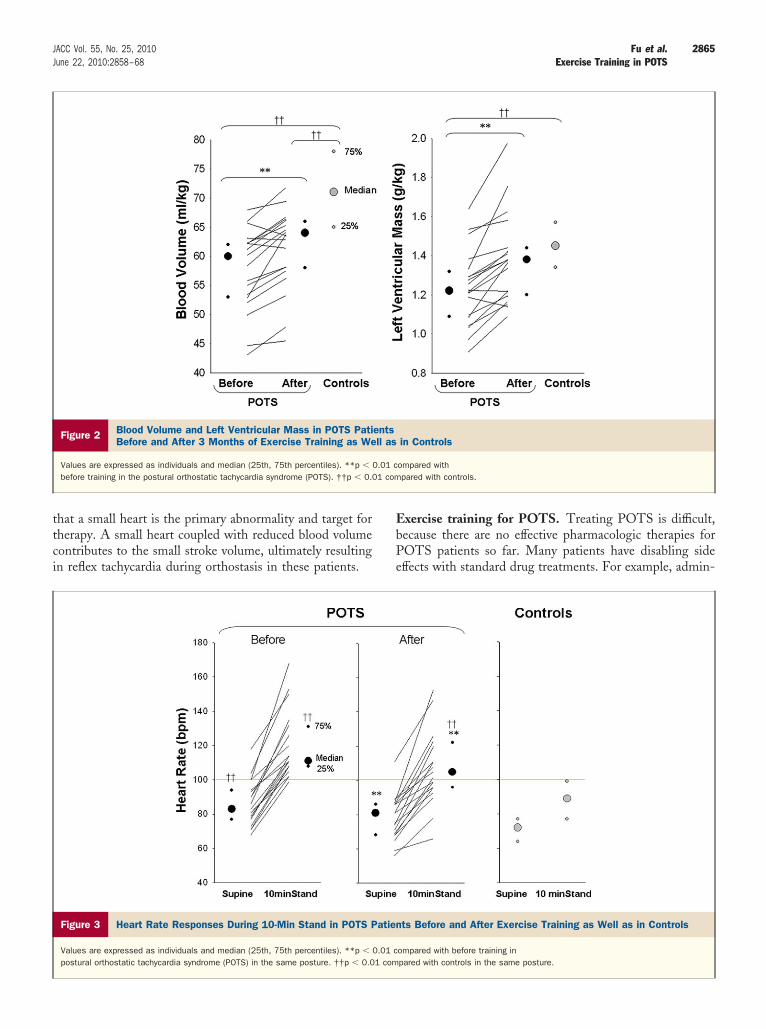
OLD PRESSOR TEST AND STATIC HANDGRIP. Cardiovas-ular and sympathetic responses during the cold pressor testid not differ between groups, even though HR wasonsistently greater in patients (Table 3). These resultsndicate that the integrity of central vasomotor processes andheir efferent pathways was intact in POTS patients. Table 4epicts responses to handgrip. At the same relative fatiguingorce, the peak BP during handgrip did not differ betweenroups. Although absolute values of HR were consistentlyreater in patients than in controls, the contraction-inducedises in HR were not different between groups (p � 0.67).ontraction-evoked peak MSNA responses were similar inatients and controls (p � 0.85 for total activity). MSNAuring post-exercise circulatory arrest was also similar betweenroups (p � 0.64). These data suggest that modulation of theympathetic nerve system by the muscle metaboreflex, mech-noreflex, and central command was intact in POTS patients.xercise training effects. Twenty-five patients initiated
Figure 1 Muscle Sympathetic Nerve Activity Responses During
Values are expressed as median (25th, 75th percentiles). †p � 0.05 and §p � 0
he exercise training program, including all of the sickest m
nd most debilitated patients, with 19 completing the-month training. The dropout rate was 24% in this study.he reasons for these dropouts were that: 1) 2 patients were
oo busy with work and no longer had time to exercise; 2) 2atients became injured (one injured her ankle falling downhe stairs, and the other one was in a car accident andnjured her legs); 3) 1 patient was diagnosed with seizures inddition to POTS; and 4) 1 patient had an arrhythmia,hich was not related to the training. HR was similaretween those who dropped out and those who completedhe program in the supine position (80 beats/min [72, 90eats/min] vs. 85 beats/min [72, 90 beats/min]; p � 0.98)nd after 10 min of standing (114 beats/min [108, 126eats/min] vs. 120 beats/min [103, 122 beats/min]; p �.85), suggesting that the severity of POTS was not theause for the dropout.
Exercise training increased peak oxygen uptake (26.8l/kg/min [24.1, 29.0 ml/kg/min] before training vs. 28.9
ed Upright Tilt
mpared with controls after 5 and 10 min of 60° upright tilt.
Grad
.10 co
l/kg/min [26.7, 32.7 ml/kg/min] after training; p � 0.01),
bmpafH(agQp
tMuiggd6v0bbn0suHss
D
TapwttaePiptwPo(dwdsom
odyn
amic
Res
pons
esD
urin
gG
rade
dU
prig
htTi
ltab
le2
Hem
odyn
amic
Res
pons
esD
urin
gG
rade
dU
prig
htTi
lt
Var
iabl
es
PO
TSP
atie
nts
(n�
27)
Hea
lthy
Con
trol
s(n
�16)
Sup
ine
30
°Ti
lt
60°
Tilt
Sup
ine
30°
Tilt
60°
Tilt
5m
in20
min
40
min
5m
in20
min
40
min
BP
(mm
Hg)
10
5(9
8,1
14
)1
12
*(1
05
,12
0)
11
3*
(10
9,1
24
)1
12
*(1
05
,11
8)
11
4*
(10
6,1
20
)1
09
(10
6,1
15
)1
16
(10
5,1
23
)1
16
(10
9,1
22
)1
14
(10
7,1
16
)1
12
(10
9,1
15
)
BP
(mm
Hg)
66
(60
,69
)7
0†
(63
,74
)7
7†
(67
,81
)7
6†
(68
,83
)7
2†
(67
,81
)6
3(5
9,6
9)
69
†(6
6,7
5)
72
†(7
0,8
2)
73
†(7
0,7
7)
75
†(7
1,7
7)
R(b
eats
/min
)7
7‡
(70
,90
)8
4†
‡(7
5,9
4)
10
4†
‡(9
6,1
11
)1
07
†‡
(10
2,1
22
)1
10
†‡
(10
3,1
25
)6
8(6
1,7
6)
70
†(6
5,8
2)
83
†(7
7,9
3)
87
†(8
2,9
9)
87
†(8
3,1
08
)
O(l/
min
)5
.0‡
(4.3
,5.4
)4
.4†
‡(4
.0,5
.0)
3.6
†‡
(3.3
,4.4
)3
.5†
‡(3
.1,3
.8)
3.2
†‡
(2.9
,3.8
)6
.8(5
.9,7
.3)
5.9
†(5
.0,6
.9)
5.1
†(4
.5,6
.1)
4.4
†(4
.0,5
.2)
4.2
†(3
.9,4
.7)
V(m
l)5
9‡
(50
,66
)4
7†
‡(3
8,5
6)
36
†‡
(28
,42
)3
0†
‡(2
5,3
7)
29
†‡
(23
,35
)8
6(7
4,1
00
)7
6†
(60
,10
2)
60
†(4
5,7
6)
47
†(3
9,6
4)
42
†(3
6,5
6)
R(d
yn·s
·cm
�5)
1,2
84
‡(1
,10
6,1
,50
1)
1,5
66
†‡
(1,3
28
,1,7
35
)1
,86
7†
‡(1
,57
3,2
,31
4)
1,9
59
†‡
(1,7
88
,2,3
36
)2
,13
7†
‡(1
,80
5,2
,49
3)
94
4(8
59
,1,0
57
)1
,06
3†
(95
7,1
,50
4)
1,3
09
†(1
,13
0,1
,62
3)
1,4
75
†(1
,34
6,1
,79
9)
1,6
35
†(1
,36
2,1
,79
0)
esar
eex
pres
sed
asm
edia
n(2
5th
,75
thpe
rcen
tiles
).*p
�0
.05
vers
usan
d†
p�
0.0
1ve
rsus
supi
neba
selin
ew
ithin
the
sam
egr
oup.
‡p
�0
.01
vers
ushe
alth
yco
ntro
ls.
�ca
rdia
cou
tput
;DB
P�
dias
tolic
bloo
dpr
essu
re;H
R�
hear
tra
te;S
BP
�sy
stol
icbl
ood
pres
sure
;SV
�st
roke
volu
me;
TPR
�to
talp
erip
hera
lres
ista
nce;
othe
rab
brev
iatio
nsas
inTa
ble
1.
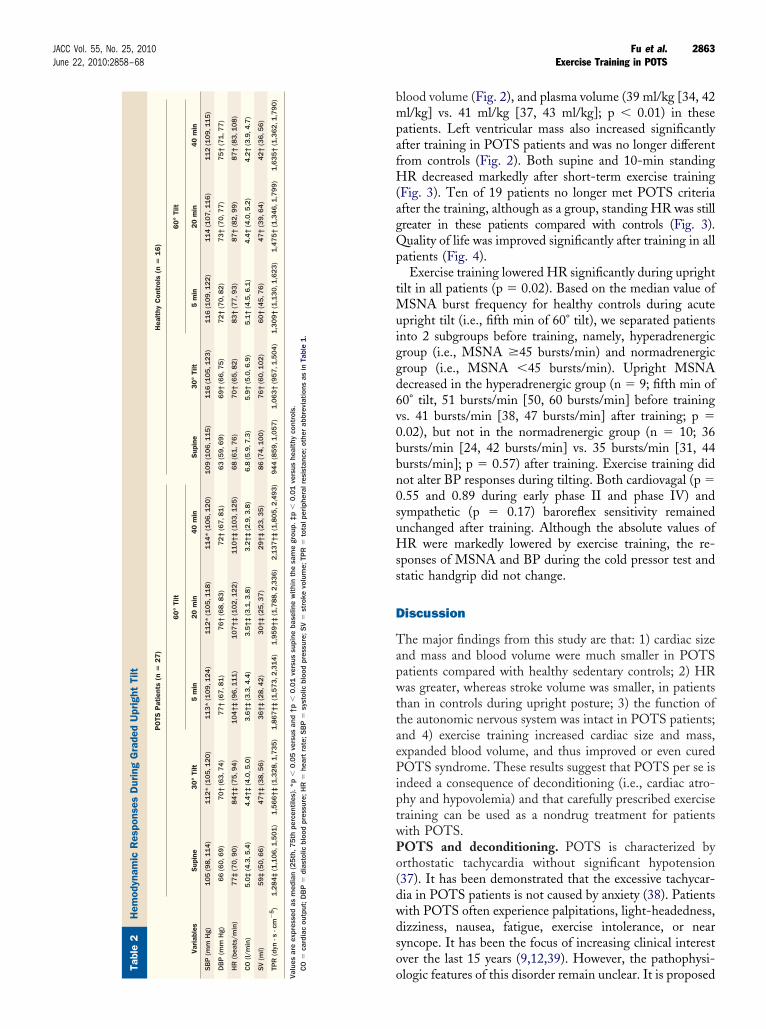
2863JACC Vol. 55, No. 25, 2010 Fu et al.June 22, 2010:2858–68 Exercise Training in POTS
lood volume (Fig. 2), and plasma volume (39 ml/kg [34, 42l/kg] vs. 41 ml/kg [37, 43 ml/kg]; p � 0.01) in these
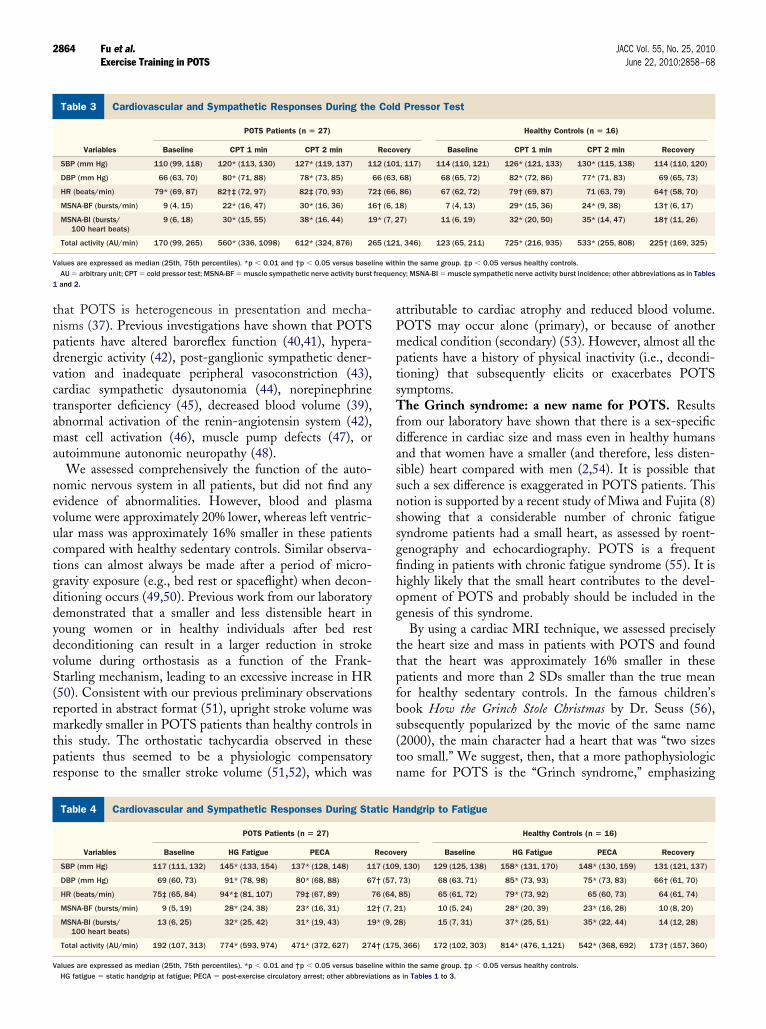
atients. Left ventricular mass also increased significantlyfter training in POTS patients and was no longer differentrom controls (Fig. 2). Both supine and 10-min standing
R decreased markedly after short-term exercise trainingFig. 3). Ten of 19 patients no longer met POTS criteriafter the training, although as a group, standing HR was stillreater in these patients compared with controls (Fig. 3).uality of life was improved significantly after training in all
atients (Fig. 4).Exercise training lowered HR significantly during upright
ilt in all patients (p � 0.02). Based on the median value ofSNA burst frequency for healthy controls during acute
pright tilt (i.e., fifth min of 60° tilt), we separated patientsnto 2 subgroups before training, namely, hyperadrenergicroup (i.e., MSNA �45 bursts/min) and normadrenergicroup (i.e., MSNA �45 bursts/min). Upright MSNAecreased in the hyperadrenergic group (n � 9; fifth min of0° tilt, 51 bursts/min [50, 60 bursts/min] before trainings. 41 bursts/min [38, 47 bursts/min] after training; p �.02), but not in the normadrenergic group (n � 10; 36ursts/min [24, 42 bursts/min] vs. 35 bursts/min [31, 44ursts/min]; p � 0.57) after training. Exercise training didot alter BP responses during tilting. Both cardiovagal (p �.55 and 0.89 during early phase II and phase IV) andympathetic (p � 0.17) baroreflex sensitivity remainednchanged after training. Although the absolute values ofR were markedly lowered by exercise training, the re-
ponses of MSNA and BP during the cold pressor test andtatic handgrip did not change.
iscussion
he major findings from this study are that: 1) cardiac sizend mass and blood volume were much smaller in POTSatients compared with healthy sedentary controls; 2) HRas greater, whereas stroke volume was smaller, in patients
han in controls during upright posture; 3) the function ofhe autonomic nervous system was intact in POTS patients;nd 4) exercise training increased cardiac size and mass,xpanded blood volume, and thus improved or even curedOTS syndrome. These results suggest that POTS per se is
ndeed a consequence of deconditioning (i.e., cardiac atro-hy and hypovolemia) and that carefully prescribed exerciseraining can be used as a nondrug treatment for patientsith POTS.OTS and deconditioning. POTS is characterized byrthostatic tachycardia without significant hypotension37). It has been demonstrated that the excessive tachycar-ia in POTS patients is not caused by anxiety (38). Patientsith POTS often experience palpitations, light-headedness,izziness, nausea, fatigue, exercise intolerance, or nearyncope. It has been the focus of increasing clinical interestver the last 15 years (9,12,39). However, the pathophysi-
ologic features of this disorder remain unclear. It is proposedHe T S D H C S TP
Valu CO
tnpdvctama
nevuctgddydvS(rmtpr
aPmptsTfdassnssgfihog
ttpfbs(tn
C
Vfrequen
1
C
V
2864 Fu et al. JACC Vol. 55, No. 25, 2010Exercise Training in POTS June 22, 2010:2858–68
hat POTS is heterogeneous in presentation and mecha-isms (37). Previous investigations have shown that POTSatients have altered baroreflex function (40,41), hypera-renergic activity (42), post-ganglionic sympathetic dener-ation and inadequate peripheral vasoconstriction (43),ardiac sympathetic dysautonomia (44), norepinephrineransporter deficiency (45), decreased blood volume (39),bnormal activation of the renin-angiotensin system (42),ast cell activation (46), muscle pump defects (47), or
utoimmune autonomic neuropathy (48).We assessed comprehensively the function of the auto-
omic nervous system in all patients, but did not find anyvidence of abnormalities. However, blood and plasmaolume were approximately 20% lower, whereas left ventric-lar mass was approximately 16% smaller in these patientsompared with healthy sedentary controls. Similar observa-ions can almost always be made after a period of micro-ravity exposure (e.g., bed rest or spaceflight) when decon-itioning occurs (49,50). Previous work from our laboratoryemonstrated that a smaller and less distensible heart inoung women or in healthy individuals after bed resteconditioning can result in a larger reduction in strokeolume during orthostasis as a function of the Frank-tarling mechanism, leading to an excessive increase in HR50). Consistent with our previous preliminary observationseported in abstract format (51), upright stroke volume wasarkedly smaller in POTS patients than healthy controls in
his study. The orthostatic tachycardia observed in theseatients thus seemed to be a physiologic compensatoryesponse to the smaller stroke volume (51,52), which was
ardiovascular and Sympathetic Responses During the Cold PressoTable 3 Cardiovascular and Sympathetic Responses During the
Variables
POTS Patients (n � 27)
Baseline CPT 1 min CPT 2 min
SBP (mm Hg) 110 (99, 118) 120* (113, 130) 127* (119, 137) 1
DBP (mm Hg) 66 (63, 70) 80* (71, 88) 78* (73, 85)
HR (beats/min) 79* (69, 87) 82†‡ (72, 97) 82‡ (70, 93) 7
MSNA-BF (bursts/min) 9 (4, 15) 22* (16, 47) 30* (16, 36) 1
MSNA-BI (bursts/100 heart beats)
9 (6, 18) 30* (15, 55) 38* (16, 44) 1
Total activity (AU/min) 170 (99, 265) 560* (336, 1098) 612* (324, 876) 2
alues are expressed as median (25th, 75th percentiles). *p � 0.01 and †p � 0.05 versus baselAU � arbitrary unit; CPT � cold pressor test; MSNA-BF � muscle sympathetic nerve activity burstand 2.
ardiovascular and Sympathetic Responses During Static HandgripTable 4 Cardiovascular and Sympathetic Responses During Sta
Variables
POTS Patients (n � 27)
Baseline HG Fatigue PECA
SBP (mm Hg) 117 (111, 132) 145* (133, 154) 137* (128, 148) 11
DBP (mm Hg) 69 (60, 73) 91* (78, 98) 80* (68, 88) 67
HR (beats/min) 75‡ (65, 84) 94*‡ (81, 107) 79‡ (67, 89) 7
MSNA-BF (bursts/min) 9 (5, 19) 28* (24, 38) 23* (16, 31) 12
MSNA-BI (bursts/100 heart beats)
13 (6, 25) 32* (25, 42) 31* (19, 43) 19
Total activity (AU/min) 192 (107, 313) 774* (593, 974) 471* (372, 627) 274
alues are expressed as median (25th, 75th percentiles). *p � 0.01 and †p � 0.05 versus baseline withHG fatigue � static handgrip at fatigue; PECA � post-exercise circulatory arrest; other abbreviations a
ttributable to cardiac atrophy and reduced blood volume.OTS may occur alone (primary), or because of anotheredical condition (secondary) (53). However, almost all the
atients have a history of physical inactivity (i.e., decondi-ioning) that subsequently elicits or exacerbates POTSymptoms.he Grinch syndrome: a new name for POTS. Results
rom our laboratory have shown that there is a sex-specificifference in cardiac size and mass even in healthy humansnd that women have a smaller (and therefore, less disten-ible) heart compared with men (2,54). It is possible thatuch a sex difference is exaggerated in POTS patients. Thisotion is supported by a recent study of Miwa and Fujita (8)howing that a considerable number of chronic fatigueyndrome patients had a small heart, as assessed by roent-enography and echocardiography. POTS is a frequentnding in patients with chronic fatigue syndrome (55). It isighly likely that the small heart contributes to the devel-pment of POTS and probably should be included in theenesis of this syndrome.
By using a cardiac MRI technique, we assessed preciselyhe heart size and mass in patients with POTS and foundhat the heart was approximately 16% smaller in theseatients and more than 2 SDs smaller than the true meanor healthy sedentary controls. In the famous children’sook How the Grinch Stole Christmas by Dr. Seuss (56),ubsequently popularized by the movie of the same name2000), the main character had a heart that was “two sizesoo small.” We suggest, then, that a more pathophysiologicame for POTS is the “Grinch syndrome,” emphasizing
tPressor Test
Healthy Controls (n � 16)
ery Baseline CPT 1 min CPT 2 min Recovery
, 117) 114 (110, 121) 126* (121, 133) 130* (115, 138) 114 (110, 120)
68) 68 (65, 72) 82* (72, 86) 77* (71, 83) 69 (65, 73)
86) 67 (62, 72) 79† (69, 87) 71 (63, 79) 64† (58, 70)
8) 7 (4, 13) 29* (15, 36) 24* (9, 38) 13† (6, 17)
7) 11 (6, 19) 32* (20, 50) 35* (14, 47) 18† (11, 26)
, 346) 123 (65, 211) 725* (216, 935) 533* (255, 808) 225† (169, 325)
in the same group. ‡p � 0.05 versus healthy controls.cy; MSNA-BI � muscle sympathetic nerve activity burst incidence; other abbreviations as in Tables
atigueandgrip to Fatigue
Healthy Controls (n � 16)
ery Baseline HG Fatigue PECA Recovery
, 130) 129 (125, 138) 158* (131, 170) 148* (130, 159) 131 (121, 137)
73) 68 (63, 71) 85* (73, 93) 75* (73, 83) 66† (61, 70)
85) 65 (61, 72) 79* (73, 92) 65 (60, 73) 64 (61, 74)
1) 10 (5, 24) 28* (20, 39) 23* (16, 28) 10 (8, 20)
8) 15 (7, 31) 37* (25, 51) 35* (22, 44) 14 (12, 28)
, 366) 172 (102, 303) 814* (476, 1,121) 542* (368, 692) 173† (157, 360)
r TesCold
Recov
12 (101
66 (63,
2‡ (66,
6† (6, 1
9* (7, 2
65 (121
ine with
to Ftic H
Recov
7 (109
† (57,
6 (64,
† (7, 2
* (9, 2
† (175
in the same group. ‡p � 0.05 versus healthy controls.s in Tables 1 to 3.
ttci
EbPe
2865JACC Vol. 55, No. 25, 2010 Fu et al.June 22, 2010:2858–68 Exercise Training in POTS
hat a small heart is the primary abnormality and target forherapy. A small heart coupled with reduced blood volumeontributes to the small stroke volume, ultimately resultingn reflex tachycardia during orthostasis in these patients.
Figure 2 Blood Volume and Left Ventricular Mass in POTS PatiBefore and After 3 Months of Exercise Training as We
Values are expressed as individuals and median (25th, 75th percentiles). **p �
before training in the postural orthostatic tachycardia syndrome (POTS). ††p � 0.0
Figure 3 Heart Rate Responses During 10-Min Stand in POTS P
Values are expressed as individuals and median (25th, 75th percentiles). **p �
postural orthostatic tachycardia syndrome (POTS) in the same posture. ††p � 0.0
xercise training for POTS. Treating POTS is difficult,ecause there are no effective pharmacologic therapies forOTS patients so far. Many patients have disabling sideffects with standard drug treatments. For example, admin-
in Controls
ompared withpared with controls.
ts Before and After Exercise Training as Well as in Controls
ompared with before training inpared with controls in the same posture.
entsll as
0.01 c1 com
atien
0.01 c1 com
iecfvwdmAcedp
awsisa(trogipvslBt
PpqStwtnpSioaelogeotmaf0sgtpetd
2866 Fu et al. JACC Vol. 55, No. 25, 2010Exercise Training in POTS June 22, 2010:2858–68
stration of beta-blockers can reduce tachycardia; but, if thexcessive reduction in stroke volume during orthostasisannot be corrected, orthostatic hypotension and severeatigue often occurs in these patients. Administration ofolume expanders increases body fluids and vascular volume,hich can result in a smaller reduction in stroke volumeuring orthostasis in POTS patients. However, leg edemaay appear and hypokalemia may develop in some patients.dministration of alpha1-adrenergic agonists also can de-
rease heart rate through the baroreflex mechanism. How-ver, hypertension or other intolerable side effects mayevelop in some patients, which is quite common in theseatients with prominent hypervigilance (37).To avoid the side effects with drug therapies, we appliednondrug treatment, namely, exercise training, to patientsith POTS. It is important to emphasize that even the
ickest patients participated in this program and that train-ng was facilitated by avoiding upright exercise in the earlytage. Endurance training has been shown to expand bloodnd plasma volumes (16), to increase cardiac size and mass49) and to prevent cardiac atrophy, and increase orthostaticolerance in healthy women after prolonged period of bedest (49) as well as in patients with unexplained syncope orrthostatic hypotension. We found that 3 months of pro-ressive exercise training in POTS patients increased max-mal oxygen uptake by 11%, indicating an increase inhysical fitness. Left ventricular mass and end-diastolicolume increased by 12% and 8% after training, resulting inignificant cardiac remodeling. The heart became mucharger and probably more distensible after exercise training.lood and plasma volumes also increased markedly after
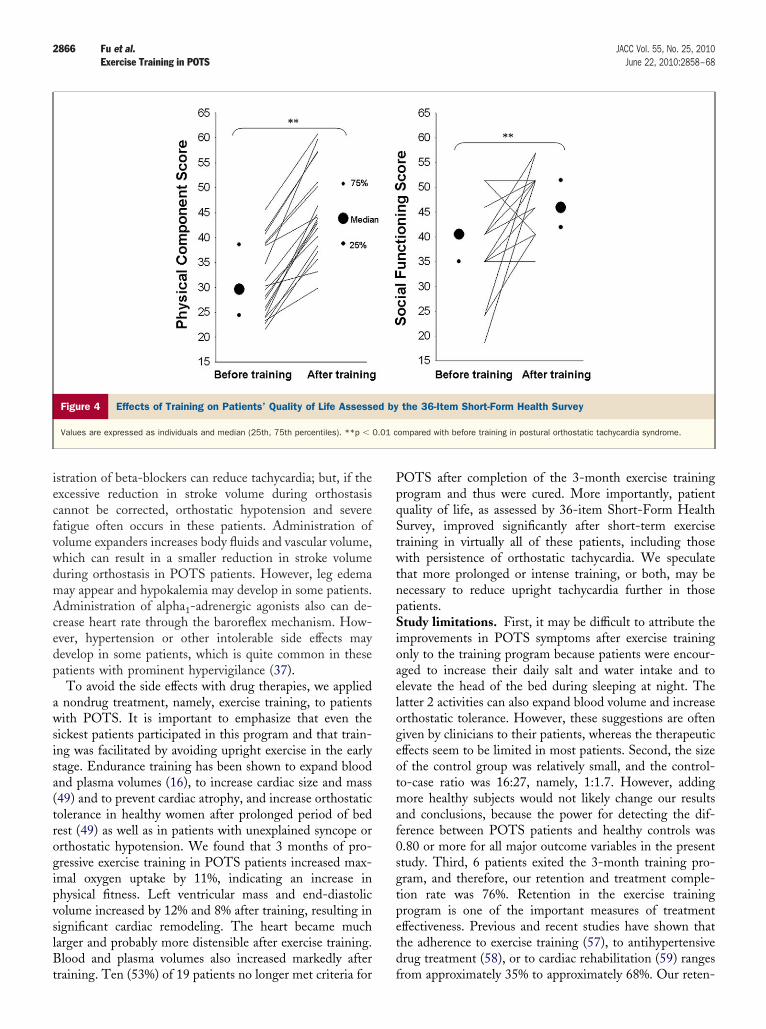
Figure 4 Effects of Training on Patients’ Quality of Life Assess
Values are expressed as individuals and median (25th, 75th percentiles). **p �
raining. Ten (53%) of 19 patients no longer met criteria for f
OTS after completion of the 3-month exercise trainingrogram and thus were cured. More importantly, patientuality of life, as assessed by 36-item Short-Form Healthurvey, improved significantly after short-term exerciseraining in virtually all of these patients, including thoseith persistence of orthostatic tachycardia. We speculate
hat more prolonged or intense training, or both, may beecessary to reduce upright tachycardia further in thoseatients.tudy limitations. First, it may be difficult to attribute the
mprovements in POTS symptoms after exercise trainingnly to the training program because patients were encour-ged to increase their daily salt and water intake and tolevate the head of the bed during sleeping at night. Theatter 2 activities can also expand blood volume and increaserthostatic tolerance. However, these suggestions are ofteniven by clinicians to their patients, whereas the therapeuticffects seem to be limited in most patients. Second, the sizef the control group was relatively small, and the control-o-case ratio was 16:27, namely, 1:1.7. However, addingore healthy subjects would not likely change our results
nd conclusions, because the power for detecting the dif-erence between POTS patients and healthy controls was.80 or more for all major outcome variables in the presenttudy. Third, 6 patients exited the 3-month training pro-ram, and therefore, our retention and treatment comple-ion rate was 76%. Retention in the exercise trainingrogram is one of the important measures of treatmentffectiveness. Previous and recent studies have shown thathe adherence to exercise training (57), to antihypertensiverug treatment (58), or to cardiac rehabilitation (59) ranges
the 36-Item Short-Form Health Survey
ompared with before training in postural orthostatic tachycardia syndrome.
ed by
0.01 c
rom approximately 35% to approximately 68%. Our reten-

tsrd
C
PrtotcatpaiPte
ATaOPkmlBB
RIPD
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
2867JACC Vol. 55, No. 25, 2010 Fu et al.June 22, 2010:2858–68 Exercise Training in POTS
ion rate is actually higher than the findings of these studies,uggesting that compliance with this approach is within theange of other drug or nondrug interventions in commoniseases.
onclusions
atients with POTS had a smaller heart coupled witheduced blood volume compared with healthy controls. Weherefore propose the name the Grinch syndrome to focusn this pathophysiologic state. The marked orthostaticachycardia in these patients seemed to be a physiologicompensatory response to a smaller stroke volume that wasttributable to cardiac atrophy and hypovolemia. The func-ion of the autonomic nervous system was intact in POTSatients. Short-term exercise training increased cardiac sizend mass and expanded blood and plasma volume, and thusmproved or even cured POTS. These results suggest thatOTS per se is indeed a consequence of deconditioning and
hat carefully prescribed exercise training can be used as anffective nondrug therapy for POTS patients.
cknowledgmentshe time and effort put forth by the subjects is greatly
ppreciated. The authors thank Robin P. Shook, Kazunobukazaki, Nainesh Gandhi, Beverley A. Huet, M. Deanalmer, Daniel L. Creson, Colin L. Conner, Diane Beden-op, Peggy Fowler, Adam Banks, Murugappan Ra-anathan, Cyrus Oufi, and Dak Quarles for their valuable
aboratory assistance; and Dr. Gordon H. Williams,righam & Women’s Hospital, Harvard Medical School,oston, Massachusetts, for invaluable advice and support.
eprint requests and correspondence: Dr. Benjamin D. Levine,nstitute for Exercise and Environmental Medicine, Texas Healthresbyterian Hospital Dallas, 7232 Greenville Avenue, Suite 435,allas, Texas 75231. E-mail: [email protected].
EFERENCES
1. Fu Q, Witkowski S, Okazaki K, Levine BD. Effects of gender andhypovolemia on sympathetic neural responses to orthostatic stress.Am J Physiol Regul Integr Comp Physiol 2005;289:R109–16.
2. Fu Q, Arbab-Zadeh A, Perhonen MA, Zhang R, Zuckerman JH,Levine BD. Hemodynamics of orthostatic intolerance: implicationsfor gender differences. Am J Physiol Heart Circ Physiol 2004;286:H449 –57.
3. Robertson D. The epidemic of orthostatic tachycardia and orthostaticintolerance. Am J Med Sci 1999;317:75–7.
4. Fritsch-Yelle JM, Whitson PA, Bondar RL, Brown TE. Subnormalnorepinephrine release relates to presyncope in astronauts after space-flight. J Appl Physiol 1996;81:2134–41.
5. Waters WW, Ziegler MG, Meck JV. Postspaceflight orthostatichypotension occurs mostly in women and is predicted by low vascularresistance. J Appl Physiol 2002;92:586–94.
6. Levine BD, Pawelczyk JA, Ertl AC, et al. Human muscle sympatheticneural and haemodynamic responses to tilt following spaceflight.J Physiol 2002;538:331–40.
7. Kamiya A, Iwase S, Kitazawa H, Mano T, Vinogradova OL, Kharch-enko IB. Baroreflex control of muscle sympathetic nerve activity after
120 days of 6 degrees head-down bed rest. Am J Physiol Regul IntegrComp Physiol 2000;278:R445–52.8. Miwa K, Fujita M. Small heart syndrome in patients with chronicfatigue syndrome. Clin Cardiol 2008;31:328–33.
9. Raj SR, Biaggioni I, Yamhure PC, et al. Renin-aldosterone paradoxand perturbed blood volume regulation underlying postural tachycardiasyndrome. Circulation 2005;111:1574–82.
0. Stewart JM, Glover JL, Medow MS. Increased plasma angiotensin IIin postural tachycardia syndrome (POTS) is related to reduced bloodflow and blood volume. Clin Sci (Lond) 2006;110:255–63.
1. Ali YS, Daamen N, Jacob G, et al. Orthostatic intolerance: a disorderof young women. Obstet Gynecol Surv 2000;55:251–9.
2. Low PA, Opfer-Gehrking TL, Textor SC, et al. Postural tachycardiasyndrome (POTS). Neurology 1995;45:S19–25.
3. Masuki S, Eisenach JH, Schrage WG, et al. Reduced stroke volumeduring exercise in postural tachycardia syndrome. J Appl Physiol2007;103:1128–35.
4. Brilla LR, Stephens AB, Knutzen KM, Caine D. Effect of strengthtraining on orthostatic hypotension in older adults. J CardiopulmRehabil 1998;18:295–300.
5. Mtinangi BL, Hainsworth R. Increased orthostatic tolerance followingmoderate exercise training in patients with unexplained syncope. Heart1998;80:596–600.
6. Saltin B, Blomqvist G, Mitchell JH, Johnson RL Jr., Wildenthal K,Chapman CB. Response to exercise after bed rest and after training.Circulation 1968;38:VII1–78.
7. Convertino VA. Endurance exercise training: conditions of enhancedhemodynamic responses and tolerance to LBNP. Med Sci SportsExerc 1993;25:705–12.
8. Levine BD. Regulation of central blood volume and cardiac filling inendurance athletes: the Frank-Starling mechanism as a determinant oforthostatic tolerance. Med Sci Sports Exerc 1993;25:727–32.
9. Levine BD, Lane LD, Buckey JC, Friedman DB, Blomqvist CG. Leftventricular pressure-volume and Frank-Starling relations in enduranceathletes. Implications for orthostatic tolerance and exercise perfor-mance. Circulation 1991;84:1016–23.
0. McDonnell NB, Gorman BL, Mandel KW, et al. Echocardiographicfindings in classical and hypermobile Ehlers-Danlos syndromes. Am JMed Genet A 2006;140:129–36.
1. Carter JB, Banister EW, Blaber AP. Effect of endurance exercise onautonomic control of heart rate. Sports Med 2003;33:33–46.
2. Fu Q, VanGundy TB, Shibata S, Creson DL, Levine BD. Exercisetraining but not beta-adrenergic blockade treatment improves therenin-aldosterone response during prolonged orthostasis in the Pos-tural Orthostatic Tachycardia Syndrome. Clin Auton Res 2008;18:267.
3. Vallbo AB, Hagbarth KE, Torebjork HE, Wallin BG. Somatosen-sory, proprioceptive, and sympathetic activity in human peripheralnerves. Physiol Rev 1979;59:919–57.
4. Triebwasser JH, Johnson RL, Burpo RP, Campbell JC, Reardon WC,Blomqvist CG. Noninvasive determination of cardiac output by amodified acetylene rebreathing procedure utilizing mass spectrometermeasurements. Aviat Space Environ Med 1977;48:203–9.
5. Fu Q, Shook RP, Okazaki K, et al. Vasomotor sympathetic neuralcontrol is maintained during sustained upright posture in humans.J Physiol 2006;577:679–87.
6. Burge CM, Skinner SL. Determination of hemoglobin mass andblood volume with CO: evaluation and application of a method. J ApplPhysiol 1995;79:623–31.
7. Gore CJ, Rodriguez FA, Truijens MJ, Townsend NE, Stray-Gundersen J, Levine BD. Increased serum erythropoietin but not redcell production after 4 wk of intermittent hypobaric hypoxia (4,000–5,500 m). J Appl Physiol 2006;101:1386–93.
8. Peshock RM, Willett DL, Sayad DE, et al. Quantitative MR imagingof the heart. Magn Reson Imaging Clin N Am 1996;4:287–305.
9. Banister EW, Morton RH, Fitz-Clarke J. Dose/response effects ofexercise modeled from training: physical and biochemical measures.Ann Physiol Anthropol 1992;11:345–56.
0. Ware JEJ, Snow KK, Kosinski M, Gandek B. SF-36 Health Survey:Manual and Interpretation Guide. Boston, MA: Health Institute,New England Medical Center, 1993.
1. Cui J, Wilson TE, Shibasaki M, Hodges NA, Crandall CG. Barore-flex modulation of muscle sympathetic nerve activity during posthand-grip muscle ischemia in humans. J Appl Physiol 2001;91:1679–86.
2. Halliwill JR. Segregated signal averaging of sympathetic baroreflex
responses in humans. J Appl Physiol 2000;88:767–73.
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
K
2868 Fu et al. JACC Vol. 55, No. 25, 2010Exercise Training in POTS June 22, 2010:2858–68
3. Fu Q, Zhang R, Witkowski S, et al. Persistent sympathetic activationduring chronic antihypertensive therapy: a potential mechanism forlong term morbidity? Hypertension 2005;45:513–21.
4. Fu Q, Okazaki K, Shibata S, et al. Menstrual cycle effects onsympathetic neural responses to upright tilt. J Physiol 2009;587:2019 –31.
5. Ali MW, Talukder E. Analysis of longitudinal binary data withmissing data due to dropouts. J Biopharm Stat 2005;15:993–1007.
6. Masuki S, Eisenach JH, Schrage WG, et al. Arterial baroreflex controlof heart rate during exercise in postural tachycardia syndrome. J ApplPhysiol 2007;103:1136–42.
7. Low PA, Sandroni P, Joyner M, Shen WK. Postural tachycardiasyndrome (POTS). J Cardiovasc Electrophysiol 2009;20:352–8.
8. Masuki S, Eisenach JH, Johnson CP, et al. Excessive heart rateresponse to orthostatic stress in postural tachycardia syndrome is notcaused by anxiety. J Appl Physiol 2007;102:896–903.
9. Raj SR, Robertson D. Blood volume perturbations in the posturaltachycardia syndrome. Am J Med Sci 2007;334:57–60.
0. Stewart JM. Autonomic nervous system dysfunction in adolescentswith postural orthostatic tachycardia syndrome and chronic fatiguesyndrome is characterized by attenuated vagal baroreflex and potenti-ated sympathetic vasomotion. Pediatr Res 2000;48:218–26.
1. Bonyhay I, Freeman R. Sympathetic nerve activity in response tohypotensive stress in the postural tachycardia syndrome. Circulation2004;110:3193–8.
2. Jacob G, Robertson D, Mosqueda-Garcia R, Ertl AC, Robertson RM,Biaggioni I. Hypovolemia in syncope and orthostatic intolerance roleof the renin-angiotensin system. Am J Med 1997;103:128–33.
3. Stewart JM, Weldon A. Vascular perturbations in the chronic ortho-static intolerance of the postural orthostatic tachycardia syndrome.J Appl Physiol 2000;89:1505–12.
4. Goldstein DS, Holmes C, Frank SM, et al. Cardiac sympatheticdysautonomia in chronic orthostatic intolerance syndromes. Circula-tion 2002;106:2358–65.
5. Shannon JR, Flattem NL, Jordan J, et al. Orthostatic intolerance andtachycardia associated with norepinephrine-transporter deficiency.N Engl J Med 2000;342:541–9.
6. Shibao C, Arzubiaga C, Roberts LJ 2nd, et al. Hyperadrenergicpostural tachycardia syndrome in mast cell activation disorders. Hy-
pertension 2005;45:385–90. y7. Stewart JM, Medow MS, Montgomery LD, McLeod K. Decreasedskeletal muscle pump activity in patients with postural tachycardiasyndrome and low peripheral blood flow. Am J Physiol Heart CircPhysiol 2004;286:H1216–22.
8. Vernino S, Low PA, Fealey RD, Stewart JD, Farrugia G, Lennon VA.Autoantibodies to ganglionic acetylcholine receptors in autoimmuneautonomic neuropathies. N Engl J Med 2000;343:847–55.
9. Dorfman TA, Levine BD, Tillery T, et al. Cardiac atrophy in womenfollowing bed rest. J Appl Physiol 2007;103:8–16.
0. Levine BD, Zuckerman JH, Pawelczyk JA. Cardiac atrophy afterbed-rest deconditioning: a nonneural mechanism for orthostatic intol-erance. Circulation 1997;96:517–25.
1. Fu Q, Shook RP, Shibata S, et al. Vasomotor sympathetic andhemodynamic responses during upright tilt in the Postural OrthostaticTachycardia Syndrome. FASEB J 2007;21:750.20.
2. Joyner MJ, Masuki S. POTS versus deconditioning: the same ordifferent? Clin Auton Res 2008;18:300–7.
3. Grubb BP, Karabin B. Cardiology patient pages. Postural tachycardiasyndrome: perspectives for patients. Circulation 2008;118:e61–2.
4. Levine BD. The Grinch syndrome: a new name for orthostatichypotension and syncope. In: 2006 ACSM Annual Meeting NamedLectures [DVD]. Monterey, CA: Health Learning, American Collegeof Sports Medicine, 2006.
5. Hoad A, Spickett G, Elliott J, Newton J. Postural orthostatic tachy-cardia syndrome is an under-recognized condition in chronic fatiguesyndrome. QJM 2008;101:961–5.
6. Seuss Enterprises LP. How the Grinch Stole Christmas. New York,NY: Random House, Inc., 1957.
7. Sloan RP, Shapiro PA, DeMeersman RE, et al. The effect of aerobictraining and cardiac autonomic regulation in young adults. Am JPublic Health 2009;99:921–8.
8. Flack JM, Novikov SV, Ferrario CM. Benefits of adherence toanti-hypertensive drug therapy. Eur Heart J 1996;17 Suppl A:16 –20.
9. Sharp J, Freeman C. Patterns and predictors of uptake and adherenceto cardiac rehabilitation. J Cardiopulm Rehabil Prev 2009;29:241–7.
ey Words: arterial pressure y autonomic control y endurance training
orthostatic tolerance y vasomotor sympathetic activity.