Embed Size (px)
Citation preview
Capturing Relevant Capturing Relevant Patient Toxicity in CAT Patient Toxicity in CAT
(Cancer Associated (Cancer Associated Thrombosis)Thrombosis)
Anthony Maraveyas Anthony Maraveyas FRCP, PhDFRCP, PhD HULL YORK MEDICAL SCHOOLHULL YORK MEDICAL SCHOOL
33RDRD TRAD-ALLIANCE TRAD-ALLIANCE CONFERENCECONFERENCE
YORK 2013YORK 2013
DisclosuresDisclosures
ConsultancyConsultancy Pfizer (Dalteparin)Pfizer (Dalteparin) Leo (Tinzaparin)Leo (Tinzaparin) Sanofi (Semuloparin)Sanofi (Semuloparin)
GrantGrant Pfizer/PharmaciaPfizer/Pharmacia
CAT and ToxicityCAT and Toxicity Capturing VTE (DVT and AT) as a Capturing VTE (DVT and AT) as a
toxicity of Cancer Treatmenttoxicity of Cancer Treatment Recognising the clinical impactRecognising the clinical impact Attributing CausalityAttributing Causality
Relevance of Toxicity of anti-coagulants Relevance of Toxicity of anti-coagulants in the Palliative cancer patientin the Palliative cancer patient Scoring system of main toxicity (Bleeding)Scoring system of main toxicity (Bleeding) Scoring and impact of ‘trivial’ bleedingScoring and impact of ‘trivial’ bleeding
VTE = venous thromboembolism.
The ChallengeThe Challenge
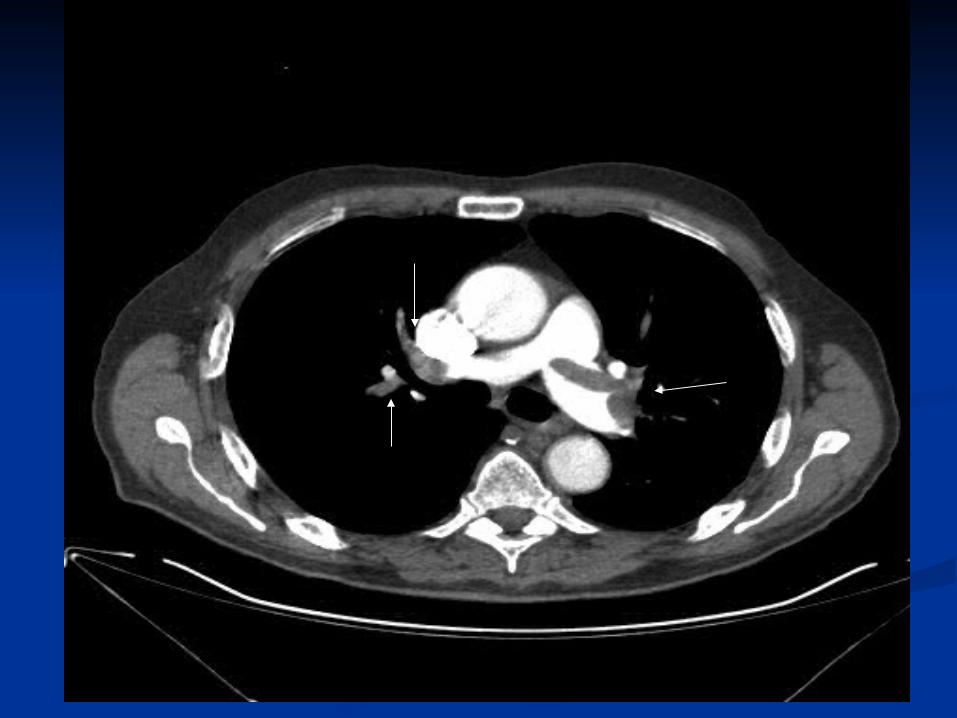
50% of DVT at diagnosis harbor PE50% of DVT at diagnosis harbor PE Up to 60% are Up to 60% are asymptomaticasymptomatic
DVT is not diagnosed more than 60% of DVT is not diagnosed more than 60% of patients who have a DVT and malignancypatients who have a DVT and malignancy
‘‘Practically Undiagnosable condition’Practically Undiagnosable condition’
Cronin et al . AJR 189(1):162-70 2007Ogren et al. Thr. Haemost 95: 541-5 2006
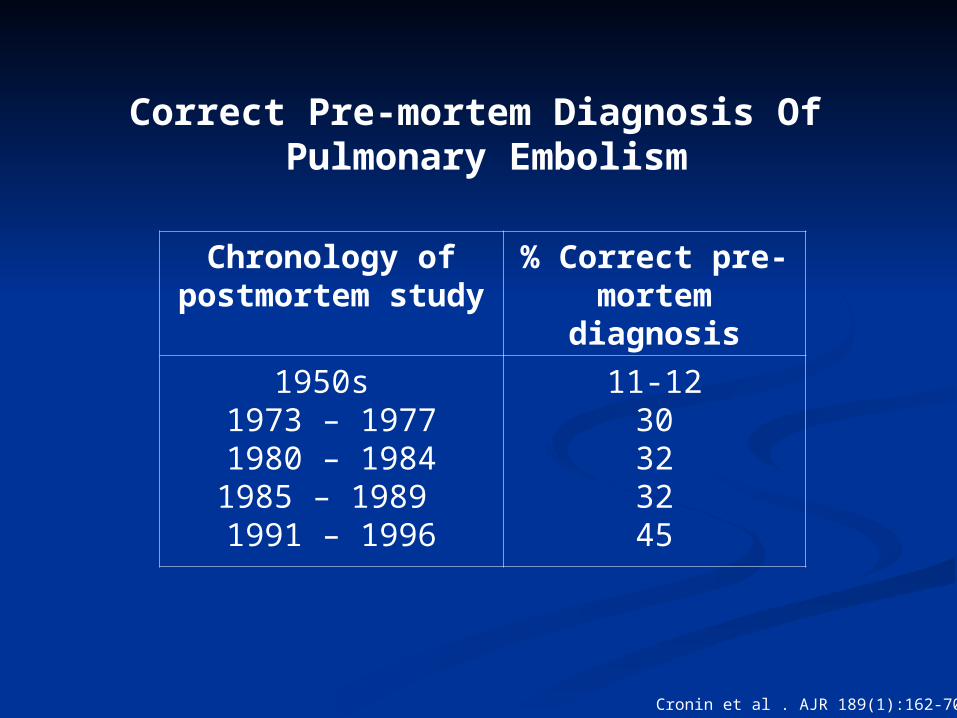
Correct Pre-mortem Diagnosis Of Pulmonary Embolism
Chronology of postmortem study
% Correct pre-mortem diagnosis
1950s 1973 – 19771980 – 19841985 – 1989 1991 – 1996
11-1230323245
Cronin et al . AJR 189(1):162-70 2007
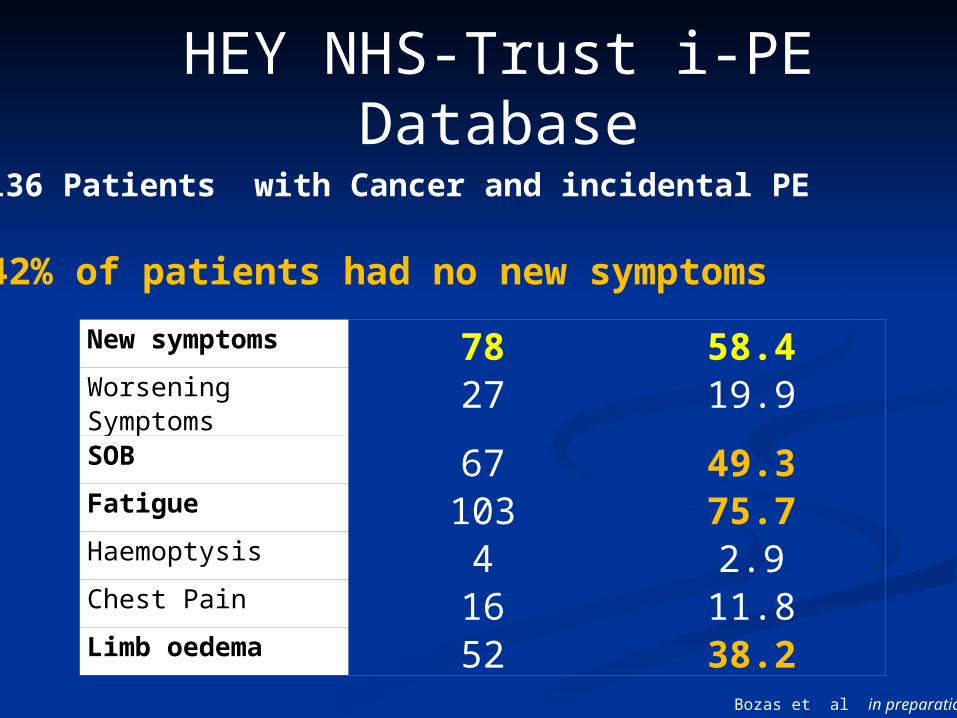
New symptoms 78 58.4Worsening Symptoms
27 19.9
SOB 67 49.3Fatigue 103 75.7Haemoptysis 4 2.9Chest Pain 16 11.8Limb oedema 52 38.2
HEY NHS-Trust i-PE Database
136 Patients with Cancer and incidental PE
42% of patients had no new symptoms
Bozas et al in preparation
The ChallengeThe Challenge
50% of DVT at diagnosis harbor PE50% of DVT at diagnosis harbor PE Up to 60% are Up to 60% are asymptomaticasymptomatic
DVT is not diagnosed more than 60% of DVT is not diagnosed more than 60% of patients who have a DVT and malignancypatients who have a DVT and malignancy
‘‘Practically Undiagnosable condition’Practically Undiagnosable condition’ See no Evil Report No EvilSee no Evil Report No Evil
Cronin et al . AJR 189(1):162-70 2007Ogren et al. Thr. Haemost 95: 541-5 2006
‘‘Clinical Method’ Clinical Method’ LimitationsLimitations
Limitations – Masking VTELimitations – Masking VTE Inadequate Recognition of clinical impactInadequate Recognition of clinical impact Inadequate recognition of ‘additional-Inadequate recognition of ‘additional-
impact’ from intervention -Cancer impact’ from intervention -Cancer Treatments- Treatments-
Risk obscured by discrepant demographics Risk obscured by discrepant demographics of Trial sample vs. Real world populationsof Trial sample vs. Real world populations
Reporting methodologyReporting methodology Attributing causalityAttributing causality
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Inadequate Recognition of clinical Inadequate Recognition of clinical impactimpact
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
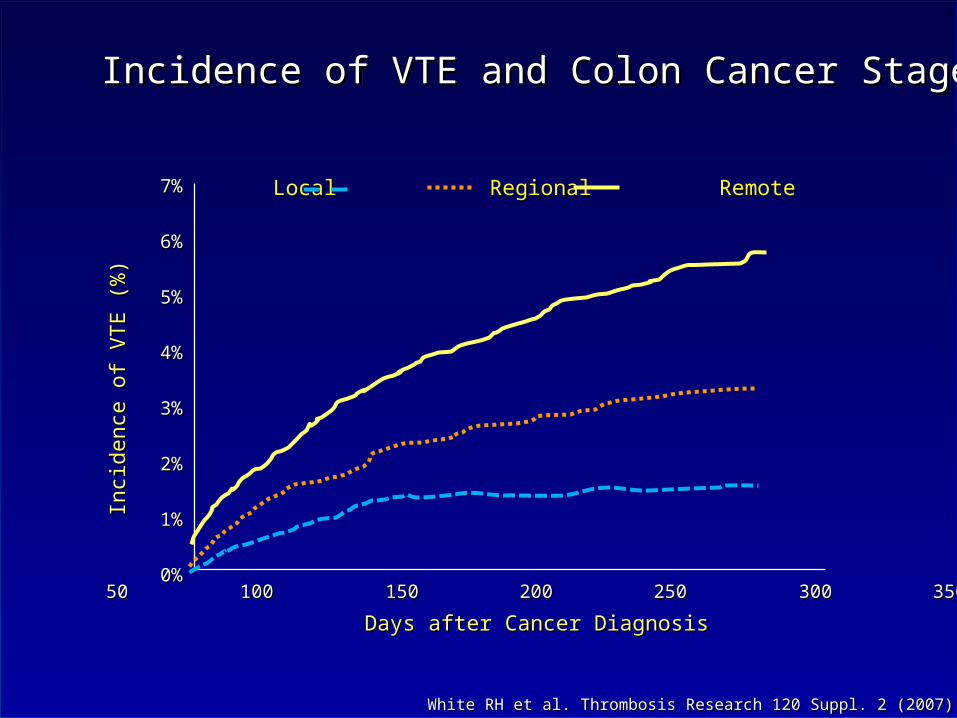
Incidence of VTE and Colon Cancer StageIncidence of VTE and Colon Cancer StageIncidence of VTE and Colon Cancer StageIncidence of VTE and Colon Cancer Stage
White RH et al. Thrombosis Research 120 Suppl. 2 (2007) S29-40White RH et al. Thrombosis Research 120 Suppl. 2 (2007) S29-40
Days after Cancer DiagnosisDays after Cancer Diagnosis
Inci
denc
e of
VT
E (
%)
Inci
denc
e of
VT
E (
%)
0 50 100 150 200 250 300 350 4000 50 100 150 200 250 300 350 400
7%7%
6%6%
5%5%
4%4%
3%3%
2%2%
1%1%
0%0%
Local Regional RemoteLocal Regional Remote
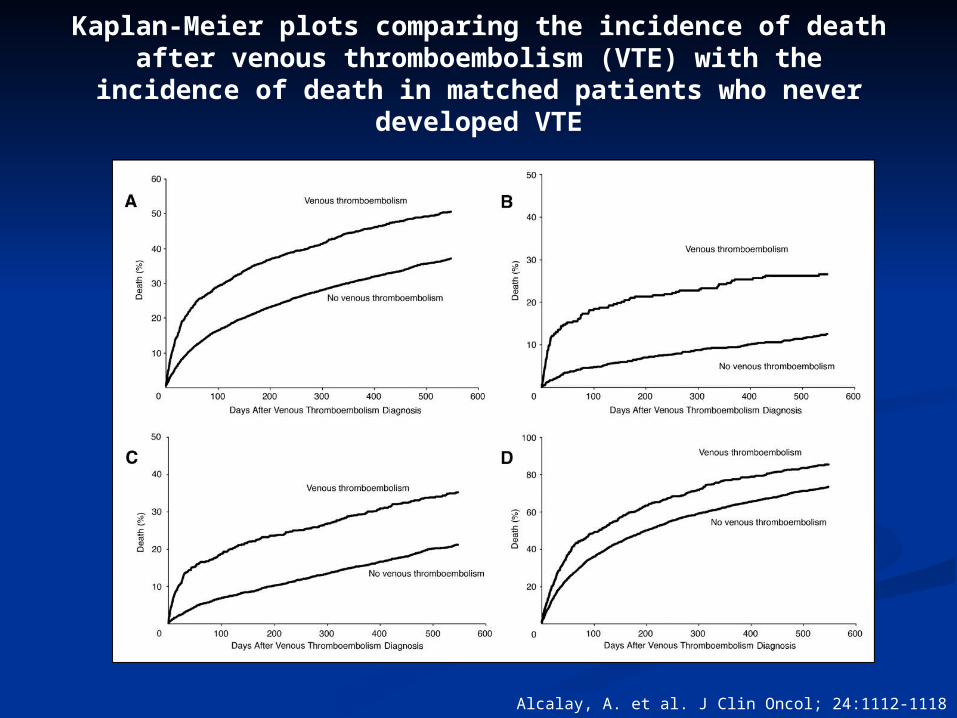
Kaplan-Meier plots comparing the incidence of death after venous thromboembolism (VTE) with the incidence of death in matched
patients who never developed VTE
Alcalay, A. et al. J Clin Oncol; 24:1112-1118 2006

Inadequate Recognition of clinical Inadequate Recognition of clinical impactimpact
Inadequate recognition of Inadequate recognition of ‘additional-impact’ from Cancer ‘additional-impact’ from Cancer Treatments Treatments Erythropoietin data ?Erythropoietin data ?
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
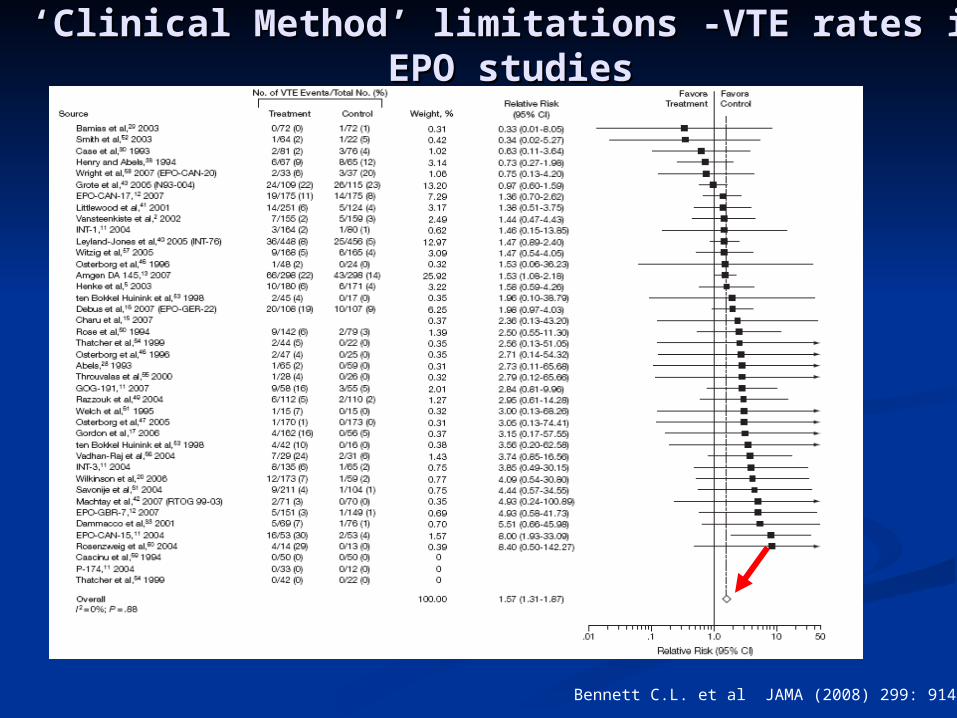
‘‘Clinical Method’ limitations -Clinical Method’ limitations -VTE rates in EPO VTE rates in EPO studiesstudies
Bennett C.L. et al JAMA (2008) 299: 914–924
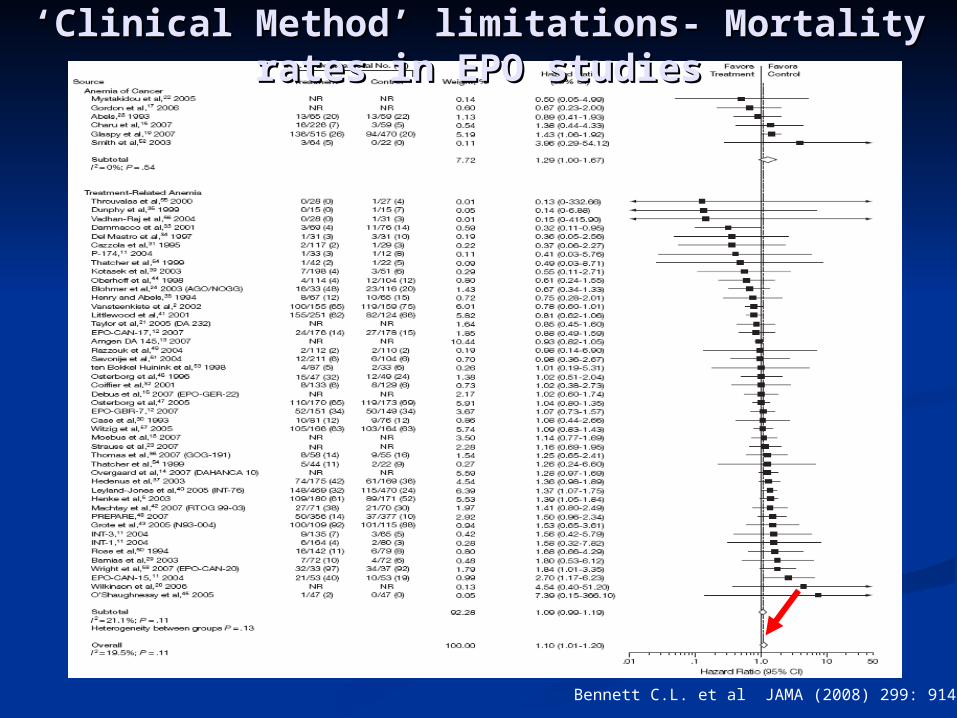
‘‘Clinical Method’ limitations- Clinical Method’ limitations- Mortality rates in Mortality rates in EPO studiesEPO studies
Bennett C.L. et al JAMA (2008) 299: 914–924
Inadequate Recognition of clinical impactInadequate Recognition of clinical impact Inadequate recognition of ‘additional-impact’ Inadequate recognition of ‘additional-impact’
from Cancer Treatmentsfrom Cancer Treatments Erythropoietin data ?Erythropoietin data ? New agents?New agents?
AvastinAvastin SunitinibSunitinib SorafenibSorafenib AxitinibAxitinib PazopanibPazopanib VEGF trap (Aflibercept)VEGF trap (Aflibercept) Anti-EGF strategiesAnti-EGF strategies
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
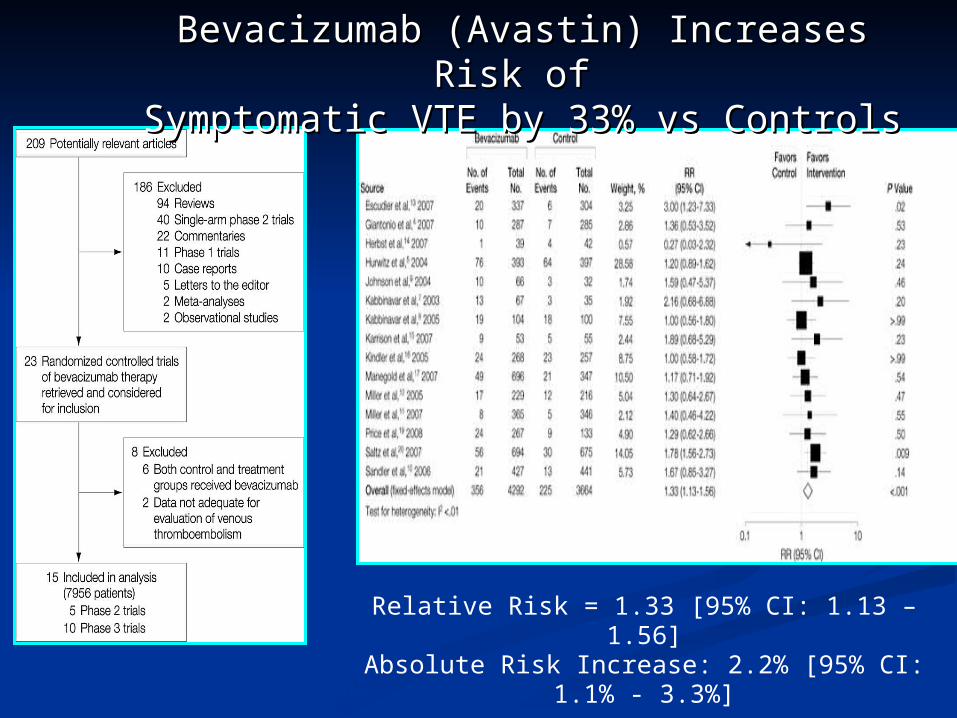
Nalluri, S. R. et al. JAMA 2008;300:2277-2285.
Relative Risk = 1.33 [95% CI: 1.13 – 1.56]Absolute Risk Increase: 2.2% [95% CI: 1.1% -
3.3%]
Bevacizumab (Avastin) Increases Risk of Bevacizumab (Avastin) Increases Risk of Symptomatic VTE by 33% vs ControlsSymptomatic VTE by 33% vs Controls
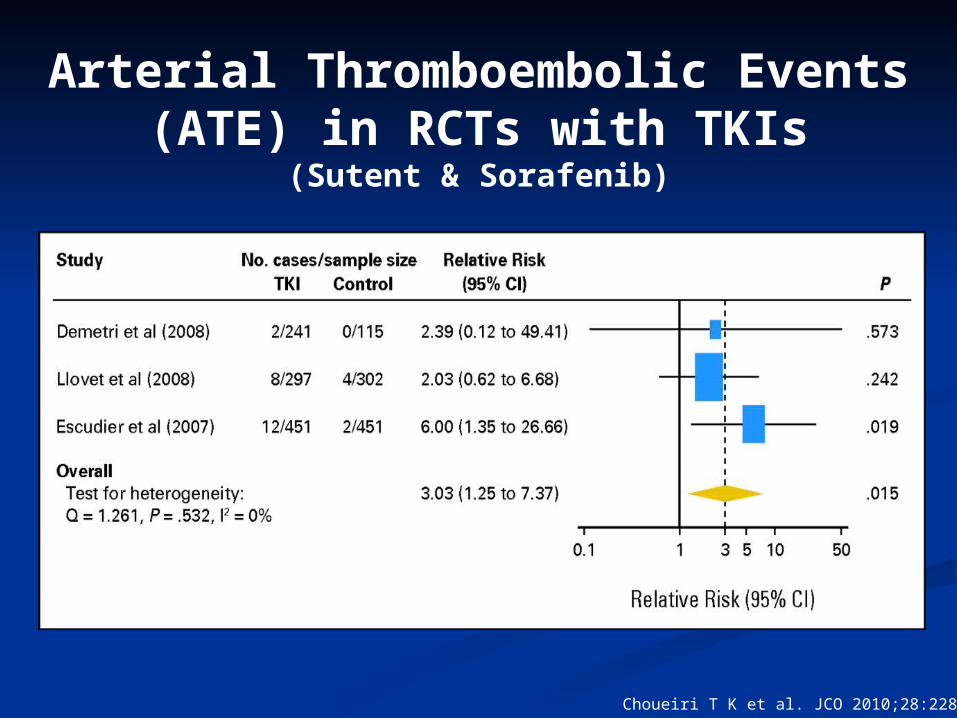
Arterial Thromboembolic Events (ATE) in RCTs with TKIs
(Sutent & Sorafenib)
Choueiri T K et al. JCO 2010;28:2280-2285
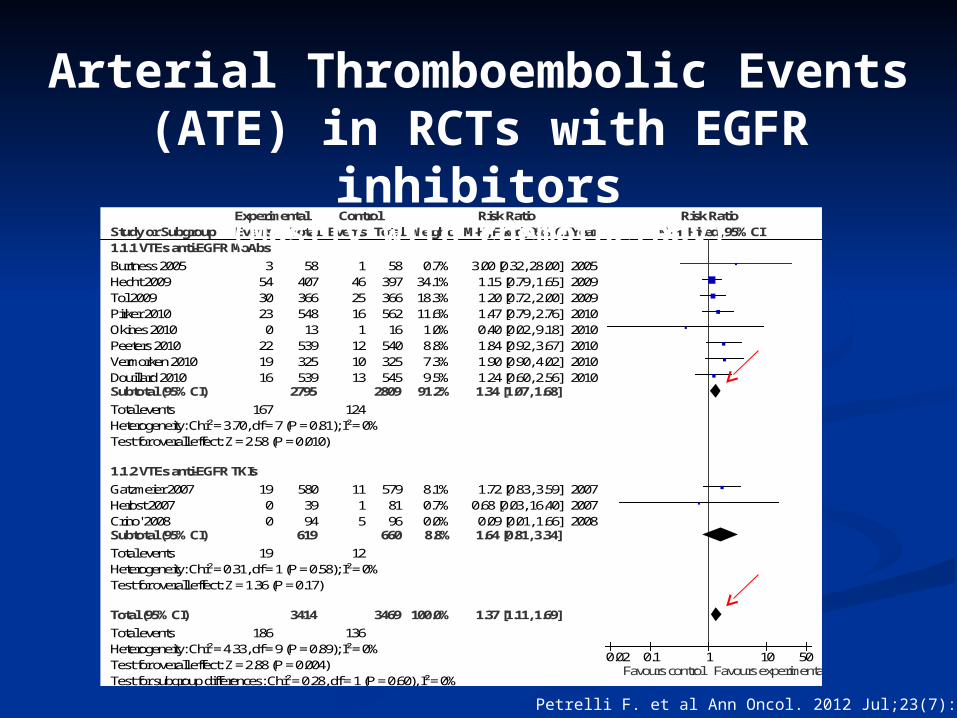
Study or Subgroup1.1.1 VTEs anti-EGFR MoAbs
Burtness 2005Hecht 2009Tol 2009Pirker 2010Okines 2010Peeters 2010Vermorken 2010Douillard 2010Subtotal (95% CI)
Total eventsHeterogeneity: Chi² = 3.70, df = 7 (P = 0.81); I² = 0%Test for overall effect: Z = 2.58 (P = 0.010)
1.1.2 VTEs anti-EGFR TKIs
Gatzmeier 2007Herbst 2007Crino' 2008Subtotal (95% CI)
Total eventsHeterogeneity: Chi² = 0.31, df = 1 (P = 0.58); I² = 0%Test for overall effect: Z = 1.36 (P = 0.17)
Total (95% CI)
Total eventsHeterogeneity: Chi² = 4.33, df = 9 (P = 0.89); I² = 0%Test for overall effect: Z = 2.88 (P = 0.004)Test for subgroup differences: Chi² = 0.28, df = 1 (P = 0.60), I² = 0%
Events
35430230
221916
167
1900
19
186
Total
5840736654813
539325539
2795
5803994
619
3414
Events
14625161
121013
124
1115
12
136
Total
5839736656216
540325545
2809
5798196
660
3469
Weight
0.7%34.1%18.3%11.6%1.0%8.8%7.3%9.5%
91.2%
8.1%0.7%0.0%8.8%
100.0%
M-H, Fixed, 95% CI
3.00 [0.32, 28.00]1.15 [0.79, 1.65]1.20 [0.72, 2.00]1.47 [0.79, 2.76]0.40 [0.02, 9.18]1.84 [0.92, 3.67]1.90 [0.90, 4.02]1.24 [0.60, 2.56]1.34 [1.07, 1.68]
1.72 [0.83, 3.59]0.68 [0.03, 16.40]0.09 [0.01, 1.66]1.64 [0.81, 3.34]
1.37 [1.11, 1.69]
Year
20052009200920102010201020102010
200720072008
Experimental Control Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.02 0.1 1 10 50Favours control Favours experimental
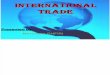
Arterial Thromboembolic Events (ATE) in RCTs with EGFR inhibitors
(Mostly with chemotherapy)
Petrelli F. et al Ann Oncol. 2012 Jul;23(7):1672-9
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Risk obscured by discrepant Risk obscured by discrepant demographics of Trial sample vs demographics of Trial sample vs Real World populationsReal World populations AgeAge
Mean age of trial patients commonly 60-65Mean age of trial patients commonly 60-65 Mean age community population treated Mean age community population treated
70-7570-75
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
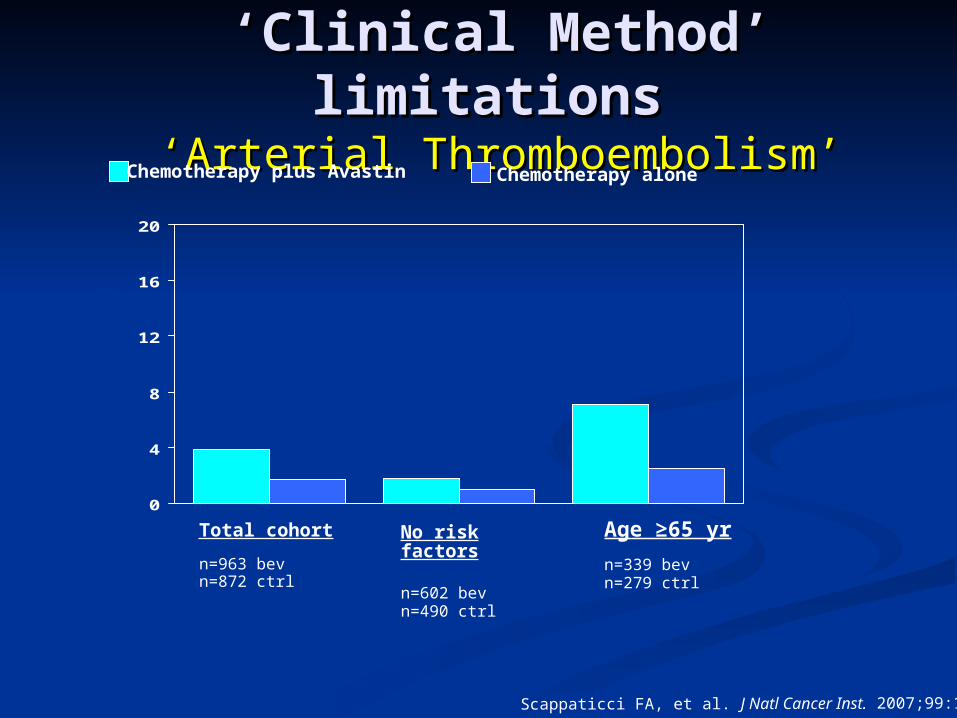
‘‘Clinical Method’ limitationsClinical Method’ limitations ‘‘Arterial ThromboembolismArterial Thromboembolism’’
0
4
8
12
16
20
Chemotherapy plus Avastin Chemotherapy alone
ATE R
ate
(%
)
Total cohort n=963 bevn=872 ctrl
Age ≥65 yr n=339 bevn=279 ctrl
No risk factors
n=602 bevn=490 ctrl
Scappaticci FA, et al. J Natl Cancer Inst. 2007;99:1232-1239.
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Risk obscured by discrepant Risk obscured by discrepant demographics of Trial sample vs demographics of Trial sample vs Community populationsCommunity populations AgeAge
Mean age of trial patients commonly 60-65Mean age of trial patients commonly 60-65 Mean age community population treated Mean age community population treated
70-7570-75 History of VTE (any)History of VTE (any)
How many of us take a proper thrombosis How many of us take a proper thrombosis history?history?
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
0
4
8
12
16
20
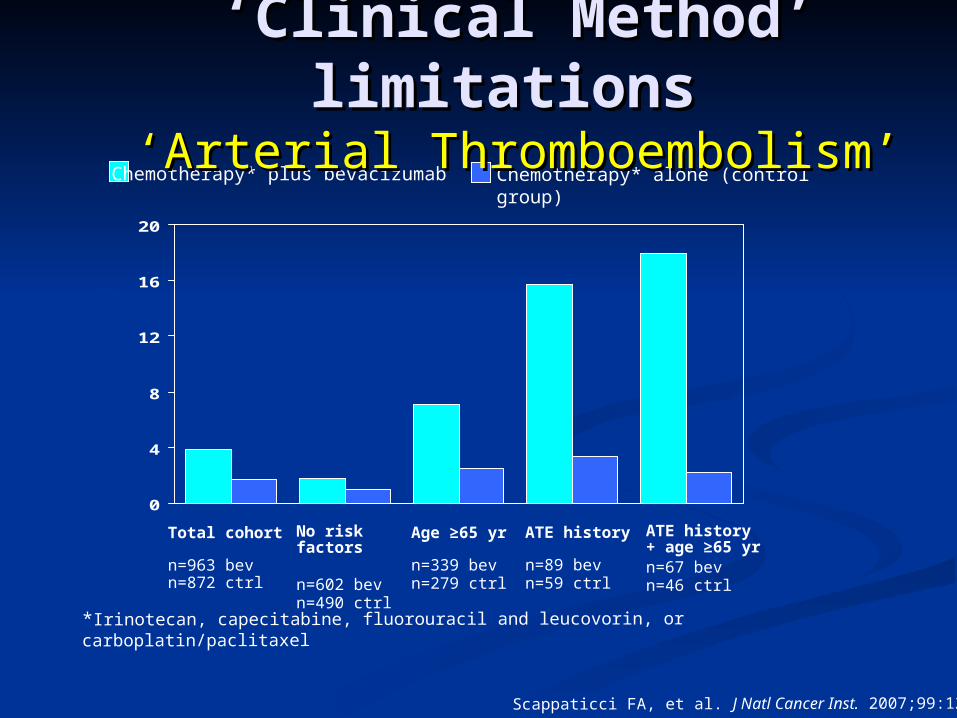
Chemotherapy* plus bevacizumab Chemotherapy* alone (control group)
ATE R
ate
(%
)
Total cohort n=963 bevn=872 ctrl
ATE history + age ≥65 yrn=67 bevn=46 ctrl
ATE history n=89 bevn=59 ctrl
Age ≥65 yr n=339 bevn=279 ctrl
No risk factors
n=602 bevn=490 ctrl
Scappaticci FA, et al. J Natl Cancer Inst. 2007;99:1232-1239.
*Irinotecan, capecitabine, fluorouracil and leucovorin, or carboplatin/paclitaxel
‘‘Clinical Method’ Clinical Method’ limitationslimitations
‘‘Arterial ThromboembolismArterial Thromboembolism’’
Inadequate Recognition of clinical Inadequate Recognition of clinical impactimpact
Inadequate recognition of Inadequate recognition of ‘additional-impact’ from intervention ‘additional-impact’ from intervention
Risk obscured by discrepant Risk obscured by discrepant demographics of Trial sample vs demographics of Trial sample vs Community populationsCommunity populations
Reporting MethodologyReporting Methodology
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
Reporting MethodologyReporting Methodology Standards of Care set by trialsStandards of Care set by trials
Grading toolGrading tool
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
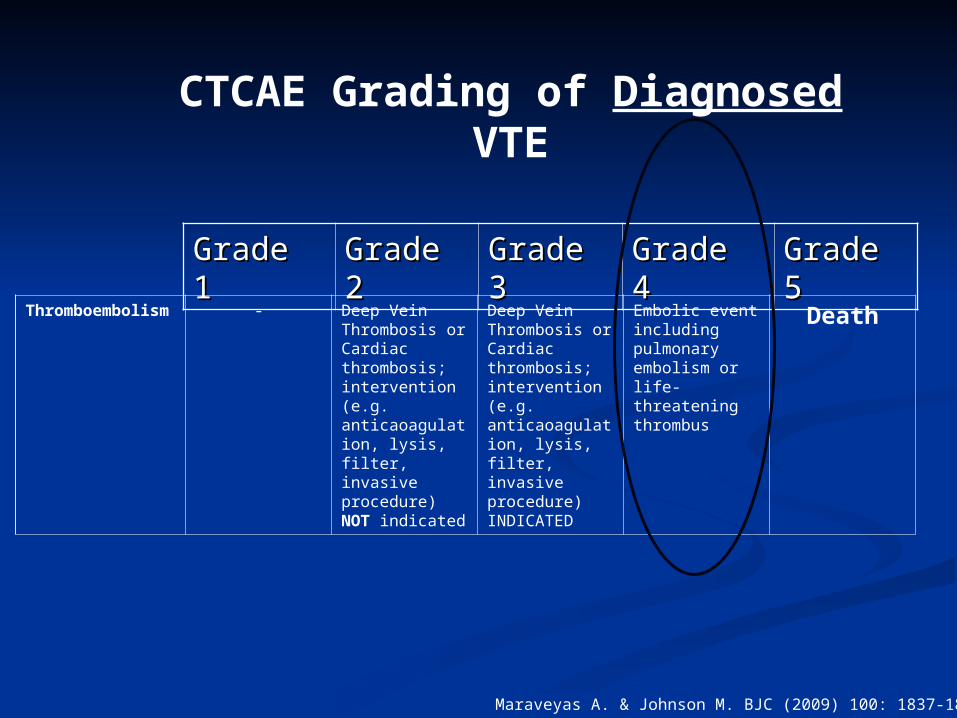
Grade 1Grade 1 Grade Grade 22
Grade Grade 33
Grade 4Grade 4 Grade Grade 55
Thromboembolism - Deep Vein Thrombosis or Cardiac thrombosis; intervention (e.g. anticaoagulation, lysis, filter, invasive procedure) NOT indicated
Deep Vein Thrombosis or Cardiac thrombosis; intervention (e.g. anticaoagulation, lysis, filter, invasive procedure) INDICATED
Embolic event including pulmonary embolism or life-threatening thrombus
Death
CTCAE Grading of Diagnosed VTE
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841

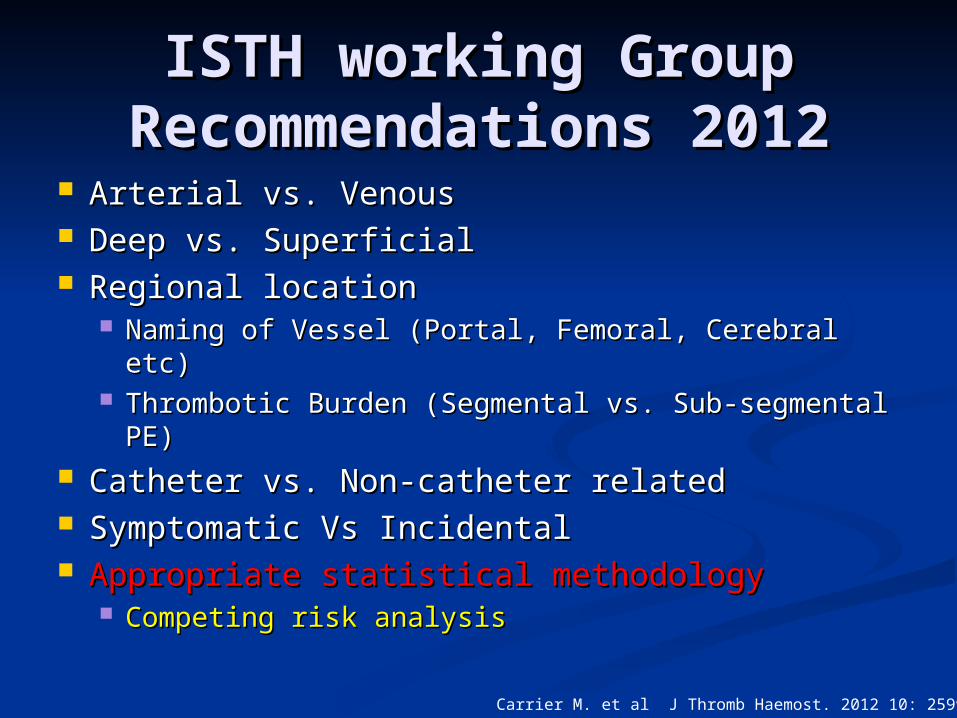
ISTH working Group ISTH working Group Recommendations 2012Recommendations 2012
Arterial vs. VenousArterial vs. Venous Deep vs. SuperficialDeep vs. Superficial Regional locationRegional location
Naming of Vessel (Portal, Femoral, Cerebral etc)Naming of Vessel (Portal, Femoral, Cerebral etc) Thrombotic Burden (Segmental vs. Sub-Thrombotic Burden (Segmental vs. Sub-
segmental PE)segmental PE) Catheter vs. Non-catheter relatedCatheter vs. Non-catheter related Symptomatic Vs IncidentalSymptomatic Vs Incidental Appropriate statistical methodologyAppropriate statistical methodology
Competing risk analysisCompeting risk analysis
Carrier M. et al J Thromb Haemost. 2012 10: 2599-601
Reporting MethodologyReporting MethodologyStandards of Care set by trialsStandards of Care set by trials
Grading toolGrading toolSAE -AESAE -AE
IdentificationIdentification
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
VTE in APC TrialsVTE in APC Trials 19 phase III randomised trials19 phase III randomised trials 6212 patients 6212 patients 1447 (23.3%) died in the first three-month 1447 (23.3%) died in the first three-month
period.period. PresumedPresumed progressive cancer in 1407 (97.2%) progressive cancer in 1407 (97.2%) Cause of death was reported in only 40 cases Cause of death was reported in only 40 cases
(2.8%).(2.8%). Progressive cancer 21 (52.5%) Progressive cancer 21 (52.5%) Infection (20%) Infection (20%) ‘‘Cancer-related complications’ (10%)Cancer-related complications’ (10%) ARF (5%).ARF (5%). VTE (5%)VTE (5%)
Sgouros J, Maraveyas A. Acta Oncologica, 47(3): 2008, 337 – 346.Sgouros J, Maraveyas A. Acta Oncologica, 47(3): 2008, 337 – 346.
Of 1447 patients who died in 12 Of 1447 patients who died in 12 weeks from commencing trialweeks from commencing trial 2 (!) Were reported as having died of a 2 (!) Were reported as having died of a
VTE VTE (0.1%) (0.1%)
Not Recognized or Not Not Recognized or Not Reported?Reported?
Sgouros J, Maraveyas A. Acta Oncologica, 47(3): 2008, 337 – 346.Sgouros J, Maraveyas A. Acta Oncologica, 47(3): 2008, 337 – 346.
PA.3 TrialPA.3 TrialGem-Erlotinib Vs GemGem-Erlotinib Vs Gem
Initial publication had no mention of Initial publication had no mention of VTEVTE
‘‘Correspondence request’Correspondence request’ 14% VTE in each arm14% VTE in each arm
40/245 Gem Erlotinib40/245 Gem Erlotinib 41/243 Gem SA41/243 Gem SA
Moore MJ, et al: J Clin Oncol 25:1960-1966, 2007
GISCAD RCT-Colorectal GISCAD RCT-Colorectal CancerCancer
During the trial the Co-ordinating During the trial the Co-ordinating centre had VTE reported by the centre had VTE reported by the investigators investigators 2/266 (0.7%) 2/266 (0.7%)
Retrospective Trial Monitoring Retrospective Trial Monitoring revealedrevealed
27/266 (10.1%)27/266 (10.1%)
14-fold difference14-fold difference
Mandalà M et al. Eur J Cancer. 2009 Jan;45(1):65-73
Active ascertainment of Active ascertainment of Thrombosis Thrombosis can produce an up to can produce an up to 55-fold greater incidence than 55-fold greater incidence than passive ascertainmentpassive ascertainment Reynolds M.W. et al Current Medical Research Reynolds M.W. et al Current Medical Research
and Opinions (2008) 24: 497-505 and Opinions (2008) 24: 497-505
Not Recognized or Not Not Recognized or Not Reported?Reported?
Reporting MethodologyReporting MethodologyStandards of Care set by trialsStandards of Care set by trials
Grading toolGrading toolSAE-AE SAE-AE
IdentificationIdentification Attributing CausalityAttributing Causality
‘‘Clinical Method’ Clinical Method’ limitationslimitations
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
Attributing CausalityAttributing Causality
Long term morbidity and outcome Long term morbidity and outcome compromise?compromise? CCF after MICCF after MI Paresis and aftermath after CVAParesis and aftermath after CVA Cancer treatment termination due to Cancer treatment termination due to
MI/CVAMI/CVA Pulmonary insufficiency from chronic Pulmonary insufficiency from chronic
PE effectsPE effects
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
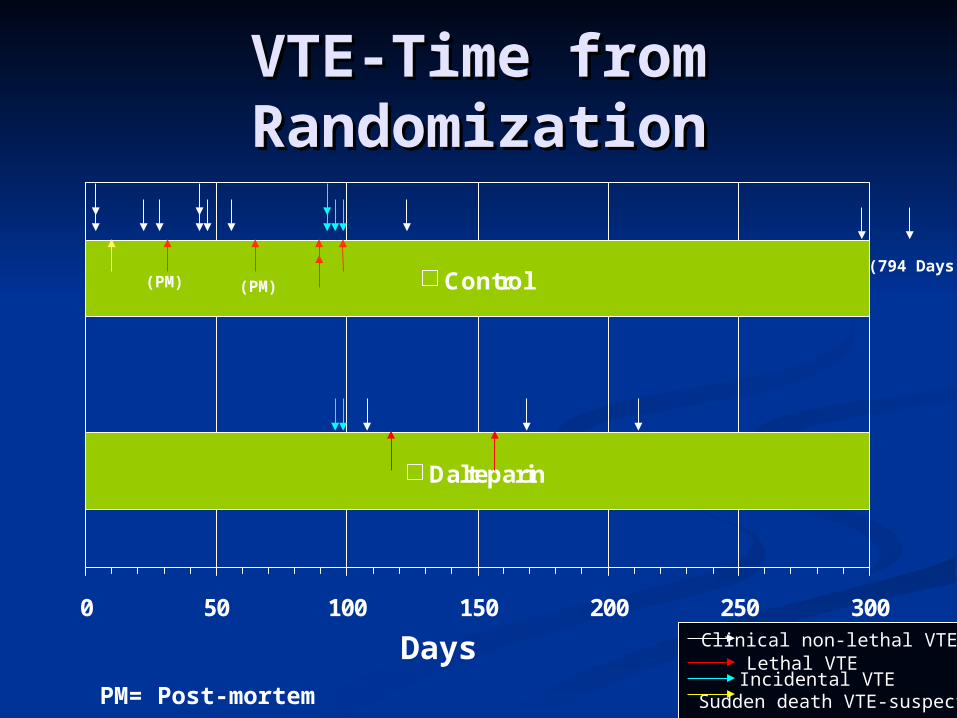
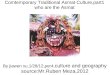
VTE-Time from VTE-Time from RandomizationRandomization
Dalteparin
Control
0 50 100 150 200 250 300
Days
(794 Days)(PM) (PM)
Clinical non-lethal VTELethal VTEIncidental VTE
Sudden death VTE-suspectedPM= Post-mortem
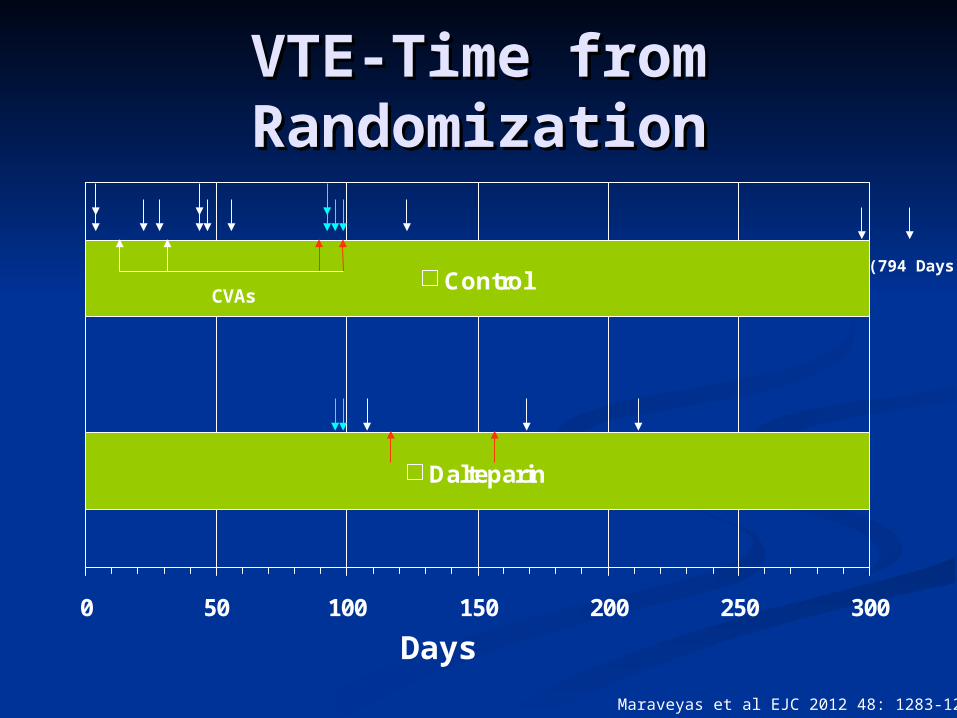
VTE-Time from VTE-Time from RandomizationRandomization
Dalteparin
Control
0 50 100 150 200 250 300
Days
(794 Days)
CVAs
Maraveyas et al EJC 2012 48: 1283-1292
Follow-up MethodologyFollow-up Methodology
Long term morbidity and outcome Long term morbidity and outcome compromise?compromise? CCF after MICCF after MI Paresis and aftermath after CVAParesis and aftermath after CVA Cancer treatment termination due to Cancer treatment termination due to
MI/CVAMI/CVA Pulmonary insufficiency from chronic Pulmonary insufficiency from chronic
PE effectsPE effects
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
Follow-up MethodologyFollow-up Methodology
Long term morbidity and outcome Long term morbidity and outcome compromise?compromise? CCF after MICCF after MI Paresis and aftermath after CVAParesis and aftermath after CVA Cancer treatment termination due to Cancer treatment termination due to
MI/CVAMI/CVA Pulmonary insufficiency from chronic Pulmonary insufficiency from chronic
PE effectsPE effects VTE domino-effect?VTE domino-effect?
Maraveyas A. & Johnson M. BJC (2009) 100: 1837-1841
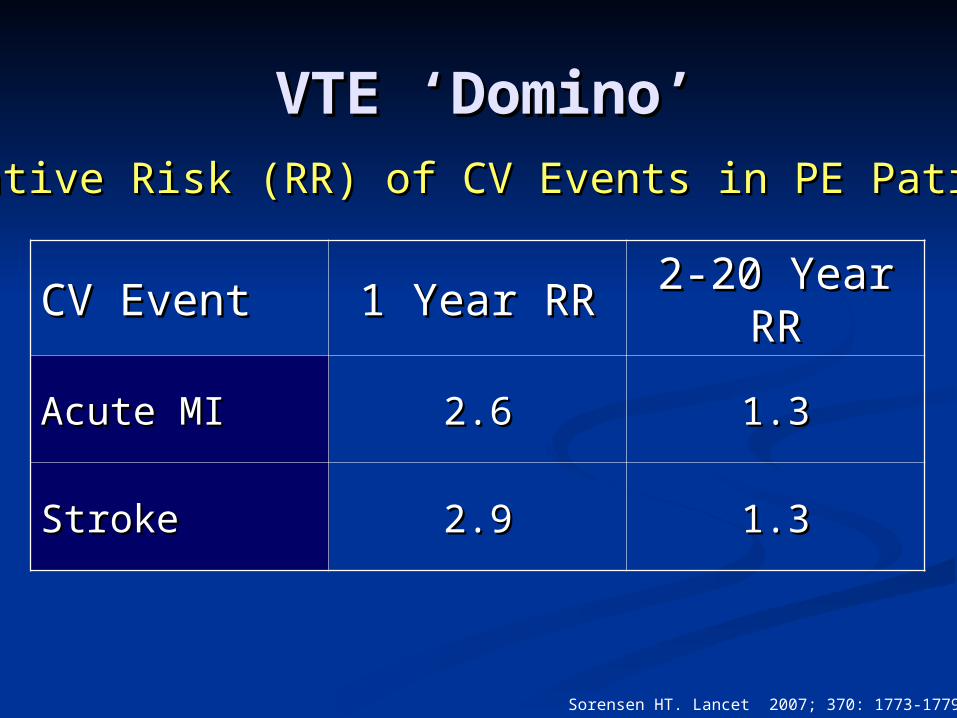
VTE ‘Domino’VTE ‘Domino’
CV EventCV Event 1 Year RR1 Year RR 2-20 Year 2-20 Year RRRR
Acute MIAcute MI 2.62.6 1.31.3
StrokeStroke 2.92.9 1.31.3
Sorensen HT. Lancet 2007; 370: 1773-1779
Relative Risk (RR) of CV Events in PE PatientsRelative Risk (RR) of CV Events in PE Patients
VTE-‘Perception VTE-‘Perception Gap’Gap’
(A.A. Turpie)(A.A. Turpie)Clinically non-recognized Clinically non-recognized
VTE –syndrome does VTE –syndrome does
not meannot mean clinically insignificant VTEclinically insignificant VTE
CAT-treatment CAT-treatment (Prophylaxis) (Prophylaxis)
Related ToxicityRelated Toxicity
BleedingBleeding
5
10
15
20
2 4 6 8 10 12
%
Months
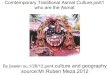
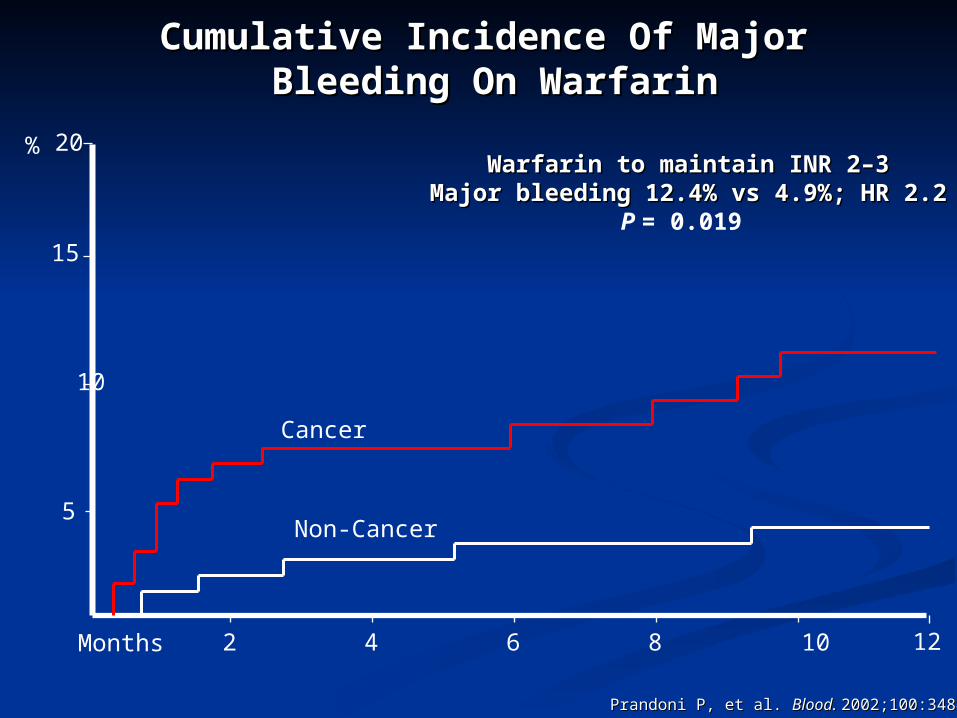
Cumulative Incidence Of Major Cumulative Incidence Of Major Bleeding On WarfarinBleeding On Warfarin
Prandoni P, et al. Prandoni P, et al. Blood. Blood. 2002;100:3484-3488. 2002;100:3484-3488.
Warfarin to maintain INR 2Warfarin to maintain INR 2––33Major bleeding 12.4% vs 4.9%; HR 2.2Major bleeding 12.4% vs 4.9%; HR 2.2
P = 0.019
Cancer
Non-Cancer
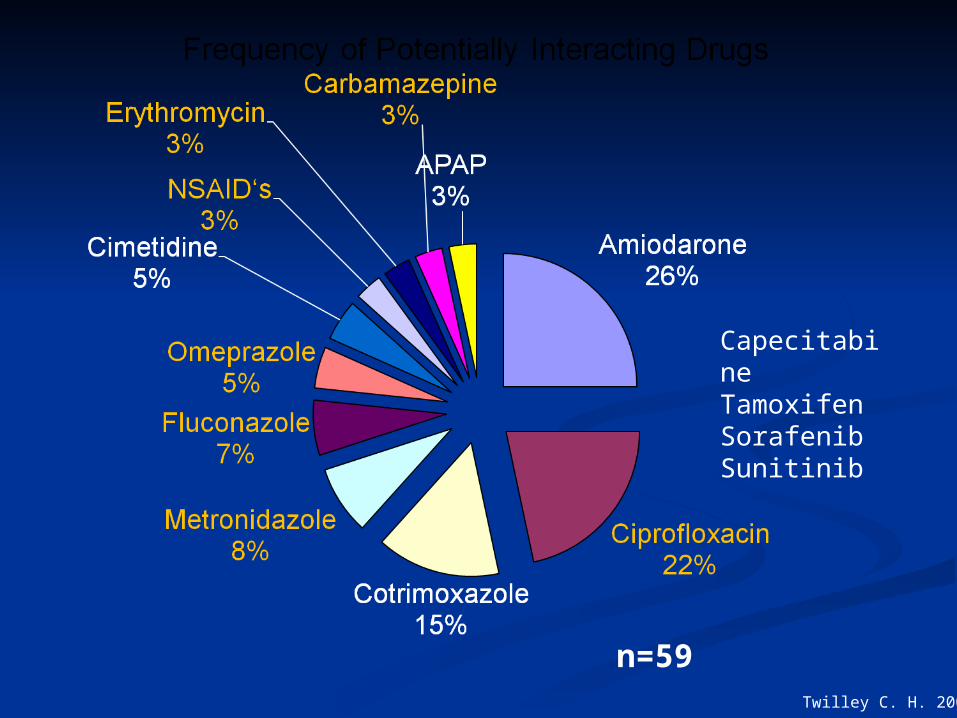
n=59
CapecitabineTamoxifenSorafenibSunitinib
Twilley C. H. 2002
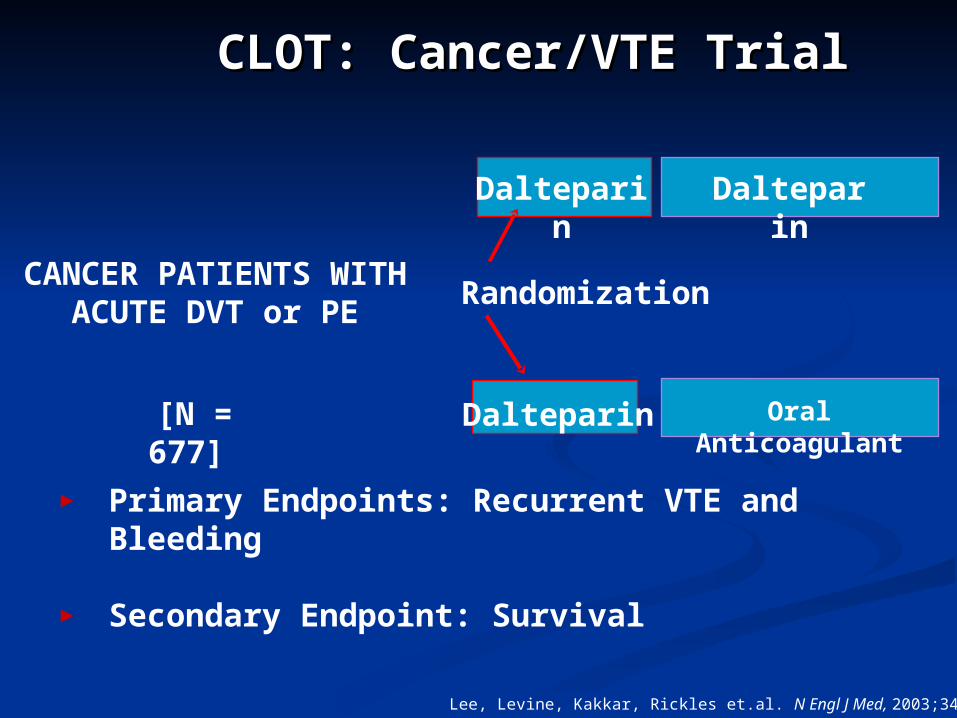
CLOT: Cancer/VTE TrialCLOT: Cancer/VTE Trial
CANCER PATIENTS WITH ACUTE DVT or
PE
Randomization
Oral Anticoagulant
Dalteparin
[N = 677]
► Primary Endpoints: Recurrent VTE and Bleeding
► Secondary Endpoint: Survival
Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, 2003;349:146
Dalteparin
Dalteparin
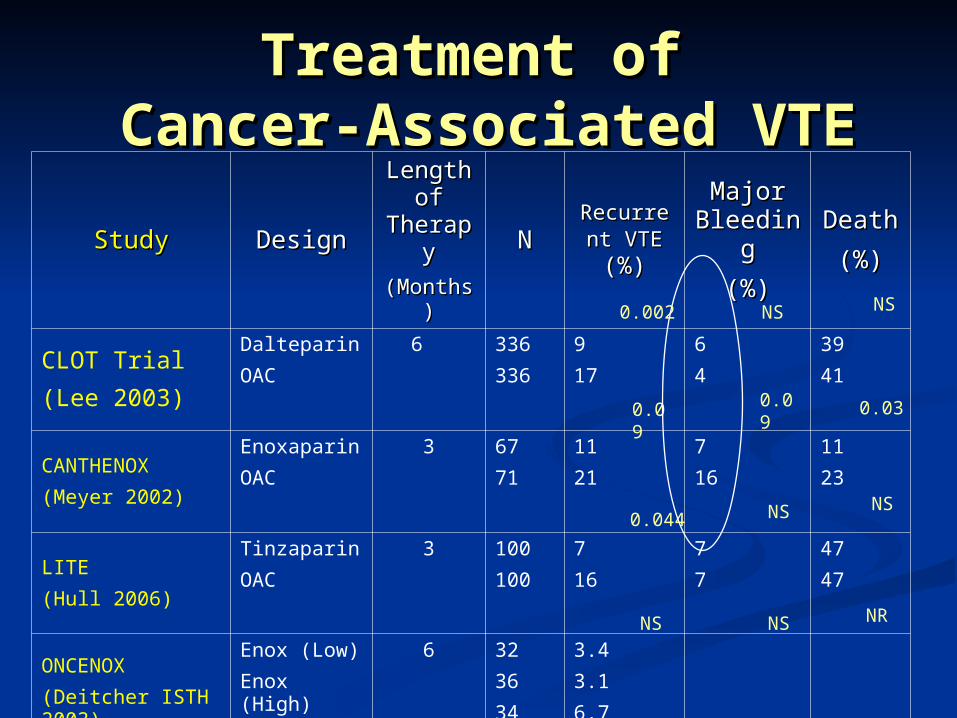
Treatment of Treatment of Cancer-Associated VTECancer-Associated VTE
StudyStudy DesignDesign
Length Length of of
TherapTherapyy
(Months(Months))
NNRecurrenRecurren
t VTEt VTE (%)(%)
Major Major BleedinBleedin
gg
(%)(%)
DeathDeath
(%)(%)
CLOT Trial
(Lee 2003)
Dalteparin
OAC
6 336
336
9
17
6
4
39
41
CANTHENOX
(Meyer 2002)
Enoxaparin
OAC
3 67
71
11
21
7
16
11
23
LITE
(Hull 2006)
Tinzaparin
OAC
3 100
100
7
16
7
7
47
47
ONCENOX
(Deitcher ISTH 2003)
Enox (Low)
Enox (High)
OAC
6 32
36
34
3.4
3.1
6.7
NS
NS0.044
NS
NS0.002
NS
NS
NR
0.09
0.030.09
Retrospective cohort Retrospective cohort studiesstudies
Bleeding was reported as major or Bleeding was reported as major or ‘clinically significant’ ‘clinically significant’ in 11in 1135%; minor in 35%; minor in 252532%32% Up to five-fold greater than recorded in RCTsUp to five-fold greater than recorded in RCTs
Risk of bleeding associated with Risk of bleeding associated with increasing age and chemotherapy in one increasing age and chemotherapy in one study.study.
In another, bleeding unrelated to In another, bleeding unrelated to thrombocytopenia, abnormal blood thrombocytopenia, abnormal blood coagulation or metastases.coagulation or metastases.
Noble S. et al Lancet Oncol. 2008; 9: 577-84
Scoring Hemorrhagic Scoring Hemorrhagic Event SeverityEvent Severity
ISTH Scoring (ISTH, 2005) ISTH Scoring (ISTH, 2005) ‘‘Severe’-MajorSevere’-Major
Fall in haemoglobin of 2 g/dL or transfusion Fall in haemoglobin of 2 g/dL or transfusion of 2 or more units of blood, bleeding that is of 2 or more units of blood, bleeding that is symptomatic in a critical organ (intra-symptomatic in a critical organ (intra-cranial, intra-spinal, intra-ocular, cranial, intra-spinal, intra-ocular, retroperitoneal, intra-articular or peri-retroperitoneal, intra-articular or peri-cardiac, or intra-muscular with cardiac, or intra-muscular with compartment syndrome) or fatal compartment syndrome) or fatal
‘‘Non severe’Non severe’
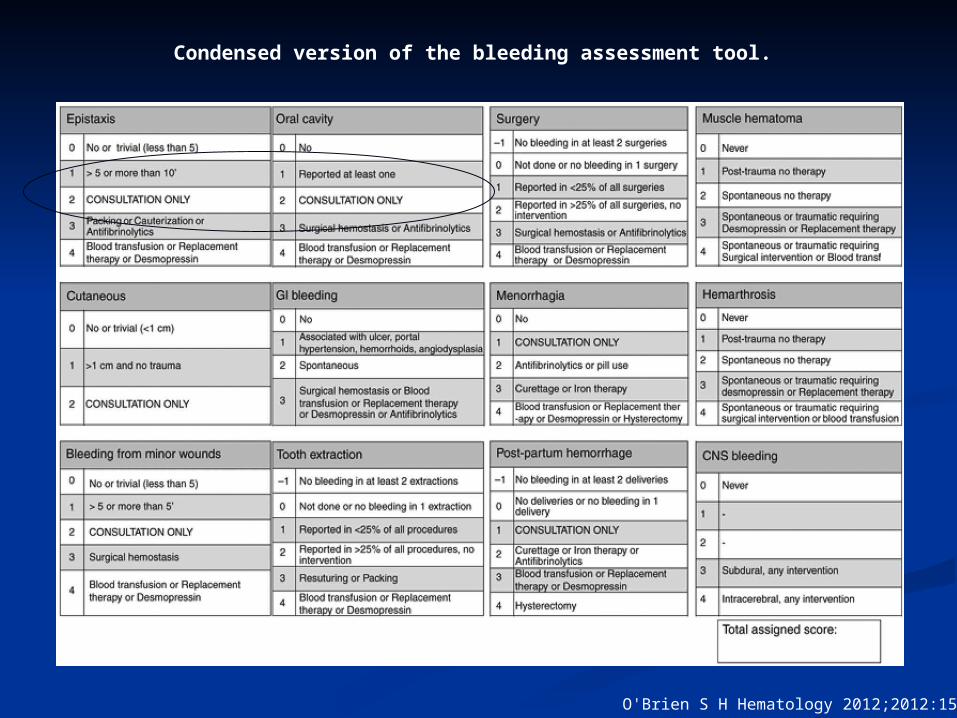
Condensed version of the bleeding assessment tool.
O'Brien S H Hematology 2012;2012:152-156
Relevant toxicity to a Relevant toxicity to a palliative care patientpalliative care patient
Current tools irrelevant for the Current tools irrelevant for the conventional palliative care patient conventional palliative care patient
Role of the clinician’s views (DD project)Role of the clinician’s views (DD project) What we call ‘low grade’ bleeding may have What we call ‘low grade’ bleeding may have
significant impact on patients who have significant impact on patients who have EoL needs and goalsEoL needs and goals
Qualitative research is needed to Qualitative research is needed to understand the patient and carer issues understand the patient and carer issues betterbetter ? Develop a relevant scoring tool? Develop a relevant scoring tool