Embed Size (px)
Citation preview

RESEARCH Open Access
Capturing cognitive and behavioralvariability among individuals with Downsyndrome a latent profile analysisMarie Moore Channell1dagger Laura J Mattie1dagger Debra R Hamilton2 George T Capone3 E Mark Mahone4Stephanie L Sherman2 Tracie C Rosser2 Roger H Reeves5 Luther G Kalb6 and The Down Syndrome CognitionProject
Abstract
Background There is a high degree of inter- and intra-individual variability observed within the phenotype ofDown syndrome The Down Syndrome Cognition Project was formed to capture this variability by developing alarge nationwide database of cognitive behavioral health and genetic information on individuals with Downsyndrome ages 6ndash25 years The current study used the Down Syndrome Cognition Project database to characterizecognitive and behavioral variability among individuals with Down syndrome
Methods Latent profile analysis was used to identify classes across a sample of 314 participants based on theircognition (IQ and executive functioning) adaptive and maladaptive behavior and autism spectrum disordersymptomatology A multivariate multinomial regression model simultaneously examined demographic correlates ofclass
Results Results supported a 3-class model Each class demonstrated a unique profile across the subdomains ofcognition and behavior The ldquonormativerdquo class was the largest (n = 153 48) and displayed a relatively consistentprofile of cognition and adaptive behavior with low rates of maladaptive behavior and autism symptomatologyThe ldquocognitiverdquo class (n = 109 35) displayed low cognitive scores and adaptive behavior and more autismsymptomatology but with low rates of maladaptive behavior The ldquobehavioralrdquo class the smallest group (n = 5217) demonstrated higher rates of maladaptive behavior and autism symptomatology but with cognition levelssimilar to the ldquonormativerdquo class their adaptive behavior scores fell in between the other two classes Householdincome and sex were the only demographic variables to differ among classes
Conclusions These findings highlight the importance of subtyping the cognitive and behavioral phenotype amongindividuals with Down syndrome to identify more homogeneous classes for future intervention and etiologic studiesResults also demonstrate the feasibility of using latent profile analysis to distinguish subtypes in this populationLimitations and future directions are discussed
Keywords Down syndrome Phenotypes Intellectual disability Latent profile analysis Cognition Adaptive behaviorMaladaptive behavior Autism symptomatology
copy The Author(s) 2021 Open Access This article is licensed under a Creative Commons Attribution 40 International Licensewhich permits use sharing adaptation distribution and reproduction in any medium or format as long as you giveappropriate credit to the original author(s) and the source provide a link to the Creative Commons licence and indicate ifchanges were made The images or other third party material in this article are included in the articles Creative Commonslicence unless indicated otherwise in a credit line to the material If material is not included in the articles Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use you will need to obtainpermission directly from the copyright holder To view a copy of this licence visit httpcreativecommonsorglicensesby40The Creative Commons Public Domain Dedication waiver (httpcreativecommonsorgpublicdomainzero10) applies to thedata made available in this article unless otherwise stated in a credit line to the data
Correspondence channellillinoisedudaggerMarie Moore Channell and Laura J Mattie are the co-first authors of thestudy1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USAFull list of author information is available at the end of the article
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 httpsdoiorg101186s11689-021-09365-2
Down syndrome (DS) is the most common chromo-somal disorder among births and is the leading geneticcause of intellectual disability [1] Individuals with DShave an extra copy of chromosome 21 in all or some oftheir cells This genetic difference results in a phenotypethat increases the likelihood of certain medical condi-tions (eg congenital heart disease sleep apnea [2]) andcognitive and behavioral characteristics [3] These char-acteristics include lower than average IQ and reducedadaptive functioning both of which are associated withintellectual disability in general [4] However DS also re-sults in phenotype-specific characteristics (eg relativedifficulties in verbal processing relative strengths in so-cial functioning [3]) that distinguish it from other neuro-genetic disorders associated with intellectual disabilityThese phenotype-specific features are due to the in-creased dosage of chromosome 21 genes and resultingdysregulation genome-widePerhaps most striking is the high degree of variability ob-
served among individuals with DS regarding the presenceand severity of associated symptoms and conditions Thisvariability is likely due to a combination of genetic and envir-onmental risk factors that alter the expression of many as-pects of the DS phenotype including cognition behaviorand health across the lifespan [5] However the nature ofthis variability in DS is still not well understood complicatingintervention and treatment decisions We hypothesize thatwithin-syndrome variability can be characterized systematic-ally through the identification of subgroups based on cogni-tive and behavioral profiles Thus the current study takes anindividual-differences approach to identify within-group pro-files of cognition and behavior among individuals with DSacross a wide age range (6ndash25 years) using latent profile ana-lysis (LPA) The identification of more homogeneous sub-types of individuals with DS may help increase the ability todiscover associated genetic and environmental risk factors ofseverity Clinically the resulting data will emphasize differentpatterns of strengths and areas in need of additional supportamong individuals with DS Ultimately more precision incharacterization of the individual variability within DS willlead to more targeted treatment and intervention approachesto optimize daily function for this population In the currentstudy we focused on the domains of cognition (IQ and ex-ecutive functioning) adaptive and maladaptive behavior andautism spectrum disorder (ASD) symptomatology
Challenges to the assessment of the cognitive andbehavioral phenotype of DSCognitionResearch on cognition in DS has focused broadly on IQand executive functioning IQ represents overall cogni-tive ability and is thought to broadly impact other areasof functioning (eg adaptive behavior maladaptive be-havior) Another particularly important area of cognition
is executive functioning which encompasses the higher-order cognitive and self-regulatory abilities that are im-portant for goal-directed behavior and daily functioning(eg social interactions academic achievement work be-havior [6ndash10]) The abilities housed under the umbrellaterm of executive functioning include working memoryinhibition shiftingcognitive flexibility attention andplanning Both IQ and executive functioning are import-ant components of the DS phenotype while also show-ing inter-individual variability [11]
IQIQ is perhaps one of the more variable constructs amongindividuals with DS ranging from approximately 40 (orthe lowest score possible on many standardizedintelligence tests) to around 70 (the cutoff score for intel-lectual disability) and in some cases even higher [12]There are two main issues associated with interpreting IQscores in individuals with DS use of age-based norms andscoring at the floor (ie the lowest score possible [13 14])Like others with intellectual disability the rate of
growth in cognitive skills is slower for individuals withDS than in the general population Therefore the use ofage-based norms (ie IQ standard scores) from the gen-eral population leads to a discrepancy that becomes lar-ger with age This discrepancy causes IQ standard scoresto decrease or at least not increase over time despitecontinued growth in cognitive skills [12 15ndash17]Using age-based norms can also lead to many individ-
uals with DS and intellectual disability scoring at thefloor To address this problem some research groupshave developed Z-score-based deviation IQ scores thataccount for performance below the floor-level standardscore (Hessl et al [18] for the Wechsler IntelligenceScale for Children-III Sansone et al [13] for the Stan-ford Binet-5) Another solution to the floor effect prob-lem is to use raw scores or growth scores that representperformance on a standardized IQ test without takinginto account age-based norms [16] This approach is es-pecially useful for interpreting growth over time For ex-ample a review of longitudinal studies using theStanford Binet IV to assess individuals with DS from age4 to 24 years found that 37 scored at the floor leveland thus growth could not be examined with standardscores [12] Raw scores however increased over timeThe rate of growth over time measured using ageequivalent scores was non-linear and highly variableacross individuals Interpretation of these results is lim-ited due to their use of age equivalent scores which donot provide accurate estimates of ability level and havepoor psychometric properties [19] However these re-sults do highlight the high degree of variation associatedwith the DS phenotype The current study takes into ac-count this variation by examining age-corrected raw
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 2 of 14
scores from another IQ measure the Kaufman BriefIntelligence Test 2nd edition (KBIT-2 [20]) in the pro-file analyses
Executive functioningExecutive functioning is an area in which many individ-uals with DS struggle compared to both chronologicaland mental age-matched peers [3 21] Within executivefunctioning the areas of working memory planning andinhibition are particularly difficult for individuals withDS emotional control is considered a relative strength[22 23] Although this pattern appears to be relativelyconsistent across development Loveall et al [23] notedsome nuanced differences in the executive functioningprofile in childhood and adulthoodWorking memory is the component that has been ex-
amined in greater depth across the literature on DS thanother abilities under the executive functioning umbrellaDefined as the simultaneous storing and manipulationprocessing of information [24 25] working memory oftenhas been characterized as an area of weakness for individ-uals with DS with greater difficulties reported in verbalworking memory than visuospatial working memory [2627] Verbal working memory appears to be weak com-pared to both mental age-matched typically developingchildren [28 29] and individuals with other intellectualand developmental disabilities [30ndash33] it also develops ata slower rate in individuals with DS than in peers withother intellectual and developmental disabilities [34]Although historically visuospatial working memory
has been thought to be intact in the DS phenotype [26]recent research suggests variability in performanceamong individuals with DS across different visuospatialworking memory tasks [35] Collectively the literaturepoints to impairments in the spatial-simultaneous [36ndash38] and visual [39 40] components with the spatial-sequential component relatively intact [41]
Adaptive behaviorAdaptive behavior involves the skills needed to functionindependently in everyday life such as self-care domes-tic function and community interactions [4 42 43]These skills are critical to positive long-term outcomesincluding academic success and independence [44ndash47]Research on adaptive behavior generally categorizes as-sociated skills into four broad domains socializationcommunication daily living and motor skillsIndividuals with DS demonstrate relative strengths in
socialization and difficulties in communication andmotor skills [48ndash51] As for daily living the research ismixed on whether this is an area of strength or difficulty[47 49] However Daunhauer [47] analyzed within-group effect sizes for previously conducted adaptive be-havior studies and noted that daily living skills may
actually be an area of relative difficulty due to its overlapwith other adaptive domains For example being able todress oneself is a daily living skill but this can be diffi-cult if an individual has compromised motor skills Re-gardless adaptive behavior is holistically an area ofdifficulty for individuals with DS again with consider-able inter-individual variabilityOne of the challenges to understanding adaptive be-
havior within the DS phenotype is that it is often exam-ined separately from other aspects of the phenotypeHowever it is important to recognize that onersquos abilityto function independently is likely intertwined withother aspects of cognition and behavior For exampleboth executive functioning and IQ are strongly associ-ated with level of adaptive functioning [21 22] and maybe related to the presence of maladaptive behaviors [4752] The present study is specifically designed to investi-gate within-group profiles of adaptive behavior relativeto IQ and executive functioning rather than simplycomparing sample means across these constructs
Maladaptive behaviorsIn contrast to adaptive behavior maladaptive behaviorsrepresent a range of behaviors that impede health well-being educational and occupational outcomes and dailyfunctioning These behaviors are traditionally catego-rized as internalizing (eg anxious or depressed symp-toms) or externalizing (eg inattentionhyperactivityaggressive behaviors) Higher levels of maladaptive be-haviors have been noted in individuals with DS who alsohave identified comorbid neurobehavioral disorders (egASD disruptive behavior disorder [53ndash56])Children and adolescents with DS have higher rates of
maladaptive behaviors than the general population [57ndash59] However the within-DS profile of maladaptive be-haviors appears nuanced For example population-basedstudies of Dutch individuals with DS showed high ratesof problems in the ldquosocialrdquo and ldquoinattentionrdquo domains onthe Child Behavior Checklist but relatively low rates ofinternalizing problems in the ldquoanxious-depressedrdquo do-main [58 59] Although scores in the ldquodelinquent behav-iorrdquo and ldquoaggressive behaviorrdquo domains were slightlyelevated in the child cohort the effect size was smallsuggesting a nuanced difference at best [58] A develop-mental pattern also emerged such that more difficultieswith ldquoanxious-depressedrdquo symptoms were found in theadolescent group than in younger children This patternis consistent with other within-syndrome reports as wellas the broader literature on internalizing behaviors inadolescents [57 60] One aspect that remains unclear ishow maladaptive behaviors relate to cognition Thecurrent study directly addresses this gap by using clusterprofiles to examine these associations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 3 of 14
Comorbid autism spectrum disorder (ASD) in DSIndividuals with DS are at a greater risk of comorbid ASDthan the general population with prevalence estimates sug-gesting up to 19 [61] Notably comorbid ASD tends to im-pact both cognitive and behavioral aspects of the DSphenotype Compared to individuals with DS who do nothave comorbid ASD individuals with DS and comorbidASD tend to display more maladaptive behaviors (ie stereo-typic and anxiouswithdrawn domains [53 55]) and lowerIQ and adaptive functioning [61 62] Additionally studiesexamining broader ASD-like symptomatology among indi-viduals with DS who are at low risk for comorbid ASD havefound a similar pattern lower IQ and adaptive functioningand higher rates of maladaptive behaviors are associated withbroader ASD-like symptoms [63ndash65] Therefore it appearsthat there is some overlap between ASD-like symptoms andthe behavioral phenotype associated with DS However it isunclear if the use of group-level means obscures a more nu-anced profile of cognition and adaptive behavior in relationto ASD symptomatology in DS similar to what is observedin non-syndromic ASD [66]
Current studyThe literature on cognition (IQ and executive function-ing) adaptive and maladaptive behaviors and ASDsymptomatology associated with the DS phenotype indi-cates a general syndrome-specific pattern however asreviewed above it also indicates significant variabilityThus we hypothesize that the general syndrome-specificpattern does not represent all individuals with DS andthat within-group profiles can be identified More nu-anced within-group profiles may vary by age becausegeneral developmental differences within the syndrome-specific pattern of strengths and weakness have beennoted in the literature Thus we also hypothesize thatage is associated with within-group profilesUsing LPA as an exploratory approach we aimed to test
our hypotheses by (1) determining whether subgroups of in-dividuals with DS can be characterized using performance-based and caregiver-informed ratings of behavior and cogni-tion and (2) examining the demographic characteristics asso-ciated with the latent subgroups To achieve these aims westudied a large sample of individuals with DS ages 6ndash25years who were recruited through a network of sites acrossthe USA called the Down Syndrome Cognition Project (seeRosser et al [14])
MethodsParticipantsThree hundred fifty-six individuals with DS ages 6ndash25years old participated in the larger study the Down Syn-drome Cognition Project (see Rosser et al [14] for inclu-sion criteria and participation rates) Using that samplewe retained all members of the original cohort except
for participants who were missing data on three or moreof the primary measures (n = 42) resulting in a finalsample size of 314 Participants were recruited fromclinics community eventssupport groups conferencesadvertisements and previous research studies by mul-tiple sites across the USA See Table 1 for participantdemographic information
Measures and procedureThe Down Syndrome Cognition Project testing battery [14]included a series of performance-based neuropsychologicalassessments modified from the Arizona Cognitive Test Bat-tery which was developed to produce outcome measures forclinical trials involving individuals with DS [67 68] The testbattery has good test-retest reliability [67]Examiners at each Down Syndrome Cognition Project
site were trained to fidelity to administer the testing bat-tery to individuals with DS (see Edgin et al [67 68])Sites were monitored by the University of Arizona train-ing site andor the Emory Data Coordinating CenterPeriodic quality control checks included review of fidel-ity to administration and scoring procedures All datawere double entered with comparison checks to ensureaccuracy Research Electronic Data Capture (REDCap[69]) was used for data entry and managementParticipants completed the testing battery at an assess-
ment site or another convenient location (eg commu-nity center or family home) The entire session lastedabout 2ndash3 h with frequent breaks Tests were presentedin two fixed counterbalanced orders [67] Caregiverscompleted questionnaires related to participant demo-graphics medicaldevelopmental history and behaviorsTable 2 includes a description of the primary measures in-
cluded in the model These tests were selected based on sev-eral criteria Most importantly each measure was selected onthe basis of reflecting an important and unique componentof cognition behavior or development Where possible weused total composite or summary scores from the indicatedmeasure to capture all salient information and reduce thenumber of overall variables Variables were also selectedbased on normality Variables that were highly skewed dueto floor or ceiling effects limited the ability to measure thefull range of abilities and discriminate among subgroups andthus were eliminated from the analyses Finally measureswere also selected based on number of observations becausenot all measures were administered to the entire cohort
Performance-based assessments of cognitionThree performance-based tests of cognition were in-cluded in this study Intelligence was evaluated using theKaufman Brief Intelligence Test 2nd edition (KBIT-2[20]) Verbal and nonverbal raw scores were summedand then averaged for use in the model This approachwas taken because the IQ composite variable had
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 4 of 14
significant floor effects (34 of the sample had an IQle40) Working memory was evaluated using the Cam-bridge Neuropsychological Test Automated Battery(CANTAB) Spatial Span test which required the partici-pant to recall progressively longer sequences of visual in-formation (colored squares) presented on a touchscreenVisuomotor tracking and hand-eye coordination wereevaluated using the NEPSY-II Visuomotor PrecisionTask (ages 3ndash4) For this task the participant used theirpreferred hand to draw a line as quickly as possiblewhile staying inside the tracked lines [70]
Caregiver-informed measuresFour caregiver-report measures of cognition and behav-ior were included Executive functioning impairmentswere assessed via the Global Executive Composite stand-ard score from the Behavioral Rating Inventory of Ex-ecutive Function School Age (BRIEF [71]) Adaptivebehavior was evaluated using the standard composite
score of the Scales of Independent Behavior-RevisedShort Form (SIB-R [72]) Maladaptive behavior wasassessed across three variables (conduct problems anx-iety and hyperactivity) from the Nisonger Child Behav-ior Rating Form (NCBRF [73]) These subscales wereselected because the additional subscales overlappedwith the other measures employed in this study (egASD symptoms adaptive behavior) ASD symptomswere assessed via the Social Communication Question-naire Lifetime version (SCQ [74]) The total raw scorefrom the SCQ was used All measures described aboveare psychometrically sound assessments used frequentlyin individuals with DS See Edgin et al [67] for more de-tailed informationDemographic information on participant age sex self-
identified race and ethnicity presence of a congenitalheart defect household income and maternal and pater-nal age were obtained via caregiver report and medicalrecord abstraction (Table 1)
Table 1 Demographic characteristics of the overall sample and latent classes
Overall Sample ldquoNormativerdquo class ldquoCognitiverdquo class ldquoBehavioralrdquo class
N () 314 (100) 153 (487) 109 (347) 52 (166)
Age (M SD) 137 (47) 136 (45) 135 (47) 146 (51)
Maternal age (M SD) 348 (55) 354 (53) 343 (62) 342 (45)
Paternal age (M SD) 364 (57) 370 (55) 357 (61) 359 (53)
Household income ()
lt$75000 287 223 349 314
$75000ndash$100000 155 144 170 157
$100000+ 558 623 481 529
Sex ( male) 510 569 404 558
Self-identified raceethnicity ()
White 752 808 676 750
Black 64 66 83 19
Hispanic 32 13 65 19
Asian 145 113 167 192
Other 6 0 1 19
Congenital heart defect ( yes) 610 656 544 608
Assessment scores (M SD)
KBIT-2 252 (117) 300 (108) 163 (85) 299 (90)
CANTAB spatial span 27 (16) 33 (12) 14 (16) 29 (14)
NEPSY-II visuomotor precision 133 (57) 142 (56) 115 (60) 144 (51)
BRIEF 135 (233) 1227 (193) 1442 (195) 1543 (202)
SIB-R 579 (233) 704 (196) 393 (182) 583 (167)
NCBRF conduct problems 75 (61) 51 (41) 75 (53) 148 (66)
NCBRF insecureanxious 40 (40) 27 (25) 29 (25) 100 (47)
NCBRF hyperactivity 65 (44) 45 (32) 77 (42) 101 (47)
SCQ 86 (55) 52 (32) 125 (49) 118 (55)
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF GEC Behavioral Rating Inventory ofExecutive Function SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication Questionnaire
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 5 of 14
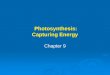
Statistical analysisThe first step in the analysis was to place all of the vari-ables on a common metric because many of the vari-ables were based on raw scores If items did not havesimilar scaling the LPA would be uninterpretable Toaccomplish this all variables were transformed using aZ-score conversion which placed all scores on a metricof Mean = 0 (reflecting the overall sample average) andSD = 1 Thus Z-score values can be interpreted in termsof standard deviations For instance a 1-point SD differ-ence is equivalent to a 682 difference between groupsThis is interpreted as a large effect size whereas a 05SD (341 difference) represents a moderate effect sizeDuring the transformation all variables including stand-ard scores were adjusted for age All variables retainedtheir original direction of measurement such that higherscores on the NCBRF SCQ and BRIEF indicated greaterimpairment and higher scores on the performance-based measures and SIB-R reflected less impairmentstronger performance See Fig 1 for visual representa-tion of each age-corrected Z-score transformed variableNext the age-corrected Z-score transformed variables
were submitted to an LPA LPA was used to identifyhomogeneous latent subgroups of individuals with DSbased on continuous indicators of cognition behaviorand development [75] Using a series of fit statistics thefirst step in this procedure is to identify how many sub-groups (hereafter referred to as ldquoclassesrdquo) existed in thesample The most commonly known fit statistics used inthis study were the Akaike (AIC) and sample size-adjusted Bayesian (SS-BIC) information criterionsLower AIC and SS-BIC values indicate a model that fitsthe data best [76] Next Vuong-Lo-Mendell-Rubin
(VLMR) and bootstrapped likelihood ratio (BLRT) testswere employed These tests iteratively examined thecurrent model compared to the previous model with oneless class When p gt 05 it suggests that the currentmodel does not fit significantly better than the K-1model [75] Additional metrics included entropy andmean class probability (M[CP]) both of which indicatemisclassification Higher scores on both metrics are bestwith a value of 1 being perfect measurement Prior workby Nylund et al [77] suggests that the BIC and BLRTare more reliable indices of class structure than the AICand VLMR respectivelyAfter arriving at the optimal class structure individual
membership to the model was exported Each individualwas assigned to a class by the software based on the classthat represented their greatest posterior probability ofmembership Finally a multivariate multinomial regres-sion model simultaneously examined all demographic cor-relates of class Only paternal age was excluded because itwas strongly associated with maternal age (r = 71) Self-identified raceethnicity was dichotomized (White vsother) because there were small sample sizes for non-White categories The multinomial model included robustvariance to address any unknown clustering or model mis-specification LPA analyses were performed in MPLUSVersion 70 [78] and all other data management and ana-lysis occurred in STATA 150 [79]Three variables used in the LPA measurement model
had substantial missingness (SIB-R 7 missing CANTAB 21 SCQ 23) MPLUS uses full information max-imum likelihood estimation (FIML) to accommodatemissing data in structural equation-based models FIMLproduces unbiased estimates and standard errors when
Table 2 Description of primary measures
Domain of assessment Measure Outcome variablea Interpretation of score
Performance-based assessments of cognition
Verbal + nonverbal intelligence KBIT-2 Raw score composite Higher score = more skills
Working memory (immediate memory forspatial-temporal sequences)
CANTAB Spatial Span Forward span length Higher score = more skills
Visuomotor scanning and hand-eyecoordination
NEPSY-II VisuomotorPrecision ages 3ndash4
Total score (time and number of errors) Higher score = more skills
Caregiver-informed assessments of cognition and behavior
Executive functioning BRIEF School Age Global Executive Composite standard score Higher score = moreimpairments
Adaptive SIB-R Short Form Standard score composite Higher score = moreadaptive skills
Maladaptive NCBRF Conduct problems insecureanxious andhyperactivity subscale raw scores
Higher score = moremaladaptive behaviors
Autism spectrum disorder (ASD)symptomatology
SCQ-Lifetime Total raw score Higher score = more ASD-like symptoms
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF Behavioral Rating Inventory of ExecutiveFunction SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication QuestionnaireaAll outcome variables were age-corrected
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 6 of 14
data are missing either at random or completely at ran-dom [80] To understand the influence of FIML theLPA was run on the sample using complete case ana-lysis which severely limited the sample size (n = 156)Importantly the findings supported the same inferencesas the model that included the entire sample via FIMLin terms of class structure and fit statistics Given thisfinding and the fact that complete case analysis has itsknown biases the full sample was employed in the LPAand regression analyses using FIML
ResultsLPAFit statistics for the iterative LPA procedure are shownin Table 3 Determining the number of classes to includein the model depends on assessing the various fit statis-tics as well as considering class size and interpretationWe examined 2- through 4-class models Table 3 showsthat the AIC and SS-BIC values decreased continuouslywith increasing class size indicating a better fit with
increasing number of classes as expected The decreasein these scores was considerably larger between the 2-and 3-class models compared to the 3- to 4-classmodels This pattern provides evidence of at least a 3-class model Entropy and M(CP) were high and fairlyconsistent across the models The VLMR suggested a 2-class model as the 3-class model did not significantlyimprove the model fit However the BLRT remained sig-nificant at p lt 001 with the 4-class model suggestingmore than four classes may be indicated A fifth classwas not evaluated due to the small class size in the 4-class modelOverall three indices (AIC BIC BLRT) provided evi-
dence for more than two classes whereas the VLMRsuggested a 2-class solution Prior work by Nylund et al[77] has shown BIC and BLRT as two of the most reli-able fit indices both of which supported a larger numberof classes in this dataset Given that the fit statistics gen-erally supported more than two classes and the 2-classsolution did not reflect important heterogeneity detected
Fig 1 Distribution of age-corrected Z-score transformed measures used in the latent profile analysis Note NCBRF Nisonger Child Behavior RatingForm Hyp hyperactivity BRIEF Behavioral Rating Inventory of Executive Function EF executive functioning SCQ Social Communication Questionnaire-Lifetime ASD autism spectrum disorder SIB-R Scales of Independent Behavior-Revised AB adaptive behavior VMP visuomotor precision CANTABCambridge Neuropsychological Test Automated Battery SS spatial span KBIT Kaufman Brief Intelligence Test 2nd edition IQ verbal and nonverbal rawscore sum (averaged)
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 7 of 14
in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

Down syndrome (DS) is the most common chromo-somal disorder among births and is the leading geneticcause of intellectual disability [1] Individuals with DShave an extra copy of chromosome 21 in all or some oftheir cells This genetic difference results in a phenotypethat increases the likelihood of certain medical condi-tions (eg congenital heart disease sleep apnea [2]) andcognitive and behavioral characteristics [3] These char-acteristics include lower than average IQ and reducedadaptive functioning both of which are associated withintellectual disability in general [4] However DS also re-sults in phenotype-specific characteristics (eg relativedifficulties in verbal processing relative strengths in so-cial functioning [3]) that distinguish it from other neuro-genetic disorders associated with intellectual disabilityThese phenotype-specific features are due to the in-creased dosage of chromosome 21 genes and resultingdysregulation genome-widePerhaps most striking is the high degree of variability ob-
served among individuals with DS regarding the presenceand severity of associated symptoms and conditions Thisvariability is likely due to a combination of genetic and envir-onmental risk factors that alter the expression of many as-pects of the DS phenotype including cognition behaviorand health across the lifespan [5] However the nature ofthis variability in DS is still not well understood complicatingintervention and treatment decisions We hypothesize thatwithin-syndrome variability can be characterized systematic-ally through the identification of subgroups based on cogni-tive and behavioral profiles Thus the current study takes anindividual-differences approach to identify within-group pro-files of cognition and behavior among individuals with DSacross a wide age range (6ndash25 years) using latent profile ana-lysis (LPA) The identification of more homogeneous sub-types of individuals with DS may help increase the ability todiscover associated genetic and environmental risk factors ofseverity Clinically the resulting data will emphasize differentpatterns of strengths and areas in need of additional supportamong individuals with DS Ultimately more precision incharacterization of the individual variability within DS willlead to more targeted treatment and intervention approachesto optimize daily function for this population In the currentstudy we focused on the domains of cognition (IQ and ex-ecutive functioning) adaptive and maladaptive behavior andautism spectrum disorder (ASD) symptomatology
Challenges to the assessment of the cognitive andbehavioral phenotype of DSCognitionResearch on cognition in DS has focused broadly on IQand executive functioning IQ represents overall cogni-tive ability and is thought to broadly impact other areasof functioning (eg adaptive behavior maladaptive be-havior) Another particularly important area of cognition
is executive functioning which encompasses the higher-order cognitive and self-regulatory abilities that are im-portant for goal-directed behavior and daily functioning(eg social interactions academic achievement work be-havior [6ndash10]) The abilities housed under the umbrellaterm of executive functioning include working memoryinhibition shiftingcognitive flexibility attention andplanning Both IQ and executive functioning are import-ant components of the DS phenotype while also show-ing inter-individual variability [11]
IQIQ is perhaps one of the more variable constructs amongindividuals with DS ranging from approximately 40 (orthe lowest score possible on many standardizedintelligence tests) to around 70 (the cutoff score for intel-lectual disability) and in some cases even higher [12]There are two main issues associated with interpreting IQscores in individuals with DS use of age-based norms andscoring at the floor (ie the lowest score possible [13 14])Like others with intellectual disability the rate of
growth in cognitive skills is slower for individuals withDS than in the general population Therefore the use ofage-based norms (ie IQ standard scores) from the gen-eral population leads to a discrepancy that becomes lar-ger with age This discrepancy causes IQ standard scoresto decrease or at least not increase over time despitecontinued growth in cognitive skills [12 15ndash17]Using age-based norms can also lead to many individ-
uals with DS and intellectual disability scoring at thefloor To address this problem some research groupshave developed Z-score-based deviation IQ scores thataccount for performance below the floor-level standardscore (Hessl et al [18] for the Wechsler IntelligenceScale for Children-III Sansone et al [13] for the Stan-ford Binet-5) Another solution to the floor effect prob-lem is to use raw scores or growth scores that representperformance on a standardized IQ test without takinginto account age-based norms [16] This approach is es-pecially useful for interpreting growth over time For ex-ample a review of longitudinal studies using theStanford Binet IV to assess individuals with DS from age4 to 24 years found that 37 scored at the floor leveland thus growth could not be examined with standardscores [12] Raw scores however increased over timeThe rate of growth over time measured using ageequivalent scores was non-linear and highly variableacross individuals Interpretation of these results is lim-ited due to their use of age equivalent scores which donot provide accurate estimates of ability level and havepoor psychometric properties [19] However these re-sults do highlight the high degree of variation associatedwith the DS phenotype The current study takes into ac-count this variation by examining age-corrected raw
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 2 of 14
scores from another IQ measure the Kaufman BriefIntelligence Test 2nd edition (KBIT-2 [20]) in the pro-file analyses
Executive functioningExecutive functioning is an area in which many individ-uals with DS struggle compared to both chronologicaland mental age-matched peers [3 21] Within executivefunctioning the areas of working memory planning andinhibition are particularly difficult for individuals withDS emotional control is considered a relative strength[22 23] Although this pattern appears to be relativelyconsistent across development Loveall et al [23] notedsome nuanced differences in the executive functioningprofile in childhood and adulthoodWorking memory is the component that has been ex-
amined in greater depth across the literature on DS thanother abilities under the executive functioning umbrellaDefined as the simultaneous storing and manipulationprocessing of information [24 25] working memory oftenhas been characterized as an area of weakness for individ-uals with DS with greater difficulties reported in verbalworking memory than visuospatial working memory [2627] Verbal working memory appears to be weak com-pared to both mental age-matched typically developingchildren [28 29] and individuals with other intellectualand developmental disabilities [30ndash33] it also develops ata slower rate in individuals with DS than in peers withother intellectual and developmental disabilities [34]Although historically visuospatial working memory
has been thought to be intact in the DS phenotype [26]recent research suggests variability in performanceamong individuals with DS across different visuospatialworking memory tasks [35] Collectively the literaturepoints to impairments in the spatial-simultaneous [36ndash38] and visual [39 40] components with the spatial-sequential component relatively intact [41]
Adaptive behaviorAdaptive behavior involves the skills needed to functionindependently in everyday life such as self-care domes-tic function and community interactions [4 42 43]These skills are critical to positive long-term outcomesincluding academic success and independence [44ndash47]Research on adaptive behavior generally categorizes as-sociated skills into four broad domains socializationcommunication daily living and motor skillsIndividuals with DS demonstrate relative strengths in
socialization and difficulties in communication andmotor skills [48ndash51] As for daily living the research ismixed on whether this is an area of strength or difficulty[47 49] However Daunhauer [47] analyzed within-group effect sizes for previously conducted adaptive be-havior studies and noted that daily living skills may
actually be an area of relative difficulty due to its overlapwith other adaptive domains For example being able todress oneself is a daily living skill but this can be diffi-cult if an individual has compromised motor skills Re-gardless adaptive behavior is holistically an area ofdifficulty for individuals with DS again with consider-able inter-individual variabilityOne of the challenges to understanding adaptive be-
havior within the DS phenotype is that it is often exam-ined separately from other aspects of the phenotypeHowever it is important to recognize that onersquos abilityto function independently is likely intertwined withother aspects of cognition and behavior For exampleboth executive functioning and IQ are strongly associ-ated with level of adaptive functioning [21 22] and maybe related to the presence of maladaptive behaviors [4752] The present study is specifically designed to investi-gate within-group profiles of adaptive behavior relativeto IQ and executive functioning rather than simplycomparing sample means across these constructs
Maladaptive behaviorsIn contrast to adaptive behavior maladaptive behaviorsrepresent a range of behaviors that impede health well-being educational and occupational outcomes and dailyfunctioning These behaviors are traditionally catego-rized as internalizing (eg anxious or depressed symp-toms) or externalizing (eg inattentionhyperactivityaggressive behaviors) Higher levels of maladaptive be-haviors have been noted in individuals with DS who alsohave identified comorbid neurobehavioral disorders (egASD disruptive behavior disorder [53ndash56])Children and adolescents with DS have higher rates of
maladaptive behaviors than the general population [57ndash59] However the within-DS profile of maladaptive be-haviors appears nuanced For example population-basedstudies of Dutch individuals with DS showed high ratesof problems in the ldquosocialrdquo and ldquoinattentionrdquo domains onthe Child Behavior Checklist but relatively low rates ofinternalizing problems in the ldquoanxious-depressedrdquo do-main [58 59] Although scores in the ldquodelinquent behav-iorrdquo and ldquoaggressive behaviorrdquo domains were slightlyelevated in the child cohort the effect size was smallsuggesting a nuanced difference at best [58] A develop-mental pattern also emerged such that more difficultieswith ldquoanxious-depressedrdquo symptoms were found in theadolescent group than in younger children This patternis consistent with other within-syndrome reports as wellas the broader literature on internalizing behaviors inadolescents [57 60] One aspect that remains unclear ishow maladaptive behaviors relate to cognition Thecurrent study directly addresses this gap by using clusterprofiles to examine these associations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 3 of 14
Comorbid autism spectrum disorder (ASD) in DSIndividuals with DS are at a greater risk of comorbid ASDthan the general population with prevalence estimates sug-gesting up to 19 [61] Notably comorbid ASD tends to im-pact both cognitive and behavioral aspects of the DSphenotype Compared to individuals with DS who do nothave comorbid ASD individuals with DS and comorbidASD tend to display more maladaptive behaviors (ie stereo-typic and anxiouswithdrawn domains [53 55]) and lowerIQ and adaptive functioning [61 62] Additionally studiesexamining broader ASD-like symptomatology among indi-viduals with DS who are at low risk for comorbid ASD havefound a similar pattern lower IQ and adaptive functioningand higher rates of maladaptive behaviors are associated withbroader ASD-like symptoms [63ndash65] Therefore it appearsthat there is some overlap between ASD-like symptoms andthe behavioral phenotype associated with DS However it isunclear if the use of group-level means obscures a more nu-anced profile of cognition and adaptive behavior in relationto ASD symptomatology in DS similar to what is observedin non-syndromic ASD [66]
Current studyThe literature on cognition (IQ and executive function-ing) adaptive and maladaptive behaviors and ASDsymptomatology associated with the DS phenotype indi-cates a general syndrome-specific pattern however asreviewed above it also indicates significant variabilityThus we hypothesize that the general syndrome-specificpattern does not represent all individuals with DS andthat within-group profiles can be identified More nu-anced within-group profiles may vary by age becausegeneral developmental differences within the syndrome-specific pattern of strengths and weakness have beennoted in the literature Thus we also hypothesize thatage is associated with within-group profilesUsing LPA as an exploratory approach we aimed to test
our hypotheses by (1) determining whether subgroups of in-dividuals with DS can be characterized using performance-based and caregiver-informed ratings of behavior and cogni-tion and (2) examining the demographic characteristics asso-ciated with the latent subgroups To achieve these aims westudied a large sample of individuals with DS ages 6ndash25years who were recruited through a network of sites acrossthe USA called the Down Syndrome Cognition Project (seeRosser et al [14])
MethodsParticipantsThree hundred fifty-six individuals with DS ages 6ndash25years old participated in the larger study the Down Syn-drome Cognition Project (see Rosser et al [14] for inclu-sion criteria and participation rates) Using that samplewe retained all members of the original cohort except
for participants who were missing data on three or moreof the primary measures (n = 42) resulting in a finalsample size of 314 Participants were recruited fromclinics community eventssupport groups conferencesadvertisements and previous research studies by mul-tiple sites across the USA See Table 1 for participantdemographic information
Measures and procedureThe Down Syndrome Cognition Project testing battery [14]included a series of performance-based neuropsychologicalassessments modified from the Arizona Cognitive Test Bat-tery which was developed to produce outcome measures forclinical trials involving individuals with DS [67 68] The testbattery has good test-retest reliability [67]Examiners at each Down Syndrome Cognition Project
site were trained to fidelity to administer the testing bat-tery to individuals with DS (see Edgin et al [67 68])Sites were monitored by the University of Arizona train-ing site andor the Emory Data Coordinating CenterPeriodic quality control checks included review of fidel-ity to administration and scoring procedures All datawere double entered with comparison checks to ensureaccuracy Research Electronic Data Capture (REDCap[69]) was used for data entry and managementParticipants completed the testing battery at an assess-
ment site or another convenient location (eg commu-nity center or family home) The entire session lastedabout 2ndash3 h with frequent breaks Tests were presentedin two fixed counterbalanced orders [67] Caregiverscompleted questionnaires related to participant demo-graphics medicaldevelopmental history and behaviorsTable 2 includes a description of the primary measures in-
cluded in the model These tests were selected based on sev-eral criteria Most importantly each measure was selected onthe basis of reflecting an important and unique componentof cognition behavior or development Where possible weused total composite or summary scores from the indicatedmeasure to capture all salient information and reduce thenumber of overall variables Variables were also selectedbased on normality Variables that were highly skewed dueto floor or ceiling effects limited the ability to measure thefull range of abilities and discriminate among subgroups andthus were eliminated from the analyses Finally measureswere also selected based on number of observations becausenot all measures were administered to the entire cohort
Performance-based assessments of cognitionThree performance-based tests of cognition were in-cluded in this study Intelligence was evaluated using theKaufman Brief Intelligence Test 2nd edition (KBIT-2[20]) Verbal and nonverbal raw scores were summedand then averaged for use in the model This approachwas taken because the IQ composite variable had
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 4 of 14
significant floor effects (34 of the sample had an IQle40) Working memory was evaluated using the Cam-bridge Neuropsychological Test Automated Battery(CANTAB) Spatial Span test which required the partici-pant to recall progressively longer sequences of visual in-formation (colored squares) presented on a touchscreenVisuomotor tracking and hand-eye coordination wereevaluated using the NEPSY-II Visuomotor PrecisionTask (ages 3ndash4) For this task the participant used theirpreferred hand to draw a line as quickly as possiblewhile staying inside the tracked lines [70]
Caregiver-informed measuresFour caregiver-report measures of cognition and behav-ior were included Executive functioning impairmentswere assessed via the Global Executive Composite stand-ard score from the Behavioral Rating Inventory of Ex-ecutive Function School Age (BRIEF [71]) Adaptivebehavior was evaluated using the standard composite
score of the Scales of Independent Behavior-RevisedShort Form (SIB-R [72]) Maladaptive behavior wasassessed across three variables (conduct problems anx-iety and hyperactivity) from the Nisonger Child Behav-ior Rating Form (NCBRF [73]) These subscales wereselected because the additional subscales overlappedwith the other measures employed in this study (egASD symptoms adaptive behavior) ASD symptomswere assessed via the Social Communication Question-naire Lifetime version (SCQ [74]) The total raw scorefrom the SCQ was used All measures described aboveare psychometrically sound assessments used frequentlyin individuals with DS See Edgin et al [67] for more de-tailed informationDemographic information on participant age sex self-
identified race and ethnicity presence of a congenitalheart defect household income and maternal and pater-nal age were obtained via caregiver report and medicalrecord abstraction (Table 1)
Table 1 Demographic characteristics of the overall sample and latent classes
Overall Sample ldquoNormativerdquo class ldquoCognitiverdquo class ldquoBehavioralrdquo class
N () 314 (100) 153 (487) 109 (347) 52 (166)
Age (M SD) 137 (47) 136 (45) 135 (47) 146 (51)
Maternal age (M SD) 348 (55) 354 (53) 343 (62) 342 (45)
Paternal age (M SD) 364 (57) 370 (55) 357 (61) 359 (53)
Household income ()
lt$75000 287 223 349 314
$75000ndash$100000 155 144 170 157
$100000+ 558 623 481 529
Sex ( male) 510 569 404 558
Self-identified raceethnicity ()
White 752 808 676 750
Black 64 66 83 19
Hispanic 32 13 65 19
Asian 145 113 167 192
Other 6 0 1 19
Congenital heart defect ( yes) 610 656 544 608
Assessment scores (M SD)
KBIT-2 252 (117) 300 (108) 163 (85) 299 (90)
CANTAB spatial span 27 (16) 33 (12) 14 (16) 29 (14)
NEPSY-II visuomotor precision 133 (57) 142 (56) 115 (60) 144 (51)
BRIEF 135 (233) 1227 (193) 1442 (195) 1543 (202)
SIB-R 579 (233) 704 (196) 393 (182) 583 (167)
NCBRF conduct problems 75 (61) 51 (41) 75 (53) 148 (66)
NCBRF insecureanxious 40 (40) 27 (25) 29 (25) 100 (47)
NCBRF hyperactivity 65 (44) 45 (32) 77 (42) 101 (47)
SCQ 86 (55) 52 (32) 125 (49) 118 (55)
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF GEC Behavioral Rating Inventory ofExecutive Function SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication Questionnaire
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 5 of 14
Statistical analysisThe first step in the analysis was to place all of the vari-ables on a common metric because many of the vari-ables were based on raw scores If items did not havesimilar scaling the LPA would be uninterpretable Toaccomplish this all variables were transformed using aZ-score conversion which placed all scores on a metricof Mean = 0 (reflecting the overall sample average) andSD = 1 Thus Z-score values can be interpreted in termsof standard deviations For instance a 1-point SD differ-ence is equivalent to a 682 difference between groupsThis is interpreted as a large effect size whereas a 05SD (341 difference) represents a moderate effect sizeDuring the transformation all variables including stand-ard scores were adjusted for age All variables retainedtheir original direction of measurement such that higherscores on the NCBRF SCQ and BRIEF indicated greaterimpairment and higher scores on the performance-based measures and SIB-R reflected less impairmentstronger performance See Fig 1 for visual representa-tion of each age-corrected Z-score transformed variableNext the age-corrected Z-score transformed variables
were submitted to an LPA LPA was used to identifyhomogeneous latent subgroups of individuals with DSbased on continuous indicators of cognition behaviorand development [75] Using a series of fit statistics thefirst step in this procedure is to identify how many sub-groups (hereafter referred to as ldquoclassesrdquo) existed in thesample The most commonly known fit statistics used inthis study were the Akaike (AIC) and sample size-adjusted Bayesian (SS-BIC) information criterionsLower AIC and SS-BIC values indicate a model that fitsthe data best [76] Next Vuong-Lo-Mendell-Rubin
(VLMR) and bootstrapped likelihood ratio (BLRT) testswere employed These tests iteratively examined thecurrent model compared to the previous model with oneless class When p gt 05 it suggests that the currentmodel does not fit significantly better than the K-1model [75] Additional metrics included entropy andmean class probability (M[CP]) both of which indicatemisclassification Higher scores on both metrics are bestwith a value of 1 being perfect measurement Prior workby Nylund et al [77] suggests that the BIC and BLRTare more reliable indices of class structure than the AICand VLMR respectivelyAfter arriving at the optimal class structure individual
membership to the model was exported Each individualwas assigned to a class by the software based on the classthat represented their greatest posterior probability ofmembership Finally a multivariate multinomial regres-sion model simultaneously examined all demographic cor-relates of class Only paternal age was excluded because itwas strongly associated with maternal age (r = 71) Self-identified raceethnicity was dichotomized (White vsother) because there were small sample sizes for non-White categories The multinomial model included robustvariance to address any unknown clustering or model mis-specification LPA analyses were performed in MPLUSVersion 70 [78] and all other data management and ana-lysis occurred in STATA 150 [79]Three variables used in the LPA measurement model
had substantial missingness (SIB-R 7 missing CANTAB 21 SCQ 23) MPLUS uses full information max-imum likelihood estimation (FIML) to accommodatemissing data in structural equation-based models FIMLproduces unbiased estimates and standard errors when
Table 2 Description of primary measures
Domain of assessment Measure Outcome variablea Interpretation of score
Performance-based assessments of cognition
Verbal + nonverbal intelligence KBIT-2 Raw score composite Higher score = more skills
Working memory (immediate memory forspatial-temporal sequences)
CANTAB Spatial Span Forward span length Higher score = more skills
Visuomotor scanning and hand-eyecoordination
NEPSY-II VisuomotorPrecision ages 3ndash4
Total score (time and number of errors) Higher score = more skills
Caregiver-informed assessments of cognition and behavior
Executive functioning BRIEF School Age Global Executive Composite standard score Higher score = moreimpairments
Adaptive SIB-R Short Form Standard score composite Higher score = moreadaptive skills
Maladaptive NCBRF Conduct problems insecureanxious andhyperactivity subscale raw scores
Higher score = moremaladaptive behaviors
Autism spectrum disorder (ASD)symptomatology
SCQ-Lifetime Total raw score Higher score = more ASD-like symptoms
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF Behavioral Rating Inventory of ExecutiveFunction SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication QuestionnaireaAll outcome variables were age-corrected
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 6 of 14
data are missing either at random or completely at ran-dom [80] To understand the influence of FIML theLPA was run on the sample using complete case ana-lysis which severely limited the sample size (n = 156)Importantly the findings supported the same inferencesas the model that included the entire sample via FIMLin terms of class structure and fit statistics Given thisfinding and the fact that complete case analysis has itsknown biases the full sample was employed in the LPAand regression analyses using FIML
ResultsLPAFit statistics for the iterative LPA procedure are shownin Table 3 Determining the number of classes to includein the model depends on assessing the various fit statis-tics as well as considering class size and interpretationWe examined 2- through 4-class models Table 3 showsthat the AIC and SS-BIC values decreased continuouslywith increasing class size indicating a better fit with
increasing number of classes as expected The decreasein these scores was considerably larger between the 2-and 3-class models compared to the 3- to 4-classmodels This pattern provides evidence of at least a 3-class model Entropy and M(CP) were high and fairlyconsistent across the models The VLMR suggested a 2-class model as the 3-class model did not significantlyimprove the model fit However the BLRT remained sig-nificant at p lt 001 with the 4-class model suggestingmore than four classes may be indicated A fifth classwas not evaluated due to the small class size in the 4-class modelOverall three indices (AIC BIC BLRT) provided evi-
dence for more than two classes whereas the VLMRsuggested a 2-class solution Prior work by Nylund et al[77] has shown BIC and BLRT as two of the most reli-able fit indices both of which supported a larger numberof classes in this dataset Given that the fit statistics gen-erally supported more than two classes and the 2-classsolution did not reflect important heterogeneity detected
Fig 1 Distribution of age-corrected Z-score transformed measures used in the latent profile analysis Note NCBRF Nisonger Child Behavior RatingForm Hyp hyperactivity BRIEF Behavioral Rating Inventory of Executive Function EF executive functioning SCQ Social Communication Questionnaire-Lifetime ASD autism spectrum disorder SIB-R Scales of Independent Behavior-Revised AB adaptive behavior VMP visuomotor precision CANTABCambridge Neuropsychological Test Automated Battery SS spatial span KBIT Kaufman Brief Intelligence Test 2nd edition IQ verbal and nonverbal rawscore sum (averaged)
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 7 of 14
in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

scores from another IQ measure the Kaufman BriefIntelligence Test 2nd edition (KBIT-2 [20]) in the pro-file analyses
Executive functioningExecutive functioning is an area in which many individ-uals with DS struggle compared to both chronologicaland mental age-matched peers [3 21] Within executivefunctioning the areas of working memory planning andinhibition are particularly difficult for individuals withDS emotional control is considered a relative strength[22 23] Although this pattern appears to be relativelyconsistent across development Loveall et al [23] notedsome nuanced differences in the executive functioningprofile in childhood and adulthoodWorking memory is the component that has been ex-
amined in greater depth across the literature on DS thanother abilities under the executive functioning umbrellaDefined as the simultaneous storing and manipulationprocessing of information [24 25] working memory oftenhas been characterized as an area of weakness for individ-uals with DS with greater difficulties reported in verbalworking memory than visuospatial working memory [2627] Verbal working memory appears to be weak com-pared to both mental age-matched typically developingchildren [28 29] and individuals with other intellectualand developmental disabilities [30ndash33] it also develops ata slower rate in individuals with DS than in peers withother intellectual and developmental disabilities [34]Although historically visuospatial working memory
has been thought to be intact in the DS phenotype [26]recent research suggests variability in performanceamong individuals with DS across different visuospatialworking memory tasks [35] Collectively the literaturepoints to impairments in the spatial-simultaneous [36ndash38] and visual [39 40] components with the spatial-sequential component relatively intact [41]
Adaptive behaviorAdaptive behavior involves the skills needed to functionindependently in everyday life such as self-care domes-tic function and community interactions [4 42 43]These skills are critical to positive long-term outcomesincluding academic success and independence [44ndash47]Research on adaptive behavior generally categorizes as-sociated skills into four broad domains socializationcommunication daily living and motor skillsIndividuals with DS demonstrate relative strengths in
socialization and difficulties in communication andmotor skills [48ndash51] As for daily living the research ismixed on whether this is an area of strength or difficulty[47 49] However Daunhauer [47] analyzed within-group effect sizes for previously conducted adaptive be-havior studies and noted that daily living skills may
actually be an area of relative difficulty due to its overlapwith other adaptive domains For example being able todress oneself is a daily living skill but this can be diffi-cult if an individual has compromised motor skills Re-gardless adaptive behavior is holistically an area ofdifficulty for individuals with DS again with consider-able inter-individual variabilityOne of the challenges to understanding adaptive be-
havior within the DS phenotype is that it is often exam-ined separately from other aspects of the phenotypeHowever it is important to recognize that onersquos abilityto function independently is likely intertwined withother aspects of cognition and behavior For exampleboth executive functioning and IQ are strongly associ-ated with level of adaptive functioning [21 22] and maybe related to the presence of maladaptive behaviors [4752] The present study is specifically designed to investi-gate within-group profiles of adaptive behavior relativeto IQ and executive functioning rather than simplycomparing sample means across these constructs
Maladaptive behaviorsIn contrast to adaptive behavior maladaptive behaviorsrepresent a range of behaviors that impede health well-being educational and occupational outcomes and dailyfunctioning These behaviors are traditionally catego-rized as internalizing (eg anxious or depressed symp-toms) or externalizing (eg inattentionhyperactivityaggressive behaviors) Higher levels of maladaptive be-haviors have been noted in individuals with DS who alsohave identified comorbid neurobehavioral disorders (egASD disruptive behavior disorder [53ndash56])Children and adolescents with DS have higher rates of
maladaptive behaviors than the general population [57ndash59] However the within-DS profile of maladaptive be-haviors appears nuanced For example population-basedstudies of Dutch individuals with DS showed high ratesof problems in the ldquosocialrdquo and ldquoinattentionrdquo domains onthe Child Behavior Checklist but relatively low rates ofinternalizing problems in the ldquoanxious-depressedrdquo do-main [58 59] Although scores in the ldquodelinquent behav-iorrdquo and ldquoaggressive behaviorrdquo domains were slightlyelevated in the child cohort the effect size was smallsuggesting a nuanced difference at best [58] A develop-mental pattern also emerged such that more difficultieswith ldquoanxious-depressedrdquo symptoms were found in theadolescent group than in younger children This patternis consistent with other within-syndrome reports as wellas the broader literature on internalizing behaviors inadolescents [57 60] One aspect that remains unclear ishow maladaptive behaviors relate to cognition Thecurrent study directly addresses this gap by using clusterprofiles to examine these associations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 3 of 14
Comorbid autism spectrum disorder (ASD) in DSIndividuals with DS are at a greater risk of comorbid ASDthan the general population with prevalence estimates sug-gesting up to 19 [61] Notably comorbid ASD tends to im-pact both cognitive and behavioral aspects of the DSphenotype Compared to individuals with DS who do nothave comorbid ASD individuals with DS and comorbidASD tend to display more maladaptive behaviors (ie stereo-typic and anxiouswithdrawn domains [53 55]) and lowerIQ and adaptive functioning [61 62] Additionally studiesexamining broader ASD-like symptomatology among indi-viduals with DS who are at low risk for comorbid ASD havefound a similar pattern lower IQ and adaptive functioningand higher rates of maladaptive behaviors are associated withbroader ASD-like symptoms [63ndash65] Therefore it appearsthat there is some overlap between ASD-like symptoms andthe behavioral phenotype associated with DS However it isunclear if the use of group-level means obscures a more nu-anced profile of cognition and adaptive behavior in relationto ASD symptomatology in DS similar to what is observedin non-syndromic ASD [66]
Current studyThe literature on cognition (IQ and executive function-ing) adaptive and maladaptive behaviors and ASDsymptomatology associated with the DS phenotype indi-cates a general syndrome-specific pattern however asreviewed above it also indicates significant variabilityThus we hypothesize that the general syndrome-specificpattern does not represent all individuals with DS andthat within-group profiles can be identified More nu-anced within-group profiles may vary by age becausegeneral developmental differences within the syndrome-specific pattern of strengths and weakness have beennoted in the literature Thus we also hypothesize thatage is associated with within-group profilesUsing LPA as an exploratory approach we aimed to test
our hypotheses by (1) determining whether subgroups of in-dividuals with DS can be characterized using performance-based and caregiver-informed ratings of behavior and cogni-tion and (2) examining the demographic characteristics asso-ciated with the latent subgroups To achieve these aims westudied a large sample of individuals with DS ages 6ndash25years who were recruited through a network of sites acrossthe USA called the Down Syndrome Cognition Project (seeRosser et al [14])
MethodsParticipantsThree hundred fifty-six individuals with DS ages 6ndash25years old participated in the larger study the Down Syn-drome Cognition Project (see Rosser et al [14] for inclu-sion criteria and participation rates) Using that samplewe retained all members of the original cohort except
for participants who were missing data on three or moreof the primary measures (n = 42) resulting in a finalsample size of 314 Participants were recruited fromclinics community eventssupport groups conferencesadvertisements and previous research studies by mul-tiple sites across the USA See Table 1 for participantdemographic information
Measures and procedureThe Down Syndrome Cognition Project testing battery [14]included a series of performance-based neuropsychologicalassessments modified from the Arizona Cognitive Test Bat-tery which was developed to produce outcome measures forclinical trials involving individuals with DS [67 68] The testbattery has good test-retest reliability [67]Examiners at each Down Syndrome Cognition Project
site were trained to fidelity to administer the testing bat-tery to individuals with DS (see Edgin et al [67 68])Sites were monitored by the University of Arizona train-ing site andor the Emory Data Coordinating CenterPeriodic quality control checks included review of fidel-ity to administration and scoring procedures All datawere double entered with comparison checks to ensureaccuracy Research Electronic Data Capture (REDCap[69]) was used for data entry and managementParticipants completed the testing battery at an assess-
ment site or another convenient location (eg commu-nity center or family home) The entire session lastedabout 2ndash3 h with frequent breaks Tests were presentedin two fixed counterbalanced orders [67] Caregiverscompleted questionnaires related to participant demo-graphics medicaldevelopmental history and behaviorsTable 2 includes a description of the primary measures in-
cluded in the model These tests were selected based on sev-eral criteria Most importantly each measure was selected onthe basis of reflecting an important and unique componentof cognition behavior or development Where possible weused total composite or summary scores from the indicatedmeasure to capture all salient information and reduce thenumber of overall variables Variables were also selectedbased on normality Variables that were highly skewed dueto floor or ceiling effects limited the ability to measure thefull range of abilities and discriminate among subgroups andthus were eliminated from the analyses Finally measureswere also selected based on number of observations becausenot all measures were administered to the entire cohort
Performance-based assessments of cognitionThree performance-based tests of cognition were in-cluded in this study Intelligence was evaluated using theKaufman Brief Intelligence Test 2nd edition (KBIT-2[20]) Verbal and nonverbal raw scores were summedand then averaged for use in the model This approachwas taken because the IQ composite variable had
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 4 of 14
significant floor effects (34 of the sample had an IQle40) Working memory was evaluated using the Cam-bridge Neuropsychological Test Automated Battery(CANTAB) Spatial Span test which required the partici-pant to recall progressively longer sequences of visual in-formation (colored squares) presented on a touchscreenVisuomotor tracking and hand-eye coordination wereevaluated using the NEPSY-II Visuomotor PrecisionTask (ages 3ndash4) For this task the participant used theirpreferred hand to draw a line as quickly as possiblewhile staying inside the tracked lines [70]
Caregiver-informed measuresFour caregiver-report measures of cognition and behav-ior were included Executive functioning impairmentswere assessed via the Global Executive Composite stand-ard score from the Behavioral Rating Inventory of Ex-ecutive Function School Age (BRIEF [71]) Adaptivebehavior was evaluated using the standard composite
score of the Scales of Independent Behavior-RevisedShort Form (SIB-R [72]) Maladaptive behavior wasassessed across three variables (conduct problems anx-iety and hyperactivity) from the Nisonger Child Behav-ior Rating Form (NCBRF [73]) These subscales wereselected because the additional subscales overlappedwith the other measures employed in this study (egASD symptoms adaptive behavior) ASD symptomswere assessed via the Social Communication Question-naire Lifetime version (SCQ [74]) The total raw scorefrom the SCQ was used All measures described aboveare psychometrically sound assessments used frequentlyin individuals with DS See Edgin et al [67] for more de-tailed informationDemographic information on participant age sex self-
identified race and ethnicity presence of a congenitalheart defect household income and maternal and pater-nal age were obtained via caregiver report and medicalrecord abstraction (Table 1)
Table 1 Demographic characteristics of the overall sample and latent classes
Overall Sample ldquoNormativerdquo class ldquoCognitiverdquo class ldquoBehavioralrdquo class
N () 314 (100) 153 (487) 109 (347) 52 (166)
Age (M SD) 137 (47) 136 (45) 135 (47) 146 (51)
Maternal age (M SD) 348 (55) 354 (53) 343 (62) 342 (45)
Paternal age (M SD) 364 (57) 370 (55) 357 (61) 359 (53)
Household income ()
lt$75000 287 223 349 314
$75000ndash$100000 155 144 170 157
$100000+ 558 623 481 529
Sex ( male) 510 569 404 558
Self-identified raceethnicity ()
White 752 808 676 750
Black 64 66 83 19
Hispanic 32 13 65 19
Asian 145 113 167 192
Other 6 0 1 19
Congenital heart defect ( yes) 610 656 544 608
Assessment scores (M SD)
KBIT-2 252 (117) 300 (108) 163 (85) 299 (90)
CANTAB spatial span 27 (16) 33 (12) 14 (16) 29 (14)
NEPSY-II visuomotor precision 133 (57) 142 (56) 115 (60) 144 (51)
BRIEF 135 (233) 1227 (193) 1442 (195) 1543 (202)
SIB-R 579 (233) 704 (196) 393 (182) 583 (167)
NCBRF conduct problems 75 (61) 51 (41) 75 (53) 148 (66)
NCBRF insecureanxious 40 (40) 27 (25) 29 (25) 100 (47)
NCBRF hyperactivity 65 (44) 45 (32) 77 (42) 101 (47)
SCQ 86 (55) 52 (32) 125 (49) 118 (55)
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF GEC Behavioral Rating Inventory ofExecutive Function SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication Questionnaire
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 5 of 14
Statistical analysisThe first step in the analysis was to place all of the vari-ables on a common metric because many of the vari-ables were based on raw scores If items did not havesimilar scaling the LPA would be uninterpretable Toaccomplish this all variables were transformed using aZ-score conversion which placed all scores on a metricof Mean = 0 (reflecting the overall sample average) andSD = 1 Thus Z-score values can be interpreted in termsof standard deviations For instance a 1-point SD differ-ence is equivalent to a 682 difference between groupsThis is interpreted as a large effect size whereas a 05SD (341 difference) represents a moderate effect sizeDuring the transformation all variables including stand-ard scores were adjusted for age All variables retainedtheir original direction of measurement such that higherscores on the NCBRF SCQ and BRIEF indicated greaterimpairment and higher scores on the performance-based measures and SIB-R reflected less impairmentstronger performance See Fig 1 for visual representa-tion of each age-corrected Z-score transformed variableNext the age-corrected Z-score transformed variables
were submitted to an LPA LPA was used to identifyhomogeneous latent subgroups of individuals with DSbased on continuous indicators of cognition behaviorand development [75] Using a series of fit statistics thefirst step in this procedure is to identify how many sub-groups (hereafter referred to as ldquoclassesrdquo) existed in thesample The most commonly known fit statistics used inthis study were the Akaike (AIC) and sample size-adjusted Bayesian (SS-BIC) information criterionsLower AIC and SS-BIC values indicate a model that fitsthe data best [76] Next Vuong-Lo-Mendell-Rubin
(VLMR) and bootstrapped likelihood ratio (BLRT) testswere employed These tests iteratively examined thecurrent model compared to the previous model with oneless class When p gt 05 it suggests that the currentmodel does not fit significantly better than the K-1model [75] Additional metrics included entropy andmean class probability (M[CP]) both of which indicatemisclassification Higher scores on both metrics are bestwith a value of 1 being perfect measurement Prior workby Nylund et al [77] suggests that the BIC and BLRTare more reliable indices of class structure than the AICand VLMR respectivelyAfter arriving at the optimal class structure individual
membership to the model was exported Each individualwas assigned to a class by the software based on the classthat represented their greatest posterior probability ofmembership Finally a multivariate multinomial regres-sion model simultaneously examined all demographic cor-relates of class Only paternal age was excluded because itwas strongly associated with maternal age (r = 71) Self-identified raceethnicity was dichotomized (White vsother) because there were small sample sizes for non-White categories The multinomial model included robustvariance to address any unknown clustering or model mis-specification LPA analyses were performed in MPLUSVersion 70 [78] and all other data management and ana-lysis occurred in STATA 150 [79]Three variables used in the LPA measurement model
had substantial missingness (SIB-R 7 missing CANTAB 21 SCQ 23) MPLUS uses full information max-imum likelihood estimation (FIML) to accommodatemissing data in structural equation-based models FIMLproduces unbiased estimates and standard errors when
Table 2 Description of primary measures
Domain of assessment Measure Outcome variablea Interpretation of score
Performance-based assessments of cognition
Verbal + nonverbal intelligence KBIT-2 Raw score composite Higher score = more skills
Working memory (immediate memory forspatial-temporal sequences)
CANTAB Spatial Span Forward span length Higher score = more skills
Visuomotor scanning and hand-eyecoordination
NEPSY-II VisuomotorPrecision ages 3ndash4
Total score (time and number of errors) Higher score = more skills
Caregiver-informed assessments of cognition and behavior
Executive functioning BRIEF School Age Global Executive Composite standard score Higher score = moreimpairments
Adaptive SIB-R Short Form Standard score composite Higher score = moreadaptive skills
Maladaptive NCBRF Conduct problems insecureanxious andhyperactivity subscale raw scores
Higher score = moremaladaptive behaviors
Autism spectrum disorder (ASD)symptomatology
SCQ-Lifetime Total raw score Higher score = more ASD-like symptoms
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF Behavioral Rating Inventory of ExecutiveFunction SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication QuestionnaireaAll outcome variables were age-corrected
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 6 of 14
data are missing either at random or completely at ran-dom [80] To understand the influence of FIML theLPA was run on the sample using complete case ana-lysis which severely limited the sample size (n = 156)Importantly the findings supported the same inferencesas the model that included the entire sample via FIMLin terms of class structure and fit statistics Given thisfinding and the fact that complete case analysis has itsknown biases the full sample was employed in the LPAand regression analyses using FIML
ResultsLPAFit statistics for the iterative LPA procedure are shownin Table 3 Determining the number of classes to includein the model depends on assessing the various fit statis-tics as well as considering class size and interpretationWe examined 2- through 4-class models Table 3 showsthat the AIC and SS-BIC values decreased continuouslywith increasing class size indicating a better fit with
increasing number of classes as expected The decreasein these scores was considerably larger between the 2-and 3-class models compared to the 3- to 4-classmodels This pattern provides evidence of at least a 3-class model Entropy and M(CP) were high and fairlyconsistent across the models The VLMR suggested a 2-class model as the 3-class model did not significantlyimprove the model fit However the BLRT remained sig-nificant at p lt 001 with the 4-class model suggestingmore than four classes may be indicated A fifth classwas not evaluated due to the small class size in the 4-class modelOverall three indices (AIC BIC BLRT) provided evi-
dence for more than two classes whereas the VLMRsuggested a 2-class solution Prior work by Nylund et al[77] has shown BIC and BLRT as two of the most reli-able fit indices both of which supported a larger numberof classes in this dataset Given that the fit statistics gen-erally supported more than two classes and the 2-classsolution did not reflect important heterogeneity detected
Fig 1 Distribution of age-corrected Z-score transformed measures used in the latent profile analysis Note NCBRF Nisonger Child Behavior RatingForm Hyp hyperactivity BRIEF Behavioral Rating Inventory of Executive Function EF executive functioning SCQ Social Communication Questionnaire-Lifetime ASD autism spectrum disorder SIB-R Scales of Independent Behavior-Revised AB adaptive behavior VMP visuomotor precision CANTABCambridge Neuropsychological Test Automated Battery SS spatial span KBIT Kaufman Brief Intelligence Test 2nd edition IQ verbal and nonverbal rawscore sum (averaged)
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 7 of 14
in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

Comorbid autism spectrum disorder (ASD) in DSIndividuals with DS are at a greater risk of comorbid ASDthan the general population with prevalence estimates sug-gesting up to 19 [61] Notably comorbid ASD tends to im-pact both cognitive and behavioral aspects of the DSphenotype Compared to individuals with DS who do nothave comorbid ASD individuals with DS and comorbidASD tend to display more maladaptive behaviors (ie stereo-typic and anxiouswithdrawn domains [53 55]) and lowerIQ and adaptive functioning [61 62] Additionally studiesexamining broader ASD-like symptomatology among indi-viduals with DS who are at low risk for comorbid ASD havefound a similar pattern lower IQ and adaptive functioningand higher rates of maladaptive behaviors are associated withbroader ASD-like symptoms [63ndash65] Therefore it appearsthat there is some overlap between ASD-like symptoms andthe behavioral phenotype associated with DS However it isunclear if the use of group-level means obscures a more nu-anced profile of cognition and adaptive behavior in relationto ASD symptomatology in DS similar to what is observedin non-syndromic ASD [66]
Current studyThe literature on cognition (IQ and executive function-ing) adaptive and maladaptive behaviors and ASDsymptomatology associated with the DS phenotype indi-cates a general syndrome-specific pattern however asreviewed above it also indicates significant variabilityThus we hypothesize that the general syndrome-specificpattern does not represent all individuals with DS andthat within-group profiles can be identified More nu-anced within-group profiles may vary by age becausegeneral developmental differences within the syndrome-specific pattern of strengths and weakness have beennoted in the literature Thus we also hypothesize thatage is associated with within-group profilesUsing LPA as an exploratory approach we aimed to test
our hypotheses by (1) determining whether subgroups of in-dividuals with DS can be characterized using performance-based and caregiver-informed ratings of behavior and cogni-tion and (2) examining the demographic characteristics asso-ciated with the latent subgroups To achieve these aims westudied a large sample of individuals with DS ages 6ndash25years who were recruited through a network of sites acrossthe USA called the Down Syndrome Cognition Project (seeRosser et al [14])
MethodsParticipantsThree hundred fifty-six individuals with DS ages 6ndash25years old participated in the larger study the Down Syn-drome Cognition Project (see Rosser et al [14] for inclu-sion criteria and participation rates) Using that samplewe retained all members of the original cohort except
for participants who were missing data on three or moreof the primary measures (n = 42) resulting in a finalsample size of 314 Participants were recruited fromclinics community eventssupport groups conferencesadvertisements and previous research studies by mul-tiple sites across the USA See Table 1 for participantdemographic information
Measures and procedureThe Down Syndrome Cognition Project testing battery [14]included a series of performance-based neuropsychologicalassessments modified from the Arizona Cognitive Test Bat-tery which was developed to produce outcome measures forclinical trials involving individuals with DS [67 68] The testbattery has good test-retest reliability [67]Examiners at each Down Syndrome Cognition Project
site were trained to fidelity to administer the testing bat-tery to individuals with DS (see Edgin et al [67 68])Sites were monitored by the University of Arizona train-ing site andor the Emory Data Coordinating CenterPeriodic quality control checks included review of fidel-ity to administration and scoring procedures All datawere double entered with comparison checks to ensureaccuracy Research Electronic Data Capture (REDCap[69]) was used for data entry and managementParticipants completed the testing battery at an assess-
ment site or another convenient location (eg commu-nity center or family home) The entire session lastedabout 2ndash3 h with frequent breaks Tests were presentedin two fixed counterbalanced orders [67] Caregiverscompleted questionnaires related to participant demo-graphics medicaldevelopmental history and behaviorsTable 2 includes a description of the primary measures in-
cluded in the model These tests were selected based on sev-eral criteria Most importantly each measure was selected onthe basis of reflecting an important and unique componentof cognition behavior or development Where possible weused total composite or summary scores from the indicatedmeasure to capture all salient information and reduce thenumber of overall variables Variables were also selectedbased on normality Variables that were highly skewed dueto floor or ceiling effects limited the ability to measure thefull range of abilities and discriminate among subgroups andthus were eliminated from the analyses Finally measureswere also selected based on number of observations becausenot all measures were administered to the entire cohort
Performance-based assessments of cognitionThree performance-based tests of cognition were in-cluded in this study Intelligence was evaluated using theKaufman Brief Intelligence Test 2nd edition (KBIT-2[20]) Verbal and nonverbal raw scores were summedand then averaged for use in the model This approachwas taken because the IQ composite variable had
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 4 of 14
significant floor effects (34 of the sample had an IQle40) Working memory was evaluated using the Cam-bridge Neuropsychological Test Automated Battery(CANTAB) Spatial Span test which required the partici-pant to recall progressively longer sequences of visual in-formation (colored squares) presented on a touchscreenVisuomotor tracking and hand-eye coordination wereevaluated using the NEPSY-II Visuomotor PrecisionTask (ages 3ndash4) For this task the participant used theirpreferred hand to draw a line as quickly as possiblewhile staying inside the tracked lines [70]
Caregiver-informed measuresFour caregiver-report measures of cognition and behav-ior were included Executive functioning impairmentswere assessed via the Global Executive Composite stand-ard score from the Behavioral Rating Inventory of Ex-ecutive Function School Age (BRIEF [71]) Adaptivebehavior was evaluated using the standard composite
score of the Scales of Independent Behavior-RevisedShort Form (SIB-R [72]) Maladaptive behavior wasassessed across three variables (conduct problems anx-iety and hyperactivity) from the Nisonger Child Behav-ior Rating Form (NCBRF [73]) These subscales wereselected because the additional subscales overlappedwith the other measures employed in this study (egASD symptoms adaptive behavior) ASD symptomswere assessed via the Social Communication Question-naire Lifetime version (SCQ [74]) The total raw scorefrom the SCQ was used All measures described aboveare psychometrically sound assessments used frequentlyin individuals with DS See Edgin et al [67] for more de-tailed informationDemographic information on participant age sex self-
identified race and ethnicity presence of a congenitalheart defect household income and maternal and pater-nal age were obtained via caregiver report and medicalrecord abstraction (Table 1)
Table 1 Demographic characteristics of the overall sample and latent classes
Overall Sample ldquoNormativerdquo class ldquoCognitiverdquo class ldquoBehavioralrdquo class
N () 314 (100) 153 (487) 109 (347) 52 (166)
Age (M SD) 137 (47) 136 (45) 135 (47) 146 (51)
Maternal age (M SD) 348 (55) 354 (53) 343 (62) 342 (45)
Paternal age (M SD) 364 (57) 370 (55) 357 (61) 359 (53)
Household income ()
lt$75000 287 223 349 314
$75000ndash$100000 155 144 170 157
$100000+ 558 623 481 529
Sex ( male) 510 569 404 558
Self-identified raceethnicity ()
White 752 808 676 750
Black 64 66 83 19
Hispanic 32 13 65 19
Asian 145 113 167 192
Other 6 0 1 19
Congenital heart defect ( yes) 610 656 544 608
Assessment scores (M SD)
KBIT-2 252 (117) 300 (108) 163 (85) 299 (90)
CANTAB spatial span 27 (16) 33 (12) 14 (16) 29 (14)
NEPSY-II visuomotor precision 133 (57) 142 (56) 115 (60) 144 (51)
BRIEF 135 (233) 1227 (193) 1442 (195) 1543 (202)
SIB-R 579 (233) 704 (196) 393 (182) 583 (167)
NCBRF conduct problems 75 (61) 51 (41) 75 (53) 148 (66)
NCBRF insecureanxious 40 (40) 27 (25) 29 (25) 100 (47)
NCBRF hyperactivity 65 (44) 45 (32) 77 (42) 101 (47)
SCQ 86 (55) 52 (32) 125 (49) 118 (55)
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF GEC Behavioral Rating Inventory ofExecutive Function SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication Questionnaire
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 5 of 14
Statistical analysisThe first step in the analysis was to place all of the vari-ables on a common metric because many of the vari-ables were based on raw scores If items did not havesimilar scaling the LPA would be uninterpretable Toaccomplish this all variables were transformed using aZ-score conversion which placed all scores on a metricof Mean = 0 (reflecting the overall sample average) andSD = 1 Thus Z-score values can be interpreted in termsof standard deviations For instance a 1-point SD differ-ence is equivalent to a 682 difference between groupsThis is interpreted as a large effect size whereas a 05SD (341 difference) represents a moderate effect sizeDuring the transformation all variables including stand-ard scores were adjusted for age All variables retainedtheir original direction of measurement such that higherscores on the NCBRF SCQ and BRIEF indicated greaterimpairment and higher scores on the performance-based measures and SIB-R reflected less impairmentstronger performance See Fig 1 for visual representa-tion of each age-corrected Z-score transformed variableNext the age-corrected Z-score transformed variables
were submitted to an LPA LPA was used to identifyhomogeneous latent subgroups of individuals with DSbased on continuous indicators of cognition behaviorand development [75] Using a series of fit statistics thefirst step in this procedure is to identify how many sub-groups (hereafter referred to as ldquoclassesrdquo) existed in thesample The most commonly known fit statistics used inthis study were the Akaike (AIC) and sample size-adjusted Bayesian (SS-BIC) information criterionsLower AIC and SS-BIC values indicate a model that fitsthe data best [76] Next Vuong-Lo-Mendell-Rubin
(VLMR) and bootstrapped likelihood ratio (BLRT) testswere employed These tests iteratively examined thecurrent model compared to the previous model with oneless class When p gt 05 it suggests that the currentmodel does not fit significantly better than the K-1model [75] Additional metrics included entropy andmean class probability (M[CP]) both of which indicatemisclassification Higher scores on both metrics are bestwith a value of 1 being perfect measurement Prior workby Nylund et al [77] suggests that the BIC and BLRTare more reliable indices of class structure than the AICand VLMR respectivelyAfter arriving at the optimal class structure individual
membership to the model was exported Each individualwas assigned to a class by the software based on the classthat represented their greatest posterior probability ofmembership Finally a multivariate multinomial regres-sion model simultaneously examined all demographic cor-relates of class Only paternal age was excluded because itwas strongly associated with maternal age (r = 71) Self-identified raceethnicity was dichotomized (White vsother) because there were small sample sizes for non-White categories The multinomial model included robustvariance to address any unknown clustering or model mis-specification LPA analyses were performed in MPLUSVersion 70 [78] and all other data management and ana-lysis occurred in STATA 150 [79]Three variables used in the LPA measurement model
had substantial missingness (SIB-R 7 missing CANTAB 21 SCQ 23) MPLUS uses full information max-imum likelihood estimation (FIML) to accommodatemissing data in structural equation-based models FIMLproduces unbiased estimates and standard errors when
Table 2 Description of primary measures
Domain of assessment Measure Outcome variablea Interpretation of score
Performance-based assessments of cognition
Verbal + nonverbal intelligence KBIT-2 Raw score composite Higher score = more skills
Working memory (immediate memory forspatial-temporal sequences)
CANTAB Spatial Span Forward span length Higher score = more skills
Visuomotor scanning and hand-eyecoordination
NEPSY-II VisuomotorPrecision ages 3ndash4
Total score (time and number of errors) Higher score = more skills
Caregiver-informed assessments of cognition and behavior
Executive functioning BRIEF School Age Global Executive Composite standard score Higher score = moreimpairments
Adaptive SIB-R Short Form Standard score composite Higher score = moreadaptive skills
Maladaptive NCBRF Conduct problems insecureanxious andhyperactivity subscale raw scores
Higher score = moremaladaptive behaviors
Autism spectrum disorder (ASD)symptomatology
SCQ-Lifetime Total raw score Higher score = more ASD-like symptoms
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF Behavioral Rating Inventory of ExecutiveFunction SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication QuestionnaireaAll outcome variables were age-corrected
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 6 of 14
data are missing either at random or completely at ran-dom [80] To understand the influence of FIML theLPA was run on the sample using complete case ana-lysis which severely limited the sample size (n = 156)Importantly the findings supported the same inferencesas the model that included the entire sample via FIMLin terms of class structure and fit statistics Given thisfinding and the fact that complete case analysis has itsknown biases the full sample was employed in the LPAand regression analyses using FIML
ResultsLPAFit statistics for the iterative LPA procedure are shownin Table 3 Determining the number of classes to includein the model depends on assessing the various fit statis-tics as well as considering class size and interpretationWe examined 2- through 4-class models Table 3 showsthat the AIC and SS-BIC values decreased continuouslywith increasing class size indicating a better fit with
increasing number of classes as expected The decreasein these scores was considerably larger between the 2-and 3-class models compared to the 3- to 4-classmodels This pattern provides evidence of at least a 3-class model Entropy and M(CP) were high and fairlyconsistent across the models The VLMR suggested a 2-class model as the 3-class model did not significantlyimprove the model fit However the BLRT remained sig-nificant at p lt 001 with the 4-class model suggestingmore than four classes may be indicated A fifth classwas not evaluated due to the small class size in the 4-class modelOverall three indices (AIC BIC BLRT) provided evi-
dence for more than two classes whereas the VLMRsuggested a 2-class solution Prior work by Nylund et al[77] has shown BIC and BLRT as two of the most reli-able fit indices both of which supported a larger numberof classes in this dataset Given that the fit statistics gen-erally supported more than two classes and the 2-classsolution did not reflect important heterogeneity detected
Fig 1 Distribution of age-corrected Z-score transformed measures used in the latent profile analysis Note NCBRF Nisonger Child Behavior RatingForm Hyp hyperactivity BRIEF Behavioral Rating Inventory of Executive Function EF executive functioning SCQ Social Communication Questionnaire-Lifetime ASD autism spectrum disorder SIB-R Scales of Independent Behavior-Revised AB adaptive behavior VMP visuomotor precision CANTABCambridge Neuropsychological Test Automated Battery SS spatial span KBIT Kaufman Brief Intelligence Test 2nd edition IQ verbal and nonverbal rawscore sum (averaged)
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 7 of 14
in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

significant floor effects (34 of the sample had an IQle40) Working memory was evaluated using the Cam-bridge Neuropsychological Test Automated Battery(CANTAB) Spatial Span test which required the partici-pant to recall progressively longer sequences of visual in-formation (colored squares) presented on a touchscreenVisuomotor tracking and hand-eye coordination wereevaluated using the NEPSY-II Visuomotor PrecisionTask (ages 3ndash4) For this task the participant used theirpreferred hand to draw a line as quickly as possiblewhile staying inside the tracked lines [70]
Caregiver-informed measuresFour caregiver-report measures of cognition and behav-ior were included Executive functioning impairmentswere assessed via the Global Executive Composite stand-ard score from the Behavioral Rating Inventory of Ex-ecutive Function School Age (BRIEF [71]) Adaptivebehavior was evaluated using the standard composite
score of the Scales of Independent Behavior-RevisedShort Form (SIB-R [72]) Maladaptive behavior wasassessed across three variables (conduct problems anx-iety and hyperactivity) from the Nisonger Child Behav-ior Rating Form (NCBRF [73]) These subscales wereselected because the additional subscales overlappedwith the other measures employed in this study (egASD symptoms adaptive behavior) ASD symptomswere assessed via the Social Communication Question-naire Lifetime version (SCQ [74]) The total raw scorefrom the SCQ was used All measures described aboveare psychometrically sound assessments used frequentlyin individuals with DS See Edgin et al [67] for more de-tailed informationDemographic information on participant age sex self-
identified race and ethnicity presence of a congenitalheart defect household income and maternal and pater-nal age were obtained via caregiver report and medicalrecord abstraction (Table 1)
Table 1 Demographic characteristics of the overall sample and latent classes
Overall Sample ldquoNormativerdquo class ldquoCognitiverdquo class ldquoBehavioralrdquo class
N () 314 (100) 153 (487) 109 (347) 52 (166)
Age (M SD) 137 (47) 136 (45) 135 (47) 146 (51)
Maternal age (M SD) 348 (55) 354 (53) 343 (62) 342 (45)
Paternal age (M SD) 364 (57) 370 (55) 357 (61) 359 (53)
Household income ()
lt$75000 287 223 349 314
$75000ndash$100000 155 144 170 157
$100000+ 558 623 481 529
Sex ( male) 510 569 404 558
Self-identified raceethnicity ()
White 752 808 676 750
Black 64 66 83 19
Hispanic 32 13 65 19
Asian 145 113 167 192
Other 6 0 1 19
Congenital heart defect ( yes) 610 656 544 608
Assessment scores (M SD)
KBIT-2 252 (117) 300 (108) 163 (85) 299 (90)
CANTAB spatial span 27 (16) 33 (12) 14 (16) 29 (14)
NEPSY-II visuomotor precision 133 (57) 142 (56) 115 (60) 144 (51)
BRIEF 135 (233) 1227 (193) 1442 (195) 1543 (202)
SIB-R 579 (233) 704 (196) 393 (182) 583 (167)
NCBRF conduct problems 75 (61) 51 (41) 75 (53) 148 (66)
NCBRF insecureanxious 40 (40) 27 (25) 29 (25) 100 (47)
NCBRF hyperactivity 65 (44) 45 (32) 77 (42) 101 (47)
SCQ 86 (55) 52 (32) 125 (49) 118 (55)
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF GEC Behavioral Rating Inventory ofExecutive Function SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication Questionnaire
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 5 of 14
Statistical analysisThe first step in the analysis was to place all of the vari-ables on a common metric because many of the vari-ables were based on raw scores If items did not havesimilar scaling the LPA would be uninterpretable Toaccomplish this all variables were transformed using aZ-score conversion which placed all scores on a metricof Mean = 0 (reflecting the overall sample average) andSD = 1 Thus Z-score values can be interpreted in termsof standard deviations For instance a 1-point SD differ-ence is equivalent to a 682 difference between groupsThis is interpreted as a large effect size whereas a 05SD (341 difference) represents a moderate effect sizeDuring the transformation all variables including stand-ard scores were adjusted for age All variables retainedtheir original direction of measurement such that higherscores on the NCBRF SCQ and BRIEF indicated greaterimpairment and higher scores on the performance-based measures and SIB-R reflected less impairmentstronger performance See Fig 1 for visual representa-tion of each age-corrected Z-score transformed variableNext the age-corrected Z-score transformed variables
were submitted to an LPA LPA was used to identifyhomogeneous latent subgroups of individuals with DSbased on continuous indicators of cognition behaviorand development [75] Using a series of fit statistics thefirst step in this procedure is to identify how many sub-groups (hereafter referred to as ldquoclassesrdquo) existed in thesample The most commonly known fit statistics used inthis study were the Akaike (AIC) and sample size-adjusted Bayesian (SS-BIC) information criterionsLower AIC and SS-BIC values indicate a model that fitsthe data best [76] Next Vuong-Lo-Mendell-Rubin
(VLMR) and bootstrapped likelihood ratio (BLRT) testswere employed These tests iteratively examined thecurrent model compared to the previous model with oneless class When p gt 05 it suggests that the currentmodel does not fit significantly better than the K-1model [75] Additional metrics included entropy andmean class probability (M[CP]) both of which indicatemisclassification Higher scores on both metrics are bestwith a value of 1 being perfect measurement Prior workby Nylund et al [77] suggests that the BIC and BLRTare more reliable indices of class structure than the AICand VLMR respectivelyAfter arriving at the optimal class structure individual
membership to the model was exported Each individualwas assigned to a class by the software based on the classthat represented their greatest posterior probability ofmembership Finally a multivariate multinomial regres-sion model simultaneously examined all demographic cor-relates of class Only paternal age was excluded because itwas strongly associated with maternal age (r = 71) Self-identified raceethnicity was dichotomized (White vsother) because there were small sample sizes for non-White categories The multinomial model included robustvariance to address any unknown clustering or model mis-specification LPA analyses were performed in MPLUSVersion 70 [78] and all other data management and ana-lysis occurred in STATA 150 [79]Three variables used in the LPA measurement model
had substantial missingness (SIB-R 7 missing CANTAB 21 SCQ 23) MPLUS uses full information max-imum likelihood estimation (FIML) to accommodatemissing data in structural equation-based models FIMLproduces unbiased estimates and standard errors when
Table 2 Description of primary measures
Domain of assessment Measure Outcome variablea Interpretation of score
Performance-based assessments of cognition
Verbal + nonverbal intelligence KBIT-2 Raw score composite Higher score = more skills
Working memory (immediate memory forspatial-temporal sequences)
CANTAB Spatial Span Forward span length Higher score = more skills
Visuomotor scanning and hand-eyecoordination
NEPSY-II VisuomotorPrecision ages 3ndash4
Total score (time and number of errors) Higher score = more skills
Caregiver-informed assessments of cognition and behavior
Executive functioning BRIEF School Age Global Executive Composite standard score Higher score = moreimpairments
Adaptive SIB-R Short Form Standard score composite Higher score = moreadaptive skills
Maladaptive NCBRF Conduct problems insecureanxious andhyperactivity subscale raw scores
Higher score = moremaladaptive behaviors
Autism spectrum disorder (ASD)symptomatology
SCQ-Lifetime Total raw score Higher score = more ASD-like symptoms
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF Behavioral Rating Inventory of ExecutiveFunction SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication QuestionnaireaAll outcome variables were age-corrected
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 6 of 14
data are missing either at random or completely at ran-dom [80] To understand the influence of FIML theLPA was run on the sample using complete case ana-lysis which severely limited the sample size (n = 156)Importantly the findings supported the same inferencesas the model that included the entire sample via FIMLin terms of class structure and fit statistics Given thisfinding and the fact that complete case analysis has itsknown biases the full sample was employed in the LPAand regression analyses using FIML
ResultsLPAFit statistics for the iterative LPA procedure are shownin Table 3 Determining the number of classes to includein the model depends on assessing the various fit statis-tics as well as considering class size and interpretationWe examined 2- through 4-class models Table 3 showsthat the AIC and SS-BIC values decreased continuouslywith increasing class size indicating a better fit with
increasing number of classes as expected The decreasein these scores was considerably larger between the 2-and 3-class models compared to the 3- to 4-classmodels This pattern provides evidence of at least a 3-class model Entropy and M(CP) were high and fairlyconsistent across the models The VLMR suggested a 2-class model as the 3-class model did not significantlyimprove the model fit However the BLRT remained sig-nificant at p lt 001 with the 4-class model suggestingmore than four classes may be indicated A fifth classwas not evaluated due to the small class size in the 4-class modelOverall three indices (AIC BIC BLRT) provided evi-
dence for more than two classes whereas the VLMRsuggested a 2-class solution Prior work by Nylund et al[77] has shown BIC and BLRT as two of the most reli-able fit indices both of which supported a larger numberof classes in this dataset Given that the fit statistics gen-erally supported more than two classes and the 2-classsolution did not reflect important heterogeneity detected
Fig 1 Distribution of age-corrected Z-score transformed measures used in the latent profile analysis Note NCBRF Nisonger Child Behavior RatingForm Hyp hyperactivity BRIEF Behavioral Rating Inventory of Executive Function EF executive functioning SCQ Social Communication Questionnaire-Lifetime ASD autism spectrum disorder SIB-R Scales of Independent Behavior-Revised AB adaptive behavior VMP visuomotor precision CANTABCambridge Neuropsychological Test Automated Battery SS spatial span KBIT Kaufman Brief Intelligence Test 2nd edition IQ verbal and nonverbal rawscore sum (averaged)
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 7 of 14
in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

Statistical analysisThe first step in the analysis was to place all of the vari-ables on a common metric because many of the vari-ables were based on raw scores If items did not havesimilar scaling the LPA would be uninterpretable Toaccomplish this all variables were transformed using aZ-score conversion which placed all scores on a metricof Mean = 0 (reflecting the overall sample average) andSD = 1 Thus Z-score values can be interpreted in termsof standard deviations For instance a 1-point SD differ-ence is equivalent to a 682 difference between groupsThis is interpreted as a large effect size whereas a 05SD (341 difference) represents a moderate effect sizeDuring the transformation all variables including stand-ard scores were adjusted for age All variables retainedtheir original direction of measurement such that higherscores on the NCBRF SCQ and BRIEF indicated greaterimpairment and higher scores on the performance-based measures and SIB-R reflected less impairmentstronger performance See Fig 1 for visual representa-tion of each age-corrected Z-score transformed variableNext the age-corrected Z-score transformed variables
were submitted to an LPA LPA was used to identifyhomogeneous latent subgroups of individuals with DSbased on continuous indicators of cognition behaviorand development [75] Using a series of fit statistics thefirst step in this procedure is to identify how many sub-groups (hereafter referred to as ldquoclassesrdquo) existed in thesample The most commonly known fit statistics used inthis study were the Akaike (AIC) and sample size-adjusted Bayesian (SS-BIC) information criterionsLower AIC and SS-BIC values indicate a model that fitsthe data best [76] Next Vuong-Lo-Mendell-Rubin
(VLMR) and bootstrapped likelihood ratio (BLRT) testswere employed These tests iteratively examined thecurrent model compared to the previous model with oneless class When p gt 05 it suggests that the currentmodel does not fit significantly better than the K-1model [75] Additional metrics included entropy andmean class probability (M[CP]) both of which indicatemisclassification Higher scores on both metrics are bestwith a value of 1 being perfect measurement Prior workby Nylund et al [77] suggests that the BIC and BLRTare more reliable indices of class structure than the AICand VLMR respectivelyAfter arriving at the optimal class structure individual
membership to the model was exported Each individualwas assigned to a class by the software based on the classthat represented their greatest posterior probability ofmembership Finally a multivariate multinomial regres-sion model simultaneously examined all demographic cor-relates of class Only paternal age was excluded because itwas strongly associated with maternal age (r = 71) Self-identified raceethnicity was dichotomized (White vsother) because there were small sample sizes for non-White categories The multinomial model included robustvariance to address any unknown clustering or model mis-specification LPA analyses were performed in MPLUSVersion 70 [78] and all other data management and ana-lysis occurred in STATA 150 [79]Three variables used in the LPA measurement model
had substantial missingness (SIB-R 7 missing CANTAB 21 SCQ 23) MPLUS uses full information max-imum likelihood estimation (FIML) to accommodatemissing data in structural equation-based models FIMLproduces unbiased estimates and standard errors when
Table 2 Description of primary measures
Domain of assessment Measure Outcome variablea Interpretation of score
Performance-based assessments of cognition
Verbal + nonverbal intelligence KBIT-2 Raw score composite Higher score = more skills
Working memory (immediate memory forspatial-temporal sequences)
CANTAB Spatial Span Forward span length Higher score = more skills
Visuomotor scanning and hand-eyecoordination
NEPSY-II VisuomotorPrecision ages 3ndash4
Total score (time and number of errors) Higher score = more skills
Caregiver-informed assessments of cognition and behavior
Executive functioning BRIEF School Age Global Executive Composite standard score Higher score = moreimpairments
Adaptive SIB-R Short Form Standard score composite Higher score = moreadaptive skills
Maladaptive NCBRF Conduct problems insecureanxious andhyperactivity subscale raw scores
Higher score = moremaladaptive behaviors
Autism spectrum disorder (ASD)symptomatology
SCQ-Lifetime Total raw score Higher score = more ASD-like symptoms
KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF Behavioral Rating Inventory of ExecutiveFunction SIB-R Scales of Independent Behavior-Revised NCBRF Nisonger Child Behavior Rating Form SCQ Social Communication QuestionnaireaAll outcome variables were age-corrected
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 6 of 14
data are missing either at random or completely at ran-dom [80] To understand the influence of FIML theLPA was run on the sample using complete case ana-lysis which severely limited the sample size (n = 156)Importantly the findings supported the same inferencesas the model that included the entire sample via FIMLin terms of class structure and fit statistics Given thisfinding and the fact that complete case analysis has itsknown biases the full sample was employed in the LPAand regression analyses using FIML
ResultsLPAFit statistics for the iterative LPA procedure are shownin Table 3 Determining the number of classes to includein the model depends on assessing the various fit statis-tics as well as considering class size and interpretationWe examined 2- through 4-class models Table 3 showsthat the AIC and SS-BIC values decreased continuouslywith increasing class size indicating a better fit with
increasing number of classes as expected The decreasein these scores was considerably larger between the 2-and 3-class models compared to the 3- to 4-classmodels This pattern provides evidence of at least a 3-class model Entropy and M(CP) were high and fairlyconsistent across the models The VLMR suggested a 2-class model as the 3-class model did not significantlyimprove the model fit However the BLRT remained sig-nificant at p lt 001 with the 4-class model suggestingmore than four classes may be indicated A fifth classwas not evaluated due to the small class size in the 4-class modelOverall three indices (AIC BIC BLRT) provided evi-
dence for more than two classes whereas the VLMRsuggested a 2-class solution Prior work by Nylund et al[77] has shown BIC and BLRT as two of the most reli-able fit indices both of which supported a larger numberof classes in this dataset Given that the fit statistics gen-erally supported more than two classes and the 2-classsolution did not reflect important heterogeneity detected
Fig 1 Distribution of age-corrected Z-score transformed measures used in the latent profile analysis Note NCBRF Nisonger Child Behavior RatingForm Hyp hyperactivity BRIEF Behavioral Rating Inventory of Executive Function EF executive functioning SCQ Social Communication Questionnaire-Lifetime ASD autism spectrum disorder SIB-R Scales of Independent Behavior-Revised AB adaptive behavior VMP visuomotor precision CANTABCambridge Neuropsychological Test Automated Battery SS spatial span KBIT Kaufman Brief Intelligence Test 2nd edition IQ verbal and nonverbal rawscore sum (averaged)
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 7 of 14
in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

data are missing either at random or completely at ran-dom [80] To understand the influence of FIML theLPA was run on the sample using complete case ana-lysis which severely limited the sample size (n = 156)Importantly the findings supported the same inferencesas the model that included the entire sample via FIMLin terms of class structure and fit statistics Given thisfinding and the fact that complete case analysis has itsknown biases the full sample was employed in the LPAand regression analyses using FIML
ResultsLPAFit statistics for the iterative LPA procedure are shownin Table 3 Determining the number of classes to includein the model depends on assessing the various fit statis-tics as well as considering class size and interpretationWe examined 2- through 4-class models Table 3 showsthat the AIC and SS-BIC values decreased continuouslywith increasing class size indicating a better fit with
increasing number of classes as expected The decreasein these scores was considerably larger between the 2-and 3-class models compared to the 3- to 4-classmodels This pattern provides evidence of at least a 3-class model Entropy and M(CP) were high and fairlyconsistent across the models The VLMR suggested a 2-class model as the 3-class model did not significantlyimprove the model fit However the BLRT remained sig-nificant at p lt 001 with the 4-class model suggestingmore than four classes may be indicated A fifth classwas not evaluated due to the small class size in the 4-class modelOverall three indices (AIC BIC BLRT) provided evi-
dence for more than two classes whereas the VLMRsuggested a 2-class solution Prior work by Nylund et al[77] has shown BIC and BLRT as two of the most reli-able fit indices both of which supported a larger numberof classes in this dataset Given that the fit statistics gen-erally supported more than two classes and the 2-classsolution did not reflect important heterogeneity detected
Fig 1 Distribution of age-corrected Z-score transformed measures used in the latent profile analysis Note NCBRF Nisonger Child Behavior RatingForm Hyp hyperactivity BRIEF Behavioral Rating Inventory of Executive Function EF executive functioning SCQ Social Communication Questionnaire-Lifetime ASD autism spectrum disorder SIB-R Scales of Independent Behavior-Revised AB adaptive behavior VMP visuomotor precision CANTABCambridge Neuropsychological Test Automated Battery SS spatial span KBIT Kaufman Brief Intelligence Test 2nd edition IQ verbal and nonverbal rawscore sum (averaged)
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 7 of 14
in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

in the 3- and 4-class solutions the 2-class model wasnot selectedThe 4-class model is shown in Figure 1 of the supple-
mental information The fourth class demonstrated thegreatest impairments both cognitively and behaviorallyNotably the sample size was small (7) for this class Thesmall sample size raises concerns about reproducibility aswell as diminished power when examining demographicdifferences As such the 3-class model was chosenFigure 2 displays the 3-class model that we adopted and
is consistent with our hypothesis that subtypes can becharacterized based on the variability observed in cogni-tive and behavioral measures We termed the classesbased on the variables around which each group clusteredrather than describing the participants themselves Thelargest group (48) had an even profile with respect to alldomains included in the analysis (Fig 2 gray line) wetermed this the ldquonormativerdquo class This class was demar-cated by relatively strong performance compared to thesample average That is negative values indicated less mal-adaptive behaviors ASD symptomatology and executivefunctioning impairments Positive scores on the SIB-R andall performance-based measures indicated stronger cogni-tive skills (IQ and visuospatial abilities) and adaptive be-havior compared to the sample average The second
largest group (double line) was termed the ldquocognitiverdquoclass (35) This class was distinguished by low scores onthe performance-based measures of cognition howevermeasures of ASD symptomatology executive functioningimpairment and hyperactivity were also elevated indicat-ing difficulties in these areas The final group (dotted line)was termed the ldquobehavioralrdquo class (17) This class hadhighly elevated scores for maladaptive behaviors followedby elevated ASD symptomatology and executive function-ing impairments Conversely their cognitive abilities fromthe performance-based assessments and adaptive behaviorwere all near or above the sample average suggestingthese abilities were similar to the ldquonormativerdquo group
Demographic correlatesA multivariate multinomial regression model was usedto simultaneously examine all demographic correlates ofclass The ldquonormativerdquo class served as the referencegroup Only two variables were significantly differentacross the latent classes (Table 4) Participants in theldquocognitiverdquo class were 47 less likely to have a family in-come of gt $100000 and 49 less likely to be femalewhen compared to the ldquonormativerdquo class (both p lt 05)No differences were found among the demographic
Table 3 Fit statistics from the latent profile analysis
Number of classes AIC SS-BIC Entropy M(CP) VLMR BLRT Smallest Class Size
2 7172 7188 76 92 lt01 lt001 39
3 7024 7046 80 90 15 lt001 18
4 6968 6996 80 89 32 lt001 7
AIC Akaike information criterion SS-BIC sample size-adjusted Bayesian information criterion M(CP) mean class probability VLMR Vuong-Lo-Mendell-Rubin Test pvalue BLRT bootstrapped likelihood ratio test p value
Fig 2 Latent profile analysis 3-class model Note All values are Z-score transformed (M = 0 SD = 1) Higher scores on the NCBRF SCQ and BRIEFindicate greater impairment higher scores on all other measures reflect less impairment
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 8 of 14
variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

variables between the ldquonormativerdquo and ldquobehavioralrdquo clas-ses See Table 4 for details
DiscussionThe current study examined variability in the DS phenotypeamong 314 children adolescents and young adults with DSa large sample size for this population Specifically we aimedto (1) determine whether subgroups of individuals with DScould be characterized using performance-based andcaregiver-informed ratings of behavior and cognition and (2)examine the demographic characteristics associated with thelatent subgroups Using LPA we identified three distinctclasses of individuals with DS referred to as the ldquonormativerdquoldquocognitiverdquo and ldquobehavioralrdquo classes these labels are basedon the variables around which the three groups clustered ra-ther than the groups themselvesRepresenting almost half of the sample (48) the
ldquonormativerdquo class demonstrated a relatively consistentprofile with respect to cognition and adaptive behaviorincluding relatively low levels of maladaptive behaviorASD symptomatology and executive functioning impair-ment Arguably this group represents a profile similar towhat is described in much of the literature on the DSphenotype [3] The next largest group of participantsrepresented more than a third of the sample (35) andwas termed the ldquocognitiverdquo class These participants weredistinguished by the lowest scores on adaptive behaviorand performance-based measures of cognition (IQ andvisuospatial abilities) coupled with high ASD
symptomatology executive functioning impairmentsand relatively low maladaptive behaviors The final andsmallest group (17) was termed the ldquobehavioralrdquo classdue to high rates of maladaptive behavior particularlyfor conduct problems and anxiety along with high ASDsymptomatology and high levels of executive functioningimpairment However their performance-based cogni-tive scores (IQ and visuospatial abilities) were similar tothat of the ldquonormativerdquo class Interestingly the adaptivebehavior scores of the ldquobehavioral classrdquo fell in betweenthe other two classesThe nuanced profiles identified by the ldquocognitiverdquo and
ldquobehavioralrdquo classes not only exemplify the inter-individual variability observed in the DS phenotype butalso the intra-individual variability among developmentalconstructs That is it has been difficult to understandthe relations among cognition adaptive and maladaptivebehavior and ASD symptomatology at the group level inDS However by using LPA we were able to observe dif-ferential patterns across these constructs within the dif-ferent classes For example as expected adaptivebehavior was strongest in the participants with highercognition as measured by IQ and visuospatial abilitiesand fewer maladaptive behaviors (ldquonormativerdquo class)Conversely adaptive behavior was weakest in the partici-pants with lower cognition (ldquocognitiverdquo class) Interest-ingly the ldquobehavioralrdquo class demonstrated a group ofindividuals with DS with adaptive behavior that fell inline with the full samplersquos mean despite displaying thehighest rates of maladaptive behaviors and executivefunctioning impairments This is somewhat surprisingbecause maladaptive behaviors and ASD symptomatol-ogy tend to be associated with greater difficulties inadaptive behavior [81] Our results suggest that for indi-viduals with DS adaptive behavior may be lessdependent on these constructs It is possible that theldquobehavioralrdquo class captured some children with DS andcomorbid developmental behavioral disorder who dis-play high rates of externalizing maladaptive behaviorswith a more inconsistent presentation of adaptive behav-ior (eg maladaptive behaviors such as refusal that onlysometimes impede adaptive function) It is also possiblethat executive functioning impairments are contributingto this discrepancy impeding certain aspects of behaviormore than others or in certain settings (eg school vshome) Additional research is needed to examine thissubgroup of individuals with DS in more depthTwo of the groups (ldquocognitiverdquo and ldquobehavioralrdquo clas-
ses) demonstrated similar levels of ASD symptomatologydespite showing divergence in maladaptive behavior andcognition This is a particularly noteworthy finding be-cause it suggests that there is more than one phenotypeassociated with ASD risk in individuals with DS That isindividuals with DS who have relatively low IQ and
Table 4 Results from the multivariate multinomial regressionmodel
Demographicvariable
ldquoCognitiverdquo class ldquoBehavioralrdquo class
RRR 95 CI RRR 95 CI
Age 98 92 105 104 97 112
Maternal age 97 92 102 97 92 102
Income
lt$75000 Ref Ref Ref Ref
$75000ndash$100000 75 32 175 89 32 250
$100000+ 53 29 84 69 21 148
Sex
Male Ref Ref Ref Ref
Female 50 29 83 98 51 189
Self-identified ethnicity
White Ref Ref Ref Ref
Non-White 61 32 114 68 31 150
CHD
No Ref Ref Ref Ref
Yes 67 39 114 82 42 162
Ref reference group (ldquoNormativerdquo class serves as the overall reference group)CHD congenital heart defect RRR relative risk ratiop lt05
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 9 of 14
visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

visuospatial abilities or who have high rates of maladap-tive behavior are at greater risk for ASD This is consist-ent with the broader literature on DS showing that ASDsymptoms are associated with lower IQ and maladaptivebehaviors [61 62] However in the current study mal-adaptive behavior and performance-based measures ofcognition appear to be separately associated with ASDsymptomology These data also suggest that it is possibleto disentangle ASD symptomatology from other mal-adaptive behaviors Moving forward this informationwill be particularly helpful in the search for biomarkersassociated with the various pathways to ASD in thispopulation Future research should also consider the roleof executive functioning difficulties as relatively highrates of impairment were present in both the ldquocognitiverdquoand ldquobehavioralrdquo classes with highest rates in the ldquobe-havioralrdquo class Further although executive functioningis part of cognition it appears that there are nuanceswithin the skills that make up this large construct in DSthat differentially impact functioningImportantly the current studyrsquos findings have identi-
fied three distinct subgroups of individuals with DS thatare likely also clinically meaningful When developinginterventions for individuals with DS researchers shouldconsider potential subgroups for which more targetedinterventions may work best rather than determining ef-ficacy (or lack thereof) among a large heterogeneousgroup These data also demonstrate the national move-ment towards precision medicine as applied to DS Takeas an example interventions for maladaptive behavior inindividuals with DS Although developmentally-basededucational intervention and behavioral managementprinciples still apply thoughtful consideration regardingwhen to introduce certain types of intervention and inwhat sequence is also important In addition consider-ation and treatment of underlying physiologic mecha-nisms that drive hyperactivityimpulsivity compulsiveperseverative behavior anxietyfearfulness mood irrit-ability and self-injury are important for these interven-tions because they can impact learning and adaptivefunction Similarly the physiologic consequences of un-treated medical comorbidities such as sleep disturbancedeprivation obstructive sleep apnea and thyroid imbal-ance can interfere with executive functioning self-regulation learning and development despite ongoingeducational and behavioral interventions Further inves-tigation into their role in shaping cognitive-behavioralsubtypes will be critical to developing more personalizedand precise treatments Long term taking a precisionmedicine approach optimizes neuromaturation and de-velopmental outcomes for individuals with DSVariability in cognition and behavior was not driven by
many of the demographic variables in our sample Theonly significant differences observed were that lower
cognitive functioning (IQ and visuospatial abilities) wasassociated with being male and lower household incomeHousehold income has been historically linked to childcognition [82] and male sex is a general risk factor forboth ASD and intellectual disability [83] Therefore futurework should also consider genetic and environmental dif-ferences as well as the interaction between the two toexplain the phenotypic profiles observed in this studyAdditional child (eg perinatal exposures) parental (egstress) and family-related (eg broader ASD phenotype insiblings) variables should be considered as wellThe field of DS research has expressed the need for
larger sample sizes that can capture the variability asso-ciated with the phenotype and that can begin to addresslarger questions regarding the mechanisms underlyingthe various expressions of the phenotype [5] A majorstrength of this study is that we achieved a large samplesize by gathering data across a network of sites This inturn allowed us to use modern statistical methods ap-propriate for larger samples to address the variabilityamong individuals with DSDespite the strengths of our large sample size we were
still limited by a convenience sample For example al-though our sample is in line with the US census data interms of the percentage of participants who were White[84] it differs in the distribution of minorities We had ahigher percentage of participants who were Asian and alower percentage who were Black and Hispanic Stillour sample was more ethnically diverse than many sam-ples of people with DS likely due to the larger samplesize and multiple sites Nonetheless further explorationof how these profiles appear in more diverse samples isneeded An additional limitation related to sampling isthat some of our measures were performance-based re-quiring families to participate in person Thus individ-uals and families unable to participate in demandingassessment batteries were excluded As a result ourfindings may underestimate the prevalence of those withmore behavioral and cognitive difficulties These individ-uals may present with a different profile than what wasrepresented in the three classes observed in the currentstudy For example they may constitute a fourth classfor which we did not have an adequate number of par-ticipants to adopt from our dataWe were limited also by the number of observations
for which we had an adequate sample size thus limitingthe measures included Some constructs were not repre-sented most notably language Because expressive lan-guage is an area of particular weakness in the DSphenotype and is often a target of interventions it iscritical to include moving forward Techniques such asexpressive language sampling will be particularly fruitfuldue to the ability to circumvent the issue of floor effectsassociated with standardized norm-referenced tests
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 10 of 14
while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

while preserving psychometric quality [85 86] To thispoint other measures of cognition in future researchshould be mindful of the assessment form and type ofscore used to minimize floor effects [87] Finally due tothe wide age range of participants we used age-corrected scores in analyses Although this approachminimized confounds it potentially limits our under-standing of age differences across the subgroups Futureresearch should consider whether the patterns observedacross subgroups of individuals with DS change overtime with age or across different developmental periods
ConclusionsAs Karmiloff-Smith et al emphasized we must considerindividual differences at multiple levels (eg genetic epi-genetic neural cognitive behavioral and environmental[5]) The current study took an important first step byidentifying within-syndrome patterns of cognition andbehavior Moving forward the identification of sub-groups within the phenotype associated with DS will bea catalyst for biomarker studies aimed at identifyingmechanisms underlying the variability observed in thephenotype To achieve the ultimate goal of more tar-geted interventions we need to better understand thepleiotropic effects observed among individuals with DSwho share a common genetic etiology
AbbreviationsDS Down syndrome LPA Latent profile analysis ASD Autism spectrumdisorder KBIT-2 Kaufman Brief Intelligence Test 2nd edition CANTAB Cambridge Neuropsychological Test Automated Battery BRIEF BehavioralRating Inventory of Executive Function SIB-R Scales of IndependentBehavior-Revised Short Form NCBRF Nisonger Child Behavior Rating FormSCQ Social Communication Questionnaire AIC Akaike information criterionSS-BIC Sample size-adjusted Bayesian information criterion VLMR Vuong-Lo-Mendell-Rubin BLRT Bootstrapped likelihood ratio M(CP) Mean classprobability FIML Full information maximum likelihood estimation
Supplementary InformationThe online version contains supplementary material available at httpsdoiorg101186s11689-021-09365-2
Additional file 1 Figure S1 Latent Profile Analysis 4-Class ModelNote All values are z-score transformed (M = 0 SD = 1) Higher scores onthe NCBRF SCQ and BRIEF indicate greater impairment higher scores onall other measures reflect less impairment
AcknowledgementsFirst and foremost we thank the families who devoted their time and effortto participate in this study We also thank the numerous Down SyndromeCognition Project staff and students who supported participant recruitmentdata collection and data management efforts at each site We thank MichaelHarpold whose tireless efforts on behalf of people with Down syndrome andhis specific advice and encouragement were critical to the success of thisproject The vision and support of the Anna and John Sie Foundation helpedto establish the LuMind Foundation and to sustain this effort
Authorsrsquo contributionsSS and RR conceived of and established the Down Syndrome CognitionProject and supervised all study efforts MMC and LM co-led this manuscriptwith primary roles in data collection data interpretation and drafting the
manuscript LK had a primary role in data analysis and assisted with data in-terpretation and drafting the manuscript SS and EMM helped with data in-terpretation and drafting the manuscript GC provided clinical interpretationof the data TR and DH had primary roles in data collection and data man-agement The authors read and approved the final manuscript
FundingFunding provided by LuMind Down Syndrome Research Foundation (PI RRand SS) supported the implementation of the Down Syndrome CognitionProject The Yellow Crayon Funds provided by the family of Joanna ElisabethStone supported recruitment efforts for the Down Syndrome CognitionProject Data analysis and interpretation was supported by the NIH-fundedIntellectual amp Developmental Disabilities Research Centers grant U54HD079123 awarded to the Kennedy Krieger Institute (PI Schlaggar)
Availability of data and materialsThe datasets used andor analyzed during the current study are availablefrom the corresponding author upon reasonable request
Declarations
Ethics approval and consent to participateThe Institutional Review Board at every participating site provided approvaland oversight to ensure ethical conduct of human subjects researchthroughout the study Informed consent was provided by all parentsguardians who participated Consent or assent was provided by eachparticipant with Down syndrome depending on age and consentingcapacity as determined by the Institutional Review Boards
Consent for publicationNot applicable
Competing interestsThe authors declare that they have no competing interests
Author details1University of Illinois at Urbana-Champaign 901 S Sixth St Champaign IL61820 USA 2Emory University 615 Michael St Atlanta GA 30322 USA3Kennedy Krieger Institute 801 N Broadway Baltimore MD 21205 USA4Kennedy Krieger Institute 1750 E Fairmount Ave Baltimore MD 21231 USA5Johns Hopkins School of Medicine 725 N Washington St Baltimore MD21205 USA 6Kennedy Krieger Institute Johns Hopkins School of PublicHealth 3901 Greenspring Avenue Baltimore MD 21211 USA
Received 16 July 2020 Accepted 3 April 2021
References1 Mai CT Isenburg JL Canfield MA Meyer RE Correa A Alverson CJ et al
National population-based estimates for major birth defects 2010ndash2014Birth Defects Res 2019111(18)1420ndash35 Available from httpsdoiorg101002bdr21589
2 Capone GT Chicoine B Bulova P Stephens M Hart S Crissman B et al Co-occurring medical conditions in adults with Down syndrome a systematicreview toward the development of health care guidelines Am J Med GenetA 2018176(1)116ndash33 Available from httpsdoiorg101002ajmga38512
3 Grieco J Pulsifer M Seligsohn K Skotko B Schwartz A Down syndromecognitive and behavioral functioning across the lifespan Am J Med Genet CSemin Med Genet 2015169(2)135ndash49 Available from httpsonlinelibrarywileycomdoiabs101002ajmgc31439
4 Schalock RL Borthwick-Duffy SA Bradley VJ Buntinx WH Coulter DL CraigEM et al Intellectual disability definition classification and systems ofsupports Washington DC American Association on Intellectual andDevelopmental Disabilities 2010
5 Karmiloff-Smith A Al-Janabi T DrsquoSouza H Groet J Massand E Mok K et alThe importance of understanding individual differences in Down syndromeF1000Res 201651ndash10 Available from httpsdoiorg1012688f1000research75061
6 Blair C Razza RP Relating effortful control executive function and falsebelief understanding to emerging math and literacy ability in kindergarten
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 11 of 14
Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

Child Dev 200778(2)647ndash63 Available from httpwwwncbinlmnihgovpubmed17381795
7 Gilotty L Kenworthy L Sirian L Black DO Wagner AE Adaptive skills andexecutive function in autism spectrum disorders Child Neuropsychol 20028(4)241ndash8 Available from httpsdoiorg101076chin8424113504
8 Gioia GA Isquith PK Kenworthy L Barton RM Profiles of everyday executivefunction in acquired and developmental disorders Child Neuropsychol20028(2)121ndash37 Available from httpsdoiorg101076chin821218727
9 Ready RE Stierman L Paulsen JS Ecological validity of neuropsychologicaland personality measures of executive functions Clin Neuropsychol 200115(3)314ndash23 Available from httpsdoiorg101076clin15331410269
10 Zingerevich C Patricia DL The contribution of executive functions toparticipation in school activities of children with high functioning autismspectrum disorder Res Autism Spectr Disord 20093(2)429ndash37 Availablefrom httpsdoiorg101016jrasd200809002
11 Tsao R Kindelberger C Variability of cognitive development in children withDown syndrome relevance of good reasons for using the clusterprocedure Res Dev Disabil 200930(3)426ndash32 Available from httpsdoiorg101016jridd200810009
12 Couzens D Cuskelly M Haynes M Cognitive development and Downsyndrome age-related change on the Stanford-Binet test Am J IntellectDev Disabil 2011116(3)181ndash204 Available from httpsdoiorg1013521944-7558-1163181
13 Sansone SM Schneider A Bickel E Berry-Kravis E Prescott C Hessl DImproving IQ measurement in intellectual disabilities using true deviationfrom population norms J Neurodev Disord 20146(1)16 Available fromhttpsdoiorg1011861866-1955-6-16
14 Rosser TC Edgin JO Capone GT Hamilton DR Allen EG Dooley KJ et alAssociations between medical history cognition and behavior in youthwith down syndrome a report from the down syndrome cognition projectAm J Intellect Dev Disabil 2018123(6)514ndash28 Available from httpsdoiorg1013521944-7558-1236514
15 Carr J Stability and change in cognitive ability over the life span acomparison of populations with and without Downrsquos syndrome J IntellectDisabil Res 200549(12)915ndash28 Available from httpsdoiorg101111j1365-2788200500735x
16 Channell MM Thurman AJ Kover ST Abbeduto L Patterns of change innonverbal cognition in adolescents with Down syndrome Res Dev Disabil201435(11)2933ndash41 Available from httpsdoiorg101016jridd201407014
17 Couzens D Cuskelly M Jobling A The Stanford Binet Fourth Edition and itsuse with individuals with Down syndrome cautions for clinicians Intl JDisabil Dev Educ 200451(1)39ndash56 Available from httpsdoiorg1010801034912042000182193
18 Hessl D Nguyen DV Green C Chavez A Tassone F Hagerman RJ et al Asolution to limitations of cognitive testing in children with intellectualdisabilities the case of fragile X syndrome J Neurodev Disord 20091(1)33ndash45 Available from httpsdoiorg101007s11689-008-9001-8
19 Maloney ES Larrivee LS Limitations of age-equivalent scores in reportingresults of norm-referenced tests Contemp Issues Commun Sci Disord 20073486ndash93 Available from httpspubsashaorgdoipdf101044cicsd_34_F_86
20 Kaufman AS Kaufman NL Kaufman Brief Intelligence Test AmericanGuidance Service 2004
21 Pulina F Vianello R Lanfranchi S Cognitive profiles in individuals withDown syndrome Int Rev Res Dev Disabil 20195667ndash92 Available fromhttpsdoiorg101016bsirrdd201906002
22 Lee NR Anand P Will E Adeyemi EI Clasen LS Blumenthal JD et al Everydayexecutive functions in Down syndrome from early childhood to youngadulthood evidence for both unique and shared characteristics compared toyouth with sex chromosome trisomy (XXX and XXY) Front Behav Neurosci20159264 Available from httpsdoiorg103389fnbeh201500264
23 Loveall SJ Conners FA Tungate AS Hahn LJ Osso TD A cross-sectionalanalysis of executive function in Down syndrome from 2 to 35 years J IntellectDisabil Res 201761(9) Available from httpsdoiorg101111jir12396
24 Baddeley A Working memory Science 1992255(5044)556ndash9 Availablefrom httpsdoiorg101126science1736359
25 Baddeley A Jarrold C Working memory and Down syndrome J IntellectDisabil Res 200751(12)925ndash31 Available from httpsdoiorg101111j1365-2788200700979x
26 Doerr E Carretti B Lanfranchi S The working memory of individuals withDown syndrome Int Rev Res Dev Disabil 20195693ndash121 Available fromhttpsdoiorg101016bsirrdd201906006
27 Godfrey M Lee NR Memory profiles in Down syndrome acrossdevelopment a review of memory abilities through the lifespan JNeurodev Disord 201810(1)5 Available from httpsdoiorg101186s11689-017-9220-y
28 Jarrold C Baddeley AD Phillips CE Verbal short-term memory in Downsyndrome J Speech Lang Hear Res 200245531ndash44 Available from httpsdoiorg1010441092-4388(2002042
29 Jarrold C Baddeley AD Short-term memory for verbal and visuospatialinformation in Downrsquos syndrome Cogn Neuropsychiatry 19972(2)101ndash22Available from httpsdoiorg101080135468097396351
30 Kittler P Krinsky-McHale SJ Devenny DA Semantic and phonological loopeffects on verbal working memory in middle-age adults with mentalretardation Am J Ment Retard 2004109(6)467ndash80 Available from httpsdoiorg1013520895-8017(2004)1093C467SAPLEO3E20CO2
31 Marcell MM Weeks SL Short-term memory difficulties and Downrsquossyndrome J Intellect Disabil Res 198832(2)153ndash62 Available from httpsdoiorg101111j1365-27881988tb01400x
32 Numminen H Service E Ahonen T Ruoppila I Working memory andeveryday cognition in adults with Downrsquos syndrome J Intellect Disabil Res200145(2)157ndash68 Available from httpsdoiorg101046j1365-2788200100298x
33 Kittler PM Krinsky-McHale SJ Devenny DA Dual-task processing as ameasure of executive function a comparison between adults with Williamsand Down syndromes Am J Ment Retard 2008113(2)117ndash32 Availablefrom httpsdoiorg1013520895-8017(2008)113[117DPAAMO]20CO2
34 Devenny DA Silverman WP Hill AL Jenkins E Sersen EA Wisniewski KENormal ageing in adults with Downrsquos syndrome a longitudinal study JIntellect Disabil Res 199640(3)208ndash21 Available from httpsdoiorg101111j1365-27881996tb00624x
35 Yang Y Conners FA Merrill EC Visuo-spatial ability in individuals with Downsyndrome is it really a strength Res Dev Disabil 201435(7)1473ndash500Available from httpsdoiorg101016jridd201404002
36 Carretti B Lanfranchi S Mammarella IC Spatial-simultaneous and spatial-sequential working memory in individuals with Down syndrome the effectof configuration Res Dev Disabil 201334(1)669ndash75 Available from httpsdoiorg101016jridd201209011
37 Carretti B Lanfranchi S The effect of configuration on VSWM performanceof Down syndrome individuals J Intellect Disabil Res 201054(12)1058ndash66Available from httpsdoiorg101111j1365-2788201001334x
38 Lanfranchi S Mammarella IC Carretti B Spatial-simultaneous working memoryand selective interference in Down syndrome Child Neuropsychol 201521(4)481ndash9 Available from httpsdoiorg101080092970492014913557
39 Laws G Working memory in children and adolescents with Downsyndrome evidence from a colour memory experiment J Child PsycholPsychiatr 200243(3)353ndash64 Available from httpsdoiorg1011111469-761000026
40 Ellis NR Woodley-Zanthos P Dulaney CL Memory for spatial location inchildren adults and mentally retarded persons Am J Ment Retard 198993(5)521ndash6
41 Lanfranchi S Carretti B Spanograve G Cornoldi C A specific deficit in visuospatialsimultaneous working memory in Down syndrome J Intellect Disabil Res200953(5)474ndash83 Available from httpsdoiorg101111j1365-2788200901165x
42 Ditterline J Oakland T Relationships between adaptive behavior andimpairment Relationships between adaptive behavior and impairment InAssessing impairment Boston Springer 2009 p 31ndash48 Available fromhttpwwwspringerlinkcomindex101007978-0-387-87542-2
43 Tasseacute MJ Luckasson R Schalock RL The relation between intellectualfunctioning and adaptive behavior in the diagnosis of intellectual disabilityIntellect Dev Disabil 201654(6)381ndash90 Available from httpsdoiorg1013521934-9556-546381
44 Miller LE Burke JD Troyb E Knoch K Herlihy LE Fein DA Preschoolpredictors of school-age academic achievement in autism spectrumdisorder Clin Neuropsychol 201731(2)382ndash403 Available from httpsdoiorg1010801385404620161225665
45 Woolf S Woolf CM Oakland T Adaptive behavior among adults withintellectual disabilities and its relationship to community independenceIntellect Dev Disabil 201048(3)209ndash15 Available from httpsdoiorg1013521944-7558-483209
46 Bornstein MH Hahn C-S Suwalsky JTD Physically developed andexploratory young infants contribute to their own long-term academic
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 12 of 14
achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

achievement Psychol Sci 201324(10)1906ndash17 Available from httpsdoiorg1011770956797613479974
47 Daunhauer LA The early development of adaptive behavior and functionalperformance in young children with Down syndrome current knowledgeand future directions Int Rev Res Dev Disabil 201140109ndash31 Availablefrom httpsdoiorg101016B978-0-12-374478-400005-8
48 Coe DA Matson JL Russell DW Slifer KJ Capone GT Baglio C et alBehavior problems of children with Down syndrome and life events JAutism Dev Disord 199929(2)149ndash56 Available from httpsdoiorg101023A1023044711293
49 Dykens EM Hodapp R Evans DW Profiles and development of adaptivebehavior in children with Down syndrome Am J Ment Retard 199498(5)580ndash7 Available from httpsdoiorg103104reprints293
50 van Duijn G Dijkxhoorn Y Scholte EM van Berckelaer-Onnes IA Thedevelopment of adaptive skills in young people with Down syndrome JIntellect Disabil Res 201054(11)943ndash54 Available from httpsdoiorg101111j1365-2788201001316x
51 Will EA Caravella KE Hahn LJ Fidler DJ Roberts JE Adaptive behavior ininfants and toddlers with Down syndrome and fragile X syndrome Am JMed Genet B Neuropsychiatr Genet 2018177(3) Available from httpsdoiorg101002ajmgb32619
52 Sabat C Arango P Tasseacute MJ Tenorio M Different abilities needed at homeand school The relation between executive function and adaptivebehaviour in adolescents with Down syndrome Scientific Rep 202010(1)1683 Available from httpsdoiorg101038s41598-020-58409-5
53 Capone GT Grados MA Kaufmann WE Bernad-Ripoll S Jewell A Downsyndrome and comorbid autism-spectrum disorder characterization usingthe aberrant behavior checklist Am J Med Genet A 2005134(4)373ndash80Available from httpsdoiorg101002ajmga30622
54 Ji NY Capone GT Kaufmann WE Kaufmann WE Krieger K Autism spectrumdisorder in Down syndrome cluster analysis of Aberrant Behaviour Checklistdata supports diagnosis J Intellect Disabil Res 201155(11)1064ndash77Available from httpsdoiorg101111j1365-2788201101465x
55 Carter JC Capone GT Gray RM Cox CS Kaufmann WE Autistic-spectrumdisorders in down syndrome further delineation and distinction from otherbehavioral abnormalities Am J Med Genet B Neuropsychiatr Genet 2007144B(1)87ndash94 Available from httpsdoiorg101002ajmgb30407
56 Hepburn SL Maclean WE Maladaptive and repetitive behaviors inchildren with Down syndrome and autism spectrum disordersimplications for screening J Ment Health Res Intellect Disabil 20092(2)67ndash88 Available from httpsdoiorg10108019315860802627627
57 Dykens EM Psychiatric and behavioral disorders in persons with Downsyndrome Ment Retard Dev Disabil Res Rev 200713(3)272ndash8 Availablefrom httpsdoiorg101002mrdd
58 van Gameren-Oosterom HBM Fekkes M Buitendijk SE Mohangoo AD BruilJ van Wouwe JP Development problem behavior and quality of life in apopulation based sample of eight-year-old children with down syndromePLoS ONE 20116(7)16ndash20 Available from httpsdoiorg101371journalpone0021879
59 van Gameren-Oosterom HBM Fekkes M van Wouwe JP Detmar SBOudesluys-Murphy AM Verkerk PH Problem behavior of individuals withdown syndrome in a nationwide cohort assessed in late adolescence JPediatr 2013163(5)1396ndash401 Available from httpsdoiorg101016jjpeds201306054
60 Visootsak J Sherman S Neuropsychiatric and behavioral aspects of trisomy21 Curr Psychiatry Rep 20079(2)135ndash40 Available from httpsdoiorg101007s11920-007-0083-x
61 Glennon JM Karmiloff-Smith A Thomas MSC Syndromic autismprogressing beyond current levels of description Rev J Autism Dev Disord20174(4)321ndash7 Available from httpsdoiorg101007s40489-017-0116-2
62 Moss J Howlin P Autism spectrum disorders in genetic syndromesimplications for diagnosis intervention and understanding the wider autismspectrum disorder population J Intellect Disabil Res 200953(10)852ndash73Available from httpsdoiorg101111j1365-2788200901197x
63 Warner G Moss J Smith P Howlin P Autism characteristics and behaviouraldisturbances in sim500 children with Downrsquos syndrome in England and WalesAutism Res 20147(4)433ndash41 Available from httpsdoiorg101002aur1371
64 Moss J Richards C Nelson L Oliver C Prevalence of autism spectrumdisorder symptomatology and related behavioural characteristics inindividuals with Down syndrome Autism 201217(4)390ndash404 Availablefrom httpsdoiorg1011771362361312442790
65 Channell MM Hahn LJ Rosser TC Hamilton D Frank-Crawford MA CaponeGT et al Characteristics associated with autism spectrum disorder risk inindividuals with Down syndrome J Autism Dev Disord 201949(9)3543ndash56Available from httpsdoiorg101007s10803-019-04074-1
66 Lecavalier L Phenotypic variability in autism spectrum disorder clinicalconsiderations In Davis III T White S Ollendick T editors Handbook of Autismand Anxiety Autism and Child Psychopathology Series Cham Springer 2014p 15ndash29 Available from httpsdoiorg101007978-3-319-06796-4_2
67 Edgin JO Anand P Rosser T Pierpont EI Figueroa C Hamilton D et al TheArizona Cognitive Test Battery for Down Syndrome test-retest reliability andpractice effects Am J Intellect Dev Disabil 2017122(3)215ndash34 Availablefrom httpsdoiorg1013521944-7558-1223215
68 Edgin JO Mason GM Allman MJ Capone GT DeLeon I Maslen C et alDevelopment and validation of the Arizona Cognitive Test Battery for Downsyndrome J Neurodev Disord 20102(3)149ndash64 Available from httpsdoiorg101007s11689-010-9054-3
69 Harris PA Taylor R Thielke R Payne J Gonzalez N Conde JG Researchelectronic data capture (REDCap)-a metadata-driven methodology andworkflow process for providing translational research informatics support JBiomed Inform 200942(2)377ndash81 Available from httpsdoiorg101016jjbi200808010
70 Korkman M Kirk U Kemp S NEPSY II clinical and interpretive manual 2nded San Antonio Harcourt Assessment PsychCorp 2007
71 Gioia GA Isquith P Guy S Kenworthy L Behavior Rating Inventory ofExecutive Function professional manual Lutz Psychological AssessmentResources 2000
72 Bruininks RH Woodcock RW Weatherman RF Hill BK SIB-R Scales ofIndependent Behavior-Revised Itasca Riverside Publishing 1996
73 Aman MG Tasseacute MJ Rojahn J Hammer D The Nisonger CBRF a childbehavior rating form for children with developmental disabilities Res DevDisabil 199617(1)41ndash57 Available from httpsdoiorg1010160891-4222(95)00039-9
74 Rutter M Bailey A Lord C The Social Communication Questionnairemanual Los Angeles Western Psychological Services 2003
75 Hagenaars JA McCutcheon AL Applied latent class analysis New YorkCambridge University Press 2002
76 Jung T Wickrama KAS An introduction to latent class growth analysis andgrowth mixture modeling Soc Personal Psychol Compass 20082(1)302ndash17Available from httpsdoiorg101111j1751-9004200700054x
77 Nylund KL Asparouhov T Mutheacuten BO Deciding on the number of classesin latent class analysis and growth mixture modeling a Monte Carlosimulation study Struct Equ Model 200714(4)535ndash69 httpsdoiorg10108010705510701575396
78 Mutheacuten LK Mutheacuten BO Mplus statistical software 200779 StataCorp Stata 150 [computer software] 201780 Cham H Reshetnyak E Rosenfeld B Breitbart W Full information maximum
likelihood estimation for latent variable interactions with incompleteindicators Multivariate Behav Res 201752(1)12ndash30 Available from httpsdoiorg1010800027317120161245600
81 de Bildt A Sytema S Kraijer D Sparrow S Minderaa R Adaptive functioningand behaviour problems in relation to level of education in children andadolescents with intellectual disability J Intellect Dev Res 200549(9)672ndash81Available from httpsdoiorg101111j1365-2788200500711x
82 von Stumm S Plomin R Socioeconomic status and the growth ofintelligence from infancy through adolescence Intell 20154830ndash6Available from httpsdoiorg101016jintell201410002
83 Constantino JN Charman T Diagnosis of autism spectrum disorderreconciling the syndrome its diverse origins and variation in expressionLancet Neurol 201615(3)279ndash91 Available from httpsdoiorg101016S1474-4422(15)00151-9
84 US Census Bureau Race Available from httpswwwcensusgovtopicspopulationracehtml Accessed 8 July 2020
85 Channell MM Loveall SJ Conners FA Harvey DJ Abbeduto L Narrativelanguage sampling in typical development implications for clinical trialsAm J Speech Lang Pathol 201827123ndash35 Available from httpsdoiorg1010442017_AJSLP-17-0046
86 Abbeduto L Berry-Kravis E Sterling A Sherman S Edgin JO McDuffie Aet al Expressive language sampling as a source of outcome measures fortreatment studies in fragile X syndrome feasibility practice effects test-retest reliability and construct validity J Neurodev Disord 202012(1)1ndash23Available from httpsdoiorg101186s11689-020-09314-5
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 13 of 14
87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14

87 Esbensen AJ Hooper SR Fidler D Hartley SL Edgin J dArdhuy XL et alOutcome measures for clinical trials in down syndrome Am J Intellect DevDisabil 2017122(3)247ndash81 Available from httpsdoiorg1013521944-7558-1223247
Publisherrsquos NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations
Channell et al Journal of Neurodevelopmental Disorders (2021) 1316 Page 14 of 14