Embed Size (px)
Citation preview

Cannabis-Sensitive Dopaminergic Markers inPostmortem Central Nervous System: Changes inSchizophrenia
Brian Dean, Robyn Bradbury, and David Leon Copolov
Background: This study investigated if changes in pre-synaptic markers on dopaminergic neurons (dopaminetransporter [DAT], tyrosine hydroxylase [TH]) werepresent in the caudate from subjects with schizophreniawho had �9(�)tetrahydrocannabinol (THC) in their bloodat autopsy. These changes were posited because animalstudies show that treatment with THC decreases dopamineuptake and TH in the striatum.
Methods: Studies utilized caudate, obtained postmortem,from 14 schizophrenic and 14 control subjects.[3H]mazindol binding to caudate, measured using auto-radiography, was taken as a measure of DAT; TH levelswere estimated using an antihuman TH antibody andWestern blotting.
Results: There was decreased [3H]mazindol binding toDAT in the caudate from the schizophrenic subjects withno detectable blood THC levels (THC(�)) compared withTHC(�) control subjects (mean � SEM: 240 � 19 vs. 296� 14 fmol/mg estimated tissue equivalents, p � .01).There were no significant differences between levels ofDAT in the caudate from schizophrenic and controlsubjects that had THC in their blood. Tyrosine hyroxylasewas not different in any diagnostic cohort.
Conclusions: Our data suggests that DAT is decreased inthe caudate from THC(�) subjects with schizophrenia, achange that may be reversed by ingesting THC fromcannabis. Biol Psychiatry 2003;53:585–592 © 2003 So-ciety of Biological Psychiatry
Key Words: Dopamine transporter, tyrosine hydroxylase,caudate-putamen, substantia nigra, schizophrenia, canna-bis
Introduction
We have recently reported that the cannabinoid1 (CB1)receptor is increased in the frontal cortex of subjects
with schizophrenia and in the caudate-putamen (CP) ofsubjects who had �9(�)tetrahydrocannabinol (THC) de-tected in their blood at autopsy, whether or not they hadschizophrenia (Dean et al 2001). The CB1 receptor is thesite in the brain where both endogenous cannabinoids andthe active component of cannabis, THC (Ameri 1999), areproposed to exert their effects. Thus our data, plus thefinding that there are elevated levels of endogenouscannabinoids in the cerebral spinal fluids from subjectswith schizophrenia (Leweke et al 1999), suggest a role forthe cannabinoid system in the pathology of schizophrenia.Moreover, clinical data suggesting that cannabis use ex-acerbates existing psychoses (Hollister 1998) raises thepossibility that inhalation of THC may modulate pathwaysin the brain that are central to psychoses.
It is still not clear which systems in the brain becomedysfunctional to induce the onset of psychoses; however,studies showing that dopamine receptor agonists cause orworsen psychoses, whereas dopamine2 receptor antago-nists act as antipsychotic agents, have underpinned thelong-standing dopamine hypothesis of schizophrenia(Meltzer and Stahl 1976). This hypothesis suggests thatoveractive dopaminergic systems in the central nervoussystem (CNS) are central to the genesis of psychoses.Based on the dopamine hypothesis of schizophrenia, it canbe postulated that any effects of THC inhalation thatincrease the activity of the dopaminergic system in theCNS could cause or exacerbate psychoses.
The difficulties in studying the effect of the inhalationof cannabis in human CNS have resulted in studies on theeffects of THC in animals. One such study showed thatTHC both inhibits dopamine uptake and facilitates itsrelease by rat striatal synaptosomes (Sakurai-Yamashita etal 1989). From these data, it was concluded that THC actsto stimulate nigrostriatal dopaminergic pathways in the rat.A more recent study has shown that anandamide, theendogenous ligand for cannabinoids receptors (Ameri
From The Rebecca L. Cooper Research Laboratories, The Mental Health ResearchInstitute of Victoria, Parkville, Victoria, Australia.
Address reprint requests to Brian Dean, The Rebecca L. Cooper ResearchLaboratories, Mental Health Research Institute of Victoria, Locked Bag 11,Parkville, Victoria 3052, Australia.
Received March 20, 2002; revised May 31, 2002; accepted July 14, 2002.
© 2003 Society of Biological Psychiatry 0006-3223/03/$30.00doi:10.1016/S0006-3223(03)01545-7

1999), increases the release of dopamine in the striatum(Cadogan et al 1997) and mesolimbic system (Gessa et al1998) of the CNS by activating the CB1 receptor. Thesedata suggest that the CB1 receptor may have a physiologicrole in regulating dopaminergic activity.
Further evidence to support the role of THC as ageneralized activator of the dopaminergic systems of theCNS has come from the study of tyrosine hydroxylase(TH), a rate-limiting enzyme in the synthesis of dopamine(Mallet 1996). A number of studies in rats have shown thatexposure to THC increases both the activity and expres-sion of TH (Bonnin et al 1996; Hernandez et al 1997).Both these findings suggest that THC would cause anincrease in the synthesis of catecholamines, includingdopamine, a hypothesis supported by the demonstrationthat THC increases the rate of conversion of radioactivetyrosine to radioactive dopamine (Rodriguez et al 1990).
Therefore, if animal studies are reflective of the actionof THC in human CNS, it would be predicted thatinhalation of cannabis would act to increase dopaminesynthesis and release while inhibiting the clearance of theneurotransmitter via the dopamine transporter (DAT).Such a series of outcomes would most likely increaselevels of extra-neuronal dopamine, increasing the activityof dopaminergic pathways in the brain and hence, accord-ing to the dopamine hypothesis of schizophrenia, wouldeither cause or exacerbate psychoses. To further ourstudies on the possible role of the cannabinoid systemand/or its pharmacologic manipulation in psychoses, wehave now examined the status of critical cannabis-sensi-tive dopaminergic markers in brains from subjects withschizophrenia and subjects who had inhaled cannabis neartime of death. To parallel studies in animals, it would havebeen necessary to measure the activity of the dopamineuptake system and TH in human brain, but such measure-ments are affected by minor variations in tissue collectionand processing (Yoshimoto et al 1993). Thus, we electedto use in situ radioligand binding to measure the density ofDAT in the striatum and Western blots to measure thelevels of TH in the caudate and substantia nigra (SN); bothof these proteins have been shown to be stable postmortem(Dean and Hussain 2001; Torack and Morris 1992). Ourstudies have initially focused on the nigrostriatal areasbecause studies suggest that the dopaminergic pathwaysbetween these regions are affected by both THC (Sakurai-Yamashita et al 1989) and the pathology of schizophrenia(Risch 1996).
Methods and Materials
Materials[3H]mazindol was obtained from NEN Life Sciences Products(Boston, MA). [3H]microscales and Hyperfilm ECL (enhanced
chemiluminescence) were obtained from Amersham Australia (Syd-ney, Australia). BAS-TR plates were obtained from Fuji Photo Film(Tokyo, Japan). Mouse monoclonal antihuman TH was obtainedfrom Chemicon Australia (Boronia, Australia). Mazindol was a giftfrom Sandoz (Sydney, Australia), and desmethylimipramine (DMI)was from Research Biochemicals and obtained, like all otherchemicals and the rabbit antimouse immunoglobulin G (IgG)antibody couple to horseradish peroxidase, from Sigma Aldrich(Castle Hill, New South Wales, Australia). Pierce Supersignalchemiluminescent kit was obtained from Pierce Biotechnology(Rockford, IL). All materials used in Western blots were obtainedfrom Bio-Rad Laboratories (Regents Park, Australia).
Tissue CollectionFollowing ethical approval from the North-Western Health CareHuman Research and Ethics Committees, CP and SN were collectedat autopsy from the left brain hemisphere of 14 subjects with aprovisional diagnosis of schizophrenia suggested in a police reportof death to the coroner and from 14 subjects with no known historyof psychiatric illness (control subjects) (Table 1). All tissue wascollected at the Victorian Institute of Forensic Medicine, follow-ing approved procedures and after consultation with the next ofkin, where a forensic neuropathologist carried out a neuropatho-logical examination. The control subjects were matched forgender and were of a similar age to the schizophrenic subjects.
To minimize variation in experimental parameters, all tissueblocks were prepared by standardized procedures. Thus, blocksof CP were taken from a rostral region so as to include thenucleus accumbens and exclude the globus pallidus (pars latera-lis). Substantia nigra tissue was from the “rostral” component ofthe structure at the level of the subthalamic nucleus in a coronalsection. We did not delineate between the pars compacta(ventral) and the pars reticulata (dorsal) components of thenucleus; hence both cell types were within SN homogenates. Theblocked tissue was rapidly frozen to �70°C and stored at thistemperature until required.
In cases where death did not involve suicide, tissue wascollected from subjects whose death was witnessed, and thepostmortem interval (PMI) was the time from death to autopsy.In cases of suicide, tissue was only taken from individuals seenalive within 5 hours of being found dead. In such cases, the PMIwas the interval between the donor being found dead and autopsyplus half the time between when they were last seen alive andfound dead. In all cases, the cadavers were refrigerated within 5hours of being found.
The provisional diagnosis of schizophrenia was confirmed bya senior psychologist and senior psychiatrist after an extensivecase history review using the Diagnostic Instrument for BrainStudies (Hill et al 1996), a structured instrument for the collec-tion of clinical, pharmacologic, and other relevant informationfrom case histories. In this study, the diagnosis of schizophreniawas made according to DSM-IV criteria (American PsychiatricAssociation 1994). In addition to the DSM-IV diagnosis ofschizophrenia, there were two schizophrenic subjects who wouldfulfill the DSM-IV criteria for cannabis abuse at death (subjects4 and 5) and two subjects who would have fulfilled those criteriaduring their lifetime (2 and 3) but not at death. Two of the
586 B. Dean et alBIOL PSYCHIATRY2003;53:585–592

schizophrenic subjects (6 and 10) would fulfill the DSM-IVcriteria for alcohol abuse. There was no evidence to suggest thatany of the schizophrenic subjects would fulfill the DSM-IVcriteria for the abuse of other substances, and there was noevidence that any of the control subjects would have fulfilled anyof the DSM-IV criteria for the abuse of any substance.
Duration of illness (DOI) was calculated as the time from firsthospital admission to death. In addition, information on the typeand amount of antipsychotic drugs prescribed close to death wasobtained from the case history, and the final recorded dose (FRD)
of antipsychotic drug was converted to chlorpromazine equiva-lents (Soulsby 1999). Toxicology reports were examined toidentify which subjects had detectable levels of THC in bloodtaken at autopsy, and case histories were carefully examined forany suggestion of cannabis use. Because of the many confound-ing variables that influence the levels of THC and its metabolitesin blood, the presence of these compounds in blood of subjectsfrom whom CNS was collected can only be interpreted asindicating that cannabis had been inhaled, most likely within 2weeks before autopsy (Solowij 1998).
Table 1. Demographic Data from, and Radioligand Data for, Schizophrenic and Control Subjects from Whom Brain Tissue WasObtained Postmortem for the Study of CB1 Receptors
ID SexAge(y)
PMI(hr) pH
DOI(y) FRD THC Cause of death
[3H]mazindolbinding (mol/
mg ETE)
Tyrosinehydroxylase
(optical density)
Caudate Caudate SN
Schizophrenic1 M 25 49 6.38 2 200 DET Suicide: overdose of mixed drugs 248 .12 .122 M 22 37 6.07 3 450 DET Pericarditis 280 .14 .053 F 35 15 6.26 7 300 75 Coronary arterial thrombosis 273 .08 .104 M 41 31 6.20 11 500 10 Suicide: combined drug toxicity 278 .08 .115 M 45 68 6.48 12 300 15 Suicide: hanging 304 .13 .166 M 38 40 5.52 15 160 Mediastinitis 222 .13 .117 M 36 38 6.04 12 200 Suicide: overdose amitryptiline 273 .10 .128 M 42 47 6.26 22 1000 Coronary arterial atheroma 306 .11 .139 F 27 41 5.85 10 750 Suicide: asphyxia 191 .03 .1310 M 44 32 6.28 23 600 Ischemic heart disease 184 .03 .1011 M 48 30 6.62 24 1250 Bronchopneumonia 341 .14 .1012 M 55 25 6.10 33 400 Coronary arterial atheroma 146 .09 .1313 M 23 43 6.40 6 1750 Suicide: hanging 194 .36 .0214 F 36 45 6.28 4 160 Suicide: CO poisoning 254 .13 .03Analyses
THC(�) Mean 34 40 6.27 7.0 350 277 .11 .11SEM 4.4 8.9 .07 2.0 55 8.9 .01 .02
THC(�) Mean 39 38 6.15 16.6 697 240 .12 .10SEM 3.3 2.5 .10 3.2 184 19 .02 .01
Control15 M 30 27 5.86 23 Coronary arterial atheroma 326 .10 .1416 M 26 24 6.42 30 Electrocution 306 .11 .1317 M 25 50 6.48 85 Exsanguination 303 .12 .1318 M 29 15 6.46 14 Congestive cardiac failure 280 .15 .1319 F 21 58 6.03 Myocarditis 214 .07 .0220 F 32 56 6.16 Coronary arterial atheroma 240 .09 .1621 M 25 36 6.15 Right ventricular hypertrophy 361 .10 .1222 M 42 26 6.32 Coronary arterial atheroma 334 .13 .0923 M 30 24 6.46 Electrocution 288 .08 .1124 M 38 46 6.42 Trauma and asphyxia 329 .11 .0925 M 50 69 6.43 Ischemic heart disease 294 .09 .0826 M 23 36 6.13 Asthma 321 .06 .1027 M 43 45 6.25 Drowning 289 .11 .1028 M 21 51 6.58 Exsanguination 286 .10 .10Analyses
THC(�) Mean 38 29 6.31 304 .12 .13SEM 1.2 7.5 .14 9.4 .01 .002
THC(�) Mean 33 45 6.29 296 .09 .10SEM 3.3 4.6 .06 14 .006 .01
CB1, cannabinoid1; PMI, postmortem interval; DOI, duration of illness; FRD, final recorded antipsychotic drug dose (chlorpromazine equivalents per day); THC, blood�9(�) tetrahydrocannabinol levels (ng/mL: DET, detected but below sensitivity of assay); ETE, estimated tissue equivalent; SN, substantia nigra; M, male; F, female.
Dopamine Markers in Schizophrenia 587BIOL PSYCHIATRY2003;53:585–592

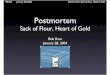
Measurement of [3H]mazindol BindingFor this study, 5 � 20 �m frozen tissue sections (�20°C) werecut from the CP from each subject so that a portion of the sectionwas missing an area of tissue that was included in the materialexcised for a Western blot (Figure 1). The specific binding of[3H]mazindol (15 nmol/L) to DAT was taken as the difference inbinding of radioligand in the presence of .3 �mol/L DMI minusbinding in the presence of DMI and mazindol (1 �mol/L) afterincubating in 50 mmol/L Tris buffer containing 300 mmol/LNaCl and 5 mmol/L KCl for 60 min at 4°C (Javitch et al 1983).The presence of [3H]mazindol at greater than three times its Kdfor binding means this study used single saturation analysis toestimate the density of binding. In such studies, specific bindingis a good estimate of the density of radioligand binding sites inthe tissue (Rodbard 1981).
After incubating with radioligand, all sections were washedtwice in ice-cold assay buffer, dipped into ice-cold distilled
water, and then thoroughly dried. The washed sections were thenfixed overnight in paraformaldehyde fumes in a desiccator. Thefixed sections and a set of [3H]microscales were then apposedagainst a BAS-TR2025 imaging plate for 7 days before the platewas scanned in the BAS 5000 phosphoimager. The density of theresulting phosphoimages was then compared with the density ofthe [3H]microscales using Analytical Imaging Station (AIS)image analysis software (Imaging Research, St. Catharines,Canada) to obtain results as dpm/mg estimated tissue equivalents(ETE). These results were then transformed to fmol radioligandbound/mg ETE (fmol/mg ETE).
Measurement of Tyrosine HydroxylaseTissue for the analysis of TH was collected from the caudate (seeFigure 1) and SN from the subjects used in the study of[3H]mazindol binding. The tissue from both regions was homog-enized with five strokes of a Teflon-glass homogenizer into 20mmol/L Tris-HCl, pH 7.4, containing .2 mmol/L ethylene glycolbis-(2 aminoethyl)-N,N,N�,N� tetraacetic acid and .1 mmol/Lethylenediaminetetraacetic acid with the protease inhibitors phe-nylmethylsulfonylfluoride (1 mmol/L), leupeptin (10 �g/mL),benzamidine (1 mmol/L), bacitracin (1 mg/mL), pepstatin (10�g/mL), and chymostatin (10 �g/mL) being added on the day ofuse. The brain homogenates were stored on ice until the concen-tration of protein in each sample was determined using theBio-Rad protein assay and then stored at �70°C.
On the day of assay, homogenates were thawed and denaturedby heating at 95°C for 4 min after being diluted in an equalvolume of electrophoresis buffer (.5 mol/L Tris-HCl, pH 6.8,containing 20% glycerol, 10% sodium dodecyl sulfate (SDS),10% 2--mercaptoethanol, and .05% bromophenol blue). Ho-mogenates (10 �g/protein per well) were then loaded onto 4%SDS stacking gels and separated on 10% SDS minigels. Theproteins were then transferred from the minigel to nitrocellulosemembrane (Bio-Rad: Trans-Blot Transfer Medium) in Towbintransfer buffer (25 mmol/L Tris, pH 8.3, containing 192 mmol/Lglycine and 20% methanol) overnight in a Bio-Rad Mini Trans-blot electrophoretic transfer cell. The proteins on each nitrocel-lulose membrane were stained with .2% Ponceau S Red in 3%trichloroacetic acid to ensure transfer had occurred.
The nitrocellulose membranes containing the separated pro-teins were placed in Tween Tris-buffered saline (TTBS: 100mmol/L Tris, pH 7.5, containing .9% sodium chloride, 5%blotting grade nonfat milk, and .1% Tween 20) for 1 hour atroom temperature with agitation. The proteins on the nitrocellu-lose membrane were then exposed to a mouse monoclonalantihuman TH diluted 1:1000 in blocking buffer for 1 hour atroom temperature with agitation. The solution containing theantihuman TH was then removed, and the nitrocellulose mem-brane washed 6� for 5 min with TTBS for 30 min. Thenitrocellulose membrane was then exposed to a rabbit antimouseIgG antibody couple to horseradish peroxidase diluted 1:2000 inblocking buffer for 1 hour at room temperature with agitation.The nitrocellulose membranes were then washed as occurredafter the incubation with the antihuman TH antibody.
The washed nitrocellulose membranes were transferred to a cleantray and exposed to the substrate solution from the Pierce Super-
Figure 1. (A) Typical high-resolution phosphoimages showing[3H]mazindol binding to human caudate-putamen in the absence(total binding) and presence (NSB) of 1 � mazindol. (B) Thespecific (total binding � NSB) binding of [3H]mazindol to thecaudate from schizophrenic and control subjects who hadTHC(�) or had not THC(�) inhaled cannabis close to death.ETE, estimated tissue equivalents; THC, �9(�)tetrahydrocan-nabinol. NSB, non-specific binding.
588 B. Dean et alBIOL PSYCHIATRY2003;53:585–592

signal chemiluminescent kit for 5 min at room temperature withagitation. Following the removal of excess substrate solution, thenitrocellulose film was placed between two pieces of transparentfilm. In a darkroom, a piece of enhanced chemiluminescence (ECL)film was opposed to the nitrocellulose membrane in the pieces oftransparent film for between 15 and 45 sec, depending on thestrength of the chemiluminescent signal. The ECL film was thendeveloped in Kodak D-19 x-ray developer and fixed with x-ray fixer.Once the ECL film was dry, it was imaged using an analog cameraand the optical density (OD) of the image measured using aMicrocomputer Imaging Device (MCID) image analysis system(Imaging Research, St. Catharines, Canada). To control for blot-to-blot variation, the ECL film was exposed so that the OD of astandard membrane preparation run on every gel was effectivelyconstant (inter-assay variation 5%).
Statistical AnalysisAll statistical analyses were carried out using GraphPad Prism.Each data set was analyzed using the Kolmogorov-Smirnov testto determine if the distribution of the data was parametric. Dataon [3H]mazindol binding and TH within region were comparedusing a two-way analysis of variance (ANOVA) with a post hocBonferonni correction, using diagnosis and drug status as vari-ables. Student’s t tests were used to determine if there were anysignificant differences in the FRD or DOI between the THC(�)and THC(�) subjects with schizophrenia. Correlations betweenradioligand binding and TH levels with demographic data andconfounding factors were expressed as a Pearson Product–Moment assuming a straight-line best fit.
Results
Because of the collection procedure described, there wereno significant differences in the age, PMI, or brain pHbetween the four cohorts of schizophrenic or controlsubjects, whether they did (THC(�)) or did not (THC(�))have THC in their blood at autopsy (Table 1).
All data sets were normally distributed, allowing para-metric analysis. No significant difference in the density of[3H]mazindol binding could be detected across the CPwithin donor. Thus, for consistency with the data fromWestern blotting, we report only data from the caudate.
Two-way ANOVA revealed that there was significantvariation in the density of [3H]mazindol binding to thecaudate with diagnosis [F(1,25) � 5.0, p .05; Table 1]but not with drug status (THC(�) vs. THC(�)) [F(1,25)� 1.5, p � .23]. There was also no significant interactionbetween the two variables [F(1,25) � .6, p � .44]. Posthoc Bonferonni analysis revealed that the source of sig-nificant variation in [3H]mazindol binding with diagnosiswas because of a decrease in [3H]mazindol binding tocaudate from the THC(�) schizophrenic subjects whencompared with the THC(�) control subjects (Table 1;Figure 1).
There was no significant variance in TH levels withdiagnosis [Caudate: F(1,25) � .25, p � .62; SN: F(1,25)� .42, p � .52; Table 1] or drug status [Caudate; F(1,25)� .05, p � .83; SN: F(1,25) � 2.3, p � .14), and there wasno interaction between the two variables (Caudate: F(1,25)� .60, p � .45; SN: F(1,25) � .59, p � .45) (Table 1,Figure 2).
There were no significant differences in the mean FRD(All: p � .46; SN: p � .47) or DOI (All: p � .11; SN: p� .12) between the THC(�) and THC(�) schizophrenicsubjects (Table 1). There were no significant correlationsbetween [3H]mazindol binding or TH in either brainregion with age, PMI, brain pH, DOI, FRD, or blood druglevels at death.
Discussion
This study has shown that there is a decrease in[3H]mazindol binding in the caudate from THC(�)schizophrenic subjects compared with that in the THC(�)control subjects, which was not apparent between the samediagnostic cohorts who had inhaled cannabis close todeath. Under the conditions used in this study, [3H]mazin-dol would predominantly bind to the DAT (Javitch et al1983). Thus these data support earlier findings that there isa decrease in DAT in the CP from subjects with schizo-phrenia (Dean and Hussain 2001; Joyce et al 1988). In the
Figure 2. Typical Western blot showing tyrosine hydroxylase inhomogenate from the caudate of a schizophrenic (A) and control(B) subject as well as the standard membrane preparation (C) runon every gel to accommodate gel-to-gel variation. MW, molec-ular weight.
Dopamine Markers in Schizophrenia 589BIOL PSYCHIATRY2003;53:585–592

same cohorts of subjects, we showed that levels of THwere not different in either the caudate or SN fromschizophrenic and control subjects whether or not they hadTHC in their blood at autopsy. In the case of both DATand TH it is important to note that the design of this studymeans it is not controlled or randomized, and this limitsthe overall interpretation of these data; however, the studyis relevant as it is the first to attempt to obtain data on theeffect of cannabis ingestion on what are thought to becannabis-sensitive markers on dopaminergic neurons inpostmortem human brain from subjects with schizophreniaand how such changes may be related to psychotic illness.
The hypothesis tested in this study was that cannabisinhalation would effect critical dopaminergic markers inthe brain, leading to overactive dopaminergic pathwaysand hence causing or worsening psychoses. In the rat, oneresponse to THC was a decrease in dopamine uptake bystriatal synaptosomes (Sakurai-Yamashita et al 1989). TheDAT is now recognized as the most critical component ofthe dopamine uptake mechanism of neurons (Amara1993), and the level of dopamine uptake is related to thelevel of the DAT (Schoemaker et al 1985). If these datawere applicable in humans, it would be predicted thatlevels of DAT would be decreased in subjects who hadrecently inhaled cannabis. Our data showing that neitherTHC(�) schizophrenic nor THC(�) control subjects haddecreased levels of DAT in the caudate, which does notsupport the hypothesis that cannabis inhalation causeschanges in DAT; however, we cannot exclude the possi-bility that changes in the activity of DAT can occurwithout changes in the levels of DAT protein. In addition,the intake of THC in humans is by inhalation, whereasstudies in animals either apply THC directly to isolatedbrain preparations or are given via injection. Therefore, itremains possible that differences in administration routes,or in the actions of pure THC versus THC inhaled fromcannabis, could account for the apparent differing effectsof THC on DAT in animal and human CNS.
The recent availability of suitable ligands to measureDAT using positron emission tomography and singlephoton emission computed tomography have resulted in anumber of studies in schizophrenia. Two of these studieshave reported no differences in levels of DAT in thestriatum of subjects with schizophrenia (Laruelle et al2000; Lavalaye et al 2001). By contrast, one study hasreported an absence of a right–left asymmetry in DAT insubjects with schizophrenia (Laakso et al 2000), andanother suggests there may be a loss of DAT in thestriatum from a subset of subjects with chronic schizo-phrenia (Laakso et al 2000, 2001). Our study only exam-ined DAT levels in one hemisphere, and therefore wecannot comment on asymmetry; however, we did notobserve any relationship between levels of DAT and DOI,
and therefore our data would not support the hypothesisthat decreases in DAT are related to the chronic form ofschizophrenia.
Overall, neuroimaging data does not suggest that thereis a decrease in DAT in schizophrenia; however, it isimportant to note that our data suggest that changes inDAT may not be apparent in subjects who have ingestedTHC close to death or, in the case of neuroimaging, closeto testing. It is not clear whether the existing neuroimagingstudies have taken cannabis use into account; however,given the relatively high incidence of cannabis use inschizophrenia (Johns 2001), controlling for this confound-ing factor could be critical in identifying the changes inDAT we report in this study.
There are a number of studies that show that THCincreases the activity, levels, and expression of TH in therat brain (Bonnin et al 1996; Hernandez et al 1997;Rodriguez et al 1990). By contrast, we have found that THis not increased in either the caudate or SN from THC(�)subjects. This does not suggest that TH changes acutelyafter the inhalation of cannabis in humans. Again, differ-ences in results because of drug purity and/or routes ofadministration cannot be excluded as an explanation ofresults in animals and humans; however, our current datawould not support the hypothesis that the inhalation ofTHC from cannabis is associated with short-term changesin TH that would be consistent with an activation of thenigrostriatal dopaminergic pathways and subsequent onsetor worsening of psychoses.
One confounding factor in this study is that tissue wasobtained from subjects that have received antipsychoticdrugs during their lifetime. This raises the possibility thatthe changes we have observed in DAT are due to antipsy-chotic drug effects and not associated with the pathologyof the schizophrenia. Against this argument is the repeatedfinding that treating rats with antipsychotic drugs does notaffect the levels of DAT (Allard et al 1990; Ase et al 1999;Reader et al 1998; Tarazi et al 2000). In addition, in thisstudy both THC(�) and THC(�) subjects with schizo-phrenia had received antipsychotic drugs, and thereforethe specificity of the change in DAT to the THC(�)schizophrenic subjects argues against this being simply anantipsychotic drug effect.
In conclusion, this study suggests that there is a de-crease in DAT in the caudate from THC(�) subjects withschizophrenia. From current knowledge of DAT it wouldbe expected that the density of DAT would, at times, proverate limiting to neuronal dopamine uptake (Horn 1990)resulting in an increase in extracellular dopamine. Anincrease in extracellular dopamine should cause an over-activation of the dopaminergic system in the brain. Thus,the decrease in DAT we have measured in caudate fromsubjects with schizophrenia could be providing direct
590 B. Dean et alBIOL PSYCHIATRY2003;53:585–592

support to the dopamine hypothesis of schizophrenia(Meltzer and Stahl 1976), which proposes that overactivedopaminergic systems are central to the pathology of theillness. Our data would also support the argument thatabsence of change in DAT in the THC(�) subjects withschizophrenia means that the ingestion of THC fromcannabis may act to reverse changes in DAT associatedwith the pathology of the disorder.
Brian Dean was a National Alliance for Research on Schizophrenia andDepression Young Investigator. This work was supported in part bygrants-in-aid from the State Government of Victoria “Turning the Tide”Initiative and the National Health and Medical Research Council (ProjectGrant: 114253).
We thank Mr. Geoffrey Pavey for his assistance in preparing the tissuefor this study and Ms. Christine Hill and Professor Nicholas Keks for theassistance with postmortem diagnosis.
ReferencesAllard P, Eriksson K, Ross SB, Marcusson JO (1990): Unaltered
[3H]GBR-12935 binding after chronic treatment with dopa-mine active drugs. Psychopharmacology (Berl) 102:291–294.
Amara SG (1993): Neurotransmitter transporters: Recentprogress. Ann Rev Neurosci 16:73–93.
Ameri A (1999): The effects of cannabinoids on the brain. ProgNeurobiol 58:315–348.
American Psychiatric Association (1994): Diagnostic and Sta-tistical Manual of Mental Disorders, Fourth Edition. Wash-ington, DC: American Psychiatric Association.
Ase AR, Amdiss F, Hebert C, Huang N, van Gelder NM, ReaderTA (1999): Effects of antipsychotic drugs on dopamine andserotonin contents and metabolites, dopamine and serotonintransporters, and serotonin1A receptors. J Neural Transm106:75–105.
Bonnin A, de Miguel R, Castro JG, Ramos JA, Fernandez-RuizJJ (1996): Effects of perinatal exposure to delta 9-tetrahydro-cannabinol on the fetal and early postnatal development oftyrosine hydroxylase-containing neurons in rat brain. J MolNeurosci 7:291–308.
Cadogan AK, Alexander SP, Boyd EA, Kendall DA (1997):Influence of cannabinoids on electrically evoked dopaminerelease and cyclic AMP generation in the rat striatum.J Neurochem 69:1131–1137.
Dean B, Hussain TP (2001): Studies on dopaminergic andGABAergic markers in caudate-putamen reveals a decreasein the dopamine transporter in schizophrenia. Schizophr Res52:107–114.
Dean B, Sundram S, Bradbury R, Copolov DL (2001): Studies on[3H]CP-55940 binding in the human central nervous system:Regional specific changes in density of cannabinoid-1 recep-tors associated with schizophrenia and cannabis use. Neuro-science 103:9–15.
Gessa GL, Melis M, Muntoni AL, Diana M (1998): Cannabi-noids activate mesolimbic dopamine neurons by an action oncannabinoid CB1 receptors. Eur J Pharmacol 341:39–44.
Hernandez ML, Garcia-Gil L, Berrendero F, Ramos JA, Fernan-dez-Ruiz JJ (1997): Delta 9-tetrahydrocannabinol increases
activity of tyrosine hydroxylase in cultured fetal mesence-phalic neurons. J Mol Neurosci 8:83–91.
Hill C, Roberts S, Keks NA, Dean B, Mackinnon A, Copolov DL(1996): Diagnostic Instrument for Brain Studies. Melbourne:Mental Health Research Institute.
Hollister LE (1998): Health aspects of cannabis: Revisited. IntJ Neuropsychopharmacol 1:71–80.
Horn AS (1990): Dopamine uptake: A review of progress in thelast decade. Prog Neurobiol 34:387–400.
Javitch JA, Blaustein RO, Snyder SH (1983): [3H]mazindolbinding associated with neuronal dopamine uptake sites incorpus striatum membranes. Eur J Pharmacol 90:461–462.
Johns A (2001): Psychiatric effects of cannabis. Br J Psychiatry178:116–122.
Joyce JN, Lexow N, Bird E, Winokur A (1988): Organization ofdopamine D1 and D2 receptors in the human striatum:Receptor autoradiographic studies in Huntington’s diseaseand schizophrenia. Synapse 2:546–557.
Laakso A, Bergman J, Haaparanta M, Vilkman H, Solin O,Syvalahti E, Hietala J (2001): Decreased striatal dopa-mine transporter binding in vivo in chronic schizophrenia.Schizophr Res 52:115–120.
Laakso A, Vilkman H, Alakare B, Haaparanta M, Bergman J, SolinO, et al (2000): Striatal dopamine transporter binding in neuro-leptic-naive patients with schizophrenia studied with positronemission tomography. Am J Psychiatry 157:269–271.
Laruelle M, Abi-Dargham A, van Dyck C, Gil R, D’Souza DC,Krystal J, et al (2000): Dopamine and serotonin transportersin patients with schizophrenia: An imaging study with[(123)I]beta-CIT. Biol Psychiatry 47:371–379.
Lavalaye J, Linszen DH, Booij J, Dingemans PM, Reneman L,Habraken JB, et al (2001): Dopamine transporter density inyoung patients with schizophrenia assessed with [123]FP-CITSPECT. Schizophr Res 47:59–67.
Leweke FM, Giuffrida A, Wurster U, Emrich HM, Piomelli D(1999): Elevated endogenous cannabinoids in schizophrenia.Neuroreport 10:1665–1669.
Mallet J (1996): The TiPS/TINS lecture. Catecholamines: Fromgene regulation to neuropsychiatric disorders. Trends Phar-macol Sci 17:129–135.
Meltzer HY, Stahl SM (1976): The dopamine hypothesis ofschizophrenia: A review. Schizophr Bull 2:19–76.
Reader TA, Ase AR, Huang N, Hebert C, van Gelder NM(1998): Neuroleptics and dopamine transporters. NeurochemRes 23:73–80.
Risch SC (1996): Pathophysiology of schizophrenia and the roleof newer antipsychotics. Pharmacotherapy 16:11–14.
Rodbard D (1981): Mathematics and statistics of ligand assays.In: Langan J, Clapp JJ, editors. Ligand Assay: Analysis ofInternational Developments on Isotopic and NonisotopicImmunoassay. New York: Masson, 55–101.
Rodriguez DF, Cebeira M, Hernandez ML, Ramos JA, Fernan-dez-Ruiz JJ (1990): Changes in brain dopaminergic indicesinduced by perinatal exposure to cannabinoids in rats. BrainRes Dev Brain Res 51:237–240.
Sakurai-Yamashita Y, Kataoka Y, Fujiwara M, Mine K, Ueki S(1989): Delta 9-tetrahydrocannabinol facilitates striatal dopami-nergic transmission. Pharmacol Biochem Behav 33:397–400.
Dopamine Markers in Schizophrenia 591BIOL PSYCHIATRY2003;53:585–592

Schoemaker H, Pimoule C, Arbilla S, Scatton B, Javoy-Agid F,Langer SZ (1985): Sodium dependent [3H]cocaine bindingassociated with dopamine uptake sites in the rat striatum andhuman putamen decrease after dopaminergic denervation andin Parkinson’s disease. Naunyn Schmiedebergs Arch Phar-macol 329:227–235.
Solowij N (1998): Cannabis and Cognitive Functioning. Cam-bridge: Cambridge University Press.
Soulsby B (1999): Drug Equivalents for Neuroleptics, Antide-pressants and Benzodiazepines. Melbourne: Mental HealthResearch Institute of Victoria.
Tarazi FI, Zhang K, Baldessarini RJ (2000): Olanzapine,quetiapine, and risperidone: Long-term effects on mono-amine transporters in rat forebrain. Neurosci Lett 287:81–84.
Torack RM, Morris JC (1992): Tyrosine hydroxylase-like(TH) immunoreactivity in Parkinson’s disease and Alzheimer’sdisease. J Neural Transm Park Dis Dement Sect 4:165–171.
Yoshimoto K, Irizawa Y, Komura S (1993): Rapid postmortemchanges of rat striatum dopamine, serotonin, and their metab-olites as monitored by brain microdialysis. Forensic Sci Int60:183–188.
592 B. Dean et alBIOL PSYCHIATRY2003;53:585–592