-
7/28/2019 Cannabinol During OS
1/11
ANESTHESIAND ANALGESIA. . Current Researches VOL. 5, No. 2,
MARCH-APRIL,976 203
C a r d i o v a s c u l a r E f f e c ts of C a n n a b i n o l
D u r i n g O ra l S u r g e r yJ O H N M. GREGG, DDS, PhD*ROBERT
L. CAMPBELL, DDSt
KENNETH J . LEVIN, MS, M D*J AWAHAR GHIA, MDSRILEY A. ELLIOTT,
BSII
Fifty-five clinical trials were conducted to de-termine the
cardiovascular combined effects ofstressful oral surgery and
systemic cannabi-nols. In a first study,
A-tetrahydrocannabinol(THC) was given IV as a premedicant
andcompared with diazepam and with a placebo.A classic dose-related
tachycardia followedTHC injection. Th e peak h eart ra te response
apatients prernedicated with 0.044 mg/kg THCwas 24.1% higher ( p
< 0 . 0 5 ) tha n th e peak effectfo r a nonsurgerized control
group, suggestinga synergistic effect between THC and
surgicalstress. A predisposition to syncopal hypoten-sion followed
THC premedication, and anti-arrhythmic effects were observed after
largedoses. The injection of local anest hetic pre par a-
HE cannabinols, the most heavily usedT sychoactive drugs in the
world, areused by an estimated 250,000,000 persons.The 1972
estimates for college-age users was54% (with about 5 to 10% of
these usingmarijuana on a daily basis), and 1980 pro-jections for
young adults have been set at66%.l Inevitably, more marijuana users
willbe approaching elective or emergency sur-gical anesthesia after
having premedicatedthemselves with cannabinols.
Marijuana has several properties that sug-gest it might be
useful as a surgical pre-medicant: analgesia in subhumans;2
antisi-alosis;3 a moderate amnesic effect;4 a low
tions containing epinephrine did not alt er TH Ccardiovascular
response. An apparent drug in-teraction was observed, however, in a
secondstudy, in patients given general anesthesiawithin 72 hours
after smoking marijuana.These patients demonstrated sustained
abnor-mal postoperative tachycardia when comparedwith control
nonsmokers, an effect which mayhave resulted from an interaction
betweenstored cannabinol metabolites and a tropin e ad-ministered
as part of the anesthetic technic.It was concluded that THC had no
particularadvan tage over diazepam o r placebo as a pre-medicant.
Further, THC altered the patientsadaptivity to stress and
interacted undesirablywith other anesthetic medications.
or nonexistent addiction potentia1;s and avery low
t~xicity.~eath from cannabinoloverdose has rarely been reported,
and mostsevere reactions have occurred followingun-controlled I V
injections. Extrapolating fromanimal toxicity studies, a human LD,,
ofat least 30 mg/kg is far above the psycho-logically effective
range, and much morefavorable than that of alcohol.5 And
finally,the extensive use of marijuana as a socialdrug suggests a
pleasant psychic experiencewhich could also serve well as a
surgicalpain and anxiety sedative.
There is considerable evidence, however,that significant
incompatibilities may exist*Associate Professor, Departments of
Oral Surgery and Anesthesiology, The University of North
Carolina,?Assistant Professor, Department of Oral Surgery, The
University of North Carolina.$Associate Professor, Department of
Anesthesiology, Th e University of North Carolina.SAssistant
Professor, Department of Anesthesiology, The University of North
Carolina.//Intern n Dentistry, The University of Vermont.This study
was supported in part by NIH Research Grant DE 02668 from the
National Institute ofDental Research and by NIH Grant RR 05333 from
the Division of Research Facilities and Resources.Paper received:
5/13/75Accepted for publication: 8/7/75
Chapel Hill, North Carolina 27514.
-
7/28/2019 Cannabinol During OS
2/11
204 ANESTHESIAND AXAI.GESIA. . C u r r e n t Researches VOL.55,
No. 2, MARCH-APRIL,976between cannabinol premedication and
sur-gical anesthesia, making this drug of ques-tionable value in
this situation. Althoughthe response to marijuana, as to most
psy-choactive drugs, is largely determined bydoseGand route of
administration,' person-ality factors,Rpsychologic set," and
especial-ly the stress of the environmental setting:3.1"appear
inordinately significant. For exam-ple, dysphoric "high" responses
("highs")with marijuana are more commonly seen inpatients with
chronic depression,ll andparanoid delusional reactions occur
morefrequently in hypnotic-suggestiblepatients. 1Marijuana is now
looked upon as a mood-intensifying drug rather than as a pureCNS
excitant, euphoriant, or depressant perse.13 Thus, it might be
anticipated that thepsychophysiologic stress of a surgical
exper-ience in the marijuana-premedicated patientcould result in an
exaggerated sympatho-adrenal stress response.
Most of the adverse effects reported formarijuana have been on
cardiovascular func-tions and related drug interactions. As in
thepresent study, the most consistently report-ed pharmacologic
response is a dose-relatedtachycardia.14.l; Both hypotensive and
hy-pertensive effects have been described.1"The combination of
increased cardiac de-mand from tachycardia with sustained
cate-cholamine elevation has led some authorsto warn tha t the use
of cannabinols inelderly or in cardiac patients may be
haz-ardous.z.12 Studies of patients with anginapectoris support
this warning, for it hasbeen shown that smoking marijuana
signifi-cantly decreases exercise tolerance whencompared to placebo
smoking.IH
Studies of long-term hashish users havedemonstrated elevated
hemoglobin andpacked-cell volumes, which have been attrib-uted to
chronic hypoxia.1 1:) There are alsoreports of increased potential
for cardiacarrhythmias,18 and ECG studies have dem-onstrated
shortening of the S-T interval anddepression of T-wave amplitude.?O
Otherstudies, however, have indicated that can-nibinols may
actually have a therapeutic orprotective effect against cardiac
arrhyth-mias." Nevertheless, because the incidenceof arrhythmia
during oral surgery withlocal anesthesia alone has been reported
asgreater than 45%,'2 our investigations ofcannabinol effects
appear warranted.
There have been other warnings of dan-gerous drug interactions
between marijuanaand anesthetic medications. Cannabinols
have been shown to double ketamine sleep-ing time and to
quadruple thiopental dura-t i ~ n . ' ~entobarbital sleeping time
in ratswas doubled after a single cannabinol dose.'-'Marijuana is
also known to potentiate thedepressant effects of alcohol'" and to
sum-mate with amphetamines. .6 Beaconsfield'sgroup1-' predicted
dangerous cardiovasculardrug interactions between marijuana andsuch
common agents as atropine or local-anesthetic preparations
containing epineph-rine.
Our studies were designed to determinethe cardiovascular effects
of cannabinols (1)by comparing the cardiovascular effects
ofpremedicant I V doses of THC, diazepam,and placebo, and ( 2 ) by
a retrospectivestudy of the cardiovascular effects of out-patient
general anesthesia in patients knownto have smoked marijuana within
72 hoursbefore anesthesia.
STUDY 1: METHODSTen healthy male patients between 19and28 years
of age (mean 26 + 2.8 yr SD) wereselected for study, without regard
to priormarijuana experience, from a populationrequiring elective
surgical removal of 4 im-pacted 3rd molars. All 10 subjects
hadsmoked marijuana, and 2 admitted to pre-
vious experiences with LSD-25 and mesca-line. After explanation
of the procedure andthe risks involved, informed consent
wasobtained. A complete physical examination,including ECG, chest
x-ray, and laboratorytests, showed all subjects to be healthy
andfree of cardiovascular or respiratory abnor-malities. Each
subject participated in 4separate weekly clinical trials, at which
timea single 3rd molar was removed, and duringwhich time he was
prernedicated with oneof the following 4 agents:1. THC: 0.044
mg/kg* ("larger dose")2. TH C: 0.022 mg/kg" ("smaller dose")3.
Diazepam: 0.157 mg/kg4. Placebo (dextrose 5%, NaC1): 0.2%These were
given in random order on 4consecutive weeks, double-blind with re
-spect to patient and surgeon. This allowedeach patient to serve as
his own control formeasuring cardiovascular changes. Th e
THCsolutions were prepared by dissolving the
*These 2 dosages were selected from a pilot studyin which 0.02
mg/kg was found to consistentlyproduce minimal subjective
"highs"and 0.04 mg/kgconsistently produced near-100% "highs."
Subjectsreported that IV "highs" were equal to or beyondthe usual
effects from smoking marijuana.
-
7/28/2019 Cannabinol During OS
3/11
Cardiovascular Effects of Cannabinol . . .Gregg, et a1 205dose
of active THC in 0.5 ml of ethyl alco-hol and adding 25 ml of human
serum albu-min.
On the morning of each clinical trial,patients, who had fasted
since midnight andhad recently voided, were brought to theclinical
research unit. All had been askedto avoid smoking in any form for
at least24 hours before each clinical trial. Patientsreclined in an
approximately 30" sittingposition throughout the test period.
TheECG was continuously recorded from amodified lead I1 placed
entirely on thethoracic cage, and heart rate was
monitoredelectronically from the ECG. Indirect sys-tolic and
diastolic blood pressures were re-corded at 2-minute intervals with
a Littonphonosensor. All transducer signals werepreamplified and
oscilloscope-displayedthrough the Litton Product Basic BedsideUnit.
Continuous recording of output wasmade on a 12-channel Honeywell
5600 elec-tromagnetic tape recorder and subsequentlyprinted out on
the Siemens Mingograph@polygraph.
Simultaneously with the cardiovascularmonitoring, subjective
psychologic drug ef-fects were studied, using the
State-TraitAnxiety Inventory (STAI) 2 7 a modifiedSubjective Drug
Effects Questionnaire(SDEQ) 28 and the measure of subjective"high"
described by Perez-Reyes and co-workers.2C' Details of these tests
are con-tained in another report.30Baseline resting physiologic
functionswere monitored for a 30-minute period, andthe injection
procedure was isolated andshielded from the patient's view.
Patientswere told that the injection was to begin,and the
premedicant was injected evenlyover a 5-minute period through an
indwell-
ing venous catheter, after which the surgeonand nurse entered
the operatory, where theyadministered the local anesthetic.
Appro-priate peripheral trigeminal blocks were per-formed by
standard aspiration technic, usingan average of 2 to 4 ml (40 o 80
mg) of2% lidocaine containing 40 to 60 mcg of1:100,000 epinephrine.
The surgeon then re-moved the molar by ordinary surgical tech-nics,
pacing the procedure to be completedexactly 30 minutes after drug
injection. Fol-lowing a 30-minute surgical test period, thepatient
remained in the operating chair foran additional 60 minutes of
monitoring andthen was escorted to a recovery room, wheremonitoring
continued for a minimum of 60minutes until discharge.
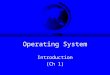
M E A N B L OOD P R E S S UR E R E S P ON S E TOSURGICAL
PREMEDICATION WIT H A9 TE TR A H Y D R OC A N N A B I N OL ,DIAZ
EPAM , AND PLACEBO ( n = 0 s u b I r c t s 1
A 9 T H C i 0 0 4 4 m q / h q l -A' TH C i O . 0 2 2 rng / hq
IPlacebo .D i a z c o a m ( 0157rnp/hql ----
~."1 r ' , ' " I20 40 6 0Surgery Surgerybegun en d
D ru gbegunT i m e ( m i n u t e s )
Ib P 'FIG 1. Measures of blood pressure response tosurgical
premedication with 'THC revealed a peaksystolic hypertension 25
minutes after injection. Amild gradual hypotensive trend followed
the end ofsurgery with the larger THC dose.The additional control
group of 5 nonsur-gerized volunteers consisted of healthy men,aged
21 to 34 (mean 26 k3.2 SD), who
underwent a single trial in which they weregiven a single dose
of THC (0.044 mg/kg)from the batch used in the main
experimentdescribed above. Cardiovascular monitoring,subjective
measurements, and experimentalsetting were identical, but no
operationswere performed. When cardiovascular datafrom this group
were compared with datafrom the main experiment, influences
thatcould be attributed solely to drug effectcould be separated
from those due to drug-surgical stress interactions.STUDY 1:
RESULTS
Blood Pressure.-The average blood pres-sure response to surgical
premedication withTHC changed little from average preopera-tive
baselines and placebo levels (fig 1 ) .Amild elevation of systolic
pressure was ob-served, with the peak effect at the 25-min-Ute
postinjection interval; the larger dose ofTHC produced an average
elevation of 8torr, and a 9-torr elevation followed thesmaller
dose. In the Iarger-dosage THCgroup, a gradual hypotensive trend
was ob-served, beginning approximately at the timeof completion of
the operative procedureand reaching an average maximum depres-sion
of 12 tom below preoperative baseline
-
7/28/2019 Cannabinol During OS
4/11
206 ANESTHESIA N D AXALGESIA . . C u r r e n t Re s e a r c he s
Vor,. 55, No. 2 , MARCH-APRIL,976and 14 torr below placebo levels
at the 55-minute postinjection time period. Bloodpressures
following larger doses of THCreturned gradually to placebo levels
an aver-age of 70 minutes after initial drug injec-tion.
The blood pressure effects of diazepamwere dissimilar to those
of THC: Diazepamconsistently induced a mild systolic hypo-tension,
ranging from 7 to 15 torr through-out the entire trial. However,
average dia-stolic responses to both dosages of THCwere
statistically and clinically similar toplacebo responses
throughout.Transient moderate hypotension of 20 to45 torr systolic
and diastolic in the intervalof 4 to 8 minutes after THC injection
oc-
curred in 3/10 subjects. These episodesappeared to be typical
syncope, associatedwith nausea, dizziness, anxiety complaints,and,
in 2 instances, loss of consciousness ac-companied by carpopedal
spasm for up to25 seconds. No similar syncopal responsesor
transient hypotension was observed withany of the patients given
placebo or diaze-pam.Blood pressure response in the periodduring
and immediately after administra-tion of the local anesthetic
(lidocaine withepinephrine) was not significantly different
from placebo responses with either dose ofTHC or diazepam.Heart
Rate.-Comparison between bothdosages of THC, which induced
tachycardiain all surgical patients, and response todiazepam and
placebo premedicants (fig 2)showed the average peak heart rate
increasewith 0.044 mg/kg THC to be 69% abovepreoperative baseline
and 36% above place-bo peak. The greatest elevation occurred
5 18 minutes after the start of drug injec-tion. Peak heart rate
increases after 0.022mg/kg THC occurred typically at the 15-minute
postinjection interval, with 53%above preoperative baseline and 26%
aboveplacebo peak. Although heart rate peak timewas similar with
both doses of THC, theduration of tachycardia differed.
Whereasaverage heart rate had returned t o placebolevels 75 minutes
after injection of 0.022mg/kg THC, heart rate after 0.044 mg/kgTHC
had not returned to placebo levelsuntil after the 100-minute
postinjectiontime.
Local-anesthetic administration in pa-tients premedicated with
THC had no sig-nificant effect on heart rate during or afterthe
injection process. "Highs" experiencedafter TH C premedication did
not coincidewith peak heart rates, peak tachycardia OC-curring
typically 12 minutes before peak
MEAN HEART RATE RESPONSES TOSURGICAL PREMEDICA TION WITH A'
TETRAHYDROCANNABINOL,DIAZEPAM, AND PLACEBO ( n =10 subjects 11401
A'TCIC ( 0 . 0 4 4 m q / k g ) -
A THC ( 0 . 0 2 2 m g / k g )Placebo .....Diazepam (0.157
g/kg)
L ' I # ' I ' ' 1 " ' 1 " ' 1 ' " 1 " ' 1-20 0 20 40 60 80 100
120
Surge ry S u r g e r ybegun end
begun T i m e ( m i n u t e s )Drug'
FIG2. Peak T H C tachycardias significantly above placebo and
diazepam levels occurred at the 15-18post-injection interval. Heart
rate returned to placebo levels approximately 100 minutes after
injection ofTHC, .044 mg/kg.
-
7/28/2019 Cannabinol During OS
5/11
Cardiovascular Effects of Cannabinol . . .Gregg, et a1 207M E A
N H E A R T R A T E . SYSTO L IC 8L00D
FOLLOWING SURGICAL PREMEDICATIONW I T H A9 TETRAHYDROCANNABINOL
,P R E S S U R E A N D SUBJECTIVE HIGH RESPONSES
( 0 04 4 mg / g ( n=IO s u b j e c t s I1307
70 -
6 0 - 1 . . , 7 1 7 , I , , # , , , --10 0 1 20 / 40 60 80
100Surgery S u r g e r y1 b e g u n e n d
70
60
50ch40z
30 9bs
20
10
0
Drugb e g u n
FIG3. Simultaneous plotting of heart rate, bloodpressure and
subjective high responses to THC dur-ing surgery showed that peak
tachycardia precededboth the peak hypertensive and subjective
higheffect, and that the heart rate and blood pressuresreturned to
placebo baselines an average of 30minutes before subjective high
was reported asnormal.
highs. Heart rates also returned to place-bo levels an average
of 30 minutes beforesubjects reported a normal psychic state
ECG Responses.-There was a dose-re-lated shortening of P-R
interval greater than33% in all subjects given THC (table 1).T-wave
amplitude reduction of greater than33% during peak drug effect was
observed
(fig 3 ) .
in 70% of subjects after the smaller dosesof THC and in 60% of
subjects after thelarger THC dose, as compared to a 30%depression
with diazepam and 10% depres-sion with placebo. ECG changes in
THC-premedicated patients were the same withlocal anesthetic
injection as with placebo.Arrhythmias, interpreted as
functionalpremature ventricular contractions (PVCs),were observed
in 11/40 clinical trials duringbaseline preoperative recording and
in 2/10subjects during intraoperative trial withplacebo
premedication. After injection of0.022 mglkg THC, arrhythmias seen
preop-eratively in 2 subjects increased slightly infrequency
intraoperatively, and PVCs wereobserved in 2 other subjects who had
notdisplayed arrhythmias during preoperativebaseline recording.
After injecting the largerdose of THC, arrhythmias observed in
asingle subject during baseline preoperativerecording disappeared
for an hour after drugadministration and intraoperative
recording(fig 4).No other instances of arrhythmiawere observed
after giving the larger doseof THC.
Surgical and Nonsurgical THC GroupsCompared.-A significant
difference ( p
-
7/28/2019 Cannabinol During OS
6/11
208 ANESTHESIAN D ANALGESIA. .C u r r e n t Researches VOL. 55,
No. 2, MARCH-APRIL,976R A T E OF C A RD IA C A R R H Y T H M I A S
F OL L O W IN GSURGICAL PREMEDlCATlON WITH A9
TETRAHYDROCANNABINOL,D I A Z E P A M , A N D P L A C E B O
P l a c e b o . . ...Diazepam ( 0 . 1 5 7 m g I k g )---THC
(0.022m g / kg l -.-THC (0.044 g/ kgl-
Surgery Surgery1 begun endDrugbegu n T i m e ( m i n u t e s
)
FIG4. Preoperative rate of arrhythmias significantly reduced
following premedication with THCcompared to diazepam and placebo.
when
TABLE 2Comparison of Mea n Cardiovascu lar Responses to 0.044
mg/kgIV A'-THC in Surgical an d in Nons urgi cal Subjects
Sur g i c a l pa t i en t s ( N=101 N ons ur g i c a l s ub i ec
t s (N =5 )(2 E) (f SE )Yo change change
Heart r a t e R a t e b a s e l i n e R a t e b a s e l i n
eBaseline 71.7 - 70.8 -
&4 .5 k 4 . 2D r u g given ( 5 m i n ) 96.8 35.0* 80.6
13.8*
rt5.l k 2 . 8Peak effect 117.8 64.3* 102.0 44.1*
k 7 . 1 2 4 . 6Trial end ( 9 0 m i n ) 80.9 12. 8t 73.0 3.lf
k 7 . 0 & 2 . 5Sy r to l i c /d i as to l i c c hange Sy s
to l i c /d i o r to l i c yoc h a n g e
B l o o d pressure pressure S/D basel ine pressure S/ D b a s e
l i n eBaseline 117.6176.2 - 128.6168.8 -
i 5 . 7 4 / & 4 . 6 24.52/14.2Drug g ivenPeak effect
117.2/7 2.0 -0.3/-5.5? 131.8/70.8 2.4/2..9?"5 .31k3 .8 k5 .3
/&3 .5122.9168.1 4.5/-10.6? 142/73.2 10.4/6.4+k 7 . 3 1 k 4 . 1
1 1 2 . 5 / & 4 . 1
Trial end (9 0 min) 111.8 /69.6 -4.91-8.6* 133 .8/68
4.0/-1.2*c4.21k3.6 ?7.0 /&6.4* p
-
7/28/2019 Cannabinol During OS
7/11
Cardiovascular Effects of Cannabinol .. .Gregg, et a1
209subjects. Dysphoria, as measured by SDEQanalysis, and low moods
predominated atthe periods of syncopal hypotension afterTHC.
STUDY 2 : METHODSThis retrospective study included 10
con-secutive patients, 7 women and 3 men (ages21 to 30, mean 25 k
3.1) undergoing outpa-tient general anesthesia for routine
removalof from 2 to 4 third molars in one clinicalprocedure. Each
patient was healthy andfree of cardiovascular or respiratory
abnor-malities and gave informed consent.At each clinical triaI,
patients were seatedin the operating chair in an approximately30
upright position with legs parallel tothe floor. A venous catheter
was inserted inthe forearm. Physiologic monitoring con-sisted of
continuous ECG, heart rate, in-direct blood pressure, and
respiratory rate,by a technic similar to that described forstudy 1.
In addition, serial blood-gas meas-urements (IL Blood Gas Analyzer)
weremade through radial-artery puncture, pre-operatively and at
selected intervaIs duringoperation,After baseline blood pressure,
ECG, heartrate, respiratory rate, and blood gases had
been recorded, all 10 patients received thesame form of general
anesthetic manage-Instrumentation Laboratories.
ment. First, 0.4 mg of atropine sulfate wasadministered IV,
followed by 0.1 mg offentanyl. Ten to 15 mg of diazepam wasthen
infused over a 6 to 8-minute period toan endpoint of hypnosis with
Verrills sign(lid lag over pupils). After adequate seda-tion,
N,O-0, (70:30) was administeredthrough a McKesson nasal inhaler by
aMcKesson Analor@ as machine. After 15 to30 seconds, 1% sodium
methohexital wasgiven at a rate of 20 mgl30 sec until voicecontact
with the patient was lost.
Following induction, respirations weregently assisted with nasal
insufflation, andadditional increments of methohexital wereinfused
as needed. Tooth extraction thenproceeded according to standard
technic, in-cluding mouth gauze packing and the P R Nadministration
of local anesthetic blocks.The total usual dose of local
anestheticranged from 4 o 6 ml of 2% lidocaine (80to 120 mg) with
40 to 60 mcg of 1:100,000epinephrine.
Surgical anesthesia ranged from 25 to 45minutes in duration. No
major complica-tions were encountered. Following awaken-ing,
patients were monitored for a minimumof 1 hour before
discharge.
STUDY 2 : RESULTSOf the 10 patients studied, 5 admitted tohaving
smoked marijuana within 72 hoursTABLE 3
Comparison of Mean Cardiovascu lar Responses to
OutpatientGeneral Anesthesia in Mar ij uan a Smokers and in
Nonsmokers(N=10subjects)
Blood gasB lood pressure Heart rate Po a Pcoa
Preoperative baselineSmokersNonsmokers
PostinductionSmokersNonsmokers
Peak anestheticSmokersNonsmokers
Peak postanestheticSmokersNonsmokers
10,1.6/68.2106.0/66.4
1(14.8/66.0106.3/68.1
102.0/64.8105.6/65.2
115.2/89.6ll6.0d91.2
83.0 90.0 35.274.8 90.6 36.0
104.0 97.6 39.090.3 98.1 44.0
98.6 160.2 40.293.6 158.4 40.4
136.8*104.6*
* p
-
7/28/2019 Cannabinol During OS
8/11
210 ASFSTHESIASD ASALCESIA Current Researches VOL.55, No. 2,
MARCH-APRIL,976ME AN HEART RATE RESPONSES TOMAR I U A NA SMOKERS
COMPAREDGENERAL ANESTHESIA IN] TO N O N - S M O K E R S (n : lO
)I40
nSmokersLbaseline anesthesla 10 20 30 40 50Pre-op ' Surgicol
Post -surgical anesthesiaMcnutes
FIG5. Tachycardia following general anesthesiawas markedly
elevated and lengthened in marijuanasmokers as compared to
non-smokers.
of operation. A comparison of cardiovascu-lar responses between
marijuana-smoker andnonsmoker groups revealed similar preoper-ative
baselines of blood pressure, heart rate,ECG, and blood gases (table
3 ) . In addi-tion, blood pressure responses and bloodgases were
found similar and within ex-pected limits for both groups
throughout theduration of anesthesia and the
postoperativeperiod.
A major difference between the 2 groupswas observed, however, in
heart rate re-sponse during the postanesthetic interval(fig 5) . In
the marijuana group, a peaktachycardia averaging 64.8% above
baselineoccurred, which did not return to baselinelevels until an
average of 38 minutes afterthe end of anesthesia. In the
nonsmokergroup, postoperative heart rate peaked at39% above
baseline at the 7-minute markafter anesthesia and returned to
baselinelevels by the 19-minute mark after anesthe-sia.
There were no significant differences be-tween smoker and
nonsmoker groups fortotal required methohexital (193 versus 194mg).
Nor were there differences betweenmean "sleep time" induced by
these con-centrations (32.4 versus 31.8 min) or inrecovery
rate.DISCUSSION
In the current studies, which involvedhealthy young adults,
there was no signifi-cant deterioration in cardiovascular
func-tions. However, certain changes were ob-
served that might hold significance for otherpatient
populations.Transient syncopal hypotension followedTHC
premedication. (Psychologic measuresduring these periods
demonstrated above-average levels of dysphoria and anxiety.)These
patients did not demonstrate syncopewhcm premedicated with placebo
or diaze-pam. Orthostatic hypotension and presynco-pal responses to
table tilt have been de-scribed as common with THC .31J2
Con-trolled animal experiments have shown thatstress exaggerates an
already elevated sym-pathoadrenal response to parenteral
can-nabinols, manifest as marked elevations inserum dopamine
hydroxylase levels.2"Beaconsfield first warned that under
stressful or emergency conditions, the vaso-motor reflex
mechanisms may be significant-ly impaired in marijuana-pretreated
sub-jects.' 4 . u He demonstrated that peripheralblood flow
increases concomitantly withpulse rates following cannabinol
administra-tion, and that peripheral flow adjustmentsto mild
psychogenic stress (mental arith-metic and ice placed on a limb)
are mark-edly slowed or absent. Careful cardiovascu-lar monitoring,
therefore, is mandatory fol-lowing THC premedication.After the
initial tendency to syncopalhypotension from THC during
operation,the blood-pressure response displayed a bi-phasic pat
tern of mild hypertension, whichpeaked at the 25-minute
postinjection in-terval, followed by a gradual hypotensivetrend
which reached its peak depression at55 minutes postinjection.
Surgical stimula-tion probably had a strong influence
onblood-pressure response. However, similararousal-depression
patterns have been ob-served in nonsurgical experiments with
can-nabinols, and there may be pharmacologicreasons for this
pattern:]' As A9-THC un-dergoes biotransformation to the more
polarform, ll-O H-ng-T HC, within 10 to 15 min-utes after
injection, it has been suggestedthat n!'-THC exerts a generalized
CNS andcardiovascular arousal effect, and that 11-OH-n!I-THC has a
longer-acting depressanteffect."4In our study, combining T H C
premedica-tion with the stress of oral surgery appearedto have a
synergistic effect on heart rate,since subjects who had received
0.044 mg/kgof T HC before operation reached peak heartrates
averaging 24.1% higher than the peaksfor the nonsurgerized
controls. These obser-vations are consistent with current
theories
-
7/28/2019 Cannabinol During OS
9/11
Cardiovascular Effects of Cannabinol . . .Gregg, e t a1 211of
the mechanism of THC cardiovascularaction. Studies have suggested
that vago-lytic action by the cannabinols is unlikelybecause
cannabinol tachycardia is inducibleeven in atropinized patients.14
Most evi-dence points to a CNS-activated sympatho-adrenal response
to cannabinol. Beta-adren-ergic receptors appear to be the final
com-mon pathway for this response, since pro-pranolol, a beta
blocker, reduces the effectsof cannabinol.35
Even though THC tachycardia appearedto be heightened by the
stress of operationin this study, it is of interest that the
ini-tiation and duration of heart rate changesappeared to precede
psychic effects. Onsetof heart rate elevation consistently
precededthe onset of highs by a few minutes, andthe peaks of heart
rate and subjective high,as well as the duration curves, were
gen-erally out of phase by a matter of manyseconds to a few
minutes. This finding isconsistent with those of Lows group,13
whoobserved that subjective THC effects maypersist even though
heart rate has returnedto normal.
It may be speculated that the inevitableTHC tachycardia acts as
a partial triggerfor the psychic effect of cannabinols, andthat the
surgically stressed patient reactsto tachycardia in a manner
different fromthe nonstressed THC subject. Whereas thenonstressed
subject interprets THC tachy-cardia as an expected and
nonthreateningaspect of his drug experience, the stressedpatient
considers it a signal that is part ofan overall harmful situation
(the operation)which is out of his control. This activatesthe
hypothalamo-pituitary complex andeventually a classic
sympathoadrenal stressresponse, which then potentiates the
pre-existing THC tachycardia.In pursuing one of the goals of the
cur-rent study, the detection of significant druginteractions
between cannabinols and a localanesthetic agent, it was observed
that usualsurgical levels of 2% lidocaine and 1 :100,000epinephrine
had no measurable effect on anycardiovascular parameter.
Bea~onsfield~~has shown that TH C potentiates the pressoreffects of
I V epinephrine in humans, whirelaboratory studies32J6 have shown
elevationof circulating epinephrine for periods of 6hours following
THC administration. Itwould appear, however, that the doses
oflidocaine and epinephrine used in our stud-ies with surgery
patients and with routineanesthetic block were insufficient to
inter-
act significantly with cannabinol premedi-cation.An apparent
drug interaction was ob-served, however, in study 2 of this
investi-gation, where a prolonged postoperativetachycardia was
observed in a series of pa-tients who had smoked marijuana within72
hours before undergoing outpatient gen-eral anesthesia. Not only is
this a poten-tially dangerous problem, but when the eti-ology of
the tachycardia is not appreciated,errors in medical management may
occur.Previous studie d4 have demonstratedsynergistic
cardiovascular effects betweencannabinols and vagolytic agents.
This sug-gests that atropine, used in the current anes-thetic
technic, was the drug most likely to
have interacted with the previously smokedcannabinol.Potential
drug interactions occurring manyhours, or even days, after
marijuana smok-ing appear quite possible, in light of theknown
distribution, catabolism, and excre-tion patterns of the
cannabinols. Plasmalevels of Ag-THC decrease rapidly
afterinjection, probably because of a great affin-ity for fat
stores.3i TH C may also be storedin significant quantities in the
enterohepatictissues and be secreted along with bile in
response to food ingestion.9 Although thisappears to be the
primary means of can-nabinol excretion, with 70 to 80% elimi-nated
in the feces and 20 to 30% in theurine, the enterohepatic
secretion, with sub-sequent plasma resorption from the gut, mayalso
account for the frequently observedmaintenance of sustained and
episodic THCplasma levels.38The plasma half-life of AS-THC is
36hours; that of the active liver metabolite,ll-OH-ny-THC, is 40
hours. The release
of active THC compounds has been shownto continue for 8 days
after a single humandose.7~34 herefore, 20 to 35% of active
can-nabinols may remain in the tissues for long-er than 72 hours
after a single administra-tion. This time course is quite
compatiblewith the sequence of drug interactions sug-gested by our
study 2.An acute dose-related antiarrhythmic ef-fect was observed
during oral surgery withTHC premedication. The smaller doses
ofAS-THC were associated with intraopera-tive PVC activity at
levels similar to thoseof placebo, whereas the larger doses
werecorrelated with the disappearance of ar-rhythmias after
injection. Although some
-
7/28/2019 Cannabinol During OS
10/11
212 AXESTHESIAXD AXALGESIA. .Current Researches VOL.55, No. 2,
MARCH-APRIL,976report possible induction ofarrhythmias by
cannabinols, other observ-ers?1,RD have shown possible
antiarrhythmiceffects. In our study, arrhythmias were ofthe benign
variety, consisting mainly oftransitory ectopic foci. It would be
unwise
to assume that a similar therapeutic effectwould have occurred
in a group of patientswith chronic cardiopathy.We conclude that
@g-THC has no par-ticular advantage over diazepam or placeboas a
premedicant; although potentially ther-apeutic antiarrhythmic
effects were seen,THC appeared to compromise to some de-gree the
surgical patients adaptivity tostress and to interact undesirably
with otheranesthetic medications.
REFERENCES1. Marijuana and Health. Washington. DC,Third Annual
Keport to Congress, DHEW Pub #(ADMI 74-50, 19742. Parker JS , Dubas
TC: Automatic determina-tion of the pain threshold to electroshock
and theeffects of a-THC. In t J Clin Phaimacol 7:75-81,19733 .
Jones RT : Marijuan a-induced high: in-fluence of expectation,
setting and previous drugexperience. Pharmacol Rev 23:359-369,
19714. Klonoff H, Low M, Marcus A: Neurapsy-chological effects of
mar ijuana. Ca n Me d Assoc J108:150-165, 19735. Nah as GG:
Toxicology and pharmacology ofCannabis S Q ~ ~ L W ith special
reference to n-THC.Bull Narc 24:l l-29 , 19726. Hill SY , Goodwin
DW, Schwin R. Powell B:Marijuana: CNS depressant or excitant? Am
JPsychiatry 131~313-315, 9747. Lemberger L, Weiss JL, Watanabe AM.
et al:Delta-9-tetrahydrocannabinol. Temporal correlationof t he
psychologic effects and blood levels aftervarious routes of
administration. N Engl J Med286: 685-688, 19728. Klapper JA,
McCollach MA, Side11 FR: Theeffect of personality on reactivity to
1,2-dimethyl-heptyl tetrahydrocannabinol. Arch Gen
Psychiatry26:483-485, 19729. Mills L, Brawley P: Th e
psychopharmacologyof Cannabis sativ a: a review. Agents Actions
2:201-215, 1972
10. Carlin AS, Bakkar CB, Halpern L, et a l:Social facilitation
of mar iju ana intoxication: impactof social set. J Abnorm Psycho1
80:132-140, 197211. Ablon SL, Goodwin FK: High frequency
ofdysphoric reactions to tetrahydrocannabinol among
depressed patients. Am J Psychiatry 132:448-453,197412. Bilash
IS, Arnold M, Zell C: Marijuana andsuggestibility. Can Psychiatr
Assoc J 17 :327-329,1972
13. Low MD, Klonoff J , Marcus A: The neuro-physiological basis
of the marijuana experience.Can Med Assoc J 108:157-165, 197314.
Beaconsfield P, Ginsburg J , Rainsbury R:Mar.ijuana smoking:
cardiovascular effects in manand possible mechanisms. N Engl J Med
287:209-212. 197215. Renault PF, Schuster CK, Heinrich R, et
al:Marijuana: standardized smoke administration anddose effect
cuives on heart rate in humans. Science174:589-591. 197111;.
VlilIiams RB, Ng LK, Lamprecht F, et al:~T etra hyd roca nna bin
ol: a hypotensive effect inrats. Isychopharmacology 28:269-274,
197317 . Johnson S, Domino E F : Some cardiovascularefferts of
marijuan a smo king in normal volunteers.Clin Pharmacol Ther 12
:762-768, 197118. Aronow WS, Cassidy J : Effect of mari juanaand
placebo-marijuana smoking on angina pectoris.
N Engl J Med 291: 65-67, 197419. Rubin V, Comitas L: Effects of
Cannabis inanother culture. Scotch Plains, NJ , Mo uton/McFar-land
Publications, 197520. Kochar MS, Hosko M J :
Electrocardiographiceffevts of marijuan a. JA MA 225: 25-27,
197321. Roth WT , Tinklenberg JR , Kopell BS, et al:Continuaus
electrocardiographic monitoring duringmarijuana intoxication. Clin
Pharmacol Ther 14:533-540, 197322. Driscoll EJ , Smilack ZH ,
Lightbody P M , etal: Sedation with intravenous diazepam. J
Oral
Surg 30: 332-343, 197223. Sofia RD, Knobloch LC : The effect
ofa-tetrahydroca nnabinol pretreatment on ketaminethiopental or
CT-1341-induced loss of righting reflexin mice. Arch Int
Phaimacodyn Ther 207:270-281,197424. Siemens AJ , Kalan t H, Khanna
JM, et al :Effect of cannabis on pentobarbital-induced sleep-ing
time and pentobarbital metabolism in the rat.Biochem Pharmacol
23:447-488, 197425. Ng LK , Lamprec ht F, Williams RE, et al :A!
tetrahyd rocannabi nol an d ethanol: differentialeffects on
sympathetic activity in differing environ-
mental settings. Science 180:1368-1369, 197326. Zalcman S,
Liskow B, Cadoret R, et al: Mari-juana and amphetamine: the
question of inter-action. Am J Psychiatry 130:707-708, 197327.
Spielberger CK, Gorsuch RL, Lushene RE:State-Trait Anxiety
Inventory. Palo Alto, Consult-ing Psychologists Press, 197028.
Waskow IE , Olsson JE , Salzman C, et al:Psychological effects of
tet rahydrocann abinol. ArchGen Psychiatry 22:97-105, 197029.
Perez-Reyes M, Timm ons MC, Lopton MA,
et al: Intravenous injection in man of nS-tetra-hydrocannabinol
a n d 11-OH-A-tetrahydrocanna-binol. Science 117:633-635, 197230.
Gregg JM, Small EW, Moore R, e t al:Emotional responses to
intravenous Atetrahydro-
-
7/28/2019 Cannabinol During OS
11/11
Cardiovascular Effects of Cannabinol ...Gregg, et a1
213cannabinol during oral surgery. J Oral Surg (inpress)
31. Hardman HF , Domino EF , Seevers MG:General nharmacoloaical
actions of some svnthetictetrahyd&cannabinor derivatives.
Pharmacol Rev23:295-316, 197132. Weiss JL, Watanabe AM, Lemberger
L, etal: Cardiovascular effects of delta-g-tetrahydrocan-nabinol in
man. Clin Pharmacol Ther 13:671-684,197233. Beaconsfield P: Some
cardiovascular effectsof cannabis. Am Heart J 87:143-146, 197434.
Lemberger L, Axelrod J, Kopin IJ: Metab-olism and disposition of
A9-tetrahydrocannabinol
in man. Pharmacol Rev 23:371-380, 197135. Drew WG, Kiplinger GF,
Miller LL, et al:Effects of propranolol on marijuana-induced
cogni-
tive dysfunctioning. Clin Pharmacol Ther 13:526-533, 197236.
Hollister LE, Moore F, Kanter S, et al:~g-tetrahydrocannabinol,
ynhexyl and marijuanaextract administered orally in man:
catecholamineexcretion, plasma cortisol levels and platelet
sero-tonin content. Psychopharmacologia 17:351-360,197037. Kreuz
DS, Axelrod J: Delta-g-tetrahvdro-cannabinol: localization in body
fat. Science 179:391-392, 197338. Lemberger L, Martz R, Rodda B, et
al:Comparative pharmacology of n9-tetrahydrocan-nabinol and its
metabolite, ll-OH-A9-tetrahydro-cannabinol. J Clin Invest 52:
2411-2417, 197339. Schaefer JF , Loetzer R, Sofia RD: Effect
ofA-tetrahydrocannabinol and propranolol on oua-bain induced
arrhythmias. Arch Int PharmacodynTher 205: 5-10, 1973
TEM PERATURE AND d- TUBOCURARI NE The influence of temperature
(28-41C)on d-tubocurarine (dTc) neuromuscular blockade and
antagonism with neostigminewas studied in anesthetized cats. dTc
infusion rate required to maintain 90 per centtwitch depression wa
s directly related to temperature . Althoug h the mechanism isnot
known, reduced renal and biliary excretion of dTc, may account for
the decreaseddTc needs during hypothermia. Hypother mia did not
affect th e magnitude b ut pro-longed the on set and then dura tion
of dTc antagonism by neostigmine. Since hypo-ther mia reduces
skelet al muscle blood flow the delayed upt ake and elimination
ofneostigmine should not be unexpected. (Miller R D , Van Nyhuis
LS, Eger E I : Theeffect of temperature on a d-tubocurarine
neuromuscular blockade and its antagonismb y neostigmine. J Pharm
Exp Ther 195:237-241, 1975)