Embed Size (px)
Citation preview

Also in this issue :
Diagnosis of P. jiroveciipneumonia Pg. 6
Detection of acute kidney injury Pg. 18
ZnO nanorod-based assayfor AKI biomarkers Pg. 20
Rapid test range for viral infections
Pg.35
New reagent to measure dabigatran
Pg.37
Compact hematology analyser
Pg.38
Candidate biomarkers for early diagnosis of acute lymphoblastic leukemia Pg.12
News updates on www.cli-online.com | June 2016 | Volume 40
by MP Diagnostics
by Stago
by Abbott Diagnostics
001_017_CLI_JUNE_2016.indd 1 15/06/16 16:15

www.cli-online.com & search 27150
001_017_CLI_JUNE_2016.indd 2 15/06/16 16:15

Frances Bushrod, Ph.D.
Colorectal cancer (CRC) is the third most frequent malignant neoplasm globally. In Europe CRC is the sec-ond most common cause of cancer death in women (breast cancer is the most common), and the third most common in men (aft er prostate and lung cancer). Data are similar from other Western countries. However if the condition is diagnosed very early via eff ective screening pro-grammes, mortality can be greatly reduced, and various screening options are available.
Th e US guidelines advise screening people every ten years from the age of 50 via colonoscopy, or every fi ve years via virtual colonoscopy, fl ex-ible sigmoidoscopy or double-con-trast barium enema. Th e reported mortality reduction ranges from 60–70% in the participating popula-tion but, because of the nature of the procedures, screening adherence is problematical. Th e EU recommends biennial screening using the fecal occult blood test (FOBT). Such tests are usually mailed to older Euro-pean residents to carry out at home, with both instructions on use and where to return tests on completion. Although this population screening method is easy and convenient it is not very reliable; specifi city is low. Ingesting certain foods and drugs prior to testing, as well as conditions such as haemorrhoids, gastrointesti-nal ulcers and infl ammations can all give false positive results. Sensitivity is also very low: various trials indi-cate that around 50% of tumours are not detected, and that reduction in mortality as a result of these screen-ing programmes ranges from only 15–21%.
Although population screening uti-lizing CRC tumour markers would seem to be an ideal approach, in practice previously developed tests incorporating CEA combined with CA 19-9 have not provided high enough sensitivity. However, a project carried out by several Rus-sian centres may well have found the solution. Th e researchers have
developed a 3D hydrogel-based bio-chip that utilizes autoantibodies to detect specifi c, tumour-associated glycans in serum. Th is test format, which allows a more equal distribu-tion of the molecular probes than planar systems, simultaneously measures protein-based tumour
markers, the autoantibodies-to-glycans ratio, and immunoglobulin levels. By testing healthy controls, patients with CRC and patients with infl ammatory bowel disease, it was possible to defi ne both prognostic and diagnostic signatures. Th e pro-totype allowed diagnosis of CRC
with a specifi city of 95% and a sen-sitivity of 87%. Th e testing system is predicted to reach clinical labora-tories in Russia in the near future. Hopefully the end result will be a simple, highly specifi c and sensitive test for CRC that can be performed at home.
An ideal method for colorectal cancer screening?
STart Max®
- ©
2015
Dia
gnos
tica
Stag
o - A
ll ri
ghts
res
erve
d - N
on-c
ontr
actu
al p
hoto
s - 0
3/20
16on
-con
trtu
actu
alp
al p
hoto
hot
s - 0
3/20
16
Simplicity born from ExpertiseDiscover the STart Max®, the new semi-automated instrument from the Max Generation.Designed by Stago, the expert in Coagulation, the STart Max® remains simple to use but with true innovation to achieve a maximum performance.Start with Max, stay with Max!
MaxInnovation
MaxAccuracy
MaxReliability
MaxPracticality
www.cli-online.com & search 27141
– June 20163EDITOR’S LETTER
001_017_CLI_JUNE_2016.indd 3 15/06/16 16:15

ContentsFRONT COVERFRONT COVER
FEATURESFEATURES
[6 - 16] MOLECULAR DIAGNOSTICS
[6 - 10] Diagnosis of Pneumocystis jirovecii pneumonia
[12- 16] Proteomic approach to investigate ALL biomarkers for early diagnosis and treatment evaluation
[18 - 31] KIDNEY DISEASE
[18 - 19] Current approaches for the detection of acute kidney injury
[20 - 26] Zinc oxide nanorod-based acute kidney injury biomarker detection technology and potential clinical implications
[28 - 31] Novel nephrological markers: anti-PLA2R, anti-THSD7A and uromodulin
[32 - 33] LABORATORY SPOTLIGHT
Faster viral load results for an improved clinical service
REGULARSREGULARS[3] Editor’s letter
[34] Industry news
[35 - 38] Product news
[38] Calendar of events
The proteomic analysis of serum from pediatric patients with B-cell acute lymphoblastic leukemia (B-ALL) makes it possible to identify candidate biomarker proteins, for use in early diagnosis and evaluation of treatment. This approach is an alternative to traditional techniques that can investigate the disease from another perspective. Acute lymphoblastic leukemia is the most common malignant cancer in childhood and the symptoms of childhood cancer are diffi cult to recognize.
Also in this issue :
Diagnosis of P. jiroveciipneumonia Pg. 6
Detection of acute kidney injury
ZnO nanorod-based assayfor AKI biomarkers Pg. 20
Rapid test range for viral infections
Pg.35
New reagent to measure dabigatran
Pg.37
Compact hematology analyser
Pg.38
Candidate biomarkers for early diagnosis of acute lymphoblastic leukemia Pg.12
News updates on www.cli-online.com | June 2016 | Volume 40
by MP Diagnostics
by Stago
by Abbott Diagnostics
For submission of editorial material, contact the editors at [email protected]
For advertising information, go online to www.cli-online.com, simply click on ‘Magazine’
and ‘Media Information’ or contact Astrid Wydouw at [email protected]
Clinical lab professionals are entitled to receive the digital edition of CLI for the next 12 months com-pletely free of charge. To begin a new subscription or to continue your existing free subscription go to
www.cli-online.comClick on Free Subscription and follow instructions
COMING UP IN CLI SEPTEMBER 2016
Pathology focus
MS in the clinical lab
Free Subscription for Clinical lab professionals
ISSN 1373-1580
Av. Princesse Elisabeth 176 • B1030 Brussels, BelgiumTel. +32-2-240 26 11 • Fax: +32-2-240 26 18
www.cli-online.com
Managing EditorAlison Sleigh, Ph.D.
Contributing EditorFrances Bushrod, Ph.D.
News EditorTony Spit, Ph.D.
Editorial CoordinatorShirley Waring
Editor in Chief/PublisherBernard Léger, M.D.
Advertising Coordinator
Jennifer Christophers
Circulation ManagerArthur Léger
Publishing Executive / Advertising ManagerAstrid Wydouw
WebmasterJennifer Christophers
©2016 by PanGlobal Media bvba-sprl. Production & Lay-out by Studiopress Communication, Brussels.
Circulation Controlled by Business of Performing Audits, Shelton, CT, USA.
The publisher assumes no responsibility for opinions or state-ments expressed in advertisements or product news items. The opinions expressed in by-lined articles are those of the author and do not necessarily refl ect those of the publisher. No conclusion can be drawn from the use of trade marks in this publication as to whether they are registered or not.
SINCE 1977
001_017_CLI_JUNE_2016.indd 4 15/06/16 16:15

STA R Max® and STA Compact Max®2 : More than just coagulation analysers, a completeStago solution to maximise your productivity.
Con
cept
ion
agen
ceL2
R.c
om -
©20
15 D
iagn
ostic
a S
tago
- A
ll rig
hts
rese
rved
- N
on-c
ontra
ctua
l pho
tos
- 12/
2015
MaxInnovation
MaxProductivity
MaxVersatility
Max Reliability
www.cli-online.com & search 27142
001_017_CLI_JUNE_2016.indd 5 15/06/16 16:16

IntroductionPneumocystis jirovecii (previously Pneu-mocystis carinii) is a pathogen capable of causing life threatening Pneumocys-tis pneumonia (PCP) in the immuno-compromised with case fatality rates among those hospitalized of around 10% [1]. PCP typically occurs in indi-viduals with hematological malignan-cies on chemotherapy or with other causes of acquired cellular immunode-ficiency or, most frequently, in human immunodeficiency virus (HIV)-posi-tive individuals with CD4 T-cell counts <200 cells/μL or <14% of total white cell count [2, 3]. First-line treatment is co-trimoxazole, a combination of the antibiotics sulfamethoxazole and tri-methoprim, at high dose for 3 weeks, which has the clinically significant potential side effects of bone marrow
suppression, rash and bronchial hyper-sensitivity. Unfortunately the classical clinical presentation of PCP of progres-sive dry cough, dyspnoea and malaise is non-specific and chest examination and radiographs are often normal or near normal [4]. Oxygen desaturation on exercise is a helpful clinical sign in the right patient population [5]. Fur-thermore, many individuals with PCP do not produce sputum, so laboratory confirmation can be challenging. Given the serious nature of the illness and the possible side effects of treatment, accurate diagnosis is key to making an informed treatment decision.
Incidence of PCP among HIV-posi-tive individuals has declined since the widespread availability of antiretroviral therapy (ART) and has also declined
as a cause of hospitalization of HIV-positive individuals [6]. In a study in a large HIV centre in London, mortal-ity for all hospitalizations was around 10% during the first 10 years of avail-ability of effective ART [1]. In our unit a decrease in mortality among those admitted to intensive care with PCP was seen between the periods of 1986–1995 and 1996–2004. This improve-ment is thought to be due to advances in critical care rather than treatment of PCP itself [7].
Reaching a diagnosisTraditional methodsP. jirovecii is a fungus that cannot be cultured in vitro and so the organism is identified using histochemical staining techniques of fluid samples. Grocott-Gomori methenamine silver nitrate or direct immunofluorescence monoclo-nal antibody (IFA) stains on deep res-piratory samples are generally regarded as the gold standard in diagnosis [8]. The life cycle of P. jirovecii is demon-strated by trophic, pre-cystic and cystic forms by morphological criteria. Diag-nosis through microscopy of the cystic stage requires significant technical expertise and can still lead to false-neg-ative results. In florid disease, P. jirovecii is present throughout the bronchial tree, from the upper respiratory tract down to the alveolar surface. Induced sputum samples are recommended by most guidelines, if routinely available, as spontaneously expectorated sputum is not considered an adequate alveo-lar sample and microscopy could be falsely negative. If the results of testing on induced sputum are not conclusive then a bronchoalveolar lavage (BAL) is recommended (sensitivity 86–98%) [9, 10]. In clinical practice, induced sputum is often not readily available, and BAL may not be possible due to hypoxia or may lead to a delay in sam-pling of several days; therefore, in clini-cal practice spontaneously expectorated samples are often processed. The dis-advantages of this are twofold: a lower yield of cystic forms for visualization and potential for false-positive results due to colonization. Only in rare cases would a lung biopsy be appropriate
Diagnosis of Pneumocystis jirovecii pneumoniaDiagnosis of Pneumocystis jirovecii pneumonia (PCP) is conventionally based on direct staining and visualization. Challenges in obtaining alveolar samples have stimulated interest in techniques for detection of Pneumocystis DNA in non-invasive samples, which can give good sensitivity and specifi city. Robust diagnosis is key to ensuring appropriate therapy.
by Dr Farnaz Dave, Dr Ashley Horsley, Dr Thomas Whitfi eld and Dr Clare van Halsema
– June 2016 Molecular diagnostics6
001_017_CLI_JUNE_2016.indd 6 15/06/16 16:16

DxN VERIS consolidates extraction, amplifi cation and detection onto a single platform, saving hands-on time as technicians are not required to pipette samples and reagents, and also saves vital laboratory space. Simple to learn and easy to use, DxN VERIS enables your team to do the work you want, when you want.
See how DxN VERIS can work for your team at:www.beckmancoulter.com/moleculardiagnostics
With the DxN VERIS Molecular Diagnostics System.*
*Not for sale or distribution in the U.S.; not available in all markets.©2016 Beckman Coulter, Inc. All rights reserved. Beckman Coulter, the stylized logo and the Beckman Coulter product and service names mentioned herein are trademarks or registered trademarksof Beckman Coulter, Inc. in the United States and other countries.
For Beckman Coulter’s worldwide offi ce locations and phone numbers,please visit “Contact Us” at www.beckmancoulter.com Move healthcare forward.
OPTIMISE MY TEAM’S EFFICIENCY
NOW I CAN
www.cli-online.com & search 27129
001_017_CLI_JUNE_2016.indd 7 15/06/16 16:16

(sensitivity 95–98%) in circumstances of poor response to empirical treatment and negative initial testing [9].
Molecular techniquesMolecular testing of lower respira-tory tract secretions and blood is an alternative and operator-independent method for confirming the presence of P. jirovecii. Nucleic acid amplification techniques (NAAT) can be used with a number of primers targeting different substrates – most commonly the major surface glycoprotein (MSG), mitochon-drial large subunit (MTLSU) rRNA and internal transcribed spacer (ITS) region genes [11]. One potential pitfall with these techniques is that the detection of specific nucleic acid sequence does not distinguish between colonization and disease or between viable and non-viable organisms [12]. P. jirovecii RNA is less stable and rapidly degraded after cell death so is a more reliable marker of viable organisms. Modification of standard PCR protocols with quantita-tive methods (e.g. quantitative touch-down PCR) may help to differentiate between colonization and infection through the selection of thresholds to maximize sensitivity [13]. An added advantage of these molecular tech-niques is they may provide information on molecular epidemiology and resist-ance-associated mutations in the gene encoding dihydropteroate synthase (DHPS), the target of sulfamethoxazole, though the benefit of this is controver-sial [14]. One caveat to this is the poten-tial for point mutations in DNA paired with primer sequences and risk of false negatives as a result.
These molecular tests are said to have increased sensitivity compared with cyst staining techniques but variable specificity depending on the specimens used, the primer chosen and whether treatment has been started [15]. The three most commonly assessed speci-men groups are sputa (ideally induced), oropharyngeal washes (OPW) and blood. The clinical relevance of the known detectability of P. jirovecii DNA in whole blood has not been fully estab-lished but could represent colonization as well as disease [16]. The use of cycle threshold values has been proposed as a method to distinguish coloniza-tion from disease using BAL samples, although further studies are needed to validate cut offs on different samples [17].
Although there has been a widespread adoption of NAATs the current British HIV Association guidance, and that of similar professional bodies, still sug-gests combining them where available with a traditional visualization tech-nique as described previously and per-forming them on alveolar specimens where possible to increase sensitivity and specificity [10, 18].
PCP diagnosis by detection of DNA in non-respiratory samplesDue to the variability in sampling methods, the challenges in obtaining ideal samples and the need for prompt diagnosis research has been conducted on the use of NAATs on OPW and blood. Samples are relatively non-inva-sive, collection is straight-forward and no special equipment or preparation is required. A study in our unit com-pared NAATs on OPW and blood with sputum, spontaneously expectorated or induced, using primers for the P. jirovecii MTLSU rRNA gene [19].
All patients were consenting adults pre-senting to a regional infectious disease unit who were being investigated for PCP as part of routine care. A spectrum of patients was included of different pre-test probabilities to allow estimates of sensitivity and specificity. Each par-ticipant was asked to provide sputum (spontaneous or induced), OPW and blood for analysis. OPW was obtained by gargling of normal saline for 10 to 30 seconds without any additional preparation.
Forty-five participants were included, 41 male (91%), 38 Caucasian (84%) with a median age of 39 years. One partici-pant was an HIV-negative renal trans-plant recipient. Forty-four were HIV-positive with a median CD4 count of 64 cells/mL. Thirty-five of the 44 were not on ART with a median HIV RNA of 164 550 copies/mL. Thirty-nine of the 45 started empirical treatment for PCP a median of 2 days before sampling. We compared the sensitivity and specificity of tests on blood and OPW compared with sputum. Sputum PCR was posi-tive in 60% of participants and in this group 47% of OPW and 50% of blood PCRs were positive. None with nega-tive sputum PCR had positive OPW or blood PCR. A diagnosis of PCP could be reached in 14 of 16 patients with positive NAAT on sputum using these non-respiratory specimens.
Among those with P. jirovecii DNA detected in sputum a sensitivity of 47% for OPW was increased to 80% when considering only OPW samples taken within 48 hours of starting treatment. When this was combined with blood sample testing in the same time frame the sensitivity increased to 88%, which is comparable to that quoted in previ-ous similar studies [12, 13, 15]. There were no false positives based on no OPW or blood PCR positives in those with negative PCR on sputum. As the laboratory techniques used were rou-tine, few additional skills or resources were required.
Overall, using molecular tests on non-respiratory samples was of diagnostic benefit and show potential for savings in time and resources. The molecular tests provide excellent specificity and good sensitivity comparable with sputum without proceeding to time-consuming and invasive tests [20]. However, in view of uncertainty regarding the specificity of testing these non-invasive samples at all, results must be interpreted with care and in the right clinical context.
ConclusionsPCP diagnosis remains a combina-tion of clinical suspicion and physical examination, supported by radiologi-cal and microbiological investigations. Using a combination of traditional microscopy with staining and NAAT on appropriate specimens, plus inter-pretation of results in the clinical con-text a clear diagnosis can be reached in most cases and this may prevent unnecessary treatment. Using non-respiratory specimens taken early to maximize sensitivity could reduce the requirement for invasive testing or diagnostic uncertainty.
Future developmentsWe expect the use of NAATs to become even more widely available and useful diagnostic aids alongside traditional techniques. With a plethora of protocols the sensitivity, specificity and utility of these will improve further over time. Combination with other laboratory techniques such as β-D-glucan may be similarly useful. Given the inability to culture the organism and so look for in vitro susceptibility to sulfamethoxazole-based treatment, molecular methods for detecting mutations and potential resistance may develop as a routinely used test.
– June 2016 Molecular diagnostics8
001_017_CLI_JUNE_2016.indd 8 15/06/16 16:16

SEKISUIDIAGNOSTICS.COM
Clinical Chemistry is a passion for any laboratory professional committed to keeping
their healthcare system running smoothly. At Sekisui Diagnostics, we share your obsession
for quality results and understand your need for exceptional support. For over 30 years
we’ve been developing and providing the highest quality clinical
reagents to laboratories and diagnostics manufacturers. And now
our relationship with chemistry continues — announcing our new
clinical chemistry system, the compact and efficient SK500, with
a full menu of quality SEKURE™ reagents.
You’re invested. We’re investing. SK500 the perfect system for your
clinical lab. We think you’ll love it!
Clinical Chemistry...it’s what we do!™
© 2015 Sekisui Diagnostics, LLC. All rights reserved. The letters SK, the SK logo, the word SEKURE and the SEKURE logo are trademarks of Sekisui Diagnostics, LLC.
COMING SOON
See us at AACC Booth #1337
www.cli-online.com & search 27243
001_017_CLI_JUNE_2016.indd 9 15/06/16 16:16

References1. Walzer P, Evans H, Copas A, Edwards S, Grant A, Miller R. Early predic-
tors of mortality from Pneumocystis jirovecii pneumonia in HIV-infected patients: 1985–2006. Clin Infect Dis. 2008; 46: 625–633.
2. Phair J, Munoz A, Detels R, Kaslow R, Rinaldo C, Saah A. The risk of Pneumocystis carinii pneumonia among men infected with human immu-nodeficiency virus type 1. Multicenter AIDS Cohort Study Group. N Engl J Med. 1990; 322: 161–165.
3. Kaplan J, Hanson D, Navin T, Jones J. Risk factors for primary Pneumo-cystis carinii pneumonia in human immunodeficiency virus-infected ado-lescents and adults in the United States: reassessment of indications for chemoprophylaxis. J Infect Dis 1998; 178: 1126–1132.
4. Opravil M, Marincek B, Fuchs WA, Weber R, Speich R, Battegay M, Russi EW, Lüthy R. Shortcomings of chest radiography in detecting Pneumocys-tis carinii pneumonia. J Acquir Immune Defic Syndr. 1994; 7: 39–45.
5. Smith D, McLuckie A, Wyatt J, Gazzard B. Severe exercise hypoxaemia with normal or near normal X-rays: a feature of Pneumocystis carinii infection. Lancet 1988; 2: 1049–1051.
6. Grubb J, Moorman A, Baker R, Masur H. The changing spectrum of pul-monary disease in patients with HIV infection on antiretroviral therapy.
AIDS 2006; 20:1095–1107.7. Travis J, Hart E, Helm J, Duncan T, Vilar J. Retrospective review of Pneu-
mocystis jirovecii pneumonia over two decades. Int J STD AIDS 2009; 20: 200-201.
8. Thomas J, Limper A. Pneumocystis pneumonia. N Engl J Med. 2004; 350: 2487–2498.
9. Broaddus C, Dake MD, Stulbarg MS, Blumenfeld W, Hadley WK, Golden JA, Hopewell PC. Bronchoalveolar lavage and transbronchial biopsy for the diagnosis of pulmonary infections in the acquired immunodeficiency syndrome. Ann Intern Med. 1985; 102: 747–752.
10. Nelson M, Dockrell D, Edwards S; BHIVA Guidelines Subcommittee, Angus B, Barton S, Beeching N, Bergin C, Boffito M, et al. British HIV Association and British Infection Association guidelines for the treat-ment of opportunistic infection in HIV-seropositive Individuals 2011. HIV Med. 2011; 12(Suppl 2): 1–140.
11. Lu J, Chen C, Bartlett M, Smith J, Lee C. Comparison of six diff erent PCR meth-ods for detection of Pneumocystis carinii. J Clin Microbiol. 1995; 33: 2785–2788.
12. Huggett J, Taylor M, Kocjan G, Evans H, Morris-Jones S, Gant V, Novak T, Costello A, Zumla A, Miller R. Development and evaluation of a real-time PCR assay for detection of Pneumocystis jirovecii DNA in bronchoalveo-lar lavage fluid of HIV-infected patients. Thorax 2008; 63: 154–159.
13. Larsen H, Huang L, Kovacs J, Crothers K, Silcott V, Morris A, Turner J, Beard C, Masur H, Fischer S. A prospective, blinded study of quantita-tive touch-down polymerase chain reaction using oral-wash samples for diagnosis of Pneumocystis pneumonia in HIV-infected patients. J Infect Dis. 2004; 189: 1679–1683.
14. Durand-Joly I, Chabé M, Fabienne Soula F, Delhaes L, Camus D, Dei-Cas E. Molecular diagnosis of Pneumocystis pneumonia. FEMS Immunol Med Microbiol. 2005; 45: 405–410.
15. Olsson M, K. Strålin K, Holmberg H. Clinical significance of nested poly-merase chain reaction and immunofluorescence for detection of Pneu-mocystis carinii pneumonia. Clin Microbiol Infect. 2001; 7: 492–497.
16. Rabodonirina M, Cotte L, Boibieux A, Kaiser K, Mayencon M, Raffenot D, Trepo C, Peyramond D, Picot S. Detection of Pneumocystis carinii DNA in blood specimens from human immunodeficiency virus-infected patients by nested PCR J. Clin Microbiol. 1999; 37: 27–131.
17. Fauchier T, Hasseine L, Gari-Toussaint M, Casanova V, Marty P, Pomares C. Detection of Pneumocystis jirovecii by quantitative PCR to differenti-ate colonization and pneumonia in immunocompromised HIV-positive and HIV-negative patients. J Clin Micro. 2016; 54: 1487–1495.
18. Centers for Disease Control and Prevention, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. Guidelines for the prevention and treatment of opportunistic infections in HIV-infected adults and adolescents AIDSinfo 2013. (https://aidsinfo.nih.gov/contentfiles/lvguidelines/adult_oi.pdf)
19. van Halsema C, Johnson L, Baxter J, Douthwaite S, Clowes Y, Guiver M, Ustianowski A. Diagnosis of Pneumocystis jirovecii pneumonia by detec-tion of DNA in blood and oropharyngeal wash, compared with sputum. AIDS Res Hum Retroviruses 2016; 32: 463–466.
20. de Oliveira A, Unnasch T, Crothers K, Eiser S, Zucchi P, Moir J, Beard C, Lawrence G, Huang L. Performance of a molecular viability assay for the diagnosis of Pneumocystis pneumonia in HIV-infected patients. Diagn Microbiol Infect Dis. 2007; 57: 169–176.
The authorsFarnaz Dave MBChB, MRCP; Ashley Horsley MBChB, MRCP; Thomas Whitfield MBChB, MSc, MRCP; Clare van Halsema* MBChB, MRCP, MD, DipHIVMedNorth West Infectious Diseases Unit, North Manchester General Hospital, Manchester M8 5RB, UK
*Corresponding authorE-mail: [email protected]
– June 2016 Molecular diagnostics10
BÜHLMANN fCAL® turbo Immuno turbidimetric fecal CALPROTECTIN Assay
BÜHLMANN Laboratories AG, Switzerland [email protected] | www.buhlmannlabs.ch
Speed, Quality and Flexibility in Calprotectin Quantification
Not
ava
ilab
le f
or s
ale
in t
he
US.
AACC 2016 Booth 4202
www.cli-online.com & search 27272
001_017_CLI_JUNE_2016.indd 10 15/06/16 16:16

1 In comparison to existing FilmArray Systems.
Syndromic Testing: The right test, the first time.Respiratory • Blood Culture ID • Gastrointestinal • Meningitis
BioFire Diagnostics, the leader in syndromic
infectious disease testing, brings
you the new FilmArray® Torch.
The FilmArray Torch is the latest
advancement in molecular infectious
disease diagnostics. Providing up to
six times more sample throughput per
square foot of benchtop space1, the
high throughput FilmArray Torch is a
fully-integrated, random and continuous
access system designed to meet your
laboratory’s syndromic infectious
disease testing needs.
The FilmArray Torch is compatible
with all existing FilmArray panels
providing the quick, comprehensive
and accurate results you’ve come to
expect from BioFire Diagnostics.
BioFireDX.com
www.cli-online.com & search 27185
001_017_CLI_JUNE_2016.indd 11 15/06/16 16:16

Background and signifi canceAcute lymphoblastic leukemia (ALL) is the most common malignant cancer in childhood, and is responsible for approxi-mately 25% of all childhood cancers and 72% of all cases of pediatric leukemia [1]. Th e current standards for diagnosis of ALL integrate the study of cell morphology, immunophenotyping and genetics/cytoge-netics, as described in the classifi cation of
lymphoid cancers published by the World Health Organization (WHO) in 2008 [2]. Of lymphoid cancers, as designated using the most recent WHO classifi cation, the purely leukemic presentation, B-lineage ALL (85 %) is the most common [3], and will be addressed in this study. Th e signs and symptoms of childhood cancer are very challenging to identify, as it is not the fi rst diagnosis to be considered for
nonspecifi c complaints, leading to poten-tial uncertainty in diagnosis. Moreover, children showing the fi rst signs of can-cer frequently do not appear severely ill, which may delay diagnosis. In addition, childhood cancer can mimic other com-mon childhood diseases and even normal developmental physiological processes [4]. In the specifi c case of ALL, early diagno-sis and treatment increase the chances of a cure [4].
Future prospects A label-free proteomic approach was used for the quantitative analysis. Other approaches could also be used in the future, for example it is possible to fi nd studies using RNA interference, mainly silencing expression of specifi c genes [5]. In our proteomic approach, for each pro-tein, the program ExpressionE selected all corresponding peptides from the samples and compared the intensities of these for relative protein quantifi cation. Using the intensity of a peptide of known quantity, alcohol dehydrogenase (ADH), the pro-gram performed self-standardization of data sets. Lists of proteins were then fi l-tered to show only those present in all three repeated injections of each sample, from which an output table was created. Th is table showed the names, access codes, and expression levels of the proteins, and indicated whether they were upregulated ≥2-fold, downregulated ≤0.5-fold, or whether they did not show signifi cant dif-ferences between the groups (unchanged), 0.5 < expression level < 2. Th e list of pro-teins generated from three injections of samples in MS, coupled with broad lim-its used for protein expression levels and serum samples used the controls (non-leu-kemic pediatric patients) may suggest that the panel of candidate protein biomarkers is clearly increased in the disease state.
Biotechnological resourcesAffi nity chromatography with α-D-galactose-binding lectin from Artocarpus incisa [6] immobilized on a Sepharo-seTM 4B gel, combined with identifi cation and quantifi cation of glycoproteins by mass spectrometry, are excellent tools for
Proteomic approach to investigate ALL biomarkers for early diagnosis and treatment evaluationThe aim of this study was to perform proteomic analysis of serum from pediatric patients with B-cell acute lymphoblastic leukemia (B-ALL) to identify candidate biomarker proteins, for use in early diagnosis and evaluation of treatment. This approach is an alternative to traditional techniques that can investigate the disease from another perspective. Acute lymphoblastic leukemia is the most common malignant cancer in childhood and the symptoms of childhood cancer are diffi cult to recognize.
by Dr M. de S. Cavalcante, Prof. A. E. Vieira-Neto, Dr R. de A. Moreira and Dr A. C. de O. Monteiro-Moreira
– June 2016 Molecular diagnostics12
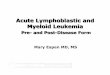
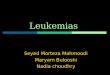
Figure 1. Graphical representation of the affi nity chromatography process on a Frutalin-immobilized column with Sepharose 4B, coupled with an ÄKTA purifi er 10 FPLC system. Peak I represents the non-retained fraction (FNR) and Peak II represents the retained fraction (FR). The fractions were obtained after elution with their respective buffers: 20 mM Tris-HCl, pH 7.4, in0.15 M NaCl (Buffer A) and 0.2 M galactose and 20 mM Tris-HCl, pH 7.4, in 0.15 M NaCl (Buffer B). The blue line represents absorbance at 280 nm and the red represents emission at 216 nm. Figure reproduced under Creative Commons 4.0 licence (http://creativecommons.org/licenses/by/4.0/) and fi rst published in Cavalcante Mde S et al. Biomarker Research 2016; 4: 1 (doi: 10.1186/s40364-016-0055-6) [14].
001_017_CLI_JUNE_2016.indd 12 15/06/16 16:16

comparative serum studies. Th e biomarker pipeline is com-monly viewed as a series of pre-clinical phases: biomarker dis-covery, and verifi cation before the fi nal clinical evaluation. Th e comparative analysis results in a list of hundreds of proteins that are diff erentially expressed between healthy and diseased samples [7]. In this study, the preclinical phase of biomarker discovery was applied and a proteomic analysis of serum samples from pediatric patients with B-ALL was performed, to analyse levels of glycoprotein expression, with the aim of identifying biomarkers to aid in the early diagnosis of B-ALL and to assess the response to induction therapy.
Th e depletion of high-abun-dance proteins in serum, human serum albumin (HSA) and IgG, followed by affi nity chromatography with the plant lectin Frutalin immobilized on SepharoseTM 4B (Fig. 1), reduced the dynamic range and increased the capacity to iden-tify lower-abundance proteins. Th e retained fraction (FR) peak containing the protein of interest was concentrated and digested, for later analysis by nano-LC-MS/MS.
Proteomic approachTh e study population was com-posed mainly of children from the lower middle class, who attended a reference hospital for the diagnosis and treat-ment of childhood cancers in the State of Ceará, Brazil. Th e study was conducted with the approval of the Research Eth-ics Committee at the Hospital Infantil Albert Sabin, asso-ciated with the Secretary of Health of the State of Ceará. Th e demographic and clinical data for the patients are sum-marized in Table 1. Th e pedi-atric patients were evaluated at two diff erent times: at diagnosis (B-ALL group; n = 10) and aft er induction therapy (AIT group; n = 10). Samples of healthy chil-dren (Control group; n = 10) were obtained for comparison.
Th e diff erentially expressed proteins were used for path-way analysis. Swiss-Prot accession numbers were inserted into the Search Tool for the Retrieval of Interact-ing Genes/Proteins (STRING) soft ware, version 9.05 (avail-able at http://string.embl.de/), with the following analysis parameters: Homo sapiens, confi dence level 0.400–0.900, using the active prediction method [8].
Biomarker panel for ALL diagnosisA panel of protein biomarker candidates has been developed for pre-diagnosis of B-ALL and also provide informa-tion that would indicate a favourable response to treat-ment aft er induction therapy. In the proteomic analysis, a total of 96 proteins were iden-tifi ed. Leucine-rich alpha-2-glycoprotein 1 (LRG1), Clusterin (CLU), thrombin
(F2), heparin cofactor II (SERPIND1), alpha-2-mac-roglobulin (A2M), alpha-2-antiplasmin (SERPINF2), Alpha-1 antitrypsin (SER-PINA1), Complement factor B (CFB) and Complement C3 (C3) were over-expressed in the B-ALL compared to the Control and AIT groups, and were, therefore, identi-fi ed as candidate biomarkers for early diagnosis of B-ALL. Th e AIT group showed no
– June 201613
MPLICON Real-time PCR KitsQuality you can Trust
See you at Booth #3635
STIsN. gonorrhoeae-SCREENM. genitaliumM. hominis
T. vaginalis V-TYPE -TYPE -SCREEN + QUANT (2C)
-SCREEN + QUANT (4C)
RespiratoryM. tuberculosis Complex
Flaviviruse Virus Type
eeeeSeSeeSeeSSeeSSSS
www.mpbio.com/[email protected]
www.cli-online.com & search 27219
001_017_CLI_JUNE_2016.indd 13 15/06/16 16:16

signifi cant diff erences in the expression levels of these pro-teins compared to the Control group, and did not show any
signifi cant change in the level of expression of these proteins, a fact that further reaffi rms the presence of these potential
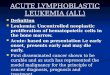
biomarkers in a disease state, as all patients achieved com-plete remission aft er treatment (Fig. 2). Our results also con-fi rm the important relation-ship between cancer and phe-nomena associated with blood coagulation. Several studies have reported that approxi-mately 50% of patients with malignant disease and more than 90% of those that evolve to metastasis present evidence of abnormalities in coagula-tion and/or fi brinolysis [9–13].
ConclusionAcute lymphoblastic leu-kemia is the most common malignant cancer in child-hood and this proteomic approach is an alternative to traditional techniques, since the signs and symptoms of childhood cancer are very challenging to identify. LRG1, CLU, F2, SERPIND1, A2M, SERPINF2, SERPINA1, CFB, and C3 were identified as candidate biomarkers for early diagnosis of B-ALL; all were over-expressed in the B-ALL group compared to the Control and AIT groups. The AIT group did not display any significant changes in the expression levels of these
proteins, compared to the Control group. All patients in the AIT group achieved com-plete remission after treat-ment; this indicates that these biomarkers are only present in the disease state. These candidate biomarkers may improve the pre-diagnosis of B-ALL, which is currently dif-ficult to diagnose in the early stages; the biomarkers may also provide key information on the response to treatment after induction therapy. Fur-ther clinical and genomic studies will be important to improve the survival of chil-dren with this disease.
AcknowledgementsFINEP, CNPq, RENORBIO-UNIFOR, ALBERT SABIN HOSPITALTh is article is a summary of a paper fi rst published in Biomarker Research: Cavalcante Mde S, Tor-res-Romero JC, Lobo MD, Moreno FB, Bezerra LP, Lima DS, Matos JC, Moreira Rde A, Monteiro-Moreira AC. A panel of glyco-proteins as candidate biomarkers for early diagnosis and treatment evaluation of B-cell acute lym-phoblastic leukemia. Biomarker Research 2016; 4: 1 (doi: 10.1186/s40364-016-0055-6) [14].
– June 2016 Molecular diagnostics14
www.oriondiagnostica.com
QuikRead go®Fast and reliable test results » CE-marked tests and system for point-
of-care: CRP, CRP+Hb, Strep A, iFOBT
» QuikRead go CRP US FDA cleared
for clinical laboratory use
» Thousands of users worldwide
» For healthcare professionals.
www.cli-online.com & search 27268
Code assigned Gender Age
at diagnosisFAB
classificationImmuno-phenotypical
classification Karyotype Risk group MRD Treatment
outcome
P1 M 3 L1 Common Absence of metaphases LR − CR
P2 F 3 L1 Pre-B Absence of metaphases LR − CR
P3 F 5 L1 Common 56,XX,+X,+4,+6,+8,+10,+11,+14,+17,+21,+mar/46,XX LR − CR
P4 M 2 L1 Common 46,XY LR − CR
P5 F 2 L1 Common 46,XX LR − CR
P6 F 3 L1 Common 54,XX,+X,+6,+15,+15,+17,+18,+21,+21/46,XX LR − CR
P7 F 5 L1 Common 47,XY,+21 c LR − CR
P8 M 6 L1 Common Absence of metaphases LR − CR
P9 F 5 L1 Pre-B 46, XX LR − CR
P10 M 3 L1 Pre-B 46,XY LR − CR
Table 1: Summary of characteristics of patients with B-ALL. Code: Internal register assigned for the study; M: Male; F: Female; LR: Low Risk; MRD: Minimum Residual Disease; CR: Complete remission. Table reproduced under Creative Commons 4.0 licence (http://creativecommons.org/licenses/by/4.0/) and fi rst published in Cavalcante Mde S et al. Biomarker Research 2016; 4: 1 (doi: 10.1186/s40364-016-0055-6) [14].
001_017_CLI_JUNE_2016.indd 14 15/06/16 16:16

A New Breakthrough in Hemostasis Quality Management.
New ACL TOP Family 50 Series* Extending standardization beyond the analytical phase
The new ACL TOP Family 50 Series offers the most advanced automation and quality management for routine and specialty Hemostasis testing in mid- to high-volume labs. All models are standardized and offer automated pre-analytical sample integrity checks to identify under-filled sample tubes, abnormal sample aspiration potentially caused by clots, and assay-specific interference from hemolysis, lipemia and bilirubin. Plus, new lab accreditation tools make compliance easier. Better efficiency and quality management for you—better quality care for your patients.
The ACL TOP Family 50 Series. Quality in. Quality out.
For more information, please contact your local Werfen representative/distributor or visit www.werfen.com.©2016 Instrumentation Laboratory. All rights reserved.* Not available in all countries.
www.cli-online.com & search 27192
VISIT US AT AACC SHOW BOOTH 801
001_017_CLI_JUNE_2016.indd 15 15/06/16 16:16

References1. Scheurer ME, Bondy ML, Gurney JG. Epidemiology of Childhood Can-
cer. In: Pizzo PA, Poplack DG, editors. Principles and practice of pediatric oncology, 6th ed, pp2–16. Lippincott Williams and Wilkins 2011.
2. Vardiman JW, Thiele J, et al. The 2008 revision of the World Health Organi-zation (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 2009; 114: 937–951.
3. Chiaretti S, Zini G, Bassan R. Diagnosis and subclassification of acute lymphoblastic leukemia. Mediterr J Hematol Infect Dis. 2014; 6: e2014073.
4. Rodrigues KE, Camargo B. Diagnóstico precoce do câncer infantil: respon-sabilidade de todos. Rev Assoc Med Bras. 2003; 49: 29–34 (in Portuguese).
5. Trougakos IP, So A, et al. Silencing expression of the clusterin/apolipo-protein j gene in human cancer cells using small interfering RNA induces spontaneous apoptosis, reduced growth ability, and cell sensitization to genotoxic and oxidative stress. Cancer Res. 2004; 64: 1834–1842.
6. Monteiro-Moreira ACO, Pereira HD, et al. Crystallization and preliminary x-ray diffraction studies of Frutalin, an α-D-galactose-binding lectin from Artocarpus incisa seeds. Acta Crystallographica Session F, 2015.
7. Parker CE, Borchers CH. Mass spectrometry based biomarker discovery, verification, and validation--quality assurance and control of protein bio-marker assays. Mol Oncol. 2014; 8(4): 840–858.
8. Jensen LJ, Kuhn M, et al. STRING 8–a global view on proteins and their functional interactions in 630 organisms. Nucleic Acids Res. 2009; 37: D412–416.
9. Kwon H-C, Oh SY, et al. Plasma levels of prothrombin fragment F112, D-dimer and prothrombin time correlate with clinical stage and lymph node metastasis in operable gastric cancer patients. Jpn J Clin Oncol. 2008; 38: 2–7.
10. Bick RL. Coagulation abnormalities in malignancy: a review. Semin Thromb Hemost. 1992; 18: 353–372.
11. Luzzatto G, Schafer Al. The prethrombotic state in cancer. Semin Oncol. 1990; 17: 147–159.
12. Nigel O’Connor, Gozzard DI, et al. Haemostatic abnormalities and malig-nant disease. Lancet 1986; 8: 303–304.
13. Hillen HF. Thrombosis in cancer patients. Ann Oncol. 2000; 11: 273–276.14. Cavalcante Mde S, Torres-Romero JC, et al. A panel of glycoproteins as
candidate biomarkers for early diagnosis and treatment evaluation of B-cell acute lymphoblastic leukemia. Biomarker Research 2016; 4: 1 (doi: 10.1186/s40364-016-0055-6).
The authorsMárcio de Souza Cavalcante1, Antonio Eufrásio Vieira-Neto², Renato de Azevedo Moreira3, Ana Cristina de Oliveira Monteiro-Moreira3*1Northeast Network of Biotechnology (RENORBIO), State Uni-versity of Ceará, Ceará, Brazil.2Center of Experimental Biology (NUBEX), University of For-taleza (UNIFOR), Ceará, Brazil.3Department of Biochemistry and Molecular Biology, Federal University of Ceará, Ceará, Brazil.4Development and Technological Innovation in Drug Program, Federal University of Ceará, Ceará, Brazil5Reference Center at Children’s Cancer Diagnosis and Adoles-cents Dr. Murilo Martins, Albert Sabin Hospital, Ceará, Brazil.
*Corresponding authorE-mail: [email protected]
– June 2016 Molecular diagnostics16
MEET US AT AACC, STAND 3538
MedixMABmonoclonal antibodies
MedixMAB by designcustom recombinant antibodies
MedixMABfab-fragments
MedixMABcontract manufacturing
MedixAntigensrecombinant antigens
www.medixbiochemica.com
FOR EXCELLENCE IN DIAGNOSTICS– We’re bound to deliver
www.cli-online.com & search 27270
Figure 2. Panel of candidate protein biomarkers for B-ALL. Blue columns represent the expression levels of the proteins in B-ALL patients at the time of diagnosis in relation to the control. Green columns represent the expression levels of the proteins in B-ALL patients after induction therapy (day 35) relative to controls. (*) (p<0.05). Figure reproduced under Creative Commons 4.0 licence (http://creativecommons.org/licenses/by/4.0/) and fi rst published in Cavalcante Mde S et al. Biomarker Research 2016; 4: 1 (doi: 10.1186/s40364-016-0055-6) [14].
001_017_CLI_JUNE_2016.indd 16 15/06/16 16:16

Our Respiratory Multiplex Array provides comprehensive screening for infections of both the upper and lower respiratory tracts.
The upgraded Version 2 Array simultaneously detects 22 bacterial and viral pathogens from a single sputum, lavage or nasopharyngeal
sample reducing testing time for patients and the laboratory.
RESPIRATORYRANDOX
Our innovative Biochip Array Technology (BAT) provides a number of benefits:
• Complete patient profile from a single sample for accurate diagnosis
• Rapid turnaround time improving patient care
• Cost effective testing
PLEASE VISIT US AT
AACC BOOTH #2941
www.cli-online.com & search 27197
001_017_CLI_JUNE_2016.indd 17 15/06/16 16:16

BackgroundAcute kidney injury (AKI) is a rec-ognized complication in hospitalized patients. A report in 2009 from National Confi dential Enquiry into Patient Out-come and Death (NCEPOD) suggested that AKI was frequently undetected in hospital patients thus contributing to patient morbidity and mortality [1]. Clinical guidelines for recognition and treatment for acute kidney injury were published by NICE (the National Insti-tute for Health and Care Excellence) in 2013 and reported an associated mortal-ity with AKI of more than 25–30% [2]. Th is guideline also recognized the preva-lence of AKI in the primary care popula-tion in patients with or without acute ill-ness. NICE also recognized the impact of AKI on healthcare resources, with costs (excluding those in the community) of £434–620 million per year, more than that associated with breast, lung and skin cancer combined [2].
AKI is characterized by an acute loss of the kidney’s excretory capacity leading to accumulation of waste products such as urea and creatinine, and decreased urine output. It is associated with rapid decline in glomerular fi ltration rate and increases in
potassium, phosphate and hydrogen ions. It has varied causes and may be secondary to a non-renal event, thus may be common in hospitalized patients and critically ill patients. It may go undetected in primary care as it can occur without any symptoms. Th ere are associations between co-morbid-ities, current medications, acute illness and AKI resulting in the high morbidity associ-ated with the condition and the impact on healthcare resources [3].
One of the most common causes of AKI is pre-renal injury due to hypovolemia (a decreased volume of circulating blood). Th is is thought to be the cause of more than 70% of AKI in the community [4]. Th is may be exacerbated in patients pre-scribed certain medications and should be considered carefully by primary care clinicians when assessing patients for AKI [5]. Other causes of AKI are highlighted in Table 1.
Risk factors associated with development of AKI include age, ethnicity, co-morbidi-ties and use of certain medications [3]. It is important to detect the injury as early as possible to prevent the long-term changes in renal function that have been noted to be associated with even less-severe AKI [6].
Defi ning acute kidney injuryPrevious defi nitions of acute kidney injury had been published, such as RIFLE criteria (Risk Injury, Failure, Loss, End stage renal failure) and AKIN (acute kidney injury network) [7]. KDIGO (Kidney Disease Improving Global Outcomes) published clinical practice guidance in 2011 that cat-egorized AKI based on changes in serum creatinine and/or urine output as defi ned in both of these previous publications [8]. Th is categorized AKI into stages 1, 2 and 3 dependent on severity. Evidence sug-gests that even small, reversible changes in creatinine are associated with worse out-comes, and indeed AKI and severity of AKI is associated with development of chronic kidney disease [6].
Th e KIDIGO criteria for AKI references changes in creatinine or changes in urine output as a marker for acute kidney injury [8]. Urine output may be the functional marker of kidney function, but can be dif-fi cult to monitor. Accurate fl uid balance recordings are imperative in management and prevention of AKI in a hospitalized setting, but may be diffi cult to do accurately especially if the patient is mobile and able to use a toilet unaided. Th is is also diffi cult to assess in community patients who obvi-ously will not have recorded urine output as specifi ed in the guidelines. Th us serum creatinine measurements can be used as a marker of kidney function.
Detection of acute kidney injuryCreatinine is used a biomarker for renal function because it is easy and inexpen-sive to measure. It is also part of most
Current approaches for the detection of acute kidney injuryAcute kidney injury is a recognized complication in hospitalized patients and is associated with a high morbidity and high mortality. This brief article aims to summarize the need for early detection of acute kidney injury and the current approach within NHS England to identify such patients.
by Charlotte Fairclough
– June 2016 Kidney disease18
Type of acute kidney injury Cause
Pre-renalHypovolemia
VasoconstrictionSepsis
Intrinsic
Intrinsic damage, e.g. infection, medicationGlomerular damage
Tubular damage, e.g. contrast agents, other nephrotoxinsVascular
Post-renal Obstruction, e.g. stones, cancer
Table 1. Common causes of acute kidney injury.
018_033_CLI_JUNE_2016.indd 18 15/06/16 16:02

common biochemical panels in blood tests ordered in both hospital and com-munity patients. Th is means it is easy to monitor trends and to compare to his-torical data for the patient as required for the diagnosis of AKI. But it may be slow to respond to changes in renal function, and this may be important in the early detection of AKI. Creatinine concentration in the blood and urine is also infl uenced by other factors such as age, muscle mass, diet, tubular secre-tion, hydration status and is subject to analytical interferences. Two methods for measuring creatinine are in common use in biochemistry laboratories, the traditional Jaff e methodology and enzy-matic methods. Enzymatic methodol-ogy for measurement of serum creati-nine has been recommended by NICE in the AKI guidelines [2]. As noted above, it has been documented that changes in creatinine only occur when 50% of kid-ney function has been lost. Th erefore, other markers of AKI such as neutrophil gelatinase- associated lipocalin (NGAL) and tissue inhibitors of metalloprotein-ases- 2 (TIMP-2) have been investigated as alternatives to serum creatinine.
NGAL is a 25-kDa protein in the lipocalin family and is associated with ischaemic kidney injury and may be measured in urine. NGAL is thought to increase in the early stages of AKI as it acts to limit and repair damage caused by the insult and is mediated by NF-κB which is rapidly increased aft er injury and promotes cell survival and prolif-eration. It has been found to be detect-able in urine in the very early stages of AKI [9].
Tissue inhibitor of metallinoproteinases-2 (TIMP-2) and insulin-like growth factor binding protein 7 (IGFBP7) have been explored as biomarkers of AKI in critically ill patients in an intensive care setting in the Sapphire study [10]. Both of these pro-teins are inducers of the G1 cell cycle arrest thought to be critical in the development of AKI.
Th e management of AKI, especially in the community is oft en focused on removal of the risk factors and inducers of AKI. Gen-eral Practice can play a role in reduction of the risk of developing AKI such as regular review of those patients on medication associated with increased risk of develop-ment of AKI and review of patients with chronic kidney disease who are inherently at increased risk of AKI [5].
NHS England AKI detection algorithmIt was recognized that detecting AKI based on identifying changes in serum creatinine as according to KDIGO guidelines was eas-ily automatable using laboratory informa-tion management systems (LIMS). In 2014, NHS England published a patient safety alert to all NHS Trusts with pathology ser-vices, to standardize the reporting of AKI [11]. Th is recognized that some Trusts had already implemented an AKI alert system based on changes in creatinine and the KDIGO guidelines, but aimed to standard-ize the reporting and ensure reporting was done in real-time.
Th e alert system algorithm is based on comparison of a patient’s creatinine con-centration with that of a baseline creati-nine – either a result within the last 48 hours, 7 days or 12 months based on the KDIGO criteria [12]. Th e patient safety alert algorithm is mandatory for all pathol-ogy laboratories in the UK and was devel-oped with the major LIMS providers, thus enabling standardization and a model that is compatible with all systems. Th e mode of alerting users is not described and thus subject to diff ering practices within the UK NHS Trusts. Th is allows for laboratory interaction with users to determine the required practice for each individual Trust. For example the alerts will be reported to the electronic patient record, but whether these results are to be telephoned, emailed, etc., to users is to be individually deter-mined. Implementation into primary care is expected to occur by April 2016 [12].
ConclusionIn summary, AKI is an important issue in healthcare due to the high level of mor-bidity and mortality associated with it. It is also associated with increased demand on healthcare resources throughout the system including primary and secondary care. Early detection is vital in order to reduce the morbidity and mortality associ-ated with the condition. Every part of the healthcare system, therefore, has a part to play, including GP identifi cation of those patients at increased risk of development of AKI and reduction of that risk, labora-tory detection of AKI from serum creati-nine measurements or potentially other biomarkers, and to the clinician acting on those alerts and initiating treatment early to preserve renal function.
References1. Stewart J, Findlay G, Smith N, Kelly K, Mason
M. Adding insult to injury. A review of the care
of patients who died in hospital with a primary diagnosis of acute kidney injury (acute renal fail-ure). National Confi dential Enquiry into Patient Outcome and Death 2009. (http://www.ncepod.org.uk/2009report1/Downloads/AKI_summary.pdf)
2. NICE guidelines CG169. Acute kidney injury: prevention, detection and management. NICE 2013. (https://www.nice.org.uk/guidance/cg169)
3. Wang HE, Muntner P, Chertow GM, Warnock GE. Acute kidney injury and mortality in hospi-talized patients. Am J Nephrol. 2012; 35: 349–355.
4. Kaufman J, Dhakal M, Patel B, Hamburger R. Community-acquired acute renal failure. Am J Kidney Dis. 1991; 17(2): 191–198.
5. Blakeman T, Harding S, O’Donoghue D. Acute kidney injury in the community: why primary care has an important role. Br J Gen Pract. 2013; 63(609): 173–174.
6. Chawler LS, Andur R L, Amodeo RL, Kimmel PL, Palant C. Th e severity of acute kidney injury predicts progression to chronic kidney disease. Kidney Int. 2011; 79 (12): 1361–1369.
7. Lopes JA, Jorge S. Th e RIFLE and AKIN classi-fi cations for acute kidney injury: a critical and comprehensive review. Clin Kidney J. 2013; 6: 8–14.
8. Kidney disease: improving global outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical practice guideline for acute kid-ney injury. Kidney Inter. Suppl. 2012; 2: 1–138.
9. Devarajan P. Neutrophil gelatinase associated lipocalin: a promising biomarker for human acute kidney injury. Biomark Med. 2010; 4(2): 265–280.
10. Pilarczyk K, Edayadiyil-Dudasova M, Wendt D, Demircioglu E, Benedik J, Dohle DS, Jakob H, Duss F. Urinary [TIMP-2]*[IGFBP7] for early prediction of acute kidney injury aft er coronary artery bypass surgery. Ann intensive care 2015; 5: 50
11. Standardising the early identifi cation of acute kidney injury. NHS England 2014. (https://www.renalreg.org/wp-content/uploads/2014/08/Patient-Safety-Alert-AKI-algorithm-2014_06_04.pdf)
12. -Acute kidney injury warning algorithm best practice guidance. NHS England and UK Renal Registry 2014. (https://www.thinkkidneys.nhs.uk/aki/wp-content/uploads/sites/2/2014/12/AKI-Warning-Algorithm-Best-PracticeGuid-ance-10.03.16.pdf)
The authorCharlotte Fairclough, MScDepartment of Clinical Chemistry and Met-abolic Medicine, Liverpool Clinical Labora-tories, Royal Liverpool and Broadgreen Uni-versity Hospitals NHS Trust, Liverpool, UK
*Corresponding authorE-mail: [email protected]
– June 201619
018_033_CLI_JUNE_2016.indd 19 15/06/16 16:02

IntroductionCytokines and chemokines are impor-tant immunoregulatory molecules pro-duced by many cells such as neutrophils, monocytes, macrophages and T-cells that can serve as biomarkers of inflam-matory diseases to predict and track disease pathogenesis [1–4]. Various cytokines and chemokines like inter-leukins (ILs) and tumour necrosis fac-tors (TNFs) can serve as valuable clini-cal biomarkers of acute kidney injury (AKI), a rapidly acquired disorder asso-ciated with high morbidity and mortal-ity that is commonly seen in hospitalized patients. As elevated levels of cytokines may reveal the activation of signalling pathways leading to inflammation and disease progression, methods enabling prompt and sensitive detection and quantification of multiple cytokines/chemokines simultaneously in a clinical setting are highly sought. Although con-ventional techniques such as enzyme-linked immunosorbent assays (ELISAs) are widely available and reliable, their applications may not be suitable for the rapid, multiplexed detection of weakly expressed cytokines due to their detec-tion limits (DLs) of typically greater than tens of pg/mL, long assay times of several hours, and extensive serial workflows for detecting multiple protein analytes.
As the typical levels of important AKI-implicated cytokines and chemokines in healthy populations can often be well below the customary DLs of standard cytokine assays, which are generally around tens of pg/mL, there is great clin-ical interest in reducing the lower limits
of detection down to the fg/mL range. In particular, the increasing need for early diagnosis and treatment in AKI and other cytokine-implicated diseases has driven the development of innovative detection schemes capable of reaching even lower DLs than have convention-ally been offered. In this context, we have shown that zinc oxide nanorods (ZnO NRs) permit enhanced detection of fluo-rescence signals emitted by fluorophore-coupled biomolecules in the forms of custom-prepared oligonucleotide constructs and highly purified single-composition proteins in simple media [5–8]. In our most recent work, which is highlighted here, we have developed and validated an ultrasensitive fluorescence-based bioassay using micropatterned ZnO NRs as a novel optical platform for the multiplexed detection and quan-tification of two urinary biomarkers of AKI, tumour necrosis factor-α (TNF-α) and interleukin-8 (IL-8), in samples of patients at risk for and diagnosed with AKI [9].
In addition to the biomedical relevance of TNF-α and IL-8 in the pathophysi-ology of AKI, the biomarkers are ideal model cytokines and chemokines for this study due to the differences in their typical concentration levels found in human urine. The baseline expression of IL-8 in healthy populations gener-ally ranges from tens of pg/mL to ng/mL and can be ascertained using con-ventional approaches, whereas TNF-α levels are typically below the DLs of tra-ditional cytokine detection platforms. Accordingly, we performed ELISA- and ZnO NR-based assays on the same set of
Zinc oxide nanorod-based acute kidney injury biomarker detection technology and potential clinical implicationsWe developed an ultrasensitive bioassay using micropatterned zinc oxide nanorods (ZnO NRs) for the multiplexed detection and quantifi cation of trace levels of cytokines implicated in acute kidney injury (AKI) directly from patient samples. The remarkable limits of detection of the novel ZnO NR-based assay are compared directly with conventional methods.
by Manpreet Singh, Anginelle Alabanza, Lorelis E. Gonzalez, Weiwei Wang, Prof. W. Brian Reeves, and Prof. Jong-in Hahm
– June 2016 Kidney disease20
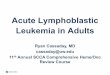
Figure 1. (A) Representative emission data collected after performing the sandwich assay on the ZnO NR platform for Alexa 488-labelled TNF- and Alexa 546-labelled IL-8. (B) The scanning electron microscope (SEM) panels display the morphology and dimensions of the square patches of densely packed, vertically oriented ZnO NRs serving as the detection platform. The inset, F, shows the fl uorescence panel of the ZnO NR array probed with ex, 450–490 nm. ZnO NRs exhibit no background fl uorescence emission upon excitation at the wavelength ranges used to detect these and other common fl uorophores. (C) Several examples of the fl uorescence readings obtained for both biomarkers from selected patient samples. (D) The bar graphs display the inter-assay (*) and intra-assay (**) variability for the same patients run on three different ZnO NR arrays and fi ve times on the same platform, respectively. Figure fi rst published in Singh M, et al. Nanoscale 2016; 8: 4613–4622 [9]. Reproduced with permission; copyrights (2016) Royal Society of Chemistry Publishing.
018_033_CLI_JUNE_2016.indd 20 15/06/16 16:02

Good News: You’re automating your lab.Best News: We’ve done it more than 1400 times.
Visit us at AACC booth #2101
www.cli-online.com & search 27181
018_033_CLI_JUNE_2016.indd 21 15/06/16 16:02

patient samples to first examine whether the highly expressed IL-8 levels agree between both detection methods and further demonstrated the detection capability of the ZnO NRs to reveal the ultralow protein levels of TNF-α that cannot otherwise be ascertained via ELISA.
Results and discussionOverall approach of ZnO NRs-based fl uorescence assayUsing a micropatterned array of densely grown, vertically oriented ZnO NRs synthesized using a facile, low-cost, chemical vapour-phase method, we employed a sandwich assay scheme for the multiplexed detection of both AKI-relevant biomarkers. The sequen-tial assay steps included incubation of the ZnO NR platform with primary TNF-α and IL-8 antibodies, bovine serum albumin for surface blocking,
standards for both proteins for gen-erating calibration curves or patient urine samples for determining bio-marker levels in subject individuals, and fluorophore-conjugated secondary antibodies. In Figure 1(A), representa-tive emission data from the multi-plexed assay are qualitatively presented for Alexa 488-labelled TNF-α (left) and Alexa 546-labelled IL-8 (right). As a direct comparison, the panels in Figure 1(B) display scanning electron micro-scope (SEM) images of the ZnO NR array platform to show the morphol-ogy and dimensions of the individual square patches of ZnO NRs. The highly crystalline ZnO NRs do not exhibit any background fluorescence, as evi-denced in the inset (F) of image 1(B), and, hence, all optical signals detected for protein quantification are derived only from the surface-adsorbed fluoro-phore-tagged biomolecules.
Reproducibility and calibrationIn Figure 1(C), exemplar fluores-cence intensity plots show the different amounts of TNF-α and IL-8 simulta-neously detected from selected patient urine samples as obtained by averag-ing the optical signal from about 550 NR square patches on different areas of the same ZnO NR detection platform. The reproducibility of the fluorescence signal on the ZnO NRs-based platform is shown in Figure 1(D) in which the same patient sample was assayed five times on the same ZnO NR platform for intra-assay variability (**) as well as on three different ZnO NR plates for inter-assay variations (*) that may arise from assay or array-to-array differences. This scheme was conducted for two patient samples, and the coefficients of variation for the intra-assay (16.5% for TNF-α and 2.5% for IL-8) and inter-assay (12% for TNF-α and 2.8% for IL-8) results were found to be below the generally accepted value of 10–20%.
In order to quantitatively compare the levels of TNF-α and IL-8 obtained via the ELISA- and ZnO NRs-based assays, calibration curves were generated using standard solutions of each cytokine. The DLs of the ELISA-based method, defined as 2 standard deviations above the mean of 20 zero concentration replicates, were determined as 5.5 and 7.5 pg/mL for TNF-α and IL-8, respectively. On the other hand, the DLs of the ZnO NR plat-form, assessed using the upper boundary of blank samples with a 95% accuracy goal, were found to be 4.2 and 5.5 fg/mL for TNF-α and IL-8, respectively. The unparalleled sensitivity down to the sev-eral fg/mL range enabled by the ZnO NR platform can reveal the levels of weakly expressed, disease-implicated cytokines such as TNF-α to promote early clinical diagnostics.
IL-8 testing and statistical analysisFollowing calibration, the same patient samples were assayed on both the ELISA and ZnO NR platforms for quantitative comparison between both assays. When comparing the highly expressed IL-8 levels in the urine of 38 patients that ranged between several tens of pg/mL to a few ng/mL, the ZnO NRs-based assay had strong statistical agreement with the ELISA-based results allowing for direct validation of the novel bioassay. In Fig-ure 2(A), a correlative plot displays the IL-8 readings from the same patients determined by the ELISA and ZnO NR
– June 2016 Kidney disease22
Figure 2. (A) The correlative comparison of IL-8 readings evaluated by the ELISA (x-axis) and ZnO NR (y-axis) assays from the same set of patients is plotted in red and fi t linearly in the dashed red line. The ELISA- and ZnO NR-based results fall on or near the black line of y=x, indicating good agreement between the patient IL-8 values established by the two assay techniques. (B) The histogram distributions show patient counts versus the differences in the evaluated IL-8 concentrations between the two assays for the (ZnO NR–ELISA) range of less than 40 pg/mL. The majority of the differences between the patients’ IL-8 readings fell within the range of ±2.5 pg/mL. (C) The IL-8 concentrations in pg/mL determined from the ZnO NR and ELISA assays are compared by plotting the differences between the two techniques, (ZnO NRs-ELISA), on the y-axis and the means of the two techniques, (ZnO NRs + ELISA)/2, on the x-axis. The evaluated data lie close to the black line of y = 0, whose trace corresponds to equivalent readings of IL-8 concentrations in the two assays from the same patients. (D) The scatter plot shown in (C) is rescaled to clearly present the lower range data. Figure fi rst published in Singh M, et al. Nanoscale 2016; 8: 4613–4622 [9]. Reproduced with permission; copyrights (2016) Royal Society of Chemistry Publishing.
018_033_CLI_JUNE_2016.indd 22 15/06/16 16:02

www.cli-online.com & search 27135
018_033_CLI_JUNE_2016.indd 23 15/06/16 16:02

assays on the x and y axes, respectively. The linear fit of the data points, shown in the dashed red line, lies very close to the superimposed line of y = x, shown in black, indicating excellent agreement between the two assay methods. In Fig-ure 2(B), a histogram distribution chart reporting the differences in IL-8 read-ings between the two methods shows the majority of IL-8 readings from both assays fell within the range of ±2.5 pg/mL of each other. The IL-8 levels were
further evaluated using the Bland-Alt-man analysis in Figure 2(C & D) in which the differences between the ELISA and ZnO NR readings for each patient were plotted against the mean concentration values. As shown, the data analysed over a large range of concentrations centred near the black lines, which represent the case of equivalent IL-8 readings obtained from the two different assays. The results of these comparative analy-ses validate the ZnO NR platform as a
reliable technique to accurately quan-tify urinary biomarker proteins directly from patient samples.
TNF- testingTo substantiate the applicability of the ZnO NR platforms in ultrasensitive cytokine detection using the weakly expressed biomarker of TNF-α, the pro-tein levels for 46 patients were deter-mined using both assay platforms. As seen in Figure 3(A), many of the patient samples exhibited values too close or below the DL of the ELISA assay (5.5 pg/mL) and are marked accordingly as grey blocks in the ELISA row. By contrast, the TNF-α values of all the patients were successfully quantified on the ZnO NR platform, well below several tens of pg/mL and into the low fg/mLrange. For the ZnO NR row in Figure 3(A), those samples that could not be measured via ELISA are shown with a magnifier sign, and their TNF-α concentrations, as determined by the ZnO NRs-based assay, are then shown in Figure 3(B & C) on two different scales for clar-ity. As demonstrated, the optical signal enhancement provided by the ZnO NR array platform enables the ultrasensi-tive detection of trace levels of proteins directly from patient samples.
Advantages of the ZnO NR-based approach and future outlookWithin the realm of biodetection, the ZnO NR-based approach can provide many direct advantages including fac-ile platform fabrication, desirable opti-cal properties, biocompatibility, and promising multiplexed/high-throughput integration capacities. The ZnO NR arrays are easily fabricated using a gas-phase method through well-established synthesis procedures and can be used directly after growth without any post-synthetic modifications. Further, the highly crystalline NRs exhibit many desirable optical properties including no intrinsic fluorescence (i.e. absence of autofluorescence) as well as enhance-ment of the optical intensity and photo-stability of nearby signal emitters. Since the ZnO NRs do not display any pho-toluminescence in the visible and near-infrared range, they do not interfere with the spectroscopic profiles of fluo-rophores commonly used in biology and biomedical detection. At the same time, the reduced dimensions and high shape anisotropy of the ZnO NRs enable opti-cal enhancement and prolonged stability
– June 2016 Kidney disease24
Figure 3. (A) The comparative TNF- concentrations in which the grey regions in the ELISA row correspond to undetermined TNF- levels below the ELISA DL of 5.5 pg/mL. All 46 patients were successfully quantifi ed on the ZnO NR platform, and the low-level concentrations with magnifi er signs in the ZnO NRs row are shown separately in (B) and (C) for clarity. (B & C) The zoomed-in plots show the missing TNF- levels that were revealed by the ZnO NR-based assay. The upper limits of the vertical ranges in (B) and (C) are adjusted to 2 pg/mL and 350 fg/mL, respectively, in order to show the variations in the TNF- concentrations between patients more clearly. The truncated bars indicate that those TNF- concentrations exceed the upper limit of the 3D graph. Figure fi rst published in Singh M, et al. Nanoscale 2016; 8: 4613–4622 [9]. Reproduced with permission; copyrights (2016) Royal Society of Chemistry Publishing.
018_033_CLI_JUNE_2016.indd 24 15/06/16 16:02

OUR IN VITRO DIAGNOSTICS IDENTITY
CLINICAL CHEMISTRY SEROLOGY
COAGULATION SPECIFIC PROTEINS
IMMUNOASSAY AND AUTOMATION
AUTOIMMUNITY
Sclavo KOS 1 & KOS 2 Semi-automated Coagulation System. Compact, 1 or 2
channels, high reliability. Fully
optical measurement. Complete
panel of Sclavo reagents.
SkyLAB™ 752 Fully automated ELISA and IFA platform. Able
to process EIA microplates and
IFA slides simultaneously.
Designed to be easily integrated
with a preanalytical system.
Sclavo Palio™ 200N
Fully automated Clinical Chemistry and Specific Proteins System. Compact, benchtop,
random access, throughput up
to 360 tests/hour.
[email protected] [email protected] Via R. Merendi 22 - 20010 Cornaredo MI ITALY
VISIT US AT BOOTH # 4177
www.cli-online.com & search 27226
018_033_CLI_JUNE_2016.indd 25 15/06/16 16:02

of the signal from fluorophore-tagged biomolecules adsorbed on their surface allowing for the ultrasensitive detection of trace levels of bioconstituents.
In addition to the demonstrated sensitivity permitted by the ZnO NR-based platform, the cytokine bioassay also has the direct advan-tages of rapid analysis, minimal volume requirements, and reus-ability. Th e multiplexed detection was achieved with 90 min of total assay time and only 60 μL of total bioreagent/sample volume using commonly employed fl uorescence microscopy instrumentation. Further, the highly biocompatible ZnO NRs platform was found to withstand at least 25 repeated assays in complex biological and chemical reaction environments that include urine samples.
As modern automation strategies in high-throughput screen-ing have seen great advancements in the sophistication of robotic sample delivery strategies and the detection of many analytes simultaneously via multichannel optical sensors, the ZnO NR-based platform may be able to provide much-sought detection sensitivity when integrated into these breakthrough technologies. In the microarray, each square patch of densely grown ZnO NRs with a typical dimension of 3~50 μm in side length can be configured to serve as a discrete detection ele-ment for different patient samples when coupled with appro-priate sample delivery and multiplexed optical sensing/readout platforms. The demonstrated detection capabilities combined with this integration potential suggests that the ZnO NR-based approach serves as more than just an alternative or tandem detection platform to existing methods, but rather provides an advanced approach which allows the much needed, ultrasensi-tive detection of biomarker proteins in samples that exhibit
concentration levels much lower than those which standard techniques can ascertain.
ConclusionWe successfully demonstrated a ZnO NRs-based fluorescence bioassay for the rapid, ultrasensitive, quantitative and multi-plexed detection of AKI-related biomarkers in patient urine samples. We first statistically validated the ZnO NR-based approach against a conventional ELISA-based method by com-paring the measurements of highly expressed levels of IL-8 that were above the DLs of ELISA. We further revealed the full detection capabilities of the ZnO NRs platform by quantify-ing ultratrace amounts of a weakly expressed cytokine, TNF-α, whose levels in urine are often below the DLs of conventional cytokine assays. The unparalleled detection sensitivity and other discussed advantages of the ZnO NR-based bioassay can be readily extended to advance other optical-sensing applica-tions in biological research and clinical diagnostics.
AcknowledgementThis article is a summary of the work first presented in Singh M, Alabanza A, Gonzalez LE, Wang W, Reeves WB, Hahm J. Ultratrace level determination and quantitative analysis of kid-ney injury biomarkers in patient samples attained by zinc oxide nanorods. Nanoscale 2016; 8: 4613–4622 [9].
References1. Feldmann MJ. Many cytokines are very useful therapeutic targets in disease.
Clin Invest. 2008; 118: 3533–3536.2. Fichorova RN, Richardson-Harman N, Alfano M, et al. Biological and tech-
nical variables aff ecting immunoassay recovery of cytokines from human serum and simulated vaginal fl uid: a multicenter study. Anal Chem. 2008; 80: 4741–4751.
3. Borish LC, Steinke JWJ. Cytokines and chemokines. Allergy Clin Immunol. 2003; 111: S460–S475.
4. Nathan C, Sporn M. Cytokines in context. J Cell Biol. 1991; 113: 981–986.5. Adalsteinsson V, Parajuli O, Kepics S, et al. Ultrasensitive detection of
cytokines enabled by nanoscale ZnO arrays. Anal Chem. 2008; 80: 6594–6601.6. Dorfman A, Kumar N, Hahm J. Nanoscale ZnO-enhanced fl uorescence detec-
tion of protein interactions. Adv. Mater. 2006; 18: 2685–2690.7. Singh M, Song S, Hahm J. Unique temporal and spatial biomolecular emission
profi le on individual zinc oxide nanorods. Nanoscale 2014; 6: 308–315.8. Singh M, Jiang R, Coia H, et al. Insight into factors aff ecting the presence,
degree, and temporal stability of fl uorescence intensifi cation on ZnO nanorod ends. Nanoscale 2015; 7: 1424–1436.
9. Singh M, Alabanza A, Gonzalez LE, et al. Ultratrace level determination and quantitative analysis of kidney injury biomarkers in patient samples attained by zinc oxide nanorods. Nanoscale 2016; 8: 4613–4622.
The authorsManpreet Singh1 BS, Anginelle Alabanza1 BS, Lorelis E. Gonza-lez1 BS, Weiwei Wang2 BS, W. Brian Reeves3 MD, and Jong-in Hahm*1 PhD1Department of Chemistry, Georgetown University, Washington, DC 20057, USA2Division of Nephrology, The Penn State College of Medicine, Milton S. Hershey Medical Center, Hershey, Pennsylvania 17033, USA3Department of Medicine, University of Texas Health Sciences Center at San Antonio, San Antonio, TX 78229, USA
*Corresponding authorE-mail: [email protected]
– June 2016 Kidney disease26
DiaSys. Liquid-Stable Solutions.www.hba1cnet.com
The Future of Diabetes Management
· Enzymatic HbA1c assay with excellent precision
· Liquid-stable, ready-to-use 2-component reagent
· Superior on-board and calibration stability
· Results equivalent to HPLC
· No interferences by Hb variants or other blood components
· Standardized against IFCC reference method, traceable according to the DCCT/NGSP network
www.cli-online.com & search 27209
018_033_CLI_JUNE_2016.indd 26 15/06/16 16:02

www.cli-online.com & search 00000
www.cli-online.com & search 27242
018_033_CLI_JUNE_2016.indd 27 15/06/16 16:02

Membranous nephropathyMembranous nephropathy is an organ-specifi c autoimmune disease and a major cause of nephrotic syndrome in adults. Th e disease is characterized by formation of immune complexes in the glomerular basement membrane, resulting in comple-ment-mediated proteinuria and progres-sive loss of kidney function. 70-80% of cases are of the primary or idiopathic form. Th e remaining 20-30% of cases are second-ary, arising from underlying causes such as malignancy, infection, drug intoxication or another autoimmune disease such as systemic lupus erythematosus. Diagnostic diff erentiation of primary and secondary
forms is crucial due to diff erent treatment regimes. Primary MN is treated with immu-nosuppressants, while therapy for the sec-ondary form is targeted at the underlying disease. Treatment decisions for primary MN are further complicated by the extreme variability in clinical outcome. Patients can experience spontaneous remission or per-sistent proteinuria without renal failure, or progress to end-stage renal disease.
Anti-PLA2R antibodiesAutoantibodies against PLA2R are a highly specifi c marker for primary MN. Th ey occur in around 70% to 75% of patients at time of diagnosis, while they are only very
rarely found in patients with secondary MN or in healthy individuals. Th eir titer, moreo-ver refl ects the disease activity and severity. Th e target antigen, which was identifi ed in 2009, is a type 1 transmembrane glycopro-tein which is expressed on the surface of podocytes.
Following the discovery of the target anti-gen, standardized assays for the determina-tion of anti-PLA2R antibodies in a routine setting were rapidly developed. Th e recom-binant-cell indirect immunofl uorescence test (RC-IIFT, Figure 1) utilizes transfected cells expressing full-length PLA2R on the cell surface as the antigenic substrate. Th e RC-IIFT is a reliable screening test for qual-itative detection of anti-PLA2R autoan-tibodies. Using this assay, anti-PLA2R antibodies were detected with maximum specifi city (100%) and a sensitivity of 77% in a cohort of 275 biopsy-proven primary MN patients. In the Anti-PLA2R ELISA, purifi ed recombinant receptor is used as a solid-phase coating of microtitre plates. Th is assay provides accurate quantifi cation of autoantibody concentrations and is par-ticularly useful for disease monitoring. In a large cohort of clinically well characterized patients, the assay revealed very high sensi-tivity with respect to the RC-IIFT (96.5%) at a set specifi city of 99.9%. Th e quantitative results of ELISA and RC-IIFT show a good correlation.
Anti-PLA2R is now an established param-eter for diagnosing primary MN, diff erenti-ating it from secondary MN, assessing the disease status and monitoring responses to therapy [1, 2]. Th e antibody titre refl ects the immunological as opposed to the clinical
Novel nephrological markers: anti-PLA2R, anti-THSD7A and uromodulinAutoantibody diagnostics have in recent years transformed the diagnosis of the rare kidney disease primary membranous nephropathy (MN). The identifi cation of the target antigens M-type phospholipase A2 receptor (PLA2R) and thrombospondin type 1-domain-containing 7A (THSD7A) paved the way for the development of specifi c immunological assays to detect the corresponding antibodies. Determination of both anti-PLA2R and anti-THSD7A antibodies allows serological diagnosis in 75% to 80% of cases of primary MN. Anti-PLA2R tests are, moreover, an indispensable tool for patient monitoring. A further new biomarker, uromodulin, acts as an indicator of impaired renal function, especially in chronic kidney disease, supplementing established markers such as creatine and cystatin C.
– June 2016 Kidney disease28
Figure 2. Relationship between clinical disease and immunological activity.
Figure 1. Positive reaction in Anti-PLA2R RC-IIFT.
018_033_CLI_JUNE_2016.indd 28 15/06/16 16:02

Visit us
at
AACC
Booth
#2927
#FutureDiagnosticsrandox.com/future-diagnostics
shaping the future ofclinical diagnostics
Providing you withtrue third party Quality Controls,
biochemistry Reagents &the RX seriesof chemistry analyzers.
www.cli-online.com & search 27196
018_033_CLI_JUNE_2016.indd 29 15/06/16 16:02

– June 2016 Kidney disease30
disease activity, and a change in the anti-body titer, either spontaneous or treat-ment-induced, precedes the corresponding change in proteinuria by weeks or months (Figure 2) [3]. Thus, anti-PLA2R measure-ments provide a much earlier indicator than proteinuria of patient improvement or deterioration, helping to guide therapy decisions. Complete remission is always preceded by complete antibody depletion.
Anti-PLA2R titres also allow predictions regarding clinical outcome. High antibody titres are associated with a lower chance of spontaneous remission, a longer therapy period to achieve remission, and progres-sion to kidney failure (Table 1) [4]. A low anti-PLA2R antibody titre at baseline, on the other hand, is the most pronounced independent predictor of spontaneous remission [5]. Patients with low anti-PLA2R titres are less likely to require immunosup-pressive therapy than those with high titres. Overall, anti-PLA2R assessment is recom-mended every two months before start-ing immunosuppressive therapy to avoid unnecessary treatment in patients entering remission, and every month for the first six months of immunosuppression [2].
Anti-PLA2R analysis is also useful for predicting primary MN recurrence after kidney transplantation. Up to 40% of patients relapse after transplantation, and anti-PLA2R positivity is associated with a higher risk of recurrence. In a recent study, pre-transplant anti-PLA2R determina-tion demonstrated a positive predictive value of 100% and a negative predictive value of 91% for a diagnosis of recurrent MN [6]. Further, if anti-PLA2R antibod-ies are persistently found during the first six months after transplantation, the risk
of relapse is particularly high. Antibody determination may therefore be helpful for assessing the necessary and intensity of immunosuppressive therapy following transplantation.
Anti-THSD7A antibodiesAutoantibodies against THSD7A have been recently identified as a further marker in primary MN [7]. Similarly to PLA2R, THSD7A is an N-glycosylated, high-molecular-mass protein expressed on the podocyte membrane. Antibodies against THSD7A occur in around 2.5% to 5% of patients with idiopathic MN. Significantly, they are found predominantly in patients who are negative for anti-PLA2R, suggest-ing a distinct disease subgroup. Neverthe-less, some rare cases with dual positivity for anti-PLA2R and anti-THSD7A have recently been described [8]. No reactivity to THSD7A has been observed in healthy controls or patients with other proteinuric or renal autoimmune diseases.
Anti-THSD7A serves as an additional, complementary marker in primary MN, reducing the diagnostic gap of anti-PLA2R analysis. Moreover, like anti-PLA2R, anti-THSD7A antibody levels also appear to be associated with disease activity. Further studies are currently underway to investi-gate this link.
Circulating anti-THSD7A antibodies can be determined by RC-IIFT using trans-fected cells expressing recombinant anti-gen (Figure 3). Combined testing for anti-PLA2R and anti-THSD7A provides a comprehensive screening for primary MN.
UromodulinUromodulin, also known as
Tamm-Horsfall protein, is a glycoprotein which is synthesized exclusively in the kid-neys in the ascending limb of the loop of Henle, and subsequently secreted. When renal function is impaired, the uromodu-lin concentration in the serum or plasma decreases [9]. The concentration exhibits a linear correlation to the estimated glo-merular filtration rate (eGFR) (Figure 4). Thus, uromodulin shows inverse kinetics to conventional markers like creatine and cystatin C, which increase with declining kidney function. Moreover, uromodu-lin concentrations change already in the early stages of chronic kidney disease, when there are few symptoms. Thus, uro-modulin measurements enable detection of renal insufficiency in the creatine-blind area in the initial stages of kidney disease. Measurement of uromodulin is also suit-able for monitoring kidney vitality during therapy and as a predictive marker after kidney transplantation.
Uromodulin can be measured in the serum or plasma by ELISA based on microplates coated with anti-uromodu-lin antibodies. The patient uromodulin concentrations are established using a simple cut-off-based interpretation, with a normal value being above 100 ng/ml. External factors such as body weight, nutrition or muscle mass do not need to be factored into the results by additional calculations, as is the case with classic markers. Further, since the uromodu-lin concentration is measured in serum or plasma, the laborious and error-prone collection of 24-hour urine is not required. This makes it a fast, easy and sensitive supplementary test for the early identification of nephropathies and loss in renal function.
Outcome Low aPLA2R titre
Moderate aPLA2R titre
High aPLA2R titre
Partial remission 42% 31% 41%
Complete remission 27% 35% 30%
Kidney failure 4% 12% 19%
Persistent proteinuria 27% 23% 11%
Spontaneous remission 38% 31% 4%
Immunosuppressive therapy needed 48% 54% 88%
Median after therapy for remission
5 (3-7)months
7 (5-32)months
10 (6-219)months
Table 1. Outcome in relation to anti-PLA2R titre.
Figure 3. Positive reaction in Anti-THSD7A RC-IIFT.

– June 201631
PerspectivesAnti-PLA2R and anti-THSD7A assays are now a mainstay for the diagnosis of primary MN. Due to the high specifi city, anti-PLA2R detection may even enable biopsy to be post-poned or omitted in elderly patients, persons with poor clinical condition, or patients with life-threatening complications of nephrotic
syndrome such as lung emboli. Neverthe-less, a proportion of primary MN patients (around 20%) shows negative results for both anti-PLA2R and anti-THSD7A anti-bodies. Th is may refl ect the disease activity at time of blood sampling (e.g. spontaneous remission) or a misclassifi cation of patients who actually have secondary MN. It is also
supposed that some primary MN patients react to other, as yet unidentifi ed antigens. Anti-PLA2R measurements are also play-ing an increasingly central role in therapy decisions and prognosis, as the relationship between the anti-PLA2R titre and clinical outcome becomes better understood. Cur-rent research is directed at further elucidat-ing the complex pathogenesis of primary MN and applying this knowledge to improve therapeutic care.
References1. Mastroianni-Kirsztajn et al. Frontiers in Immunol. 2015: 6:2212. Ronco et al. Lancet 2016: 385 (9981): 1983-923. Beck et al. Kidney Int. 2010: 77: 765-704. Hofstra et al. J. Am. Soc. Nephrol. 2012: 23(10): 1735-435. Timmermans et al. Am. J. Nephrol. 2015: 42(1): 70-76. Gupta et al. Clin. Transplant. 2016: 30: 461-97. Tomas et al. N. Engl. J. Med. 2014: 371(24): 2277-878. Larsen et al. Modern Pathol. 2016: 29: 421-69. Steubl et al. Medicine 2016: 95(10): e3011
The authorJacqueline Gosink, PhDEUROIMMUN AGSeekamp 31,23560 Luebeck, GermanyE-mail:[email protected]
Figure 4. Relationship of uromodulin concentration to eGFR.
www.cli-online.com & search 27100
018_033_CLI_JUNE_2016.indd 31 15/06/16 16:02

Th e hospital’s Clinical Microbiology Depart-ment has a signifi cant serology workload, pro-cessing more than 250 serology samples every day. Th is includes viral load testing for targets such as cytomegalovirus (CMV), hepatitis B virus (HBV), hepatitis C virus (HCV) and human immunodefi ciency virus type 1 (HIV-1).
Th e serology laboratory faces a number of challenges that need to be addressed in order to meet future workload and service user requirements. Not least, the available space in the laboratory is limited due to the instrumentation that is required. Our exist-ing viral load method requires separate sam-ple preparation and amplifi cation/detection platforms, and involves considerable manual intervention. Furthermore, as samples are processed in batches, this requires additional space for pre-analytical sample storage.
On reviewing our processes, we identifi ed the need for increased automation within the laboratory, to reduce the number of manual steps and improve workfl ow effi ciencies, and improve laboratory response times.
Evaluating new technologyIn 2014-2015, we had the opportunity to evaluate a new, fully automated, random
access platform for viral load analyses. Th e DxN VERIS Molecular Diagnostics System (Beckman Coulter) consolidates DNA extraction, nucleic acid amplifi ca-tion, quantifi cation and detection onto a single automated instrument for a num-ber of molecular targets. We evaluated the performance of the VERIS assays for CMV, HBV, HCV and HIV-1 using standard and control samples, as well as clinical sam-ples, comparing them to our existing viral load method (COBAS Ampliprep®/COBAS TaqMan® assays, Roche).
All four assays were found to have compa-rable performance to our existing method, demonstrating excellent sensitivity, speci-fi city and precision [1,2]. Th e correla-tion between both methods for HBV viral load quantifi cation, for example, is shown in fi gure 1. A precision analysis for the VERIS HBV assay, which was calculated for fi ve levels tested in duplicate over 20 days, gave a ‘within run’ standard devia-tion of ≤0.09 Log IU/mL and a ‘between run’ standard deviation of ≤0.09 Log IU/mL (table 1). Moreover, repeated analysis of negative samples alongside high positive samples at diff erent rack positions showed no cross contamination, giving confi dence
in results. Th is random access technology provided the fi rst result in just 75 minutes for HBV and CMV DNA, and in 90 min-utes for HCV and HIV-1 RNA, with subse-quent results every 2.5 minutes.
Our experiences in evaluating the DxN VERIS system led us to appreciate its potential as an enabler for an improved molecular biology clinical service. Th e increased automation and random access off er workfl ow improvements that simplify laboratory tasks and reduce the potential for human error. Furthermore, its overall performance and ease of use facilitated the smooth introduction of the technology in our laboratory.
Rapid results inform prompt treatment decisionsEarly in 2016, we began to use the DxN VERIS System routinely for HBV and HCV viral load quantifi cations. Our annual vol-ume of HBV and HCV samples is around 7,000 and, as a clinical laboratory working closely alongside medical staff , our viral load results support timely clinical deci-sion making and subsequent patient man-agement. In this respect the DxN VERIS system is ideal for our needs, providing same day results to our outpatient clinics.
One of the most important aspects of the system for our laboratory is the ability to process samples as they are received in the laboratory. With our previous method, we had to work in batches of 24 or 48, collect-ing and storing samples throughout the day (or overnight) until we had a suffi cient
Faster viral load results for an improved clinical serviceWith 1,300 beds and over 6,000 employees, the Hospital Universitario 12 de Octubre in Madrid is one of the largest hospitals in Spain, serving a population of more than 500,000 people in and around the capital. It is an important teaching and research centre with a number of areas of expertise, including organ transplantation and the diagnosis and treatment of cancer.
– June 2016 Laboratory spotlight32
Figure 1. Comparison of VERIS HBV viral load assay with existing technology.
a) Scatter plot with Passing & Bablok Fit Pearson correlation r = 0.92
b) Difference plot
018_033_CLI_JUNE_2016.indd 32 15/06/16 16:02

number of samples for a single run. Th en results were not avail-able until the entire run was completed. Th is had a huge impact on response times.
Now, with the random access capabilities of the DxN VERIS sys-tem, this has changed. We receive samples around the clock and we are able to run them straight away. Th is has improved our response times signifi cantly, from 24-28 hours to just 4-5 hours from sample receipt, and with comparable quality of results com-pared to our previous method.
At the moment we enter results into the patient record manually, but soon we will be moving to a barcode system that will transfer all details and results into the electronic patient record automati-cally, saving time and further reducing opportunities for human error.
Expanding laboratory capabilitiesTh e DxN VERIS system has been well received by laboratory staff and has expanded our service capabilities. Fully automated from the loading of samples to obtaining results, it is easy to operate by laboratory technicians of all abilities. In addition, since it involves minimal manual intervention and fewer steps than our previous method, there is less opportunity for error and staff have more time to perform other important tasks in the laboratory.
One of our objectives as a clinical microbiology department is to off er a more complete panel of assays on a 24-hour basis. Previ-ously, this was not possible for molecular diagnostic investigations such as HBV and HCV viral loads, because it was not practical to run one or two samples at a time on our previous system. Th e ran-dom access and ease of use of the DxN VERIS system has enabled us to operate our HBV/HCV viral load service 24 hours per day, making it ideal to meet the variable needs of our laboratory in terms of workload volume and response times.
For further information about the DxN VERIS Molecular Diagnos-tic System and the VERIS assays currently available, please contact: Tiff any Page, Senior Pan European Marketing Manager Molecular Diagnostics, Email: [email protected] or visit www.beckmancoulter.com/moleculardiagnostics
References1. Rafael Delgado (2015) Evaluation in a Clinical Setting of the General Perfor-
mance of DxN VERIS CMV and HBV Viral Load Assay. Oral presentation, ECCMID, Copenhagen.
2. Gutiérrez, F, Zurita, S, Pérez-Rivilla, A and Delgado, R (2015) Evaluation of the Automated DxN VERIS System for Human Immunodefi ciency Virus Type-1 (HIV-1) and Hepatitis C Virus (HCV) Viral Load (VL) Monitoring. Poster pres-entation ESCV, Edinburgh.
The authorRafael Delgado, Head of Clinical Microbiology Hospital Universitario 12 de Octubre, Madrid, Spain.
– June 201633
QUANTA Flash® dsDNA
• Excellent agreement with Farr assay without hazardous and laborious techniques.
• First result is available in 30 minutes.1
• Strong correlation with kidney involvement in lupus nephritis patients2, 3
• Excellent agreement between anti-dsDNA antibody results and SLE activity parameters such as SLEDAI, C3, C4, and total complement activity4
• Now FDA Cleared!
References 1. Toh, B. H., et al. QUANTA Flash dsDNA antibody results show close correlation with Farr assay results. Poster. 9th International Autoimmunity
Congress, Nice France. 2. Garcia, M. et al. The QUANTA Flash dsDNA assay demonstrates reliable clinical performance in systemic lupus
erythematosus. Poster. 9th International Autoimmunity Congress, Nice France. 3. Data on file. Inova Diagnostics. 4. Garcia, M. et al. Strong
correlation between QUANTA Flash anti-dsDNA results and disease activity parameters in systemic lupus erythematosus. Poster. 9th
International Autoimmunity Congress, Nice France.
QUANTA Flash is a registered trademark of Inova Diagnostics, Inc. © 2016 Inova Diagnostics, Inc. All rights reserved.
690550 June 2016 Rev. 0
See us at AACC booth 807
dsDNA positive
agreement to Farr+
QUANTA Flash dsDNA outperforms other
leading systems in comparison to Farr1
65
70
75
80
85
80.2%
78.3%
76.5%
67.4%
dsDNA negative
agreement to Farr++
+Equivocal samples considered positive ++Equivocal samples considered negative
QUANTA Flash dsDNA
Other dsDNA Test System
E VOLUTIONARYA fully automated, chemiluminescent assay to aid in the diagnosis of systemic lupus erythematosus (SLE)
www.cli-online.com & search 27277
Table 1. VERIS HBV assay precision calculated on the basis of the EP05-A2 Precision Protocol.
018_033_CLI_JUNE_2016.indd 33 15/06/16 16:02

Sekisui Diagnostics to distribute Qualigen Inc.’s POC immunoassay products
Sekisui Diag-nostics and Qualigen Inc. announce a new strategic part-nership, encom-passing both
current business and future collabora-tion opportunities. Effective immedi-ately Sekisui Diagnostics will assume commercial activities and distribution management for the FastPack IP System and associated products in the U.S. and international markets. The FastPack IP System is an established, point of care immunoassay system designed to enable physician office laboratories (POLs) to offer key quantitative test results where there is immediate clinical value. The test menu includes Vitamin D, Testos-terone, TSH, Free T4, PSA, and hCG.www.sekisuidiagnostics.com
QuikRead go CRP test cleared in the US
Orion Diagnos-tica’s QuikRead go CRP test received clear-ance from the
US FDA to market the device for clini-cal laboratories. The QuikRead go test system measures C-reactive protein (CRP) in whole blood, plasma and serum in 2 minutes. The system con-sists of a small device and a ready-to-use reagent kit with all the materials
for performing the test. This easy-to-use system is in wide use worldwide. The tests available for the system out-side US includes CRP, CRP+Hb, Strep A and iFOBT. Measurement of CRP aids in the evaluation of injury to body tissues, and infection and inflam-matory disorders. The advantages of measuring CRP lie in it being a sensi-tive, early, and reliable reflector of the acute-phase response. Quantitative measurement of CRP concentration has been reported to be a sensitive indicator of the efficacy of antimicro-bial therapy and the course of bacte-rial infections. The rise in CRP level is non-specific. www.oriondiagnostica.com
GeT online – the new microsite from Greiner Bio-One
Under the ban-ner “GeT Per-fect”, Greiner Bio-One has kicked off the European pro-motion of the
Greiner eHealth Technologies Solu-tion – GeT. For this purpose, a mod-ern microsite in German and English has been created. The one page site provides all essential information at a glance. GeT utilizes a flexible modular based software solution whilst applying the advantages of pre-barcoded VACU-ETTE tubes. The aim is to increase the efficiency of routine procedures in and around the laboratory. This page pro-vides information on events, reference
customers as well as study material. Testimonials from reference customers report on their experiences. Advantages of the system and working procedures can be seen in the form of videos and animation. All in all, the user has here a compact version of all initial informa-tion required for initiating any further steps.www.gbo.com/get
Siemens Healthcare becomes Siemens Healthineers
In early May Siemens Health-care unveiled its new brand name
Siemens Healthineers. The new brand underlines Siemens Healthcare’s pio-neering spirit and its engineering exper-tise in the healthcare industry. It is meant to describe the healthcare organization and its people – the people accompa-nying, serving and inspiring customers – the people behind outstanding prod-ucts and solutions. As part of its Vision 2020 strategy Siemens AG announced nearly two years ago that its healthcare business would be separately managed as a company within the company with a new organizational setup. Siemens Healthineers will continue to strengthen its leading portfolio across the medical imaging and laboratory diagnostics busi-ness while adding new offerings such as managed services, consulting and digital services as well as further technologies in the growing market for therapeutic and molecular diagnostics.www.healthcare.siemens.com
INDUSTRY NEWS – June 2016 34
www.cli-online.com & search 27173
034_040_CLI_JUNE_2016.indd 34 15/06/16 16:03

Immunoturbidimetric fecal calprotectin assay
Fecal calprotectin (fCAL) is the most important marker for in vitro diagnostic detection of gut infl ammation. Immunological quantitation is well established and is used in the diagnos-tic process of infl ammatory bowel diseases (IBD) and in the lifelong monitoring of these chronic conditions. fCAL test-ing today requires a signifi cant level of lab resources including stool sample handling, extrac-tion and the use of traditional immunological testing meth-ods. Th e BÜHLMANN fCAL turbo assay is a big step towards full automation. It reduces the time to result as well as the total hands-on time signifi cantly. It off ers the possibility of random access and is independent of the clinical chemistry platform. Validated applications are avail-able for the most common ana-lysers. Th e combination with the proprietary extraction device CALEX Cap for pre-analytical sample preparation simplifi es and accelerates stool diagnosis signifi cantly. Th e BÜHLMANN fCAL turbo utilizes the well-established standardization of the BÜHLMANN fCAL ELISA to provide reliability and conti-nuity of measurements.
BÜHLMANN LABORATORIESAACC Booth 4202 www.cli-online.com & search 27285
– June 201635PRODUCT NEWS
Rapid test range for viral infectionsMP Diagnostics’ newly launched MULTISURE Range consists of three separate devices for the diagnosis of diseases that are of major health concern: Dengue, HIV
and HCV. Th e MULTISURE rapid tests are qualitative immunochromatographic assays intended for the screening of dengue, HIV
and HCV infections and are equipped with MP Diagnostics’ patented reverse fl ow technology. Th e patented reverse fl ow technology enhances visual identifi cation for easier interpretation of results. MP Diagnostics’ ASSURE Reader and ASSURE Palm Reader are developed for use with the MULTISURE range of rapid tests and are fully integrated instruments designed for the institution’s needs. Th e MP ASSURE readers complement the reading and doc-
umentation of results for both laboratory and point-of-care settings. With the lat-est upgrade in soft ware, the MP ASSURE readers’ integration to management sys-tems would be seamless for all users.Th e new test range is for research use only in the United States.
MP DIAGNOSTICSAACC Booth 3635
www.cli-online.com & search 27286
Greiner Bio-One GmbH | Bad Haller Straße 32 | A-4550 KremsmünsterPhone: (+43) 75 83 67 91-0 | Fax: (+43) 75 83 63 18 | E-mail: [email protected] www.gbo.com/preanalytics
� For the diagnosis of diabetes mellitus and gestational diabetes
� Unique additive mixture in the tube
� Immediate stabilisation based on the in vivo value for 48 hours
� Prevents false negative diagnoses
� Longer sample stabilisation enables longer transport
� Stabilisation in whole blood, no immediate centrifugation required
Glucose Stabilisation Right from the BeginningThe birth of the new FC Mix tube
www.cli-online.com & search 27178
034_040_CLI_JUNE_2016.indd 35 15/06/16 16:03

034_040_CLI_JUNE_2016.indd 36 15/06/16 16:03

Urine Oxalate assayB i o S y s -t e m s l au n c h e s a new rea-gent for the meas-urement of
oxalate (oxalic acid) in urine. Oxalate is an end product of metabolism, predominantly derived from the breakdown of glyoxylate and glycine. It is eliminated entirely by urine and only about 15% of urinary oxalate is derived directly from dietary sources. Hyperoxalu-ria is a powerful promoter of calcium oxalate stone forma-tion. An increased excretion of oxalate in urine may occur as a result of an excessive ingestion of oxalate-rich foods, because of malabsorption due to dif-ferent gastrointestinal disor-ders (enteric hyperoxaluria) or because of an inborn error of metabolism (primary hyper-oxaluria). Low oxalate values in urine are associated with hyperglycinemia or hypergly-cinuria. BioSystems introduces this method (Oxalate Oxidase/Peroxidase - diff erential birea-gent) in dedicated presenta-tion for A15 and A25 analysers (code 12539: 1x25mL, 20 tests). It is calibrated using its own standard included in the kit. Th e kit also includes 20 pre-treatment tubes which are also available separately in 100-unit packs (Oxalate Pretreatments Reagents: code 11839).
BIOSYSTEMSAACC Booth 3563 www.cli-online.com & search 27291
– June 201637PRODUCT NEWS
New reagent to measure dabigatranStago completes its anticoagulant line with a new reagent, STA-ECA II, for the measure-ment of dabigatran plasma concentration in patients under treatment, in case of emer-gency (hemorrhage, urgent surgery or inva-sive procedure). STA-ECA II is an ecarin-based chromogenic assay which specifi cally measures the anticoagulant eff ect of direct thrombin inhibitors like dabigatran. Th e use of dedicated calibrators and controls
is necessary. Th is assay is insensitive to lupus anticoagu-lant, heparin and variations in lev-els of coagulation
factors and fi brinogen. Available on STA R Max, STA-R and STA Compact Max, STA-ECA II shows excellent analytical perfor-mances down to 15 ng/mL in the low range, with a high correlation to the reference
technique for dabigatran measurement, LC-MS using “total dabigatran” protocol. With a long on-board stability (3 days) and at 2-8°C (28 days), this reagent is suitable for all types of laboratory activities. In the USA and Canada this product is classifi ed as “For Research Use Only”.
STAGOAACC Booth 827
www.cli-online.com & search 27290
MULTISURE HIVThe new benchmark for HIV-1/2 screening
www.mpbio.com/[email protected]
100% Sensitivity, 99.12% Specificity
Detects & Differentiates HIV-1/2
Patented Reverse Flow TechnologyASSURE Palm Reader
See you at Booth #3635
www.cli-online.com & search 27218
034_040_CLI_JUNE_2016.indd 37 15/06/16 16:03

HbA1c enzymatic assay
Th e HbA1c value correlates with the average blood glucose level over the last 8-12 weeks and is used for monitoring and diagnosis of diabetes. DiaSys off ers HbA1c net FS as a liquid-stable and ready-to-use 2-compo-nent assay. Due to the enzymatic test princi-ple, excellent precision is ensured. Interfer-ence from a variety of hemoglobin variants like HbS, HbC, HbD, HbE, or HbF can be excluded. HbA1c net FS is characterized by a wide measuring range from 20 to 150 mmol/mol IFCC (4-6% DCCT/NGSP) and high on-board and calibration stability of up to 6 weeks. Moreover, this assay is standardized against the IFCC reference method and trace-able according to the DCCT/NGSP network.
DIASYSAACC Booth 2056
www.cli-online.com & search 27284
PRODUCT NEWS – June 2016 38
MSACL 2017 US9th Annual Conference & Exhibits
J a n u a r y 2 2 - 2 6Palm Springs, California
Deadl ine : September 28
Podium Abst racts
Deadl ine : Nov 16 - Dec 21
Poster Abst racts
Travel Grants
www.msacl .o rg
Regis t rat ion Deadl inesEar ly : Ju ly 13Regular : August 03Late : August 10
MSACL 2016 EU3rd Annual Congress & Exhibits
SSeepppttteeemmbbeerr 1122--1155
Poster Abst ract Deadl ine :
June 22 - Ju ly 20
dec i s ion not i ca t ion wi th in
10 days o f submiss ion
www.msacl .o rg
Compact hematology analyserThe CELL-DYN Emerald 22 hema-tology system is designed to be a full perfor-mance solution for smaller labo-ratories seeking
greater productivity under tighter space limitations. Startup and shut-down can be programmed to occur automatically each workday. The instrument requires zero daily main-tenance. This compact, easy-to-use 5-part differential hematology ana-lyser offers a small footprint, low rea-gent consumption and easy-to-use features like touch-screen technol-ogy, automatic startup, shutdown and cleaning, making it the ideal choice where space and specialized staff are limited.
ABBOTT DIAGNOSTICS AACC Booth 1701
www.cli-online.com & search 27291
CALENDAR OF EVENTS
July 31-August 4, 2016AACCAtlanta, GA, USAwww.aacc.org
September 12-15, 2016MSACL EUSalzburg, Austriawww.msacl.org
September 14-17, 201619th Annual ESCV Meeting Lisbon, Portugalwww.escv2016.com
September 21-24, 2016EFLM-UEMS CongressWarsaw, Polandwww.efl m-uems.warsaw2016.eu
September 25-29, 2016European Congress of PathologyCologne, Germanywww.esp-congress.org/2016
September 28-30, 2016Analytical and Bio-analytical TechniquesOrlando, FL, USAwww.analytical-bio-analytical.pharmaceu-ticalconferences.com
September 29-1 October, 2016British Society for Allergy & Clinical ImmunologyTelford, Shropshire, UKwww.bsaci.org
Dates and descriptions of future events have been obtained from offi cial industrial sources. CLi cannot be held responsible for errors, changes or cancellations.
For more events see:www.cli-online.com/events/
034_040_CLI_JUNE_2016.indd 38 15/06/16 16:03

The life science business of Merck now offers:• An extended global network across more than 66 countries• A world-class e-commerce platform to simplify transactions• A vast portfolio that has grown to over 300,000 productsOur combined strengths will deliver the knowledge, know-how, and best-in-class resources.
Learn more at merckgroup.com/life-science
EXPERTlife science
The life science leaders ofMerck Millipore + Sigma-Aldrichhave joined together and, with our agile e-commerce and global distribution, we can help to simplify your world. So you can focus with confidence on tackling life science’s biggest challenges.
and e-commerce leader
Merck, Merck Millipore and the vibrant M are trademarks of Merck KGaA and its affiliates. Sigma-Aldrich is a trademark of Sigma-Aldrich Co. LLC and its affiliates. Copyright © 2016 Merck KGaA. All Rights Reserved.
The life science business of Merck operates as MilliporeSigma in the U.S. and Canada.
www.cli-online.com & search 27275
034_040_CLI_JUNE_2016.indd 39 15/06/16 16:03

Are you still diagnosing Trichomonas with a microscope or waiting forlab results? Trixie here is an amazing swimmer and is a very tricky bug todetect, and treatment is important.
The OSOM® Trichomonas Test is the only CLIA waived rapid diagnosticdesigned for labs or decentralized testing. It does not rely on the detection of a live organism and can be completed in 10 minutes!
What does this mean to you and your patients? Far more accurate detection and the ability to test and treat in onevisit which helps improve patient care and reduce costs.
Answers for Healthcare. Awesome...yes, OSOM®.Call +44-1622-607800 or email [email protected].
TRICH OR TREAT?
© 2016 Sekisui Diagnostics, LLC. All rights reserved. OSOM® is a registered U.S. trademark of Sekisui Diagnostics, LLC.MADE IN THE USA
www.cli-online.com & search 27282
034_040_CLI_JUNE_2016.indd 40 15/06/16 16:03