Embed Size (px)
Citation preview

Candidal PneumoniaCandidal Pneumonia
Case IICase II 70 y female seen in oncology clinic Jan 5/0570 y female seen in oncology clinic Jan 5/05
PMH : MDS PMH : MDS NHL IV large cell NHL IV large cell
Initial Dx 2001 Initial Dx 2001 chemo 2001 & 2002 chemo 2001 & 2002
& XRT (axilla & groin) & XRT (axilla & groin)
2003 2003 remission remission
2004 Nov 2004 Nov recurrence recurrence
Fludarapine & steroidFludarapine & steroid

HistoryHistory
3/52 unresolving SOBE , Dry cough3/52 unresolving SOBE , Dry cough
intermittent fever & sweatingintermittent fever & sweating
No response to 2 courses of AbxNo response to 2 courses of Abx
Azithromycin & CefuroximeAzithromycin & Cefuroxime Wt loss 15 lb Wt loss 15 lb
No H/O TB or contactNo H/O TB or contact
HistoryHistory No travel , petsNo travel , pets
Being receiving IVIG for ITPBeing receiving IVIG for ITP
PMH : HTN , Hpothyroidism PMH : HTN , Hpothyroidism
Lt nephrectomy for persistent hydronephrosis from LN Lt nephrectomy for persistent hydronephrosis from LN compression Baseline Creat 80compression Baseline Creat 80
Med : ASA , Ramipril , Predinsone Med : ASA , Ramipril , Predinsone

ExaminationExamination
Temp 37 BP 100/60 HR 100Temp 37 BP 100/60 HR 100 RR 16 Sat 95 % RR 16 Sat 95 % No desaturation with walkingNo desaturation with walking
Palpable LN , central tracheaPalpable LN , central trachea
Chest : Good BS , Crackles Rt baseChest : Good BS , Crackles Rt base
LL edema LL edema

InvestigationInvestigation WBC 8 N Diff Hb 95 MCV NWBC 8 N Diff Hb 95 MCV N
Plt 25 PTT & INR NPlt 25 PTT & INR N
Lytes , BUN & Creat N Lytes , BUN & Creat N
LFT & UA NLFT & UA N
CXR & CT chestCXR & CT chest

CourseCourse
BAL Jan 6BAL Jan 6thth /05 /05
BAL BAL -ve PCP , AFB & cytology -ve PCP , AFB & cytology
Empiric Rx with Septra , Gatifluxacine Empiric Rx with Septra , Gatifluxacine
BAL C/S BAL C/S Candid Albicans Candid Albicans
& Enterococcus& Enterococcus No improvement on AbxNo improvement on Abx

CourseCourse Seen in St.B ER Jan 14Seen in St.B ER Jan 14thth /05 /05 Nausea , Vometing & Abdominal pain 2/7Nausea , Vometing & Abdominal pain 2/7
Seen by Gen Sx Seen by Gen Sx ? Bowel obstruction? Bowel obstruction
Waiting CT Waiting CT Increase work of breathing Increase work of breathing & Hypoxia & decrease LOC & Hypoxia & decrease LOC
Intubated , Hypotensive Intubated , Hypotensive
CourseCourse
CT Abdomen CT Abdomen extensive LN extensive LN Non mechanical obstructionNon mechanical obstruction
Septic shock , Acute renal failure Septic shock , Acute renal failure DIC & lactic acidosisDIC & lactic acidosis
Empiric Abx Vanco , Cipro & MetroEmpiric Abx Vanco , Cipro & Metro
Repeat BronchRepeat Bronch

CourseCourse
BAL BAL +ve Candida Albicans +ve Candida Albicans
Blood C/S 2/2 Blood C/S 2/2 yeast yeast
Empiric Ampho BEmpiric Ampho B
Yeast Yeast Candida Albicans Candida Albicans
Ampho B Ampho B Fluconazole Fluconazole

CourseCourse Persistent Shock , ARFPersistent Shock , ARF
GI bleeding GI bleeding ischemic colitis Vs CMV ischemic colitis Vs CMV
Withdrawal of care upon family requestWithdrawal of care upon family request
Candida PneumoniaCandida Pneumonia
Retrospective study 20 y of oncology ptsRetrospective study 20 y of oncology pts
Isolation of Candida from lung tissueIsolation of Candida from lung tissue
No candidemiaNo candidemia
31 cases 9 only neutropenic 84% mortality31 cases 9 only neutropenic 84% mortality
High incidence of candida osophagitisHigh incidence of candida osophagitis
? Aspiration lead to pneumonia ? Aspiration lead to pneumonia
Medicine (Baltimore). 1993 MayMedicine (Baltimore). 1993 May

CandidemiaCandidemia
Fourth leading cause of blood stream infection Fourth leading cause of blood stream infection following staph aureus following staph aureus
, C/N staph & enterococcus, C/N staph & enterococcus
Surrogate marker of deep seated infectionSurrogate marker of deep seated infection
Untreated Untreated 15% endophthalmitis 15% endophthalmitis endocarditis ,arthritis & reanl candiadiasisendocarditis ,arthritis & reanl candiadiasis
NEJM Dec 2002NEJM Dec 2002

CandidemiaCandidemia
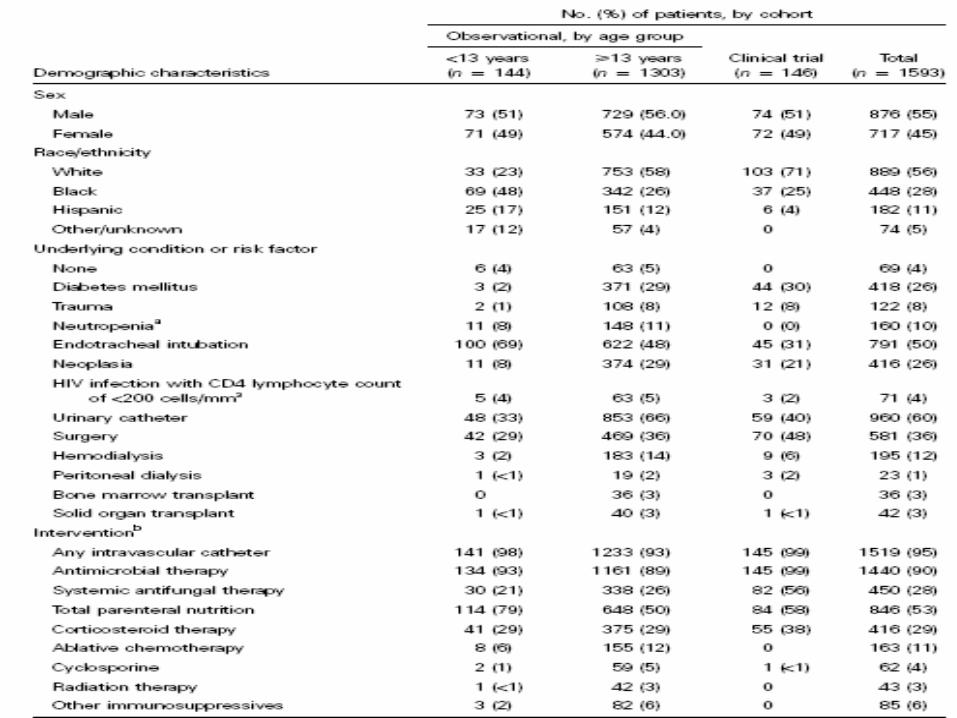
Prospective Multicenter observational Prospective Multicenter observational study 1997 study 1997 1999 Adults & Pediatric Pt1999 Adults & Pediatric Pt
Incidence of Candidemia & isolateIncidence of Candidemia & isolate Candidemia mortality : <24 of +ve C/SCandidemia mortality : <24 of +ve C/S persistent +ve C/Spersistent +ve C/S postmortem postmortem 1449 Adults & 144 peadiatric Pts1449 Adults & 144 peadiatric Pts Clinical Infectious Dis Sept 2003Clinical Infectious Dis Sept 2003


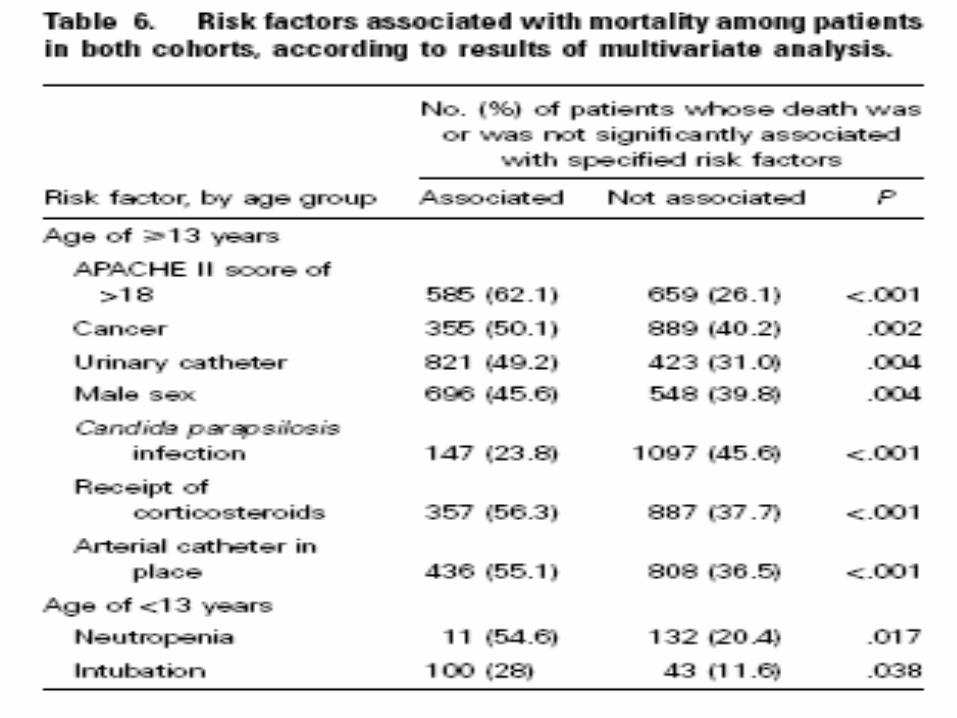
CandidemiaCandidemia Overall 3 months mortality 40% Overall 3 months mortality 40% Cause specific mortality 12%Cause specific mortality 12%
Candida Albican was associated with higher mortality Candida Albican was associated with higher mortality 47% Adults 23% peads47% Adults 23% peads
Candida Parapsilosis had the lowest Candida Parapsilosis had the lowest
Risk factor associated with mortality Risk factor associated with mortality Underlying malignancy ,Neutropenia Underlying malignancy ,Neutropenia Steroid & Lines Steroid & Lines Clinical Infectious Dis Sept 2003Clinical Infectious Dis Sept 2003
Fluconazole Vs Ampho BFluconazole Vs Ampho B Prospective randomized Plcb ControlProspective randomized Plcb Control
Multicenter 106 pateintsMulticenter 106 pateints
Ampho B 0.6 mg/kg / dayAmpho B 0.6 mg/kg / day
Vs Fluconazole 800mg loading &400 mg/dVs Fluconazole 800mg loading &400 mg/d
Switch to Ampho B in case of C.glabrata & C.crusie Switch to Ampho B in case of C.glabrata & C.crusie
Eur J Clin Microbiol Infect Dis. 1997 MayEur J Clin Microbiol Infect Dis. 1997 May

Fluconazole Vs Ampho BFluconazole Vs Ampho B
Successful Rx Successful Rx
Fluconazole 50% Vs Ampho B 57% P 0.39Fluconazole 50% Vs Ampho B 57% P 0.39
14 day mortality14 day mortality
27% Vs 21% P 0.5727% Vs 21% P 0.57
Side effect 0% 4% Side effect 0% 4% Eur J Clin Microbiol Infect Dis. 1997 MayEur J Clin Microbiol Infect Dis. 1997 May

High Dose Flucon Vs Flucon + Ampho BHigh Dose Flucon Vs Flucon + Ampho B
Randomized multicenter 219 ptsRandomized multicenter 219 pts
Non neutropenic nor expected to brNon neutropenic nor expected to br
Non Candida. CrusieNon Candida. Crusie
No Liver , renal impairment No Liver , renal impairment Clinical infectious Dis May 2003Clinical infectious Dis May 2003

High Dose Flucon Vs Flucon + Ampho BHigh Dose Flucon Vs Flucon + Ampho B
Flucon 800 mg + Plcb (first 7 days)Flucon 800 mg + Plcb (first 7 days) Flucon 800 mg +Ampho B .07 mg/kg Flucon 800 mg +Ampho B .07 mg/kg April 95 April 95 May 99 May 99
Successful Rx Successful Rx clinical improvement clinical improvement & -ve blood C/S& -ve blood C/S
Failed Rx Failed Rx no clinical improvement no clinical improvement persistent fungemiapersistent fungemia side effectsside effects Clinical infectious Dis May 2003Clinical infectious Dis May 2003


High Dose Flucon Vs Flucon + Ampho BHigh Dose Flucon Vs Flucon + Ampho B
Candida Albicans most commonCandida Albicans most common
Persistent fungemia 53%Persistent fungemia 53%
Renal Imapirment 3% Vs 23%Renal Imapirment 3% Vs 23%
Successful Rx 56% Vs 69% P 0.43Successful Rx 56% Vs 69% P 0.43
90 Mortality 39% Vs 40%90 Mortality 39% Vs 40%
Higher failure with Higher APACHE , TPNHigher failure with Higher APACHE , TPN Clinical infectious Dis May 2003Clinical infectious Dis May 2003