Embed Size (px)
Citation preview

Cancers Invading the Bones of the Face and Skull *
CLAUDE C. COLEMAN, JR., M.D., F.A.C.S., WILLcox RUFFIN, JR., M.D.
From the University of Virginia School of Medicine, Charlottesville, Virginia.
NEGLECrED or inadequately treated can-cers of the scalp, face and paranasal sinusesextend into the contiguous bones of theskull and maxillofacial skeleton. The prox-imity of the brain, major venous sinuses ofthe dura and carotid artery has generallyrelegated treatment of such lesions to theradiotherapist despite the fact that thesetumors are singularly refractory to anyform of radiotherapy, curettage or desicca-tion. Endocranial extension may involvethe brain, cranial nerves and major vessels.Intractable pain, deafness and repeatedprofuse hemorrhage precede somnolence,pernicious vomiting and coma.
Radiotherapy, coagulation or curettagerenders the margins of such cancers nebu--lous and ill-defined. Secondary infectionand tissue changes resulting from over-zealous irradiation virtually eliminate thereliability of histologic interpretation.' Thenecessity for removing the additional rav-ages of over-iTradiation greatly magnifiesthe problem of complete removal of thecancer and effective management of theresultant defect. These defects harbor thevital structures deep in the field of dissec-tion. The topography of such woundscreates many difficulties in wound manage-ment. The uneven, sharp margins of sur-rounding bone eliminate the possibility offree skin grafting in most instances, andvascular changes caused by previous radio-
* Submitted for publication September 28,1961.
Presented at the Seventh Annual Meeting ofthe Society of Head and Neck Surgeons, MiamiBeach, Florida, March 17, 1961.
129
therapy make pedicle-flap coverage a ne-cessity. Such maneuvers, which consider-ably lengthen the duration of the operation,should be avoided if possible; however,when indicated, we have successfully uti-lized large, previously undelayed rotationscalp flaps to cover these defects.4 16,17
Clinical Data
Eleven patients are reported, seven ofwhom had been operated upon one ormore times and/or had received radio-therapy. Five of these individuals had sub-total resection of the temporal bone withcontiguous structures, two had combinedresections of the skull and maxillofacialskeleton, two underwent extensive skull re-sections, and two had composite resectionsof the face and maxillofacial skeleton be-cause of recurrent carcinoma in the regionof the orbit.
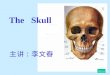
Case 1, 447665, a 70-year-old white woman,was admitted in July 1958 with a fungating,ulcerative carcinoma of the left orbit and medialperiorbital structures with extension into the con-junctival folds of the lower lid, the left half ofthe nose and the supraorbital region. The upperlid was fixed with tumor in the medial portion ofthe supraorbital ridge (Fig. la). X-rays demon-strated destruction of the inferior rim of the orbitand anterior wall of the antrum (Fig. lb). Biopsyof the lesion showed basal cell carcinoma withsquamous cell characteristics.
An en bloc orbito-antral exenteration with re-section of the left half of the nose and partialresection of the cheek was performed and thewound was closed with a free split graft. The leftcheek, orbit and nose were reconstructed in stageswith a transthoracic tubed pedicle flap, one endof which was employed as a dermal-fat flap to

COLEMAN AND RUFFIN
obliterate the left frontal sinus (Fig. lc). Sub-sequent revisions and defatting procedures havebeen completed. There is no evidence of re-
current tumor after a three-year follow up period(Fig. id).
Annals of SurgeryJuly 1962
Case 2, 432539, a 78-year-old Negro woman,
was admitted in June 1959 because of severe
hemorrhage from a recurrent ulcerated lesionextending from the medial canthus into the con-
junctiva and cheek, medially into the lateral wall
.tDo: .... ... ,2.1 .:I
FIG. 1. Case 1. (a) Extensive basal cell carcinoma of left orbit and cheek. (b) Destructionof the floor and rim of orbit. (c) Well-healed graft in left orbito-antral defect. Transthoracicpedicle flap is ready for transfer to facial defect. (d) Obliteration of bone defect with double-layered pedicle flap.
130

Volume 156 CANCERS INVADING BCNumber 1
of the nose and superiorly into the anterior eth-moid cells. The lesion appeared 12 years previ-ously and had been excised in 1946 and re-excisedin 1948. X-ray examination revealed invasion ofthe inferior orbital rim.
A left orbito-antral exenteration with resectionof the left half of the nose and partial resectionof the cheek was performed and the wound wasclosed with a large rotation scalp flap. On No-vember 8, 1957, the unused portion of the scalpflap was returned to the head. Reconstruction ofthe nose has been essentially completed. She isfree of cancer nearly four years after resection.
Comment. Total elimination of the can-cers as seen in Cases 1 and 2 creates exten-sive orbito-antral defects, the boundariesof which may be the uneven remnants ofthe sphenoid sinuses, zygoma and hardpalate. We are therefore faced with thetwo-fold task of total tumor destructionand the reconstruction of highly complexwounds. The use of a split graft is the mostexpedient means to cover wounds whichhave not been irradiated because thesegrafts are readily fixed into the pterygoidfossa, pharynx and orbital remnants.
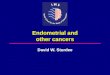
FIG. 2a. Case 4. a Displacement of right eyefrom cancer of fronto-ethmoid-antral labyrinth.Opthalmoplegia and blindness.
)NES OF FACE AND SKULL 131
FIG. 2b. Destruction of rim of orbit, ethmoid andmedial wall of orbit.
Case 3, 438059, a 59-year-old white man, ad-mitted in October 1957, gave a history of chronicsinusitis and reported the removal of a malignantpolyp from the right middle turbinate on January10, 1957. The right globe was markedly elevatedand swollen and the palpebral fissure was nar-rowed. X-rays revealed a cloudy right maxillaryantrum and destruction of the infra-orbital rimand floor of the orbit. The diagnosis, confirmedby biopsy, was transitional epidermoid cell carci-noma of the antrum with orbital extension andpossible extension into the anterior ethmoid cells.
An orbito-antral exenteration with resection ofthe right maxilla and right hemisection of thenose was performed. The wound was closed witha free split graft. On the fourteenth postoperativeday, he was discharged with a functioning palatalprosthesis. There is no evidence of cancer threeand one-half years since the initial operation. Hisspeech and deglutition are satisfactory. Stagedreconstruction, utilizing a delayed, lined, loop-shaped forehead flap, has been partially com-pleted. The defect of the palate will be closedpermanently with a cervical flap carried throughthe floor of the mouth.
Case 4, 453141, a 50-year-old white man, wasadmitted in November 1958 because of a pro-gressive right ophthalmoplegia and loss of vision.The right eye was markedly proptosed and dis-placed laterally (Fig. 2a) and there was tender-ness over the antrum. X-rays showed an expandinglesion of the antrum with destructive changes in

132 COLEMAN AND RUFFIN
FIG. 2c. Monobloc resection of right frontalbone, dura, floor of skull with ethmoid labyrinth,orbit and maxillary sinus. Dural defect filled withfascia lata.
the fronto-ethmoid region and antrum (Fig. 2b),and biopsy of the lesion revealed undifferentiatedcancer.
A monobloc resection of the right fronto-ethmoid labyrinth, dura, right orbit, and maxillawas performed (Fig. 2c). Extension of the can-cer through the frontal bone into the dura neces-sitated the removal of most of the dura coveringthe right frontal lobe. This defect was closed witha fascia lata graft. The huge defect in the skulland maxillofacial skeleton was filled by rotatingthe frontal scalp flap inferiorly to the free marginof the lesser wing of the sphenoid. This procedureprotected the fascial graft and, to some extent,replaced the floor of the anterior fossa of theskull thereby affording support to the frontallobe. The pterygoid fossa and the apex of theorbit were resurfaced with a split-thickness graft.The patient was ambulatory on the second post-operative day (Fig. 2d). Function was reconsti-tuted with a prosthesis. Histologic diagnosis ofthe specimen was highly undifferentiated epi-dermoid carcinoma with sarcomatous elements.Although the sphenoid sinus was not grossly in-volved, microscopic examination revealed exten-
Annals of SurgeryJuly 1962
sion to the posterior margin of the resection and,in view of the natural course of such tumors,cobalt-60 radiotherapy to the frontal lobe throughthe scalp flap was started on the twelfth post-operative day. The patient was lost to follow upuntil October 1959 at which time reconstructionwas initiated but was abandoned because of ex-tensive recurrence in the right frontal lobe. Hesuccumbed to his disease 16 months after hisoriginal resection.
Comment. Cancers of the ethmoid laby-rinth, usually considered nonresectable be-cause of their posterior extension, inacces-sibility and their high grade of malignancy,are generally treated by piece-meal surgeryplus some form of radiotherapy.The principles of block resection were
used in Case 4, and it is conceivable thatsuch an approach, if applied to cancers ofless magnitude, could offer more hope tothese patients. A pertinent factor in the sur-gical approach to this cancer was the skinincision. If the orthodox coronal scalp flaphad been turned down to approach thefrontal bone, wound closure would have
FIG. 2d. Well-healed frontal scalp flap.

CANCERS INVADING BONES OF FACE AND SKULL
been impossible. By planning the woundreconstruction in conjunction with the ap-
proach to the tumor, a large rotation scalpflap could be turned back to expose thecranium and was utilized to cover andsupport the brain.
Case 5, 418730, a 75-year-old white man, withthe complaint of constant headache and partialdeafness was referred in July 1956 with a diag-nosis of recurrent squamous cell carcinoma ofthe left ear. Cancer of the left helix had beenexcised in April 1955, treated with two courses
of x-ray therapy in May 1955, and again excised
FIG. 3. Case 5. (a) Recurrent epidermoid cancer of ear with extension into mastoid andparotid. (b) Drawing of composite resection of ear, scalp, parotid and temporal bone. (c) Re-construction with large undelayed rotation scalp and cheek flaps. Split grafts to flap donorsites. (d) Patient has no recurrence of cancer nearly five years after resection.
Volume 156Number 1 133

134 COLEMAN AND RUFFIN
in October 1955. A foul, fungating cancer filledthe external ear and extended posteriorly throughthe concha into the postauricular scalp (Fig. 3a).There was conduction deafness and seventh nerveparesis. Destruction of the left mastoid bone wasevident on x-ray.
Block resection of the ear, periauricular skinand scalp, parotid gland and subtotal resectionof the temporal bone were done and the defectimmediately reconstructed utilizing a rotationscalp flap and a rotation cheek flap (Figs. 3b, c).The patient has been followed four and a halfyears and has no evidence of recurrence (Fig. 3d).
Case 6, 475125, a 78-year-old white man, hadexcision of an ulcerated basal cell carcinoma fromthe posterior surface of the right ear in 1955.In 1957, a recurrence at the cephalo-auricularangle was widely excised and split-grafted. InFebruary 1960, he was admitted because of re-current basal cell carcinoma. Examination revealedonly linear ulceration and erythema in the cephalo-auricular crease. X-rays of he facial and temporalbones revealed sclerosis of both mastoid boneswith no definite bony destruction.
At operation, the tumor was found to extendalong the auditory canal with fixation of the peri-osteum of the mastoid bone. In view of thesefindings and the previous history, a block resectionof the right ear, periauricular skin and scalp, andthe parotid gland was done in continuity with asubtotal resection of the temporal bone. A ro-tation scalp flap provided healthy, full-thicknesscoverage of the defect. He was discharged on thefourteenth postoperative day. Reconstructive pro-cedures, including fascial slings and rhytidectomy,were carried out in November 1960, and followup examinations to date reveal no recurrence.
Case 8, 460412, a 68-year-old white man, wasadmitted in June 1959 with a previously irradiated,painful, recurrent epidermoid carcinoma of theleft parotid area. There was left facial paralysis,involvement of the temporomandibular joint,large nodes in the left jugular chain and exten-sion of the tumor anteriorly and posteriorly aroundthe ear essentially obliterating the external audi-tory meatus. There were marked radiation bumsof the left cheek, ear, and mastoid bone. X-raysof the skull revealed no definite bony involvement.
Block resection of the left cheek, parotidgland, ear, left half of the mandible, and tem-poromandibular joint and temporal bone wasperformed in continuity with a formal neck dissec-tion. While resecting the temporal bone, theinternal carotid artery and internal jugular veinand the petrosal sinus were torn requiring intra-
Annals of SurgeryJuly 1962
cranial ligation of the carotid artery after expos-ing the retracted stump in the carotid canal. Arotation scalp flap was used to cover the defect.The scalp defect was split-grafted on the tenthpostoperative day. In the ensuing days, however,the patient developed an abscess of the lefttemporal bone and, despite surgical drainage, hedied on the thirty-fifth postoperative day.
Case 9, 480401, a 58-year-old white man, wasreferred on January 20, 1961, with a recurrent,previously irradiated basal cell carcinoma of theleft postauricular area. The lesion, measuring 3.0cm., was ulcerated, necrotic and had crossed thepostauricular sulcus and destroyed the lower halfof the auricle. There was marked surroundinginduration and fixation to the mastoid periosteum.The canal was clear and there were no symptomsof deafness, tinnitus or vertigo. X-ray did notreveal destruction of bone.
A composite resection of the ear, periauricularscalp and parotid gland along with subtotal re-section of the temporal bone was carried out. Alarge rotation scalp flap provided healthy coverfor the defect. Wide margins were reported bythe pathologist. The patient was discharged onthe eighteenth postoperative day.
Comments. Cases 5 through 9 demon-strate our surgical approach to deep inva-sive carcinomas involving the ear, periau-ricular area, mastoid bone and/or parotidgland. The rationale and technical ap-proach to temporal bone resections havebeen reported,2'3'5' 8,12 and our approachis similar to that advocated by Parsons.'8These lesions require monobloc resection ofthe involved tissues with varying amounts ofthe petrous pyramid. Exposure of the bonystructures in the middle and posteriorfossae of the skull and the dural sinuses inthe posterior fossa is made possible bycontinuous decompression of the cerebro-spinal fluid by the insertion of a poly-ethylene catheter in the subarachnoid spacethrough the fourth lumbar interspace. Afterthe temporal squama is adequately re-moved, the dura over the temporal boneis stripped from the middle and posteriorfossae. Elevation of the temporal bone suf-ficient to transect the petrous ridge withaccuracy is difficult unless the volume of

CANCERS INVADING BONES OF FACE AND SKULL
the cerebrospinal fluid in the cisterns andventricles is reduced to soften the brain.The same principle is applicable to resec-
tions involving the occipital and frontalbones. The use of large, undelayed rotationscalp flaps has proved effective in achiev-ing full-thickness coverage in these com-
plex compound wounds. These malignan-cies are locally highly invasive and oftenextend endocranially, but regional nodalmetastases have been shown to occur latein the course of the disease.20 For this rea-
son, a neck dissection is not performedunless there is clinical evidence of metas-
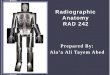
FIG. 4. Case 10. (a) Recurrent bleeding radioresistant basal cell cancer of occiput.Patient referred for terminal care. (b) Basal view showing cancer and/or x-ray destruction ofright occipital bone. (c) Drawing of resection of scalp, occipital bone and mastoid. (d) Patientis free of disease for 18 months.
Volume 156Number 1 135

136 COLEMAN AND RUFFIN
tasis.7'4 Enlarged nodes, if found whenthe sternocleidomastoid is severed, aresent for frozen section. Negative subdigas-tric nodes usually indicate no involvementof the lower regional nodes.
Case 10, 427201, a 78-year-old white man,bleeding profusely from the right occipital artery,was admitted November 1959. Examination re-vealed a 9.0 X 8.0 cm. dirty, postauricular ul-cerated cancer involving the right occiptal bone(Fig. 4a). X-ray examination revealed destruc-tion of the occiptal bone (Fig. 4b).The patient underwent block resection of the
right occipital scalp and bone, the right posteriorcervical muscles, mastoid bone and the inferiorthird of the ear (Fig. 4c). The defect was cov-ered with a rotation scalp flap. He has been fol-lowed for 16 months, and there is no recurrenceof tumor (Fig. 4d).
Case 11, 332690, a 67-year-old white woman,in 1949 had local excision of a basal cell carci-noma of the parietal scalp. A recurrent tumor wastreated with x-ray in 1949 and again in 1952. In1954 a left neck dissection was performed becauseof a solitary clinical metastasis in the subdigastricarea. The regional nodes were free of disease. In1955, a recurrence in the posterior parietal scalpwas incompletely excised with underlying skull.One month later, the margins of the resection weresurgically enlarged. In April 1955, she was re-ferred to us for reconstruction of the scalp defect.The dura was covered with a free split graft. Arecurrence at the junction of the dura and theposterior skull defect prompted resection of moreskull and grafting in January 1959. Another localrecurrence in June 1960 necessitated a similaroperation. Follow up examinations to date revealno tumor.
Comment. This case is presented to em-phasize the necessity for complete com-posite removal of the skull with the over-lying cancer. The difficulty of completeremoval of this lesion was magnified byinjudicious, inadequate, piece-meal removalof the skull. This case appears to supportthe contention that the malignant potentialof basal cell carcinoma is enhanced byextension into underlying bone.6 19
Annals of SurgeryJuly 1962
Discussion
Any therapeutic approach for malignantlesions invading the maxillofacial skeletonand skull by methods other than surgery,which could result in the initiation of fur-ther malignancy would seem contraindi-cated from the outset. McIndoe, in 1956,substantiated this viewpoint.'5 Such a dis-tinct disadvantage cannot be denied evenby those who are strong proponents of sur-face radiation. This is not a peculiarity en-tirely dependent upon the length of ex-posure, penetration or site. The importanceof individual sensitivity to radiation is illus-trated by Franklin-Bishop who discussedradiation burns and the sequelae whichmay follow single, simple diagnostic exami-nations.9 The production of unstable avas-cular scars, necrotic bone, cartilage andvessels would be predicted sequelae ofradiation therapy for the eleven patientswho have been reported. Even if deeplyrooted cancers are sterilized, the problemsof subsequent reconstruction are com-pounded by the destruction of adjacenthealthy tissue by radiation. Only with widesurgical margins can the pathologist accu-rately interpret a specimen. The prognosismust be closely guarded and repeatedly re-evaluated even in the face of favorablereports.The utilization of large scalp flaps as
advocated by Gaisford et al.,1" Lewis etal.,'3 Fredricks10 and Coleman4 is not in-tended as a definitive reconstructive pro-cedure, but simply provides temporaryfull-thickness coverage of the wound anddecreases the morbidity associated with ex-posure of these complex compound de-fects.4 The possible objection that an earlyrecurrence might not be detected is obvi-ated when wide surgical margins are ob-tained. If total extirpation is impossibledue to extension, radiation, as in Case 4,can be initiated through the flap.4

Volume 156 CANCERS INVADING BONES OF FACE AND SKULL 137Niimhbr 1
ConclusionsEleven patients are presented who have
had surgery for advanced carcinomas in-vading the bones of the maxillofacial skele-ton and skull. The disadvantages anddangers of a nonsurgical approach to theeradication of these malignancies are dis-cussed. It is concluded that the logicaltreatment of the resectable lesion is widemonobloc excision and, when indicated,regional lymph-node dissection in conti-nuity. The deformities which result fromresections including multiple vital struc-tures become the responsibility of thesurgeon who must plan the reconstructivesurgery as an inseparable part of the treat-ment to effect satisfactory rehabilitation ofthe patient.
References1. Bodenham, D. C.: Malignant Disease-Some
Problems of Diagnosis and Initial Manage-ment. Brit. J. Plastic Surg., 4:173, 1951-1952.
2. Campbell, E., B. M. Volk and C. W. Burk-land: Total Resection of the Temporal Bonefor Malignancies of the Middle Ear. Ann.Surg., 134:397, 1951.
3. Coleman, C. C., Jr. and A. Khuri: A Ra-tional Treatment of Advanced Cancer of theExternal Ear and Temporal Bone. Va. Med.Month., 86:21, 1959.
4. Coleman, C. C., Jr.: Scalp Flap Reconstructionin Head and Neck Cancer Patients. Plas-tic and Reconstruct. Surg., 24:45, 1959.
5. Conley, J. J. and A. J. Novack: SurgicalTreatment of Malignant Tumors of the Earand Temporal Bone. Arch. Otolaryngol., 71:635, 1960.
6. Conway, H.: Tumors of the Skin. Charles CThomas, Springfield, Ill., 1956.
7. Copeland, M.: An Evaluation of Neck Dis-section Associated with Other Radical Pro-cedures for the Treatment of Cancer in theHead and Neck. Ann. Surg., 141:910, 1955.
8. Figi, F. A. and P. Wiseman: Cancer andChemodectomas of the Middle Ear andMastoid. J. A. M. A., 156:1157, 1954.
9. Franklin-Bishop, B. W.: The Problems ofOver-Radiation. Brit. J. Plastic Surg., 13:354, 1961.
10. Fredricks, S.: External Ear Malignancy. Brit.J. Plastic Surg., 9:136, 1956.
11. Gaisford, J. D., D. C. Hanna and A. F. Susen:Major Resections of the Scalp and Skull forCancer with Immediate Complete Recon-struction. Plastic and Resonstruct. Surg.,21:335, 1958.
12. Lewis, J. S.: Cancer of the Ear. Laryngo-scope, 70:551, 1960.
13. Lewis, S. R., T. G. Blocker and G. G. Eade:Problem of Scalp Reconstruction. Plasticand Reconstruct. Surg., 20:133, 1957.
14. Martin, H., D. Del Valle, H. Erlich and W. G.Cokes: Neck Dissection, Cancer, 4:441,1951.
15. Mclndoe, A.: Brit. J. Med., 2:171, 1956.16. Moore, F. T. and T. Faulkner: Plastic Sur-
gery in Malignant Disease of the Head andNeck. Brit. J. Plastic Surg., 7:123, 1945-55.
17. New, G. B. and J. B. Erich: Pedicle Flaps inPlastic Surgery of the Head and Neck.Springfield, Ill., Charles C Thomas, 1950.
18. Parson, H. and J. S. Lewis: Subtotal Resec-tion of the Temporal Bone for Cancer ofthe Ear. Cancer, 7:995, 1954.
19. Tabb, H. G.: Carcinoma of the Antrum. TheLaryngoscope, 67:269, 1957.
20. Ward and Hendrick: Tumors of the Head andNeck. Baltimore, Williams and Wilkins,1950.