Embed Size (px)
Citation preview
CANCER, TRATAMIENTO Y CANCER, TRATAMIENTO Y TRABAJO/TRABAJO/QoLQoLTRABAJO/TRABAJO/QoLQoL
J i C téJavier CortésHospital Vall d´Hebron
H it l Q i óHospital QuirónBarcelona
Visibility of Cancer Survivorshipat the (Inter) National Levelat the (Inter) National Level
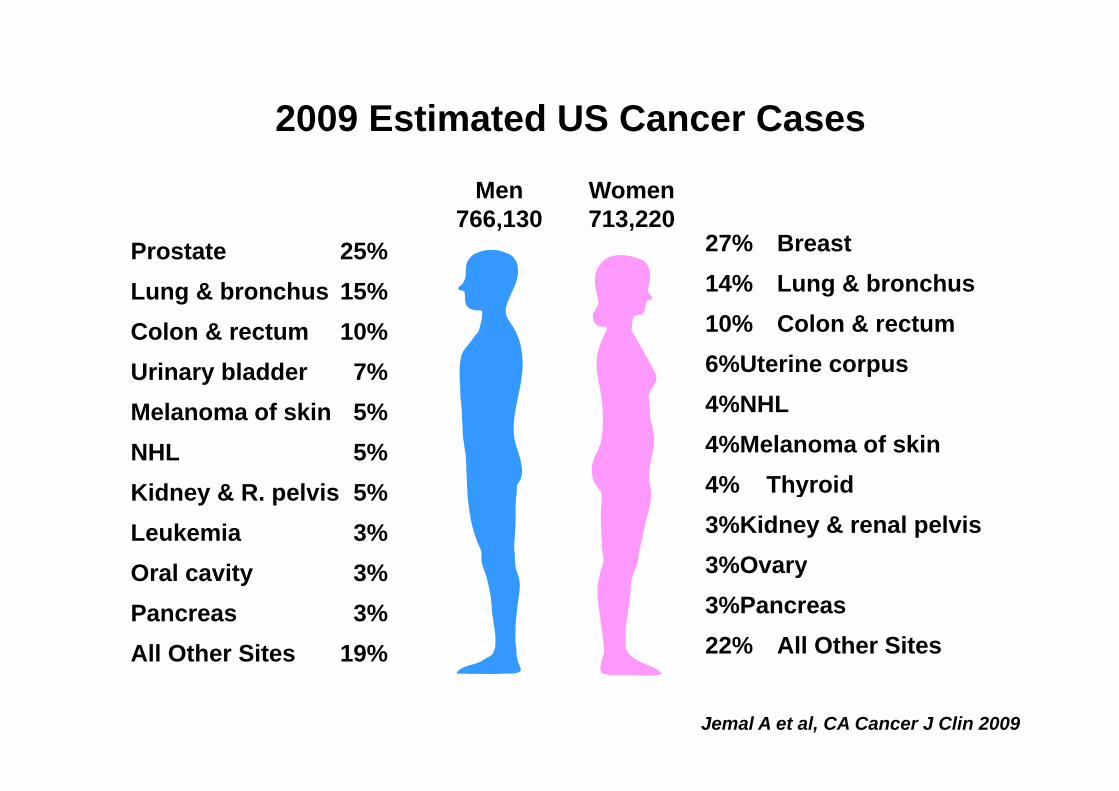
2009 Estimated US Cancer Cases2009 Estimated US Cancer Cases
Women713 220
Men766 130 713,220
27% Breast14% Lung & bronchus
Prostate 25%Lung & bronchus 15%
766,130
10% Colon & rectum6%Uterine corpus 4%NHL
Colon & rectum 10%Urinary bladder 7%
4%NHL4%Melanoma of skin4% Thyroid
Melanoma of skin 5%NHL 5% Kid & R l i 5% 4% Thyroid
3%Kidney & renal pelvis3%Ovary
Kidney & R. pelvis 5%Leukemia 3%Oral cavity 3% y
3%Pancreas22% All Other Sites
Oral cavity 3%Pancreas 3%All Other Sites 19%
Jemal A et al, CA Cancer J Clin 2009
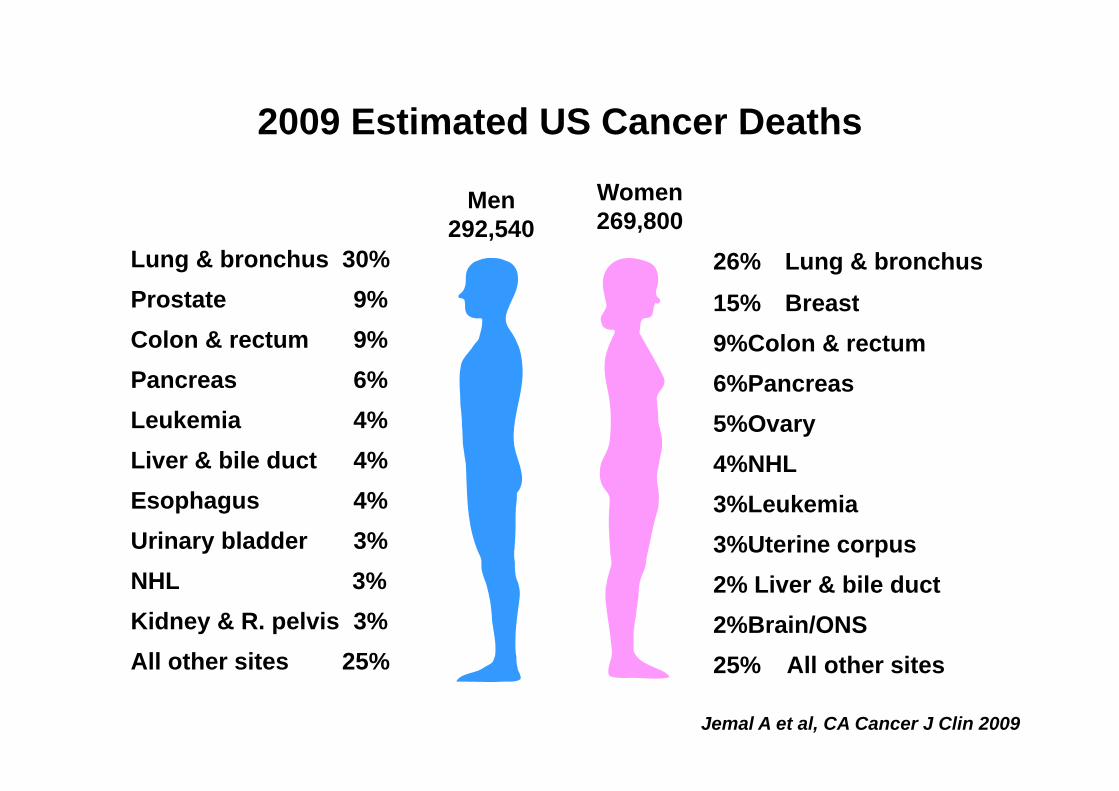
2009 Estimated US Cancer Deaths2009 Estimated US Cancer Deaths
Men Women269 800292,540 269,800
26% Lung & bronchus
15% Breast
Lung & bronchus 30%Prostate 9% 15% Breast
9%Colon & rectum6%Pancreas
Prostate 9%Colon & rectum 9%Pancreas 6%
5%Ovary4%NHL
Leukemia 4%Liver & bile duct 4%
3%Leukemia3%Uterine corpus
Esophagus 4%Urinary bladder 3% NHL 3% 2% Liver & bile duct
2%Brain/ONS25% All other sites
NHL 3% Kidney & R. pelvis 3%All other sites 25% 25% All other sitesAll other sites 25%
Jemal A et al, CA Cancer J Clin 2009
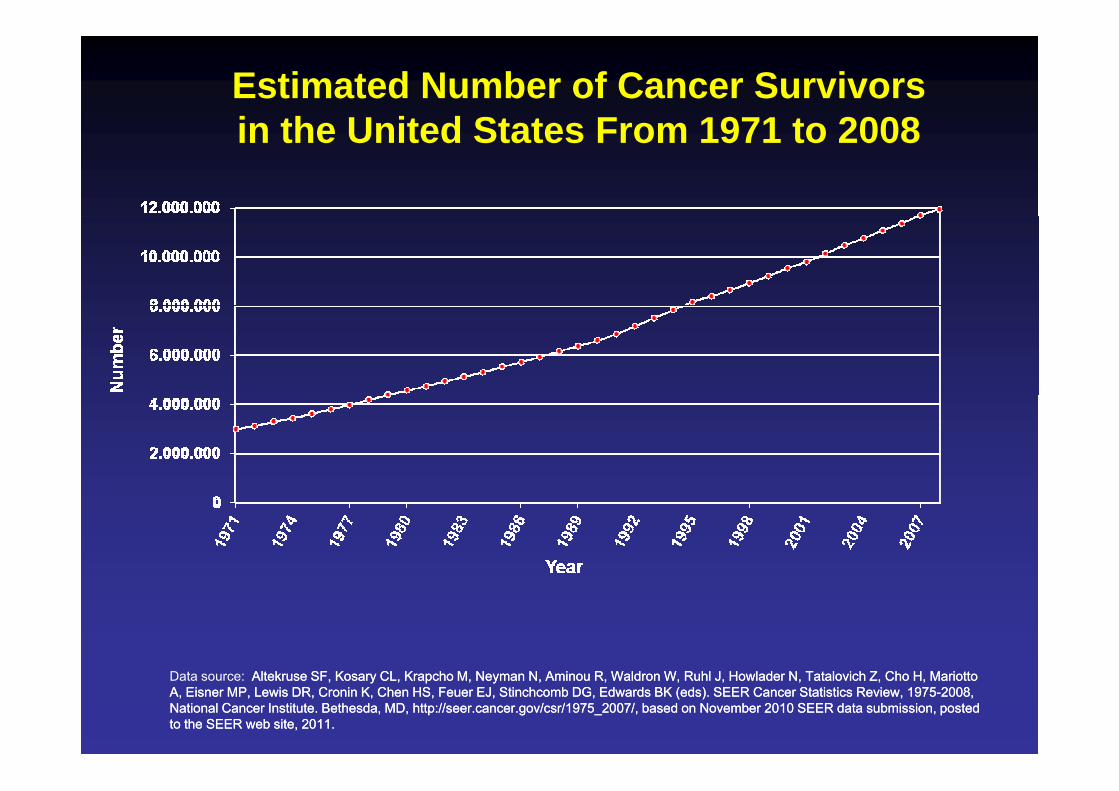
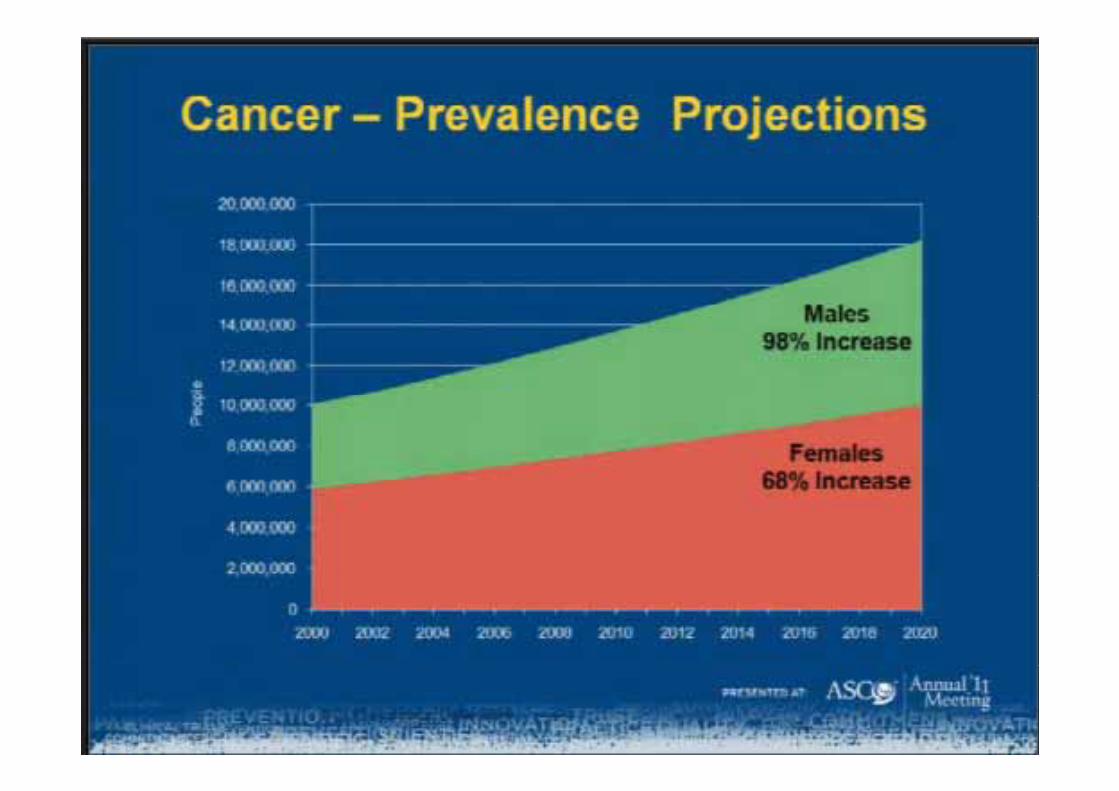
Estimated Number of Cancer Survivors in the United States From 1971 to 2008in the United States From 1971 to 2008
Data source: AltekruseAltekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, HowladerHowlader N, N, TatalovichTatalovich Z, Cho H, Mariotto Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK (A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK (edseds). SEER Cancer Statistics Review, 1975). SEER Cancer Statistics Review, 1975--2008, 2008, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2007/, based on November 2010 SEER data submission, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2007/, based on November 2010 SEER data submission, posposted ted to the SEER web site, 2011.to the SEER web site, 2011.
*Age-adjusted to the 2000 US standard population and adjusted for delays in reporting.Source: Surveillance, Epidemiology, and End Results Program, Delay-adjusted Incidence database:
SEER Incidence Delay-adjusted Rates, 9 Registries, 1975-2005, National Cancer Institute, 2008.
*Age-adjusted to the 2000 US standard population and adjusted for delays in reporting.Source: Surveillance, Epidemiology, and End Results Program, Delay-adjusted Incidence database:
SEER Incidence Delay-adjusted Rates, 9 Registries, 1975-2005, National Cancer Institute, 2008.
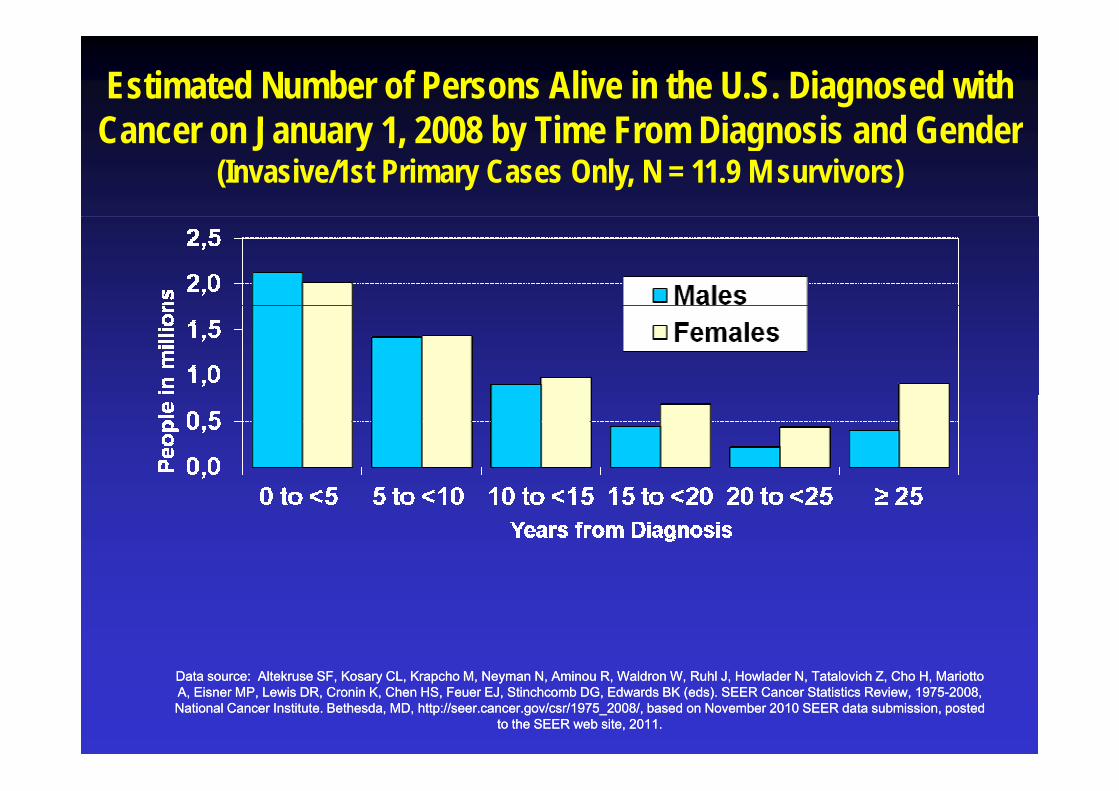
Estimated Number of Persons Alive in the U.S. Diagnosed with Cancer on January 1 2008 by Time From Diagnosis and GenderCancer on January 1, 2008 by Time From Diagnosis and Gender
(Invasive/1st Primary Cases Only, N = 11.9 M survivors)
Data source: Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, Howlader N, Tatalovich Z, Cho H, MarData source: Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, Howlader N, Tatalovich Z, Cho H, Mariotiotto to A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK (eds). SEER Cancer Statistics Review, 1975A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK (eds). SEER Cancer Statistics Review, 1975--2008, 2008, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posposted ted
to the SEER web site, 2011.to the SEER web site, 2011.
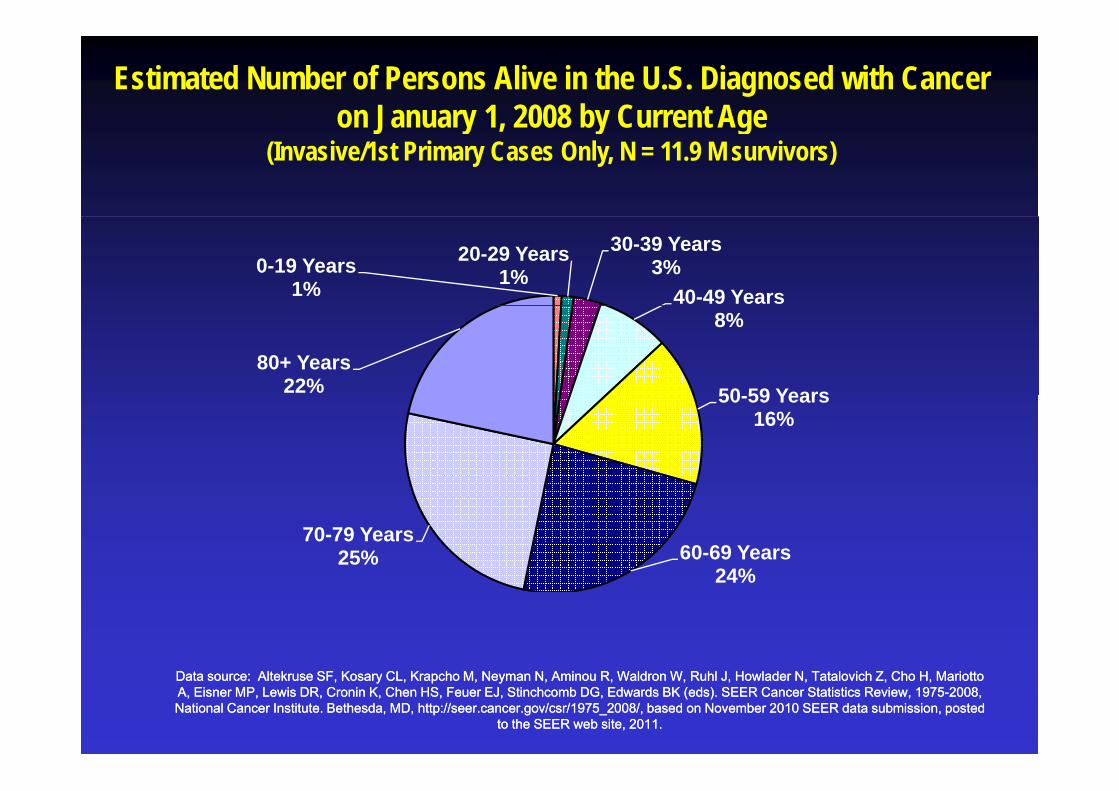
Estimated Number of Persons Alive in the U.S. Diagnosed with Cancer on January 1, 2008 by Current Age on January 1, 2008 by Current Age
(Invasive/1st Primary Cases Only, N = 11.9 M survivors)
0-19 Years 1%
20-29 Years 1%
30-39 Years3%
40-49 Years8%
50 59 Years80+ Years
22% 50-59 Years16%
60-69 Years 24%
70-79 Years25%
24%
Data source: Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, Howlader N, Tatalovich Z, Cho H, MarData source: Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, Howlader N, Tatalovich Z, Cho H, Mariotiotto to A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK (eds). SEER Cancer Statistics Review, 1975A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK (eds). SEER Cancer Statistics Review, 1975--2008, 2008, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posposted ted
to the SEER web site, 2011.to the SEER web site, 2011.
Lessons Learned…
Lesson # 1:Lesson # 1:Post-treatment/survivorship phase brings its own set of unique needs
and challengesg
Persistent or ChronicChronic Effects of Cancer Treatment
• Physical/Medical (e.g., fatigue, pain, memory problems, lymphedema, sexual impairment, p , y p , p ,incontinence)
• Psychological (e g depression anxiety uncertainty • Psychological (e.g., depression, anxiety, uncertainty, isolation, altered body image)
S i l ( h i i t l l ti hi • Social (e.g., changes in interpersonal relationships, concerns regarding health or life insurance, job lock/loss return to school financial burden)lock/loss, return to school, financial burden)
• Existential and Spiritual Issues (e.g., altered sense of p rpose or meaning appreciation of life)of purpose or meaning, appreciation of life)
Cancer Survivors at Increased Risk for LateLate Effects
Disease recurrence/ new cancersDisease recurrence/ new cancers (>756K multiple ca; 16% of new diagnoses)*diagnoses)Cardiovascular diseaseOb it /Di b tObesity/DiabetesOsteoporosis Functional declinePoor quality of lifePoor quality of life
* Mariotto et al., CEBP 2007
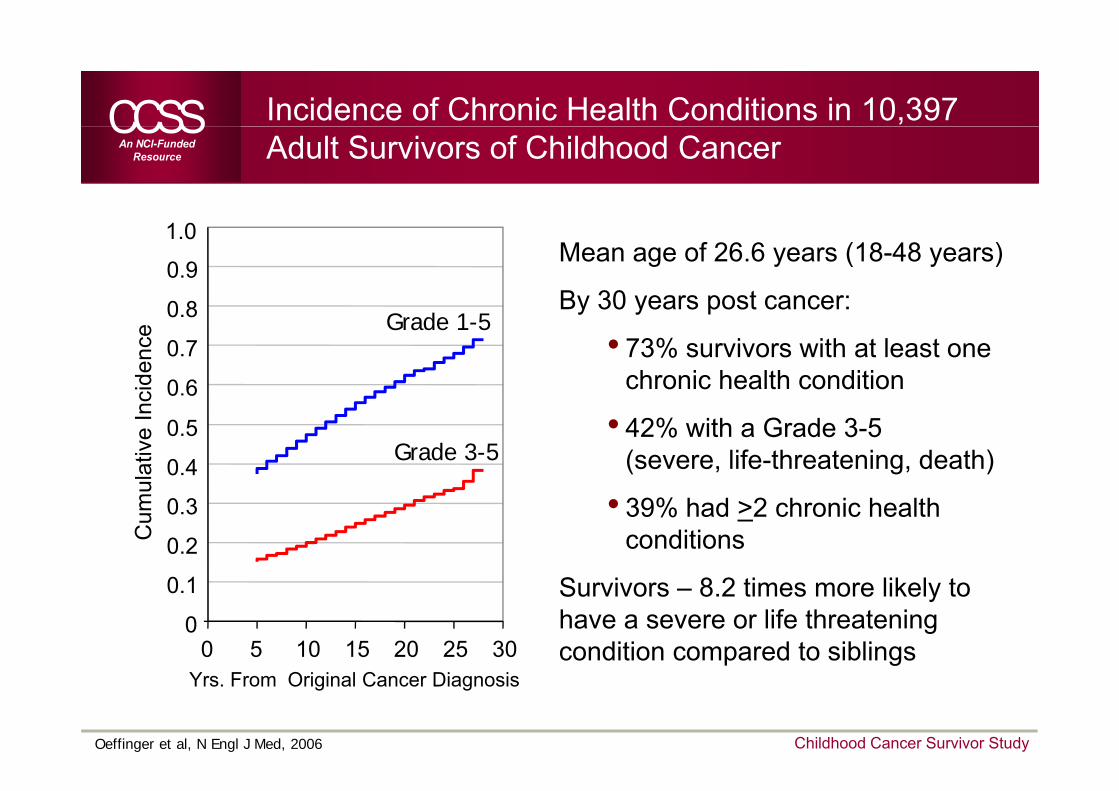
Incidence of Chronic Health Conditions in 10,397 Adult Survivors of Childhood Cancer
0 8
0.9
1.0Mean age of 26.6 years (18-48 years)
By 30 years post cancer:
0.6
0.7
0.8
cide
nce Grade 1-5
By 30 years post cancer:
• 73% survivors with at least one chronic health condition
0.4
0.5
0 6
ulat
ive
Inc
Grade 3-5• 42% with a Grade 3-5
(severe, life-threatening, death)
0.2
0.3
Cum
u • 39% had >2 chronic health conditions
0
0.1
0 5 10 15 20 25 30
Survivors – 8.2 times more likely to have a severe or life threatening condition compared to siblings
Oeffinger et al, N Engl J Med, 2006
Yrs. From Original Cancer Diagnosisp g
Childhood Cancer Survivor Study
Lesson # 2:Lesson # 2:Intervening early (when problems arise)
leads to better outcomes
Lesson # 3:Lesson # 3:Cancer for many may provide a
‘teachable moment’ in particular with respect to lifestyle ---in particular with respect to lifestyle
and health behaviors
Wh th i t t i S i ’Why the interest in Survivors’ Health Behaviors?
Growing number of cancer survivors who… 1. Are living longer1. Are living longer2. Are older, and also aging3 Are at risk for a number of co-morbid health 3. Are at risk for a number of co-morbid health
conditions (and may also have a history of others))
4. Often gain wt, stop exercising during Rx5 Are asking for help in reducing cancer-related 5. Are asking for help in reducing cancer related
morbidity and mortality6 Can benefit from health promoting inventions6. Can benefit from health promoting inventions
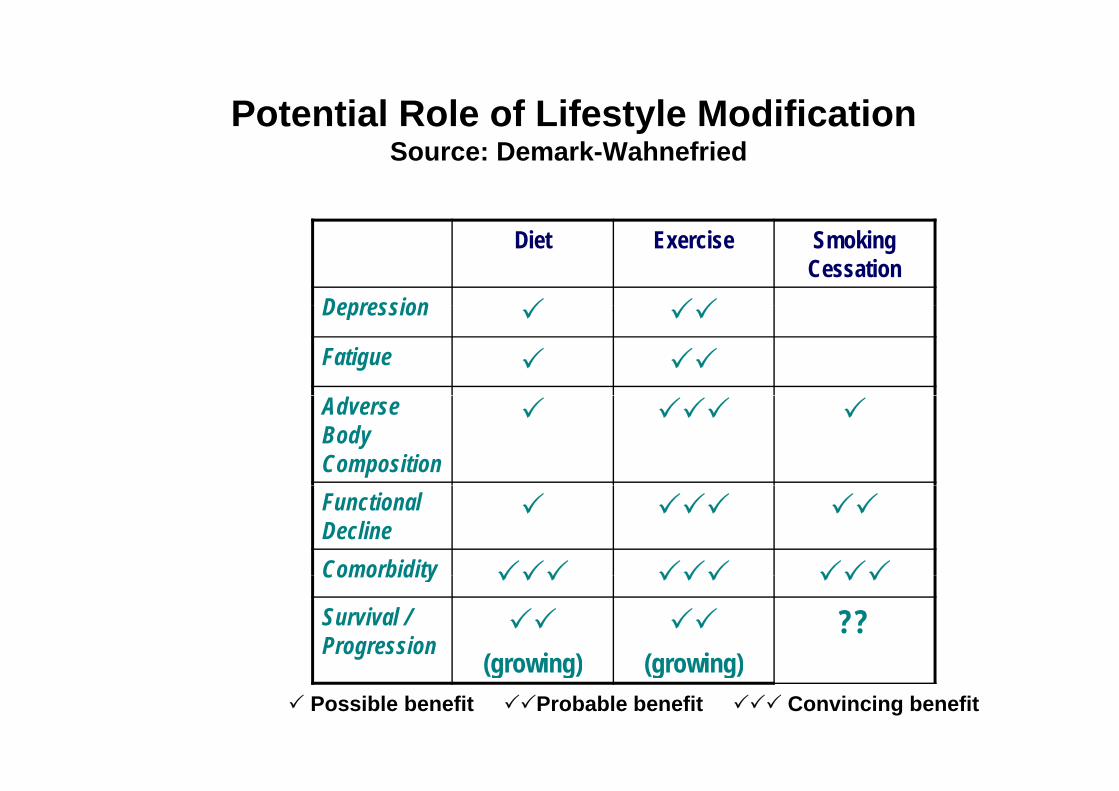
Potential Role of Lifestyle Modification ote t a o e o esty e od cat oSource: Demark-Wahnefried
Diet Exercise Smoking Cessation
DepressionDepression
Fatigue
Adverse Body CompositionFunctional DeclineComorbidityComorbidity
Survival / Progression (growing) (growing)
??(growing) (growing)
Possible benefit Probable benefit Convincing benefit
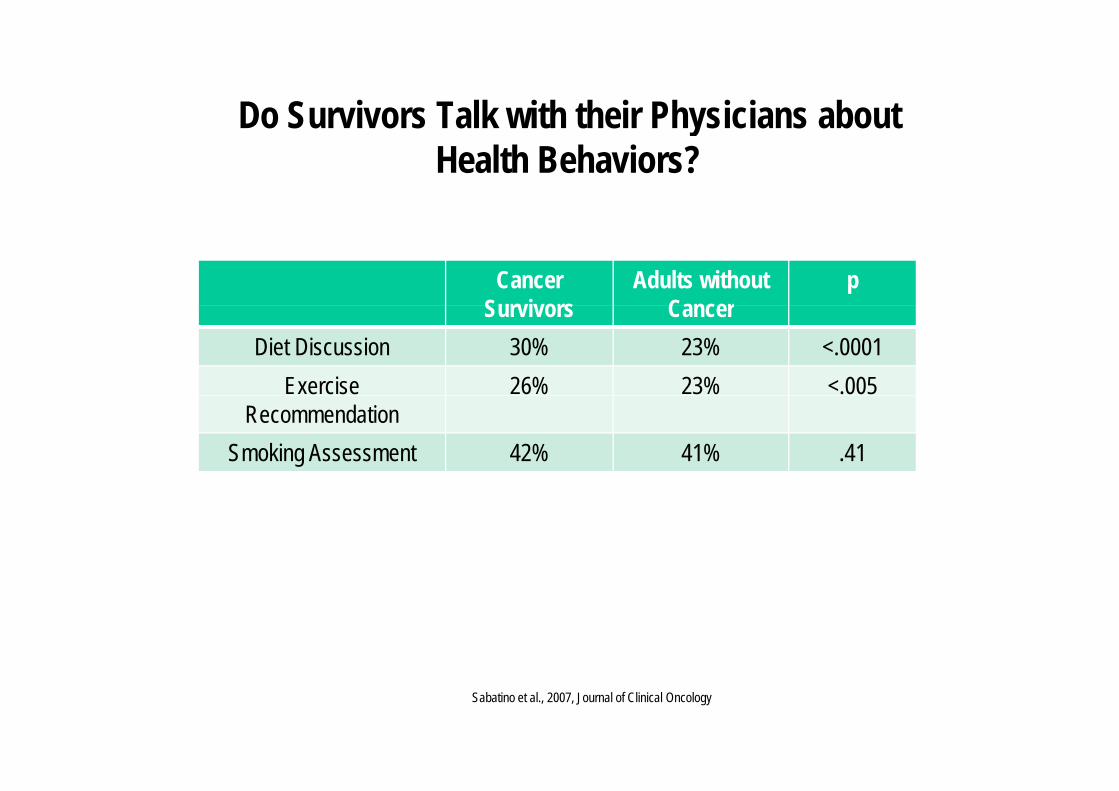
Do Survivors Talk with their Physicians about Do Survivors Talk with their Physicians about Health Behaviors?
Cancer Survivors
Adults without Cancer
pSurvivors Cancer
Diet Discussion 30% 23% <.0001Exercise 26% 23% <.005
RecommendationSmoking Assessment 42% 41% .41
Sabatino et al., 2007, Journal of Clinical Oncology
Lost in Transition!…
Patients report feeling ‘abandoned’ and ‘at sea’ at abandoned and at sea at the end of therapy
Many complete treatment Many complete treatment with persistent problems
Planning for recovery is Planning for recovery is important!
Selected Recommendations from the President’sSelected Recommendations from the President s Cancer Panel & IOM Reports
• When treatment ends, all survivors should ,receive a summary record that includes important disease characteristics and treatments received.
• In addition, they should be provided with a f ll l i ti il blfollow-up care plan incorporating available evidence-based standards of care.
S i hi l iSurvivorship care planning
• What care should be provided?• When and where is this done?•• Who should provide what care to whom? Who should provide what care to whom?
(Oncologists, PCP, CNP); role of medical (Oncologists, PCP, CNP); role of medical homes?homes?homes?homes?
• What impact does this care planning have onon• patient behavior• physician behaviorp y• practice costs/processes and payor investment • patient health outcomes (morbidity & mortality)
Physician roles in survivorship care:Physician roles in survivorship care: perspectives of oncologists and primary
care physicianscare physicians
ObjectivesCharacterize U.S. Primary Care Physicians’ and Oncologists’
b li f k l d ttit d d ti l t d t th
Objectives
beliefs, knowledge, attitudes and practices related to the care of cancer survivors
Main areas of interest (defined by IOM):( y )– Prevention and detection of new and recurring cancers, and medical
and psychosocial late effects– Interventions to manage the consequences of cancer and its– Interventions to manage the consequences of cancer and its
treatment– Coordination of care between cancer specialists and primary care
providers to meet survivors’ health needsproviders to meet survivors health needsFocus on breast and colorectal cancer survivor care
MethodsMethods
Nationally representative sample of U.S. physiciansy y– Medical oncologists (Oncology/Hematology specialists)– PCPs (Internal Medicine, Family Practice)
• Small sample of OB/GYN physicians• Small sample of OB/GYN physiciansEligibility criteria
– Non-federal practice settings– Age < 76– Oncologists: provision of care for breast or colon cancer patients– PCPs: Office-based practice ≥ 20% time in clinical carePCPs: Office based practice, ≥ 20% time in clinical care
Systematic stratified sampling: specialty, census region, metropolitan status, age, sex from the AMA Masterfile
Mode: self-administered mail survey, $50 incentiveOverall response rate = 58%: 1,130 Oncologists, 1,032 PCPs
DomainsDomains
Perceptions and attitudesPerceptions and attitudes– Perceived competence in caring for cancer survivors– Perceived roles and responsibilities of oncologists and PCPs in cancer survivor
carecare– Optimal care delivery models for cancer survivor care– Barriers to provision of optimal care
P tiPractices– Surveillance testing for recurrent cancer– Coordination of care between oncologists and PCPs– Use of survivorship care plans, treatment summaries
Knowledge– Long-term or late effects of cancer treatmentg
Physician and practice characteristics
Perceptions and attitudes:Perceptions and attitudes:Skills and responsibilities in cancer survivor
carecare
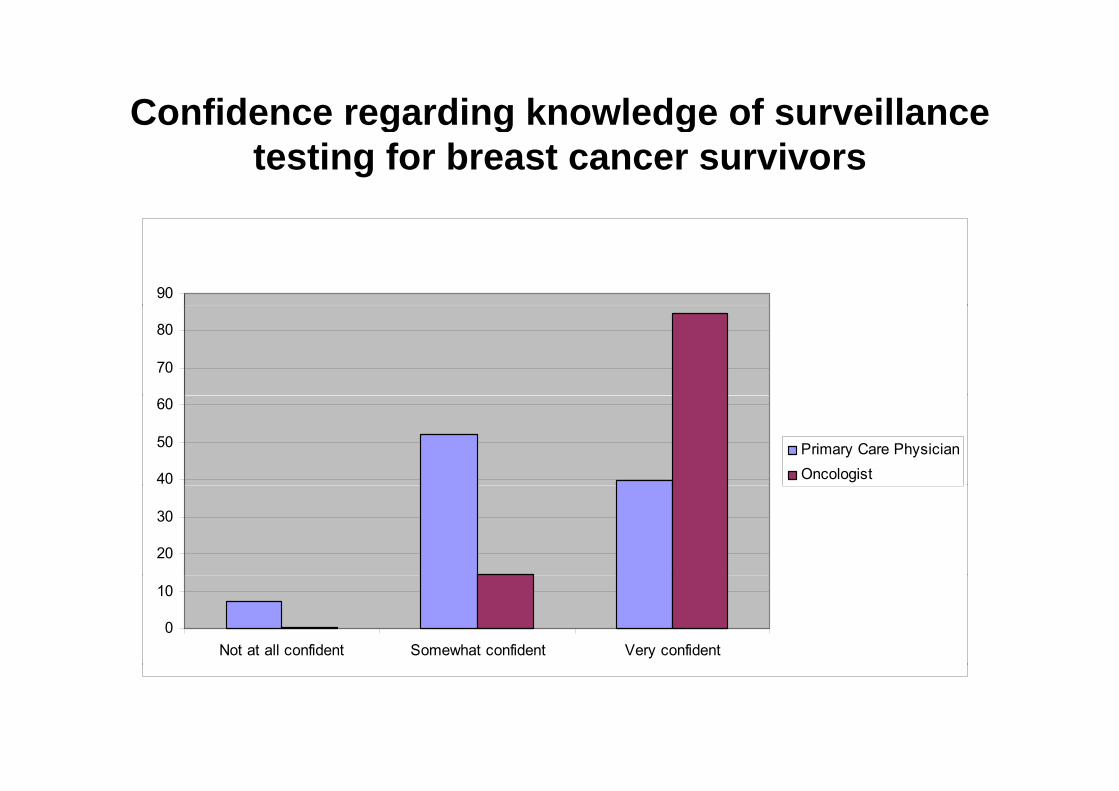
Confidence regarding knowledge of surveillance g g gtesting for breast cancer survivors
90
70
80
40
50
60
Primary Care PhysicianOncologist
20
30
0
10
Not at all confident Somewhat confident Very confident
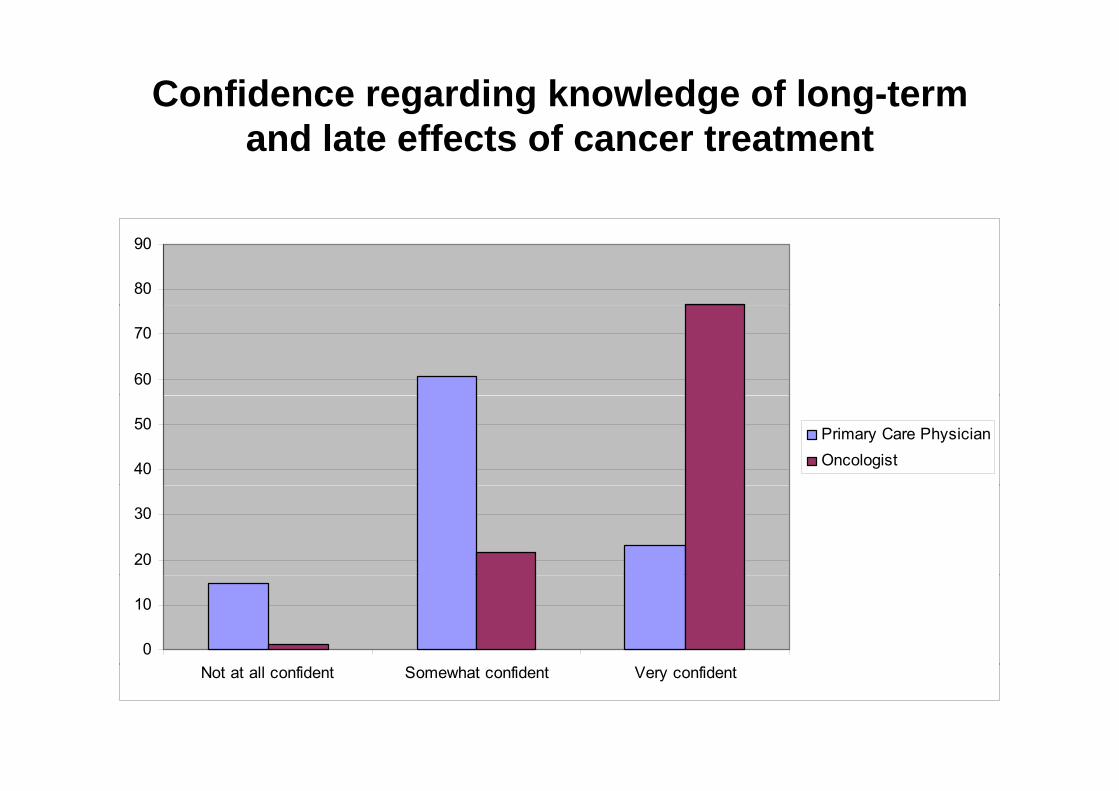
Confidence regarding knowledge of long-term d l t ff t f t t tand late effects of cancer treatment
80
90
60
70
40
50 Primary Care PhysicianOncologist
20
30
0
10
Not at all confident Somewhat confident Very confident
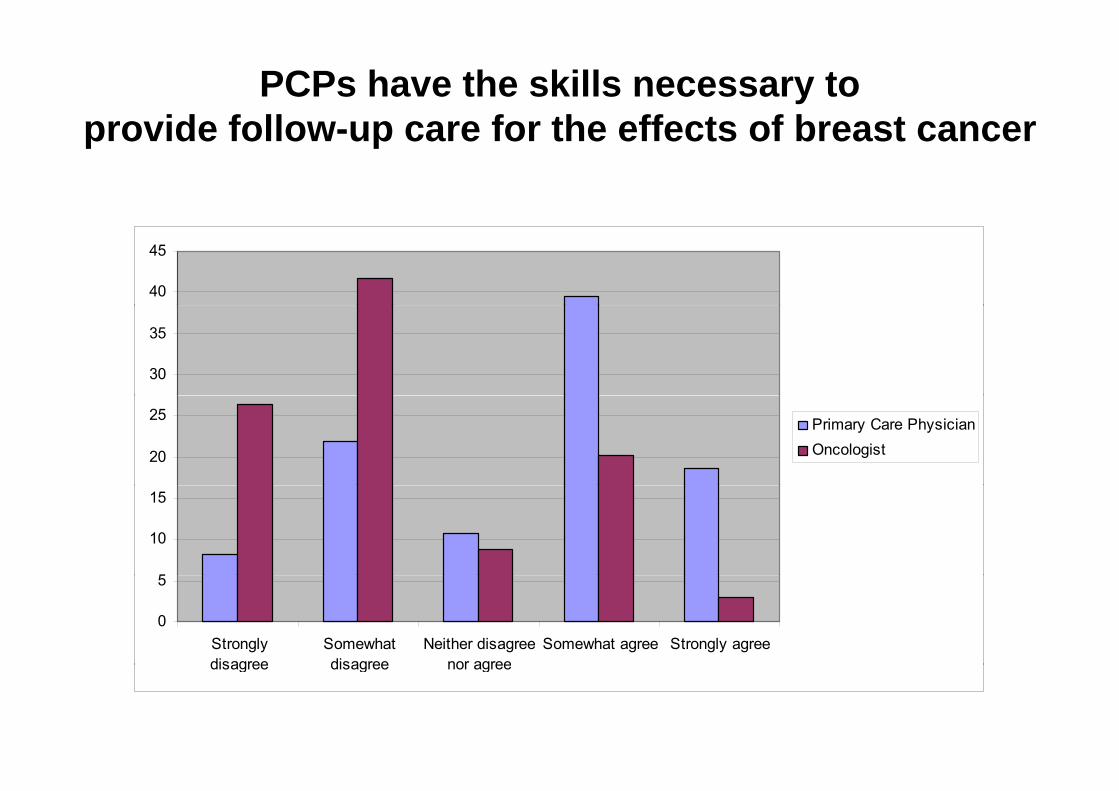
PCPs have the skills necessary to provide follow up care for the effects of breast cancerprovide follow-up care for the effects of breast cancer
40
45
30
35
20
25 Primary Care PhysicianOncologist
5
10
15
0
5
Stronglydisagree
Somewhatdisagree
Neither disagreenor agree
Somewhat agree Strongly agreedisagree disagree nor agree
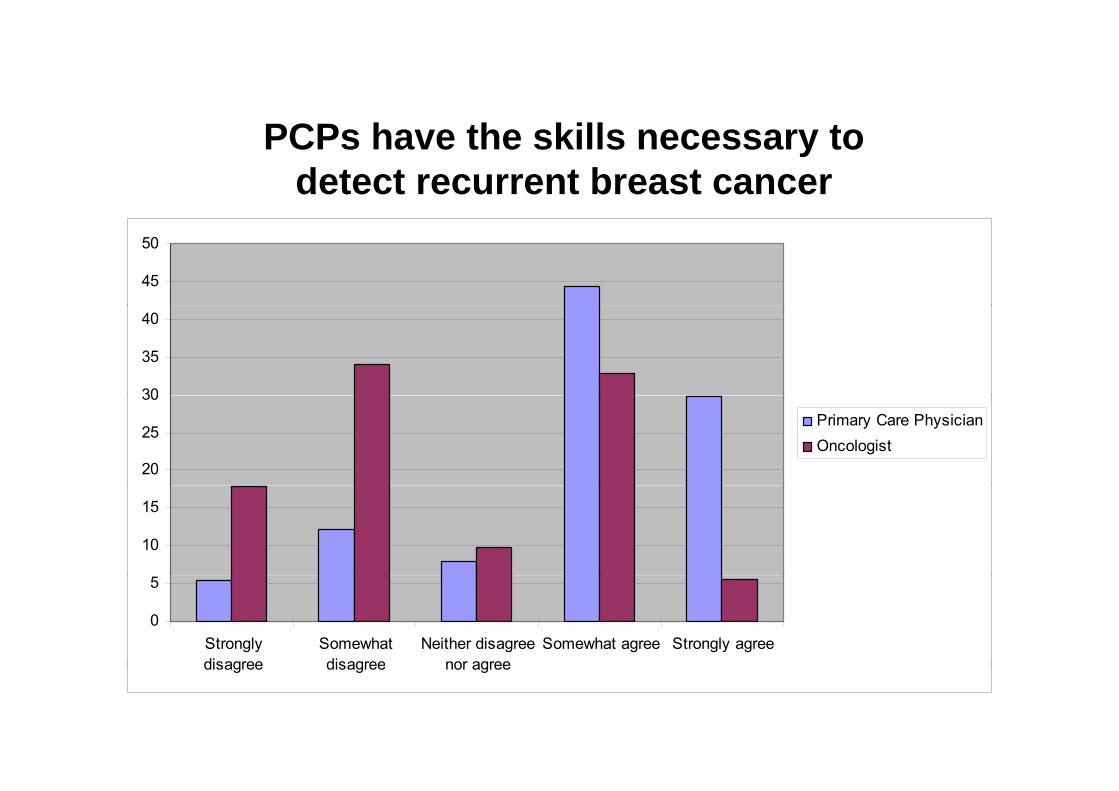
PCP h th kill tPCPs have the skills necessary to detect recurrent breast cancer
45
50
30
35
40
20
25
30Primary Care PhysicianOncologist
10
15
0
5
Stronglydisagree
Somewhatdisagree
Neither disagreenor agree
Somewhat agree Strongly agreedisagree disagree nor agree
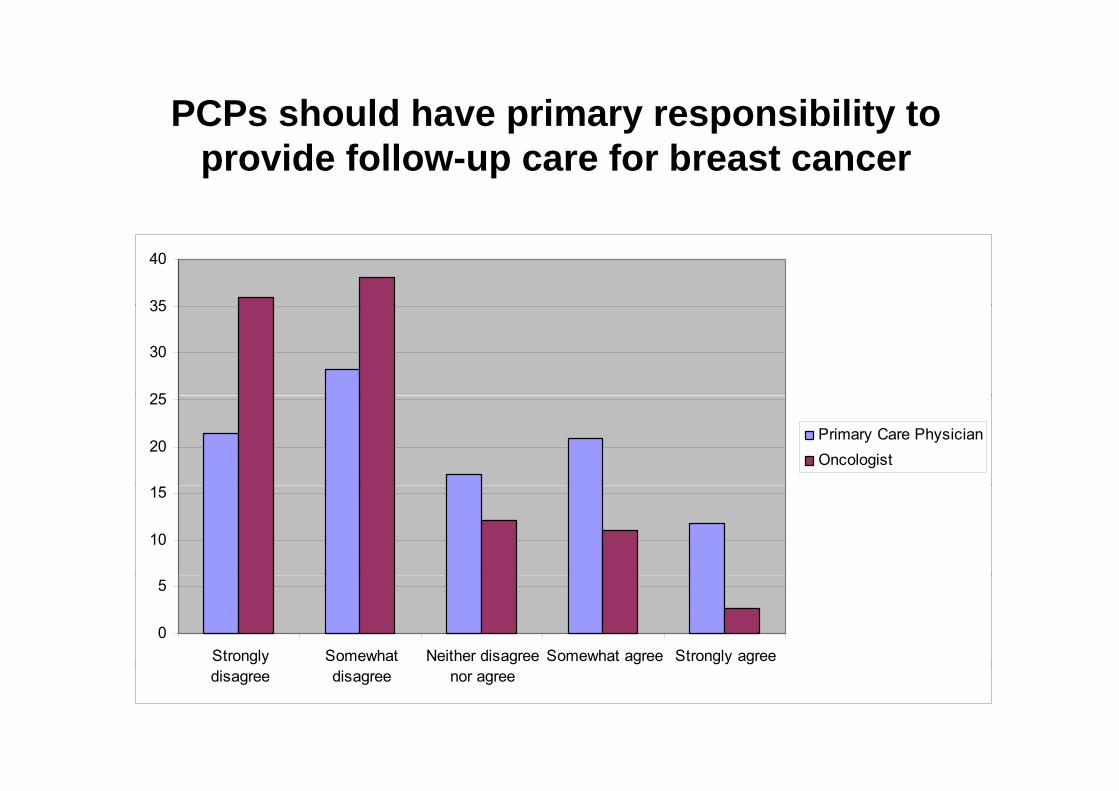
PCPs should have primary responsibility to C s s ou d a e p a y espo s b ty toprovide follow-up care for breast cancer
35
40
25
30
35
20
25
Primary Care PhysicianOncologist
10
15
0
5
Strongly Somewhat Neither disagree Somewhat agree Strongly agreedisagree disagree nor agree
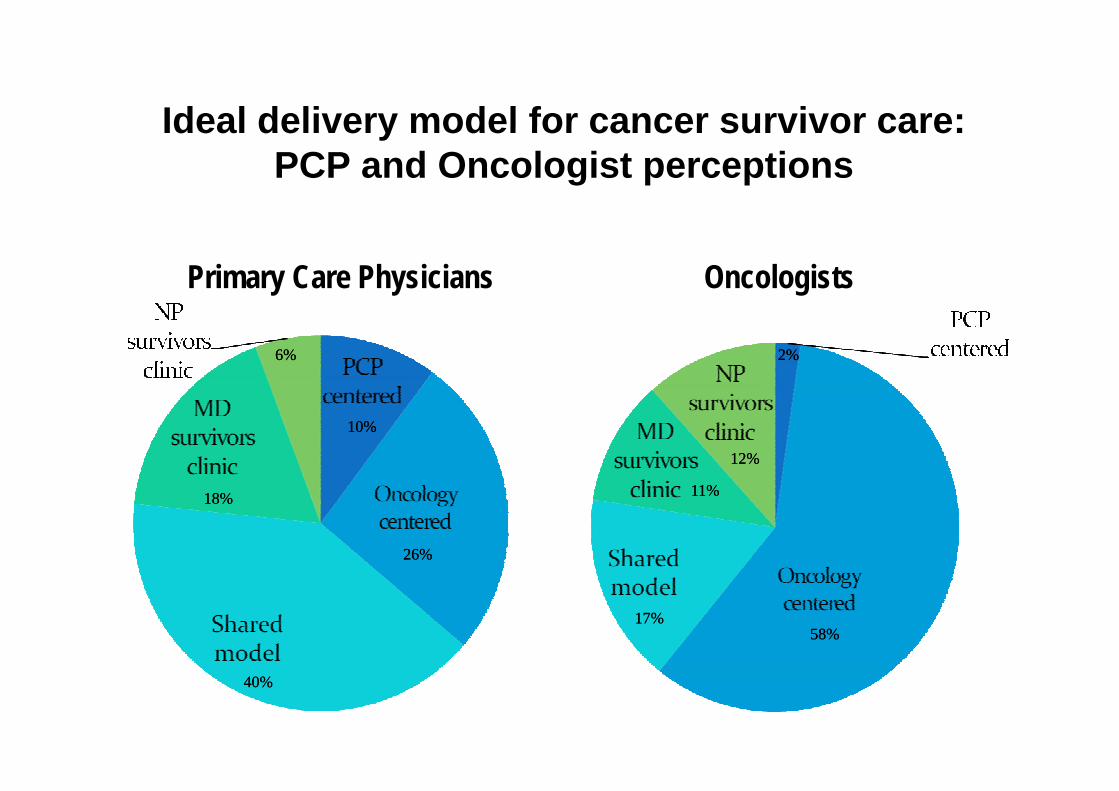
Ideal delivery model for cancer survivor care:Ideal delivery model for cancer survivor care: PCP and Oncologist perceptions
Primary Care Physicians Oncologists
6%6% 2%2%
10%10%
11%11%
12%12%
26%26%
18%18% 11%11%
58%58%17%17%
40%40%
Practices: Coordination of care
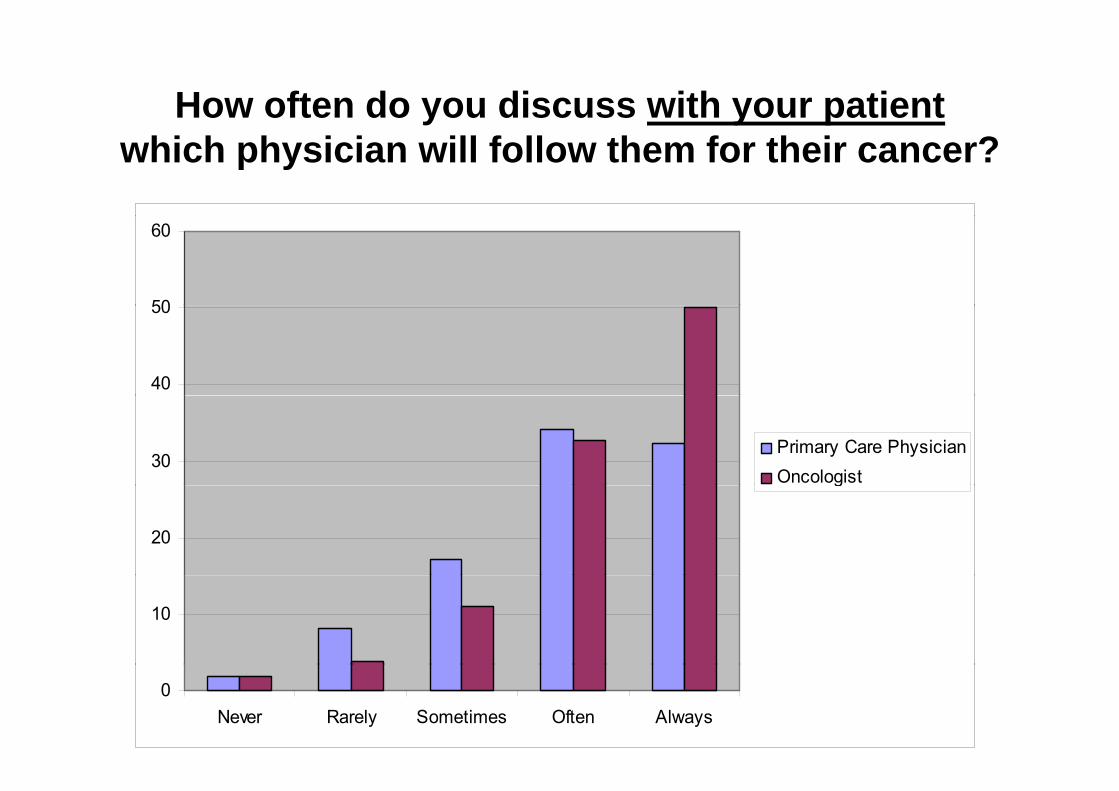
How often do you discuss with your patientwhich physician will follow them for their cancer?
50
60
40
50
30Primary Care PhysicianOncologist
20
g
10
0Never Rarely Sometimes Often Always
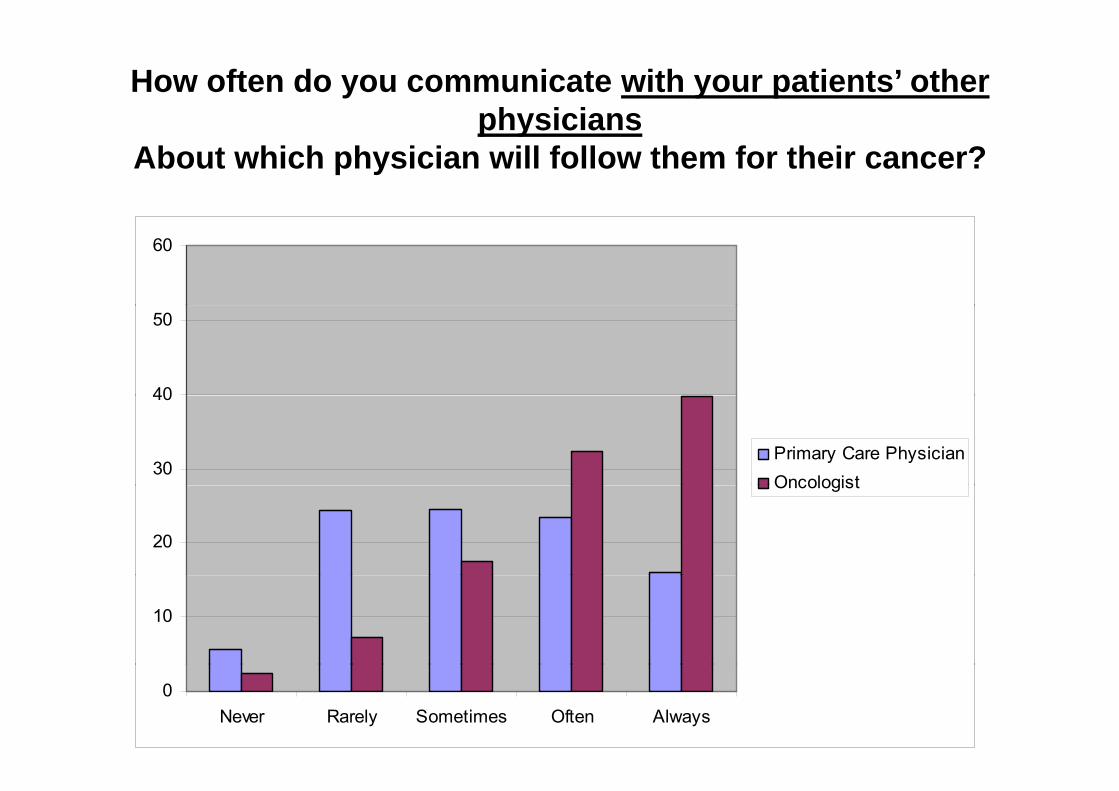
How often do you communicate with your patients’ other physiciansphysicians
About which physician will follow them for their cancer?
60
40
50
30
40
Primary Care PhysicianOncologist
20
Oncologist
10
0Never Rarely Sometimes Often Always
Practices: Use of survivorship care plans
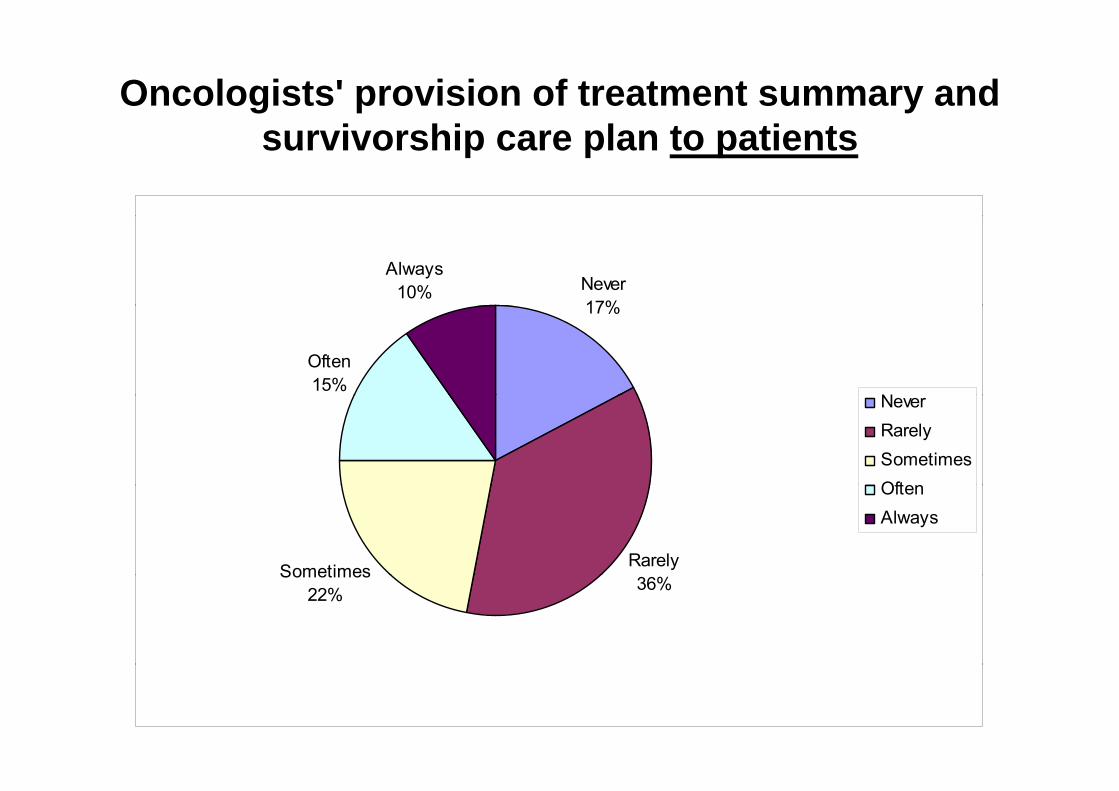
Oncologists' provision of treatment summary and i hi l t ti tsurvivorship care plan to patients
Never17%
Always10%
17%
Often15%
NNeverRarelySometimesOften
RarelySometimes
OftenAlways
36%Sometimes
22%
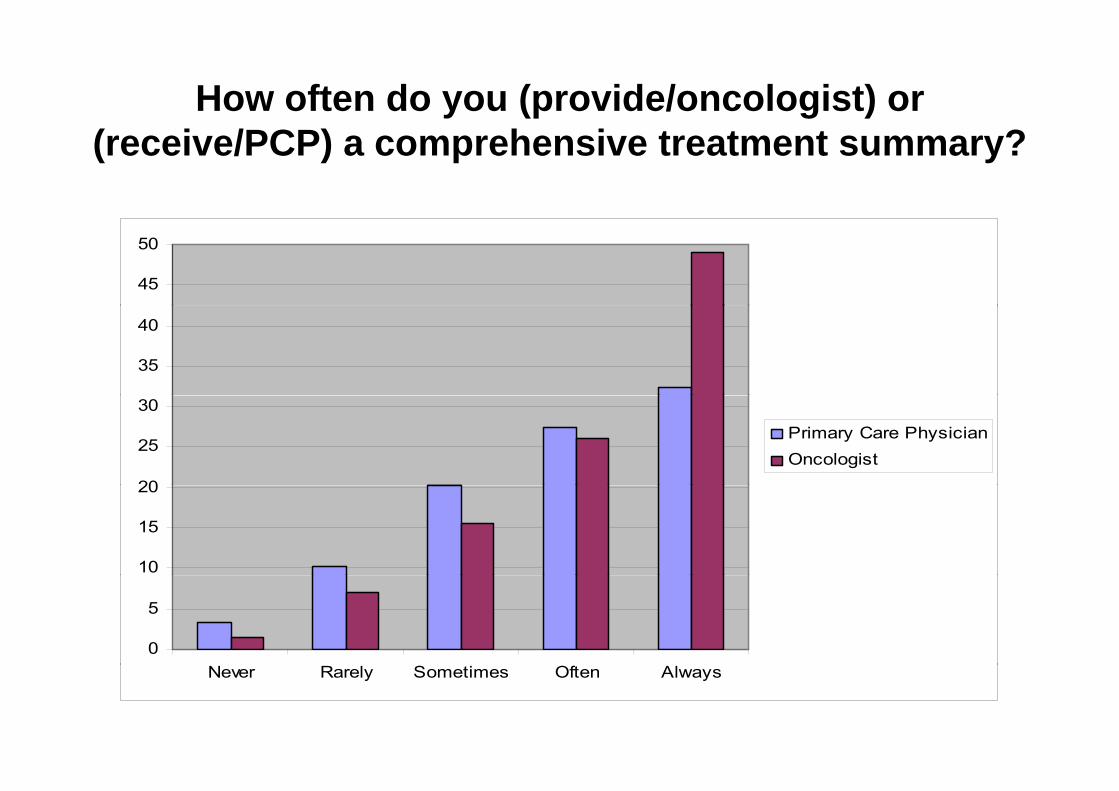
How often do you (provide/oncologist) or (receive/PCP) a comprehensive treatment summary?
45
50
35
40
20
25
30
Primary Care PhysicianOncologist
10
15
20
0
5
Never Rarely Sometimes Often Always
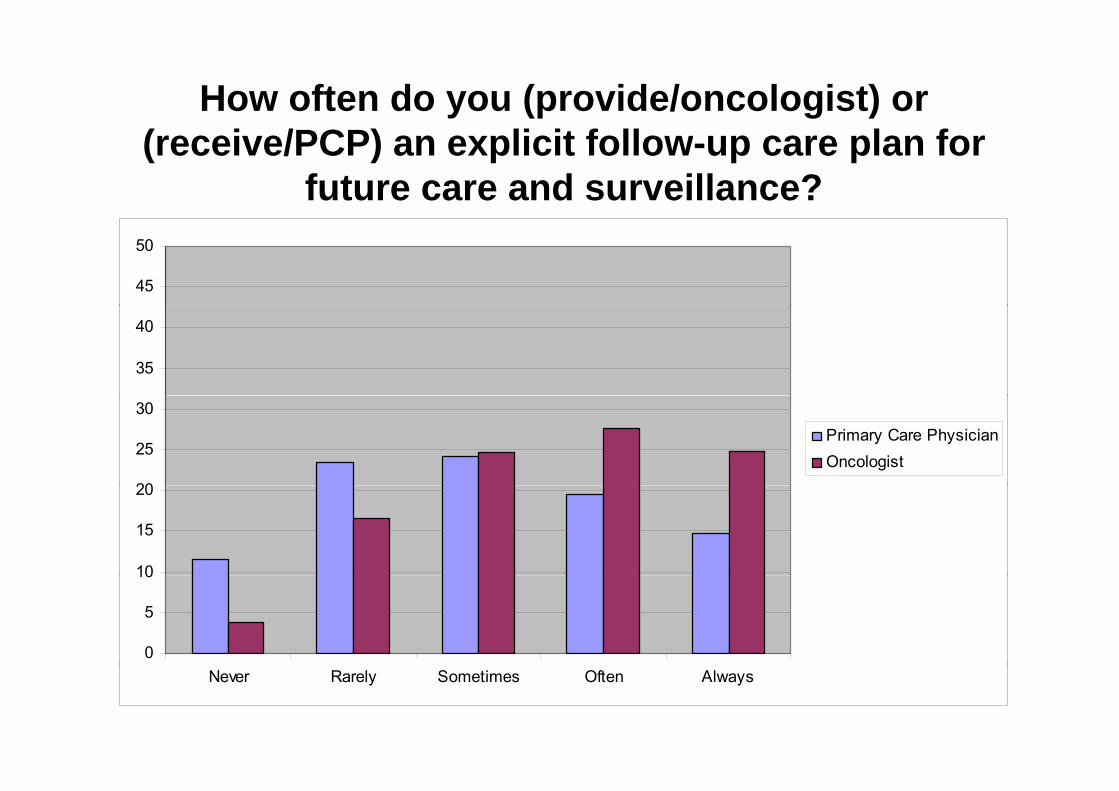
How often do you (provide/oncologist) or (receive/PCP) an explicit follow-up care plan for
future care and surveillance?
45
50
35
40
20
25
30Primary Care PhysicianOncologist
10
15
20
0
5
10
Never Rarely Sometimes Often Always
Survivorship care: whose job is it – and whose should it be?S l i
At a national level confidence in knowledge of the care of breast and
Some conclusions
At a national level, confidence in knowledge of the care of breast and colorectal cancer patients is low among PCPs
PCPs’ skill in caring for cancer survivors is rated low by oncologists, and ambivalently by PCPsambivalently by PCPs
A minority of physicians (both PCPs and oncologists) advocate primary PCP responsibility for cancer survivor care
M t PCP f h d l t d d l– Most PCPs favor shared or oncology-centered model– Most oncologists favor oncology-centered model
PCPs and oncologists report engaging in care coordination practices, but have divergent perceptions about the extent
– Communication about physician roles– Sharing of specific aspects of cancer survivor careg p p
Self-rated provision of treatment summaries / care plans is less than ideal– Provision to patients is relatively low– Provision to PCPs is higher but discordant perceptions among PCPsProvision to PCPs is higher, but discordant perceptions among PCPs
Applying Screening and InterventionApplying Screening and Intervention into Clinical PracticeDepression is merely anger without enthusiasm. ~ Depression is merely anger without enthusiasm. ~ Steven WrightSteven Wright
If you are physically sick you can elicit the interest of a battery of physicians; but if you are mentally sick you are lucIf you are physically sick you can elicit the interest of a battery of physicians; but if you are mentally sick you are luckykyIf you are physically sick, you can elicit the interest of a battery of physicians; but if you are mentally sick, you are lucIf you are physically sick, you can elicit the interest of a battery of physicians; but if you are mentally sick, you are lucky ky if the janitor comes around.if the janitor comes around. ~Martin H. Fischer~Martin H. Fischer
Is it Common?
Meta-Analysis – Mitchell et al 201170 studies 10 071 pts70 studies 10,071 ptsPrevalence any mood disorder – 38%NCCN G id liNCCN Guidelines“Clinicians should recognize, monitor, and
treat distress at all stages of cancer which requires screening for distress from the initial visit through the course of the disease andbeyond.”

A l i t i t i ?Are oncologists intervening?
Multi-institution cross sectional study [251/397 approached] showed that only 45% of those identified on screening in the study to have a major depressive illness had been referred for a
t l h lth imental health service.– - Kadan-Lottick NS Cancer 2005
A one study of 472 low income women with breast or gynecologic A one study of 472 low-income women with breast or gynecologic cancer, 12% of those with major depression were prescribed antidepressants and 5% received psychological treatment.
- Ell K J ClinOncol 2005Ell K J ClinOncol 2005
5,613 patients were consecutively screened in UK oncology outpatients, 8% major mood disorder. Reviewed 150 with major p , 8% j 50 jdepression, 1/3 had any medication, none adequate and no other mental health referrals.
– Sharpe et al Br J Cancer 2004
Intervention
Distress Sixth vital sign along with temperature, respiration, heart rate, blood pressure, and pain, respiration, heart rate, blood pressure, and pain, “as a core indicator of a patient’s health and well being” that all cancer professionals should be g a a ca ce p o ess o a s s ou dmeasure.– Bultz B and Carlson LE J ClinOncol 2005Bultz B and Carlson LE J ClinOncol 2005
Does it matter
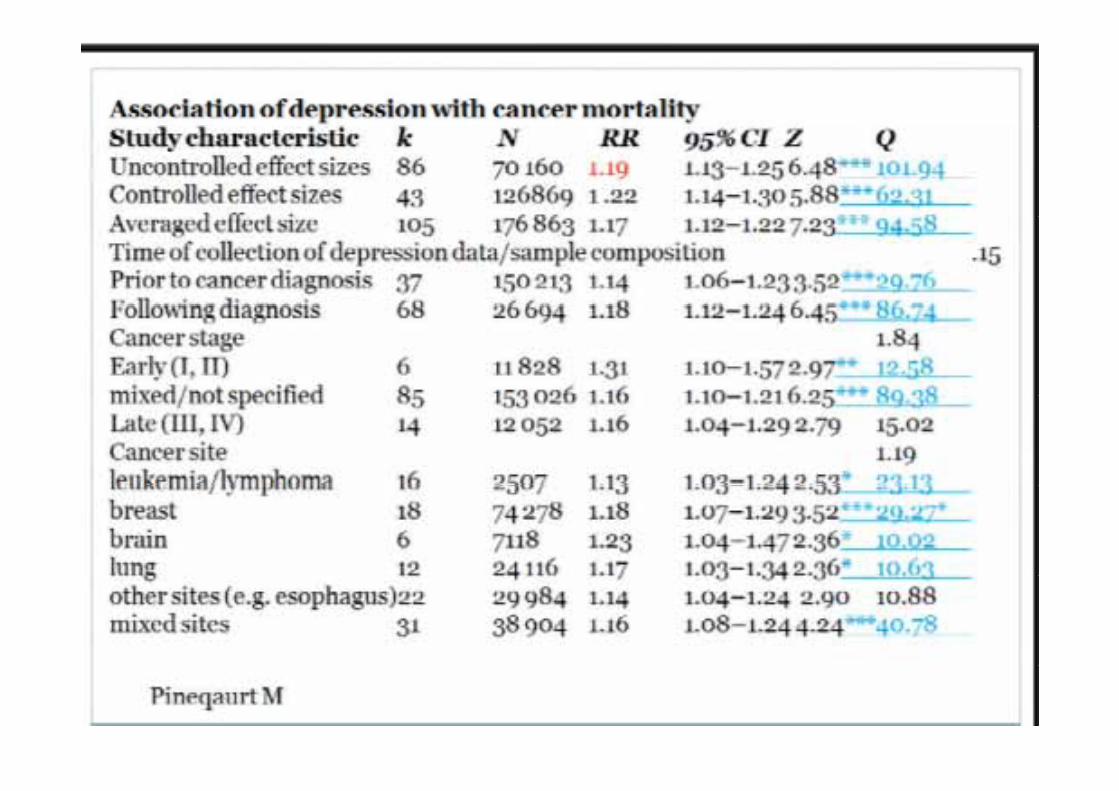
Association of Depression and Survival2 Meta-Analyses – 17-25% increase in mortality in 2 Meta-Analyses – 17-25% increase in mortality in
those with sig depression76 studies Pinequart M Duberstein Psychol Med – 76 studies, Pinequart M, Duberstein Psychol Med 2010
Individual StudiesIndividual Studies– Giese-Davis
Temel– Temel
D i d CDepression and CancerRCT Giese-Davis et al JCO 2011
Randomised Trial of 1 year of Supportive-expressive group therapy (SET) , weekly 1 5 h i1.5-hour group sessions
125 women with documented metastatic or recurrent (n = 3) breast cancerrecurrent (n = 3) breast cancer.
All participants (N = 125) received educational materials and completed theeducational materials and completed the Center for Epidemiologic Studies–Depression Scale (CES-D) at baseline p ( )(before random assignment) and at 4, 8, and 12 months
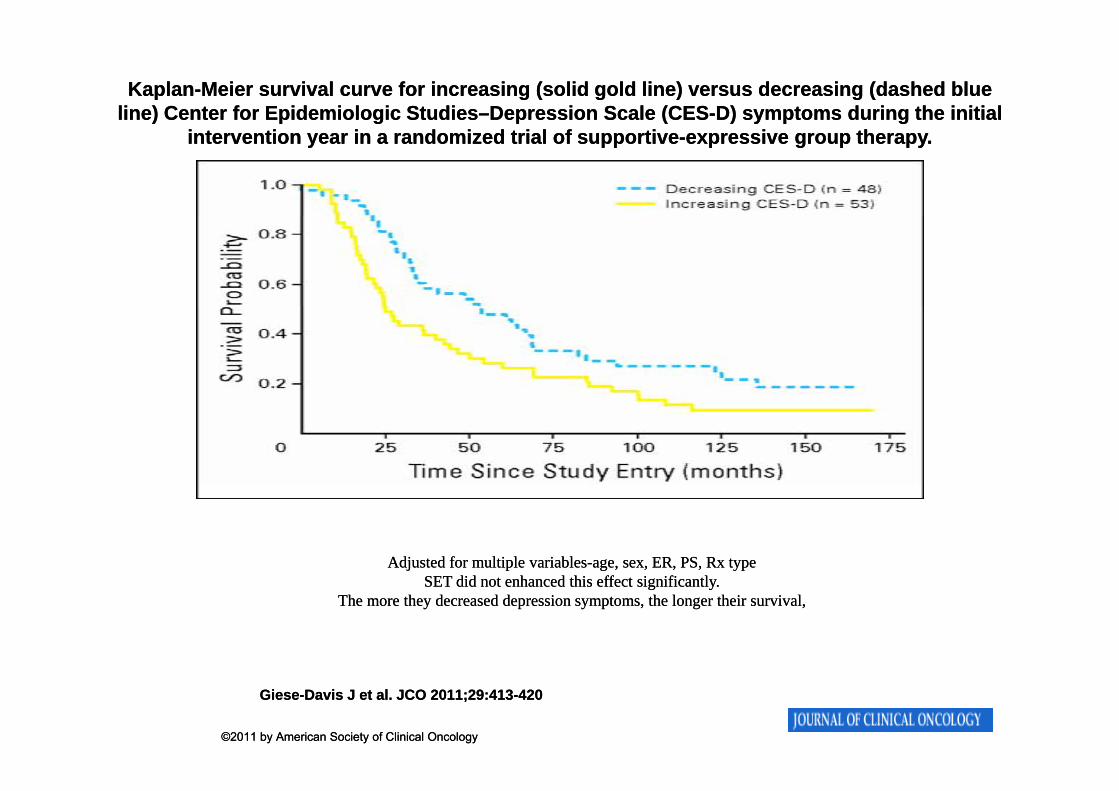
KaplanKaplan--Meier survival curve for increasing (solid gold line) versus decreasing (dashed blue Meier survival curve for increasing (solid gold line) versus decreasing (dashed blue line) line) CenterCenter for Epidemiologic Studiesfor Epidemiologic Studies––Depression Scale (CESDepression Scale (CES--D) symptoms during the initial D) symptoms during the initial
intervention year in a randomized trial of supportiveintervention year in a randomized trial of supportive--expressive group therapy.expressive group therapy.
Adjusted for multiple variablesAdjusted for multiple variables--age, sex, ER, PS, Rx type age, sex, ER, PS, Rx type SET did not enhanced this effect significantly.SET did not enhanced this effect significantly.
The more they decreased depression symptoms, the longer their survival,The more they decreased depression symptoms, the longer their survival,
GieseGiese--Davis J et al. JCO 2011;29:413Davis J et al. JCO 2011;29:413--420420
©2011 by American Society of Clinical Oncology©2011 by American Society of Clinical Oncology
Screening
Are Screening studies feasible?
UK study - 286 patients and 28 oncologists were randomized to measuring quality of life and depression using EORTC QLQC 30 and the Hospital depression using EORTC QLQC-30 and the Hospital Anxiety and Depression Scale (HADS) or usual care.
The use of these tools before seeing their oncologistThe use of these tools before seeing their oncologist– did not prolong interview time,– Increased discussion of chronic nonspecific symptoms, and
improved subsequent quality of life measurementimproved subsequent quality of life measurement.– Encouraged patients to be more forthcoming in stating their
needs and increased their satisfactionNo clear effect on patient management.
– Velikova G J ClinOncol 2004
Care Manager in Primary Care
A model was examined in the subset of 215 elderly patients with both 5 e de y pat e ts t botdepression and cancer from the Unutzerstudy.y
50% vs 34% reduction in symptoms at 6 mosmos
39% vs 20% at 12 mosG t i i t d iGreater remission rates, more depression
free days, increased Q of L
Cancer Centre
More patients with 50% reduction in depression scores - 53% vs. 34% dep ess o sco es 53% s 3 %
Higher remission rates - 68% vs. 45%. This was despite usual care includingThis was despite usual care including
reporting the diagnosis and medication recommendationsrecommendations.
Although intervention was short the effect t i d t 12 thwas sustained at 12 months.
Key Messages?
A treatment model that engages front line cancer care practitioners by providing support, resources, and guidanceguidance.
Care managers are front-line oncology health professionalsp– that are trained in oncology first– then receive additional mental heath training using well
developed protocol-based manualsdeveloped protocol based manuals.A small number of specialised mental health
practitioners supply, support, and manage the i t ti b i il bl intervention by accessing more available practitioners
Key Messages?
In smaller community practices, variants utilize either distant interventions and/or ut e e t e d sta t te e t o s a d/osupport for local nurse or physician assistants that can be trained and supervised at a distance,
A systematic introduction ofA systematic introduction of multidisciplinary care of the psycho social needs of patients with cancer cansocial needs of patients with cancer can be a reality in a practice of any size.
C t f S i hi C PlComponents of a Survivorship Care Plan: 1) Treatment Summary
Type of cancer (dates of diagnosis and treatment, stage, tumor characteristics), g , )Type(s) of treatment received
-Surgery (nature, extent)-Chemotherapy (drugs, dose, delivery)-Radiation (dose, port, fractionation & schedule)
Complications experienced (side effects, transfusions, recurrence/additional treatments, etc)etc)Services used
Components of a Survivorship Care Plan: 1) Follow-up Care (IOM, Lost in Transition, 2006, pg 188)) p ( pg )
Surveillance for recurrence/2nd cancers Assessment and treatment/referral for side effects (e.g., pain, functional impairment, fatigue, depression,
l t )employment concerns)Evaluation of risk for and prevention of late effects (e.g., second cancer cardiac dysfunction bone health); health second cancer, cardiac dysfunction, bone health); health promotionCoordination of care (incl frequency of visits tests and Coordination of care (incl. frequency of visits, tests, and who is performing these)
NIH 2011NIH 2011NIH, 2011NIH, 2011



![PROPOSED 2018 - floridadep.gov Region - DRAFT... · Docme COLL!qoL COLL!qoL luJ go COLL!q L nouucello -OLLI neao 00 L CCGC!I COLL!qoL IVX Lorue COLL!qoL ash 01] q so LL!qoL u BIAq](https://img.pdfslide.us/doc/110x75/5aa619db7f8b9ae7438e63bc/proposed-2018-region-draftdocme-collqol-collqol-luj-go-collq-l-nouucello.jpg)