-
Cancer of the prostate glandThomas Swallow
Simon Chowdhury
Roger S Kirby
AbstractProstate cancer constitutes a major health problem. It
is estimated that the
lifetime risk of western men having prostate cancer is about
30%, with the
risk of dying from the cancer being 3%. Increasing age is the
strongest pre-
y fat
consumed seems to be a risk factor for the development of
COMMON CANCERSSimon Chowdhury MRCP is a Consultant Medical
Oncologist specializing
in the treatment of prostate cancer at Guys Hospital, London,
UK.
Conflicts of interest: none declared.
Roger S Kirby FRCS(Urol) is a Honorary Professor of Urology
at
St Georges Hospital, and University College London, London,
UK.
Conflicts of interest: none declared.determinant for the
development of prostate cancer. Virtually all cancers are
adenocarcinomas, the grade being indicated by the Gleason score.
Often,
there are no presenting symptoms. Investigations such as
serum
prostate-specific antigen (PSA), digital rectal examination and
biopsies
via a transrectal ultrasound probe are required for diagnosis.
Staging, if
required, consists of magnetic resonance imaging or computed
tomog-
raphy for locally advanced disease and/or a bone scan for
detection of
bony metastases. Management depends largely on the stage of
the
disease. For localized prostate cancer, radical prostatectomy
can offer
a cure. Adverse consequences include erectile dysfunction and
inconti-
nence. Prostate cancer is also radiosensitive and treatment can
be given
as external-beam radiotherapy or in the form of brachytherapy.
Hormonal
therapy, such as luteinizing hormone-releasing hormone analogues
and
anti-androgens, is used in locally advanced and metastatic
disease.
Hormones do not cure but slow the progression of the cancer.
Follow-up
consists of PSA surveillance and other therapeutic options can
be consid-
ered if the PSA starts to rise. Cytotoxic chemotherapy is
increasingly
being used for hormone-escaped prostate cancer. The survival
rate at 10
years may be as high as 90% for a well-differentiated, localized
prostate
cancer.
Keywords brachytherapy; Gleason score; hormonal therapy;
prostate
cancer; prostatectomy; PSA; radiotherapy
Prostate cancer is becoming an increasingly significant
interna-
tional health problem; it may soon overtake lung cancer as
the
leading cause of cancer-related mortality in men in
developed
countries. For a western male, the lifetime risk of:
developing microscopic prostate cancer is 30% developing
clinical disease is 10% death from the disease is 3%.
Thomas Swallow MRCS is a Clinical Research Fellow in Urology
at
St Georges Hospital, London, UK. Conflicts of interest: none
declared.MEDICINE 40:1 10prostate cancer. The diet is rich in dairy
products and red meat in
areas with a high incidence (e.g. USA). Studies have
indicated
that vitamins E and D, as well as the trace element selenium,
may
protect against prostate cancer.
Testosterone and its main metabolite, dihydrotestosterone,
are
the principal hormones regulating the growth and function of
the
prostate gland. Cancer of the prostate is rarely found in
castrated
men. Conversely, relatively high concentrations of
circulating
testosterone have been found in African-American men,
possibly
explaining their higher incidence of prostate cancer compared
to
Caucasian men.
Other risk factors have been suggested, including vasectomy,
environmental (e.g. exposure to cadmium) and viral factors.Diet
appears to have a significant influence on the risk
prevention of prostate cancer. The amount of
dietarEpidemiology
Prostate cancer is diagnosed in about 30,000 and 200,000men
each
year in the UK and USA, respectively. These figures have
risen
steadily over the last 20 years. This statistic should be
interpreted
with caution because of increased detection due to the
prostate-
specific antigen (PSA) serum test (though an increase in
clini-
cally significant cancer appears to have occurred). Prostate
cancer
kills more than 9,000 men in the UK each year.
There is significant variation in the incidence of clinical
prostate cancer worldwide. It is relatively high in northern
Europe and North America, intermediate in southern Europe
and
South America, and low in the Far East and Asia. The highest
incidences are found in African-American men and the lowest
in
Chinese men.
Aetiology and risk factors
A direct cause of prostate cancer has not been discovered,
but
several risk factors have been identified.
Familial: several studies have shown the prevalence of
prostate
cancer within certain families. This familial or hereditary form
of
cancer is characterized by either:
three successive generations being affected with thedisease
a clustering of three or more men with the disease ina nuclear
family
two men with early-onset prostate cancer (i.e. age
-
The likelihood of local extension outside the prostate
capsule,
COMMON CANCERSinvasion into the seminal vesicle, and nodal and
distant metas-
tases increases with increasing PSA, tumour volume and
Gleason
score. Invasion into the seminal vesicle is associated with
nodal
and distant spread. The obturator lymph node chain is the
most
common site for lymphatic spread. Metastatic spread usually
involves non-regional lymphatics and the axial skeleton.
Diagnosis
Early low-grade prostate cancer is usually asymptomatic.
Locally
advanced or metastatic disease is usually the cause if men
present with symptoms. Local growth can cause obstructive or
irritative urinary symptoms. Metastatic spread can present
as
bone pain and even compression of the spinal cord. The main
investigations to diagnose prostate cancer are discussed
below.
PSA: most cancers are discovered by routine measurement of
PSA in serum. A screening programme for prostate cancer
andProstate cancer is graded using the Gleason grading system,
which
is based on the microscopic appearance of the glandular
architec-
ture of the prostate. The system is in two parts: a grade
between
1 and 5 is given to themost dominant pattern; then a
gradebetween
1 and 5 is given to the second commonest pattern. The two
are
added together to give the Gleason score. Thus, a Gleason
score
ranges from 2 to 10 and is usually fully annotated (e.g. 3 4
7).The grade indicates the degree of glandular differentiation:
grade 1
indicates a well-differentiated tumour, whereas grade 5 is a
poorly
differentiated tumour. The Gleason score gives an indication
of
prognosis and tumour progression.
The staging of prostate cancer is assessed using a number of
diagnostic tools, including digital rectal examination, bone
scintigraphy and MRI. Not all are essential in every case;
the
decision is guided by the concentration of PSA in serum,
Gleason
score and the clinical stage. Imaging is often unnecessary
in
patients who are at low risk of metastases using these
parameters.
Tumour progressionGrading and stagingProstatic intraepithelial
neoplasia (PIN) is the precursor of
prostate cancer. Cells show similar characteristics to those
of
prostate cancer cells, but the basal cell layer is present. PIN
is
often found adjacent to areas of prostate cancer, and its
identi-
fication in biopsy specimens in the absence of cancer
warrants
further investigation for concurrent invasive
carcinoma.Pathology
Over 95% of prostate cancers are adenocarcinomas; the
remainder are neuroendocrine tumours or sarcomas. Character-
istic prostate adenocarcinoma cells have hyperchromatic,
enlarged nuclei with prominent nucleoli and abundant cyto-
plasm. The basal cell layer is absent in prostate cancer,
but
present in normal glands and the glands of benign prostatic
hyperplasia. Prostate cancer is often multifocal. About 70%
are
found in the peripheral zone, 20% originate in the
transition
zone, and 10% are within the central zone.MEDICINE 40:1 11the
routine measurement of PSA is not present in the UK. The
advantages would be:
an initial increase in incidence rates as more cancers
aredetected, followed by a fall as they are treated
detection of the disease at earlier stages and decrease
inmortality from advanced disease
an increase in relative survival rate as compared to othercauses
of death
detection of disease at a younger age and at lowerconcentrations
of PSA.
The disadvantages include the:
number of false-positives e the PSA test lacks specificity,and
the concentration may be high due to other causes
(e.g. infection (prostatitis), benign prostatic hyperplasia
(BPH), acute urinary retention, vigorous digital rectal
examination)
number of false-negatives e the PSA test lacks sensitivity,and
the concentration may be within the typical normal
range even in the presence of cancer
potential identification and subsequent treatment of clini-cally
irrelevant disease.
The upper limit of normal PSA is usually 4 ng/ml, but this
value
will include some patients with BPH and some with prostate
cancer. The PSA increases with age, so the value must be
adjusted
for age. Further refinements of the PSA have been employed.
The speed of rise of PSA concentration (PSA velocity)during the
year before the diagnosis of cancer is strongly
associated with the risk of death from prostate cancer.
The ratio of free:total concentration of PSA can indicatewhether
a rise is due to BPH or cancer. A value of less than
18% suggests cancer and biopsy is indicated.
The digital rectal examination is an essential part of the
urolog-
ical examination, enabling the size of the prostate gland to
be
assessed, and nodules or lumps to be detected. The digital
rectal
examination alone can determine the need for further
investiga-
tion. The cancer can be staged by assessing whether the
tumour
extends to the seminal vesicles or invades adjacent
structures.
Transrectal ultrasound and biopsy are indicated if cancer is
suspected because of a raised PSA and the findings of the
digital
rectal examination. This procedure is done under local
anaes-
thesia and biopsies of the prostate are taken via a
transrectal
ultrasound probe. Ultrasound-guided biopsy:
provides more accurate staging than the digital
rectalexamination
allows lesions to be identified enables the volume of the
prostate gland to be measured.
Biopsies are taken with a Tru-Cut needle and 6e12 cores are
removed. This process samples a small percentage of the
prostate
gland, but the urologist or radiologist can focus on taking
samples
from lesions that feel or look suspicious on ultrasound.
Occa-
sionally, despite a high PSA, the biopsies are negative for
cancer,
or PIN is found. Most urologists recommend repeat biopsies
or
even saturation biopsies (20 biopsies are taken) if
suspicion
remains high. In general, transrectal ultrasound and biopsies
have
a low morbidity. Infection is seen in less than 5% (provided
anti-
biotic prophylaxis is used) and less than 2% have
significant
bleeding. Anticoagulants should be stopped before biopsy. 2011
Published by Elsevier Ltd.
-
the entire prostate gland, which reduces the risk of disease
tate gland. The urethra is then anastomosed to the base of
the
fewer adverse effects, but proctitis, rectal bleeding and
haema-
turia can occur. There is also a 1e3% risk of incontinence.
In
carefully selected patients, external-beam radiotherapy
offers
a 15-year overall survival, similar to that seen after
radical
prostatectomy. Radiotherapy may be combined with hormonal
therapy and two trials have shown improved overall survival
in
high-grade and locally advanced disease with the use of pro-
longed androgen deprivation therapy (see below) following
radiotherapy. The cancer cannot usually be treated by surgery
if
recurrence occurs. One study has revealed a doubling of
inci-
dence of rectal carcinoma in patients treated with
external-beam
radiotherapy, so post-treatment rectal bleeding should be
investigated.
Brachytherapy is the deployment of radioactive seeds
directly
into the prostate gland. It can be done as a two-stage (two
visits
to hospital; to be measured and then implanted with the
seeds)
or a one-stage procedure. Brachytherapy can be combined with
external-beam radiotherapy in patients considered at high risk
of
recurrence. Brachytherapy is most suitable for patients with
smaller, lower-risk cancers and for men with small or
medium-
sized prostate glands. Long-term tumour control from mature
series appears to be equivalent to prostatectomy and
external-
beam radiotherapy. Without careful case selection, the
predom-
inant complication is the occurrence of obstructive urinary
symptoms, including the need for prolonged catheterization.
Sexual function is thought to be better preserved after
brachy-
therapy compared to surgery and radiotherapy.
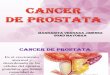
COMMON CANCERSbladder. The obturator lymph nodes are sampled. A
catheter is
left for 2 weeks while the urethra and bladder heal. A
recent
randomized controlled clinical trial showed a significant
improvement in mean survival in patients treated by radical
prostatectomy compared to those managed by watchful waiting,
and a 50% reduction in the development of metastases.
Erectile dysfunctionmay result in up to 50%of patients, but
can
be greatly improved with phosphodiesterase-5 inhibitors.
Stress
incontinence is seen in 2e3% and almost invariably improves
with pelvic floor exercises, physiotherapy and/or
anticholinergics.
Careful histopathological examination of the whole tumour
specimen can identify patients at higher risk of recurrence,
which
can be reduced by postoperative radiotherapy.
External-beam radiotherapy: radiation therapy provides
a definitive treatment approach for localized and
locallyrecurrence. The procedure is commonly done through a
hori-
zontal or vertical incision on the lower abdomen.
Laparoscopic
and robot-assisted laparoscopic removal of the prostate are
becoming more common. Particular care is taken to preserve
the
delicate nerves on either side of the prostate; this reduces the
risk
of impotency. The seminal vesicles are removed with the
pros-Radical prostatectomy (Figure 1) has the advantage of
removingoccur if the cancer progresses.Other investigations
MRI or CT of the pelvic area is indicated if biopsies are
positive
for adenocarcinoma. This gives anatomical information about
the local extension of the cancer and lymph node
involvement,
which is important if a radical prostatectomy is considered.
Whole-body bone scintigraphy is carried out if the PSA is
over 10 ng/ml. This gives information on bony metastases
that
may influence management.
New molecular studies are available that may negate the need
for prostate biopsies. A specific urine sample assay can
detect
PCA3, a gene that is overexpressed in prostate cancer tissue.
A
prostate massage is done so that prostate cells are shed; these
are
then caught via a urine sample for analysis.
Differential diagnosis
Induration of the prostate, apparent on digital rectal
examination,
is also associated with prostatitis, previous transurethral
resection
of the prostate, needle biopsy or prostatic calculi. The
main
differential diagnoses are BPH, prostatic calculi and
prostatitis.
Management
Localized prostate cancer
Watchful waiting/active surveillance may be the most appro-
priate course for men aged over 70 years and/or those with
significant co-morbidity, particularly if the cancer is low
volume
and the Gleason score is low. Careful follow-up with regular
digital rectal examination and monitoring of PSA is
important.
Counselling and implementation of active treatment
shouldMEDICINE 40:1 12advanced disease. Pelvic lymph nodes can be
included in the
treatment field. Advances in radiotherapy have led to the
radia-
tion beam being focused on the prostate gland. This has led
to
Watchful waiting
Number at risk
347Radicalprostatectomy
348
343
341
332
326
284
279
210
198 104
118
Incidence of death from prostate cancer: watchful waitingversus
radical prostatectomy
00
40
30
10
20
2 4 6
Years of follow-up
hta
ed
fo
ecn
edic
nievit
alu
mu
C)
%(r
ecn
acet
atsor
pm
orf
8 10
Radical prostatectomy
Watchful waiting
Source: Bill-Axelson A, Holmberg L, Ruutu M et al. Scandinavian
ProstateCancer Group Study No. 4. Radical prostatectomy versus
watchful waiting inearly prostate cancer. New Engl J Med 2005; 352:
197784. Reproduced withpermission.
Figure 1 2011 Published by Elsevier Ltd.
-
Locally advanced prostate cancer
Hormonal therapy
Analogues of luteinizing hormone-releasing hormone
(LHRHa) are usually given as a depot injection every 3
months.
They act by over-stimulating LHRH receptors in the pituitary
gland
and, via negative feedback, stop the release of luteinizing
hormone
from the pituitary gland. The concentration of circulating
testos-
terone is reduced to a castration level. These agents reduce the
size
of the cancer and slow progression, but do not eradicate the
disease. Themain adverse effects of androgen deprivation
therapy
(ADT) are hot flushes, sweats, and reduced libido. Patients
may
also notice reduced muscle mass, reduced strength and weight
gain. A proportion of patients suffer reduced bone mineral
density
and there is known to be an increased risk of non-traumatic
frac-
LHRHa and anti-androgens in combination confer complete
testosterone blockade. It is not clear whether this
combination
therapy significantly increases the time to progression or
overall
survival. Combination therapy is probably best suited to
younger, relatively fit men with advanced prostate cancer
because it may result in a longer period before disease
progression.
Follow-up: most patients have regular measurement of PSA.
After radical prostatectomy, the PSA should remain at zero if
all
the cancer has been removed. In locally advanced and
metastatic
disease treated with hormones, it should fall to very low
levels
initially.
COMMON CANCERSLHRHa: the response to this treatment in
metastatic cancer is
about 80%, and benefits last for 18e36 months. A large rise
in
circulating testosterone may be seen when the injection is
first
given, causing bone pain and even spinal cord stenosis;
anti-
androgens are given to protect against this tumour flare.
Newer LHRH antagonists (e.g. degarelix) do not cause a surge
and may have a role in emergency situations e such as newly
diagnosed cancer presenting with cord compression.months.tures,
somen at risk of osteoporosis should be carefullymonitored
or treated with bisphosphonates where necessary.
Anti-androgens block the action of testosterone on the pros-
tate gland. Adverse effects include breast enlargement and
soreness. They can also cause mild stomach upset and damage
the liver. They do not have such a profound effect as LHRHa
on
potency and libido. Anti-androgens slow the progression of,
but
do not cure prostate cancer.
Metastatic prostate cancer
About 70% of men with metastatic prostate cancer die from
their
cancer within 5 years. Progression can be delayed for
several
years by the treatments discussed below.
Bilateral orchidectomy is the surgical removal of both
testicles
so that testosterone is no longer produced. Prosthetic testes
can
be inserted for a better cosmetic appearance. A subcapsular
orchidectomy (only the cells of the testes are removed and
the
capsule is left) can be done. The main adverse effects are
hot
flushes, loss of libido and impotence. About 80% of men
respond
to this treatment, which slows disease progression for about
18MEDICINE 40:1 13and practice. London: Taylor and Francis,
2005.Castrate-refractory prostate cancer
Prostate cancer eventually becomes insensitive to hormone
ablation and the PSA begins to rise (castrate-refractory
prostate
cancer). This rise is often accompanied by clinical
symptoms,
particularly bone pain. Whole-body bone scintigraphy must be
repeated to see if the cancer has spread. This is an area that
is
changing rapidly and therapeutic options that have been
shown
to benefit the patient include:
modifying existing hormonal therapy (e.g. abiraterone) cytotoxic
chemotherapy (e.g. docetaxel) bone-directed therapies (e.g.
bisphosphonates, monoclonal
antibodies to RANK-ligand, radioisotopes)
palliative radiotherapy.Most of these treatments have shown a
small benefit in the late
stages of disease and it is hoped that, by using them earlier in
the
treatment of locally advanced and metastatic disease, they
will
have a greater effect.
Prognosis
The natural history of prostate cancer is highly dependent
on
stage, grade, co-morbidity and age. The survival rate at 10
years
for a well-differentiated, localized prostate cancer may be as
high
as 90%; for a poorly differentiated tumour it drops to 60%
or
less. Prostate cancer is one of the few solid cancers that is
readily
curable, if it is detected early. A
FURTHER READING
Kirby RS, Partin A, Feneley M, Parsons K, eds. Prostate cancer:
principles 2011 Published by Elsevier Ltd.
Cancer of the prostate gland Epidemiology Aetiology and risk
factors
Pathology Grading and staging Tumour progression
Diagnosis Other investigations Differential diagnosis Management
Localized prostate cancer Locally advanced prostate cancer
Metastatic prostate cancer Castrate-refractory prostate cancer
Prognosis Further reading