-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
1/167
Pharmacotherapy
of Cancer
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
2/167
Cancer
A cellular disorder, clonal origin
Progressive accumulation of a mass of
cells Progressive invasion of surrounding
tissues and organs
Ability to metastasize to distant organs
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
3/167
Cancer
Essentially, a genetic disease
Mutation of genes: Oncogenes
Tumor suppressor genes Mismatch repair genes
Germline mutation: hereditary or familial
cancer Somatic mutation: sporadic cancer
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
4/167
Cellular Kinetics
Human body contains 5x1013 cells
Cells can either be- non dividing and terminally
differentiated
- continually proliferating
- rest but may be recruited into cell cycle
Tumour becomes clinically detectable when
there is a mass of 109 cells (1g)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
5/167
The Cell Cycle
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
6/167
Tumor kinetic
Growth rate depends on:
growth fraction
-percent of proliferating cells within a given system
-human malignacy ranges from 20-70%
-bone marrow 30 %
cell cycle time
-time required for tumour to double in size
rate of cell loss
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
7/167
Tumor Kinetics Original Hypothesis
Conventional views in the field of oncologysupport the notion
that:
tumor growth is exponential
chemotherapy treatment is designed tokill in log intervals
(kills constant fractionsof tumor)
Combination therapy and increased drug doselevels aim at
improving ovarian cancerchemotherapy.
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
8/167
Gompertzian Growth
Growth rates are exponential at early stages of
development and slower at later stages of
development.
- Biological growth follows this characteristic curve.-
Biological growth follows this characteristic curve.
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
9/167
Gompertzian growth model
Initial tumour growth is first order, with later growth
beingmuch slower
Smaller tumour grows slowly but large % of cell dividing
Medium size tumour grows more quickly but with smaller
growth fraction
Large tumour has small growth rate and growth fraction
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
10/167
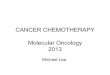
number ofnumber ofcancer cellscancer cells
diagnosticdiagnostic
thresholdthreshold
(1cm)(1cm)
timetime
undetectableundetectable
cancercancer
detectabledetectable
cancercancer
limit of
clinicaldetection
host
death
10101212
101099
Tumor Growth
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
11/167
Rationales in Human Cancers
Small tumors grow faster than larger
tumors
Human cancers grow by non-exponential
Gompertzian kinetics
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
12/167
Principle of chemotherapy
First order cell kill theory
- a given dose of drug kills a constant percentage
of tumour cells rather than an absolute number
Maximum kill
Broad coverage of cell resistance
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
13/167
The rate of tumor volume regression isproportional to the rate
of growth.
Tumor cell regrowth can be prevented if tumor cells are
eradicated using a denser dose rate of cytotoxic therapy.
Tumors given less
time to grow in
between treatmentsare more likely to be
destroyed.
Hypothesis of Alternative Intervals
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
14/167
Principle of chemotherapy
Rationale for combination chemotherapy
Different drugs exert their effect through different
mechanisms and at different stages of the cell cycle,
thus maximize cell kill
Decease the chance of drug resistance
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
15/167
Paraneoplastic syndrome
Syndrome Clinical manifestationSystemic anorexia, cachexia,
weight
loss, fever
Endocrine hypercalcemia,
hyponatremia,hypoglycemia, Cushingsyndrome
Skeletal / connective tissue digital clubbing,hypertrophic
pulmonaryosteoarthropathy
Neurolgic / muscular myasthenia gravis, Eaton-Lambertsyndrome,
polymyositis, peripheralneuropathy, subacute
cerebellardegeneration
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
16/167
Paraneoplastic syndrome
Syndrome Clinical manifestation
Hematologic anemia, polycythemia,
leukocytosis, thrombocytosis,deep vein thrombosis
Skin dermatomyositis, acanthosis
nigricans
Renal nephrotic syndrome,glomerulonephritis
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
17/167
Psychosocial effects of cancer
Loss of control
Fear of pain and mutilation
Separation and loneliness
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
18/167
The Changing Nature of Palliative Care
CURATIVE
CARE
PALLIATIVE
CARE
CURATIVE CARE
PALLIATIVE CARE
TIME
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
19/167
AIM OF COMBINATION THERAPY
INCREASED EFFICACYINCREASED EFFICACY
Different mechanisms of action Compatible side effects
Different mechanisms of resistance
ACTIVITYACTIVITY SAFETYSAFETY
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
20/167
It is easy to kill cancerIt is easy to kill cancer
cells, but the challenge iscells, but the challenge iskeeping
the patient alive atkeeping the patient alive at
the same time..!the same time..!
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
21/167
How to treat cancer
Clinical evaluation and treatment options
1. Diagnosis: pathological diagnosis
2. Evaluation of disease: staging
3. Treatment objectives: curative, palliative
4. Treatment options
5. Evaluation of response
6. Supportive therapy
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
22/167
Modalities of treatment
Local treatment options
Surgery
Radiation
Systemic treatment options
Chemotherapy
Hormonal therapy
Biotherapy
Molecular-targeted therapy
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
23/167
Principle of Treatment :
Most anticancer treatment is directed
towards killing actively dividing cells.
Complications: Marrow aplasia, alopecia,
sterility, GIT, lung, kidney damage).
Newer drugs target tumor cells by immune
mechanisms or hormones.
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
24/167
General Disease-Related
Consequences of Cancer
Impaired immune and hematopoietic function
Altered gastrointestinal structure and function
Motor and sensory deficits
Decreased respiratory function
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
25/167
Karnofsky Performance Scales
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
26/167
Chemotherapy
Treating cancer with chemical agents
Major role in cancer therapy
Used to cure and increase survival time Some selectivity for
killing cancer cells
over normal cells
Normal cells most affected: the skin, hair,intestinal tissues,
spermatocytes, and
blood-forming cells
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
27/167
Chemotherapy Drugs
Antimetabolites
Antitumor antibodies
Alkylating agents Antimitotic agents
Topoisomerase inhibitors
Miscellaneous chemotherapeutic agents Combination
chemotherapy
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
28/167
Treatment Issues
Drug dosage
Drug schedule
Drug administration Route : IV, IM, SC, IT
Extravasation
Vesicants
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
29/167
Side Effects of Chemotherapy
Alopecia or hair loss Nausea and vomiting Mucositis in the
entire gastrointestinal tract
Skin changes Anxiety, sleep disturbance Altered bowel
elimination Decreased mobility
Hematopoietic system changes Bone marrow suppression
Hypersensitivity (esp. taxanes, platinums)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
30/167
Immunotherapy: Biological
Response Modifiers
Drugs that modify the clients biologic
responses to tumor cells
Cytokines: enhance the immune system
Interleukins, interferons
Side effects: generalized and sometimes
severe inflammatory reactions, peripheralneuropathy, skin
rashes, increased
depression
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
31/167
Gene Therapy
Experimental as a cancer treatment
Renders tumor cells more susceptible to
damage or death by other treatments
Injection into tumor cells, enabling the
immune system to better recognize cancer
cells as foreign and kill them
Antisense drugs
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
32/167
Definition
New technology and drugs that allow the cancer
treatment to target a certain cancer cell by interfering
with
the natural functions of tumor growth
How they work
They target specific parts of a cancer cell or its actions;
hand in a glove analogy
What it means in cancer treatment Potentially fewer side
effects
Targeted Therapies
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
33/167
Targeted Therapies
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
34/167
Targeted Therapies Monoclonal antibodies: proteins that trigger
the bodys
pathways involved in cancer growth to fight cancer
moreeffectively.
EGFR: family of receptors found on surface of normal and
cancer cells that bind with an epidermal growth factor
(EGF)causing cells to divide.
Tyrosine Kinase Inhibitors: Part of the cell that signals it
todivide and multiply; enhances cell growth.
Stillinvestigational
Vaccines: stimulate the bodys immune system to fight
thecancer
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
35/167
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
36/167
Role of Chemotherapy in
Cancer Treatment
Adjuvant chemotherapy a short course of combination
chemotherapy
in a patient with no evidence of residualcancer after surgery or
radiotherapy, given
with the intent of destroying a small number
of residual tumor cells
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
37/167
Neoadjuvant chemotherapy given in the preoperative or
perioperative period
Primary: same as neoadjuvant chemotherapy, also
applied to chemotherapy given in the absence of intended surgery
or radiotherapy
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
38/167
Salvage:- combination chemotherapy given in a
patient who has failed or recurred following
a different curative regimen
Palliative: chemotherapy given to control symptoms or
prolong life in a patient in whom cure isunlikely
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
39/167
Induction: combination chemotherapy given
with the intent of inducing completeremission when initiating a
curative regimen
Consolidation: repetition of the inductionregimen in a patient
who has achieved a co
mplete remission after induction
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
40/167
Intensification: chemotherapy after
complete remission with higher doses, with
the intent of increasing the cure rate or remi
ssion duration
Maintenance: long-term, low-dose
chemotherapy in a patient who has achieve
d a complete remission
Cli i l E d i t i E l ti
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
41/167
Clinical Endpoints in Evaluating
Response to Chemotherapy
Objective Response Measurable disease (longest diameter)
Complete Response (CR)
Relapse-free survival after stopping treatment (>= 4 wks)
Partial Response (PR)
At least a 50% reduction in measurable tumor mass
Progressive Disease (PD)
> 25% increase in one or more lesions
Stable Disease (SD)
Neither PR nor PD (no changes)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
42/167
Tumor which are Curable with
Chemotherapy : in advanced disease
Choriocarcinoma
Acute leukemia
Hodgkins disease High grade non-
Hodgkins lymphoma
Germ cell tumor
Wilms tumor
Embryonal
rhabdomyosarcoma Ewings sarcoma
Neuroblastoma
Small cell lung cancer
Ovarian cancer
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
43/167
Neoadjuvant chemotherapy
Preservation of the tumor mass as a
biologic marker of responsiveness to the d
rugs
Sparing of vital normal organs
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
44/167
Chemotherapy has Minor Activity
Brain tumor
(astrocytoma)
Cervical cancer
Colorectal cancer
Non small cell lung
cancer
Melanoma
Pancreatic cancer
Prostate cancer Soft tissue sarcoma
Hepatoma
Renal cell carcinoma
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
45/167
CHEMOTHERAPEUTIC
AGENT :CLASSIFICATION
Alkylating agents: mechlorethamine, busulfan, nitrosoureas,
cyclophosphamide, chlorambucil, melphalan
Antimetabolites:
methotrexate, 5-fluorouracil, nucleoside
analogues
Anthracyclines:
doxorubicin, epirubicin
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
46/167
Antimicrotubule agents: vinca alkaloids, taxanes
Platinum analogues: cisplatin, carboplatin
Topoisomerase II inhibitors: etoposide, tenoposide
Topoisomerase I inhibitors: camptothecins
Antibiotics: bleomycin, dactinomycin
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
47/167
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
48/167
Types of chemotherapy
Cell cycle dependent
Cell cycle phase specific
Cell cycle independent Cell cycle phase non-specific
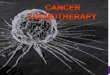
Sites of Action of Cytotoxic Agents
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
49/167
Antibiotics Antimetabolites
S
(2-6h)G2
(2-32h)
M
(0.5-2h)
Alkylating agents
G1(2-h)
G0
Vinca alkaloids
Mitotic inhibitors
Taxoids
Sites of Action of Cytotoxic Agents
Cell Cycle Level
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
50/167
Cycle-Specific Agents
Sites of Action of Cytotoxic Agents
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
51/167
DNA synthesis
AntimetabolitesAntimetabolites
DNA
DNA transcription DNA duplication
Mitosis
Alkylating agentsAlkylating agents
Spindle poisonsSpindle poisons &&
Microtuble StablizersMicrotuble Stablizers
Intercalating agentsIntercalating agents
Sites of Action of Cytotoxic Agents
Cellular Level
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
52/167
ALKYLATING AGENTS
Cyclophosphamide
alkylation of DNA through the formation of
reactive intermediates
oral bioavailability 100%
T1/2
3-10 hrs -- parent compound, 8.7 hrs --
phosphoramide mustard
metabolism:
microsomal hydroxylation
hydrolysis to phosphoramide mustard (active) and
acrolein
M t b li f
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
53/167
CYCLOPHOSPHAMIDE
4-OH CYCLOPHOSPHAMIDE
ALDOPHOSPHAMIDE
PHOSPHORAMIDE
MUSTARD
4-KETOCYCLOPHOSPHAMIDE
CARBOXYPHOSPHAMIDE
ACROLEIN
HEPATICCYTOCHROMES
P 450ACTIVATION
CYTOTOXICITYTOXICITY
INACTIVATIONALDEHYDE
DEHYDROGENASE
Metabolism of
Cyclophosphamide
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
54/167
Cyclophosphamide
toxicity: myelosuppression
alopecia
pulmonary fibrosis
cystitis: use MESNA with high-dose therapy SIADH
cardiac toxicity
leukemogenesis
infertility teratogenesis
Intake daytime pill
MESNA = 2-mercaptoethane sulfonate Na(Na = sodium), used
as chemotherapy adjuvant to detoxify metabolites of
cyclophosphamide & ifosfamide
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
55/167
ANTIMETABOLITES
Methotrexate (MTX)
inhibition of dihydrofolate reductaseinhibition of dihydrofolate
reductase--->partial
depletion of reduced folates
polyglutamates of MTX and dihydrofolate inhibitinhibit
purine and thymidylate biosynthesispurine and thymidylate
biosynthesis
metabolism: converted to polyglutamates in normal
and malignant tissues
elimination: primarily as intact drug in urine, third-
space retention
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
56/167
Methotrexate (MTX)
High dose toxicity: rescue by leucovorin
Pretreatment with MTX increases 5-FU and ara-C
nucleotide formation
NSAIDs decrease renal clearance and increase toxicity
Reduce dose in proportion to decrease in creatinine
clearance
NO high-dose MTX to patients with abnormal renal
function
Monitor plasma conc. of drug and hydrate patients
during high-dose therapy
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
57/167
Methotrexate (MTX)
toxicity: myelosuppression
mucositis
renal tubular obstruction and injury
in high-dose therapy, requires urine alkalinizati
on and hydration
hepatotoxicity in chronic therapy
pneumonitis
hypersensitivity: rare
neurotoxicity
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
58/167
5-fluorouracil (5-FU)
Interferes with RNA synthesis and functionInterferes with RNA
synthesis and function
inhibition of thymidylate synthase (TS)inhibition of thymidylate
synthase (TS)
Affect DNA stabilityAffect DNA stability
primary T1/2 8-14 min, clearance is faster withinfusional
schedules, non-linear pharmacokinetics
90% is eliminated by metabolism,
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
59/167
5-FU
Leucovorin increases activity and toxicity
Toxicity: GI epithelial ulceration
myelosuppression
skin toxicity
ocular toxicity
neurotoxicity
cardiac toxicitybiliary sclerosis (hepatic arterial infusion
of FUDR)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
60/167
Cytidine analogues
Cytosine arabinoside (araC)
2-2-difluoro-deoxycytidine (gemcitabine)
AraC inhibits DNA polymerase alpha
short plasma T1/2
elimination: deamination in liver, plasma and peripheral
tissue 100%
blocks DNA repair, enhances activity of alkylating
agents
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
61/167
AraC
toxicity: myelosuppression
GI epithelial ulceration
intrahepatic cholestasis, pancreatitiscerebellar and cerebral
dysfunction (high-
dose, elderly, impaired renal function)
conjuctivitis (high-dose)
hidradenitisnoncardiogenic pulmonary edema
ANTHRACYCLINES
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
62/167
ANTHRACYCLINES
Pleiotropic effects:
Inhibition of dna topoisomerase ii activity
Activation of protein kinase c,
Generation of reactive oxygen and stimulation
of apoptosis Doxorubicin: protein binding 60-70%
Elimination: 50-60% by hepatic aldo-keto reductase
Drug clearance is decreased in the presence ofhyperbilirubinemia
or patients with marked burden of metastatic tumor in liver
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
63/167
Heparin binds to doxorubicin causing
aggregation
Toxicity:
Myelosuppression
Mucositis
Alopecia
Cardiac toxicity: acute and chronic, cumulative dose-
related (hypertensive heart disease, mediastinal)
Severe local tissue damage after drug extravasation Radiation
sensitization of normal tissue
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
64/167
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
65/167
Vinca alkaloids
toxicity: Neutropenia except vincristine thrombocytopenia
(vinblastine)
Peripheral neuropathy (capping of vincristine to
2.0 mg) jaw pain Constipation
SIADH (vincristine, vinblastine)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
66/167
Taxanes (paclitaxel, docetaxel)
High-affinity binding to microtubules,High-affinity binding to
microtubules,
Stabilize microtubules against depolymerization,Stabilize
microtubules against depolymerization,
Inhibit mitosisInhibit mitosis
Elimination: predominantly by hepatic hydroxylation
(p450 enzyme) and biliary excretion of metabolites,
less than 10% eliminated intact in urine
Dose should be modified in patients with abnormal liverfunction
test
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
67/167
Paclitaxel & Docetaxel
1971
1986
OH
European Yew: Taxus baccata
Pacific Yew: Taxus brevifolia
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
68/167
Taxanes:
Toxicity: acute hypersensitivity reactions,
premedication with corticosteroid and antihistamines
(h1 and h2 blockers)
neutropenia, thrombocytopeniamucositis (esp. prolonged infusion,
96-hr)
alopecia
sensory neuropathy
cardiac conduction disturbances
fluid retention (docetaxel)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
69/167
PLATINUM ANALOGUES
Cisplatin, carboplatin, oxaliplatin
Cisplatin
Covalent binding to DNA Inactivated by sulfhydryl groups,
covalently binds to
glutathione, metallothioneins, and sulfhydryls on
proteins
25% is excreted during the first 24 hrs, renal > 90%,bile
< 10%
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
70/167
Cisplatin
toxicity: renal insufficiency with Mg2+ wasting,
monitor electrolytes, Mg2+, Ca2+, use with caution in
the presence of other nephrotoxic drugs
nausea and vomiting
peripheral neuropathy
auditory impairment
myelosuppression
visual disturbance (rare)hypersensitivity (rare)
seizures (rare)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
71/167
Carboplatin
drug is primarily excreted, only a small fraction is
metabolized
90% excreted in urine in 24 hrs
toxicity: myelosuppression, esp.thrombocytopenia
nausea and vomiting
nephrotoxicity at high doses and in
patients with prior renal dysfuction reduce dose in proportion
to reductions in
creatinine clearance
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
72/167
Oxaliplatin
Greater distribution to tissue than cisplatin
(50 times)
Excrete by urine in metabolite form Never reconstitute in 0.9%
NaCl (unstable)
Toxicities :
neurotoxic peripheral sensory neuropathy
N/V/D
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
73/167
TOPOISOMERASE II INHIBITORS
Etoposide
Inhibition of DNA topoisomerase IIInhibition of DNA
topoisomerase II
Terminal t1/2 6-8 hrs Hepatic metabolism, renal excretion
35-40%
Reduced dose proportionate to creatinine clearance
Toxicity: neutropenia, thrombocytopenia (mild), alopecia
hypersensitivity, mucositis (high doses)
CAMPTOTHECINS
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
74/167
CAMPTOTHECINS
Irinotecan (CPT-11)Topotecan
Irinotecan inhibit topoisomerase Iinhibit topoisomerase I by
stabilizing the cleavablecomplex in which the enzyme is covalently
bound to DNA
at a single-stranded break site
is aprodrugprodrugwhich requires enzymatic cleavage by
thecarboxylesterase converting enzyme to generate the biolo
gically active metabolite, SN-38
I i t
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
75/167
Irinotecan
elimination: 22% is excreted unchanged in the urine,the rest by
biliary excretion and conversion to SN-38
toxicity: diarrhea- early onset within hours or during the
infusion associated with cramping, vomiting, flushing and
diap
horesis, controlled by atropine. late-onset diarrhea can occur
later than 12 hoursfollowing drug administration, may be controlled
by high-dose loperamide (an initial dose of 4 mg followed by 2
mg
every 2 hours or 4 mg every 4 hours during the night)
Irinotecan
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
76/167
Irinotecan
toxicity: myelosuppression, neutropenia alopecia
nausea and vomiting
mucositis
fatigue
elevated liver function, caution in
patients with liver dysfunction
pulmanary toxicity (uncommon)
associated with a reticulonodular
infiltrate, fever, dyspnea, and
eosinophilia
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
77/167
ANTIBIOTICS
Bleomycin, dactinomycin
Bleomycin
Oxidative cleavage of DNA initiated by hydrogenOxidative
cleavage of DNA initiated by hydrogen
abstractionabstraction
Metabolism: activated by microsomal reduction and
degraded by hydrolase found in multiple tissues
Elemination: renal 45-70% in first 24 hrs
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
78/167
Bleomycin
Reduce dose for creatinine clearance < 60 ml/min
Toxicity: pulmonary interstitial infiltrates and fibrosis,
increased risk in patients with underlying pulmonary disease
, age > 70, renal insufficiency, prior chest radiation,
oxygenduring surgery, cisplatin
desquamation, esp of fingers and elbows
Reynaud phenomenon
hypersensitivity reaction (fever, anaphylaxis,eosinophilic
pulmonary infiltrates)
Dactinomycin (actinomycin D)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
79/167
Dactinomycin (actinomycin D)
Inhibition of RNA and protein synthesis Elimination: renal
6-30%, bile 5-11%
Avoid extravasation: necrosis
Toxicity: myelosuppression
nausea and vomiting mucositis
diarrhea
radiation sensitization and recall reactions
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
80/167
PROPHYLACTIC AGENTS
Antiemetic regimens: Acute emesis: serotonin antagonist +
dexamethasone or metoclopramide (1 mg/kg) + dexa
methasone
Delayed emesis: (cisplatin, carboplatin, doxorubicin,high dose
cyclophosphamide):metoclopramide 0.5
mg/kg IV/PO QID x 2-4 d (8-16 doses) then every 4 hr
s PRN
Dexamethasone 4-8 mg IV/PO x 4 dDiphenhydramine 50 mg PO every 4
hrs, PRN only
for restlessness or acute dystonic reactions
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
81/167
Hydration: cisplatin, ifosfamide, high dosemethotrexate
Premedications for paclitaxel: (preventhypersensitive
reaction)
dexamethasone 20 mg PO 12 and 6 hrs prior topaclitaxel
20 mg IV 30-60 min prior to paclitaxel
diphenhydramine 50 mg IV/PO 30-60 min prior topaclitaxel
cimetidine 300 mg or ranitidine 50 mg IV 30-60 min priorto
paclitaxel
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
82/167
Growth factors: G-CSF for prophylaxis inprevious febrile
neutropenia or high incidenc
e of grade IV neutropenia
MESNA
Prevention of Ifosfamide-induced hemorrhagic
cystitis
Prevention of high-dose cyclophosphamide-induced hemorrhagic
cystitis
D l l ti i l
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
83/167
Dosage calculation in oncology
Body surface area
derived in 1916 by Du Bois and Du Bois
reduce the interpatient variability of drug
exposure and, hence, drug effects
AUC (carboplatin) Dose (mg) = Target AUC (mg/mL/min) x [GFR
(mL/min) + 25]
Fix dosing
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
84/167
Body surface areacalculation:
Nomogram
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
85/167
Managing Cancer TreatmentSide Effects and Toxicity
SIDE EFFECTS OF
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
86/167
SIDE EFFECTS OF
CHEMOTHERAPY
Mucositis
Nausea/vomiting
Diarrhea
Cystitis
Sterility
Myalgia
Neuropathy
Alopecia
Pulmonary fibrosis
Cardiotoxicity
Local reaction
Renal failure
Myelosuppression
Phlebitis
I it t V i t
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
87/167
Irritant vs. Vesicant
Local inflammatoryreaction
Intact blood return
Short-term injury Bleomycin
Platinum
Doxorubicin (bothforms)
Etoposide
Ifosfamide
Infiltrating surroundingtissue blistering
May be delayed 6-12hr
Severe necrosis
Absent of blood returnAnthracyclins
Vinca alkaloids Teniposide
Streptozocin
E t ti f C t t i d
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
88/167
Extravasation of Cytotoxic drug
P t th
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
89/167
Port-a-cathPort inserted in vein
for chemotherapy
A Port
B Catheter [tubing]
C Subclavian vein
D Superior Vena cava
E Pulmonary vein
F Aorta
G Heart
Sid Eff t f Ch th
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
90/167
Side Effects of Chemotherapy
Alopecia or hair loss Nausea and vomiting Mucositis in the
entire gastrointestinal tract Skin changes
Anxiety, sleep disturbance Altered bowel elimination Decreased
mobility
Hematopoietic system changes Bone marrow suppression
Hypersensitivity (esp. taxanes, platinums)
Al i (h i l )
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
91/167
Alopecia (hair loss)
Anthracyclins Etoposide
Irinotecan (Campto)
Cyclophosphamide Taxanes
Ifosphamide
Vindesine
Vinorelbine
Topotecan
Alopecia (hair loss)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
92/167
Alopecia (hair loss)
2-3 days after within a few weeks
3-6 months regain after stopping treatment
baldness may be temporary, partial or
total
Tx
Cold cap
Wig
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
93/167
Cancer-induced nausea and
vomitting
Etiology of Nausea and Vomiting in
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
94/167
gy g
Patients with Cancer
Direct TreatmentRelated:
chemotherapy
- acute - delayed
- anticipatory
- breakthrough N/V
- refractory N/V
radiation therapy
prophylactic
antibiotics
Indirect Treatment Related:
mucositis
opiates
anti-infectives
gastroparesis
infection
hyperacidity
anorexia diarrhea
pain
anxiety
Etiologies of Nausea and
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
95/167
g
Vomiting in Oncology Patients
Chemical (chemotherapy-induced: acute anddelayed; opioids)
Vestibular
CNS (increased intracranial pressure)
Visceral (direct disease-related sources,
abdominal irradiation)
Proposed Pathways for Chemotherapy-
Induced Nausea and Vomiting (CINV)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
96/167
Induced Nausea and Vomiting (CINV)
Increased afferent input to thechemoreceptor trigger zone
and
vomiting center
Chemotherapy
Cell damage
Higher CNS centers
Release of neuroactive agentsActivation of vagus
and splanchnic nerves
Small
intestine
Chemoreceptor trigger zone
Medullaoblongata
Vomiting center
Adapted from Grunberg SM et al N Engl J
Med1993;329:17901796.
CINV: Emetogenic risk
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
97/167
g
CINV: Classification
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
98/167
CINV: Classification
Anticipatory Acute Delayed
Chemo 16 - 24 hours
CINV: A Broad Definition
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
99/167
CINV: A Broad Definition
Anticipatory Early acute
Chemo
Late acute Delayed
16 hours 24 hours
A t CINV D l d CINV
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
100/167
Acute CINV Delayed CINV
No Acute
CINV
No Delayed76%
Delayed
24%
Yes Acute
CINV
No Delayed
20%
Delayed
80%
CINV: Current Problem
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
101/167
CINV: Current Problem
CINV is still a clinical problem do not fully understand the
pathophysiology of
CINV (e.g. acute, delayed)
traditional definition of acute and delayedCINV does not match
the physiology
Appears that:
acute CINV impacts delayed CINV
prevention of acute CINV may help management of
delayed CINV
A t CINV
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
102/167
Acute CINV
Starts within the first24 hours after
chemotherapy administration
Majority of chemotherapeutic agents induce emesis
approximately 13 hours following administration
Most researched type of CINV
Remains common despite dramatically improved
protection
Pisters KMW, Kris MG. In: Principles and Practice of Supportive
Oncology. Lippincott-Raven; 1998. Antiemetic Subcommittee of the
Multinational
Association of Supportive Care in Cancer.Ann
Oncol1998;9:811819.
Delayed Chemotherapy-Induced Nausea
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
103/167
and Vomiting (CINV)
Starts 24 hours or more afterchemotherapy administration
First defined with high doses of cisplatin but known to
occur
with other chemotherapy agents
Carboplatin
Cyclophosphamide
Doxorubicin
Epirubicin
Anthracyclines
Mechanism not known; appears to differ from acute emesis
Berger AM et al. In: Cancer: Principles and Practice of
Oncology. 6th ed. Lippincott Williams & Wilkins, 2001:28692880.
Antiemetic
Subcommittee of the Multinational Association of Supportive Care
in Cancer.Ann Oncol1998;9:811819.
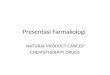
Ci l ti Bi h i P tt f CINV
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
104/167
Cisplatin Biphasic Pattern of CINV
Maximal emetic intensity seen within 24 hours postdose
Distinct second phase seen, occurring on Days 25 postdose
Adapted from Tavorath R, Hesketh PJ Drugs 1996;52:639648. 1996.
Used with permission from Adis International Limited.
Acute Delayed
Time (Days)
Postcisplatin: Differential Involvement
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
105/167
of Neurotransmitters Over Time
Hesketh PJ et al Eur J Cancer2003;39:10741080.
0 8 2412 120
Hours after cisplatin
Substance Pdependentmechanisms
(central)
DELAYED (Days 25)ACUTE (Day 1)
Serotonin-dependent
mechanisms
(peripheral)
Serotonin and 5 HT Receptor Pathway
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
106/167
Serotonin and 5-HT3 Receptor Pathway
First recognized with high-dosemetoclopramide
Development of 5-HT3 antagonists has had
dramatic impact
Highly effective in acute vomiting, less effectivefor delayed
events
Optimal use is with dexamethasone
Primary mechanism of action appears to beperipheral
Berger AM et al. In: Cancer: Principles and Practice of
Oncology. 6th ed. Lippincott Williams & Wilkins; 2001:28692880.
Gralla RJ et al J Clin
Oncol1999;17:29712994. Antiemetic Subcommittee of the
Multinational Association of Supportive Care in Cancer. Ann
Oncol1998;9:811819.
Endo T et al Toxicology2000;153:189201. Hesketh PJ et al Eur J
Cancer2003;39:10741080.
5HT3 Receptor Antagonists
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
107/167
Prototypes:
Ondansetron Granisetron
Dolasetron
Palonosetron
MOA: Inhibition of 5-HT3 receptors on vagalafferent neurons in
GI and in CTZ
Efficacy improved when used with a steroid
Well tolerated, minimal side effects headache
constipation
bradycardia
Half-Life and Binding Affinities of
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
108/167
*Log-scale.In vitro data; clinical significance has not been
established.
5-HT3 Antagonist Half-Life (h) Binding Affinity (pKi)*
Palonosetron (Aloxi) 40.0 10.45
Ondansetron (Zofran) 4.0 8.39
Dolasetron (Anzemet) 7.3 7.60
Granisetron (Kytril) 9.0 8.91
5-HT3
Receptor Antagonists
Substance P
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
109/167
prototypic neuropeptide of the 50 knownneuroactive molecules now
recognized as a member of the tachykinin family
of neurotransmitters
neurokinins are tachykinins found in mammals(substance P, NKA,
NKB)
3 categories of NK receptors NK1 - affinity for substance P
NK2 - affinity for NKA
NK3 - affinity for NKB
currently considered a modulator of nociception,stress, anxiety,
nausea / vomiting
DeVane CL. Pharmacotherapy 2001:21:1061-9
CINV
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
110/167
CINV
Emetic Center
CorticalGI
vestibular
Nausea / Vomiting
CTZ
Neurokinins:
Substance P
CINV: Aprepitant
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
111/167
p p aprepitant (Emend, Merck & Co., Inc.) approved in
the US in 2003 Mechanism of action:
selective, high affinity antagonist of human substance P
atneurokinin 1 (NK
1) receptors interferes with the substance
P pathway that produces N/V no affinity for serotonin (5HT
3), dopamine and corticosteroid
receptors
Indication:
combination with other antiemetics
indicated for the prevention of acute and delayed nausea
and vomiting associated with initial and repeat courses of
highly emetogenic cancer chemotherapy
A it t Ad i i t ti
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
112/167
Aprepitant Administration
Given for three days as part of a regimenthat includes a
5-HT
3antagonist and a
corticosteroid
Recommended dose
125 mg po 1 hour prior to chemotherapy
80 mg daily in the morning on days 2 and 3
Supplied in 125- and 80-mg capsules
Aprepitant: Challenges for Care
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
113/167
Aprepitant: Challenges for Care
Potential drug interactions with anticancermedication
Evaluation of drug interactions should look
at impact beyond 24 hours Potential drug interactions with
other
medications (e.g. chronic)
CINV
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
114/167
CINV
Emetic Center
CorticalGI
vestibular
Nausea / Vomiting
CTZ
Neurokinins:
Substance P DA
5HT
CINV: Triple Upfront Therapy
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
115/167
Rationale: Clinical Guidelines
Guidelines include triple upfront
therapy for highly emetogenic
regimens:
MASCC
NCCN 2007
ASCO 2006
Kris MG, et al. JCO 2006:24:2932
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
116/167
Nausea:
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
117/167
Nausea:
Antiemetics
Diet (avoid fried, fatty foods)
Smaller meals
Diarrhea: Causes
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
118/167
Diarrhea: Causes
Chemotherapy
Infection
Malabsorption
Radiation induced
Clostridium diffecile infection
Diarrhea
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
119/167
Diarrhea
Chemotherapy induced Irinotecan
5-FU (50-80%)
Supportive management
Fluids & Electrolytes
Nutrition
Avoid problem foods and drugs
Medication management Opioids
Loperamide (more effective)
Diphenoxylate
Nephrotoxicity
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
120/167
Nephrotoxicity
Chemotherapy induced nephrotoxicityAlkylating agents
Cisplatin
Ifosfamide
Carmustine Carboplatin
Antimetabolites
Methotrexate
Gemcitabine Other
Mitomycin C
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
121/167
Bladder Toxicity:Hemorrhegic Cystitis
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
122/167
g y
Agents Ifosfamide, cyclophosphamide high dose
acroleinaccumulation in bladder
Clinical presentation
Onset : 2-3 days Hematuria, dysuria
Prevention MESNA + adequate prehydration
Treatment Stop chemo
Hydration
Adequate platelet
CNS Toxicity
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
123/167
CNS Toxicity
Agents MTX (IT or IV)
Cytarabine
Ifosfamide
L-asparaginase
Cisplatin Lhermitts phenomena 5-FU
Taxanes IFN alpha
Vinca alkaloid (wrong route NEVER IT)
Neurotoxicity
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
124/167
Neurotoxicity
High dose cytarabine ataxia L-asparaginase drowsiness,
stupor
Cisplatin ototoxic, ataxia
Etoposide
Vinca alkaloid jaw pain,cranial nerve pulsies
Procarbazine
Metrotrexate acute arachnoiditis
Oxaliplatin sensory neurotoxic (cold triggersymptom
parathesia
Prevention/Treatment chemotherapy
ind ced ne ropath
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
125/167
induced neuropathy
Drug Prevention/ Treatment
Cisplatin Amifostine inj
Ifosfamide Methylene blue
Oxaliplatin Ca-gluconate & Mg sulfate
Paclitaxel Glutamine oral powder
Peripheral Neuropathy
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
126/167
p p y
Sense of touch is distorted- ordinary touch can beunpleasant or
painful.
Burning or prickling feeling without stimulus
Decreased touch sensation
Difficulty sensing the position, location, orientation,and
movement of the body and its parts(Proprioception)
Important to report ANY of these symptoms to healthcare
provider
Colon Cancer Treatment-Progressand Progress, Summer 2005,
Vol.1
Cardiotoxicity
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
127/167
y
Agents Anthracyclines
Cyclophosphamide
5-FU Trastuzumab (Herceptin)
Bevacizumab
Cisplatinin (Platinol)
Anthracyclin induce
cardioto icit
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
128/167
cardiotoxicity
Congestive heart failure (mortality >20%) Risk factors
Cumulative dose (> 450 mg/m2 in Thai)
Dosing schedule
Age (>65 or
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
129/167
prevention and treatement
Avoiding anthracyclines
Lowering cumulative dose
Lowering peak dose
2nd generation anthracyclines (Idarubicin,epirubicin,
mitoxantrone)
Early detection of subclinical
cardiotoxicity(Echocardiography)
Oxygen free radical scavengers vit.E, C,CoQ10
Liposomal formulations
Pulmonary Toxicity
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
130/167
Risk factor Cumulative dose: bleomycin busulfan carmustine,
aldesleukin
Age: bleomycin
Radiotherapy: bleomycin busulfan, mitomycin,cyclophosphamide,
doxorubicin, actinomycin
Oxygen therapy: bleomycin, cyclophosphamide, mitomycin
Prevention Avoid risk factors
Amifostine
Free radical scavenger
Early detection
Treatment Corticosteroids
Diuretics (edema)
Hand-Foot Syndrome
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
131/167
y
Description Local cutaneous reaction
after chemo.
Seen on palms, finger,soles
2-12 days after chemo
Tingling, burning of palms,hand, feet
Pain, peeling
Resolution in 7-14 daysafter stopping medication
Hand-Foot syndrome
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
132/167
y
Common in high dosetherapy, prolonged
infusion, liposomal forms
Agents
Capecitabine Cytarabine
Docetaxel
Daunorubicin
Doxorubicin
5-FU (infusion)
MTX
Management Stop dosing
Topical wound care &
cold cream base
Pain management
Steroid creams
Pyridoxine
Avoid heat andpressure
Hematologic complications
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
133/167
g p
Febrile neutropenia Anemia
Thrombocytopenia
Hematologic Toxicity: Prophylaxis
Recommendations (NCCN 2008 guidelines)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
134/167
Recommendations (NCCN 2008 guidelines)
Prevention & Treatment
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
135/167
Febrile neutropenia Monitor fever (>38.5
C)
ANC < 1.0 x 109 /L
Anemia
Hb < 10 g/dL
Thrombocytopenia
Platelet < 20,000 /mm3
Antibiotics/antifungal/antiviral prophylaxis
(CSF prophylaxis)
Blood transfusion (Epoitin alpha)
Platelet transfusion
Stomatitis and Mucositis
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
136/167
Occurs later in cycle with capecitabine Baking Soda and salt
mouthwash Over the counter (OTC) enzyme containing mouthwash
for dry mouth
OTC dental anesthetic Stomatitis cocktail: 1:1:1 antacid
solution containing
aluminum hydroxide, magnesium
hydroxide/viscouslidocaine/diphenhydramine
National Peer Reviews in Colorectal Cancer, Scientific
Updatesfrom the 30 th annual ONS Meeting, Orlando, Fl. 2005
Stomatitis
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
137/167
Soft toothbrush Mild toothpaste
Mild gargles
Ice cubes Ibuprofen
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
138/167
Monitoring Outcome: The 4 As
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
139/167
Analgesia (pain relief)
Activities of Daily Living (psychosocialfunctioning)
Adverse effects (side effects)
Aberrant drug taking (addiction-related
outcomes)
(Passik and Weinreb, 1998)
Communicating About Pain
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
140/167
Communicate Intensity
Location
What the pain feels like What makes it worse
What helps
Pain Intensity RatingNumerical Rating Scale
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
141/167
Wong-Baker FACES Pain Rating Scales
g
Category Scale
WHO Analgesic
http://www.ganfyd.org/index.php?title=Image:WHO_Analgesic_Ladder.pnghttp://www.ganfyd.org/index.php?title=Image:WHO_Analgesic_Ladder.png
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
142/167
WHO Analgesic
Ladders
Analgesic Classification
http://www.ganfyd.org/index.php?title=Image:WHO_Analgesic_Ladder.pnghttp://www.ganfyd.org/index.php?title=Image:WHO_Analgesic_Ladder.pnghttp://www.ganfyd.org/index.php?title=Image:WHO_Analgesic_Ladder.png
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
143/167
1. Opioids
1. weak/full agonist, partial agonist and mixed
agonist-antagonist (ceiling effect)
2. strong/full agonist (no ceiling effect no maximum
dose)
2. NSAIDs (ceiling effect) good for bone pain
3. Adjuvant analgesic or coanalgesics
1. TCA (amitryptyline) for neuropathic pain
2. Antiepileptics (gabapentin, oxcarbazepine) forneuropathic
pain
3. Steroids for cord compression
4. Bisphosphonates
Concern about analgesics
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
144/167
Opioids Some Should not for chronic use
Meperidine (neurotoxic)
Dextropropoxyphene (toxic)
Buprenorphine (partial agonist)
Nalbuphine (mix ago/antagonist)
Constipation sennosides, bisacodyl, MgOH
N/V
ondansetron Respiratory depression (Naloxone)
Sedation caffeine to resolve
What Not to Fear
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
145/167
Addiction Tolerance (using meds too soon, i.e.,
before I really need them)
Side effects Good treatments exist for nausea, sedation
and a ground breaking treatment will soon be
available for constipation
Pain Treatment
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
146/167
Acute Pain (Somatic and visceral pain)
Morphine bolus or IM morphine
When pain is relieved, off morphine oral weak opioidsor
NSAIDS
Chronic painAround the clock medication opioids (long
acting)
Neuropathic painAmitriptyline (10-75 mg/d) or
Pregabalin (150-600 mg/d)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
147/167
Maintaining Weight and MuscleMass
Cachexia and Nutritional Risk
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
148/167
Nutritional risk (ie, unwanted weight loss), includingcachexia,
is a common and distressing problem inadvanced cancer, affecting up
to 80% of patients (Bruera,1993)
Negatively affects survival as well as quality of life(Delmore,
1993)
Etiologies: abnormal gastrointestinal functioning anorexia from
nausea, anxiety, depression and cognitive
dysfunction metabolic abnormalities caused principally by
cytokines(Keller, 1993)
Cachexia and Nutritional Risk
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
149/167
4 main clinical manifestations of cachexia:Anorexia
Chronic nausea
Asthenia
Change in body image
Pharmacologic treatment of cachexia is targeted
principally at anorexia and chronic nausea (Bruera,1993)
Pharmacological Approaches
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
150/167
The main pharmacologic approachesinclude:
Corticosteroids
Progestational agents (ie, megestrol acetate)
Cannabinoids (ie, dronabinol)
Antihistamines (ie, cyproheptadine)
Unique agents (ie, hydrazine sulfate)
Omega-3 fatty acids,EPA and
docosahexaneoic acid (DHA) (n-3s) (Barber, et al,2000; Hussey
& Tisdale, 1999; Wigmore, et al, 2000)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
151/167
Fatigue and Chemobrain
Fatigue
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
152/167
Highly prevalent effecting 2/3s ofpatients
Very disabling
Also makes the job of caregiving morestressful and exhausting
for family
Fatigue what works?
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
153/167
Exercise Modifications in diet
Stimulant medications
Acneform Rash
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
154/167
Pharmacologic Mgmt.
Topical and/or
antibiotics
Topical and/or oral
antihistamines
Cool compresses
Petroleum jelly, silver
sulfadiazine ointment
for ulcerative lesions
Avoid sun, heat &
humidityUse mild soapsWater based makeup is
generally well tolerated
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
155/167
Multiple white bands in the nails,
representing periods of growth
arrest, in this case due to cycles
of treatment with 5-fluorouracil.
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
156/167
Oncologic Emergency
Oncologic Emergencies
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
157/167
Sepsis and disseminated intravascularcoagulation
Collaborative management includes: Prevention (the best
measure)
Intravenous antibiotic therapy
Anticoagulants, cryoprecipitated clottingfactors
Spinal Cord Compression
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
158/167
Tumor directly enters the spinal cord orthe vertebrae collapse
from tumor
degradation of the bone.(Continued)
Spinal Cord Compression(Continued)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
159/167
( )
Collaborative management includes: Early recognition and
treatment
Palliative
High-dose corticosteroids High-dose radiation
Surgery
External back or neck braces to reducepressure in the spinal
cord
Hypercalcemia
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
160/167
Occurs most often in clients with bonemetastasis
Fatigue, loss of appetite, nausea and
vomiting, constipation, polyuria, severemuscle weakness, loss of
deep tendon
reflexes, paralytic ileus, dehydration,
electrocardiographic changes
(Continued)
Hypercalcemia (Continued)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
161/167
Collaborative management includes: Oral hydration
Drug therapy
Dialysis
Superior Vena Cava Syndrome
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
162/167
Superior vena cava is compressed orobstructed by tumor
growth.
Condition can lead to a painful, life-
threatening emergency. Signs include edema of face, Stokes
sign, edema of arms and hands,
dyspnea, erythema, and epistaxis.
(Continued)
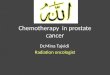
Figure 1 Photographs of the patient showing the reduction in
swelling of the
f k d t iti
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
163/167
face, neck and upper extremities
Chee CE et al. (2007) Superior vena cava syndrome: an
increasingly frequent complication
of cardiac procedures
Nat Clin Pract Cardiovasc Med4: 226230
doi:10.1038/ncpcardio0850
Superior Vena Cava Syndrome(Continued)
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
164/167
Late-stage signs include hemorrhage,cyanosis, change in mental
status,
decreased cardiac output, and
hypotension.
Collaborative management includes high-
dose radiation therapy, but surgery onlyrarely.
Tumor Lysis Syndrome
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
165/167
Large numbers of tumor cells aredestroyed rapidly, resulting
in
intracellular contents being released
into the bloodstream faster than thebody can eliminate them.
Collaborative management includes:
Prevention Hydration
Drug therapy (Allopurinol)
Conclusions
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
166/167
People with cancer are living longer The focus is on quality of
life in addition to
quantity
People surviving cancer want to live normal lives
People with cancer have multiple symptoms
New treatments of various kinds are available
and there is no need to suffer
-
7/30/2019 Cancer Chemotherapy Lecture [Dr. Edy]
167/167