Embed Size (px)
Citation preview

Canadian Nosocomial Infection Surveillance Program (CNISP) Overview, HAI case definitions & rates
Healthcare-Associated Infections (HAI) Section Surveillance and Epidemiology Division (SED)
Centre for Communicable diseases and Infection Control (CCDIC) Public Health Agency of Canada (PHAC)
February 10, 2015 SAEIG, IPAC

Linda Pelude Senior Epidemiologist Healthcare-Associated Infections Section - CNISP Centre for Communicable Diseases and Infection Control Public Health Agency of Canada/Agence de la santé publique du Canada 613 854 5186 [email protected] [email protected]
Ottawa, ON Canada

Canadian Nosocomial Infection Surveillance Program (CNISP) established in 1994, collecting data since 1995
62 hospitals in 10 provinces
Partnership between
Public Health Agency of Canada
Centre for Communicable Disease and Infection Control (CCDIC), PHAC
Healthcare Associated Infections, CCDIC (Ottawa), PHAC
National Microbiology Laboratory (Winnipeg), PHAC
AND
Canadian Hospital Epidemiology Committee (CHEC), AMMI-Canada

Geographic Location Of CNISP Hospitals
Adult or mixed Adult/Pediatric HospitalsPediatric Hospitals (stand- alone)

Burden of HAIs in Canada
• HAIs cause significant morbidity & mortality in hospitalized patients, with considerable economic burden.
1 in 12 adults & 1 in 10 children admitted to a Canadian hospital will develop a HAI
Approximately 220,000 Canadians suffer from HAIs each year & approximately 8,000 deaths occur.
Risk of dying following an episode of CDI is 6%
• Annual healthcare costs for HAIs are significant: CDI ($46.1M), MRSA ($36.3M), surgical site infections ($24M)
• Vulnerable populations are at increased risk for HAIs (elderly, infants, immuno-suppressed individuals, those undergoing multiple medical procedures)
5
Healthcare-Associated Infections

CNISP Objectives
establish and maintain ongoing national surveillance system to determine the epidemiology of nosocomial infections in Canadian hospitals
establish “benchmark” data
provide data that can be used to develop national guidelines for infection prevention and control

CNISP
• collaborative network of hospitals and PHAC; good geographic representation; lab, epidemiologic, and statistical expertise
• national, regional and site-specific rates
• ability to link epidemiologic and lab data
• able to distinguish infection vs colonization

CNISP Hospitals
• predominantly teaching hospitals, with required expertise
and commitment
• However, mostly tertiary-care teaching hospitals; few
community hospitals
• Recently evaluated representativeness of CNISP

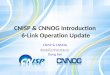
Map of Canada - CNISP hospitals in green with 100 km buffers (white) Population mapped by census division using a colour gradient: Darker shade = higher population
Approximately 78 % of the Canadian population lives
within 100 km of a CNISP site

CNISP….
• Provides good geographical coverage, EXCEPT in northern Canada
• Represents regions where most Canadians live
• Represents large, tertiary care centres in cities, but NOT smaller community hospitals in rural areas - CNISP rates should be interpreted with caution by smaller hospitals seeking a benchmark

CNISP Limitations
mostly tertiary-care teaching hospitals; few community hospitals; no Northern hospitals
significant workload at hospital sites
CNISP Achievements
only national surveillance system in Canada collecting epidemiologic and
linked microbiology data regarding HCA infections
network of hospitals that has worked in partnership with PHAC/NML since
1995
has provided Canadian “benchmark” data for a variety of infections

CNISP core surveillance projects
MRSA, VRE, CDI,
Central venous catheter associated blood stream infections (CVC-BSI)
Carbapenem-Resistant Gram-Negative Enterobacteriaceae
In addition,
3 SSI surveillance projects
Pediatric Cardiac surgical site infections
CSF shunt surgical site infections
Knee & Hip surgical site infections
Antimicrobial Utilization data (Hospital pharmacies)
Periodic point-prevalence surveys of HCA infection

CNISP Surveillance
• Each CNISP surveillance project has a working group comprised of CHEC and PHAC members
• working groups direct the development and implementation of surveillance projects including the development of case definitions
• CHEC members participate voluntarily in CNISP by collecting standardized, case-by-case, non-nominal data on hospitalized patients at risk of HAI
• Data submitted to PHAC for compilation and analysis
• all data is analyzed by region or larger geographical area
• at no time is data reported by individual hospital or site

CNISP Protocols include
• Methodology
• Case definitions
• Patient identification and data collection
• Patient population (inclusion & exclusion criteria)
• Outcome measures
• Analysis
• Workload
• Ethics

CNPHI on-line data entry system • Currently MRSA, VRE, CDI & CVC-BSI on-line

16
Any CNISP module is accessed from the CNISP surveillance ‘dashboard’
CNPHI – CNISP Surveillance

17
This the MDS Option form
Questions ‘explained’ by hovering the mouse over the ? Applicable to all CNISP CNPHI modules

In 2013, CNISP conducted an analysis of Case Definitions and Surveillance Methodologies in Use by National and International Stakeholders
HAI case definitions used by Canadian provinces and territories, as well as select Canadian non-governmental organizations (Accreditation Canada, Canadian Patient Safety Institute (CPSI)), international agencies, (CDC-NHSN, ECDC), and international governments (Australia and Germany) for a total of 19 other case definitions that were examined. The case definitions and surveillance methodologies used by these stakeholders were identified for eight CNISP surveillance projects MRSA, CDI, VRE, CRE, SSIs, CVC-BSI

CNISP MRSA case definition 2015 Isolation of Staphylococcus aureus from any body site AND resistance of isolate to oxacillin AND patient must be admitted to the hospital AND is a "newly identified MRSA case" at a CNISP hospital at the time of hospital admission or identified during hospitalization
Classified as HA based on following criteria and best judgement of practitioner • Exposure to any healthcare setting (including LTC facilities or clinics) in previous 12 months OR pt is on calendar day
3 of their hospitalization (Calendar day 1 is day of hospital admission)
CNISP MRSA surveillance
Of the 19 agencies/organizations examined – • 8 have comparable case definitions to CNISP (BC, AB, MB, NB, NF, NHSN/CDC, Germany)
Differences include slight deviations in the time elapsed since admission (48-72 hrs) for classification as HA (most commonly identified minor difference.) • 7 have major differences in case definitions compared to CNISP (SK, ON, QC, NS, CPSI, ECDC, Australia)
Major differences include surveillance usually restricted to only MRSA bacteremia or CSF and population-based surveillance compared to hospital-based surveillance
Case definitions could not be retrieved for 4 agencies/organizations (NWT, NU, YK, ACC Canada)

BC – Not notifiable Minor differences
Classification of HA MRSA must be detected after 3 calendar days of hospitalization to be classified as HA, or pt must have been hospitalized for more than 3 calendar days within the last 12 months)
Additional criteria for identification of MRSA (molecular testing and PCR are included in BC definition)
AB - Notifiable Minor differences
Classification of HA MRSA strain must be detected 72 hours after admission to be classified as HA) Case definition not unique to MRSA, rather for all AROs
SK - Notifiable Major differences
No case definition for identifying MRSA cases in an acute care setting Surveillance is population-based
MB - Notifiable No difference
ON - Not notifiable Major differences
Surveillance is only for MRSA bacteremia (detection based on positive blood culture as opposed to isolation from any site)
Classification of HA MRSA strain must be detected 72 hours after admission to be classified as HA
QC - Notifiable Major differences
Surveillance is only for SA bacteremia (case finding based on positive blood culture as opposed to isolation from any site)
Strain of SA may be resistant to methicillin or oxacillin
NS - Notifiable Major differences
Surveillance is based solely on laboratory identification of MRSA
Unknown whether cases are differentiated by site of acquisition in NS
NB - Notifiable Minor difference
No specification for time elapsed since admission to be considered HA
NF - Notifiable Minor difference
There is a case definition for both HA infected and colonized cases
PEI - Notifiable Minor difference PEI definition differentiates between HA nosocomial and non-nosocomial
NWT, NU, YK - MRSA notifiable in NWT & YK – UNK in Nunavut
Unable to obtain case definitions for NWT, NU, YK
CNISP compared to provinces

CNISP CDI surveillance
Surveillance case definition for primary episodes of CDI
“Primary” CDI = first episode of CDI ever experienced by the patient OR a new episode of CDI occurring > than 8 weeks after previous confirmed case of CDI in the same patient, i.e. after the first C.difficile toxin-positive assay or PCR test.
A patient is identified as having CDI if: Have diarrhea* or fever, abdominal pain and/or ileus AND a laboratory confirmation of a positive toxin assay or positive PCR for C. difficile (without reasonable evidence of another cause of diarrhea?) OR Have diagnosis of pseudomembranes on sigmoidoscopy or colonoscopy (or after colectomy) or histological/pathological diagnosis of CDI OR Diagnosed with toxic megacolon (in adult patients only)
*Diarrhea defined as one of the following: 6 or more watery stools in 36-hour period; 3 or more unformed stools in 24-hour period and this is new or unusual for the patient (in adult patients only)
NOTE: If the information about the frequency and consistency of diarrhea is not available, a toxin-positive stool or positive PCR will be considered as a case.
Of the 19 agencies/organizations examined – • 1 is identical (NS)
• 10 have comparable case definitions to CNISP (BC, AB, SK, MB, ON, QC, NF, PEI, ECDC, Germany)
Differences include slight deviations in the time elapsed since admission for classification as HA (most commonly identified minor difference.)
• 2 have major difference in case definitions compared to CNISP (NHSN/CDC, Australia)
Major difference is the case definitions which relies exclusively on positive laboratory assays
case definitions could not be retrieved for 6 agencies/organizations (NB, NWT, NU, YK, ACC Canada, CPSI)

In 2015 added criteria to differentiate between…
HA – your facility = admitted ≥ 3 days HA- another healthcare facility = admitted < 3 days but known to have been in another healthcare facility & CA-CDI = pt seen in ER with +ve CDI lab OR CDI occurs < 3 days after admission
Also trying to pick up recurrent cases of CDI = occurs ≤ 8 weeks after primary episode providing initial treatment was successful
CNISP CDI surveillance
These definitions are based on practice recommendations by SHEA/IDSA in 2014 and adopted by the NHSN/CDC
‘Strategies to Prevent Clostridium difficile Infections in Acute Care Hospitals: 2014 Update’
ICHE vol 36: 6, June 2014
Available at URL : http://www.jstor.org/stable/10.1086/676023?origin=JSTOR-pdf

CNISP VRE surveillance
CNISP VRE case definition 2015 Isolation of Enterococcus faecalis or faecium AND Vancomycin MIC ≥ 8 ug/ml AND Patient is admitted to the hospital AND Is a "newly” identified VRE infection or colonization at a CHEC facility at the time of hospital admission or identified during hospitalization VRE infection is determined using the January 2015 CDC NHSN definitions/criteria for infections, and in accordance with the best judgment of the ICP. These criteria should be met at the time of the culture that yielded VRE, or within 72 hours of the culture. The NHSN definitions/criteria can be accessed at URL: www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf
Of the 19 agencies/organizations examined –
• 1 has a comparable case definitions to CNISP (QC) Differences include slight deviations in the time elapsed since admission for classification as HA (most commonly identified minor difference.)
• 9 have major difference in case definitions compared to CNISP (AB, SK, MB, ON, QC, NS, PEI, ECDC, Germany , NHSN/CDC)
Major differences include case definitions that are not specific to VRE, but rather pertain to AROs more broadly; population - based surveillance; surveillance limited to VRE bacteremia; and additional criteria for classification as healthcare-associated
case definitions could not be retrieved for 9 agencies/organizations (BC, NB, NF, NWT, NU, YK, ACC Canada, CPSI, Australia)

CNISP CVC-BSI surveillance
ONLY CVC-associated BSIs related to an ICU admission are to be reported.
BSI case definition: Criterion 1: Recognized pathogen cultured from at least 1 blood culture, unrelated to infection at another site. OR Criterion 2: At least one of: fever (>38°C core), chills, hypotension (if aged < 1 year: fever (>38°C core), hypothermia (<36°C core, apnea, or bradycardia) AND common skin contaminant cultured from 2 blood cultures drawn on separate occasions and positive laboratory results are unrelated to infection at another site.
2. CVC-associated BSI: A laboratory-confirmed BSI where a CVC or UC in place for >2 calendar days on the date of the positive blood culture with day of device placement being Day 1 AND A CVC or UC was in place on the date of the positive blood culture or the day before. If a CVC or UC was in place for >2 calendar days and then removed, the BSI criteria must be fully met on the day of discontinuation or the next day. If the patient is admitted or transferred into the ICU with a CVC in place and that is the patient’s only CVC, day of first access is considered Day 1
ICU-related: CVC-BSI onset during ICU stay or within 2 calendar days of leaving ICU Exclusions: Infection already present on admission to ICU and/or BSI in neonate < 48 hours old, unless epidemiologic evidence indicates acquisition in the neonatal ICU (e.g., procedure-associated; known endemic neonatal ICU strain)
Of the 19 agencies/organizations examined – • 2 have identical case definition (AB, Australia) • 5 have a comparable case definitions to CNISP (ON, CPSI, CDC/NHSN, ECDC, Germany) Differences include slight deviations in the time elapsed since admission for classification as HA (most commonly identified minor difference.)
• 1 has major difference in case definitions compared to CNISP (QC,) Different criteria for CVC-BSI, no time criteria for CVC-associated BSI, no definition of ICU-related • 5 do not conduct surveillance for CVC-BSI (BC, SK, NS, NF, PEI Case definitions could not be retrieved for 6 agencies/organizations (MB, NB, NWT, NU, YK, ACC Canada)

.
CNISP CRGN surveillance
CNISP CRGN case definition: Laboratory confirmation of carbapenem resistance/carbapenem reduced susceptible in specified Gram negative organisms in Enterobacteriacae and Acinetobacter spp.
At least ONE
of the
following:
Enterobacteriaceae:
At least ONE
of the
following:
Acinetobacter:
MIC (μg/ml) Disk diffusion
(mm) MIC (μg/ml)
Disk diffusion
(mm)
Imipenem > 2 < 22 Imipenem > 4 < 21
Meropenem > 2 < 22 Meropenem > 4 < 17
Doripenem > 2 < 22 Doripenem > 4 < 17
Ertapenem > 1 < 21
Each time an eligible Enterobacteriacae or Acinetobacter spp. is identified by the NML as harbouring a carbapenemase, the NML will send the results via email to the site and the site will complete a Patient Questionnaire for this specimen.
Of the 19 agencies/organizations examined – • 1 has a comparable case definition to CNISP (QC) include only Enterobacteriaceae strains • 5 have major difference in case definitions compared to CNISP (AB, MB, NHSN/CDC, ECDC, Germany) Include other AROs (ESBLs, Pseudomonas), lab criteria not included in case definition • 6 do not conduct surveillance for CVC-BSI (BC, ON, SK, NS, NF, PEI)
Case definitions could not be retrieved for 7 agencies/organizations (NB, NWT, NU, YK, ACC Canada, CPSI, Australia)

Knee & hip SSI Inclusions: Primary total and hemiarthroplasties will be included in the surveillance and only clean procedures will be included in the surveillance. Exclusions: Revisions and resurfacings, surgeries in which the patient died in the OR, within 24 hours of surgery, where the skin incision is not entirely closed at procedure’s end are excluded from the surveillance. Infections that develop within 90 days (3 months) of procedure will be included and reported retrospectively based on the date of procedure. 8 agencies/organizations had a SSI case definition 2 had identical definition 5 had similar case definitions 1 had major difference - no classification of surgery (i.e. superficial, deep, organ) Most commonly recorded minor difference related to discrepancies in the time elapsed between the operative procedure and clinical presentation of infection. 6 agencies/organizations were identified as not having a case definition of SSI Case definition for 5 agencies/organizations could not be retrieved.
CNISP SSI surveillance

Case definitions for pediatric cardiac surgery could not be identified for any of the stakeholders examined
Case definitions for CSF shunt infection could only be identified for two of the agencies/organizations (NHSN/CDC, ECDC) examined and major discrepancies were noted that render their respective surveillance data incomparable to that of CNISP – classified as CNS infections

28
CNISP HAI rates
The following tables provide a summary of rates and trends for CNISP surveillance activities. Annual incidence rates were calculated using patient admissions, and patient-days The territories do not currently submit data to the Agency and Prince Edward Island only began submitting data in 2011

3 kinds of rates are used in HAI surveillance
Rate An expression of probability of occurrence of an event = (x/y)*k
x = numerator: number of times event occurred during a specified time period y = denominator = population from where event was occurring k = base number (e.g. 100, 1,000 or 10,000) that is used to express the rate
Multiplying by 100 is used for proportions or percents
egs, 1 case per 4 pts = 25% ill
2 SSI per 84 surgical procedures = 0.024 or 2.4%
Multiplying by 1000 is used to present (compare) patient admissions
1853 MRSA infections and 848,512 pt adm = 2.18 per 1,000 pt adm
Multiplying by 10,000 is used to present (compare) patient days
1853 MRSA infections and 6,516,081 pt days =2.84 per 10,000 pt days

Number of HA-CDI cases and incidence rate per 10,000 patient days
Rate per 10,000 patient days by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
2009 907 6.68 1,401 5.91 175 3.23 2,483 5.81
2010 1,282 6.82 1,589 6.67 155 2.27 3,026 6.12
2011 1,241 5.77 2,075 7.86 101 2.88 3,417 6.65
2012 1,282 5.71 1,997 7.14 203 2.80 3,482 6.04
2013 1,203 4.86 1,730 5.82 228 3.04 3,161 5.10
Number of MRSA infections and incidence rate per 10,000 patient days
Rate per 10,000 patient days by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
2009 962 4.85 852 3.23 219 2.90 2,033 3.78
2010 898 3.87 846 3.05 247 3.24 1,991 3.40
2011 891 3.56 720 2.26 246 2.82 1,857 2.83
2012 844 3.30 703 2.35 240 2.87 1,787 2.80
2013 901 3.42 740 2.48 212 2.34 1,853 2.88

Number of healthcare-associated MRSA infections and incidence rates per 10,000 patient days*
Rate per 10,000 patient days by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
607 3.06 575 2.18 196 2.60 1,278 2.56
562 2.42 563 2.03 202 2.65 1,327 2.26
558 2.23 486 1.53 217 2.49 1,261 1.92
517 2.02 382 1.28 213 2.55 1,112 1.74
556 2.11 398 1.34 184 2.03 1,138 1.75
Number of community-associated MRSA infections and incidence rates per 1,000 patient admissions
Rate per 1,000 patient admissions by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
2009 270 0.95 180 0.54 6 0.07 456 0.65
2010 299 0.88 175 0.44 26 0.31 500 0.61
2011 303 0.89 150 0.37 15 0.16 468 0.56
2012 309 0.89 216 0.56 14 0.15 539 0.65
2013 322 0.89 211 0.54 23 0.23 556 0.66

Number of MRSA bacteremia infections and incidence rates per 10,000 patient days
Rate per 10,000 patient days by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
2009 112 0.56 232 0.88 43 0.57 387 0.72
2010 113 0.49 174 0.63 45 0.59 332 0.57
2011 139 0.56 185 0.58 46 0.53 370 0.56
2012 116 0.45 164 0.55 45 0.54 325 0.51
2013 130 0.49 195 0.65 43 0.48 368 0.56
All-cause mortality rate 30 days after date of positive culture per 100 MRSA bacteremia cases
Number of death * All-cause mortality rate per 100 MRSA-
BSI cases
* All-cause mortality rate based on the number of cases with associated 30-day outcome data.
2009 94 24.4
2010 74 22.4
2011 102 27.8
2012 71 22.0
2013 92 25.1

Number of MRSA bacteremia infections and incidence rates per 10,000 patient days
Rate per 10,000 patient days by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
2009 112 0.56 232 0.88 43 0.57 387 0.72
2010 113 0.49 174 0.63 45 0.59 332 0.57
2011 139 0.56 185 0.58 46 0.53 370 0.56
2012 116 0.45 164 0.55 45 0.54 325 0.51
2013 130 0.49 195 0.65 43 0.48 368 0.56
All-cause mortality rate 30 days after date of positive culture per 100 MRSA bacteremia cases
Number of death * All-cause mortality rate per 100 MRSA-
BSI cases
* All-cause mortality rate based on the number of cases with associated 30-day outcome data.
2009 94 24.4
2010 74 22.4
2011 102 27.8
2012 71 22.0
2013 92 25.1

Number of VRE infections and incidence rates per 10,000 patient days
Rate per 10,000 patient days by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
2009 107 0.54 61 0.23 2 0.03 170 0.32
2010 213 0.92 63 0.23 0 0 276 0.47
2011 231 0.92 193 0.61 3 0.03 427 0.65
2012 223 0.87 166 0.56 3 0.04 392 0.62
2013 160 0.76 157 0.49 7 0.08 324 0.53
Number of CPOs and incidence rates per 10,000 patient days*
Rate per 10,000 patient days by region
Western Central Eastern Overall
No.cases Rate No.cases Rate No.cases Rate No.cases Rate
2010 10 0.09 25 0.17 0 0 35 0.10
2011 4 0.03 61 0.29 0 0 65 0.16
2012 12 0.10 41 0.16 1 0.01 54 0.12
2013 23 0.11 41 0.13 1 0.01 65 0.11

CVC-BSI - Adult ICUs 2006 2009 2010
2011
National all CVC-BSI reported 264 291 192 159
CVC-BSI eligible* (CVC-days) 210 223 158 142
Rate per 1,000 CVC-days (95%CI) 1.78 1.54 1.13 0.94
Number of ICUs† 36 37 40 41
West all CVC-BSI reported 58 54 43 41
CVC-BSI eligible (CVC-days) 29 50 42 39
Rate per 1,000 CVC-days (95% CI) 0.73 1.11 0.95 0.86
Number of ICUs 13 14 17 13
Central all CVC-BSI reported 180 190 131 98
CVC-BSI eligible (CVC-days) 155 141 98 88
Rate per 1,000 CVC-days (95% CI) 2.38 1.70 1.14 1.00
Number of ICUs 17 16 17 18
East all CVC-BSI reported 26 47 18 20
CVC-BSI eligible (CVC-days) 26 32 18 15
Rate per 1,000 CVC-days (95% CI) 2.04 1.87 1.80 0.85
Number of ICUs 6 7 6 10

Approximately 1 in 10 adults and 1 in 12 children contract a HAI while in an acute care hospital C. difficile–associated diarrhea and MRSA, are associated with considerable illness, hospital readmissions and deaths Costs associated with MRSA in Canadian hospitals have been estimated between $42 & $59 million annually A large national surveillance project found that, on average, a hospital is likely to have 10 readmissions each year, at a total estimated hospital cost of $128,200, from patients developing HA - C. difficile–associated diarrhea after discharge. Patients who develop HAI tend to stay longer in hospital (~2.5 times longer than uninfected patients)
Why Are HAI an Important Patient Safety Concern?
Source CIHI , Oct 30, 2008 Patient Safety in Ontario Acute Care Hospitals: A snapshot o of Hoapital-Acquired Infection Control Policies

While prolonged hospitalization and immunosuppression may contribute to the risk that an individual will contract an infection, research shows that implementing and adhering to infection control practices can reduce such risks and significantly decrease rates of HAIs Such practices include: • hand hygiene policies and compliance, • screening • surveillance of infections • isolation and decontamination of infected patients and health care workers
Source CIHI , Oct 30, 2008 Patient Safety in Ontario Acute Care Hospitals: A snapshot o of Hoapital-Acquired Infection Control Policies

Surveillance is considered an essential component of
infection prevention and control.
Purpose
• report various kinds of rates using a routine & orderly
collection of data
• based on standard definitions of cases

If carried out in a uniform manner, surveillance provides
• measure of the burden of illness
• establishes benchmark rates for internal and external comparisons
• identifies potential risk factors
• allows assessment of specific interventions
Surveillance for HA infections is considered an important measure of quality of patient care.

CNISP • contributes to scientific medical literature (publications; abstracts)
• has established and currently maintains ongoing national surveillance
system to determine the epidemiology of HAI in Canadian hospitals
• provides Canadian hospitals with “benchmark” data
• provides evidence-based data for Canadian infection prevention and
control guideline preparation
• raises public awareness of important infection control issues relating to
MRSA, CDI, VRE, other Antimicrobial resistant organisms (AROs) and
device-related HAIs such as CVC-BSI, Hip & knee SSIs, CSF SSI, Peds
Cardiac SSI