Embed Size (px)
Citation preview
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
A patient with pneumonia visited a health care centre for treatment and was admitted to the hospital. After 10 days of admission, this patient developed UTI. In this case, all of the following could be the most probable source of infection except:
a) Patient visitors
b) Hospital staffs
c) Hospital devices used in the process of treatment
d) His home place
Shyam Kumar Mishra
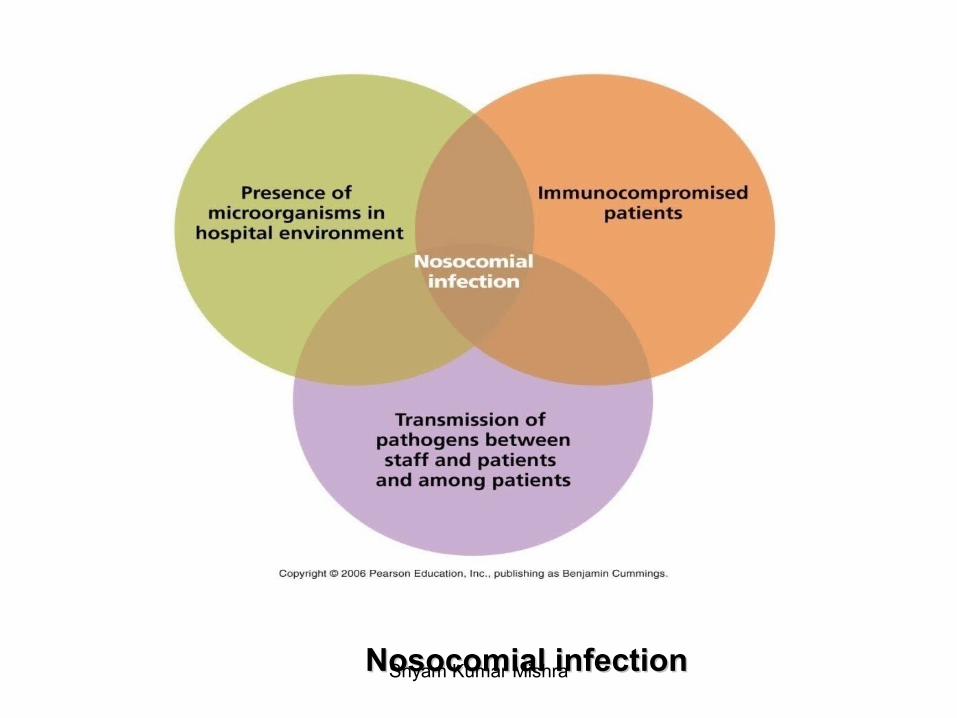
Nosocomial infection
Shyam Kumar MishraAssistant Professor,Institute of Medicine
Shyam Kumar Mishra
Etymology
- In Greek, nosocomialis = hospital
Nosokomos (nosos = disease, komeo = to take care of)
• Related to hospital, so it is also termed as ‘Hospital Acquired Infection (HAI)’
• Now, new term ‘’Health-care associated infection’’
Shyam Kumar Mishra
Nosocomial infection
Any clinically recognizable microbiologic disease that affects the patients as a consequences of his being admitted to the hospital or attending for treatment or acquired from hospital staff as a consequence of their works whether or not the symptoms of disease appear while the affected person is in the hospital (WHO).
A localized or systemic condition that results from adverse reaction to the presence of an infectious agent(s) or its toxin(s) and that was not present or incubating at the time of admission to the hospital. (Center for Disease Control)
Shyam Kumar Mishra
• Those infections which are a result of treatment in a hospital or hospital like setting but secondary to the patients' original condition. Infections are considered nosocomial if they first appear 48 hours or more after hospital admission or within 30 days after discharge.
• For most bacterial nosocomial infections usually become evident after 48 hours (i.e., the typical incubation period) or more after admission. However, because the incubation period varies with the type of pathogen and to some extent with the patient's underlying condition, each infection must be assessed individually for evidence that links it to the hospitalization.Shyam Kumar Mishra
History
Dr. Ignaz Semmelweis
Shyam Kumar Mishra
Florence Nightingale
• At 1863 established the importance principle of nursing, hospital design and hygiene.
• Quoted remark in her book Notes on Hospitals.
Shyam Kumar Mishra
Joseph Lister
Father of antiseptic surgery
Shyam Kumar Mishra
Even today,HAI has been the problem both in developed and developing world. Its' explanation could be any one or more of the following:
• Hospitals receive large numbers of sick people and whose immune systems are often in a weakened state.
• Medical staff move from patient to patient without washing their hands in-between, providing a way for pathogens to spread.
• Many medical procedures bypass the body’s natural protective barriers.
• Unnecessary use of antimicrobial agents in hospitals creates selection pressure for the emergence of resistant strains
• Other factors like hospitals age, infrastructure repairs and renovations will create risks of airborne diseases caused by dust and spores released during demolition and construction.
Shyam Kumar Mishra
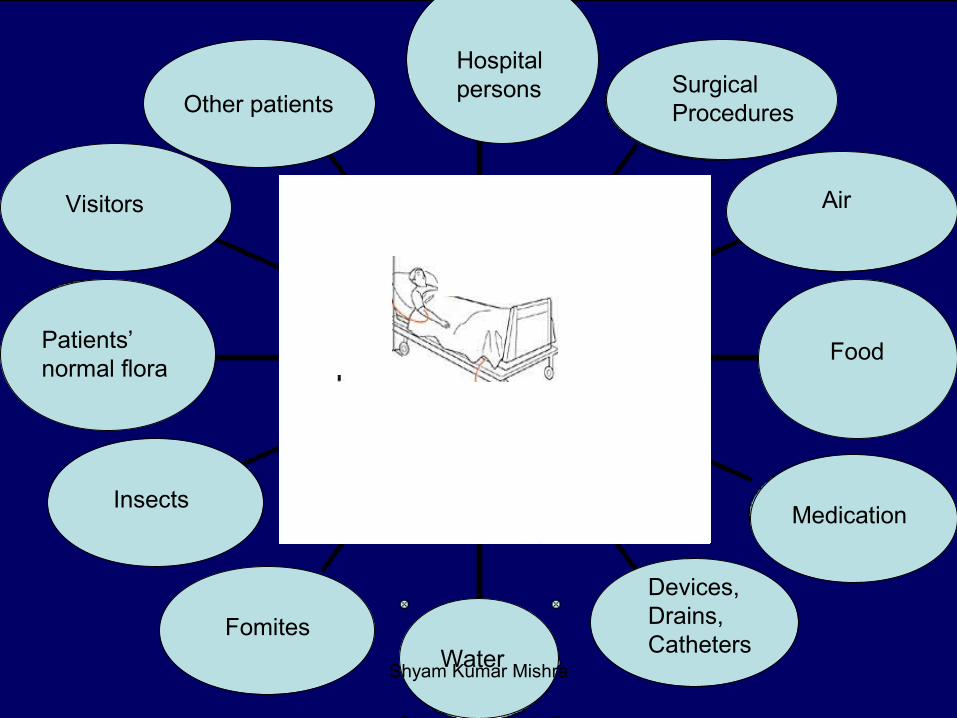
Hospital persons Hospital
personSurgicalProcedures
Air
Food
Medication
Devices,Drains,Catheters
WaterFomites
Insects
Patients’ normal flora
Visitors
Other patients
Shyam Kumar Mishra
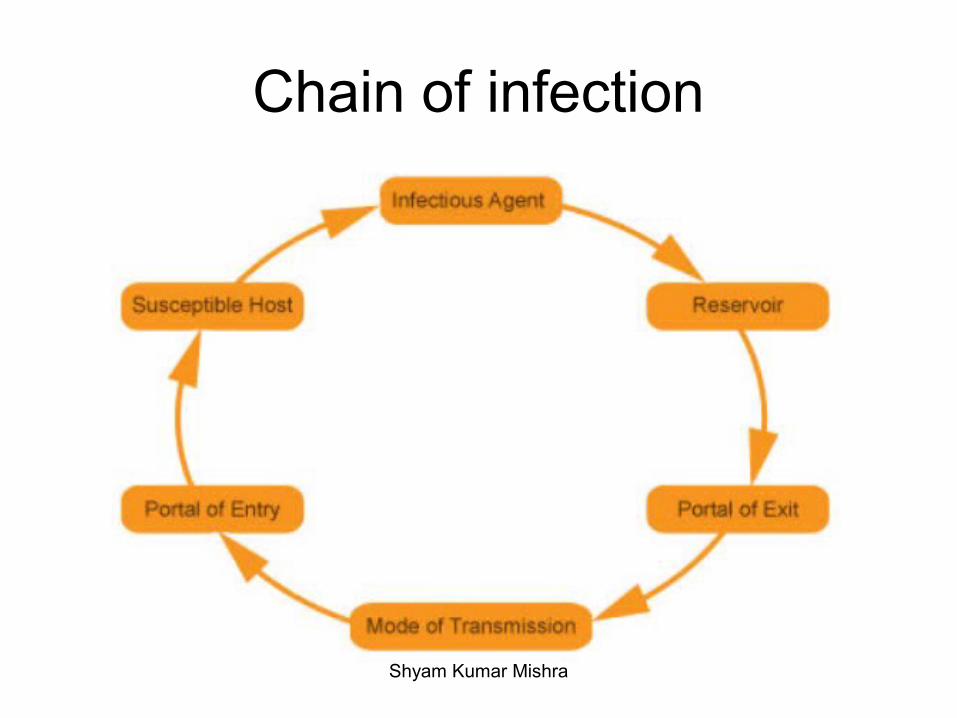
Chain of infection
Shyam Kumar Mishra
Nosocomial infectionNosocomial infectionShyam Kumar Mishra
Shyam Kumar Mishra
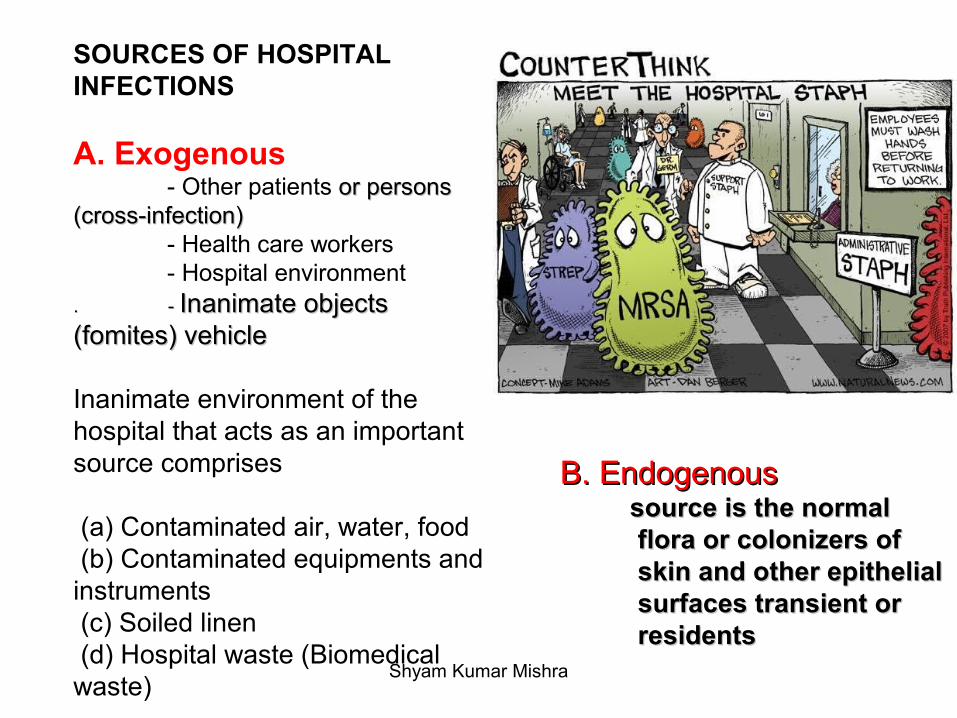
SOURCES OF HOSPITAL INFECTIONS
A. Exogenous - Other patients or persons or persons (cross-infection) (cross-infection) - Health care workers - Hospital environment. - . - Inanimate objects Inanimate objects (fomites) vehicle (fomites) vehicle
Inanimate environment of the hospital that acts as an important source comprises
(a) Contaminated air, water, food (b) Contaminated equipments and instruments (c) Soiled linen (d) Hospital waste (Biomedical waste)
B. EndogenousB. Endogenous source is the normal source is the normal
flora or colonizers of flora or colonizers of skin and other epithelial skin and other epithelial surfaces transient or surfaces transient or residentsresidents
Shyam Kumar Mishra
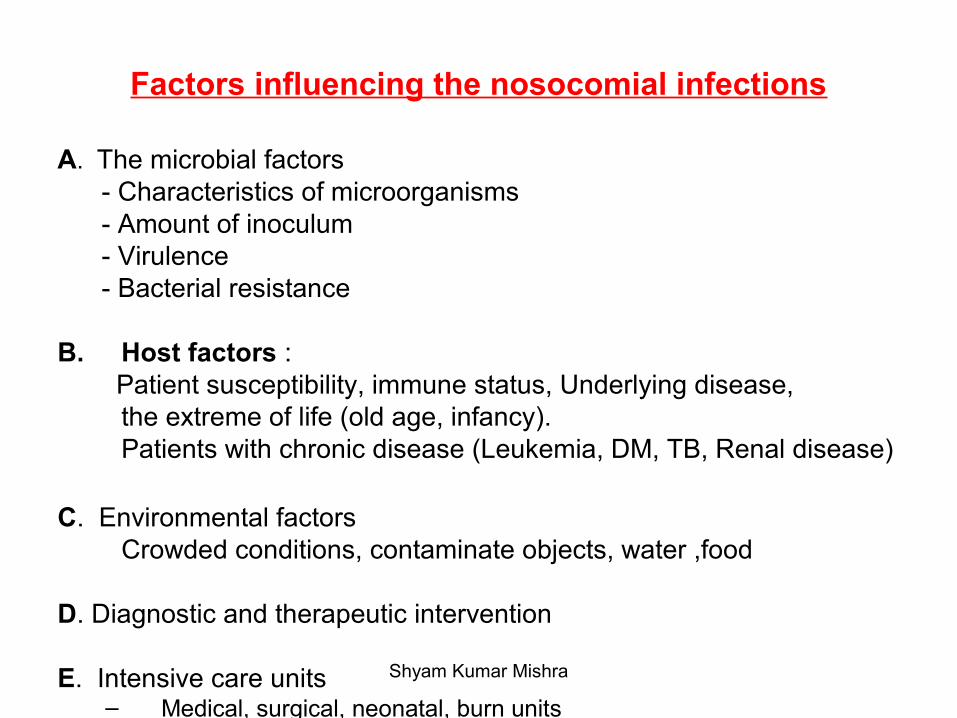
Factors influencing the nosocomial infections
A. The microbial factors - Characteristics of microorganisms - Amount of inoculum - Virulence - Bacterial resistance B. Host factors : Patient susceptibility, immune status, Underlying disease,
the extreme of life (old age, infancy).Patients with chronic disease (Leukemia, DM, TB, Renal disease)
C. Environmental factors Crowded conditions, contaminate objects, water ,food
D. Diagnostic and therapeutic intervention
E. Intensive care units– Medical, surgical, neonatal, burn units
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
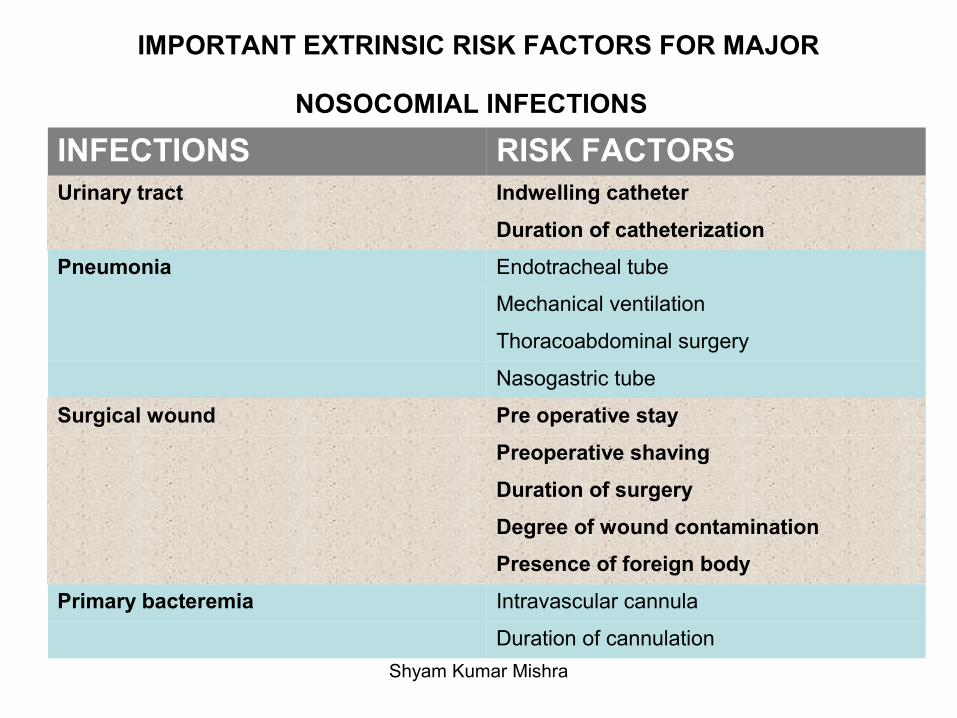
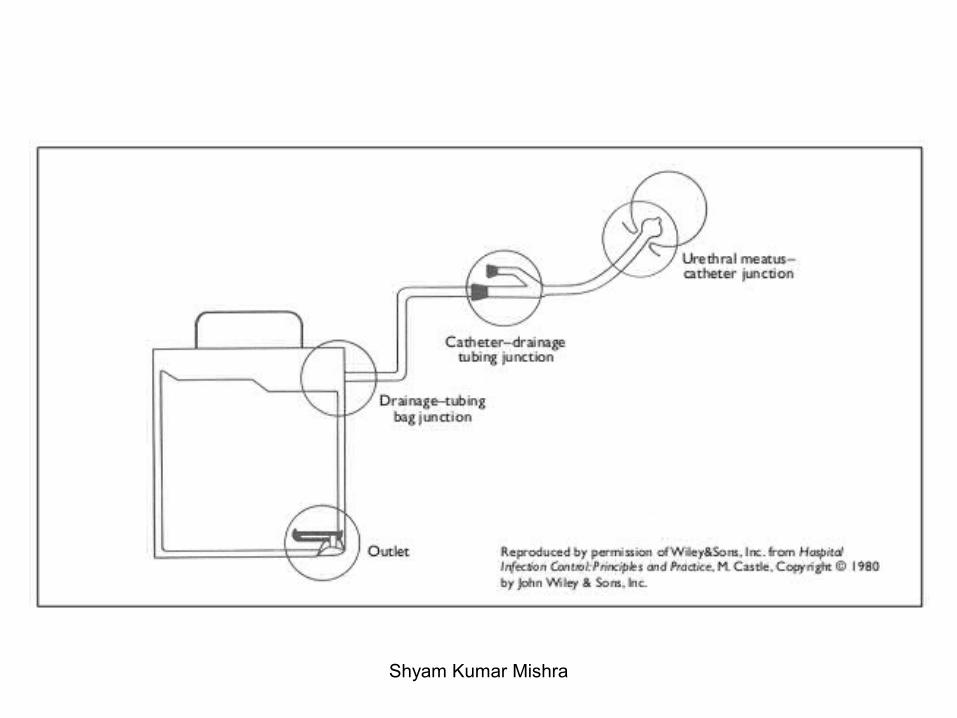
IMPORTANT EXTRINSIC RISK FACTORS FOR MAJOR
NOSOCOMIAL INFECTIONS INFECTIONS RISK FACTORSUrinary tract Indwelling catheter
Duration of catheterization
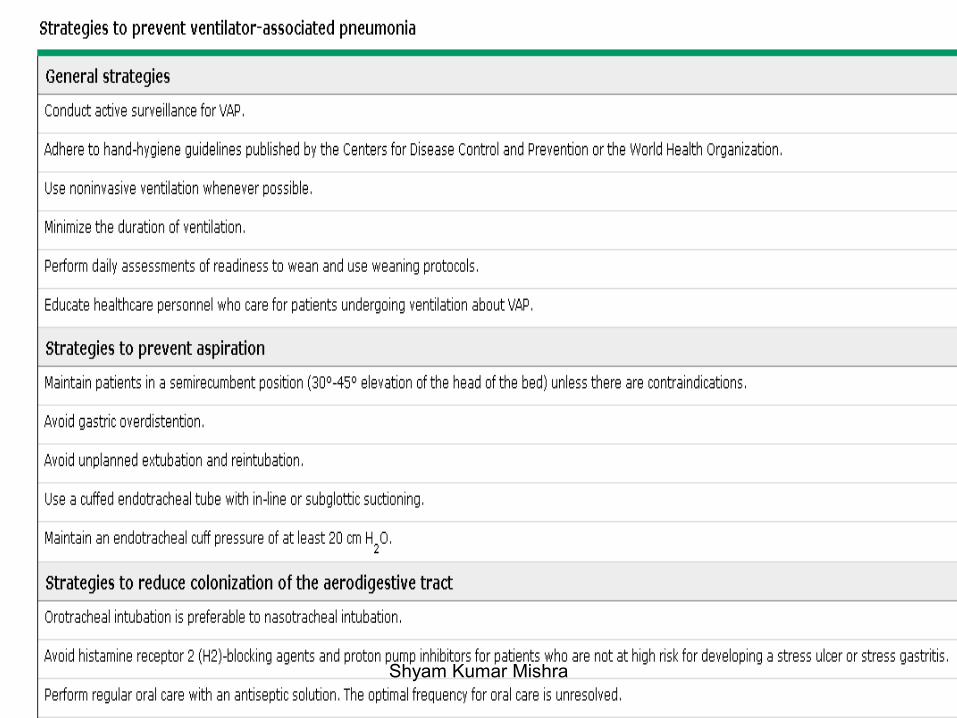
Pneumonia Endotracheal tube
Mechanical ventilation
Thoracoabdominal surgery
Nasogastric tube
Surgical wound Pre operative stay
Preoperative shaving
Duration of surgery
Degree of wound contamination
Presence of foreign body
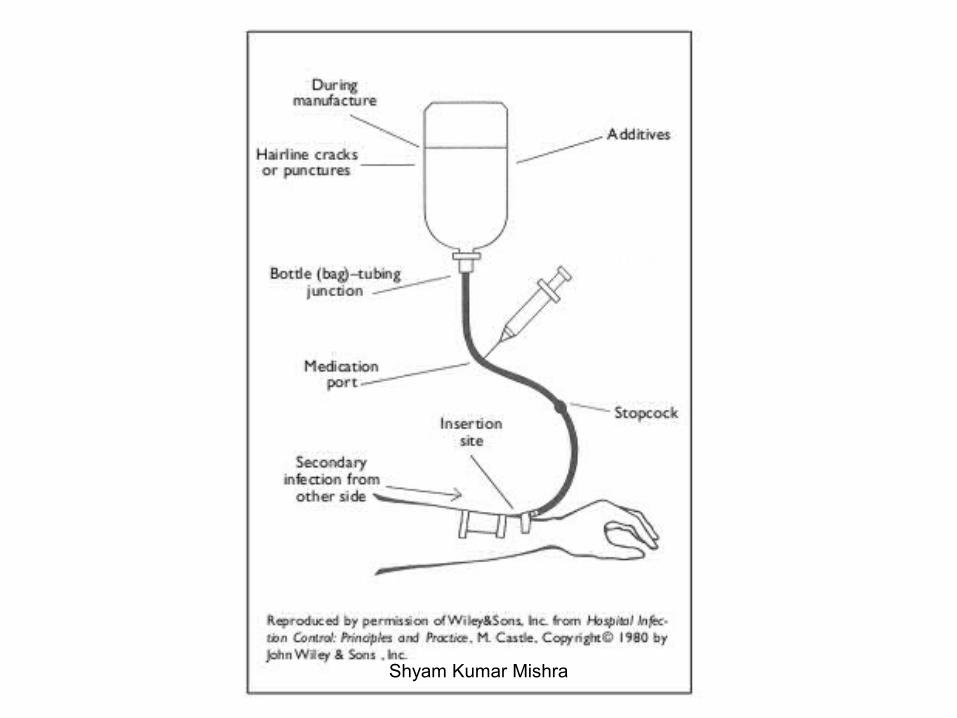
Primary bacteremia Intravascular cannula
Duration of cannulation
Shyam Kumar Mishra
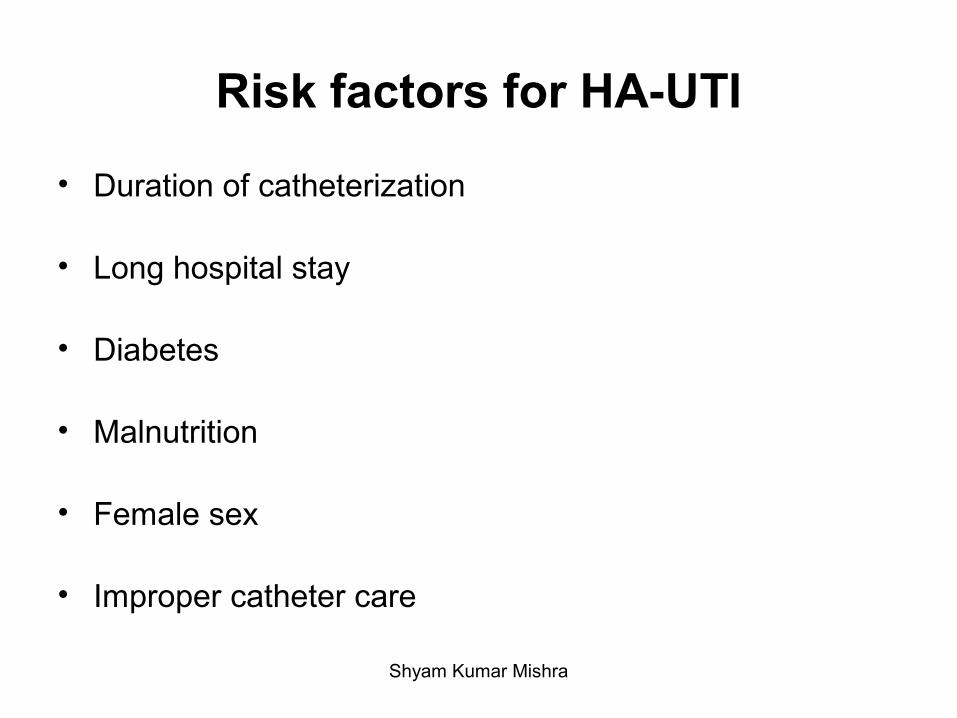
Risk factors for HA-UTI
• Duration of catheterization
• Long hospital stay
• Diabetes
• Malnutrition
• Female sex
• Improper catheter care
Shyam Kumar Mishra
● Previous antibiotic exposure, particularly to third generation cephalosporins
● Reintubation or prolonged intubation
● Mechanical ventilation
● Age >70 years
● Chronic lung disease ● Decreased consciousness
● Chest surgery ● Presence of an nasogastric tube
Risk factors for HAP
Shyam Kumar Mishra
• Diabetes
• Over 60 years of age
• Long duration of the surgical procedure
• Pre-existing infection at the site of the wound
• Systemic corticosteroids or treatment with other immunosuppressive drugs
• Malnutrition
• Preoperative nasal carriage or colonization at other sites with S. aureus
• Presence of a remote focus of infection
• Duration of preoperative hospitalization
• Preoperative preparation, shaving of hair from the site
Risk factors for SSI
Shyam Kumar Mishra
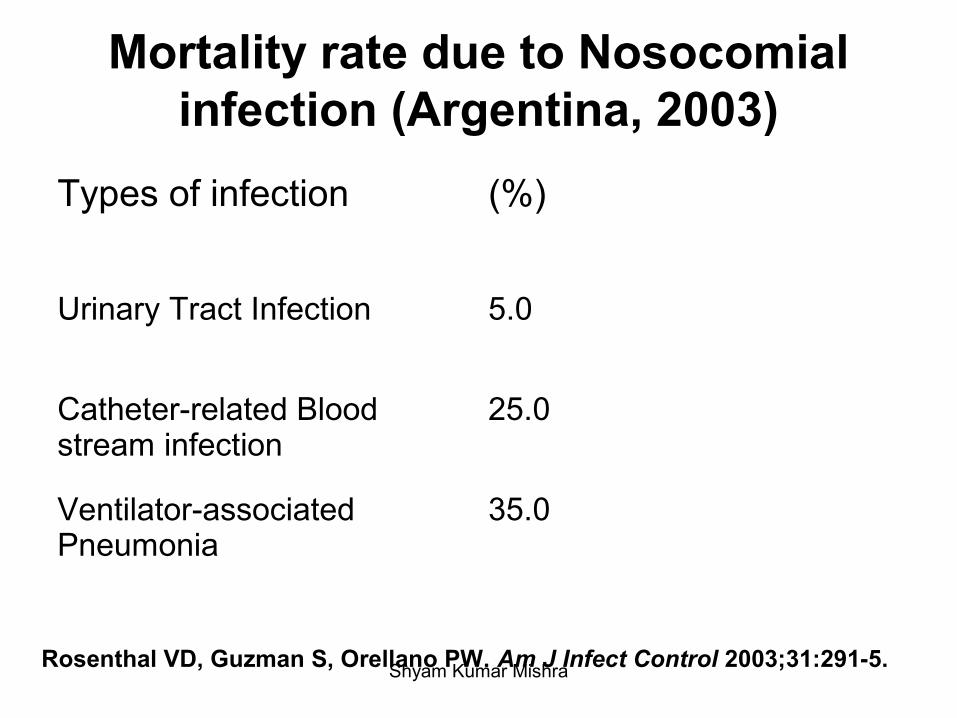
Mortality rate due to Nosocomial infection (Argentina, 2003)
Types of infection (%)
Urinary Tract Infection 5.0
Catheter-related Blood stream infection
25.0
Ventilator-associated Pneumonia
35.0
Rosenthal VD, Guzman S, Orellano PW. Am J Infect Control 2003;31:291-5. Shyam Kumar Mishra
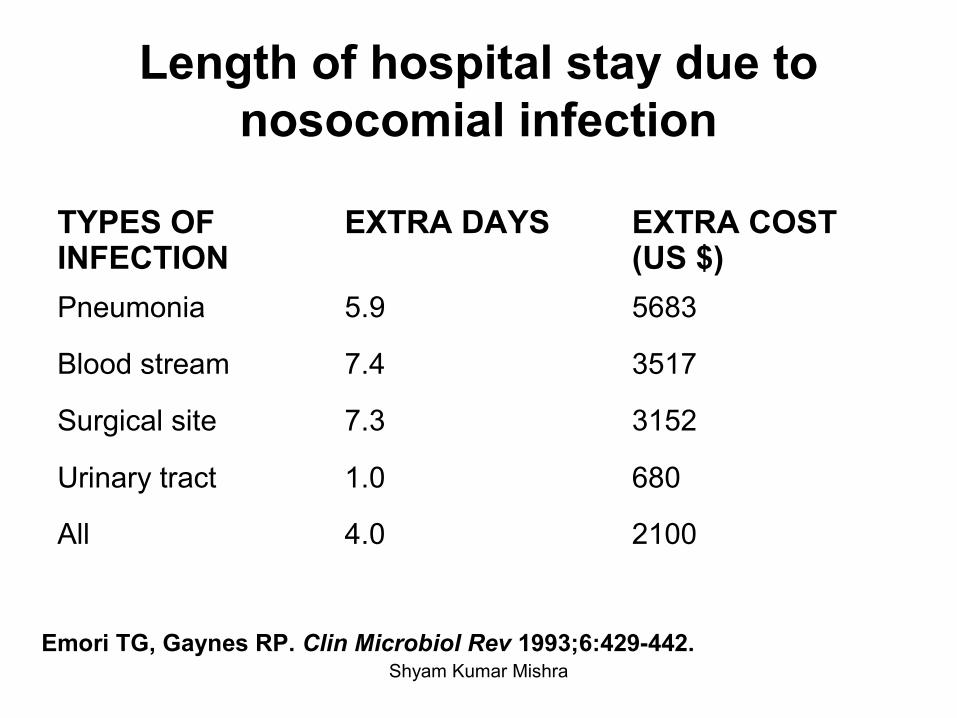
Length of hospital stay due to nosocomial infection
TYPES OF INFECTION
EXTRA DAYS EXTRA COST (US $)
Pneumonia 5.9 5683
Blood stream 7.4 3517
Surgical site 7.3 3152
Urinary tract 1.0 680
All 4.0 2100
Emori TG, Gaynes RP. Clin Microbiol Rev 1993;6:429-442.Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
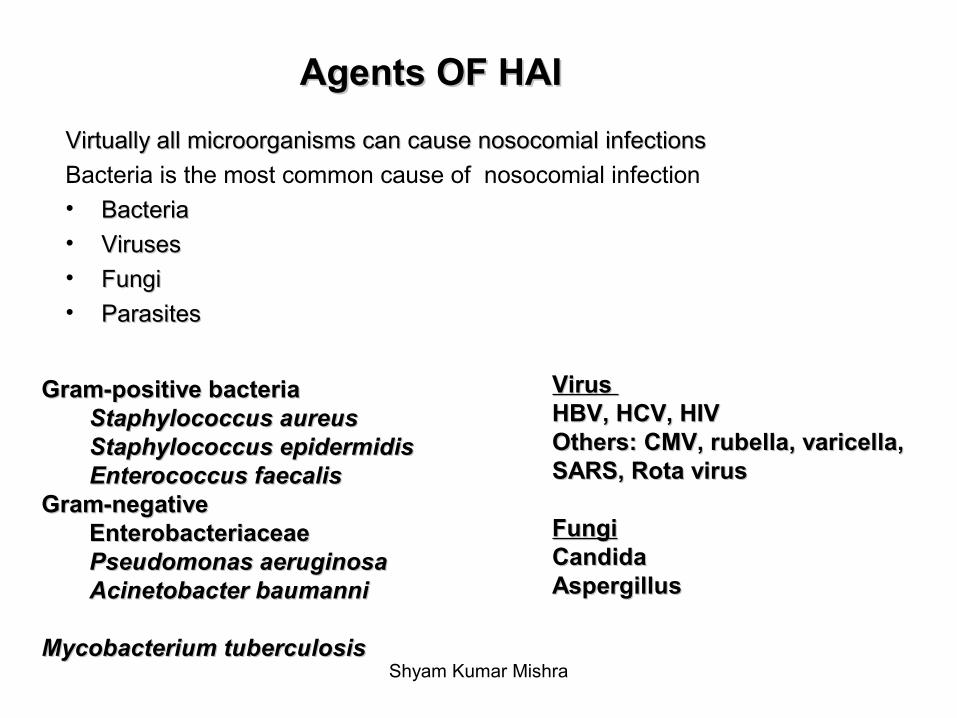
Agents OF HAIAgents OF HAI
Virtually all microorganisms can cause nosocomial infectionsVirtually all microorganisms can cause nosocomial infections
Bacteria is the most common cause of nosocomial infection• BacteriaBacteria• VirusesViruses
• FungiFungi• ParasitesParasites
Gram-positive bacteriaGram-positive bacteriaStaphylococcus aureusStaphylococcus aureusStaphylococcus epidermidisStaphylococcus epidermidisEnterococcus faecalisEnterococcus faecalis
Gram-negativeGram-negativeEnterobacteriaceae Enterobacteriaceae Pseudomonas aeruginosaPseudomonas aeruginosaAcinetobacter baumanniAcinetobacter baumanni
Mycobacterium tuberculosisMycobacterium tuberculosis
Virus Virus HBV, HCV, HIVHBV, HCV, HIVOthers: CMV, rubella, varicella, Others: CMV, rubella, varicella, SARS, Rota virusSARS, Rota virus
FungiFungiCandida Candida AspergillusAspergillus
Shyam Kumar Mishra
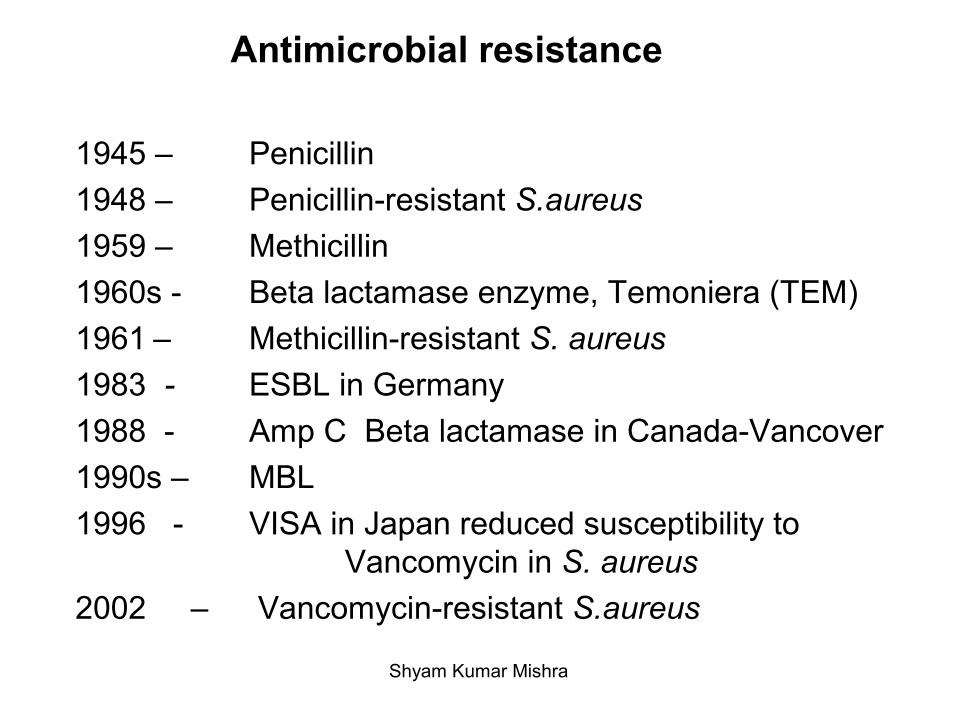
Antimicrobial resistance
1945 – Penicillin
1948 – Penicillin-resistant S.aureus
1959 – Methicillin
1960s - Beta lactamase enzyme, Temoniera (TEM)
1961 – Methicillin-resistant S. aureus
1983 - ESBL in Germany
1988 - Amp C Beta lactamase in Canada-Vancover
1990s – MBL
1996 - VISA in Japan reduced susceptibility to Vancomycin in S. aureus
2002 – Vancomycin-resistant S.aureus
Shyam Kumar Mishra
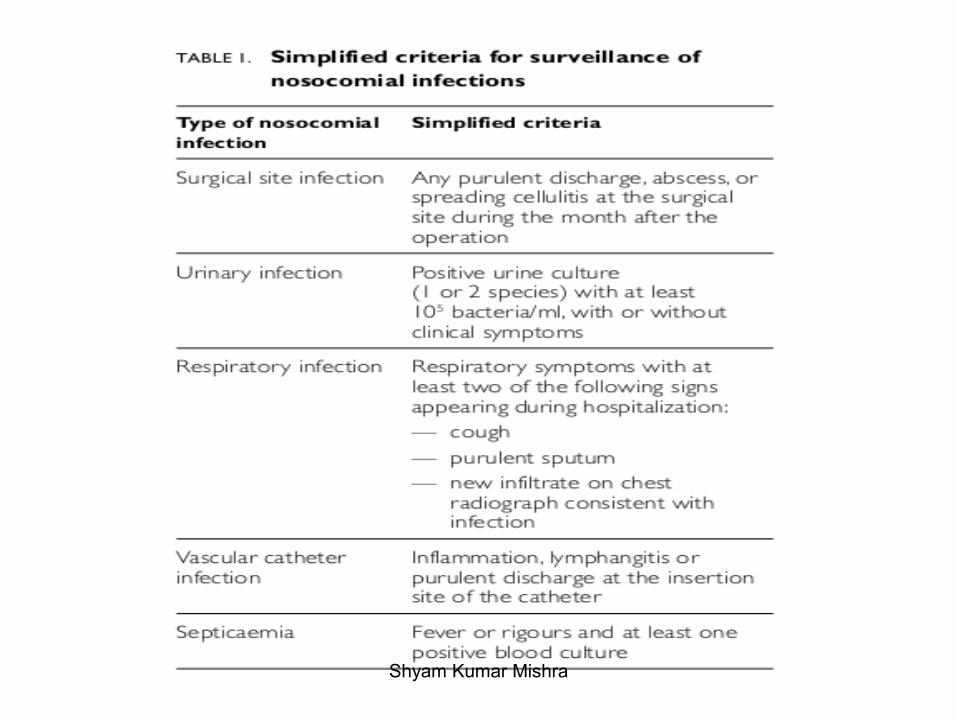
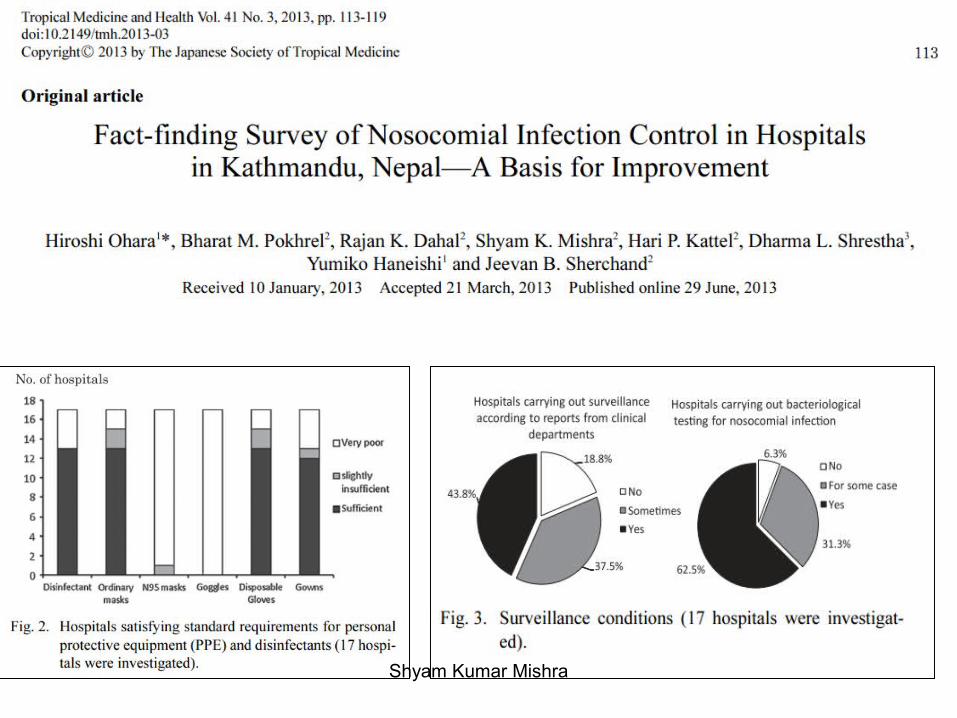
Surveillance
Shyam Kumar Mishra
• Surveillance can be defined as the systematic, active on-going observation of the occurrence and distribution of a disease within a population and of the events that increase or decrease the risk of the disease occurrence. If the incidence, distribution and associations of a disease are known, then resources can be targeted, predisposing factors can be reduced or eliminated, and the incidence of the disease reduced.
Shyam Kumar Mishra
Why surveillance???
• To reduce the incidence of HAI and thus to reduce the associated morbidity, mortality, and costs.– To assess magnitude of problem– To monitor implementation of health programs– To understand local epidemiology of the problem– To assess changes in trend of disease or its distribution– To identify specific groups at risk– To enable predictions about pattern of occurrence of diseases– To assess the impact of the programme intervention for control
of diseases
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
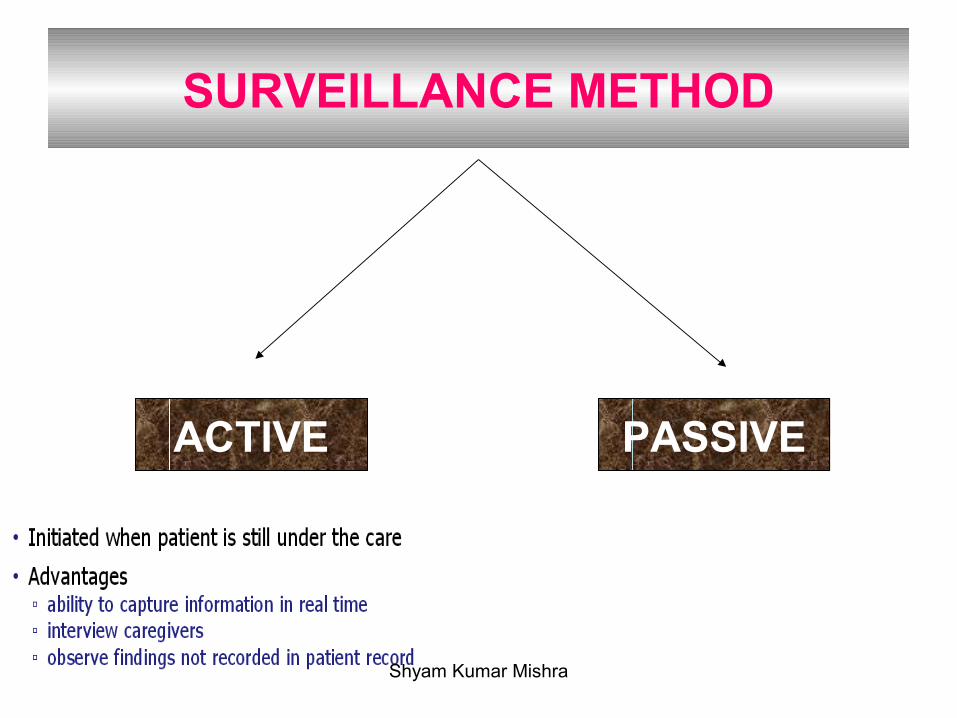
SURVEILLANCE METHOD
ACTIVE PASSIVE
Shyam Kumar Mishra
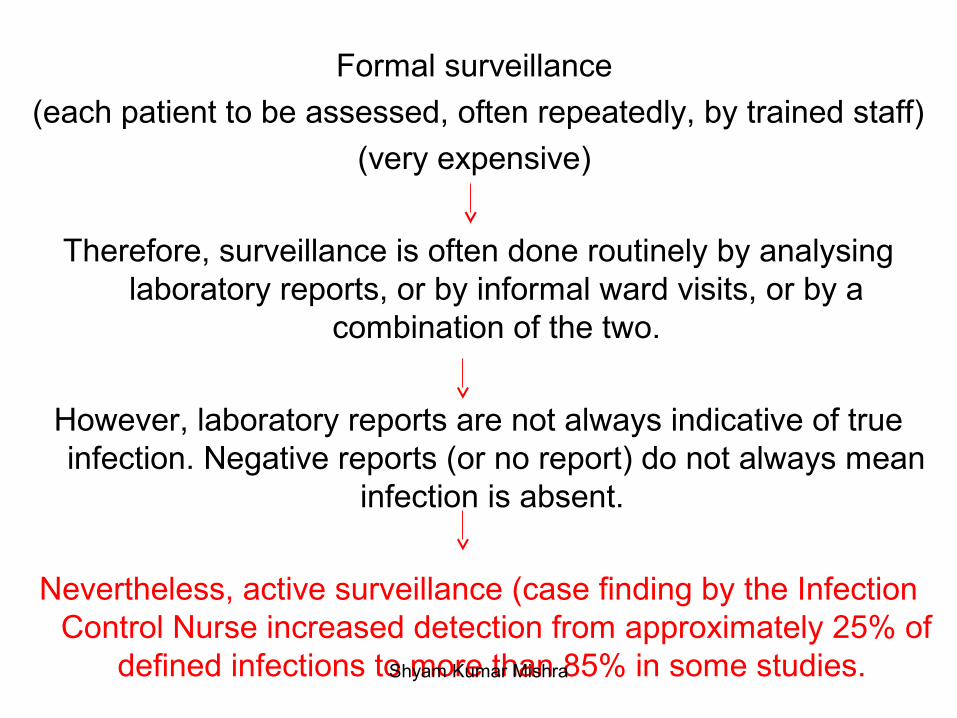
Formal surveillance
(each patient to be assessed, often repeatedly, by trained staff)
(very expensive)
Therefore, surveillance is often done routinely by analysing laboratory reports, or by informal ward visits, or by a
combination of the two.
However, laboratory reports are not always indicative of true infection. Negative reports (or no report) do not always mean
infection is absent.
Nevertheless, active surveillance (case finding by the Infection Control Nurse increased detection from approximately 25% of
defined infections to more than 85% in some studies. Shyam Kumar Mishra
Incidence and prevalence of HAI
• The prevalence of HAI is the number of cases of active HAI in a defined patient population either during a specified period of time (the period prevalence) or at a specified point in time (point prevalence).
• The incidence of HAI is the number of new cases of disease that occur in the defined patient population during a specified time period.
Shyam Kumar Mishra
Targeted surveillance
• Site-oriented surveillance
• Unit-oriented surveillance
• Priority-oriented surveillance– Alert-condition surveillance– Alert-organism surveillance
Shyam Kumar Mishra
Patient-based surveillance
a) Count HAI, assess risk factors, and monitor patient care procedures and practices for adherence to infection control principles
b) Requires ward rounds and discussion with caregivers
Laboratory-based surveillance
a) Detection is based solely on the findings of laboratory studies of clinical specimens
Shyam Kumar Mishra
Shyam Kumar Mishra
Prospective surveillance a) Monitor patients during their hospitalization b) For SSIs, also monitor during the post-discharge period
Retrospective surveillance a) Identify infections via chart reviews after patient
discharge
Shyam Kumar Mishra
Risk-adjusted rates
a) Rates are controlled for variations in the distribution of major risk factors associated with an event’s occurrence
b) Such rates allow inter- and intra-facility rate comparisons
Crude rates
a) Rates assume equal distribution of risk factors for all events
b) Such rates cannot be used for inter-facility comparisons
Shyam Kumar Mishra
Data to collect
1. Demographic – name, date of birth, gender, hospital identification number, admission date
2. Infection – onset date, site of infection, patient care location of HAI onset
3. Risk factors – devices, procedures, other factors associated with HAI
4. Laboratory – pathogens, antibiogram, serology, pathology
5. Radiology/imaging – X-ray, CT scan, MRI, etc.
Shyam Kumar Mishra
Sources of data
1. Admission/discharge/transfer records, microbiology laboratory records
2. Visits to patient wards for observation and discussion with caregivers
3. Patient charts (paper or computerized) for case confirmation
a) Laboratory and radiology/imaging results
b) Nursing and physician’s notes and consults
c) Admission diagnosis
d) History and physical examination findings
e) Records of diagnostic and surgical interventions
f) Temperature chart
g) Information on administration of antibiotics Shyam Kumar Mishra

Shyam Kumar Mishra
• Most infectious disease physicians, infection preventionists and epidemiologists agree that HAIs are under-reported. Why?
Shyam Kumar Mishra
Post-discharge surveillance often poses considerable logistic problems and may add further expense to surveillance activities.
Shyam Kumar Mishra
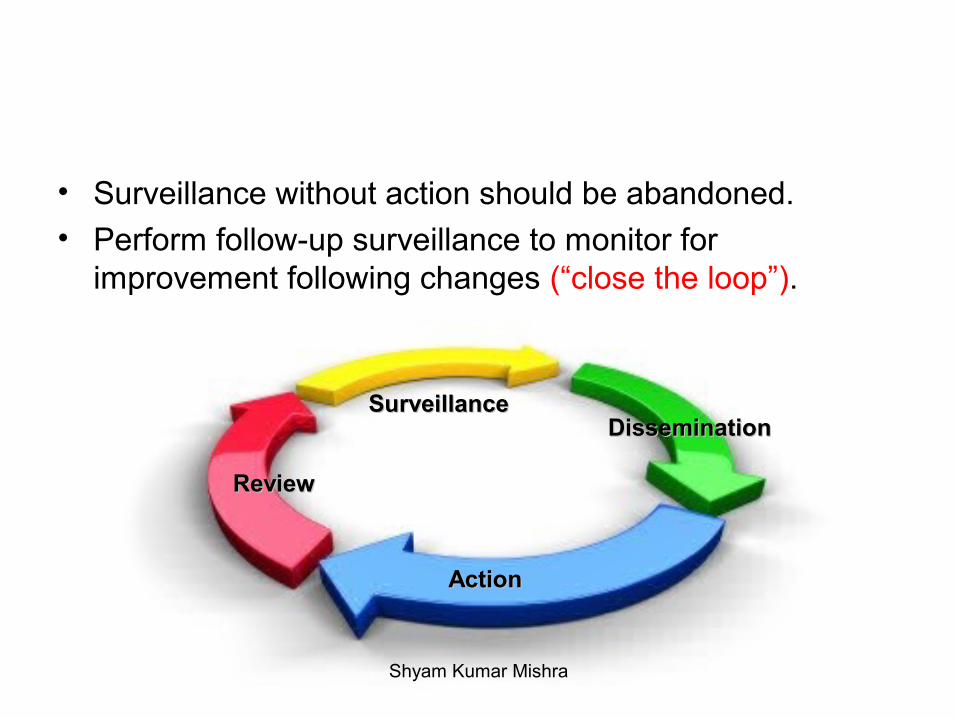
• Surveillance without action should be abandoned.
• Perform follow-up surveillance to monitor for improvement following changes (“close the loop”).
SurveillanceSurveillance
ReviewReview
DisseminationDissemination
Action Action
Shyam Kumar Mishra
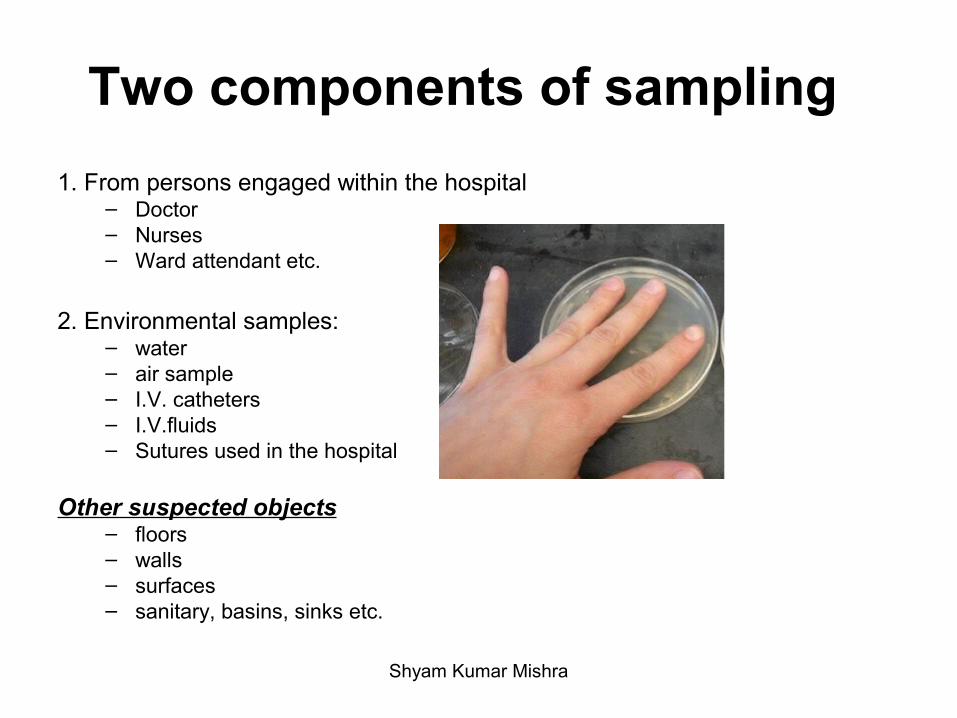
Two components of sampling
1. From persons engaged within the hospital– Doctor– Nurses– Ward attendant etc.
2. Environmental samples:– water– air sample– I.V. catheters– I.V.fluids– Sutures used in the hospital
Other suspected objects– floors– walls– surfaces– sanitary, basins, sinks etc.
Shyam Kumar Mishra
EPIDEMIOLOGICAL MARKERS FOR NOSOCOMIAL INFECTION
• Biotyping
• Antibiogram• Serotyping• Bacteriophage typing• Bacteriocin typing
• Dienes phenomenon
• Bettelheim reaction (colony incompatibility)
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
• Plasmid analysis• RFLP• PCR-RFLP
• DNA/DNA hybridization• DNA/RNA hybridization• Pulse field gel electrophoresis• Randomly amplified polymorphic DNA (RAPD)• LCR
• Ribotyping• Spoligotyping• MLST• Cloning• Sequencing
Shyam Kumar Mishra
Prevention of Nosocomial infections
There is a Nosocomial infection control committee (NICC) which includes:
Matron
Physician
Surgeon
Administrator
Microbiologist
Medical laboratory technologist
Pharmacist
House-keeping staffShyam Kumar Mishra
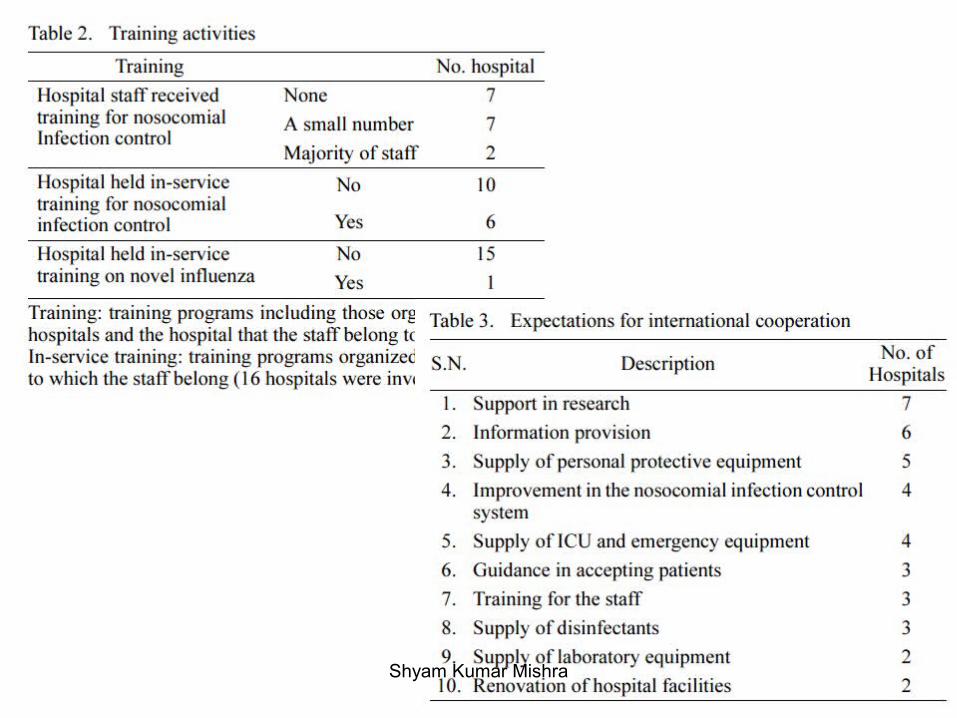
Periodical training of staffs regarding nosocomial infection control
Immunizations for the staffs; PEPs
Microbial monitoring of hospital: Periodical exposure of culture plates/ swabbing (wards, ICUs, Operation theatre)
Carrier detection: Microbial culture of Nasal Swab, Hand Swab, Masks & gowns of Surgeons, Physicians, Nurses and other Staffs involved in Patient CareShyam Kumar Mishra
Much attention needs to be paid to Multidrug resistant (MDR) isolates.
Status of MDR bacterial isolates should be disseminated through scientific conferences, newsletters, journals and personal communication.
Hospital infection control guidelines should be prepared to investigate and control nosocomial infections.
Shyam Kumar Mishra
Use of color-coded containers for segregation of laboratory and hospital wastes
Proper disposal of hospital waste products
Hospital building must meet ISO standard
(Ventilation, Water, Waste)
Shyam Kumar Mishra
Shyam Kumar Mishra
Role of Microbiologist
• Developing guidelines for appropriate collection, transport and handling of specimens.
• Ensuring that the laboratory practice meet appropriate standards.
• Ensuring safe laboratory practice to prevent infections in staff
• Perform AST of clinical isolates• Monitor sterilization, disinfection procedures /
environment where necessary• Timely communicate results to Infection Prevention
Committee• Epidemiological typing of hospital microorganisms • Follow Antibiotic stewardship
Shyam Kumar Mishra
• Antimicrobial stewardship refers to coordinated interventions designed to improve and measure the appropriate use of antimicrobials by promoting the selection of the optimal antimicrobial drug regimen, dose, duration of therapy, and route of administration.
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
Shyam Kumar Mishra
Infection Prevention (IP)
“Infection prevention largely depends on placing the barriers between a susceptible host and microorganisms”
Shyam Kumar Mishra
Shyam Kumar Mishra
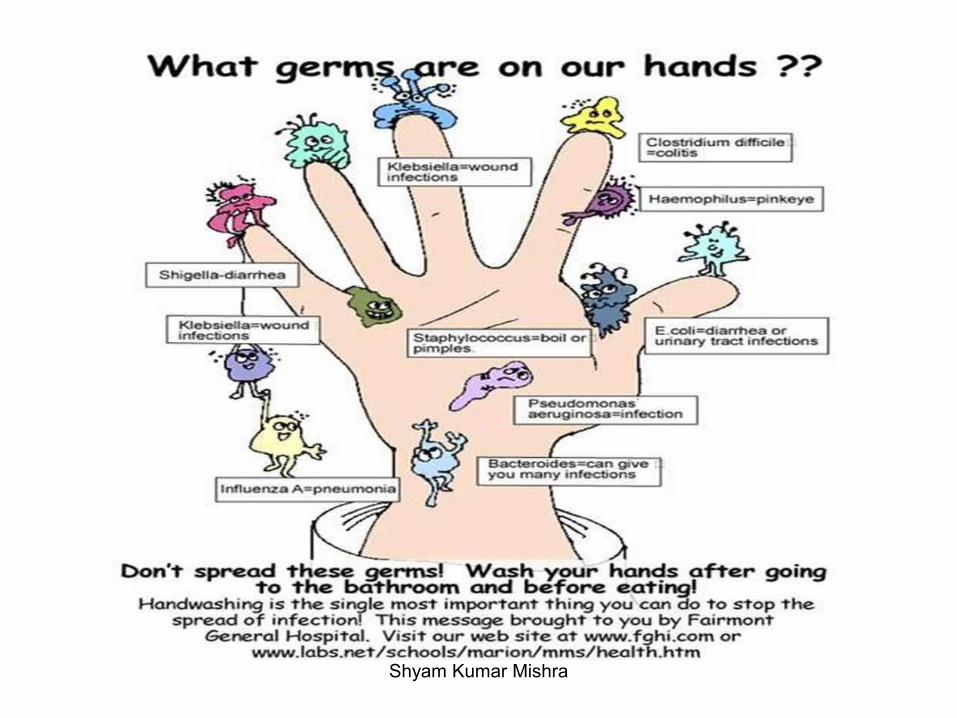
HAND WASHING
“Hand washing is the most practical procedure for preventing cross-contamination (person to person). Hand washing may be the single most important procedure for preventing infection.”
Global handwashing Day (15th October)
Shyam Kumar Mishra
1. Wash your hands when they are dirty and BEFORE eating
2. DO NOT cough into your hand
3. DO NOT sneeze into your hands
4. Above all, DO NOT put your fingers into your eyes, nose or mouth
Shyam Kumar Mishra
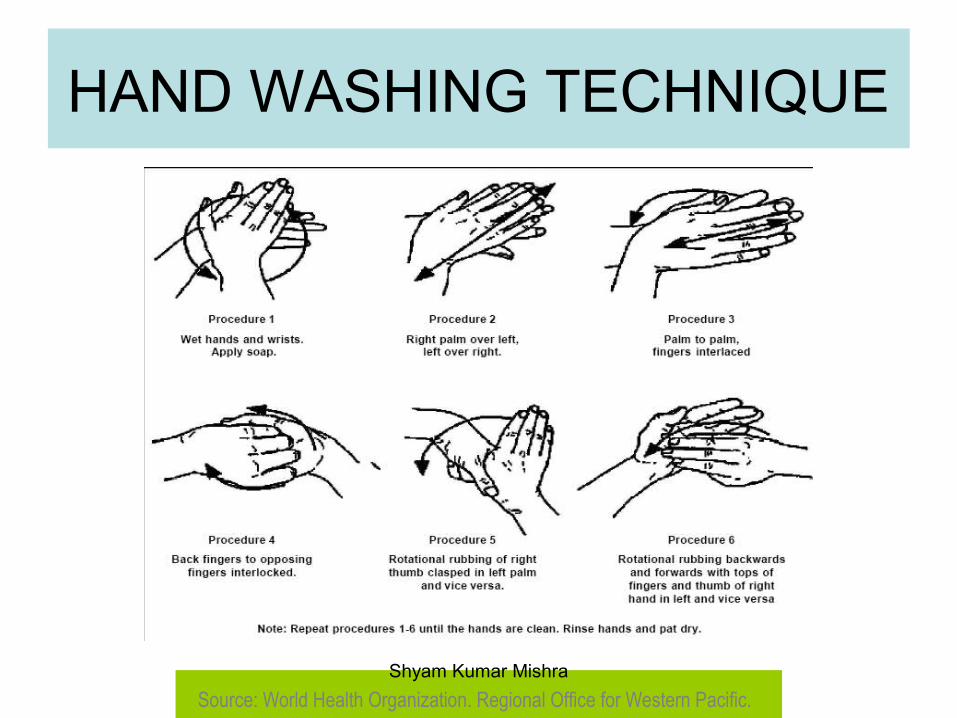
HAND WASHING TECHNIQUE
Source: World Health Organization. Regional Office for Western Pacific. Shyam Kumar Mishra
SIR WILLIAM OSLER-
“Soap, Water and common sense are the best disinfectants in the hospital.”
Shyam Kumar Mishra
Shyam Kumar Mishra