Embed Size (px)
Citation preview

Can we ever make nursing decisions “evidence based”?
Carl ThompsonUK, Centre for Evidence Based Nursing

Evidence Based Decisions
(cf. Dicenso, Cullum,Ciliska et al. 1998)
“The consideration of relevant, valid, research evidence when making clinical and policy decisions in nursing”
Research
preferences
Context (resources, expertise)
Research
preferences
Context (resourcesexpertise)

The 5 Ages Of Evidence Based Practice
Complacency and consensus The recognition of uncertaintyTrials, laggards, innovation and
diffusionGuidelines and “mindlines”The evidence based toolkit

Progress towards EBN (i)

Progress (ii) Policy
EBN explicit in UK Nursing and Midwifery Council Standards and Code of Conduct “You have a responsibility to deliver care
based on current evidence, best practice and, where applicable, validated research when it is available”.

Progress (iii) Nursing And National Standards
Nursing and the National Institute For Health and Clinical Excellence(NICE) into professional knowledge
Knowledge = “actionable understanding”

Progress (iv) education
UK Nursing and Midwifery Council and Standards of Proficiency

Progress (vi) raw knowledge materials
0
50
100
150
200
250
300
350
400
QualRCTSys rev

Progress (vii) impact on clinical practice
Then (1980s) Mainly venous in origin –
compression bandaging is first line treatment
>80% of leg ulcer patients managed in community by nurses (responsible for treatment decisions)
Only <25% of those requiring compression bandaging received it
Now (2000s) Screening for arterial disease
using Doppler ankle brachial pressure index (ABPI) increased from 71.9% to 88.8%
Assessment of patients’ pain increased from 65.8% to 83.4%
Use of compression bandaging increased from 76.4% to 90.5%
Time to healing reduced significantly
www.rcn.org.uk/publications/pdf/guidelines/leg_ulcer_sentinel_audit1.pdf

I’m confused…so what’s the problem?
“As we know, There are known knowns. There are things we know we know. We also know There are known unknowns. That is to say We know there are some things We do not know. But there are also unknown unknowns, The ones we don't know We don't know.”
© Rumsfeld, Feb. 12, 2002

A “Known Unknown”
The relationship between information use and decision making

Two approaches – to judgement and decisions
The black box of the “expert” decision maker Benner and “expertise” Qualitative “exploration”
and description intangible Intra category comparison
with no objective measures
Expertise is what experts do…
The empirical alternative
Operationalise key terms Compare performance for
tasks know something about
Clinical judgement: assessment of alternatives
Clinical decision: choosing an alternative
Expertise: the ability to consistently make more good than bad judgements.

Knowns And Unknowns – Decision Making and Judgement
What kinds of uncertainties, judgements and decisions do nurses face and how do they handle these? interviews observation and Q
methodological modelling with 200+ nurses in primary and acute care.
Thompson et al. Journal of Advanced Nursing 2001 – 2004

Types of uncertainty
INTERVENTIONS Targeting Timing Prevention Referral
ASSESSMENT DIAGNOSIS COMMUNICATION SERVICE ORGANISATION/DELIVERY INFORMATION SEEKING EXPERIENTIAL

How Often Do Nurses Face These Uncertainties?
Once every 30 seconds in critical care (Bucknall, 2000)
Circa 50 decisions every 8 hour shift in Medical Admissions (Thompson et al. 2001 – 2005)
5 judgement or decision challenges per consult for health visitors.

How do nurses respond to uncertainty?
Experiential/internal knowledge Very limited textual information use and for
certain kinds of decisions (British National Formulary and local protocols) 90 hours of primary care = 1 telephone call 180 hours of acute care (1080 decisions) = local
protocols x4 times, BNF x50 times). ‘sophistication’ and technology doesn’t matter
(Randell et al. 2007). Demography and biography poor predictors of
use

Explanations?
barriers to research utilisationNo time, no access, no skills, no control
interventions to increase research use ineffective
It’s nurses’ DECISIONS themselves that influence information use!

The theory – cognitive continuum
Hamm,R (1988) in Dowie & Elstein, Clinical Judgement and decision making, Cambridge University Press

So…
EBN all about combining information information handling and cognition depends
on: The ways that nurses structure decisions The time available The ‘visibility’ of decision making required
More time, more structure, and more visibility = greater use of research in decision making
Problem – how to unpack information use in context of cognition and decision making and link to decision performance/expertise?


Expertise [properly] defined!
22 11 esesa RRCRGRR In English:
Decision making quality/achievement is a function of the nurse’s judgement consistency, the “fit” between decision task and the nurse’s way of thinking and the uncertainty in clinical practice.
Brunwik’s lens model equation
AAARGH….

How (i) methodology Social judgement lens modelling
Achievement (Ra) Linear reasoning (G) Non linear reasoning (C) Control (Rs) Unpredictability (Re)
Signal detection modelling d’ (or ability to discriminate signal from noise) Β (decision threshold)
risk No risk
Yes TP FP
no FN TN

How (ii) method245 acute care nurses
Critical care experience & non-experiencedUK, Canada, Australia, Netherlands50 scenarios – perioperative MI
50% of arrests have documented but unacted upon changes in basic markers (BP, resps, pulse)
Changes result in intervention only 2.8% of the time (Daffurn et al, 1994)
Criterion: Modified Early Warning Score predicted outcome (true positive rate = 72%)
Varying educational levelsVariable time pressure and a protocol
Thompson et al. journal of clinical nursing (in review)

We found
Significant variability in estimated likelihood, Dx judgement of risk, and Rx (intervention) decisions despite identical information Dx = 3/50 through 50/50 Rx = 5/50 through 48/50
Achievement/accuracy .42 (.41 - .44) Consistency .79 (.77 - .80) Linear reasoning .50 (.48 - .52)
>Rm = >achievement <Rm .33, >Rm .52 p<0.001) Mean R2 .96 (.93-.98) Non-linear reasoning .06 (.04 - .09)

Time and experience (i)
Mean 95% CI
d' Time pressure 0.98 0.91-1.05
No time pressure 1.67 1.58-1.8
lnβ Time pressure -0.07 -0.14-0.01
No time pressure -0.28 -0.36 - -0.19

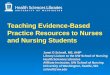
Time and experience (ii)
=> 3 yearstwo yearsone yearzero years
experience critical care - 4 categ
2.00
1.75
1.50
1.25
1.00
0.75
0.50
Es
tim
ate
d M
arg
ina
l M
ea
ns
2
1time
Estimated Marginal Means of d_prime
No time pressure
time pressure

Variability: evidence based protocol use
4.003.002.001.00
country
0.70
0.60
0.50
0.40
0.30
0.20
0.10
0.00
rela
tive
wei
gh
t: p
roto
col
UK Netherlands Canada Australia
% co
ntrib
utio
n to
jud
gem
ent

To what extent are nurse decisions evidence based NOW?
Is research knowledge even part of nurses’ decision ingredients | information behaviour?
To what extent do nurses’ decisions mirror research knowledge?
Yes EBN in some nurses, for some decisions, in some contexts. (time, structure and visibility) Good information ≠ good decisions
Expectation management No time for benefits of experience = no benefits

What’s the potential?
What happens if we educate all nurses for uncertainty not certainty?
Can large scale gains in quality (Linda Aiken’s) be replicated on a much smaller scale and with performance measures?
Do we need to rethink Benner and nursing given differences in decisions? expertise in all contexts and all decisions within
clinical domains? What happens if we fit decision technologies
to decisions?

More Research Needed!
Decisions and judgements as a dimension of research-utilisation and knowledge transfer studies?
Challenges of evaluating decision technologiesContext and decision specificStudy design

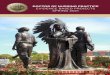
Some good news: nursing started early…
Florence Nightingale’s “coxcomb”
Blue = contagious diseaseRed = deaths from woundsBlack = other causes
Jan 1855: 3168 deaths32k manpower that month1,174/10k overall mortality rate1,023/10k contagious mortality rate
disease alone would have killed the British army in the Crimea