Embed Size (px)
Citation preview

Letters to the Editor
Disability teaching formedical students: disabledpeople contribute tocurriculum development
Editor – More people are living with
chronic disease as life-expectancy rises.
Disability, recognized as a core curri-
culum theme in undergraduate medical
education,1 is taught in an inconsistent
and fragmented way.2 Attempts have
been made to define a core curricu-
lum3,4 but these have had a strong
medical emphasis.
Disabled people have taught on the
Bristol Medical School Disability course
since its inception in 1993. At feedback
it was noted that non-disabled and dis-
abled presenters had different priorities
for teaching. A Disability and Rehabil-
itation panel, comprising disabled and
able-bodied people in equal propor-
tions, was set up to reach consensus on
disability teaching.
The nominal group technique5 with 2
rounds of scoring was used to distil a
list and definitions of key teaching ele-
ments. Anonymity and a wide range of
backgrounds in the panel ensured that
no particular interest or preconceived
opinion was likely to predominate.5
After the second feedback session, it was
decided into which category (Attitudes,
Skills or Knowledge) the elements were
best placed, and which were considered
essential or desirable for competency as
a doctor. After 2 years these elements
were extensively revised, as ideas and
understanding evolved and the com-
munication between panel memebers
matured.
Table 1 shows the current attitudes,
skills and knowledge elements. Of the
essential elements, Attitudes predomin-
ated (6 key elements), followed by Skills
(4) and Knowledge (3). The Attitudes
elements focused on awareness of atti-
tudes and working in partnership; the
Skills elements related to communi-
cation.
The Social Model of Disability now
underpins our teaching. This model
sees people as having �impairment(s)�but being �disabled� by physical, organ-
isational and attitudinal ⁄ behavioural
barriers in society. We aim to challenge
students to examine their own, the
Health Service’s and society’s attitudes
and prejudices towards disability. In
smaller workshops, led solely by dis-
abled presenters, students are encour-
aged to talk about their own experience
of disability. It has been claimed that
students learn from disabled people by
encountering them as patients.4 Our
experience indicates that, from an edu-
cational point of view, recognition of
the disabled person’s own expertise
and the idea of partnership is only fully
realised when the disabled person is
introduced as �the teacher�. Our com-
munication workshops are led along
these lines by people with specific
communication impairments: visual,
speech, hearing and learning difficul-
ties. Some students have commented
on the authenticity that this brings to
their understanding. Direct teaching by
disabled people is always highly valued
by the students.
The teaching elements have been
used to audit the medical curriculum.
Gaps have been identified as well as the
diverse understanding of the term �dis-
ability� among course organisers. As a
result we have developed a module
concerned with Disability Equality as
part of a Diploma or Masters in Medical
Education. Our aim in �Teaching the
teachers� is to embed the underlying
philosophy throughout the whole of the
medical course. Disability should be
visible to students as a clear vertical
theme running throughout the pro-
gramme, with the issues seen as integral
to medical practice.
Thomas P E Wells
Margaret A Byron
Susan H P McMullen
Martin A Birchall
Disability and Rehabilitation Panel,
Department of Clinical Medicine,
University of Bristol
AcknowledgementsWe acknowledge the work of Professor
Paul Dieppe and the late Professor John
Farndon, whose ideas led to the estab-
lishment of this initative.
FundingThe work was supported by a grant
from Remedi.Correspondence: Dr M A Byron, Co-chair of
Disability and Rehabilitation Panel,
Department of Clinical Medicine, c⁄oMRC⁄HSRC, Canynge Hall, Whiteladies
Road, Bristol, BS8 2PR, UK. Tel.: 44 (0)
117 928 7343; Fax: 44 (0) 117 928 7236;
E-mail: [email protected]
788 � Blackwell Science Ltd MEDICAL EDUCATION 2002;36:788–792
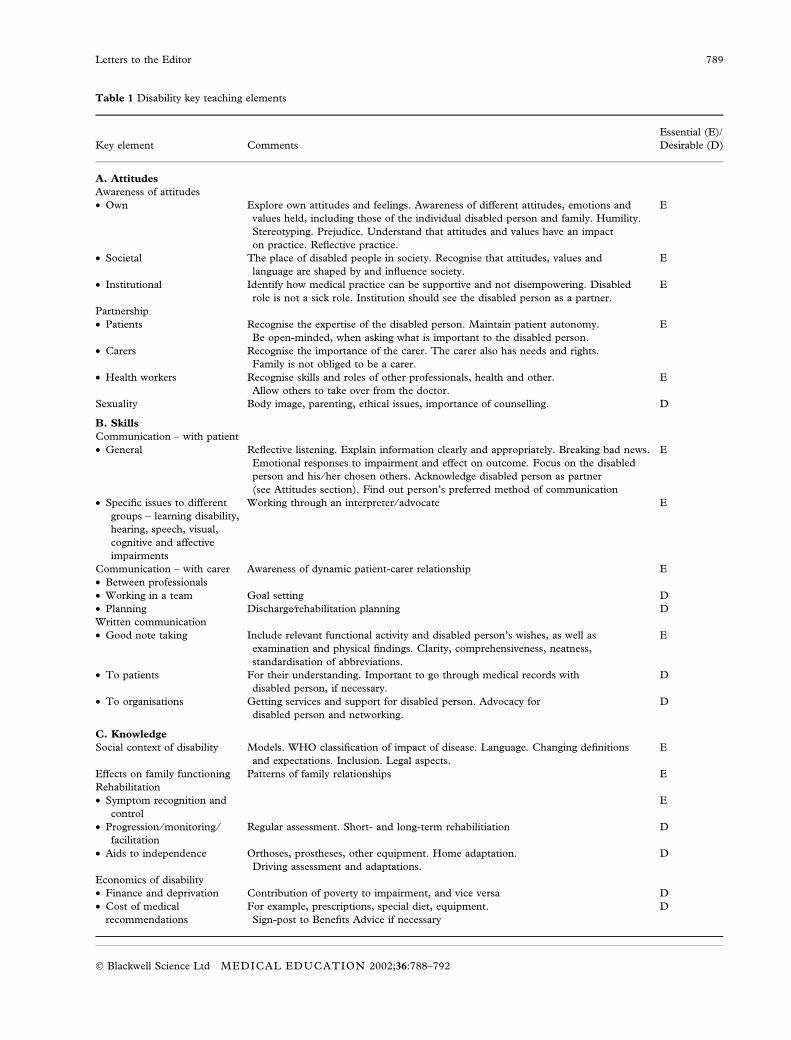
Table 1 Disability key teaching elements
Key element Comments
Essential (E)/
Desirable (D)
A. Attitudes
Awareness of attitudes
• Own Explore own attitudes and feelings. Awareness of different attitudes, emotions and
values held, including those of the individual disabled person and family. Humility.
Stereotyping. Prejudice. Understand that attitudes and values have an impact
on practice. Reflective practice.
E
• Societal The place of disabled people in society. Recognise that attitudes, values and
language are shaped by and influence society.
E
• Institutional Identify how medical practice can be supportive and not disempowering. Disabled
role is not a sick role. Institution should see the disabled person as a partner.
E
Partnership
• Patients Recognise the expertise of the disabled person. Maintain patient autonomy.
Be open-minded, when asking what is important to the disabled person.
E
• Carers Recognise the importance of the carer. The carer also has needs and rights.
Family is not obliged to be a carer.
• Health workers Recognise skills and roles of other professionals, health and other.
Allow others to take over from the doctor.
E
Sexuality Body image, parenting, ethical issues, importance of counselling. D
B. Skills
Communication – with patient
• General Reflective listening. Explain information clearly and appropriately. Breaking bad news.
Emotional responses to impairment and effect on outcome. Focus on the disabled
person and his ⁄her chosen others. Acknowledge disabled person as partner
(see Attitudes section). Find out person’s preferred method of communication
E
• Specific issues to different
groups – learning disability,
hearing, speech, visual,
cognitive and affective
impairments
Working through an interpreter ⁄ advocate E
Communication – with carer Awareness of dynamic patient-carer relationship E
• Between professionals
• Working in a team Goal setting D
• Planning Discharge⁄rehabilitation planning D
Written communication
• Good note taking Include relevant functional activity and disabled person’s wishes, as well as
examination and physical findings. Clarity, comprehensiveness, neatness,
standardisation of abbreviations.
E
• To patients For their understanding. Important to go through medical records with
disabled person, if necessary.
D
• To organisations Getting services and support for disabled person. Advocacy for
disabled person and networking.
D
C. Knowledge
Social context of disability Models. WHO classification of impact of disease. Language. Changing definitions
and expectations. Inclusion. Legal aspects.
E
Effects on family functioning Patterns of family relationships E
Rehabilitation
• Symptom recognition and
control
E
• Progression ⁄monitoring ⁄facilitation
Regular assessment. Short- and long-term rehabilitiation D
• Aids to independence Orthoses, prostheses, other equipment. Home adaptation.
Driving assessment and adaptations.
D
Economics of disability
• Finance and deprivation Contribution of poverty to impairment, and vice versa D
• Cost of medical
recommendations
For example, prescriptions, special diet, equipment.
Sign-post to Benefits Advice if necessary
D
Letters to the Editor 789
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:788–792

References1 Education Committee of the General
Medical Council. Tomorrow’s Doctors:
recommendations in undergraduate medical
education. London: General Medical
Council; 1993.
2 Khatan S, Inman C, Haines A, Holland
P. Teaching disability and rehabilitation
to medical students. Med Educ
1994;28:386–393.
3 British Society for Rehabilitation Medi-
cine. Disability and rehabilitation for
undergraduate medical students: suggestions
for the core curriculum. London: British
Society for Rehabilitation Medicine with
support from the Nuffield Provincial Hos-
pital Trust; 1995.
4 Crotty M, Finucane P, Ahern M.
Teaching students about disability and
rehabilitation: methods and student
feedback. Med Educ 2000;34:659–664.
5 Jones J, Hunter D. Consensus methods
for medical and health services research.
In: N Mays, C Pope (eds). Qualitative
research in health care. London: BMJ
Publishing Group; 1996: pp. 46–58.
Problems with problemsin problem-based curricula
Editor – Biases towards more acute
problems in the younger age groups
are not the only biases seen in prob-
lems designed for PBL curricula.1 My
experience in the development of new
medical programmes in Australia has
shown that biases also exist towards
urban health care and dominant cul-
ture issues. Even when curriculum
designers seek clinical problems that
reflect the broader societal contexts
that will be faced by medical gradu-
ates, the quality of the problems varies
considerably. Many problems with
rural health learning objectives illus-
trate poor health care in a rural set-
ting, with patients being �rescued� by
clinicians in large teaching hospitals.
Further, many of the problems with
learning objectives concerning Indi-
genous peoples’ health illustrate dom-
inant culture cliches about Indigenous
health. Because assessment is often
based on what is taught, these mes-
sages can be reinforced through
assessment. At best, astute students
will recognize the biases and devalue
the curriculum. At worst, these biases
have the potential to further entrench
perceptions that rural health is a career
of last resort and that little can be
done to address the complex issues
within Indigenous peoples’ health.
Problem design should follow a
curriculum design process whereby
curriculum content matches the overall
learning objectives, usually matched to a
vision of what graduates should know
and understand. Ideally, teams that
include expertise in those contexts
should design problems intended to
improve understanding of particular
contexts. That is, aged care health
professionals, managers of chronic dis-
ease, rural doctors and Indigenous
people should be involved in designing
problems that aim to include issues
pertaining to those contexts. While this
may be a stronger feature in the more
socially accountable medical schools2
should not all schools aim for a curri-
culum that reflects reality?
Richard Hays
Townsville, Australia
References1 Finucane P, Nair B. Is there a problem
with the problems in problem-based
learning? Med Educ 2002;36:279–81.
2 Murphy B, Hays RB. Accrediting
educational institutions for their social
accountability: a national need, a global
expectation. Towards Unity for Health
2001;3:20–1.
Consequences of Tomorrow’sDoctors
Editor – I read with interest Christopher
et al.’s review of the GMC visits to
check the implementation of Tomorrow’s
Doctors.1 It was noticeable and perhaps
surprising that the aims of the visits did
not include evaluation of the impact of
the changes on schools or students’
learning. Even if the aims of Tomorrow’s
Doctors are taken to be self-evidently
�good� – something which would not be
accepted by all medical teachers – there
is still a need to evaluate the intended
Table 1 (Continued)
Key element Comments
Essential (E)/
Desirable (D)
Social institutions Employment, training and leisure opportunities. School and education.
Mainstream and special facilities.
D
Sources of information and
routes of referral
Recognise the skill and importance of the social worker. Have a knowledge of
health and social care workers, and their contribution. Voluntary services contribution
D
Knowledge of functional
implications of specific
impairments
For example, foot protection and chiropody for a patient
with peripheral sensory neuropathy
D
Sexuality How to obtain specialist information and advice. Genetics, screening D
Correspondence: Richard Hays, Professor of
General Practice and Rural Medicine,
Foundation Dean, School of Medicine,
James Cook University, Townsville,
Queensland 4811, Australia. Tel.: 00 61 7
4781 6821; Fax: 00 61 7 4781 6986; E-mail:
Letters to the Editor790
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:788–792

and perhaps unintended consequences
of the changes. It may be that the GMC
expects individual schools to do this.
Whilst this is certainly happening in
some schools, it would be reasonable to
expect the GMC as the instigator of the
change to expedite a national evalu-
ation.
In 1988, Bloom described the myriad
attempts to change curricula up to that
point as �reform without change�.2 He
argued that the scientific mission of
academic medicine had dominated the
institutional structures to the extent that
curriculum reform was little more than a
screen to present a semblance of
rational change. This picture still res-
onates today – the Research Assessment
Exercise may have more impact on
teaching than any educational initiative.
More effort directed at ensuring condi-
tions which facilitate teaching at a
national level (e.g. redressing the fund-
ing imperative to prioritise research,
making SIFT more visible and account-
able) could impact in a more posit-
ive and lasting way than a new set of
curriculum recommendations, however
worthy.
Mary Seabrook
London, UK
References1 Christopher DF, Harte K, George CF.
The implementation of Tomorrow’s
Doctors. Med Educ 2002;36:282–8.
2 Bloom SW. Structure and ideology in
medical education: an analysis of resist-
ance to change. Journ Health Soc Behav
1988;29:294–306.
Can students in a modifiedPBL curriculum exceed thenational mean on USMLEPart 1?
Editor – The objective of this study was
to compare scores of students in a mo-
dified problem-based learning (PBL)
curriculum to national means on Step 1
of USMLE for the years 1992–2001.
The design was to compare student
performance on Step 1 of USMLE for
the years 1992–2001 to national means
by a paired t-test. The programme’s
inception date was the autumn of 1990.
Also, performance in the years 1994–99
was compared to national means by
paired t-test after adjusting for entering
Grade Point Average and Medical
College Admission Test scores. The
setting was a 2-year regional center of a
state-supported US medical school with
a hybrid lecture-based and problem-
based curriculum. One hundred and
eighty-eight students assigned to the
Northwest Center (one of the regional
centers of Indiana University School of
Medicine) were used in the study. Total
scores on Step 1 for the years 1992–
2001 showed that PBL students from
the Northwest Center scored signifi-
cantly higher than the national mean
with a P-value equal to 0Æ0006. This was
also true on 5 of the 8 discipline scores
for the years 1992–98. The P-values for
Biochemistry ¼ 0Æ00, Gross Anatomy
¼ 0Æ01, Histology ¼ 0Æ03, Microbio-
logy ¼ 0Æ02 and Pathology ¼ 0Æ00.
The P-value in Physiology was 0Æ06.
Two discipline scores, Behavioural Sci-
ence (P ¼ 0Æ18) and Pharmacology
(P ¼ 0Æ24), were higher than national
means, but not at the 0Æ05 level of sig-
nificance. Discipline scores were not
reported after 1998. When the results
for the years 1994–99 were normalised
by correcting for variations in student
performance on MCAT and GPA,
Northwest Center students’ total scores
were significantly higher than the
national mean with P-value equal to
0Æ0002. The retention rate for the
Northwest Center was 0Æ08% higher
than for Indiana University School of
Medicine at large. Our conclusions were
that medical students exposed to the
PBL curriculum, as practised at the
Northwest Center, score significantly
higher than the national mean on Step 1
of USMLE. Neither selection of high-
quality students nor an increased failure
rate could explain these findings. The
major difference between our system
and most PBL curricula is that ours is
mostly discipline-based.
William Baldwin
Patrick Bankston
W Marshall Anderson
Steve Echtenkamp
Richard Haak
Paula Smith
P G Iatridis
Gary, Indiana, USA
Effect of an early rural place-ment on internship choices ofmedical students
Editor – In an earlier issue of the journal
we reported that a voluntary rural
placement in the third year of a medical
course had a positive effect on students’
feelings towards rural practice.1 Because
of the lack of longitudinal studies, we
recommended that the 1992–94 student
cohorts who had been offered the
placement should be followed up to
determine whether an early rural place-
ment actually does influence career
choices. We are now able to report on
whether the placement influenced
where students undertook their intern-
ships.
Between 1998 and 2002, 480 (89%)
of the Australian students in the cohort
undertook internships at Victorian hos-
pitals. During that period, up to 328
internships had been offered each year:
75% by inner Melbourne hospitals,
15% by outer Melbourne hospitals and
10% by regional hospitals. All were at
least affiliated with a medical school,
with the inner Melbourne and one of
the regional hospitals being major
teaching institutions. Almost all of the
internships had been available only to
Victorian medical graduates with per-
Correspondence: William Baldwin, Northwest
Center for Medical Education, Indiana
University School of Medicine, 3400
Broadway, Gary, IN 46408, USA. Tel.: 00
1219 9806509; E-mail: [email protected]
Correspondence: Mary Seabrook, Department
of Medical and Dental Education, Sherman
Education Centre, 4th Floor, Thomas Guy
House, Guys Hospital, London, SE1 9RT,
UK. Tel.: 0207 955 5000 · 5635; Fax:
0207 955 2766; E-mail: Mary.seabrook@
kcl.ac.uk
Letters to the Editor 791
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:788–792

manent residency status. The Victorian
Postgraduate Medical Council matched
the preferences of the graduates as
closely as possible with those of the
hospitals.
The proportion of students under-
taking internships in regional as well as
outer Melbourne hospitals increased
significantly between the 1992 and 1994
cohorts. The combined figure for
regional and outer Melbourne hospitals
increased from 6Æ2% for the 1992
cohort, through 14Æ9% for the 1993
cohort, to 17Æ1% for the 1994 cohort
(Mantel-Haenszel test for a linear trend,
P ¼ 0Æ011). However, the proportion
of students having completed the third
year placement who undertook intern-
ships in a regional or outer Melbourne
hospital did not differ significantly from
that of other students (13% vs. 14%).
The proportion of students with a rural
background undertaking internships in
such hospitals also did not differ signif-
icantly from that of other students (17%
vs. 13%). Thus neither the early place-
ment nor a rural background accounted
for the increase.
When selecting interns hospitals use a
score allocated to students according to
marks obtained in subjects throughout
their course. Students who undertook
an internship in a regional or outer
Melbourne hospital had scores which
were, on average, significantly lower
than that of other students (61Æ8% vs.
66Æ4%, t-test, P ¼ 0Æ002). Moreover,
the scores of such students were, on
average, significantly lower for the later
cohort than the early one (59Æ0% vs.
64Æ9%, t-test, P < 0Æ001). Conversely,
students who had undertaken the rural
placement or with a rural background
had significantly higher scores than
other students. They would, therefore,
have been well placed to obtain their
preferred internships.
It would appear that the higher
achieving students are sought by and
seek out the inner Melbourne hospitals
for internships, regardless of the effect
an early placement had on their feelings
towards rural practice at the time or
their background. The cohorts could
continue to be followed to determine
whether an early placement or rural
background influences career choices
later on. A longitudinal study of the
later career choices of regional interns
might also prove insightful.
Hedley Peach
Nicole Barnett
The University of Melbourne,
Ballarat Health Services,
Australia
Reference1 Peach HG, Bath NE. Comparison of
rural and non-rural students undertak-
ing a voluntary rural placement in the
early years of a medical course. Med
Educ 2000;34:231–3.
Correspondence: Professor Hedley Peach, The
University of Melbourne, Ballarat Health
Services Base Hospital, PO Box 577,
Ballarat, Victoria, 3353, Australia. Tel.: 00
3 5320 4077; Fax: 00 3 5320 4078; E-mail:
Letters to the Editor792
� Blackwell Science Ltd MEDICAL EDUCATION 2002;36:788–792