Embed Size (px)
Citation preview

American Journal of Medical Genetics Part B (Neuropsychiatric Genetics) 141B:173–176 (2006)
CAG Repeats in Restless Legs SyndromeMarkus Konieczny,1,5 Peter Bauer,2 Jurgen Tomiuk,2 Gabriele Weisser,2 Jean Haan,3 Klaus Berger,4 Olaf Riess,2
and Ludger Schols1*1Department of Neurology and Hertie Institute for Clinical Brain Research, University of Tubingen, Tubingen, Germany2Medical Genetics, University of Tubingen, Tubingen, Germany3Department of Neurology, Maria-Hilf Krankenhaus, Monchengladbach, Germany4Institute of Epidemiology and Social Medicine, University of Muenster, Muenster, Germany5Department of Neurology, St. Josef Hospital, Ruhr-University Bochum, Bochum, Germany
Recent reports established an association of rest-less legs syndrome (RLS) and spinocerebellarataxia (SCA) type 1, 2, and 3. To evaluate thecontribution of SCA alleles to idiopathic RLS weinvestigated the CAG repeat length at the SCA1,SCA2, SCA3, SCA6, SCA7, and SCA17 loci in215 patients who fulfilled the clinical criteria ofRLS and presented periodic leg movements insleep (PLMS) in polysomnographic recording.Fifty percent of patients had a positive familyhistory of RLS. We found one intermediate(CAG)43 allele for SCA17 in a 44-year-old femalewith RLS starting at the age of 43. Neurologicexamination and family history were unremark-able in this patient. Otherwise, allele distributiondid not differ between RLS patients and healthycontrols. Stratification for age, age of onset, sex,peripheral neuropathy, and sporadic or familialRLS revealed no effect. Thus, CAG repeat lengthin the investigated genes is not a major determi-nant of idiopathic or familial RLS.� 2006 Wiley-Liss, Inc.
KEY WORDS: restless legs syndrome; spinocer-ebellar ataxia; CAG repeat length
INTRODUCTION
Restless legs syndrome (RLS) is definedby thedesire tomovethe limbs usually associated with dysesthesias of the legs, amotor restlessness, a worsening or exclusive presence ofsymptoms at rest with relief by activity, and a worsening ofthe symptoms in the evening or during the night. RLS isfrequently (80–90%) associated with periodic leg movementsin sleep (PLMS) resulting inmultiple arousals anddisturbanceof sleep profile. RLS affects 5–15% of the general populationand shows familial aggregation in about 60% of reported cases[Rothdach et al., 2000]. Further evidence for the involvement ofgenetic factors in the etiology of RLS is derived from a twinstudy that found a concordance rate of 85% in identical twins.Recently, two susceptibility loci for RLS with autosomalrecessive and autosomal dominant inheritance have been
mapped to chromosomes 12q and 14q, respectively [Desautelset al., 2001; Bonati et al., 2003].
Two studies described increased frequencies of RLS inspinocerebellar ataxia (SCA) type 1, 2, and 3 [Schols et al.,1998; Abele et al., 2001]. Additionally, our observation in apatient who suffered for 25 years from RLS and peripheralneuropathy before, at age 65 years the onset of ataxia led to thediagnosis of SCA3 with a mild expansion (CAG)63, stimulatedus to test the hypothesis that large normal or intermediatealleles of polyglutamine disorders may be linked to RLS [VanAlfen et al., 2001]. To clarify this issue, we analyzed CAGrepeat length in six SCA genes in 215 polysomnographicallyproven RLS/PLMS patients in comparison to 70 controls froman elderly population without a history of RLS.
PATIENTS AND METHODS
Patients
We included 215 patients with the diagnosis of RLSaccording to the minimal criteria of the International RestlessLegsStudyGroup [Allen et al., 2003]. In all patientsPLMSwasalso diagnosed in polysomnographic recordings at the sleeplaboratory of the Maria-Hilf Hospital in Monchengladbach.Detailed clinical characteristics of the patient group areprovided in Table I. Seventy elderly control subjects withexclusion of RLS by interview and neurologic examinationwere recruited from the MEMO Study [Rothdach et al., 2000].All participants signed an appropriate informed consent formbefore blood was taken for genetic analysis.
PCR Genotyping of SCA Loci
Genomic DNA of 50–100 ng was used per PCR reaction. Weestablished two triplex primer assays for fast genotyping ofSCA2, SCA3, and SCA17 or SCA1, SCA6, and SCA7. Primersequences, PCR components, and profiles are given in Table II.After PCR reaction the amplicons were diluted 1:100 and 5 ml
TABLE I. Clinical Characteristics of RLS Patients andPopulation Controls
CharacteristicsRLS patients,
N¼215 Controls, N¼70
Age [years] 58.3�12.8 67.6� 1.7Sex (male/female) 105/110 35/35Peripheral neuropathy [%] 9.3 n.a.Age at onset of RLS [years] 49.3�15.7Familial RLS [%] 50Severity of RLSa 14.9�5.5
Data are given as mean� standard deviation.aInternational RLS Study Group Rating Scale.
*Correspondence to: Ludger Schols, M.D., Department ofNeurology and Hertie Institute for Clinical Brain Research,University of Tubingen, Hoppe-Seyler-Str. 3, D-72076 Tubingen,Germany. E-mail: [email protected]
Received 23 June 2005; Accepted 21 October 2005
DOI 10.1002/ajmg.b.30265
� 2006 Wiley-Liss, Inc.

was mixed with 35 ml sample loading solution (BeckmanCoulter, Krefeld, Germany). Fragments were run on aCEQ8000 capillary sequencer (Beckman Coulter) and geno-types were called using the ‘‘fragments’’ software tool of theCEQ8000 software. As CAG repeats do not perfectly result in a3-bp spacing, expected fragment lengths were compared withknown (sequenced) genotype standards and the allele callingwas adapted accordingly.
Statistics
Non-parametric statistics were used when the distributionof repeat length was compared between both groups (Wilcoxontwo sample test; NPAR1WAY procedure, SAS 2003). Pairwisecorrelations between parameters were analyzed with theCORR procedure (SAS, 2003). In cases of multiple testing, a
sequential Bonferoni procedure was applied in order tocompensate for an inflating type 1 error. For all tests asignificance level of 5% was accepted.
RESULTS
Wedetected an intermediate (CAG/CAA)43 allele in the genefor TATA binding protein (SCA17) in a 44-year-old female whoattended the sleep laboratory because of RLS starting at theage of 43 years. Neurologic examination was normal; inparticular there were no signs of ataxia. Family history wasunremarkable, especially for RLSbut also for gait disturbance,and dementia. No other CAG repeat in the pathogenic orintermediate rangewas identified in RLS or control subjects inanyof theSCAgenes studied.Allele distribution and statisticalevaluation for the different genotypes is given in Figure 1. Our
TABLE II. Primer Sequences and Fluorescent Labels
Forward primer Reverse primer
SCA1 50 CY5 caa cat ggg cag tct gag c 30 50 gaa ctg gaa atg tgg acg tac 30
SCA2 50 CY5 ccc tca cca tgt cgc tga agc 30 50 cga cgc tag aag gcc gct g 30
SCA3 50 CY5.5 cca gtg act act ttg att cg 30 50 tgg cct ttc aca tgg atg tga a 30
SCA6 50 CY5 cac gtg tcc tat tcc cct gtg atc c 30 50 tgg gta cct ccg agg gcc gct ggt g 30
SCA7 50 CY5.5 tgt tac att gta gga gcg gaa 30 50 cac gac tgt ccc agc atc act t 30
SCA17 50 CY5 gac ccc aca gcc tat tca ga 30 50 ttg act gct gaa cgg ctg ca 30
PCR conditions for SCA1, 6, 7 PCR (25 ml volume): 1� PCR buffer, 2.0 mMMgCl2, 0.4 mMdNTPs, 10% DMSO, 1 UTaq polymerase (Roche Expand Long, Roche, Mannheim, Germany), 35 pmol SCA1 primers, 15 pmol SCA6primers, 15 pmol SCA7 primers (forward and reverse, each), 50 ng genomic DNA. Cycling: 4 min 948C; 34 cycles[30 sec 948C, 30 sec 578C, 30 sec 728C], 10 min 728C.PCR conditions for SCA2, 3, 17 PCR (25 ml volume): 1� PCR buffer, 2.5 mMMgCl2, 0.4 mMdNTPs, 5% DMSO, 1 UTaq polymerase (Roche Expand Long, Roche), 20 pmol SCA2 primers, 15 pmol SCA3 primers, 30 pmol SCA17primers (forward and reverse, each), 50 ng genomic DNA. Cycling: 4 min 948C; 30 cycles [30 sec 948C, 30 sec 608C,30 sec 728C], 10 min 728C.
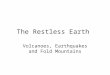
Fig. 1. Allele distribution in RLS patients (black bars) provided for and control subjects (white bars) are provided for (A) SCA1, (B) SCA2, (C) SCA3, (D)SCA6, (E) SCA7, and (F) SCA17. Wilcoxon z values are given for two-sided normal approximation of allele frequencies in the respective SCA subtype. Afterapplication of the sequential Bonferoni procedure as correction for multiple testing, no significant P values remained.
174 Konieczny et al.

statistical analyses outlined three Wilcoxon scores to bemarginally (0.05>P> 0.01) significant between the medianrepeat length differences in SCA1, SCA3, and SCA7 (medianrepeat lengths had been�0.15CAG repeats for SCA1, 1.2 CAGrepeats for SCA3, and �0.32 CAG repeats for SCA7). Afterapplication of the sequential Bonferoni procedure, no signifi-cant P values remained. Stratification for gender, familiarity,age at onset, presence of polyneuropathy, and severity of RLSaccording to the International RLS Study Group Rating Scalerevealed only an association of polyneuropathy and CAGrepeat length in SCA1. Likewise, this difference did not resistthe Bonferoni procedure (Table III).
DISCUSSION
RLS occurs with higher frequency in patients with SCA1,SCA2, and especially SCA3 than in the general population[Schols et al., 1998; Abele et al., 2001]. Additionally, priorstudies observed patients who had RLS for many years beforethe onset of ataxia led to thediagnosis of SCA3 [VanAlfenet al.,
2001]. These observations prompted us to look for abnormaldistribution of SCA alleles in a population of patients withidiopathic or familial RLS.
All known SCA subtypes caused by expanded polyglutaminestretches were screened for the polymorphic CAG repeats inthe respective genes. In this association study we could notestablish a substantial link betweenCAGrepeat length in SCAgenes and RLS.
This interpretation is in accordance with a recent study ofDesautels et al. [2003] who found similar CAG repeat lengthsin the SCA3 gene between RLS patients and healthy controls.However, interpretation ofDesautels’ study is limited in that itis likely that the control group enclosed up to 15% of RLSpatients occurring in the general population [Rothdach et al.,2000] and thus may have missed minor shifts in SCA3 alleledistribution. To avoid such biaswe excluded individuals with ahistory of RLS according to a standardized RLS questionnairefrom the control group. Additionally, we substantiated thediagnosis of RLS by recruiting only patients with polysomno-graphic evidence of PLMS. In contrast to Desautels et al., wedid not excludeRLSpatientswith peripheral neuropathy sinceneuropathy is frequent in SCA1, SCA2, and SCA3 andexclusion of such patients may cause a bias against largeSCA alleles. Average age at onset of RLS in our populationwas49 years and matched well with age of RLS onset reported inSCA patients (44–54 years depending on genotype) [Scholset al., 1998; Abele et al., 2001].
The finding of a (CAG/CAA)43 allele in the gene for TATAbinding protein (SCA17) is difficult to interpret. There are noreports on RLS in SCA17; however, this issue has not beenstudied systematically. Since we analyzed CAG repeats of sixgene loci in 215 RLS patients, the statistical chance to find anexpanded allele was 1:13 when the prevalence of SCA in thegeneral population is 3:100,000 [Van de Warrenburg et al.,2002]. Considering the absence of a general shift towards largenormal alleles in SCA17 in our RLS population we do not seeevidence that the finding of one intermediate SCA17 allelepoints towards an association of SCA alleles and RLS.
SCA17 is special among SCAs in that it shows reducedpenetrance for alleles with 43–48 CAG repeats [Zuhlke et al.,2003].However, patientswith intermediate SCA17alleleswhodo not develop ataxia or cognitive deficits have not beenreported to present with RLS or other alternate signs as aminimal variant of SCA17 [Zuhlke et al., 2003]. This isdifferent in SCA3 in which intermediate alleles of 53–56CAG repeats are reported to be associated with familial formsof RLS and peripheral neuropathy [Van Alfen et al., 2001].
In conclusion, our study excludes CAG repeats in SCA genesas amajor cause of idiopathic or familial RLS.Different geneticfactors are likely to be responsible for the high percentage ofRLS patients (up to 60%) having a positive family history andremain to be elucidated.
Fig. 1. (Continued)
TABLE III. Wilcoxon z Values for the Differences in CAG Repeat Lengths in RLS Patients Stratified for Gender, Familiarity, andPolyneuropathy
Gender allele count[male/female]
Familiarity allele count [positive/negative/not informative]
Polyneuropathy allelecount [present/absent]
Age at onset[observations]
RLS score[observations]
SCA1 z¼0.335; n.s. [202/206] z¼0.815; n.s. [80/82/246] z< 0.05; [38/364] r2¼0.465 [252] r2¼0.518 [192]SCA2 z¼0.230; n.s. [206/216] z¼0.957; n.s. [84/86/252] z¼0.628; n.s. [38/378] r2¼0.728 [260] r2¼0.411 [202]SCA3 z¼0.964; n.s. [202/214] z¼0.837; n.s. [82/84/250] z¼0.079; n.s. [38/372] r2¼0.434 [254] r2¼0.611 [198]SCA6 z¼0.259; n.s. [204/210] z¼0.775; n.s. [82/84/248] z¼0.548; n.s. [36/372] r2¼0.349 [256] r2¼0.732 [196]SCA7 z¼0.679; n.s. [112/130] z¼0.677; n.s. [48/56/138] z¼0.806; n.s. [24/212] r2¼0.838 [156] r2¼0.934 [114]SCA17 z¼0.850; n.s. [206/212] z¼0.156; n.s. [80/86/252] z¼0.499; n.s. [38/374] r2¼0.728 [256] r2¼0.368 [198]
z values are given for two-sided normal approximation. n.s.¼not significant. For correlation analysis (age at onset and RLS severity) Pearson correlationcoefficients are given.
CAG in RLS 175

REFERENCES
Abele M, Burk K, Laccone F, et al. 2001. Restless legs syndrome inspinocerebellar ataxia types 1, 2, and 3. J Neurol 248:311–314.
Allen RP, Oicchietti D, Hening WA, et al. 2003. Restless legs syndrome:Diagnostic criteria, special considerations, and epidemiology. A reportfrom the restless legs syndrome diagnosis and epidemiologyworkshop atthe National Institute of Health. Sleep Med 4:101–119.
Bonati MT, Ferini-Strambi L, Aridon P, et al. 2003. Autosomal dominantrestless legs syndromemaps on chromosome 14q. Brain 126:1485–1492.
Desautels A, Turecke G, Montplaisir J, et al. 2001. Identification of a majorsusceptibility locus for restless legs syndrome on chromosome 12q. Am JHum Genet 69:1266–1270.
Desautels A, Turecke G, Montplaisir J, et al. 2003. Analysis of CAG repeatexpansions in restless legs syndrome. Sleep 26:1055–1057.
Rothdach AJ, Trenkwalder C,Haberstock J, et al. 2000. Prevalence and riskfactors of RLS in an elderly population: The MEMO study. Memory andMorbidity in Augsburg Elderly. Neurology 54:1064–1068.
Schols L, Haan J, Riess O, et al. 1998. Sleep disturbance in spinocerebellarataxia type 3: Is the SCA3 mutation a cause of restless legs syndrome?Neurology 51:1603–1607.
Van Alfen N, Sinke RJ, Zwarts MJ, et al. 2001. Intermediate CAG repeatlengths (53, 54) for MJD/SCA3 are associated with an abnormalphenotype. Ann Neurol 49:805–807.
Van de Warrenburg BPC, Sinke RJ, Verschuuren-Bemelmans CC, et al.2002. Spinocerebellar ataxias in theNetherlands. Provalence and age atonset variance. Neurology 58:702–708.
ZuhlkeC,GehlkenU,HellenbroichY, et al. 2003. Phenotypical variability ofexpanded alleles in theTATA-bindingprotein gene.Reducedpenetrancein SCA17? J Neurol 250:161–163.
176 Konieczny et al.