Embed Size (px)
Citation preview

COLONCOLONJames Taclin C. Banez, MD, James Taclin C. Banez, MD, FPCS, FPSGS, DPBS, DPSAFPCS, FPSGS, DPBS, DPSA

Anatomy / Physiology:Anatomy / Physiology:• Location, blood supply Location, blood supply
& venous drainage, & venous drainage, lymphatic drainage lymphatic drainage and nerve supplyand nerve supply
• Function: Function: • absorption of fluid absorption of fluid
and electrolyteand electrolyte• Transport and Transport and
temporary storage temporary storage of fecesof feces

Anatomy / Physiology:Anatomy / Physiology:

1.1. Amebic colitis:Amebic colitis: Entamoeba histolyticaEntamoeba histolytica Primary – colon : secondary – liverPrimary – colon : secondary – liver Fecal to oral route: (sexual contact, Fecal to oral route: (sexual contact,
contaminated water & food)contaminated water & food) Abdominal pain, bloody diarrhea, Abdominal pain, bloody diarrhea,
tenesmus, fevertenesmus, fever Complication: megacolon / colonic Complication: megacolon / colonic
obstruction (partial) ---obstruction (partial) ---> > AMEBOMAAMEBOMA – – mass of inflammatory tissuemass of inflammatory tissue
Dx: clin hx / stool exam / indirect Dx: clin hx / stool exam / indirect hemagglutination testhemagglutination test
Tx: metronidazole / iodoquinol : rare Tx: metronidazole / iodoquinol : rare COLECTOMYCOLECTOMY
Infectious:Infectious:

Infectious:Infectious:2.2. Pseudomembranous colitis:Pseudomembranous colitis:
• Complication of antibiotics ---> alteration of normal Complication of antibiotics ---> alteration of normal floraflora
• Overgrowth of Overgrowth of Clostridium deficileClostridium deficile::• Has Has cytopathic cytopathic and and enteropathic toxinsenteropathic toxins
• Develops 6wks after:Develops 6wks after:a.a. ClindamycinClindamycinb.b. AmpicillinAmpicillinc.c. CephalosporinCephalosporin
Dx:Dx: - history- history- latex fixation test- latex fixation test- colonoscopy (- colonoscopy (PseudomembranePseudomembrane))
Tx: - stopped antibiotic ----> Tx: - stopped antibiotic ----> metronidazole/vancomycinmetronidazole/vancomycin- - cholestyraminecholestyramine ---> binds w/ toxin ---> binds w/ toxin- Toxic megacolon---> - Toxic megacolon---> total colectomy w/ ileostomytotal colectomy w/ ileostomy

Infectious:Infectious:
3.3. Salmonellosis: Salmonellosis: • Salmonella typhi (typhoid fever)Salmonella typhi (typhoid fever)• Dx: perforation / bleedingDx: perforation / bleeding• Tx: antibiotic / transfusion / right Tx: antibiotic / transfusion / right
hemicolectomy w/ or w/o hemicolectomy w/ or w/o ileostomyileostomy

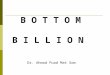
Volvulus:Volvulus:• Twisting of an air-filled segment of Twisting of an air-filled segment of
bowel about its narrow mesentery ---> bowel about its narrow mesentery ---> OBSTRUCTIONOBSTRUCTION -------> -------> STRANGULATION STRANGULATION ----> ----> GANGRENEGANGRENE----> ----> PERFORATIONPERFORATION ----> ----> PERITONITISPERITONITIS
1.1. SIGMOID VOLVULUS (90%):SIGMOID VOLVULUS (90%):• Redundant sigmoid colonRedundant sigmoid colon
w/ a narrow based mesocolonw/ a narrow based mesocolon• Sx: colicky abd. pain, distentionSx: colicky abd. pain, distention
obstipation, rectal collapseobstipation, rectal collapses/sx of dehydration s/sx of dehydration

Volvulus:Volvulus:SIGMOIDSIGMOID
VOLVULUS (90%):VOLVULUS (90%):Dx:Dx: FPA – FPA – inverted inverted
U shaped U shaped sausage like sausage like loop (diagnostic)loop (diagnostic)
• Barium enema – Barium enema – bird beaks bird beaks deformitydeformity
• Gangrene –Gangrene – chills/fever, chills/fever, leukocytosis w/ s/x leukocytosis w/ s/x of peritoniof peritoni

Volvulus:Volvulus:1.1. SIGMOID VOLVULUS (90%):SIGMOID VOLVULUS (90%):
Tx: Tx:
(-) Signs of Peritonitis:(-) Signs of Peritonitis: Reduced the volvulus --->prepare for Reduced the volvulus --->prepare for
elective colonic surgery for the recurrence elective colonic surgery for the recurrence is 40%:is 40%:
- use of flexible scope- use of flexible scope
(+) Signs of Peritonitis / Unsuccessful (+) Signs of Peritonitis / Unsuccessful reduction:reduction:
Sigmoidectomy w/ Hartmanns or Divine’s Sigmoidectomy w/ Hartmanns or Divine’s colostomycolostomy

Volvulus:Volvulus:2.2. Cecal Volvulus:Cecal Volvulus:
Tx: reduction is impossible --> emergency Tx: reduction is impossible --> emergency explorationexploration(+) Gangrene: (+) Gangrene: - right hemicolectomy- right hemicolectomy
- end to end ileo-transverse colostomy- end to end ileo-transverse colostomy
(-) Gangrene:(-) Gangrene: a) – same –a) – same –
b) Cecopexyb) Cecopexy
c) Pure detorsion (recurrence 7 – c) Pure detorsion (recurrence 7 – 15%)15%)
3.3. Transverse colon volvulus:Transverse colon volvulus: Rare, due to it’s broad based and short Rare, due to it’s broad based and short
mesenterymesentery Tx: resection of redundant transverse colonTx: resection of redundant transverse colon

DIVERTICULOSIS:DIVERTICULOSIS: Abnormal pouchAbnormal pouch from the wall of a hollow organ from the wall of a hollow organ Types:Types:
1.1. True diverticulaTrue diverticula (rare) – right side (rare) – right side
2.2. False diverticulaFalse diverticula (common – due to low fiber diet: (common – due to low fiber diet: left side)left side)
Rare before 30y/o; common > 75 y/oRare before 30y/o; common > 75 y/o Female > MaleFemale > Male Etiology:Etiology:
1.1. UnknownUnknown
2.2. Theories by Painter et al:Theories by Painter et al:
a)a) Contraction ringContraction ring (thickening of circular muscle) (thickening of circular muscle)
b)b) Depletion of dietary fibersDepletion of dietary fibers ---> narrow lumen ---> narrow lumen
c)c) Deteriorating integrity of the bowel wallDeteriorating integrity of the bowel wall; elderly ; elderly has lower tensile strength, lowest in the sigmoid)has lower tensile strength, lowest in the sigmoid)

DIVERTICULOSIS:DIVERTICULOSIS: Pathology:Pathology:
Site: anteriole Site: anteriole penetrates the penetrates the mesenteric side mesenteric side of the of the antimesenteric antimesenteric teniae coli:teniae coli:
1.1. Sigmoid Sigmoid (50%)(50%)
2.2. Descending Descending colon (40%)colon (40%)
3.3. Entire colon Entire colon (2-10%)(2-10%)

DIVERTICULOSIS:DIVERTICULOSIS:Clinical Manifestation:Clinical Manifestation:A.A. Majority are Majority are asymptomaticasymptomatic
B.B. Symptomatic patients:Symptomatic patients:1.1. Uncomplicated painful diverticular Uncomplicated painful diverticular
dse.dse. (+) LLQ (+) LLQ pain and tenderness; pain and tenderness; (+) change in bowel habits(+) change in bowel habits (-) rebound tenderness(-) rebound tenderness (-) fever nor leukocytosis(-) fever nor leukocytosis
Dx: Gastrografin enemaDx: Gastrografin enema Tx: high fiber dietTx: high fiber diet

DIVERTICULOSIS:DIVERTICULOSIS:Clinical Manifestation:Clinical Manifestation:B.B. Symptomatic patients:Symptomatic patients:
2.2. Complicated diverticular disease:Complicated diverticular disease:
a.a. Diverticulitis / Peridiverticulitis:Diverticulitis / Peridiverticulitis: Infected diverticulaInfected diverticula Diverticula is filled up ---> Diverticula is filled up --->
obstructed ---> mucus secretion and obstructed ---> mucus secretion and bacteria ---> inflammation at the bacteria ---> inflammation at the apex ---> unresolved --> extend apex ---> unresolved --> extend intramurally ---> intramurally ---> perforate.perforate.

DIVERTICULOSIS:DIVERTICULOSIS:
a.a. Diverticulitis / Peridiverticulitis:Diverticulitis / Peridiverticulitis:Sx:Sx: - left lower abd. pain / - left lower abd. pain /
chills & fever / chills & fever / bowel habit changesbowel habit changes
- (+) abd. Tenderness, - (+) abd. Tenderness, distension if w/ distension if w/
partial obstructionpartial obstruction- pararectal tenderness - pararectal tenderness - frequency / urgency of - frequency / urgency of
urination urination (inflamed bladder)(inflamed bladder)

DIVERTICULOSIS:DIVERTICULOSIS:a.a. Diverticulitis Diverticulitis
/ / PeridiverticulPeridiverticulitis:itis:Dx: Dx: 1)1) Cln. Hx.Cln. Hx.2)2) Ct scan of the abd Ct scan of the abd
/ utrasonography / utrasonography (thickened wall & (thickened wall & abscess can be abscess can be seen)seen)
3)3) Contrast enema / Contrast enema / sigmoidoscopy sigmoidoscopy (risk of spreading (risk of spreading infection)infection)

DIVERTICULOSIS:DIVERTICULOSIS:
a.a. Diverticulitis / Diverticulitis / Peridiverticulitis:Peridiverticulitis:
Tx:Tx:
1)1) NPO or liquid dietNPO or liquid diet
2)2) Broad spectrum antibioticBroad spectrum antibiotic
3)3) Meperidine (not morphine)Meperidine (not morphine)
4)4) If improved If improved endoscopy to r/o endoscopy to r/o CACA

DIVERTICULOSIS:DIVERTICULOSIS:2.2. Complicated diverticular disease:Complicated diverticular disease:
b.b. Perforated Diverticulitis:Perforated Diverticulitis:Sx:Sx: - similar to appendicitis - similar to appendicitis
(Phlegmon mass)(Phlegmon mass)- (+) pneumoperitoneum- (+) pneumoperitoneum- Classification of perforated - Classification of perforated diverticulitis diverticulitis
(Hinchy)(Hinchy)Stage IStage I: abscess confined by : abscess confined by mesentery of colonmesentery of colonStage IIStage II: pelvic abscess : pelvic abscess Stage IIIStage III: generalized peritonitis: generalized peritonitisStage IVStage IV: fecal peritonitis : fecal peritonitis

DIVERTICULOSIS:DIVERTICULOSIS:b.b. Perforated Diverticulitis:Perforated Diverticulitis:
Tx: initial nonoperative:Tx: initial nonoperative:
- NPO / IVF / Broad spectrum - NPO / IVF / Broad spectrum antibiotic/antibiotic/
meperidinemeperidine Stage I & II: Stage I & II:
(+) improvement (+) improvement elective Surgery (4 elective Surgery (4 wks)wks)
(-) improvement (-) improvement percutaneous percutaneous drainagedrainage
(-) improvement ---> Surgery(-) improvement ---> Surgery

DIVERTICULOSIS:DIVERTICULOSIS:Perforated Diverticulitis:Perforated Diverticulitis:
Tx: initial nonoperative:Tx: initial nonoperative:
- NPO / IVF / Broad spectrum - NPO / IVF / Broad spectrum antibiotic/meperidineantibiotic/meperidine Stage III & IV:Stage III & IV:
explore after initial resuscitationexplore after initial resuscitation
a. sigmoidectomy w/ primary anastomosisa. sigmoidectomy w/ primary anastomosis
b. sigmoidectomy w/ Hartmann’s colostomyb. sigmoidectomy w/ Hartmann’s colostomy
c. resection w/ primary anastomosis w/ c. resection w/ primary anastomosis w/ proximal proximal
diverting stomadiverting stoma
d. drainage w/ diverting transverse d. drainage w/ diverting transverse colostomycolostomy

DIVERTICULOSIS:DIVERTICULOSIS:2.2. Complicated diverticular disease:Complicated diverticular disease:
c.c. Obstructing diverticulitis:Obstructing diverticulitis: 90% partial – due to spasm, edema 90% partial – due to spasm, edema
& ileus& ileus 10% complete – fibrosis and 10% complete – fibrosis and
stenosisstenosis S/Sx: of large intestinal obstructionS/Sx: of large intestinal obstruction Tx: conservative mx (3-5 days) ---> Tx: conservative mx (3-5 days) --->
(-) response -----> cecum dilates to (-) response -----> cecum dilates to 10-12 cm. ---> surgery.10-12 cm. ---> surgery.

DIVERTICULOSIS:DIVERTICULOSIS:Clinical Clinical
Manifestation:Manifestation:B.B. Symptomatic Symptomatic
patients:patients:2.2. Complicated Complicated
diverticular diverticular disease:disease:d.d. Acute Acute
hemorrhage:hemorrhage: Due to erosion Due to erosion
of the of the peridiverticular peridiverticular arteriole by arteriole by inspissated stool inspissated stool w/in the w/in the diverticulum diverticulum and thinning of and thinning of the tunica mediathe tunica media

DIVERTICULOSIS:DIVERTICULOSIS:d.d. Acute hemorrhage:Acute hemorrhage:- Resuscitate the patientResuscitate the patient- Locate the site of Locate the site of
bleeding (Tc labeled bleeding (Tc labeled RBC/selective RBC/selective arteriography)arteriography)
- Vasopressin infusion, Vasopressin infusion, transcatheter emboli transcatheter emboli infusion using gelfoaminfusion using gelfoam
- ColonoscopyColonoscopy- Tx: segmental resection / Tx: segmental resection /
blind subtotal colectomyblind subtotal colectomy

DIVERTICULOSIS:DIVERTICULOSIS:2.2. Complicated diverticular disease:Complicated diverticular disease:
d.d. Fistula formation:Fistula formation: Bladder, vagina, small bowel, skinBladder, vagina, small bowel, skin Dx: - clin hx & PE (pneumaturia, Dx: - clin hx & PE (pneumaturia,
fecaluria and fecaluria and frequent frequent
UTI)UTI)
- cystoscopy, IE, speculum - cystoscopy, IE, speculum examexam
- methylene blue enema- methylene blue enema
- colonoscopy to r/o CA- colonoscopy to r/o CA

DIVERTICULOSIS:DIVERTICULOSIS:d.d. Fistula formation:Fistula formation:
Tx: - bowel rest w/ TPN or elemental dietTx: - bowel rest w/ TPN or elemental diet - Foley catheter (10 days postop) / - Foley catheter (10 days postop) /
antibioticantibiotic - placement of ureteral catheter prior - placement of ureteral catheter prior
to to celiotomyceliotomy
- sigmoidectomy w/ primary - sigmoidectomy w/ primary anastomosisanastomosis
- fistulectomy and closure of - fistulectomy and closure of secondary secondary
openingopening

Hemorrhage from the Hemorrhage from the Colon:Colon:1.1. Diverticular diseaseDiverticular disease2.2. AngiodysplasiaAngiodysplasia (Vascular (Vascular
ectasia, AV malformation, ectasia, AV malformation, AngiectasiaAngiectasia))

ANGIODYSPLASIAANGIODYSPLASIA Acquired lesionAcquired lesion Proximal colon (cecum) where Proximal colon (cecum) where
tension is greatest (Laplace’s law – tension is greatest (Laplace’s law – tension in the wall is highest in the tension in the wall is highest in the widest circumference)widest circumference)
Rare < 40y/o; common in elderlyRare < 40y/o; common in elderly Etiology: - chronic intermittent Etiology: - chronic intermittent
obstruction of submucosal veins due obstruction of submucosal veins due to repeated muscular contractionto repeated muscular contraction

ANGIODYSPLASIAANGIODYSPLASIA
Dx: Dx: - - Nuclear scan / Nuclear scan /
angiographyangiography = =
(vascular tuft and (vascular tuft and
early filling of veins)early filling of veins)
- - colonoscopycolonoscopy = =
distinct red distinct red
mucosal patchmucosal patch

Bleeding distal to the ligament of Bleeding distal to the ligament of Treitz:Treitz:
1.1. Diverticular diseaseDiverticular disease2.2. AngiodysplasiaAngiodysplasia3.3. Inflammatory bowel diseaseInflammatory bowel disease4.4. Ischemic colitisIschemic colitis5.5. TumorTumor6.6. Anticoagulant therapyAnticoagulant therapy
Gastroduodenal hgeGastroduodenal hge -> can present -> can present as rectal bleedingas rectal bleeding
It is more important to identify the It is more important to identify the location of the location of the BLEEDING POINTBLEEDING POINT than the immediate diagnosis as than the immediate diagnosis as the cause.the cause.

Diagnostic:Diagnostic:1.1. Nuclear imaging Nuclear imaging
(bleeding (bleeding scan/scintigraphy)scan/scintigraphy)
a.a. Technetium-Sulfur Colloid Technetium-Sulfur Colloid ScanScan
Sensitive Sensitive (0.5ml/min)(0.5ml/min)b.b. Autologous labeled RBC scanAutologous labeled RBC scan
Stays in the circulation for Stays in the circulation for as long as 24 hrs as long as 24 hrs (monitoring)(monitoring)
(1ml/min bleeding)(1ml/min bleeding)
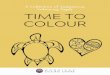
2.2. Mesenteric Mesenteric AngiographyAngiography
Done once patient’s Done once patient’s condition is stable and condition is stable and hydration is adequatehydration is adequate
Identify bleeding point ---> Identify bleeding point ---> 1ml/min1ml/min
Could be therapeutic ---> Could be therapeutic ---> Vasopressin/emboliVasopressin/emboli
Vascular taft (A)Vascular taft (A)Early filling vein (B)Early filling vein (B)

Diagnostic:Diagnostic:3.3. Emergent colonoscopy:Emergent colonoscopy:
Possible w/ use of GOLYTELYPossible w/ use of GOLYTELY TherapeuticTherapeutic
Treatment:Treatment: Restore intravascular volume (85% Restore intravascular volume (85%
stop spontaneously)stop spontaneously) Persistent --> celiotomy (segmental Persistent --> celiotomy (segmental
or total colectomy)or total colectomy)

Ischemic ColitisIschemic Colitis Due to occlusion of major mesenteric vesselDue to occlusion of major mesenteric vessel
Thrombosis, embolization, iatrogenic Thrombosis, embolization, iatrogenic ligationligation
Elderly:Elderly: - contraceptive pills- contraceptive pills
- medical problems:- medical problems:
a) cardiovascular diseasea) cardiovascular disease
b) DMb) DM
c) Rheumatoid arthritisc) Rheumatoid arthritis Splenic flexureSplenic flexure – most common site in the – most common site in the
coloncolon

Ischemic Colitis:Ischemic Colitis:Clinical Syndrome Based on:Clinical Syndrome Based on:
1.1. Extent of vascular occlusionExtent of vascular occlusion
2.2. Duration of occlusionDuration of occlusion
3.3. Efficiency of collateral circulationEfficiency of collateral circulation
4.4. Extent of secondary bacterial invasionExtent of secondary bacterial invasion
1.1. Reversible or Transient Ischemic Reversible or Transient Ischemic Colitis:Colitis:
Partial mucosal slough that healed after 2-3 daysPartial mucosal slough that healed after 2-3 days
2.2. Stricturing Ischemic Colitis:Stricturing Ischemic Colitis: Arterial occlusion ---> hge’ic infarct of mucosa ---Arterial occlusion ---> hge’ic infarct of mucosa ---
> ulcerates ----> bacterial invasion of bowel ---> > ulcerates ----> bacterial invasion of bowel ---> fibrosisfibrosis

Ischemic Colitis:Ischemic Colitis:
Clinical Syndrome Based on:Clinical Syndrome Based on:3.3. Gangrenous ischemic Colitis:Gangrenous ischemic Colitis:
Complete arterial occlusion ---> full Complete arterial occlusion ---> full thickness infarction ---> gangrene ---> thickness infarction ---> gangrene ---> perforation ----> PERITONITIS.perforation ----> PERITONITIS.

Ischemic Colitis:Ischemic Colitis:Symptoms:Symptoms:
Depends on the stage of the lesionDepends on the stage of the lesion Acute mild to moderate generalized Acute mild to moderate generalized
or lower abdominal crampy pain ---> or lower abdominal crampy pain ---> HEMATOCHEZIAHEMATOCHEZIA
Hyperactive bowel sound ---> silentHyperactive bowel sound ---> silent Abdominal tenderness ---> persist ---Abdominal tenderness ---> persist ---
>r/o peritonitis>r/o peritonitis

Ischemic Colitis:Ischemic Colitis:
Diagnosis:Diagnosis: Clinical hx & PEClinical hx & PE FPAFPA ---> ---> adynamic ileusadynamic ileus (stops at (stops at
the involved segment); the involved segment); PneumoperitoneumPneumoperitoneum
Contrast enemaContrast enema (water soluble) (water soluble)
- - thumb printingthumb printing in the in the mucosamucosa
EndoscopyEndoscopy (risky) (risky)

Ischemic Colitis:Ischemic Colitis:
Treatment:Treatment:Emergency celiotomyEmergency celiotomy
- segmental resection - segmental resection w/ primary w/ primary
anastomosis or anastomosis or colostomycolostomy

Fecal impaction:Fecal impaction: Is the arrest and accumulation of the Is the arrest and accumulation of the
feces in the rectum or colon feces in the rectum or colon (dehydrated feces).(dehydrated feces).
Overflow diarrhea w/o relief of the Overflow diarrhea w/o relief of the sense of rectal fullnesssense of rectal fullness
Result to Result to stercoral ulcerstercoral ulcer --> bleeding --> bleeding and perforation and perforation
Mx:Mx: - tap water enema / manual - tap water enema / manual extractionextraction
- hot sitz bath- hot sitz bath

Inflammatory Bowel Inflammatory Bowel Diseases:Diseases:1.1. Ulcerative colitisUlcerative colitis (Mucosal (Mucosal
Ulcerative Colitis / Idiopathic Ulcerative Ulcerative Colitis / Idiopathic Ulcerative Colitis):Colitis):
involve the colonic mucosainvolve the colonic mucosa male > femalemale > female limited to the colon and rectumlimited to the colon and rectum
2.2. Crohn’s DiseaseCrohn’s Disease (Chronic (Chronic Interstitial Enteritis/Regional Ilietis):Interstitial Enteritis/Regional Ilietis):
transmural inflammation anywhere in the transmural inflammation anywhere in the GITGIT
extraintestinal symptoms proceeds those extraintestinal symptoms proceeds those of intestinal symptomsof intestinal symptoms
female > malefemale > male

Inflammatory Bowel Inflammatory Bowel Disease: Disease:
Signs and SymptomsSigns and SymptomsCrohn’s DiseaseCrohn’s Disease Ulcerative Ulcerative
ColitisColitis
SymptomsSymptomsdiarrheadiarrhea ++++++ ++++++
rectal bleedingrectal bleeding ++ ++++++
tenesmustenesmus 00 ++++++
abdominal painabdominal pain ++++++ ++
feverfever ++++ ++
vomitingvomiting ++++++ 00
weight lossweight loss ++++++ ++
SignsSigns
perianal diseaseperianal disease ++++++ 00
abdominal massabdominal mass ++++++ 00
malnutritonmalnutriton ++++++ ++

Inflammatory Bowel Inflammatory Bowel Diseases:Diseases:
Ulcerative Ulcerative ColitisColitis
Crohn’s Crohn’s ColitisColitis
Usual LocationUsual Location rectum, left colonrectum, left colon anywhereanywhere
Rectal BleedingRectal Bleeding common, common, continuouscontinuous
uncommon, uncommon, intermittentintermittent
Rectal Rectal involvementinvolvement
almost alwaysalmost always approximate 50%approximate 50%
FistulasFistulas rarerare commoncommon
UlcersUlcers shaggy, irregular, shaggy, irregular, continuous continuous distributiondistribution
linear w/ linear w/ transverse fissures transverse fissures (cobblestone)(cobblestone)
Bowel strictureBowel stricture rare (suspect rare (suspect carcinoma)carcinoma)
commoncommon
CarcinomaCarcinoma increase incidenceincrease incidence increased increased incidenceincidence
Toxic dilatation Toxic dilatation of colonof colon
Occurs in bothOccurs in both

Medical Therapy for Ulcerative Medical Therapy for Ulcerative Colitis & Crohn’s DiseaseColitis & Crohn’s Disease
1.1. SulfasalazineSulfasalazine2.2. MetronidazoleMetronidazole
Crohn’s ileocolitis & colitisCrohn’s ileocolitis & colitis Perineal colitisPerineal colitis Not effective in active ulcerative colitisNot effective in active ulcerative colitis
3.3. Corticosteroid Corticosteroid Oral for mild to moderate active ulcerative Oral for mild to moderate active ulcerative
colitis and Crohn’s diseasecolitis and Crohn’s disease Parenteral for severe or toxic ulcerative Parenteral for severe or toxic ulcerative
colitis or Crohn’s diseasecolitis or Crohn’s disease
4.4. Immunosuppressive agents:Immunosuppressive agents: Steroid sparingSteroid sparing Refractory diseaseRefractory disease

Indications for Surgical Indications for Surgical Interventions for Ulcerative Interventions for Ulcerative
Colitis:Colitis:
1.1. Active disease Active disease unresponsive to medical unresponsive to medical therapytherapy
2.2. Risks of cancerRisks of cancer
3.3. Severe bleedingSevere bleeding

Surgical treatment for Surgical treatment for Ulcerative ColitisUlcerative Colitis
1.1. Proctocolectomy w/ Brooke Proctocolectomy w/ Brooke ileostomy:ileostomy:
curative w/ one operationcurative w/ one operation
2.2. Colectomy w/ ileorectal anastomosis:Colectomy w/ ileorectal anastomosis: not curative; cancer risk persists (5-50%)not curative; cancer risk persists (5-50%) contraindicated for severe rectal dse, rectal contraindicated for severe rectal dse, rectal
dysplasia and rectal CAdysplasia and rectal CA
3.3. Total proctocolectomy w/ ileoanal Total proctocolectomy w/ ileoanal anastomosis w/ pouch:anastomosis w/ pouch:
curative w/ continencecurative w/ continence contraindicated for Crohn’s dse, diarrhea, contraindicated for Crohn’s dse, diarrhea,
rectal CA rectal CA

Surgical treatment for Surgical treatment for Ulcerative ColitisUlcerative Colitis

Indications for Indications for Surgical Treatment of Surgical Treatment of
Crohn’s DseaseCrohn’s Dsease1.1. Ileocolic Crohn’s Disease:Ileocolic Crohn’s Disease: Internal fistula and abscessInternal fistula and abscess 38%38% Intestinal obstructionIntestinal obstruction 37%37% Perianal fistulaPerianal fistula 15%15% Poor response to medical therapyPoor response to medical therapy 6%6%
2.2. Colonic Crohn’s Disease:Colonic Crohn’s Disease: Internal fistula and abscessesInternal fistula and abscesses
25%25% Perianal diseasePerianal disease 23%23% Severe dse w/ poor response Severe dse w/ poor response to medical therapyto medical therapy 21%21% Toxic megacolonToxic megacolon 19%19% Intestinal obstructionIntestinal obstruction 12%12%

COLO – RECTAL POLYPSCOLO – RECTAL POLYPS Projection from the surface of Projection from the surface of
the intestinal mucosa regardless the intestinal mucosa regardless of it’s histologic nature:of it’s histologic nature:
Types:Types:1.1. NeoplasticNeoplastic2.2. HamartomatousHamartomatous3.3. InflammatoryInflammatory4.4. UnclassifiedUnclassified

COLO – RECTAL POLYPSCOLO – RECTAL POLYPSNeoplastic Polyps:Neoplastic Polyps:
Invasive CA are common in polyps smaller Invasive CA are common in polyps smaller than 1 cm in diameter and incidence than 1 cm in diameter and incidence increases w/ increase in sizeincreases w/ increase in size
TypesTypes IncidenceIncidence
(%)(%)Malignant Malignant Potential Potential
(%)(%)
TubularTubular 7575 55
VillousVillous 1010 4040
TubulovillouTubulovillouss
1515 2222

COLO – RECTAL POLYPSCOLO – RECTAL POLYPS
Neoplastic Polyps:Neoplastic Polyps:Diagnosis:Diagnosis:
bleeding per rectum (most common)bleeding per rectum (most common) Villous polyp (large) ---> watery diarrhea Villous polyp (large) ---> watery diarrhea
and in rare cases can have fluid and and in rare cases can have fluid and electrolyte imbalanceelectrolyte imbalance
do complete examination of the colon - do complete examination of the colon - colonoscopycolonoscopy
biopsy / transrectal ultrasonographybiopsy / transrectal ultrasonography

COLO – RECTAL POLYPSCOLO – RECTAL POLYPSNeoplastic Polyps:Neoplastic Polyps:Treatment:Treatment:
Polypectomy for benign Polypectomy for benign ---> follow up---> follow up
(+) CA in situ ----> (+) CA in situ ----> polypectomypolypectomy
(+) invasive CA (invade (+) invasive CA (invade the muscularis mucosa) the muscularis mucosa)
9% metastasize to LN if 9% metastasize to LN if pedunculated pedunculated
20% metastasize to LN if 20% metastasize to LN if it invades the stalk or neckit invades the stalk or neck
15% metastasize to LN if 15% metastasize to LN if sessilesessile
CANCER SURGERYCANCER SURGERY

Neoplastic Polyps:Neoplastic Polyps:Treatment:Treatment:
If entire mucosal surface is covered by If entire mucosal surface is covered by villous tumor ---> segmental resection, villous tumor ---> segmental resection, if in rectum can do full thickness if in rectum can do full thickness proximal protectomy w/ colo-anal proximal protectomy w/ colo-anal anastomosisanastomosis

Hamartomatous Polyp:Hamartomatous Polyp:1.1. Juvenile Polyp:Juvenile Polyp:
not precancerousnot precancerous excisionexcision Swiss cheese appearanceSwiss cheese appearance from dilated from dilated
cystic spacescystic spaces
2.2. Familial Juvenile Polyposis Coli:Familial Juvenile Polyposis Coli: thousands polyps in the colon and rectumthousands polyps in the colon and rectum can degenerate to adenoma ----> can degenerate to adenoma ---->
malignancymalignancy subtotal colectomy or proctocolectomysubtotal colectomy or proctocolectomy

Hamartomatous Polyp:Hamartomatous Polyp:3.3. Peutz-jegher SyndromePeutz-jegher Syndrome
a.a. Melanin spot on buccal mucosa, lips, face and Melanin spot on buccal mucosa, lips, face and digitsdigits
b.b. Polyps of small bowel (always), stomach, colon and Polyps of small bowel (always), stomach, colon and rectum (branching of lamina propria like rectum (branching of lamina propria like Christmas treeChristmas tree).).
Can degenerate into malignancyCan degenerate into malignancy
4.4. Cronkhite – Canada Syndrome:Cronkhite – Canada Syndrome: GIT polyposis, alopecia, cutaneous pigmentation, GIT polyposis, alopecia, cutaneous pigmentation,
atrophy of fingernails and toe nailsatrophy of fingernails and toe nails
5.5. Cowden’s Syndrome:Cowden’s Syndrome: Autosomal dominant, hamartomas of all three Autosomal dominant, hamartomas of all three
embryonal cell layersembryonal cell layers Facial trichilemomas, breast cancer, thyroid dse, Facial trichilemomas, breast cancer, thyroid dse,
GIT polypGIT polyp

Infammatory Polyp:Infammatory Polyp: Caused by previous attacks of severe colitis Caused by previous attacks of severe colitis
resulting in partial loss of mucosa leaving resulting in partial loss of mucosa leaving remnants or islands of normal mucosaremnants or islands of normal mucosa
Occurs after amebic colitis, ischemic colitis Occurs after amebic colitis, ischemic colitis and Schistosomal colitisand Schistosomal colitis
Not premalignantNot premalignant
Hyperplastic Polyp:Hyperplastic Polyp: Usually small < 5mm not premalignantUsually small < 5mm not premalignant > 2cm. have a slight risk of malignant > 2cm. have a slight risk of malignant
degenerationdegeneration Saw tooth appearance of the lining Saw tooth appearance of the lining
epithelial cellsepithelial cells

COLO – RECTAL POLYPSCOLO – RECTAL POLYPSFamilial Adenomatous Polyposis Coli:Familial Adenomatous Polyposis Coli:
Inherited non-sex linked autosomal dominant Inherited non-sex linked autosomal dominant disease w/ hundreds of adenomatous polyps disease w/ hundreds of adenomatous polyps through the entire colon and rectumthrough the entire colon and rectum
1.1. Gardner’s Syndrome:Gardner’s Syndrome: Familial polyposis, osteomatosis, epidermoid Familial polyposis, osteomatosis, epidermoid
cyst, fibromas of the skin (desmoid tumor) – the cyst, fibromas of the skin (desmoid tumor) – the most important extra-colonic expression.most important extra-colonic expression.
Tx: Tx: - total proctocolectomy w/ ileostomy- total proctocolectomy w/ ileostomy
- colectomy w/ ileorectal anastomosis- colectomy w/ ileorectal anastomosis
- examine other members of the - examine other members of the familyfamily

COLO – RECTAL POLYPSCOLO – RECTAL POLYPSFamilial Adenomatous Familial Adenomatous
Polyposis Coli:Polyposis Coli:2.2. Turcot’s Syndrome:Turcot’s Syndrome:
Familial polyposis, brains tumors Familial polyposis, brains tumors (gliomas or medulloblastomas)(gliomas or medulloblastomas)
Tx:Tx: same w/ colorectal same w/ colorectal involvementinvolvement

Carcinoma of ColonCarcinoma of Colon Most common CA of the GITMost common CA of the GIT Older age grp; peak incidence 80y/oOlder age grp; peak incidence 80y/o male ( > rectum) ; female ( > colon)male ( > rectum) ; female ( > colon) Etiology:Etiology:
1.1. UnknownUnknown
2.2. HereditaryHereditary
3.3. Diet --> low fiber diet and high animal fatDiet --> low fiber diet and high animal fat Distribution --> shifting to the right Distribution --> shifting to the right
side side

Carcinoma of ColonCarcinoma of ColonMacroscopic form:Macroscopic form:1.1. Ulcerating typeUlcerating type most commonmost common2.2. Polypoid or fungatingPolypoid or fungating3.3. Colloid CA Colloid CA
bulky growth w/ gelatinous appearancebulky growth w/ gelatinous appearance 10-15%10-15%
4.4. Signet ring cell CASignet ring cell CA intracellular mucinous intracellular mucinous
5.5. Infiltrating CAInfiltrating CA submucosal spreadsubmucosal spread

Carcinoma of ColonCarcinoma of Colon
Microscopic form:Microscopic form:adenocarcinomaadenocarcinoma
GronnellGronnell: based on invasive tendency, : based on invasive tendency, glandular arrangement, nuclear polarity glandular arrangement, nuclear polarity and frequency of mitosis.and frequency of mitosis.Grade IGrade I - low grade / well - low grade / well
differentiateddifferentiated
Grade IIGrade II - average grade / mod. - average grade / mod. differentiateddifferentiated
Grade IIIGrade III - high grade / poorly differentiated- high grade / poorly differentiated

Carcinoma of ColonCarcinoma of ColonMechanism of Spread:Mechanism of Spread:
1.1. Direct spreadDirect spread
2.2. Transperitoneal spreadTransperitoneal spread
3.3. ImplantationImplantation
4.4. LymphaticLymphatic
5.5. HematogenousHematogenous Liver & LungsLiver & Lungs – most common – most common
distant spreaddistant spread

Carcinoma of ColonCarcinoma of ColonDuke’s Stage:Duke’s Stage:
Depth of bowel wall involvementDepth of bowel wall involvement Presence or absence of LN metastasisPresence or absence of LN metastasis
Stage A:Stage A: Invasion at least through the muscularis Invasion at least through the muscularis
mucosa but not through the muscularis mucosa but not through the muscularis propriapropria
98% ---> 5yr survival98% ---> 5yr survival
Stage B:Stage B: Invasion through full thickness of bowel wall; Invasion through full thickness of bowel wall;
(-) LN(-) LN 78% ----> 5yr survival78% ----> 5yr survival

Carcinoma of ColonCarcinoma of ColonDuke’s Stage:Duke’s Stage:Stage C:Stage C:
LN metastasis, regardless of depthLN metastasis, regardless of depth
Stage C1Stage C1:: - only adjacent LN metastasis- only adjacent LN metastasis
Stage C2Stage C2: - LN involves are nodes at : - LN involves are nodes at point of ligature of blood vesselspoint of ligature of blood vessels
32% 5 yr survival32% 5 yr survival
Stage D:Stage D: Distant metastasis or w/ adjacent organ Distant metastasis or w/ adjacent organ
involvementinvolvement 0% 5 yr survival0% 5 yr survival

TNM Staging of Colonic TNM Staging of Colonic CACA
Primary Tumor (T):Primary Tumor (T):TXTX - Primary tumor cannot be assessed- Primary tumor cannot be assessedT0 T0 - No evidence of primary tumor- No evidence of primary tumorT1T1 - Tumor invades submucosa- Tumor invades submucosaT2T2 - Tumor invades muscularis proper- Tumor invades muscularis properT3T3 - Tumor invades through the muscularis - Tumor invades through the muscularis properproper
into the subserosa or into into the subserosa or into nonperitonealized nonperitonealized
pericolic or perirectal tissuepericolic or perirectal tissueT4T4 - Tumor perforates the visceral peritoneum - Tumor perforates the visceral peritoneum or or
directly invades the organs or structuresdirectly invades the organs or structures

TNM Staging of Colonic TNM Staging of Colonic CACARegional Lymph Node (N):Regional Lymph Node (N):
NXNX – Regional LN cannot be assessed – Regional LN cannot be assessedN0N0 - No regional LN metastasis - No regional LN metastasisN1 N1 - Metastasis in 1 to 3 pericolic or perirectal - Metastasis in 1 to 3 pericolic or perirectal LNLNN2N2 - metastasis in 4 or more pericolic or - metastasis in 4 or more pericolic or
perirectal LNperirectal LNN3N3 - Metastasis in any LN along the course of a - Metastasis in any LN along the course of a
named vascular trunknamed vascular trunk
Distant Metastasis (M):Distant Metastasis (M):MXMX – Presence of distant metastasis cannot be – Presence of distant metastasis cannot be assessedassessedM0 M0 - No distant metastasis- No distant metastasisM1 M1 - w/ distant metastasis - w/ distant metastasis

TNM Staging of Colonic TNM Staging of Colonic CACA
StageStage I:I: T1 –T2T1 –T2 N0N0 M0M090% 5y/r Survival90% 5y/r Survival
Stage II:Stage II: T3 – T4T3 – T4 N0N0 M0M060 – 80% 5 y/r survival60 – 80% 5 y/r survival
Stage III:Stage III: Any TAny T N1N1 M0M0Any TAny T N2, N3N2, N3 M0M020 – 50% 5y/r survival20 – 50% 5y/r survival
Stage IV;Stage IV; Any TAny T Any NAny N M1M1< 5% 5 yr survival< 5% 5 yr survival

Risk Factors for Risk Factors for Colorectal CAColorectal CA
1.1. Aging is the dominant risk factorAging is the dominant risk factor w/ w/ rising incidence after rising incidence after 50 y/o.50 y/o.
2.2. Hereditary risk factor:Hereditary risk factor: 80% colorectal are sporadic80% colorectal are sporadic 20% w/ known family hx.20% w/ known family hx.
3.3. Dietary factors:Dietary factors: high animal fathigh animal fat (saturated or polyunsaturated (saturated or polyunsaturated
fats), but oleic acid (coconut & fish oil does not).fats), but oleic acid (coconut & fish oil does not). Vegetable fiber, Ca, selenium, Vits. A, C, & E Vegetable fiber, Ca, selenium, Vits. A, C, & E
are protectiveare protective Alcohol Alcohol increase colonic CAincrease colonic CA
4.4. Obesity and sedentary lifestyle Obesity and sedentary lifestyle contributorycontributory
5.5. SmokingSmoking increased the incidence increased the incidence

Premalignant Diseases of Premalignant Diseases of Colon & RectumColon & Rectum
1.1. AdenomaAdenoma
2.2. Familial adenomatous polyposis Familial adenomatous polyposis syndromesyndrome
3.3. Gardner’s syndromeGardner’s syndrome
4.4. HamartomaHamartomas (familial juvenile polyposis s (familial juvenile polyposis coli & Peutz-Jegher polypcoli & Peutz-Jegher polyp
5.5. Inflammatory bowel diseaseInflammatory bowel diseasea.a. Ulcerative colitisUlcerative colitis
b.b. Crohn’s diseaseCrohn’s disease
6.6. SchistosomiasisSchistosomiasis (Billharziasis) – S. (Billharziasis) – S. mansoni & mansoni &
S. japonicumS. japonicum
7.7. Utero-sigmoidostomy Utero-sigmoidostomy

Carcinoma of ColonCarcinoma of ColonClinical Manifestation:Clinical Manifestation:
Change in bowel habitChange in bowel habit classic classic symptomssymptoms
Rectal bleedingRectal bleeding Weight lossWeight loss Abdominal pain, bloating and other signs of Abdominal pain, bloating and other signs of
obstructionobstruction Anemia and anorexiaAnemia and anorexia Tenesmus, feeling of incomplete evacuation, Tenesmus, feeling of incomplete evacuation,
and rectal bleeding if lesion is in the rectumand rectal bleeding if lesion is in the rectum

Screening Modalities For Screening Modalities For Colonic TumorsColonic Tumors
1.1. Fecal occult blood testing:Fecal occult blood testing: Annual FOBT screening for asymptomatic 50 Annual FOBT screening for asymptomatic 50
y/oy/o
2.2. Rigid proctoscopy / flexible Rigid proctoscopy / flexible sigmoidoscopysigmoidoscopy
3.3. Colonoscopy:Colonoscopy: The most accurate and most complete method The most accurate and most complete method
for examining the colonfor examining the colon
4.4. Air contrast Barium enema:Air contrast Barium enema:5.5. CT colonography (virtual CT colonography (virtual
colonoscopy):colonoscopy): Colon is insufflated with air and a spiral CT is Colon is insufflated with air and a spiral CT is
performed.performed. Useful for imaging the proximal colon in case of Useful for imaging the proximal colon in case of
obstructionobstruction

Therapy for Colonic Therapy for Colonic CarcinomaCarcinoma
Principle:Principle: Objective is to remove the primary tumor Objective is to remove the primary tumor
w/ its lymphovascular supplyw/ its lymphovascular supply Adjacent organs or tissue invaded shd be Adjacent organs or tissue invaded shd be
resected en block w/ the tumorresected en block w/ the tumor Tumors cannot be removed, a palliative Tumors cannot be removed, a palliative
procedure shd be done.procedure shd be done. Synchronous CASynchronous CA ---> subtotal or total ---> subtotal or total
colectomycolectomy Metachronous tumorMetachronous tumor (second primary (second primary
colon CA) treated similarlycolon CA) treated similarly Hemorrhage in an unresectable tumor Hemorrhage in an unresectable tumor
can be controlled w/ angiographic can be controlled w/ angiographic embolizationembolization

Therapy for Colonic Therapy for Colonic CarcinomaCarcinoma
Stage 0:Stage 0: No risk of LN metastasisNo risk of LN metastasis Pedunculated / sessile polyp -> Pedunculated / sessile polyp -> endoscopic endoscopic
polypectomypolypectomy If polyp cannot be removed completely segmental If polyp cannot be removed completely segmental
resection shd be doneresection shd be done
Stage I: (T1,N0,M0):Stage I: (T1,N0,M0): PolypectomyPolypectomy --> for uninvolved stalk (pedunculated) --> for uninvolved stalk (pedunculated) Segmental resection:Segmental resection:
1.1. Sessile polypSessile polyp
2.2. Pedunculated polyp ( Pedunculated polyp ( lymphovascular invasion, lymphovascular invasion, poorly differentiated or tumor w/in 1mm. of poorly differentiated or tumor w/in 1mm. of resection marginresection margin ---> high risk of local recurence ---> high risk of local recurence and metastatic spread)and metastatic spread)

Therapy for Colonic Therapy for Colonic CarcinomaCarcinoma
Stage II (T3-4,N0,M0):Stage II (T3-4,N0,M0): Surgical resection Surgical resection Adjuvant chemotherapy is suggested for:Adjuvant chemotherapy is suggested for:
1.1. Young patientYoung patient2.2. Moderate to poorly differentiatedModerate to poorly differentiated
Stage III (Tany,N1,M0):Stage III (Tany,N1,M0): Surgical resection + adjuvant Surgical resection + adjuvant
chemotherapy chemotherapy (5-Fluorouracil, (5-Fluorouracil, levamisole or leucovorin, capecitabine, levamisole or leucovorin, capecitabine, irinotecan, oxaliplatin, angiogenesis irinotecan, oxaliplatin, angiogenesis inhibitor and immunotherapy)inhibitor and immunotherapy)

Therapy for Colonic Therapy for Colonic CarcinomaCarcinoma
Stage IV: (Tany, Nany, M1)Stage IV: (Tany, Nany, M1) Palliative resection of primary and Palliative resection of primary and
isolated liver metastasis isolated liver metastasis Adjuvant chemotherapyAdjuvant chemotherapy Irresectable ---> diverting colostomyIrresectable ---> diverting colostomy

THANK THANK YOUYOU

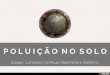
Anorectal AbscessAnorectal Abscess5 potential 5 potential
spaces:spaces:1.1. Perianal spacePerianal space2.2. Ischiorectal Ischiorectal
spacespace3.3. Intersphincteric Intersphincteric
spacespace4.4. Deep posterior Deep posterior
anal spaceanal space5.5. Supralevator Supralevator
spacespace

Anorectal AbscessAnorectal AbscessEtiology:Etiology:
Infection of anal glandInfection of anal gland Organism (fecal & cutaneous flora)Organism (fecal & cutaneous flora)
1.1. E. coliE. coli 4. Clostridium sp.4. Clostridium sp.2.2. Bacteroides fragilisBacteroides fragilis 5. 5.
StaphylococcusStaphylococcus3.3. StreptococcusStreptococcus
Manifestation:Manifestation: Pain in the anal regionPain in the anal region
Treatment:Treatment: Drainage / antibioticDrainage / antibiotic HygieneHygiene Hot sitz bathHot sitz bath

Anorectal AbscessAnorectal AbscessTypes :Types :
1.1. Perianal abscessPerianal abscess
2.2. Ischiorectal abscessIschiorectal abscess – diffuse – diffuse
swelling of ischiorectal fossaswelling of ischiorectal fossa

Anorectal AbscessAnorectal Abscess3.3. Intersphincteric abscess:Intersphincteric abscess:
No apparent sign of swelling or induration in No apparent sign of swelling or induration in the perianal areathe perianal area
CLUE: --> deep seated tenderness when CLUE: --> deep seated tenderness when circum-anal pressure is applied above the circum-anal pressure is applied above the dentate line.dentate line.
Drainage: thru the anal canal lining or thru Drainage: thru the anal canal lining or thru internal sphincteric muscleinternal sphincteric muscle
4.4. Supralevator abscess:Supralevator abscess: UncommonUncommon Mimmic acute intra-abdominal conditionMimmic acute intra-abdominal condition Etiology: extension ofEtiology: extension of
a.a. Intersphincteric abscessIntersphincteric abscessb.b. Ischiorectal abscessIschiorectal abscessc.c. Intra-abdominal abscess Intra-abdominal abscess

Necrotizing Peri-anal & Perineal Necrotizing Peri-anal & Perineal Infection:Infection:
Etiology:Etiology:1.1. Neglected or delayed treatment of primary Neglected or delayed treatment of primary
anorectal infectionanorectal infection
2.2. Extension of UTI particularly the periurethral glandExtension of UTI particularly the periurethral gland
Manifestation:Manifestation: Pain, tenderness and swelling with crepitation of Pain, tenderness and swelling with crepitation of
perianal and scrotum or labiaperianal and scrotum or labia Black spot on the site (necrosis)Black spot on the site (necrosis)
Treatment:Treatment: Broad spectrum antibioticBroad spectrum antibiotic Debridement Debridement Hyperalimentation / diverting colostomy &/or Hyperalimentation / diverting colostomy &/or
cystostomycystostomy

Fistula-In-Fistula-In-Ano:Ano:
Inflammatory tract w/ Inflammatory tract w/ secondary opening secondary opening (external) and a primary (external) and a primary opening (internal) in the opening (internal) in the anal canal.anal canal.
Etiology:Etiology: Complication of perianal Complication of perianal
abscessabscess
Goodsalls Rule: Goodsalls Rule: to locate internal openingto locate internal opening
Classification of Fistula-Classification of Fistula-in-ano:in-ano:
1.1. Inter-sphinctericInter-sphincteric
2.2. Trans-sphinctericTrans-sphincteric
3.3. Supra-sphinctericSupra-sphincteric
4.4. Extra-sphinctericExtra-sphincteric

Fistula-in-anoFistula-in-anoManifestation:Manifestation:
Previous history of Previous history of perianal abscessperianal abscess
Rule out ulcerative Rule out ulcerative colitis and Crohn’s colitis and Crohn’s dse (colonoscopy / dse (colonoscopy / barium enema)barium enema)
Treatment:Treatment:1.1. Identify the primary Identify the primary
opening opening (probing/methylene (probing/methylene blue/fistulography)blue/fistulography)
2.2. Fistulotomy / Fistulotomy / fistulectomy fistulectomy (healing by (healing by secondary intensionsecondary intension

Fistula-in-anoFistula-in-ano If fistula is high in relation to anorectal If fistula is high in relation to anorectal
ring do 2 stage procedure:ring do 2 stage procedure:1.1. Insert a seton wire or suture to the tract Insert a seton wire or suture to the tract
for several wks to create fibrosisfor several wks to create fibrosis2.2. Open the fibrous track on the second stage Open the fibrous track on the second stage
after 6-8 wksafter 6-8 wks

HemorrhoidHemorrhoid Are cushions of submucosal tissue in Are cushions of submucosal tissue in
the anal canal composed of the anal canal composed of connective tissue containing venules, connective tissue containing venules, arterioles and smooth muscle fibers.arterioles and smooth muscle fibers.
Purposed – aids in anal continence Purposed – aids in anal continence and cushion the anal canal and and cushion the anal canal and support the lining during defecationsupport the lining during defecation
1.1. External skin tagExternal skin tag Redundant fibrotic skin at the anal Redundant fibrotic skin at the anal
verge due to previous thrombosed verge due to previous thrombosed external hemorrhoid of past operationexternal hemorrhoid of past operation

HemorrhoidHemorrhoid 2.2. External hemorrhoidExternal hemorrhoid
Dilated venules of the inferior Dilated venules of the inferior hemorrhoidal plexus located distal to hemorrhoidal plexus located distal to the pectinate or dentate linethe pectinate or dentate line

HemorrhoidHemorrhoid3.3. Internal hemorrhoid:Internal hemorrhoid:
Manifestation:Manifestation: Painless bright red rectal bleeding associated w/ Painless bright red rectal bleeding associated w/
bowel movementbowel movement Feeling of incomplete evacuation of fecesFeeling of incomplete evacuation of feces Pain is experienced if w/ complication of anal Pain is experienced if w/ complication of anal
fissure, stenosis of thrombosisfissure, stenosis of thrombosis
Grade According to Degree of Prolapse:Grade According to Degree of Prolapse:11stst degree degree: anal cushion slide down beyond : anal cushion slide down beyond the the
dentate line on strainingdentate line on strainingMx: Mx: - painless rectal bleeding- painless rectal bleedingTx: Tx: - bulk forming agents - bulk forming agents
(psyllium seed)(psyllium seed)- rubber band ligation- rubber band ligation

HemorrhoidHemorrhoidRubber band ligation:Rubber band ligation:

HemorrhoidHemorrhoid22ndnd degree: degree:
Prolapse through the anus on straining but Prolapse through the anus on straining but spontaneously reducedspontaneously reduced
33rdrd degree: degree: Requires manual reduction into the anal canalRequires manual reduction into the anal canal Tx: rubber band ligation / hemorrhoidectomyTx: rubber band ligation / hemorrhoidectomy
44thth degree: degree: Prolapse cannot be reducedProlapse cannot be reduced hemorrhoidectomyhemorrhoidectomy

Anal FissureAnal Fissure Tear from the dentate line up to the Tear from the dentate line up to the
anal verge lined by skinanal verge lined by skin Seen in young and middle age groupSeen in young and middle age group Majority occurs at the at the Majority occurs at the at the
posterior midline due to poor posterior midline due to poor muscular supportmuscular support

Anal FissureAnal FissureEtiology:Etiology:1.1. Passage of large hard stoolPassage of large hard stool2.2. Conditions ( Crohn’s dse, ulcerative colitis, Conditions ( Crohn’s dse, ulcerative colitis,
syphilis’ tuberculosis and leukemia)syphilis’ tuberculosis and leukemia)Manifestation:Manifestation:
Burning pain during and after bowel movementBurning pain during and after bowel movement Bright red blood on toilet paperBright red blood on toilet paper
Diagnosis: Diagnosis: Rectal examination / proctosigmoidoscopyRectal examination / proctosigmoidoscopy
Treatment:Treatment: Conservative:Conservative: - anal hygiene / bulk forming - anal hygiene / bulk forming
agentsagents- hot sitz bath- hot sitz bath- local anesthetic jelly- local anesthetic jelly
Surgical: - chronic stage (lateral internal Surgical: - chronic stage (lateral internal sphincterotomy)sphincterotomy)

Anal FissureAnal FissureTreatment:Treatment:
Conservative:Conservative: anal hygiene / bulk anal hygiene / bulk
forming agentsforming agents hot sitz bathhot sitz bath local anesthetic local anesthetic
jellyjelly
Surgical: Surgical: chronic stage chronic stage
(lateral internal (lateral internal sphincterotomy)sphincterotomy)

THANK THANK YOUYOU