Embed Size (px)
Citation preview

Biomedicine & Pharmacotherapy 67 (2013) 445–449
Original article
c-FLIP does not correlate with response to immunochemotherapy treatment andoutcome of patients with nodal diffuse large B-cell lymphoma
Olivera Markovic a,e,*, Dragomir Marisavljevic a,e, Vesna Cemerikic-Martinovic b, Branka Filipovic a,e,Slavica Radovanovic a, Marija Zdravkovic a,e, Dejana Stanisavljevic d,e, Biljana Mihaljevic c,e
a Clinical Hospital Center ‘‘Bezanijska kosa’’, Belgrade, Serbiab Beolab, Belgrade, Serbiac Institute of Hematology, Clinical Center of Serbia, Belgrade, Serbiad Institute of Statistic, Clinical Center of Serbia, Belgrade, Serbiae Faculty of Medicine, University of Belgrade, Belgrade, Serbia
A R T I C L E I N F O
Article history:
Received 20 January 2013
Accepted 4 February 2013
Keywords:
Diffuse large B-cell lymphoma
c-FLIP
Apoptosis
Immunohistochemistry
Prognosis
A B S T R A C T
Cellular FLICE-inhibitory protein (c-FLIP) is a critical anti-apoptotic regulator that inhibits apoptosis-
inducing ligand, (TRAIL)-induced apoptosis as well as chemotherapy-triggered apoptosis in malignant
cells. The present study was designed to investigate the clinical and prognostic significance of c-FLIP
expression in patients with nodal diffuse large B-cell lymphoma (DLBCL) treated with immunochem-
otherapy.
Methods: We have analyzed lymph node biopsy specimens, obtained from 60 patients with newly
diagnosed nodal DLBCL treated with immunochemotherapy (R-CHOP or R-EPOCH). The expression of
c-FLIP was analyzed using the standard imunohistochemical method on formalin-fixed and routinely
processed paraffin-embedded lymph node specimens and evaluated semi quantitavely as a percentage
of tumor cells.
Results: c-FLIP immunoexpression (> 50% positive tumor cells) has been found in 28 (46.7%) patients, and
observed as cytoplasmic staining. There was not significant difference in c-FLIP immunoexpression
between GCB and non-GCB subtype of DLBCL (P = 0.639). Besides, c-FLIP immunoexpression had no
significant association with IPI, ‘‘bulky’’ disease, extranodal localization, haemoglobin, Ki-67
immunoexpression or other clinico-pathological parameters. c-FLIP positivity has no significant
influence on therapy response and survival in patients with DLBCL (P = 0.562 and P = 0.093, respectively).
Patients with c-FLIP overexpression did not relapse more often that patients without expression of this
apoptotic protein (P = 0.365).
Conclusion: Our results suggest that c-FLIP immunoexpression can not be used as a prognostic factor in
patients with nodal DLBCL treated with immunochemotherapy.
� 2013 Elsevier Masson SAS. All rights reserved.
Available online at
www.sciencedirect.com
1. Introduction
Cellular FLICE-inhibitory protein (c-FLIP) is a key inhibitor ofextrinsic apoptotic pathway. c-FLIP regulates one of the mostproximal steps of death receptor signaling – autoproteolyticprocessing of caspase [1]. c-FLIP structurally resemble caspases,but lack the proteolytic activity. There are three isoforms of cellularc-FLIP: long (c-FLIPL), short (c-FLIPS) and c-FLIPR splice variants [1].All of them can be incorporated into the death-inducing signaling
* Corresponding author. KBC ‘‘Bezanijska kosa’’, Bezanijska kosa bb, 11000
Belgrade, Serbia. Tel.: +381 113 559 896; fax: +381 112 699 937.
E-mail address: [email protected] (O. Markovic).
0753-3322/$ – see front matter � 2013 Elsevier Masson SAS. All rights reserved.
http://dx.doi.org/10.1016/j.biopha.2013.02.002
complex (DISC) and modulate the activation of procaspase-8 andthereby, prevent induction of apoptosis mediated by deathreceptors [2–4]. As an important modulator of caspase-8, c-FLIPregulates life and death in various types of normal cells and tissues,such as lymphoid cells, and renders resistance to death receptor-mediated apoptosis in many types of cancer cells. In addition to anapoptosis modulator, c-FLIP has been shown to exert otherphysiological functions related to cell cycle and proliferation [5].
Diffuse large B-cell lymphoma (DLBCL) is an aggressive diseasewith variable clinical, histological, immunophenotypic cytogeneticfeatures and variable prognosis [6]. Therefore, precise prognostictools that can help in predicting therapy response and designingindividualized therapy are necessary. Using immunohistochemis-try, DLBCL can be divided into prognostically significant GCB and

1 - Spec ificit y
1.00.80.60.40.20.0
Se
ns
itiv
ity
1.0
0.8
0.6
0.4
0.2
0.0
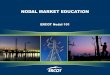
ROC Curve
Diagonal segments are produced by ties.
Fig. 1. Receiver operating curve for determining the optimal cut-off value for the
percentage of c-FLIP positive lymphoma cells.
O. Markovic et al. / Biomedicine & Pharmacotherapy 67 (2013) 445–449446
non-GCB subgroups [7]. It was determined that patients with non-GCB subtype have a worse prognosis [7,8], but the mechanismsresponsible for the poorer prognosis in this group of patients havenot yet been precisely determined.
Previous studies have shown that the expression of theinhibitory apoptotic proteins may be the important cause forchemotherapy resistance and a poor prognosis in DLBCL [9–11]. Inthis study, we analyzed prognostic significance of c-FLIP immu-noexpression in patients treated with immunochemotherapy andits expression in relation to GCB/non-GCB subtype.
2. Patients and methods
2.1. Patients
We analyzed 60 patients with de novo nodal DLBCLdiagnosed from January 2004 to September 2009. The diagnosiswas established according to the criteria of the World HealthOrganization classification [12]. A number of clinical variableswere particularly analyzed: age, gender, clinical stage, perfor-mance status (ECOG), International Prognostic Index (IPI), serumalbumin, C-reactive protein, ß2-microglobulin, LDH, hemoglobinconcentration and platelet count. The staging of the diseasewas done according to Ann Arbor classification [13]. IPIscore was determined, as described previously [14]. The patientswere subdivided into GBC and non-GBC type according to themodel proposed by Hans et al. [7]. The patients with humanimmunodeficiency virus positivity and the patients withprimary extranodal disease (CS IE or IIE) were excluded fromthe study.
This study complies with all provisions of the Declaration ofHelsinki and its current amendments and was conducted inaccordance with Good Clinical Practice Guidelines. The study wasapproved by the Institutional Ethical Committee.
2.2. Treatment
All patients were treated with immunochemotherapy: 55patients received R-CHOP regimen, consisted of cyclophosphamide750 mg/m2, doxorubicin 50 mg/m2, vincristine 1.4 mg/m2 (up to amaximal dose of 2 mg), on day 2 and prednisone 60 mg/m2, orally,on days 2–6. Rituximab was administrated at the dose of 375 mg/m2, on day 1. The treatment was repeated every 3 weeks. Fivepatients received R-EPOCH regimen consisted of rituximab on day1, etopside 50 mg/m2 on days 2–5, doxorubicin 10 mg/m2 on days2–5, vincristine 0.4 mg/m2 on days 2–5 as continuous i.e. infusion,prednisone 60 mg/m2 orally on days 2–7, cyclophosphamide750 mg/m2 on day 7. The patients in clinical stages II–IV weretreated with six to eight cycles of immunochemotherapy. Thepatients in the first clinical stage were treated with three cycles ofimmunochemotherapy and ‘‘involved’’ field radiotherapy. Theirradiation therapy (30–40 Gy) was applied after immunochem-otherapy in the patients with ‘‘bulky’’ disease or with residualdisease. Treatment response was evaluated according to theInternational Workshop criteria [15].
2.3. Immunohistochemical studies
A tumor tissue was obtained from every patient by lymphnode biopsy, fixed in buffered formalin, pH 7.4 and embedded inparaffin. Paraffin-embedded tissue samples were cut 3 mm thick,deparaffinized in xylene and rehydrated in water. The lymphnode specimens were analyzed by conventional light microsco-py examination and immunohistochemical analysis. The immu-noexpression of c-FLIP was analyzed by the avidin/biotin/peroxidase complex method (LSAB 2, DAKO or Ultravision LP
Detection system, Labvision) using aminoethylcarbazole or DABas a chromogen. A heat-induced epitope retrieval method wasused before the immunostaining. Namely, sections were placedin 0.01 mmol/L citrate buffer at pH 6.0 and heated twice in amicrowave over for 10 min per cycle. The sections were stainedwith c-FLIP antibody (RB-1552-P1, Labvision, dilution 1:100).The antibody was incubated for half an hour at roomtemperature. After the development of the chromogen, all theslides were counterstained with hematoxylin. The controlsections were immunostained under identical conditions,substituting the primary antibody with the buffer solution.The tissue of lymph reactive nodes served as a positive control.Endothelial cells served as an internal control. The expression ofc-FLIP was evaluated semi quantitatively as a percentage ofpositive cells of all tumor cells. Only cells three times larger thansmall lymphocytes were analyzed. At least 10 fields wereconsidered for each case. Lymph node samples were evaluatedat 100� and 400� magnifications and independently analyzedby two observers (O.M., V.C.). In case of disagreement, theobservers reanalyzed the staining results until they reached aconsensus.
2.4. Statistical analysis
The statistical analysis was performed using SPSS version 15software (SPSS Inc, Chicago Illinois, USA). The optimal cut-offvalue for the percentage of c-FLIP positive lymphoma cells wasdetermined using receiver operating curve (ROC) method withdetermination of sensitivity and specificity of all cut-off values.According to ROC analysis, the optimal cut-off value is 50%(Fig. 1), and this value is used in the study. The median of c-FLIPpositive cells (40%) was also used as cut-off value, but identicalresults were obtained. Chi-Square test was used to evaluate thedifferences in therapy response and survival in relation toclinical and apoptotic parameters. Overall survival (OS) wascalculated as the time from the diagnosis to the date of death orlast follow-up. Overall survival was analyzed using the Kaplan–Meier method and log-rank test was used to compare thedifference of the survival data. All statistical tests were two-sided, with P value � 0.05.

Table 1Clinical data and histological features of 60 DLBCL patients.
Age (years)
Median (IQR) 53.5 (18)
Range (19–87)
> 60 14 (23.33%)
Gender
Male/Female 35 (58.33%)/25 (41.66%)
Stage
I 1 (1.6%)
II 19 (31.1%)
III 21 (34.4%)
IV 19 (31.1%)
ECOG
0 27 (45.0%)
1 24 (40.0%)
2 6 (10.0)
3 3 (5.0%
B symptoms 33 (55.0%)
IPI
Low 23 (38.3%)
Low/intermediate 18 (30.0%)
High/intermediate 12 (20.0%)
High 7 (11.7%)
‘‘Bulky’’ disease
(> 7 cm) 32 (53.3%)
(> 10 cm) 14 (23.3 %)
Extranodal localisation 1 9 (31.7 %)
LDH
(> 460 U/L) 38 (63.3 %)
Median (IQR) 550 (340)
Range 212–2598
ß-2-microglobulin (mg/L)
Median (IQR) 4.8 (3.9)
Range 1.18–13.9
CRP (mg/L)
Median (IQR) 18 (40.1)
Range 1.4–285
Lymphocyte count (� 109/L) 1.9 (1.3)
Range 0.3–11
Therapy
R-CHOP/R-EPOCH 55 (91.66 %)/5 (9.33 %)
GBC/non-GBC subtype 21 (48.8%)/22 (51.2%)
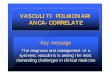
Fig. 2. Immunoexpression of c-FLIP in biopsy specimens of primary nodal diffuse large B
O. Markovic et al. / Biomedicine & Pharmacotherapy 67 (2013) 445–449 447
3. Results
3.1. Patient’s characteristics
Clinical data related to the patients are summarized in Table 1.
3.2. Immunohistochemical analysis
The percentage of positive tumor cells ranged from 3 to 96%(mean percent of positive cells was 45.33% [IQR 50]). As it wasfound that the optimal cut-off value for the percentage of c-FLIPpositive cells by ROC method was 50%, we used this value as cut-offof positivity. c-FLIP immunoexpression was found in 28patients(46.7%) and observed as diffuse cytoplasmic staining(Fig. 2). The expression of c-FLIP-a was registrated also onendothelial cells, which was used as a positive internal control.
3.3. Correlation between c-FLIP immunoexpression and subtype and
clinical parameters
We did not notice significant difference in c-FLIP immunoexpres-sion between GCB and non-GCB subtype of DLBCL (P = 0.639) (Table2). Similarly, c-FLIP immunoexpression was not in significantcorrelation with the analyzed clinical parameters: B symptoms(P = 0.446), hemoglobin (P = 0.357), LDH (P = 0,496), IPI (P = 0.078),‘‘bulky’’ disease (P = 0.41), extranodal localisation (P = 0.941),lymphocyte count (P = 0.121) and Ki-67 immunoexpression(P = 0.356).
3.4. Response to therapy
The therapy response was achieved in 49 patients (81.66%). Wedid not notice significant difference in chance to achieve therapyresponse regarding surviving immunoexpression (P = 0.562)(Table 3).
The relapse of disease was noticed in 12 patients (20%) aftermedian time of follow-up of 40 months. There was no difference inthe relapse rate in accordance to immunoexpression of c-FLIP.Namely, the relapse of the disease appeared in 7 (25%) c-FLIP positivepatientsand in5(15.6%)c-FLIPnegativepatients(P = 0.365)(Table3).
3.5. Overall survival
The median follow-up period for OS of patients was 46 months(range 9–86 months). At the time of the final analysis, 39 patients
-cell lymphoma; diffuse cytoplasmic staining (original magnification �200, �400).

Table 2Expression of c-FLIP regarding GCB and the non-GCB subtype and other clinical
parameters.
Parameters c-FLIP < 50% c-FLIP > 50% P
Subtype
GCB 9 (45.0%) 12 (52.2%)
Non-GCB 11 (55.0%) 11 (47.8%) 0.639
B symptoms
No 16 (50%) 11 (39.3%) 0.405
Yes 16 (50%) 17 (60.7%)
Lymphocytes count
< 1.5 � 109/L 19 (59.4%) 11 (39.3%) 0.121
� 1.5 � 109/L 13 (40.6%) 17 (60.7%)
LDH
� 460 U/L 13 (40.6%) 9 (32.1%) 0.469
< 460 U/L 19 (59.4%) 19 (67.9%)
Clinical stage
I/II 12 (38.7 %) 7 (25.0 %) 0.260
III/IV 19 (61.3%) 21 (75.0%)
Extranodal localization
No 22 (68.7%) 19 (67.9%) 0.941
Yes 10 (31.3%) 9 (32.1%)
‘‘Bulky’’ disease
No 14 (43.7%) 15 (53.57%) 0.891
Yes 18 (56.3%) 13 (46.42%)
IPI
Low 13 (40.6%) 10 (35.7%)
Intermediate 8 (25.6%) 10 (35.7%)
High/intermediate 9 (28.1%) 3 (10.7%) 0.199
High 2 (6.3%) 5 (17.9%)
Ki-67
� 50% 6 (18.8%) 6 (21.4%) 0.796
> 50% 26 (81.3%) 22 (78.6%)
Overall survi val (months)
120100806040200
Cum Survival
1.0
0.8
0.6
0.4
0.2
0.0
c-Flip <50%c-Flip >50%
Fig. 3. Kaplan–Meier curve of survival according to c-FLIP immunoexpression
(P = 0.098).
O. Markovic et al. / Biomedicine & Pharmacotherapy 67 (2013) 445–449448
(65%) were alive and 21 patients (35%) died. The median survival ofthe whole group of the analyzed patients was 39 months. Theimmunoexpression of c-FLIP was not significantly associated withthe overall survival (P = 0.098) (Table 3). Namely, the meansurvival of c-FLIP positive patients was 46.2, while the meansurvival of c-FLIP negative patients was 87.3 months (Fig. 3).
4. Discussion
Previous studies have shown that deregulation of inhibitoryapoptotic proteins is an important factor in the pathogenesis oflymphoma and that such deregulation may be the important causefor chemotherapy resistance and poor prognosis in DLBCL [9–11].However, there are a few data about prognostic significance ofc-FLIP in DLBCL. The present study was conducted in order toclarify the importance of c-FLIP immunoexpression in patientswith nodal DLBCL treated with immunochemotherapy.c-FLIP is amajor resistance factor and critical anti-apoptotic regulator thatinhibits Fas-L and TNF-related apoptosis-inducing ligand (TRAIL)-induced apoptosis [2,3]. c-FLIP binds to FADD and/or caspase-8or -10 in a ligand-dependent and -independent fashion, which inturn prevents DISC formation and subsequent activation of thecaspase cascade [2,5]. Moreover, c-FLIPL and c-FLIPS are known to
Table 3Therapy response, recidive and survival according to expression of surviving.
c-FLIP P
� 50% > 50%
Rate of therapy response 27 (84.4%) 22 (78.6%) 0.562
Percent of survived patients 24 (75%) 15 (53.6%) 0.083
Percent of relapse 5 (15.6%) 7 (25%) 0.365
have multifunctional roles in various signaling pathways, as wellas activating and/or upregulating several cytoprotective signalingmolecules [2,3]. It, constitutively, expresses in a wide variety ofnormal tissues [16] and in different malignancies [2,16,17].Increased expression of c-FLIP protein was first established inhuman metastatic melanoma [16] and subsequently, in manyother malignancies, including non-Hodgkin’s lymphoma [18,19]and chronic lymphocytic leukemia [20]. Under experimentalconditions, it has been shown that in different types of humancancer cell resistance to apoptosis is caused by increasedexpression of c-FLIP protein and that blocking c-FLIP protein leadsto the loss of resistance and to restore apoptosis triggered bycytokines and various chemotherapeutic agents [18,21]. Expres-sion of c-FLIP is associated with resistance of Reed–Stemberg cellsto Fas-induced apoptosis [19]. However, data about correlationbetween the expression of c-FLIP protein and resistance to Fas-mediated apoptosis in non-Hodgkin’s lymphoma are not consis-tent. Namely, the constitutive expression of c-FLIP in B-lymphoidcells derived from non-Hodgkin’s lymphoma was found to conferresistance to Fas-induced apoptosis in one study [22], whereas nocorrelation between c-FLIP level and resistance to Fas-dependentapoptosis was observed in another study [23].
In our study, increased expression of c-FLIP protein wasdemonstrated in 28 patients (46.7%) with nodal DLBCL, which isconsistent with the results of the previous studies [9,24,25].Bearing in mind the results of in vitro studies, we would expectthat increased expression of c-FLIP protein result in forming ofhemoresistant disease and poor outcome. However, the results ofits prognostic significance are not consistent.
Muris et al. found that c-FLIP is a favorable prognostic factor forpredicting response to therapy in patients with DLBCL [9]. In thisstudy, five-year survival rate of patients with the expression ofc-FLIP was significantly longer compared to patients withoutexpression of this protein. On the contrary, Harris et al. showedthat c-FLIP identifies poor prognostic subset of patients with DLBCL[26]. Valente et al. showed that c-FLIP expression is a significantadverse prognostic factor for predicting therapy response andsurvival in patients with ‘‘low grade’’ lymphoma, regardless of thetype of therapy (IHT or HT), but not in patients with agressive non-Hodgkin’s lymphoma [24]. Thiebault et al. found a significantcorrelation between the expression of c-FLIP protein and shortersurvival in the group of patients with Burkitt lymphoma [27]. Inour study, c-FLIP was not significantly related neither to responseto therapy nor survival of patients with DLBCL. In fact, patientswith c-FLIP expression had shorter survival, but this difference didnot reach statistical significance.

O. Markovic et al. / Biomedicine & Pharmacotherapy 67 (2013) 445–449 449
The confusing and opposite results regarding the prognosticsignificance of expression of c-FLIP can be explained by the dualfunction c-FLIP protein. Namely, it was determined that differentisoforms have different abilities in controlling chemotherapy-induced apoptosis [28]. Although it was initially described as aninhibitor of caspase-8, it turned out that c-FLIPL isoform could alsocontribute to caspase-8 activation. It can be pro-apoptotic or anti-apoptotic protein depending on the degree of expression, which isnot the case with the other isoforms of c-FLIP protein [3,28]. Whenit is highly expressed, c-FLIPL isoform competes with procaspase-8/10 for the recruitment into the DISC, acting as a potent inhibitor ofdeath receptor-induced apoptosis. On the contrary, at lowconcentration, c-FLIPL heterodimerizes with caspase-8 and cas-pase-8 auto-processing occurs [2,28]. In addition, extrinsicapoptosis pathway does not depend on the absolute level ofexpression of c-FLIPS, but also on the ratio of CD95 and c-FLIPS
expression as well as on the amount of different c-FLIP isoformsand the cellular context [2,28]. Finally, the differences in the levelof expression of c-FLIP protein in various studies may be alsoexplained by the use of different antibodies that either reacts withall splice variant (antibodies that recognize the N terminal part) orwith only one isoform of c-FLIP protein (antibodies that bind to theC terminal part only detect c-FLIPL splice variant).
Similarly with results of Haris et al. (2012), we did not noticesignificant difference in surviving expression between GCB andnon-GCB subtype, which means that c-FLIP does not contribute to aworse prognosis of non-GBC subtype.
Our study has contributed to the clarification of prognosticsignificance of c-FLIP in patients with DLBCL. This is the first studyin which the expression of c-FLIP is analyzed in a homogeneousgroup of patients with nodal DLBCL treated exclusively withimmunochemotherapy.
Although our results showed that c-FLIP can not be considereduseful for predicting prognosis in patients with DLBCL, furtherlarger studies are needed in order to examine the expression ofeach of splice variants separately and their prognostic significancein DLBCL patients.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
References
[1] Safa AR. c-FLIP, a master anti-apoptotic regulator. Exp Oncol 2012;34(3):176–84.
[2] Ozturka S, Schleicha K, Lavrika. Cellular FLICE-like inhibitory proteins (c-FLIPs): fine-tuners of life and death decisions. Exp Cell Res 2012;318:1324–31.
[3] Bagnoli M, Canevari S, Mezzanzanica D. Cellular FLICE-inhibitory protein(c-FLIP) signalling: a key regulator of receptor-mediated apoptosis in physio-logic context and in cancer. Internat J Biochem Cell Biol 2010;42:210–3.
[4] Scaffidi C, Schmitz I, Krammer PH, Peter ME. The role of c-FLIP in modulation ofCD95-induced apoptosis. J Biol Chem 1999;274:1541–8.
[5] Krueger A, Schmitz I, Baumann S, Krammer PH, Kirchhoff S. Cellular FLICE-inhibitory protein splice variants inhibit different steps of caspase-8 activationat the CD95 death-inducing signaling complex. J Biol Chem 2001;276:20633–40.
[6] De Paepe P, De Wolf-Peeters C. Diffuse large B-cell lymphoma: a heteroge-neous group of non-Hodgkin lymphomas comprising several distinct clinico-pathological entities. Leukemia 2007;21(1):37–43.
[7] Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al.Confirmation of the molecular classification of diffuse large B-cell lymphomaby immunohistochemistry using a tissue microarray. Blood 2004;103(1):275–82.
[8] Nyman H, Jerkeman M, Karjalainen-LindsbergML, Banham AH, Leppa S, et al.Prognostic impact of activated B-cell focused classification in diffuse large B-cell lymphoma patients treated with R-CHOP. Mod Pathol 2009;22:1094–101.
[9] Muris JJ, Meijer CJ, Vos W, van Krieken JH, Jiwa NM, Ossenkoppele GJ, et al.Immunohistochemical profiling based on Bcl-2, CD10 and MUM1 expressionimproves risk stratification in patients with primary nodal diffuse large B celllymphoma. J Pathol 2006;208(5):714–23.
[10] Troutaud D, Petit B, Bellanger C, Marin B, Gourin-Chaury MP, Petit D, et al.Prognostic significance of BAD and AIF apoptotic pathways in diffuse largeB-cell lymphoma. Clin Lymphoma Myeloma Leuk 2010;10(2):118–24.
[11] Markovic O, Marisavljevic D, Cemerikic V, Perunicic M, Savic S, Filipovic B, et al.Clinical and prognostic significance of apoptotic profile in patients with newlydiagnosed nodal diffuse large B-cell lymphoma (DLBCL). Eur J Haematol2011;86(3):246–55.
[12] Stein H. In: Jaffe ES, Harris NL, editors. World Health Organization Classifica-tion of Tumours Pathology and Genetics of Tumours of Haemopoietic andLymphoid Tissues. IARC Press: Lyon, France; 2001.
[13] Lister TA, Crowther D, Sutcliffe SB, et al. Report of a committee convened todiscuss the evaluation and staging of patients with Hodgkin’s disease: Cots-wolds meeting. J Clin Oncol 1989;7(11):1630–6.
[14] The international non-Hodgkin lymphoma Prognostic factors Project, 1993.[15] Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, et al. Report
of an international workshop to standardize response criteria for non-Hodg-kin’s lymphomas. NCI sponsored International Working Group. J Clin Oncol1999;17(4):1244–9.
[16] Irmler M, Thome M, Hahne P, Schneider K, Hofmann K, et al. Inhibition of deathreceptor signals by cellular FLIP. Nature 1997;388:190–5.
[17] KimY, Suh N, Sporn M, Reed JC. An inducible pathway for degradation of FLIPprotien sensitizes tumor cells to TRAIL-induced Apoptosis. J Biol Chem 2002;277:223–9.
[18] Dutton A, O’Neil JD, Milner AE, Reynolds GM, Starczynski J, Crocker J, et al.Expression of the cellular FLICE-inhibitory protein (c-FLIP) protects Hodgkin’slymphoma cells from autonomous Fas-mediated death. Proc Natl Acad Sci U SA 2004;101(17):6611–6.
[19] Mathas S, Lietz A, Anagnostopoulos I, Hummel F, Wiesner B, Janz M. c-FLIPmediates resistance of Hodgkin/Reed-Sternberg cells to death receptor–in-duced apoptosis. J Exp Med 2004;199(8):1041–52.
[20] MacFarlane M, Harper N, Snowden RT, Dyer MJ, Barnett GA, Pringle JH, et al.Mechanisms of resistance to TRAIL-induced apoptosis in primary B cellchronic lymphocytic leukaemia. Oncogene 2002;21(44):6809–18.
[21] Longley DB, Wilson TR, McEwan M, Allen WL, McDermott U, Galligan L, et al. c-FLIP inhibits chemotherapy-induced colorectal cancer cell death. Oncogene2006;25(6):838–48.
[22] Irisarri M, Plumas J, Bonnefoix T, Jacob MC, Roucard C, Pasquier MA, et al.Resistance to CD95-mediated apoptosis through constitutive c-FLIP expres-sion in a non-Hodgkin’s lymphoma B cell line. Curr Biol 2000;10:640–8.
[23] Lajmanovich A, Irisarri M, Molens JP, Pasquier MA, Sotto JJ, Bensa JC. Im-pairment of death-inducing signalling complex formation in CD95-resistanthuman primary lymphoma cells. Br J Haematol 2004;124:746–53.
[24] Valente G, Manfroi F, Peracchio C, Nicotra G, Castino R, Nicosia G, et al. c-FLIPexpression correlates with tumor progression and patient outcome in non-Hodgkin lymphomas of low grade of malignancies. Br J Haematol 2006;132:560–70.
[25] Van Houdt IS, Muris JJ, Hesselink AT, et al. Expression of c-FLIP is primarilydetected in diffuse large B-cell lymphoma and Hodgkin’s lymphoma andcorrelates with lack of caspase 8 activation. Histopathology 2007;51:778–84.
[26] Harris J, Ibrahim H, Amen F, Karadimitris A, Naresh KN. Cellular (FLICE) likeinhibitory protein (c-FLIP) expression in diffuse large B-cell lymphoma iden-tifies a poor prognostic subset, but fails to predict the molecular subtype.Hematol Oncol 2012;30:8–12.
[27] Thiebault S, et al. c-Flip protein expression in Burkitt’s lymphomas is associ-ated with a poor clinical outcome. Br J Haematol 2005;128:767–73.
[28] Chang DW, Xing Z, Pan Y, Algeciras-Schimnich A, Barnhart BC, Yaish-Ohad S,et al. c-FLIP(L) is a dual function regulator for caspase 8 activation and CD 95mediates apoptosis. EMBO J 2002;21:3704–14.