Embed Size (px)
Citation preview

Nursing Management During Labor and Birth
14ch
ap
ter
KeyTERMSaccelerationsartifactbaseline fetal heart ratebaseline variabilitycrowningdecelerationelectronic fetal monitoringepisiotomyLeopold’s maneuversneuraxial
analgesia/anesthesiaperiodic baseline changes
LearningOBJECTIVESAfter studying the chapter content, the student should be able toaccomplish the following:
1. Define the key terms.2. Describe the assessment data collected on admission to the perinatal unit.3. Identify the measures used to evaluate maternal status during labor and birth.4. Compare and contrast the advantages and disadvantages of external and
internal fetal monitoring, including the appropriate use for each.5. Describe appropriate nursing interventions to address nonreassuring fetal heart
rate patterns.6. Outline the nurse’s role in fetal assessment.7. Explain the various comfort-promotion and pain-relief strategies used during
labor and birth.8. Discuss the ongoing assessment involved in each stage of labor and birth.9. Delineate the nurse’s role throughout the labor and birth process.
Key Learning

he laboring and birthing processis a life-changing event for many women. Nurses need tobe respectful, available, encouraging, supportive, and pro-fessional in dealing with all women. The nursing manage-ment for labor and birth should include comfort measures,emotional support, information and instruction, advocacy,and support for the partner (Simkin, 2002).
pregnant women who attend a series of prepared child-birth classes. (See Chapters 12 and 22 for more informa-tion on these objectives.)
This chapter provides information about nursingmanagement during labor and birth. It describes the nec-essary data to be obtained with the admission assessmentand methods to evaluate labor progress and maternal andfetal status. The chapter also describes the major meth-ods for comfort promotion and pain management. Thechapter concludes with a discussion of the nursing man-agement specific to each stage of labor, including keynursing measures that focus on maternal and fetal assess-ments and pain relief.
Admission AssessmentsThe nurse usually first comes in contact with the womaneither by phone or in person. It is important to ascertainwhether the woman is in true or false labor and whethershe should be admitted or sent home.
If the initial contact is by phone, the nurse needs toestablish a therapeutic relationship with the woman. Thisis facilitated by speaking in a calm, caring tone. Whencompleting a phone assessment, include questions aboutthe following:
• Estimated date of birth, to determine if term or preterm• Fetal movement (frequency in the past few days)• Other premonitory signs of labor experienced• Parity, gravida, and previous childbirth experiences• Time from start of labor to birth in previous labors• Characteristics of contractions, including frequency,
duration, and intensity• Appearance of any vaginal bloody show• Membrane status (ruptured or intact)• Presence of supportive adult in household or if she
is alone
When speaking with the woman over the telephone,review the signs and symptoms that denote true versusfalse labor, and suggest various positions she can assumeto provide comfort and increase placental perfusion. Alsosuggest walking, massaging, and taking a warm shower topromote relaxation. Outline what foods and fluids areappropriate for oral intake in early labor. Throughout thephone call, listen to the woman’s concerns and answerany questions clearly.
Reducing the risk of liability exposure and avoidingpreventable injuries to mothers and fetuses during laborand birth can be accomplished by adhering to two basictenets of clinical practice: (1) use applicable evidenceand/or published standards and guidelines as the foun-
Wise nurses are not always silent, but they know when to be
during the miracle of birth.
wow
332
T
The health of mothers and their infants is of criticalimportance, both as a reflection of the current health sta-tus of a large segment of our population and as a predictorof the health of the next generation. Healthy People 2010(DHHS, 2000) addresses maternal health in two objectivesfor reducing maternal deaths and for reducing maternalillness and complications due to pregnancy. In addition,another objective addresses increasing the proportion of
ConsiderTHIS!Since I was expecting my first child, I was determined toput my best foot forward and do everything right, for I wasan experienced OB nurse and in my mind it was expectedbehavior. I was already 2 weeks past my “calculated duedate” and I was becoming increasingly worried. Today I went to work with a backache but felt no contractions. I managed to finish my shift but felt wiped out. As I walkedto my car outside the hospital, my water broke and I feltthe warm fluid run down my legs. I went back inside tobe admitted for this much-awaited event.
Although I had helped thousands of women go throughtheir childbirth experience, I was now the one in the bedand not standing alongside it. My husband and I hadpracticed our breathing techniques to cope with the dis-comfort of labor, but this “discomfort” in my mind wasmore than I could tolerate. So despite my best inten-tions of doing everything right, within an hour I beggedfor a “painkiller” to ease the pain. While the medicationtook the edge off my pain, I still felt every contractionand truly now appreciate the meaning of the word“labor.” Although I wanted to use natural childbirthwithout any medication, I know that I was a full partici-pant in my son’s birthing experience, and that is what“doing everything right” was for me!
Thoughts: Doing what is right varies for each indi-vidual, and as nurses we need to support whateverthat is. Having a positive outcome from the child-birth experience is the goal, not the means it takes toachieve it. How can nurses support women in mak-ing their personal choices to achieve a healthy out-come? Are any women “failures” if they ask for painmedication to tolerate labor? How can nurses helpwomen overcome this stigma of being a “wimp”?
Consider

dation of care, and (2) whenever a clinical choice is pre-sented, chose client safety (Simpson & Knox, 2003). Withthis advice in mind, advise the woman on the phone tocontact her healthcare provider for further instructionsor to come to the facility to be evaluated, since ruling outtrue labor and possible maternal-fetal complications can-not be done accurately over the phone.
Additional nursing responsibilities associated with aphone assessment include:
• Consult the woman’s prenatal record for parity status,estimated date of birth, and untoward events.
• Call the healthcare provider to inform him or her of thewoman’s status.
• Prepare for admission to the perinatal unit to ensure ade-quate staff assignment.
• Notify the admissions office of a pending admission.
If the nurse’s first encounter with the woman is in per-son, an assessment is completed to determine whether sheshould be admitted to the perinatal unit or sent home untilher labor advances. Entering a facility is often an intimi-dating and stressful event for women since it is an unfamil-iar environment. Giving birth for the first time is a pivotalevent in the lives of most women. Therefore, demonstraterespect when addressing the client and thoroughly listenand express interest and concern. Nurses must value andrespect women and promote their self-worth by allowingthem to participate in making decisions and fostering asense of control (Matthews & Callister, 2004).
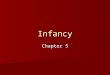
An admission assessment includes maternal healthhistory, physical assessment, fetal assessment, laboratorystudies, and assessment of psychological status. Usuallythe facility has a specialized form that can be used through-out labor and birth to document assessment findings(Fig. 14-1).
Maternal Health HistoryA maternal health history should include typical bio-graphical data such as the woman’s name and age and thename of delivering healthcare provider. Other informationthat is collected includes the prenatal record data, includ-ing the estimated date of birth, a history of the currentpregnancy, and the results of any laboratory and diagnos-tic tests, such as blood type and Rh status; past pregnancyand obstetric history; past health history and family his-tory; prenatal education; list of medications; risk factorssuch as diabetes, hypertension, use of tobacco, alcohol, orillicit drugs; reason for admission, such as labor, cesareanbirth, or observation for a complication; history of poten-tial domestic violence; history of previous preterm births;allergies; time of last food ingestion; method chosen forinfant feeding; name of birth attendant and pediatrician;and pain management plan.
Ascertaining this information is important to developan individualized plan of care for the woman. If, for
example, the woman’s due date is still 2 months away, itis important to establish this information so interventionscan be initiated to arrest the labor immediately or notifythe intensive perinatal team to be available. In addition,if the woman is a diabetic, it is critical to monitor her glu-cose levels during labor, to prepare for a surgical birth ifdystocia of labor occurs, and to alert the newborn nurs-ery of potential hypoglycemia in the newborn after birth.By collecting important information about each womanthey care for, nurses can help improve the outcomes forall concerned.
Be sure to observe the woman’s emotions, supportsystem, verbal interaction, body language and posture,perceptual acuity, and energy level. Also note her culturalbackground and language spoken. This psychosocial infor-mation provides cues about the woman’s emotional state,culture, and communication systems. For example, if thewoman arrives at the labor and birth suite extremely anx-ious, alone, and unable to communicate in English, howcan the nurse meet her needs and plan her care appropri-ately? It is only by assessing each woman physically andpsychosocially that the nurse can make astute decisionsregarding proper care. In this case, an interpreter would beneeded to assist in the communication process betweenthe healthcare staff and the woman to initiate proper care.
It is important for the nurse to acknowledge and try tounderstand the cultural differences in women with culturalbackgrounds different from that of the nurse. Attitudestoward childbirth are heavily influenced by the culture inwhich the woman has been raised. As a result, within everysociety, specific attitudes and values shape the woman’schildbearing behaviors. Be aware of what these are. Whencarrying out a cultural assessment during the admissionprocess, ask questions (Box 14-1) to help plan culturallycompetent care during labor and birth.
Physical ExaminationThe physical examination typically includes a generalizedassessment of the woman’s body systems, including hydra-tion status, vital signs, auscultation of heart and lungsounds, and measurement of height and weight. The phys-ical examination also includes the following assessments:
• Fundal height measurement• Uterine activity, including contraction frequency, dura-
tion, and intensity• Status of membranes (intact or ruptured)• Cervical dilatation and degree of effacement• Fetal status, including heart rate, position, and station• Pain level
These assessment parameters (described in greaterdetail later in this chapter), form a baseline against whichthe nurse can compare all future values throughout labor.The findings should be similar to those of the woman’sprepregnancy and pregnancy findings, with the exception
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 333

Chronic HTN
ViaADMISSION DATA NEUROLOGICAL
Reason for Admission
Current Pregnancy Labs
Previous OB History
ADMISSION ASSESSMENT OBSTETRICS
Ambulatory Wheelchair StretcherGA
HA
Reflexes
WNL WNL
PATIENT IDENTIFICATION
WNL
WNL
WNL
WNL
WNL
WNL
NRFSFHR
WNL
WNLHeartburn
Tingling
MVP< 60
< 30 cc/Hr.
> 100
> 90> 140
< 50< 90
LMPEDCLivingPre-term Ab.
TimeDate
Grav.
Prev. adm. date
Term
ReasonObstetrician Pediatrician
Ht. Wt. gainWt.
NoneAllergies (meds/food) Hx latex sensitivity
BP
Labor / SROM
FHR
T P R
Vag exam
Induction
Primary C/S Repeat C/S
Observation
Onset of labor:
OB / Medical complication
Date
POL
Membranes: IntactRuptured / DateClear
Vaginal bleeding:Normal show
Time
Time
NoneMeconium Bloody Foul
Not in labor
PIHPPROM
NPC
Chr. HTNCerclageOther
Diet
Results
DiabetesInsulinAmniocentesis
Bld type / RH Date RhogamAntibody screen Rubella
Neg PosPos Neg Tested
Non-immune Immune
NormalDiabetic screen AbnormalRecent exposure to chick poxCurrent meds:
Hepatitis BHIV
POL
PIH
Group B strepGCChlamydiaRPR No
NoNoNoNoNo
Multiple gestationReason
DiabetesPrev C/S type
Anomalies
No
Macrosomia
Yes
NeodeathStillbirth/demisePrecipitous labor (<3 H)PP HemorrhageHx Transfusion reactionOther
1.2.
Latest risk assessment None3.4.
Signature
Date
Time
CARDIOVASCULAR
MUSCULOSKELETAL
GASTROINTESTINAL
INTEGUMENTARY
EARS, NOSE, THROAT, AND EYES
GENITOURINARY
PESPIRATORY
Variance: Variance:
Variance:
Variance:
Variance:
Variance:
Variance:
Variance:
Sore throat
Variance:
Variance:
Scotoma / visual changes
NumbnessHx Seizures
Hx Asthma
< 2 + > 2 +Clonus bts
Tingling
Heart rate:B/P: Systolic:
Diastolic:
EdemaChest pain / palpitations
Numbness
ScoliosisParalysis Deformity
URI< 12 > 24
SOBEffort:Respirations:
Shallow LaboredAuscultation:
Diminished CracklesWheezes Rhonchi No Yes
Cough for greater than 2 weeks?Is the cough productive? Blood in the sputum?
Ever had TB in the past?Experiencing any fever or night sweats?
Recent exposure to TB?Weight loss in last 3 weeks?If the patient answers yes to any threeof the above questions implementpolicy and procedure # 5725-0704.
AlbuminOutput:
RxUTI FrequencyDysuria HematuriaCVA TendernessHx STDVag. dischargeRash
Rash
WartsBlistersLesions
Runny noseNasal congestion
Eyeglasses
Contact lenses
Hx depression
PSYCHOSOCIAL
FETAL ASSESSMENT
PAIN ASSESSMENT
NauseaDiarrhea
Pain
Epigastric painVomitingConstipationWt. Gain < 2lbs / month**Recent change in appetite of < 50% of usual intake for > 5 days
LacerationsAbrasionUticariaDiaphoretic/hotClammy/coldScars
BruisingSwelling
LTV< 110 > 160
Decelerations:STV Absent
Absent MinimalIncreased
Decreased fetal movementIUGR
DeniesTobacco use
1. Do you have any ongoing pain problems?
Primary languageDrug useAlcohol use Denies
DeniesEnglish
Yes
Yes
Yes
Yes
Yes AmtAmtAmt type
Spanish
YesYes
No
No
No
No
NoNo
YesYes
Emotional behavioral careAffect: Flat Anxious
Uncooperative Combative
Living will
Healthcare surrogateOn chart
On chart
Religious preference
Are you being hurt, hit, frightened by anyoneat home or in your life?
4. Patient to be given pain management education material. Complete pain / symptom assessment on flowsheet.5. Please proceed to complete pain assessment.
3. If any of the above questions are answered yes, the patient has a positive pain screening.2. Do you have any pain now?
l Figure 14-1 Sample documentation form used for admission to the perinatal unit. (Used with permission. Briggs Corporation, 2001.)
334

versal phenomenon, it is a unique experience for eachwoman. Continuous evaluation and appropriate inter-vention for women during labor are key to promoting apositive outcome for the family.
The nurse’s role in childbirth is to ensure a safe envi-ronment for the mother and the birth of her newborn.Nurses begin evaluating the mother and fetus during theadmission procedures at the healthcare agency and con-tinue throughout labor. It is critical to provide anticipatoryguidance and explain each procedure (fetal monitoring,intravenous therapy, medications given, and expectedreactions) and what will happen next. This will preparethe woman for the upcoming physical and emotionalchallenges, thereby helping to reduce her anxiety. Ack-nowledging her support systems (family or partner) helpsallay their fears and concerns, thereby assisting them incarrying out their supportive role. Knowing how and whento evaluate a woman during the various stages of labor isessential for all labor and birth nurses to ensure a positivematernal experience and a healthy newborn.
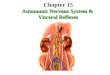
Maternal AssessmentDuring labor and birth, various techniques are used toassess maternal status. These techniques provide an ongo-ing source of data to determine the woman’s responseto and her progress in labor. Assess maternal vital signs,including temperature, blood pressure, pulse, respiration,and pain, which are primary components of the physicalexamination and ongoing assessment (Fig. 14-2). Alsoreview the prenatal record to identify risk factors that maycontribute to a decrease in uteroplacental circulation dur-ing labor. Monitor vital signs (blood pressure, pulse, andrespirations) every 4 hours in the latent phase of labor,hourly in the active phase, and every 15 to 30 minutesduring the transition phase of labor. Monitor temperatureevery 4 hours until the membranes have ruptured, andthen every 1 to 2 hours thereafter. Assess uterine activityand fetal heart rate (FHR) every 30 to 60 minutes in thefirst stage of labor and every 15 to 30 minutes in the active
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 335
• Where were you born? How long have you lived in theUntied States?
• What languages do you speak and read?• Who are your major support people?• What are your religious practices?• How do you view childbearing?• Are there any special precautions or restrictions that
are important?• Is birth considered a private or a social experience?• How would you like to manage your labor discomfort?• Who will provide your labor support? (Moore &
Moos, 2003)
BOX 14-1QUESTIONS FOR PROVIDING CULTURALLY COMPETENTCARE DURING LABOR AND BIRTH
A B
l Figure 14-2 Assessment of vital signs. (A) Nurse monitoring temperature. (B) Nurseassessing blood pressure.
of her pulse rate, which might be elevated secondary toher anxious state with beginning labor.
Laboratory StudiesOn admission, laboratory studies typically are done toestablish a baseline. Although the exact tests may varyamong facilities, they usually include a urinalysis via clean-catch urine specimen and complete blood count (CBC).Blood typing and Rh factor analysis may be necessary if theresults of these are unknown or unavailable. Other teststhat may be done include syphilis screening, hepatitis B(HbsAg) screening, HIV testing (if woman gives consent),and possible drug screening if history is positive.
Evaluation of Labor ProgressChildbirth, a physiologic process that is fundamental toall human existence, is one of the most significant cul-tural, psychological, spiritual, and behavioral events in awoman’s life. Although the act of giving birth is a uni-

and transition phases. If there is no vaginal bleeding onadmission, a vaginal examination is performed to assesscervical dilation, after which it is monitored periodicallyas necessary to identify progress. Evaluate maternal painand the effectiveness of pain-management strategies atregular intervals during labor and birth.
Vaginal ExaminationAlthough not all nurses perform vaginal examinations onlaboring women in all practice settings, most nurses work-ing in community hospitals do so because physicians arenot routinely present in labor and birth suites. Since mostnewborns in the United States are born in community hos-pitals, nurses are performing vaginal examinations (AHA,2003). Vaginal examinations are also performed by mid-wives and physicians. It is an assessment skill that takestime and experience to develop; only by doing it frequentlyin clinical practice can the practitioner’s skill level improve.
The purpose of performing a vaginal examination isto assess the amount of cervical dilation, percentage ofcervical effacement, and fetal membrane status and gatherinformation on presentation, position, station, degree offetal head flexion, and presence of fetal skull swelling ormolding (Fig. 14-3). Prepare the woman by informing herabout the procedure, what information will be obtainedfrom it, how she can assist with the procedure, how it willbe performed, and who will be performing it.
The woman is typically on her back during the vagi-nal examination. The vaginal examination is performedgently, with concern for the woman’s comfort. If it is theinitial vaginal examination to check for membrane status,water is used as a lubricant. If membranes have alreadyruptured, an antiseptic solution is used to prevent an
ascending infection. After donning sterile gloves, the exam-iner inserts his or her index and middle fingers into the vagi-nal introitus. Next, the cervix is palpated to assess dilation,effacement, and position (e.g., posterior or anterior). Ifthe cervix is open to any degree, the presenting fetal part,fetal position, station, and presence of molding can beassessed. In addition, the membranes can be evaluatedand described as intact, bulging, or ruptured.
At the conclusion of the vaginal examination, the find-ings are discussed with the woman and her partner to bringthem up to date about labor progress. In addition, the find-ings are documented either electronically or in writing andreported to the primary healthcare professional in chargeof the case.
Cervical Dilation and EffacementThe amount of cervical dilation and the degree of cervi-cal effacement are key areas assessed during the vaginalexamination as the cervix is palpated with the gloved indexfinger. Although this finding is somewhat subjective, expe-rienced examiners typically come up with similar findings.The width of the cervical opening determines dilation, andthe length of the cervix assesses effacement. The infor-mation yielded by this examination serves as a basis fordetermining which stage of labor the woman is in andwhat her ongoing care should be.
Fetal Descent and Presenting PartIn addition to cervical dilation and effacement findings,the vaginal examination can also determine fetal descent(station) and presenting part. During the vaginal exami-nation, the gloved index finger is used to palpate the fetalskull (if vertex presentation) through the opened cervix orthe buttocks in the case of a breech presentation. Stationis assessed in relation to the maternal ischial spines andthe presenting fetal part. These spines are not sharp pro-trusions but rather blunted prominences at the mid-pelvis. The ischial spines serve as landmarks and havebeen designated as zero station. If the presenting part ispalpated higher than the maternal ischial spines, a negativenumber is assigned; if the presenting fetal part is felt belowthe maternal ischial spines, a plus number is assigned,denoting how many centimeters below zero station.
Progressive fetal descent (−5 to +4) is the expectednorm during labor—moving downward from the negativestations to zero station to the positive stations in a timelymanner. If progressive fetal descent does not occur, a dis-proportion between the maternal pelvis and the fetus mightexist and needs to be investigated.
Rupture of MembranesThe integrity of the membranes can be determined duringthe vaginal examination. Typically, if intact, the mem-branes will be felt as a soft bulge that is more prominentduring a contraction. If the membranes have ruptured,the woman may have reported a sudden gush of fluid.Membrane rupture also may occur as a slow trickle of fluid.
336 Unit 4 LABOR AND BIRTH
l Figure 14-3 Vaginal examination to determine cervicaldilation and effacement.

To confirm that membranes have ruptured, a sampleof fluid is taken from the vagina and tested with Nitrazinepaper to determine the fluid’s pH. Vaginal fluid is acidic,whereas amniotic fluid is alkaline and turns Nitrazinepaper blue. Sometimes, however, false-positive results mayoccur, especially in women experiencing a large amount ofbloody show, because blood is alkaline. The membranesare most likely intact if the Nitrazine test tape remainsyellow to olive green, with pH between 5 and 6. Themembranes are probably ruptured if the Nitrazine testtape turns a blue-green to deep blue, with pH ranging from6.5 to 7.5 (Olds et al., 2004).
If the Nitrazine test is inconclusive, an additional test,called the fern test, can be used to confirm rupture ofmembranes. With this test, a sample of fluid is obtained,applied to a microscope slide, and allowed to dry. Using amicroscope, the slide is examined for a characteristic fernpattern that indicates the presence of amniotic fluid.
Uterine ContractionsThe primary power of labor is uterine contractions, whichare involuntary. Uterine contractions increase intrauterinepressure, causing tension on the cervix. This tension leadsto cervical dilation and thinning, which in turn eventuallyforces the fetus through the birth canal. Normal uterinecontractions have a contraction (systole) and a relaxation(diastole) phase. The contraction resembles a wave, mov-ing downward to the cervix and upward to the fundusof the uterus. Each contraction starts with a building up(increment), gradually reaching an acme (peak intensity),and then a letting down (decrement). Each contraction isfollowed by an interval of rest, which ends when the nextcontraction begins. At the acme (peak) of the contrac-tion, the entire uterus is contracting, with the greatestintensity in the fundal area. The relaxation phase followsand occurs simultaneously throughout the uterus.
Uterine contractions during labor are monitored bypalpation and by electronic monitoring. Assessment ofthe contractions includes frequency, duration, inten-sity, and uterine resting tone (see Chapter 13 for a moredetailed discussion).
Uterine contractions with an intensity of 30 mm Hgor greater initiate cervical dilation. During active labor,the intensity usually reaches 50 to 80 mm Hg. Restingtone is normally between 5 and 10 mm Hg in early laborand between 12 and 18 mm Hg in active labor (Gilbert& Harmon, 2003).
To palpate the fundus for contraction intensity, placethe pads of your fingers on the fundus and describe howit feels: like the tip of the nose (mild), like the chin (mod-erate), or like the forehead (strong). Palpation of inten-sity is a subjective judgment of the indentability of theuterine wall; a descriptive term is assigned (mild, moder-ate, or strong (Fig. 14-4). Frequent clinical experience isneeded to gain accuracy in assessing the intensity of uter-ine contractions.
The second method used to assess the intensity ofuterine contractions is electronic monitoring, either exter-nal or internal. Both methods provide an accurate mea-surement of the actual intensity of uterine contractions.Although the external fetal monitor is sometimes used toestimate the intensity of uterine contractions, it is not asaccurate an assessment tool.
For woman at risk for preterm birth, home uterineactivity monitoring can be used to screen for prelabor uter-ine contractility so that escalating contractility can beidentified, allowing earlier intervention to prevent pretermbirth. The home uterine activity monitor consists of a pres-sure sensor attached to a belt that is held against theabdomen and a recording/storage device that is carried ona belt or hung from the shoulder. Uterine activity is typi-cally recorded by the woman for one hour twice daily,while performing routine activities. The stored data aretransmitted via telephone to a perinatal nurse, where areceiving device prints out the data. The woman is con-tacted if there are any problems.
Although in theory identifying early contractions toinitiate interventions to arrest the labor sounds reason-able, research shows that uterine activity monitoring inasymptomatic high-risk women is inadequate for pre-dicting preterm birth (Newman, 2003). This practicecontinues even though numerous randomized trials havefound no relationship between monitoring and actualreduction of preterm labor. The value of monitoring uter-ine contraction frequency as a predictor of preterm deliv-ery remains unclear (Iams et al., 2002).
Leopold’s ManeuversLeopold’s maneuvers are a method for determiningthe presentation, position, and lie of the fetus through theuse of four specific steps. This method involves inspec-tion and palpation of the maternal abdomen as a screen-ing assessment for malpresentation. A longitudinal lie is
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 337
l Figure 14-4 Nurse palpating the woman’s fundusduring a contraction.

expected, and the presentation can be cephalic, breech,or shoulder. Each maneuver answers a question:
• What fetal part (head or buttocks) is located in thefundus (top of the uterus)?
• On which maternal side is the fetal back located? (Fetalheart tones are best auscultated through the back ofthe fetus.)
• What is the presenting part?• Is the fetal head flexed and engaged in the pelvis?
(Nursing Procedure 14-1)
Fetal AssessmentA fetal assessment identifies well-being and signs indicativeof compromise. It primarily focuses on determining the
338 Unit 4 LABOR AND BIRTH
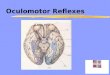
Nursing Procedure 14-1Performing Leopold’s Maneuvers
Purpose: To Determine Fetal Presentation, Position, and Lie
1. Place the woman in the supine position andstand beside her.
2. Perform the first maneuver to determine presentation.a. Facing the woman’s head, place both hands
on the abdomen to determine fetal position inthe uterine fundus.
b. Feel for the buttocks, which will feel soft andirregular (indicates vertex presentation); feelfor the head, which will feel hard, smooth,and round (indicates a breech presentation).
4. Perform the third maneuver to confirm presentation.a. Move hands down the sides of the abdomen
to grasp the lower uterine segment and pal-pate the area just above the symphysis pubis.
b. Place thumb and fingers of one hand apartand grasp the presenting part by bringing fingers together.
c. Feel for the presenting part. If the presentingpart is the head, it will be round, firm, andballottable; if it is the buttocks, it will feel softand irregular.
3. Complete the second maneuver to determineposition.a. While still facing the woman, move hands
down the lateral sides of the abdomen to palpate on which side the back is (feels hardand smooth).
b. Continue to palpate to determine on whichside the limbs are located (irregular noduleswith kicking and movement).
First maneuverSecond maneuver

FHR pattern, but the character of the amniotic fluid is alsoassessed. Amniotic fluid should be clear when membranesrupture, either spontaneously or artificially through anamniotomy (a disposable plastic hook [Amnihook] is usedto perforates the amniotic sac). Cloudy or foul-smellingamniotic fluid indicates infection, whereas green fluid indi-cates that the fetus has passed meconium secondary totransient hypoxia (McKinney et al., 2005).
Analysis of the FHR is one of the primary evalua-tion tools used to determine fetal oxygen status indi-rectly. FHR assessment can be done intermittently usinga fetoscope (a modified stethoscope attached to a head-piece) or a Doppler (ultrasound) device or continuouslywith an electronic fetal monitor applied externally orinternally.
Intermittent FHR MonitoringIntermittent FHR monitoring involves auscultation viaa fetoscope or a hand-held Doppler device that usesultrasound waves that bounce off the fetal heart, pro-ducing echoes or clicks that reflect the rate of the fetalheart (Fig. 14-5). Traditionally, a fetoscope was used to assess fetal heart rate, but the Doppler device hasbeen found to have a greater sensitivity than the feto-scope (Engstrom, 2004); thus, at present it is morecommonly used.
Doppler devices are relatively low in cost and are notused only in hospitals. Pregnant women can purchasethem to aid in reducing anxiety between clinical exami-nations if they had a previous problem during pregnancy(Mainstone, 2004).
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 339
Nursing Procedure 14-1Performing Leopold’s Maneuvers (continued)
Purpose: To Determine Fetal Presentation, Position, and Lie
b. Move fingers toward each other while apply-ing downward pressure in the direction of the symphysis pubis. If you palpate a hard area on the side opposite the fetal back, the fetus is in flexion, because youhave palpated the chin. If the hard area is on the same side as the back, the fetus is inextension, because the area palpated is theocciput.
c. Also, note how your hands move. If thehands move together easily, the fetal head isnot descended into the woman’s pelvic inlet.If the hands do not move together and stopbecause of resistance, the fetal head isengaged into the woman’s pelvic inlet(Dillon, 2003).
5. Perform the fourth maneuver to determine attitude.a. Turn to face the client’s feet and use the
tips of the first three fingers of each hand topalpate the abdomen.
Third maneuver Fourth maneuver

The procedure for using a fetoscope or Doppler deviceto assess FHR is similar (see Nursing Procedure 12-1 inChapter 12). The main difference is that a small amount ofwater-soluble gel is applied to the woman’s abdomen orultrasound device before auscultation to promote soundwave transmission. This gel is not needed when a fetoscopeis used. Usually the FHR is best heard in the woman’slower abdominal quadrants, but if it is not found quickly,it may help to locate the fetal back by performing Leopold’smaneuvers.
Although the intermittent method of FHR assessmentallows the client to move about during her labor, the infor-mation obtained fails to provide a complete picture of thewell-being of the fetus moment to moment. This leads tothe question of what the fetal status is during the times thatare not assessed. For women who are considered at lowrisk for complications, this period of non-assessment isnot a problem. However, for the undiagnosed high-riskwoman, it might prove ominous.
National professional organizations have providedgeneral guidelines for the frequency of assessments basedon existing evidence. The American College of Obstetri-cians and Gynecologists (ACOG), the Institute for Clini-cal Systems Improvement (ICSI), and the Associationof Women’s Health, Obstetric, and Neonatal Nurses(AWHONN) have published guidelines designed to assistclinicians in caring for laboring clients. Their recom-mendations are supported by large controlled studies.They recommend the following guidelines for assess-ing FHR:
• Initial 10- to 20-minute continuous FHR assessment onentry into labor/birth area
• Completion of a prenatal and labor risk assessment onall clients
• Intermittent auscultation every 30 minutes during activelabor for a low-risk woman and every 15 minutes for ahigh-risk woman
• During the second stage of labor, every 15 minutes forthe low-risk woman and every 5 minutes for the high-riskwoman and during the pushing stage (ACOG, 2005;AWHONN, 2000; ICSI, 2003).
In several randomized controlled studies comparingintermittent auscultation with electronic monitoring inboth low- and high-risk clients, no difference in intra-partum fetal death was found. However, in each study anurse–client ratio of 1:1 was consistently maintained dur-ing labor (ICSI, 2003). This suggests that adequate staffingis essential with intermittent FHR monitoring to ensureoptimal outcomes for the mother and fetus. Althoughthere is insufficient evidence to indicate specific situationswhere continuous electronic fetal monitoring might resultin better outcomes when compared to intermittent assess-ment, for pregnancies involving an increased risk of peri-
Intermittent FHR monitoring affords the advantageof mobility for the woman in the first stage of labor. Sheis free to move around and change position at will sinceshe is not attached to a stationary electronic fetal moni-tor. However, intermittent monitoring does not docu-ment how the fetus responds to the stress of labor anddoes not provide a continuous recording of the fetal heartrate. In addition, it does not show the fetal responseduring the acme of a contraction, because intermittentmonitoring is typically done after a contraction, when theuterus is relaxed. The pressure of the device during a con-traction is uncomfortable and can distract the womanfrom using her paced-breathing patterns.
Intermittent FHR auscultation can be used to detectFHR baseline and rhythm and changes from baseline.However, it cannot detect variability and types of deceler-ations, as electronic fetal monitoring can (Feinstein et al.,2003). During intermittent auscultation to establish abaseline, the FHR is assessed for a full minute after a con-traction. From then on, unless there is a problem, listen-ing for 30 seconds and multiplying the value by two issufficient. If the woman experiences a change in conditionduring labor, auscultation assessments should be more fre-quent. Changes in condition include ruptured membranesor the onset of bleeding. In addition, more frequent assess-ments occur after periods of ambulation, after a vaginalexamination, after administration of pain medications, orother clinical important events (SOGC, 2002).
The FHR is heard most clearly at the fetal back. In acephalic presentation, the FHR is best heard in the lowerquadrant of the maternal abdomen. In a breech presenta-tion, it is heard at or above the level of the maternal umbili-cus (Fig. 14-6). As labor progresses, the FHR location willchange accordingly as the fetus descends lower into thematernal pelvis for the birthing process. To ensure thatthe maternal heart rate is not confused with the fetal heartrate, palpate the client’s radial pulse simultaneously whilethe FHR is being auscultated through the abdomen.
340 Unit 4 LABOR AND BIRTH
l Figure 14-5 Auscultating fetal heart rate.

natal death, cerebral palsy, or neonatal encephalopathy anduse of oxytocin for induction or augmentation, it is recom-mended that continuous electronic fetal monitoring beused rather than intermittent fetal auscultation (SOGC,2002, p. 6).
Continuous Electronic Fetal MonitoringElectronic fetal monitoring uses a machine to pro-duce a continuous tracing of the FHR. When the moni-toring device is in place, an audible sound is produced
with each heartbeat. In addition, a graphic record of theFHR pattern is produced.
Current methods of continuous electronic fetal mon-itoring were introduced in the United States during the1960s, specifically for use in clients considered to behigh risk. However, the use of these methods graduallyincreased and they eventually came to be used for womenconsidered to be high or low risk. This increased use hasbecome controversial, because it was suspected of beingassociated with unnecessary cesarean birth, rates of which
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 341
A B
D E
C
l Figure 14-6 Locations for auscultating fetal heart rate based on fetal position. (A) Leftocciput anterior (LOA). (B) Right occiput anterior (ROA). (C) Left occiput posterior(LOP). (D) Right occiput posterior (ROP). (E) Left sacral anterior (LSA).

have climbed steadily (Sisk, 2002). The efficacy of elec-tronic fetal monitoring depends on the accurate inter-pretation of the tracings, not necessarily which method(external vs. internal) is used.
Having a continuous assessment of fetal well-beingdocumented during the stress of labor is important.The concept of hearing and evaluating every beat of thefetus’s heart to allow for early intervention seems logical.However, the use of continuous electronic fetal monitor-ing has had no demonstrated effect on the incidence ofnewborns born with neurologic damage. Furthermore, therate of preterm birth and cesarean births has increasedmarkedly (Priddy, 2004).
The use of continuous fetal monitoring for all preg-nant clients, whether high risk or low risk, has been crit-icized by various groups within the medical community.Concerns about the efficiency and safety of routine elec-tronic fetal monitoring in labor have led expert panels inthe United States to recommend that such monitoring belimited to high-risk pregnancies. However, its use in low-risk pregnancies continues globally (Thacker & Stroup,2003). This remains an important research issue.
With electronic fetal monitoring, there is a continu-ous record of the fetal heart rate, and thus no gaps exist,as they do with intermittent auscultation. On the down-side, using continuous monitoring can limit maternalmovement and encourages her to lie in the supine posi-tion, which reduces placental perfusion. Despite the crit-icism, electronic fetal monitoring remains an accuratemethod for determining fetal health status by providing amoment-to-moment printout of FHR status.
Continuous electronic fetal monitoring can be per-formed externally (indirectly) with attachment to thematernal abdominal wall or internally (directly) withattachment to the fetus. Both methods provide a continu-ous printout of the FHR, but they differ in their specificity.
External MonitoringIn external or indirect monitoring, two ultrasound trans-ducers, each of which is attached to a belt, are appliedaround the woman’s abdomen. They are similar to thehand-held Doppler device. One transducer, called a toco-transducer, detects changes in uterine pressure and con-verts the pressure registered into an electronic signal thatis recorded on graph paper (Pillitteri, 2003). The toco-transducer is placed over the uterine fundus in the area ofgreatest contractility to monitor uterine contractions. Theother ultrasound transducer records the baseline FHR,long-term variability, accelerations, and decelerations. Itis positioned on the maternal abdomen in the midlinebetween the umbilicus and the symphysis pubis. Thediaphragm of the ultrasound transducer is moved to eitherside of the abdomen to obtain a stronger sound and thenattached to the second elastic belt. This transducer con-verts the fetal heart movements into audible beepingsounds and records them on graph paper (Fig. 14-7).
Good continuous data are provided on the FHR.External monitoring can be used while the membranes arestill intact and the cervix is not yet dilated. It is non-invasive and can detect relative changes in abdominalpressure between uterine resting tone and contractions.External monitoring also measures the approximate dura-tion and frequency of contractions, providing a permanentrecord of FHR (Feinstein et al., 2003).
However, external monitoring can restrict themother’s movements. It also cannot detect short-termvariability. Signal disruptions can occur due to maternalobesity, fetal malpresentation, and fetal movement, aswell as by artifact. Artifact describes irregular variations orabsence of FHR on the fetal monitor record, resulting frommechanical limitations of the monitor or electrical interfer-ence. For instance, the monitor may pick up transmissionsfrom CB radios used by truck drivers on nearby roads andtranslate them into a signal. Additionally, gaps in the mon-itor strip can occur periodically without explanation.
Continuous Internal MonitoringContinuous internal monitoring is usually indicated forwomen or fetuses considered high risk. Possible condi-tions might include multiple gestation, decreased fetalmovement, abnormal FHR on auscultation, intrauterinegrowth restriction (IUGR), maternal fever, preeclampsia,dysfunctional labor, preterm birth, or medical conditionssuch as diabetes or hypertension. It involves the place-ment of a spiral electrode into the fetal presenting part,usually the head, to assess FHR and a pressure trans-ducer internally to record uterine contractions (Fig. 14-8).The fetal spiral electrode is considered the most accuratemethod of detecting fetal heart characteristics and patternsbecause it involves directly receiving a signal from the fetus(Feinstein et al., 2003).
Both the FHR and the duration and interval of uter-ine contractions are recorded on the graph paper. Thismethod permits evaluation of baseline heart rate andchanges in rate and pattern.
342 Unit 4 LABOR AND BIRTH
l Figure 14-7 Continuous external EFMdevice applied to the woman in labor.

Four specific criteria must be met for this type ofmonitoring to be used:
• Ruptured membranes• Cervical dilation of at least 2 cm• Presenting fetal part low enough to allow placement of
the scalp electrode• Skilled practitioner available to insert spiral electrode
(Ladewig, London, & Davidson, 2006)
Compared to external monitoring, continuous inter-nal monitoring can accurately detect both short-term(moment-to-moment changes) and long-term variability(fluctuations within the baseline) and FHR dysrhythmias.In addition, it allows for maternal positional changes andmovement that doesn’t interfere with the quality of thetracing.
FHR PatternsAssessment parameters of the FHR are classified asbaseline rate, baseline variability (long-term and short-term), and periodic changes in the rate (accelerationsand decelerations). The nurse must be able to interpretthe various FHR parameters to determine if the patternis reassuring (indicating fetal well-being) or nonreassuring(indicating fetal problems) to care for the woman effec-tively during labor and birth. Table 14-1 summarizesthese patterns.
Baseline FHRBaseline fetal heart rate refers to the average FHRthat occurs during a 10-minute segment that excludesperiodic or episodic rate changes, such as tachycardia or
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 343
ElectrodeScalp
Internal fetalmonitor
Intrauterinepressurecatheter
l Figure 14-8 Continuous internal EFM.
Table 14-1
Sources: Moses, 2003; Littleton & Engebretson, 2005; Feinstein et al., 2003; Engstrom, 2004; Tucker, 2004.
FHR Pattern
Reassuring FHR signs
Nonreassuring signs
Ominous signs
• Normal baseline (110–160 bpm)
• Moderate bradycardia(100–120 bpm); goodvariability
• Good beat-to-beatvariability and fetalaccelerations
• Fetal tachycardia (>160 bpm)
• Moderate bradycardia(100–110 bpm); lostvariability
• Absent beat-to-beatvariability
• Marked bradycardia(90–100 bpm)
• Moderate variabledecelerations
• Fetal tachycardia with lossof variability
• Prolonged markedbradycardia (<90 bpm)
• Severe variabledecelerations (<70 bpm)
• Persistent latedecelerations
Table 14-1 Interpreting FHR Patterns

bradycardia. It is assessed when the woman has no con-tractions and the fetus is not experiencing episodicFHR changes. The normal baseline FHR ranges between110 and 160 beats per minute (bpm). The normal base-line FHR can be obtained by auscultation, ultrasound,or Doppler, or by a continuous internal direct fetalelectrode.
Fetal bradycardia occurs when the FHR is below110 bpm and lasts 10 minutes or longer. It can be the ini-tial response of a healthy fetus to asphyxia. Causes offetal bradycardia might include fetal hypoxia, prolongedmaternal hypoglycemia, fetal acidosis, administration ofdrugs to the mother, hypothermia, maternal hypoten-sion, prolonged umbilical cord compression, and fetalcongenital heart block (Engstrom, 2004). Bradycardiamay be benign if it is an isolated event, but it is consid-ered an ominous sign when accompanied by a decreasein long-term variability and late decelerations.
Fetal tachycardia is a baseline FHR greater than160 bpm that lasts for 10 minutes or longer. It canrepresent an early compensatory response to asphyxia.Other causes of fetal tachycardia include fetal hypoxia,maternal fever, maternal dehydration, amnionitis, drugs(e.g., cocaine, amphetamines, nicotine), maternal hyper-thyroidism, maternal anxiety, fetal anemia, prematurity,fetal heart failure, and fetal arrhythmias (Ladewig,London, & Davidson, 2006). Fetal tachycardia is con-sidered an ominous sign if it is accompanied by adecrease in variability and late decelerations (Ladewig,London, & Davidson, 2006).
Baseline VariabilityBaseline variability is defined as the fluctuations of theFHR observed along the baseline in the absence of con-tractions, decelerations, and accelerations (Cypher et al.,2003). It represents the interplay between the parasym-pathetic and sympathetic nervous systems. The con-stant interplay (push-and-pull effect) on the FHR fromthe parasympathetic and sympathetic systems produces amoment-to-moment change in the FHR. Because vari-
ability is in essence the combined result of autonomicnervous system branch function, its presence impliesthat the both branches are working and receiving ade-quate oxygen (Feinstein et al., 2003). Thus, variabilityis one of the most important characteristics of the FHR.Two components of baseline variability are described:short-term and long-term.
Short-term variability is the beat-to-beat change inFHR. It represents the variations or fluctuations of thebaseline that, when seen on the fetal monitor tracing,produces the irregularity within the baseline. It can bemeasured by internal monitoring and is classified aseither present or absent. The presence of short-term vari-ability typically indicates a well-oxygenated, nonaci-demic fetus (Murray, 2004). The most practical way todetermine the presence or absence of short-term variabil-ity is visually. The fetal heart tracing line is evaluated forroughness or smoothness. If roughness is present in thebaseline, short-term variability is present; if smoothnessis present, it is absent.
Long-term variability is the waviness or rhythmic fluc-tuations, which are described as cycles per minute. Thefrequency of cycles is 3 to 6 per minute. It is classifiedas absent (<3 bpm), decreased or minimal (3 to 5 bpm),average or moderate (6 to 25 bpm), and marked or saluta-tory (>25 bpm) (Cypher et al., 2003) (Fig. 14-9).
FHR variability is an important clinical indicator thatis predictive of fetal acid–base balance and cerebral tissueperfusion (Baird & Ruth, 2002). As the central nervous sys-tem is desensitized by hypoxia and acidosis, FHR decreasesuntil a smooth baseline pattern appears. Loss of variabilitymay be associated with a poor outcome. Some causes ofdecreased variability include fetal hypoxia/acidosis, drugsthat depress the central nervous system, congenital abnor-malities, fetal sleep, prematurity, and fetal tachycardia(Pillitteri, 2003).
External electronic fetal monitoring is not able toassess short-term variability. Therefore, if external mon-itoring shows a baseline that is smoothing out, use of aninternal spiral electrode should be considered to gain amore accurate picture of the fetal health status.
344 Unit 4 LABOR AND BIRTH
240210180150120906030
100806040200
l Figure 14-9 Long-term variability (average or moderate).

Periodic Baseline ChangesPeriodic baseline changes are temporary, recurrentchanges made in response to a stimulus such as a con-traction. The FHR can demonstrate patterns of accel-eration or deceleration in response to most stimuli. Fetalaccelerations are transitory increases in the FHRabove the baseline associated with sympathetic nervousstimulation. They are visually apparent, with elevations ofFHR of at least 15 bpm above the baseline, and usuallylast longer than 15 seconds but not for longer than 2 min-utes (King & Simpson, 2001). Their appearance providesevidence of fetal well-being and is generally consideredreassuring and requires no interventions. Accelerationsdenote fetal movement and fetal well-being and are thebasis for nonstress testing.
A deceleration is a transient fall in FHR causedby stimulation of the parasympathetic nervous system.Decelerations are described by their shape and associa-tion to a uterine contraction. They are classified as early,late, variable, and prolonged (Fig. 14-10).
Early decelerations are characterized by a gradualdecrease in the FHR in which the nadir (lowest point)occurs at the peak of the contraction. They rarely decreasemore than 30 to 40 bpm below the baseline. Early decel-erations mirror the appearance of the uterine contraction
below it on the fetal tracing. They are most often seen dur-ing the active stage of any normal labor, during pushing,crowning, or vacuum extraction. They are thought to be aresult of fetal head compression that results in a reflexvagal response with a resultant slowing of the FHR duringuterine contractions. Early decelerations are not indicativeof fetal distress and do not require intervention.
Late decelerations are transitory decreases in FHRthat occur after a contraction begins. The FHR does notreturn to baseline levels until well after the contractionhas ended. Delayed timing of the deceleration occurs,with the nadir of the uterine contraction. Late decelera-tions are associated with uteroplacental insufficiency,which occurs when blood flow within the intervillousspace is decreased to the extent that fetal hypoxia exists(McKinney et al., 2005). Conditions that may decreaseuteroplacental perfusion with resultant decelerationsinclude maternal hypotension, gestational hypertension,placental aging secondary to diabetes and postmaturity,hyperstimulation via oxytocin infusion, maternal smok-ing, anemia, and cardiac disease. They imply somedegree of fetal hypoxia. Repetitive late decelerations andlate decelerations with decreasing baseline variability arenonreassuring signs. Box 14-2 highlights interventionsfor decelerations.
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 345
A. Early B. Variable C. Late
Onset Onset RecoveryRecovery Variable onset
Nadir Nadir
NadirAcme Acme Acme
Contraction Contraction Contraction
l Figure 14-10 Decelerations. (A) Early. (B) Variable. (C) Late.

Variable decelerations have an unpredictable shape onthe FHR baseline, possibly demonstrating no consistentrelationship to uterine contractions. The shape of vari-able decelerations may be U, V, or W, or they may notresemble other patterns (Feinstein et al., 2003). Variabledecelerations usually occur abruptly with quick deceler-ation. They are the most common deceleration patternfound in the laboring woman and are usually transientand correctable (Garite, 2002). Variable decelerationsare associated with cord compression. However, theybecome a nonreassuring sign when the FHR decreasesto less than 60 bpm, persists at that level for at least 60seconds, and is repetitive (ICSI, 2003). The pattern ofvariable deceleration consistently related to the contrac-tions with a slow return to FHR baseline is also nonre-assuring.
Prolonged decelerations are abrupt FHR declines of atleast 15 bpm that last longer than 2 minutes but less than10 minutes. The rate usually drops to less than 90 bpm.Many factors are associated with this pattern, includingprolonged cord compression, abruptio placentae, cordprolapse, supine maternal position, vaginal examination,fetal blood sampling, maternal seizures, regional anes-
thesia, or uterine rupture (Mattson & Smith, 2004).Prolonged decelerations can be remedied by identifyingthe underlying cause and correcting it.
Combinations of FHR patterns obtained by elec-tronic fetal monitoring during labor are not infrequent.Nonreassuring patterns are more significant if they aremixed and persist for long periods of time. Other nonre-assuring patterns include prolonged late decelerations,absent or minimal variability, bradycardia or tachycardia,and prolonged variable decelerations lower than 60 bpm.The likelihood of fetal compromise is increased if variousnonreassuring patterns coexist, particularly those associ-ated with decreased baseline variability or abnormal con-traction patterns (ICSI, 2003).
Other Fetal Assessment MethodsIn situations suggesting the possibility of fetal com-promise, such as inconclusive or nonreassuring FHR patterns, further ancillary testing such as fetal scalp sam-pling, fetal pulse oximetry, and fetal stimulation may beused to validate the FHR findings and assist in planninginterventions.
Fetal Scalp SamplingFetal scalp sampling was developed as a means of measur-ing fetal distress in conjunction with electronic fetal mon-itoring to make critical decisions about the management oflabor and to prevent unnecessary operative interventionsresulting from the use of electronic fetal monitoring alone.Nonreassuring FHR patterns may not necessarily indi-cate fetal hypoxia or acidosis. Therefore, assessing fetalacid–base status through fetal scalp sampling may help toprevent needless surgical intervention.
A sample of fetal scalp blood is obtained to measurethe pH. Sampling requires that the woman have rupturedmembranes, cervical dilation of a least 3 to 5 cm, and a ver-tex presentation at −1 station (Torgersen, 2004). Normalfetal blood pH is 7.25 to 7.35. When the fetal scalp pH isbelow 7.15, the majority of neonates will have an Apgarscore of less than 6 (Torgersen, 2004).
During the past decade, the use of fetal scalp samplinghas decreased, being replaced by less invasive techniquesthat yield similar information.
Fetal Oxygen Saturation Monitoring (Fetal Pulse Oximetry)Fetal pulse oximetry measures fetal oxygen saturationdirectly and in real time. It is used with electronic fetalmonitoring as an adjunct method of assessment when theFHR pattern is nonreassuring or inconclusive. Normaloxygen saturation of a healthy fetus is 30% to 70% (Sisk,2002). If the fetal oxygen saturation is reassuring (a trendof >30% between contractions), unnecessary cesareanbirths, invasive procedures such as fetal blood sampling,and operative vaginal births can be minimized (Simpson,
346 Unit 4 LABOR AND BIRTH
If a patient develops a nonreassuring deceleration patternsuch as late or variable decelerations:• Notify the healthcare provider about the pattern and
obtain further orders, making sure to document allinterventions and their effects on the FHR pattern.
• Reduce or discontinue oxytocin as dictated by thefacility’s protocol, if it is being administered.
• Provide reassurance that interventions are being doneto effect a pattern change.
Additional interventions specific for a late decelerationFHR pattern would include:• Turning the client on her left side to increase placental
perfusion• Administering oxygen by mask to increase fetal
oxygenation• Increasing the IV fluid rate to improve intravascular
volume• Assessing client for any underlying contributing causes• Providing reassurance that interventions are to effect
pattern change
Specific interventions for a variable deceleration FHRpattern would include:• Changing the client’s position to relieve compression
on the cord• Providing reassurance that interventions are to effect
pattern change• Giving oxygen and IV fluids as ordered
BOX 14-2INTERVENTIONS FOR NONREASSURING DECELERATIONS

2003). Any reduction in unnecessary interventions dur-ing labor and birth has the potential to improve maternaland fetal outcomes and reduce costs.
Adequate maintenance of fetal oxygenation is neces-sary for fetal well-being. Fetal oxygen saturation moni-toring is used for a singleton term fetus in a vertexpresentation, at a −2 station or below, and with a non-reassuring FHR pattern. In addition, the fetal mem-branes must be ruptured and the cervix dilated at least2 cm (Simpson & Porter, 2001). A soft sensor is intro-duced through the dilated cervix and placed on the cheek,forehead, or temple of the fetus. It is held in place by theuterine wall. The sensor then is attached to a special adap-tor on the fetal monitor that provides a real-time record-ing that is displayed on the uterine activity panel of thetracing. It is a noninvasive, safe, and accurate method forassessing fetal oxygenation.
The fetal pulse oximetry traces along the contractionportion of the monitoring strip, so it is easy to see how thesaturation changes with the contraction. This adjunct testcan help support decisions to allow labor to continue orto intervene surgically. Observing the trend of oxygen sat-uration on the tracing and documenting the values on thelabor flow sheet or other medical record forms is crucial.The physician or midwife must be notified if the fetal oxy-gen saturation becomes nonreassuring (<30% betweencontractions) in conjunction with a nonreassuring FHRpattern. Ongoing communication is needed betweenthe nurse and the primary care provider to enhance thematernal-fetus status.
Fetal StimulationAn indirect method used to evaluate fetal oxygenationand acid–base balance to identify fetal hypoxia is fetalscalp stimulation and vibroacoustic stimulation. If thefetus does not have adequate oxygen reserves, carbondioxide builds up, leading to acidemia and hypoxemia.These metabolic states are reflected in nonreassuringFHR patterns as well as fetal inactivity. Fetal stimulationis performed to promote fetal movement with the hopethat FHR accelerations will accompany the movement.
Fetal movement can be stimulated with a vibroacousticstimulator (artificial larynx) applied to the woman’s lowerabdomen and turned on for a few seconds to producesound and vibration or by tactile stimulation via pelvicexamination and stimulation of the fetal scalp with thegloved fingers. A well-oxygenated fetus will respond whenstimulated (tactile or by noise) by moving in conjunc-tion with an acceleration of 15 bpm above the baselineheart rate that lasts at least 15 seconds. This FHR acceler-ation reflects a pH of more than 7 and a fetus with an intactcentral nervous system. Fetal scalp stimulation is not doneif the fetus is preterm, or if the woman has an intrauterineinfection, a diagnosis of placenta previa (which could leadto hemorrhage), or a fever (which increases the risk of anascending infection) (McKinney et al., 2005).
Comfort Promotion and Pain ManagementPain during labor is a universal experience, althoughthe intensity of the pain may vary. Although labor andchildbirth are viewed as natural processes, both canproduce significant pain and discomfort. The physicalcauses of pain during labor include cervical stretching,hypoxia of the uterine muscle due to a decrease in per-fusion during contractions, pressure on the urethra,bladder, and rectum, and distention of the muscles ofthe pelvic floor (Leonard, 2002). A woman’s pain per-ception can be influenced by her previous experienceswith pain, fatigue, pain anticipation, positive or nega-tive support system, labor and birth environment, cul-tural expectations, and level of emotional stress andanxiety (Hodnett, 2002a).
The techniques used to manage the pain of labor varyaccording to geography and culture. For example, someAppalachian women believe that placing a hatchet or knifeunder the bed of a laboring woman may help “cut thepain of childbirth” and a woman from this backgroundmay wish to do so in the hospital setting (Stephens, 2003).Cherokee, Hmong, and Japanese women will often remainquiet during labor and birth and not complain of painbecause outwardly expressing pain is not appropriate intheir cultures. Never interpret their quietness as freedomfrom pain (Moore & Moos, 2003).
Today, women have many safe nonpharmacologicand pharmacologic choices for the management of painduring labor and birth, which may be used separately orin combination with one another.
Nurses are in an ideal position to provide childbearingwomen with balanced, clear, concise information regardingeffective nonpharmacologic and pharmacologic measuresto relieve pain. Pain management standards issued byJCAHO mandate that pain be assessed in all clients admit-ted to a healthcare facility. Thus, it is important for nursesto be knowledgeable about the most recent scientificresearch on labor pain-relief modalities, to make sure thataccurate and unbiased information about effective pain-relief measures is available to laboring women, to be surethat the woman determines what is an acceptable laborpain level for her, and to allow the woman the choiceof pain-relief method.
Nonpharmacologic MeasuresNonpharmacological measures may include continuouslabor support, hydrotherapy, ambulation and positionchanges, acupuncture and acupressure, attention focus-ing and imagery, therapeutic touch and massage, andbreathing techniques and effleurage. Most of these meth-ods are based on the “gate control” theory of pain, whichproposes that local physical stimulation can interfere with
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 347

pain stimuli by closing a hypothetical gate in the spinalcord, thus blocking pain signals from reaching the brain(Engstrom, 2004). It has long been a standard of care forlabor nurses to first provide or encourage a variety of non-pharmacologic measures before moving to the pharma-cologic interventions.
Nonpharmacologic measures are usually simple, safe,and inexpensive to use. Many of these measures are taughtin childbirth classes, and women should be encouraged totry a variety of methods prior to the real labor. Many of themeasures need to be practiced for best results and coordi-nated with the partner/coach. The nurse provides supportand encouragement for the woman and her partner usingnonpharmacologic methods. Although women can’t con-sciously direct the contractions occurring during labor, theycan control how they respond to them, thereby enhancingtheir feelings of control.
Continuous Labor SupportContinuous labor support involves offering a sustained pres-ence to the laboring woman by providing emotional sup-port, comfort measures, advocacy, information and advice,and support for the partner (Trainor, 2002). This con-tinuous presence can be provided by a woman’s family,a midwife, a nurse, a doula, or anyone else close to thewoman. A support person can assist the woman to ambu-late, reposition herself, and use breathing techniques. Asupport person can also aid with the use of acupressure,massage, music therapy, or therapeutic touch. During thenatural course of childbirth, a laboring woman’s func-tional ability is limited secondary to pain, and she oftenhas trouble making decisions. The support person canhelp make them based on his or her knowledge of thewoman’s birth plan and personal wishes.
Research has validated the value of continuous laborsupport versus intermittent support in terms of loweroperative deliveries, cesarean births, and requests forpain medication (Hodnett, 2002b; Hunter, 2002). Thehuman presence is of immeasurable value to make thelaboring woman feel secure.
HydrotherapyHydrotherapy is a nonpharmacologic measure in which thewoman immerses herself in warm water for relaxation andrelief of discomfort. Upon entering the warm water, thewarmth and buoyancy help to release muscle tension andcan impart a sense of well-being (Primeau et al., 2003).Warm water provides soothing stimulation of nerves in theskin, promoting vasodilatation, reversal of sympathetic ner-vous response, and a reduction in catecholamines (Leemanet al., 2003a). Contractions are usually less painful in warmwater because the warmth and buoyancy of the water havea relaxing effect.
There are a wide range of hydrotherapy optionsavailable, from ordinary bathtubs to whirlpool bathsand showers, combined with low lighting and music.
Many hospitals provide showers and whirlpool baths forlaboring women for pain relief. However, hydrotherapyis more commonly practiced in birthing centers man-aged by midwives. The recommendation for initiatinghydrotherapy is that that women be in active labor (>5 cmdilated) to prevent the slowing of labor contractions sec-ondary to muscular relaxation. The woman’s membranescan be intact or ruptured. Women are encouraged to stayin the bath or shower as long as they feel they are comfort-able. The water temperature should not exceed bodytemperature, and the bath time typically is limited to 1 to2 hours (Simkin & O’Hara, 2002).
Hydrotherapy is an effective pain-management optionfor many women. Women who are experiencing a healthypregnancy can be offered this option, but the poten-tial benefits or risks to the woman are still not known(Campbell, 2004).
Ambulation and Position ChangesAmbulation and position changes during labor are anotherextremely useful comfort measure. Historically, womenadopted a variety of positions during labor, rarely usingthe recumbent position until recently. The medical pro-fession has favored recumbent positions during labor,but without evidence to demonstrate their appropriate-ness (Chalk, 2004).
Changing position frequently (every 30 minutes orso)—sitting, walking, kneeling, standing, lying down,getting on hands and knees, and using a birthing ball—helps relieve pain (Fig. 14-11). Position changes alsomay help to speed labor by adding benefits of gravityand changes to the shape of the pelvis. Research reportsthat position and frequency of position change have aprofound effect on uterine activity and efficiency. Allowingthe woman to obtain a position of comfort frequentlyfacilitates a favorable fetal rotation by altering the align-ment of the presenting part with the pelvis. As the mothercontinues to change position based on comfort, the opti-mal presentation is afforded (Gilbert & Harmon, 2003).Supine and sitting positions should be avoided, since theymay interfere with labor progress and can cause com-pression of the vena cava and decrease blood return tothe heart.
Swaying from side to side, rocking, or other rhythmicmovements may also be comforting. If labor is progressingslowly, ambulating may speed it up again. Upright posi-tions such as walking, kneeling forward, or doing the lungeon the birthing ball give most women a greater sense of con-trol and active movement than just lying down. Table 14-2 highlights some of the more common positions thatcan be used during labor and birth.
Acupuncture and AcupressureAcupuncture and acupressure can be used to bring aboutpain relief during labor. Although controlled researchstudies of these methods are limited, there is adequate evi-
348 Unit 4 LABOR AND BIRTH

dence that both are useful in relieving pain associated withlabor and birth. However, both methods require a trained,certified clinician, and such a person is not available inmany birth facilities (Skilnand et al., 2002).
Acupuncture involves stimulating key trigger pointswith needles. This form of Chinese medicine has beenpracticed for approximately 3,000 years. Classical Chineseteaching holds that throughout the body there are meridi-ans or channels of energy (qi) that when in balance regulatebody functions. Pain reflects an imbalance or obstructionof the flow of energy. The purpose of acupuncture isto restore qi, thus diminishing pain (Eappen & Robbins,
2002). Stimulating the trigger points causes the releaseof endorphins, reducing the perception of pain.
Acupressure involves the application of a firm finger or massage at the same trigger points to reducethe pain sensation. The amount of pressure is import-ant. The intensity of the pressure is determined by theneeds of the woman. Holding and squeezing the handof a woman in labor may trigger the point most com-monly used for both techniques (Engstrom, 2004).Some acupressure points are found along the spine,neck, shoulder, toes, and soles of the feet (Lowdermilk &Perry, 2004).
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 349
C D
A B
l Figure 14-11 Various positions for use during labor. (A) Ambulation. (B) Leaning forward.(C) Sitting in a chair. (D) Using a birthing ball.

350 Unit 4 LABOR AND BIRTH
Table 14-2
Standing
Walking
Standing and leaning forward on partner, bed,birthing ball
Slow dancing (standing with woman’s arms aroundpartner’s neck, head resting on his chest orshoulder, with his hands rubbing your lower back;sway to music and breathe in rhythm if it helps)
The lunge (standing facing a straight chair with onefoot on the seat with knee and foot to the side;bending raised knee and hip, and lungingsideways repeatedly during a contraction, holdingeach lunge for 5 seconds; partner holds chair andhelps with balance)
Sitting upright
Sitting on toilet or commode
Semi-sitting (setting the head of the bed at a 45-degreeangle with pillows used for support)
Rocking in a chair
Sitting, leaning forward with support
On all fours, on your hands and knees
Kneeling, leaning forward with support on a chair seat,the raised head of the bed, or on a birthing ball
Side-lying
• Takes advantage of gravity during and betweencontractions
• Makes contractions feel less painful and be moreproductive
• Helps fetus line up with angle of maternal pelvis• Helps to increase urge to push in second stage
of labor
• Has the same advantages as standing• Causes changes in the pelvic joints, helping the
fetus move through the birth canal
• Has the same advantages as standing• Is a good position for a backrub• May feel more restful than standing• Can be used with electronic fetal monitor
• Has the same advantages as walking• Back pressure helps relieve back pain• Rhythm and music help you relax and provide comfort
• Widens one side of the pelvis (the side toward lunge)• Encourages rotation of baby• Can also be done in a kneeling position
• Helps promote rest• Has more gravity advantage than lying down• Can be used with electronic fetal monitor
• Has the same advantages as sitting upright• May help relax the perineum for effective
bearing down
• Has the same advantages as sitting upright• Is an easy position if on a bed
• Has the same advantages as sitting upright• May help speed labor (rocking movement)
• Has the same advantages as sitting upright• Is a good position for back rubbing
• Helps relieve backache• Assists rotation of baby in posterior position• Allows for pelvic rocking and body movement• Relieves pressure on hemorrhoids• Allows for vaginal exams• Is sometimes preferred as a pushing position by
women with back labor
• Has the same advantages as all-fours position• Puts less strain on wrists and hands
• Is a very good position for resting and convenientfor many kinds of medical interventions
• Helps lower elevated blood pressure• May promote progress of labor when alternated
with walking• Is useful to slow a very rapid second stage• Takes pressure off hemorrhoids• Facilitates relaxation between contractions
Table 14-2 Common Positions for Use During Labor and Birth

Attention Focusing and ImageryAttention focusing and imagery uses many of the senses andthe mind to focus on stimuli. The woman can focus on tac-tile stimuli such as touch, massage, or stroking. She mayfocus on auditory stimuli such as music, humming, or ver-bal encouragement. Visual stimuli might be any object inthe room, or the woman can imagine the beach, a moun-taintop, a happy memory, or even the contractions of theuterine muscle pulling the cervix open and the fetuspressing downward to open the cervix. Some womenfocus on a particular mental activity such as a song, achant, counting backwards, or a Bible verse. Breathing,relaxation, positive thinking, and positive visualizationwork well for mothers in labor. The use of these techniqueskeeps the sensory input perceived during the contractionfrom reaching the pain center in the cortex of the brain(Simkin, 2002).
Therapeutic Touch and MassageTherapeutic touch and massage use the sense of touch to pro-mote relaxation and pain relief. Massage works as a formof pain relief by increasing the production of endorphins inthe body. Endorphins reduce the transmission of signalsbetween nerve cells and thus lower the perception of pain(Duddridge, 2002). In addition, touching and massageoffer the woman a distraction from discomfort.
Therapeutic touch is based on the premises that thebody contains energy fields that lead to either good or illhealth and that the hands can be used to redirect the energyfields that lead to pain (Engstrom, 2004). To be done cor-
rectly, this technique must be learned and practiced. Somewomen prefer a light touch, while others find a firmer touchmore soothing. Massage of the neck, shoulders, back,thighs, feet, and hands can be very comforting. The useof firm counterpressure in the lower back or sacrum isespecially helpful for back pain during contractions (Fig.14-12). Contraindications for massage include skin rashes,varicose veins, bruises, or infections (Leonard, 2002).
Effleurage is a light, stroking, superficial touch of theabdomen, in rhythm with breathing during contractions.It is used as a relaxation and distraction technique fromdiscomfort. The external fetal monitor belts may interferewith her ability to accomplish this.
Breathing TechniquesBreathing techniques are effective in producing relaxationand pain relief through the use of distraction. If the womanis concentrating on slow-paced rhythmic breathing, sheisn’t likely to fully focus on contraction pain. Breathingtechniques are often taught in childbirth education classes(see Chapter 12 for additional information).
Breathing techniques use controlled breathing toreduce the pain experienced through a stimulus-responseconditioning. The woman selects a focal point within herenvironment to stare at during the first sign of a contrac-tion. This focus creates a visual stimulus that goes directlyto her brain. The woman takes a deep cleansing breath,which is followed by rhythmic breathing. Verbal com-mands from her partner supply an ongoing auditory stim-ulus to her brain. Effleurage can be combined with the
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 351
Table 14-2
Squatting
Supported squat (leaning back against partner, whosupports woman under the arms and takes theentire woman’s weight; standing up betweencontractions)
Dangle (partner sitting high on bed or counter withfeet supported on chairs or footrests and thighsspread; woman leaning back between partner’slegs, placing flexed arms over partner’s thighs;partner gripping sides with his thighs; womanlowering herself and allowing partner to support herfull weight; standing up between contractions)
• May relieve backache• Takes advantage of gravity• Requires less bearing-down effort• Widens pelvic outlet• May help fetus turn and move down in a difficult
birth• Helps if the woman feels no urge to push• Allows freedom to shift weight for comfort• Offers an advantage when pushing, since upper
trunk presses on the top of the uterus
• Requires great strength in partner• Lengthens trunk, allowing more room for fetus to
maneuver into position• Lets gravity help
• Has the same advantages of a supported squat• Requires less physical strength from the partner
Table 14-2 Common Positions for Use During Labor and Birth (continued)
Sources: Simkin, 2002; Simkin, 2003; Simkin & Ancheta, 2000; McKinney et al., 2005.

breathing to provide a tactile stimulus, all blocking painsensations to her brain.
There are five levels of breathing a woman can usedepending on the intensity of each contraction:
• First level: slow chest breathing involves 6 to 12 full res-pirations per minute; used in early labor; starting off andending with a cleansing breath, which is taking a largevolume of air into the lungs and letting it out slowly
• Second level: breathing heavy enough to expand the ribcage but light enough so the diaphragm barely moves;rate can be up to 40 breaths per minute; used duringlabor when cervical dilation is 4 to 6 cm
• Third level: shallow, sternal breathing, usually at a rateof 50 to 70 breaths per minute; used during transitionphase of labor
• Fourth level: pant-blow pattern of breathing involvestaking three to four quick breaths in and out and thenforcefully exhaling
• Fifth level: continuous chest panting involves taking shal-low breaths at a rate of about 60 breaths per minute; usedduring strong contractions to prevent pushing too early
The last two levels of breathing patterns are usedwhen the previous level is no longer effective. The levelsprogress with the discomfort of the contractions.
Pharmacologic MeasuresWith varying degrees of success, generations of womenhave sought ways to relieve the pain of childbirth. Pharma-
cologic pain relief during labor includes systemic analgesiaand regional or local anesthesia. Women have seen dra-matic changes in pharmacologic pain management optionsover the years. Methods have evolved from biting down ona stick to a more complex pharmacologic approach suchas epidural/intrathecal analgesia. Systemic analgesia andregional analgesia/anesthesia have become less common,while the use of newer neuraxial analgesia/anesthesia tech-niques involving minimal motor blockade have becomemore popular. Neuraxial analgesia/anesthesia isthe administration of analgesic (opioids) or anesthetic(medication capable of producing a loss of sensation in an area of the body) agents, either continuously orintermittently, into the epidural or intrathecal space torelieve pain (Poole, 2003a). Low-dose and ultra-low-dose epidural analgesia, spinal analgesia, and combinedspinal-epidural analgesia have replaced the once “tradi-tional” epidural for labor (Poole, 2003).
The shift in pain management allows a woman to bean active participant during labor. Regardless of whichapproach is used during labor, the woman has the rightto choose the methods of pain control that will best suither and meet her needs.
Systemic AnalgesiaSystemic analgesia involves the use of one or more drugsadministered orally, intramuscularly, or intravenously thatbecome distributed throughout the body via the circula-tory system. Depending on which administration routineis used, the therapeutic effect of pain relief can occurwithin minutes and last for several hours. The most impor-tant complication associated with the use of this classof drugs is respiratory depression. Therefore, women giventhese drugs require careful monitoring. Opioids givenclose to the time of birth can cause central nervous systemdepression in the newborn, necessitating the administra-tion of naloxone (Narcan) to reverse the depressant effectsof the opioids.
Several drug categories may be used for systemicanalgesia:
• Ataractics: such as hydroxyzine (Vistaril) or promet-hazine (Phenergan)
• Barbiturates: such as secobarbital (Seconal) or pento-barbital (Nembutal)
• Benzodiazepines: such as diazepam (Valium) or mida-zolam (Versed)
• Opioids: such as butorphanol (Stadol), nalbuphine(Nubain), meperidine (Demerol), or fentanyl (Sub-limaze)
Drug Guide 14-1 highlights some of the major drugsused for systemic analgesia.
Systemic analgesics are typically administered par-enterally, usually through an existing intravenous (IV)line. Nearly all medications given during labor cross theplacenta and have a depressant effect on the fetus; there-
352 Unit 4 LABOR AND BIRTH
l Figure 14-12 Nurse massaging the client’sback during a contraction while she ambulatesduring labor.

fore, it is important for the woman to receive the leastamount of systemic medication as possible to relieve herdiscomfort so that it does not cause any harm to the fetus(Florence & Palmer, 2003). Historically opioids havebeen administered by nurses, but in the past decade therehas been increasing use of client-controlled intravenousanalgesia (patient-controlled analgesia [PCA]). With thissystem, the woman is given a button connected to a com-puterized pump on the IV line. When the woman desiresanalgesia, she presses the button and the pump delivers a
preset amount of medication. This system provides thewoman with a sense of control over her own pain man-agement and active participation in the childbirth process.
AtaracticsThe ataractic group of medications is used in combinationwith an opioid to decrease nausea and vomiting and lessenanxiety. These adjunct drugs help potentiate the effective-ness of the opioid so that a lesser dose can be given. Theymay also be used to increase sedation. Promethazine
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 353
Drug Guide 14-1
Sources: Primeau, Lacey, & Crotty, 2003; Poole, 2003b; Florence & Palmer, 2003; Pitter &Preston, 2001; Spratto & Woods, 2004; Mahlmeister, 2003.
Type Drug Comments
Opioids
Ataractics
Benzodiazepines
Barbiturates
Morphine2–5 mg IV
Meperidine (Demerol)25–50 mg IV
Butorphanol (Stadol)1 mg IV q 3–4h
Nalbuphine (Nubain)10 mg IV
Fentanyl (Sublimaze)25–50 mcg IV
Hydroxyzine (Vistaril)50 mg IM
Promethazine (Phenergan)25 mg IV
Diazepam (Valium)2–5 mg IV
Midazolam (Versed)1–5 mg IV
Secobarbital (Seconal)100 mg PO/IM
Pentobarbital (Nembutal)100 mg PO/IM
May be given IV, intrathecally, or epidurallyRapidly crosses the placentaCan cause maternal and neonatal CNS depressionDecreases uterine contractions
May be given IV or epidurally with maximal fetal uptake 2–3 hoursafter administration
Can cause CNS depressionDecreases fetal variability
Is given IVIs rapidly transferred across the placentaCauses neonatal respiratory depression
Is given IVCauses less maternal nausea and vomitingCauses decreased FHR variability, fetal bradycardia and
respiratory depression
Is given IV or epidurallyCan cause maternal hypotension, maternal and fetal
respiratory depressionRapidly crosses placenta
Does not relieve pain but reduces anxiety and potentiatesopioid analgesic effects
Is used to decrease nausea and vomiting
Is used for antiemetic effect when combined with opioidsCauses sedation and reduces apprehensionMay contribute to maternal hypotension and neonatal
depression
Is given to enhance pain relief of opioid and cause sedationMay be used to stop eclamptic seizuresDecreases nausea and vomitingCan cause newborn depression; therefore, lowest possible dose
should be used
Is not used for analgesic but amnesia effectIs used as adjunct for anesthesiaIs excreted in breast milk
Causes sedationIs used in very early labor to alter a dysfunctional patternIs not used for pain relief in active laborCrosses placenta and is secreted in breast milk
Drug Guide 14-1 Common Agents Used for Systemic Analgesia

(Phenergan) can be given IV, but hydroxyzine (Vistaril)must be given by mouth or by intramuscular injection intoa large muscle mass. Neither drug affects the progress oflabor, but either may cause a decrease in FHR variabilityand possible newborn depression (Poole, 2003b).
BarbituratesThe barbiturate drug group is used only in early labor orin a prolonged latent phase that produces enough discom-fort that the woman cannot sleep. Barbiturates are givenorally or intramuscularly to produce a light sleep to altera dysfunctional labor pattern or to calm a very anxiouswoman in early labor. The goal in giving a barbiturate is topromote therapeutic rest for a few hours to enhance thewoman’s ability to cope with active labor. These drugscross the placenta and cause central nervous system depres-sion in the newborn (Poole, 2003a).
BenzodiazepinesBenzodiazepines are used for minor tranquilizing andsedative effects. Diazepam (Valium) also is given IV tostop seizures due to pregnancy-induced hypertension.However, it is not used during labor itself. It can be admin-istered to calm a woman who is out of control, therebyenabling her to relax enough so that she can participateeffectively during her labor process rather than fightingagainst it. Lorazepam (Ativan) can also be used for its tran-quilizing effect, but increased sedation is experienced withthis medication (Bricker & Lavender, 2002). Midazolam(Versed), also given IV, produces good amnesia but noanalgesia. It is most commonly used as an adjunct for anes-thesia. Diazepam and midazolam cause central nervoussystem depression for both the woman and the newborn.
OpioidsOpioids are morphine-like medications that are most effec-tive for the relief of moderate to severe pain. Opioids typi-cally are administered IV. Of all of the synthetic opioids(butorphanol [Stadol], nalbuphine [Nubain], fentanyl[Sublimaze], and meperidine [Demerol]), meperidine isthe most commonly used opioid for the management of pain during labor. Opioids are associated with new-born respiratory depression, decreased alertness, inhib-ited sucking, and a delay in effective feeding (Leeman et al.,2003b).
Opioids decrease the transmission of pain impulses bybinding to receptor site pathways that transmit the painsignals to the brain. The effect is increased tolerance topain and respiratory depression related to a decrease insensitivity to carbon dioxide (Skidmore-Roth, 2004).
All opioids are considered good analgesics. However,respiratory depression can occur in the mother and fetusdepending on the dose given. They may also cause adecrease in FHR variability identified on the fetal monitorstrip. This FHR pattern change is usually transient. Othersystemic side effects include nausea, vomiting, pruritus,
delayed gastric emptying, drowsiness, hypoventilation,and newborn depression. To reduce the incidence of new-born depression, birth should occur within 1 hour or after4 hours of administration to prevent the fetus from receiv-ing the peak concentration (Poole, 2003b).
Opioid antagonists such as naloxone (Narcan) aregiven to reverse the effects of the central nervous systemdepression, including respiratory depression, caused byopioids. Opioid antagonists also are used to reverse theside effects of neuraxial opioids, such as pruritus, urinaryretention, nausea, and vomiting, without significantlydecreasing analgesia (Poole, 2003b).
Consult a current drug guide for more specifics onthese drug categories.
Regional Analgesia/AnesthesiaRegional analgesia/anesthesia provides pain relief withoutloss of consciousness. It involves the use of local anes-thetic agents, with or without added opioids, to bringabout pain relief or numbness through the drug’s effectson the spinal cord and nerve roots. Obstetric regionalanalgesia generally refers to a partial or complete loss ofpain sensation below the T8 to T10 level of the spinalcord (ACOG, 2002).
The routes for regional pain relief include epiduralblock, combined spinal-epidural block, local infiltration,pudendal block, and intrathecal (spinal) analgesia/anes-thesia. Local and pudendal routes are used during birthfor episiotomies; epidural and intrathecal routes are usedfor pain relief during active labor and birth. The majoradvantage of regional pain-management techniques is thatthe woman can participate in the birthing process andstill have good pain control.
Epidural BlockApproximately 60% of laboring women in the UnitedStates receive an epidural block for pain relief duringlabor. In urban areas, many hospitals approach 90% useof epidurals (Eltzschig et al., 2003).
An epidural block involves the injection of a drug intothe epidural space, which is located outside the dura materbetween the dura and the spinal canal. The epidural spaceis typically entered through the third and fourth lumbarvertebrae with a needle, and a catheter is threaded into theepidural space. The needle is removed and the catheter isleft in place to allow for continuous infusion or intermit-tent injections of medicine (Fig. 14-13). An epidural blockprovides analgesia and anesthesia and can be used for bothvaginal and cesarean births. It has evolved from a regionalblock producing total loss of sensation to analgesia withminimal blockade. The effectiveness of epidural analgesiadepends on the technique and medications used. It is usu-ally started after labor is well established, typically whencervical dilation is greater than 5 cm.
Theoretically, epidural local anesthetics could block100 percent of labor pain if used in large volumes and high
354 Unit 4 LABOR AND BIRTH

concentrations. However, pain relief is balanced againstother goals such as walking during the first stage of labor,pushing effectively in the second stage, and minimizingmaternal and fetal side effects.
An epidural is contraindicated for women with a pre-vious history of spinal surgery or spinal abnormalities,coagulation defects, infections, and hypovolemia. It alsois contraindicated for the woman who is receiving anti-coagulation therapy.
Complications include nausea and vomiting, hypo-tension, fever, pruritus, intravascular injection, and res-piratory depression. Effects on the fetus during laborinclude fetal distress secondary to maternal hypotension(Mayberry et al., 2002). Ensuring that the woman avoids asupine position after an epidural catheter has been placedwill help to minimize hypotension.
Changes in epidural drugs and techniques have beenmade to optimize pain control while minimizing sideeffects. Today most women receive a continuous lumbarepidural infusion of a local anesthetic, typically a drugwhose name ends in “caine,” and an opioid. To decreasemotor blockade, bupivacaine (Sensorcaine) and ropiva-caine (Naropin) have replaced lidocaine (Xylocaine),and drug concentrations have been lowered (Caton et al.,2002).
The addition of opioids, such as fentanyl or mor-phine, to the local anesthetic helps decrease the amountof motor block obtained. Continuous infusion pumps areused to administer the epidural analgesia, allowing thewoman to be in control and administer a bolus dose ondemand (Mitchell, 2002).
Combined Spinal-Epidural AnalgesiaAnother epidural technique is combined spinal-epidural(CSE) analgesia. This technique involves inserting theepidural needle into the epidural space and subsequentlyinserting a small-gauge spinal needle through the epiduralneedle into the subarachnoid space. An opioid, without alocal anesthetic, is injected into this space. The spinal nee-dle is then removed and an epidural catheter is insertedfor later use.
CSE is advantageous because of its rapid onset of painrelief (within 3 to 5 minutes) that can last up to 3 hours. Italso allows the woman’s motor function to remain active.Her ability to bear down during the second stage of laboris preserved because the pushing reflex is not lost, and hermotor power remains intact. The CSE technique providesgreater flexibility and reliability for labor than eitherspinal or epidural analgesia alone (Landau, 2002). Whencompared with traditional epidural or spinal analgesia,which often keeps the woman lying in bed, CSE allowsher to ambulate (“walking epidural”) (Leeman et al.,2003b). Ambulating during labor provides several ben-efits: it may help control pain better, shorten the firststage of labor, increase the intensity of the contractions,and decrease the possibility of an operative vaginal orcesarean birth.
Although women can walk with CSE, they oftenchoose not to because of sedation and fatigue. Oftenhealthcare providers don’t encourage or assist womento ambulate for fear of injury (Mayberry et al., 2002).Currently, anesthesiologists are performing walking epidu-rals using continuous infusion techniques as well as CSE
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 355
Dura mater
Needleremoved
Catheter remains
Spinous process
Skin
Epidural space
A B
l Figure 14-13 Epidural catheter insertion. (A) A needle is inserted into the epiduralspace. (B) A Catheter is threaded into the epidural space; the needle is then removed. Thecatheter allows medication to be administered intermittently or continuously to relieve painduring labor and childbirth.

and patient-controlled epidural analgesia (PCEA) (Pitter& Preston, 2001).
Complications include maternal hypotension, intra-vascular injection, accidental intrathecal blockade, post-dural puncture headache, inadequate or failed block, andpruritus. Hypotension and associated FHR changes aremanaged with maternal positioning (semi-Fowler’s posi-tion), intravenous hydration, and supplemental oxygen(Lieberman & O’Donoghue, 2002).
Patient-Controlled Epidural AnalgesiaPatient-controlled epidural analgesia (PCEA) involvesthe use of an indwelling epidural catheter with an infu-sion of medication and a programmed pump that allowsthe woman to control the dosing. This method allows thewoman to have a sense of control over her pain and reachher own individually acceptable analgesia level. Whencompared with the traditional epidural analgesia, PCEAprovides equivalent analgesia with lower anesthetic use,lower rates of supplementation, and higher client satis-faction (Paech, 2000).
With PCEA, the woman uses a hand-held deviceconnected to an analgesic agent that is attached to anepidural catheter (Fig. 14-14). When she pushes the but-ton, a bolus dose of agent is administered via the catheterto reduce her pain. This method allows her to manageher pain at will without having to ask a staff member toprovide pain relief.
Local InfiltrationLocal infiltration involves the injection of a local anes-thetic, such as lidocaine, into the superficial perinealnerves to numb the perineal area. This technique is doneby the physician or midwife just before performing anepisiotomy (surgical incision into the perineum to facil-itate birth) or suturing a laceration. Local infiltrationdoes not alter the pain of uterine contractions, but it doesnumb the immediate area of the episiotomy or laceration.Local infiltration does not cause side effects for the womanor her newborn.
Pudendal Nerve BlockA pudendal nerve block refers to the injection of a localanesthetic agent (e.g., bupivacaine, ropivacaine) into thepudendal nerves near each ischial spine. It provides painrelief in the lower vagina, vulva, and perineum (Fig. 14-15).
A pudendal block is used for the second stage oflabor, an episiotomy, or an operative vaginal birth withoutlet forceps or vacuum extractor. It must be adminis-tered about 15 minutes before it would be needed toensure its full effect. A transvaginal approach is gener-ally used to inject an anesthetic agent at or near thepudendal nerve branch. Neither maternal nor fetal com-plications are common.
Spinal (Intrathecal) Analgesia/AnesthesiaThe spinal (intrathecal) pain-management techniqueinvolves injection of an anesthetic “caine” agent, with orwithout opioids, into the subarachnoid space to providepain relief during labor or cesarean birth. The contra-indications are similar to those for the epidural block.Adverse reactions for the woman include hypotensionand spinal headache.
The subarachnoid injection of opioids alone, a tech-nique termed intrathecal narcotics, has been gaining popu-larity since it was introduced in the 1980s. A narcotic isinjected into the subarachnoid space, providing rapid painrelief while still maintaining motor function and sensa-tion (Breslin & Lucas, 2003). An intrathecal narcotic is given during the active phase (>5 cm dilation) of labor.Compared with epidural blocks, intrathecal narcotics areeasy to administer, provide rapid-onset pain relief, are lesslikely to cause newborn respiratory depression, and do notcause motor blockade (Fontaine et al., 2002). Althoughpain relief is rapid with this technique, it is limited by thenarcotic’s duration of action, which may be only a fewhours and not last through the labor. Additional pain mea-sures may be needed to sustain pain management.
356 Unit 4 LABOR AND BIRTH
l Figure 14-14 Using a PCEA pump. Herethe client holds the button that delivers a doseof medication. l Figure 14-15 Pudendal nerve block.

General AnesthesiaGeneral anesthesia is typically reserved for emergencycesarean births when there is not enough time to providespinal or epidural anesthesia or if the woman has a con-traindication to the use of regional anesthesia. It canbe started quickly and causes a rapid loss of consciousness.General anesthesia can be administered by IV injection,inhalation of anesthetic agents, or both. Commonly,thiopental, a short-acting barbiturate, is given IV to pro-duce unconsciousness. This is followed by administra-tion of a muscle relaxant. After the woman is intubated,nitrous oxide and oxygen are administered. A volatilehalogenated agent may also be administered to produceamnesia (Hawkins et al., 2002).
All anesthetic agents cross the placenta and affectthe fetus. The primary complication with general anes-thesia is fetal depression, along with uterine relaxationand potential maternal vomiting and aspiration.
Although the anesthesiologist or nurse anesthetistadministers the various general anesthesia agents, thenurse needs to be knowledgeable about the pharmaco-logic aspects of the drugs used and must be aware of air-way management. Ensure that the woman is NPO andhas a patent IV. In addition, administer a non-particulate(clear) oral antacid (e.g., Bicitra or sodium citrate) or aproton pump inhibitor (Protonix) as ordered to reduce gas-tric acidity. Assist with placement of a wedge under thewoman’s right hip to displace the gravid uterus and preventvena cava compression in the supine position. Once thenewborn has been removed from the uterus, assist theperinatal team in providing supportive care.
Nursing Management During Labor and BirthA major focus of care for the woman during labor andbirth is maintaining control over her pain, emotions, andactions while being an active participant. Nurses can helpand support women to be actively involved in their child-birth experience by allowing time for discussion, offeringcompanionship, listening to worries and concerns, payingattention to the woman’s emotional needs, and activelyhelping and offering information to assist in her under-standing of what is happening in each stage of labor.
Nursing Management During the First Stage of LaborDepending on how far advanced the woman’s labor iswhen she arrives at the facility, the nurse will determineassessment parameters of maternal-fetal status and plancare accordingly. The nurse will provide high-touch, low-tech supportive nursing care during the first stage of laborwhen admitting the woman and orienting her to the laborand birth suite. Nursing care during this stage will includetaking an admission history (reviewing the prenatal record);
checking the results of routine laboratory tests and any spe-cial tests such as chorionic villi sampling, amniocentesis,genetic studies, and biophysical profile done during preg-nancy; asking the woman about her childbirth preparation(birth plan, classes taken, coping skills); and completing aphysical assessment of the woman to establish a baseline ofvalues for future comparison.
Key nursing interventions include:
• Identifying the estimated date of birth from the clientand the prenatal chart
• Validating the client’s prenatal history to determinefetal risk status
• Determining fundal height to validate dates and fetalgrowth
• Performing Leopold’s maneuvers to determine fetalposition, lie, and presentation
• Checking FHR• Performing a vaginal examination (as appropriate) to
evaluate effacement and dilation progress• Instructing the client and her partner about monitoring
techniques and equipment• Assessing fetal response and FHR to contractions and
recovery time• Interpreting fetal monitoring strips to provide optimal
fetal care• Checking FHR baseline for accelerations, variability,
and decelerations• Repositioning the client to obtain optimal FHR pattern• Recognizing FHR problems and initiating corrective
measures• Checking amniotic fluid for meconium staining, odor,
and amount• Comforting client throughout testing period and labor• Supporting client’s decisions regarding intervention or
avoidance of intervention• Assessing client’s support system and coping status
frequently
In addition to these interventions to promote the opti-mal outcome for the mother and fetus, the nurse must doc-ument care accurately and in a timely fashion (Fig. 14-16).Accurate and timely documentation helps to decrease pro-fessional liability exposure and minimize the risk of pre-ventable injuries to women and infants during labor andbirth (Simpson & Knox, 2003). Guidelines for recordingcare include documenting:
• All care rendered, to prove that standards were met• Conversations with all providers, including notifica-
tion times• Nursing interventions before and after notifying provider• Use of the chain of command and response at each level• All flow sheets and forms, to validate care given• All education given to client and response to it• Facts, not personal opinions• Initial nursing assessment, all encounters, and dis-
charge plan
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 357

• All telephone conversations (Greenwald & Mondor,2003)
This standard of documentation is needed to preventlitigation, which is prevalent in the childbirth arena.
AssessmentAfter the admission assessment (see discussion earlier inthe chapter) is complete, assessment continues for changesthat would indicate that labor is progressing as expected.Assess the woman’s knowledge, experience, and expec-tations of labor. Typically, blood pressure, pulse, and res-pirations are assessed every hour during the latent phaseof labor unless the clinical situation dictates that vitalsigns be taken more frequently. During the active andtransition phases, they are assessed every 30 minutes.The temperature is taken every 4 hours throughout thefirst stage of labor unless the clinical situation dictates itmore frequently (maternal fever).
Vaginal examinations are performed periodically totrack labor progress. This assessment information needsto be shared with the woman to reinforce that she is mak-ing progress toward the goal of birth. Uterine contractionsare monitored for frequency, duration, and intensity every30 to 60 minutes during the latent phase, every 15 to30 minutes during the active phase, and every 15 minutesduring transition. Note the changes in the character of thecontractions as labor progresses, and inform the womanof her progress. Continually determine the woman’s levelof pain and her ability to cope and use relaxation tech-niques effectively.
When the fetal membranes rupture, spontaneously orartificially, assess the FHR and check the amniotic fluid forcolor, odor, and amount. Assess the FHR intermittently orcontinuously via electronic monitoring. During the latentphase of labor, assess the FHR every 30 to 60 minutes; inthe active phase, assess FHR at least every 15 to 30 min-utes. Also, be sure to assess the FHR before ambulation,prior to any procedure, and prior to administering analge-
sia or anesthesia to the mother. Table 14-3 summarizesassessments for the first stage of labor.
Nursing InterventionsNursing interventions during the admission process shouldinclude:
• Asking about the client’s expectations of the birthingprocess
• Providing information about labor, birth, pain-management options, and relaxation techniques
• Presenting information about fetal monitoring equipmentand the procedures needed
• Monitoring FHR and identifying patterns that needfurther intervention
• Monitoring the mother’s vital signs to obtain a baselinefor later comparison
• Reassuring the client that her labor progress will bemonitored closely and nursing care will focus on ensur-ing fetal and maternal well-being throughout
As the woman progresses through the first stage oflabor, nursing interventions include:
• Encouraging the woman’s partner to participate• Keeping the woman and her partner up to date on the
progress of the labor• Orienting the woman and her partner to the labor and
birth unit and explaining all of the birthing procedures• Providing clear fluids (e.g., ice chips) as needed or
requested• Maintaining the woman’s parenteral fluid intake at the
prescribed rate if she has an IV• Initiating or encouraging comfort measures, such as
back rubs, cool cloths to the forehead, frequent positionchanges, ambulation, showers, slow dancing, leaningover a birth ball, side-lying, or counterpressure on lowerback (Teaching Guidelines 14-1)
• Encouraging the partner’s involvement with breathingtechniques
• Assisting the woman and her partner to focus on breath-ing techniques
• Informing the woman that the discomfort will be inter-mittent and of limited duration; urging her to rest between contractions to preserve her strength; andencouraging her to use distracting activities to lessenthe focus of uterine contractions
• Changing bed linens and gown as needed• Keeping perineal area clean and dry• Supporting the woman’s decisions about pain
management• Monitoring maternal vital signs frequently and report-
ing any abnormal values• Ensuring that the woman takes deep cleansing breaths
before and after each contraction to enhance gas ex-change and oxygen to the fetus
• Educating the woman and her partner about the need forrest and helping them plan strategies to conserve strength
358 Unit 4 LABOR AND BIRTH
l Figure 14-16 The nurse documenting care.

• Monitoring FHR for baseline, accelerations, variability,and decelerations
• Checking on bladder status and encouraging voiding atleast every 2 hours to make room for birth
• Repositioning the woman as needed to obtain optimalheart rate pattern
• Supporting requests from the woman and communi-cating them to appropriate personnel
• Respecting the woman’s sense of privacy by coveringher when appropriate
• Offering human presence (being physically present withthe woman), not leaving her alone for long periods
• Exercising patience with the natural labor pattern toallow time for change
• Reporting any deviations from normal to the healthcareprofessional so that interventions can be initiated earlyto be effective (Simkin, 2002)
See Nursing Care Plan 14-1.
Nursing Management During theSecond Stage of LaborNursing care during the second stage of labor focuses onsupporting the woman and her partner in making activedecisions about her care and labor management, imple-
menting strategies to prolong the early passive phase offetal descent, supporting involuntary bearing-down efforts,providing instruction and assistance, and using mater-nal positions that can enhance descent and reduce pain(Roberts, 2003). Research suggests that strong pushingduring the second stage may be accompanied by a sig-nificant decline in fetal pH and may cause maternalmuscle and nerve damage if done too early (Hansen et al.,2002). Shortening the phase of active pushing andlengthening the early phase of passive descent can beachieved by encouraging the woman not to push untilshe has a strong desire to do so and until the descentand rotation of the fetal head are well advanced. Effec-tive pushing can be achieved by assisting the woman toassume a more upright or squatting position (Simkin &Ancheta, 2000).
Perineal lacerations or tears can occur during the sec-ond stage when the fetal head emerges through the vaginalintroitus. The extent of the laceration is defined by depth:a first-degree laceration extends through the skin; a sec-ond-degree laceration extends through the muscles of theperineal body; a third-degree laceration continues throughthe anal sphincter muscle; and a fourth-degree lacerationalso involves the anterior rectal wall. Special attentionneeds to be paid to third- and fourth-degree lacerations toprevent future fecal incontinence (Ladewig, London, &
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 359
Table 14-3
*The frequency of assessments is dictated by the health status of the woman and fetus andcan be altered if either one of their conditions changes.
EFM, electronic fetal monitoring.
Vital signs (BP, pulse,respirations)
Temperature
Contractions(frequency,duration, intensity)
Fetal heart rate
Vaginal exam
Behavior/psychosocial
Every 30–60 min
Every 4 hours
Every 30–60 min bypalpation orcontinuously if EFM
Every hour by Doppler orcontinuously by EFM
Initially on admission todetermine phase andas needed based onmaternal cues todocument laborprogression
With every clientencounter: talkative,excited, anxious
Every 30 min
Every 4 hours
Every 15–30 min bypalpation orcontinuously if EFM
Every 30 min by Doppleror continuously by EFM
As needed to monitorlabor progression
With every clientencounter: self-absorbed in labor;intense and quiet now
Table 14-3 Summary of Assessments during the First Stage of Labor
Every 15–30 min
Every 4 hours
Every 15 min bypalpation orcontinuously if EFM
Every 15–30 min byDoppler orcontinuously by EFM
As needed to monitorlabor progression
With every clientencounter:discouraged, irritable,feels out of control,declining copingability
Assessments* Latent Phase (0–3 cm) Active Phase (4–7 cm) Transition (8–10 cm)

Davidson, 2006). Any lacerations should be repaired bythe primary care provider during the third stage of labor.
An episiotomy is an incision made in the perineum toenlarge the vaginal outlet and theoretically to shorten thesecond stage of labor. Alternative measures such as warmcompresses and continual massage with oil have been suc-cessful in stretching the perineal area to prevent cutting it.Further research needs to be done to validate the efficacyof natural measures versus the episiotomy. The midlineepisiotomy is the most common one used in the UnitedStates because it can be easily repaired and causes the leastamount of pain (Lowdermilk & Perry, 2004). Figure 14-17shows episiotomy locations.
AssessmentAssessment is continuous during the second stage of labor.Hospital policies dictate the specific type and timing ofassessments, as well as the way in which they are docu-mented. Figure 14-18 shows a sample form.
Assessment involves identifying the signs typical ofthe second stage of labor, including:
• Increase in apprehension or irritability• Spontaneous rupture of membranes• Sudden appearance of sweat on upper lip• Increase in blood-tinged show• Low grunting sounds from the woman• Complaints of rectal and perineal pressure• Beginning of involuntary bearing-down efforts
Other ongoing assessments include the contractionfrequency, duration, and intensity; maternal vital signsevery 5 to 15 minutes; fetal response to labor as indicatedby FHR monitor strips; amniotic fluid for color, odor, andamount when membranes are ruptured; and the womanand her partner’s coping status (Table 14-4).
Assessment also focuses on determining the progressof labor. Associated signs include bulging of the per-ineum, labial separation, advancing and retreating ofthe newborn’s head during and between bearing-downefforts, and crowning (fetal head is visible at vaginalopening; Fig. 14-19).
A vaginal examination is completed to determine if it is appropriate for the woman to push. Pushing isappropriate if the cervix has fully dilated to 10 cm andthe woman feels the urge to push.
Nursing InterventionsNursing interventions during this stage focus on moti-vating the woman, encouraging her to put all her effortsto pushing this newborn to the outside world, and givingher feedback on her progress. If the woman is pushingand not making progress, the nurse can suggest she keepher eyes open during the contractions and look towardwhere the infant is coming out. Changing positions every20 to 30 minutes will also help in making progress.Positioning a mirror so the woman can visualize thebirthing process and how successful her pushing effortsare can help motivate her.
During the second stage of labor, an ideal positionwould be one that opens the pelvic outlet as wide as pos-sible, provides a smooth pathway for the fetus to descendthrough the birth canal, uses the advantages of gravity toassist the fetus to descend, and gives the mother a senseof being safe and in control of the labor process (Gupta& Nikodem, 2003). Some suggestions for positions in thesecond stage include:
• Lithotomy with feet up in stirrups: most convenientposition for caregivers
• Semi-sitting with pillows underneath knees, arms,and back
• Lateral/side-lying with curved back and upper legsupported by partner
• Sitting on birthing stool: opens pelvis, enhances the pullof gravity, and helps with pushing
• Squatting/supported squatting: gives the woman a senseof control
360 Unit 4 LABOR AND BIRTH
T E A C H I N G G U I D E L I N E S 1 4 - 1
Teaching for Positioning During the First Stage of Labor
Try using some of these positions during the first stageof labor:• Walking with support from your partner (adds the force
of gravity to contractions to promote fetal descent)• Slow-dancing position with your partner holding you
(adds the force of gravity to contractions and promotessupport from and active participation of your partner)
• Side-lying with pillows between the knees for comfort(offers a restful position and improves oxygen flow tothe uterus)
• Semi-sitting in bed or on a couch leaning against thepartner (reduces back pain because fetus falls forward,away from the sacrum)
• Sitting in a chair with one foot on the floor and one onthe chair (changes pelvic shape)
• Leaning forward by straddling a chair, a table, or abed or kneeling over a birth ball (reduces back pain,adds the force of gravity to promote descent; possiblepain relief if partner can apply sacral pressure)
• Sitting in a rocking chair or on a birth ball and shiftingweight back and forth (provides comfort because rock-ing motion is soothing; uses the force of gravity to helpfetal descent)
• Lunge by rocking weight back and forth with foot up onchair during contraction (uses force of gravity by beingupright; enhances rotation of fetus through rocking)
• Open knee–chest position (helps to relieve backdiscomfort) (Simkin & Ancheta, 2000)

Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 361
Outcome identification and evaluation
Client will remain calm and in control as evidencedby ability to make decisions and use positive coping strategies.
Interventions with rationales
Provide instruction regarding the labor process toallay anxiety.
Reorient the woman to the physical environmentand equipment as necessary to keep clientinformed of events.
Encourage verbalization of feelings and concerns toreduce anxiety.
Listen attentively to woman and partner to demon-strate interest and concern.
Inform woman and partner of standard proce-dures/processes to ensure adequate understand-ing of events and procedures.
Frequently update/inform woman of progress andlabor status to provide positive reinforcement foractions.
Reinforce relaxation techniques and provide instruc-tion if needed to aid in coping.
Encourage participation of the partner in the coach-ing role; role-model to facilitate partner participa-tion in labor process to provide support andencouragement to the client.
Provide a presence and remain with woman asmuch as possible to provide comfort and support.
Candice, a 23-year-old gravida 1, para 0 (G1,P0) is admitted to the labor and birth suite at39 weeks’ gestation having contractions of moderate intensity every 5 to 6 minutes. A vagi-nal exam reveals her cervix is 80% effaced and 5 cm dilated. The presenting part (vertex)is at 0 station and her membranes ruptured spontaneously 4 hours ago at home. She isadmitted and an IV is started for hydration and vascular access. An external fetal monitoris applied. FHR is 140 bpm and regular. Her partner is present at her bedside. Candice isnow in the active phase of the first stage of labor, and her assessment findings are as follows:cervix dilated 7 cm, 80% effaced; moderate to strong contractions occurring regularly, every3 to 5 minutes, lasting 45 to 60 seconds; at 0 station on pelvic exam; FHR auscultated loud-est below umbilicus at 140 bpm; vaginal show—pink or bloody vaginal mucus; currentlyapprehensive, inwardly focused, with increased dependency; voicing concern about abilityto cope with pain; limited ability to follow directions.
Nursing Care Plan
Nursing Diagnosis: Anxiety related to labor and birth process and fear of the unknown related toclient’s first experience
(continued)
Nursing Care Plan 14-1Overview of the Woman in the Active Phase of the First Stage of Labor
Client will maintain a tolerable level of pain and dis-comfort as evidenced by statements of painrelief, pain rating of 2 or less on pain rating scale,and absence of adverse effects in client and fetusfrom analgesia or anesthesia.
Monitor vital signs, observe for signs of pain and haveclient rate pain on a scale of 0 to 10 to providebaseline for comparison.
Encourage client to void every 1 to 2 hours todecrease pressure from a full bladder.
Nursing Diagnosis: Pain related to effects of contractions and cervical dilatation and events of labor

• Kneeling with hands on bed and knees comfortablyapart
Other important nursing interventions during thesecond stage include:
• Providing continuous comfort measures such as mouthcare, position changes, changing bed linen and under-pads, and providing a quiet, focused environment
• Instructing the woman on the following bearing-downpositions and techniques:• Pushing only when she feels an urge to push• Using abdominal muscles when bearing down• Using short pushes of 6 to 7 seconds• Focusing attention on the perineal area to visualize
the newborn• Relaxing and conserving energy between contractions
362 Unit 4 LABOR AND BIRTH
Outcome identification and evaluation Interventions with rationales
Assist woman to change positions frequently toincrease comfort and promote labor progress.
Encourage use of distraction to reduce focus oncontraction pain.
Suggest pelvic rocking, massage, or counter backpressure to reduce pain.
Assist with use of relaxation and breathing techniquesto promote relaxation.
Use touch appropriately (backrub) when desired bythe woman to promote comfort.
Integrate use of nonpharmacologic measures ofpain relief, such as warm water, birthing ball, orother techniques to facilitate pain relief.
Administer pharmacologic agents as ordered whenrequested to control pain.
Provide reassurance and encouragement betweencontractions to foster self-esteem and continuedparticipation in labor process.
Overview of the Woman in the Active Phase of the First Stage of Labor (continued)
Client will remain free of infection as evidenced byabsence of signs and symptoms of infection, vitalsigns and FHR within acceptable parameters, labtest results within normal limits, and clear amnioticfluid without odor.
Monitor vital signs (every 1 to 2 hours after ROM) andFHR frequently as per protocol to allow for earlydetection of problems; report fetal tachycardia(early sign of maternal infection) to ensure prompttreatment.
Provide frequent perineal care and pad changes tomaintain good perineal hygiene.
Change linens and woman’s gown as needed tomaintain cleanliness.
Ensure that vaginal exams are performed only whenneeded to prevent introducing pathogens intothe vaginal vault.
Monitor lab test results such as white blood cell countto assess for elevations indicating infection.
Use aseptic technique for all invasive procedures toprevent infection transmission.
Carry out good handwashing techniques beforeand after procedures and use standard precau-tions as appropriate to minimize risk of infectiontransmission.
Document amniotic fluid characteristics—color,odor—to establish baseline for comparison.
Nursing Diagnosis: Risk of infection related to vaginal exams following rupture of membranes

• Pushing several times with each contraction• Pushing with an open glottis and slight exhalation
(Roberts, 2003)• Continuing to monitor contraction and FHR patterns
to identify problems• Providing brief, explicit directions throughout this stage• Continuing to provide psychosocial support by re-
assuring and coaching• Facilitating the upright position to encourage the fetus
to descend• Continuing in assessment measurements: blood pres-
sure, pulse, respirations, uterine contractions, bearing-down efforts, FHR, coping status of the client and herpartner
• Providing pain management if needed• Providing a continuous nursing presence• Offering praise for the client’s efforts• Preparing for and assisting with delivery by:
• Notifying the health care provider of the estimatedtimeframe for birth
• Preparing the delivery bed and positioning client• Preparing the perineal area according to the facility’s
protocol• Offering a mirror and adjusting it so the woman can
watch the birth• Explaining all procedures and equipment to the client
and her partner• Setting up delivery instruments needed while main-
taining sterility• Receiving newborn and transporting him or her to a
warming environment, or covering the newborn witha warmed blanket on the woman’s abdomen
• Providing initial care and assessment of the newborn(see the Birth section that follows)
BirthThe second stage of labor ends with the birth of the new-born. The maternal position for birth varies from thestandard lithotomy position to side-lying to squatting tostanding or kneeling, depending on the birthing location,the woman’s preference, and standard protocols. Oncethe woman is positioned for birth, the vulva and perinealarea are cleansed. The primary healthcare provider thentakes charge after donning protective eyewear, masks,gowns, and gloves and performing hand hygiene.
Once the fetal head has emerged, the primary careprovider explores the fetal neck to see if the umbilical cordis wrapped around it. If it is, the cord is slipped over thehead to facilitate delivery. As soon as the head emerges,the healthcare provider suctions the newborn’s mouthand nares with a bulb syringe to prevent aspiration ofmucus, amniotic fluid, or meconium (Fig. 14-20). Theumbilical cord is double-clamped and cut between theclamps. With the first cries of the newborn, the secondstage of labor ends.
Immediate Care of the NewbornOnce the infant is born, the nurse places the newbornunder the radiant warmer, dries the newborn, assessesthe newborn, wraps the newborn in warmed blankets,and places the newborn on the woman’s abdomen forwarmth and closeness. In some healthcare facilities, thenewborn is placed on the woman’s abdomen immedi-ately after birth and covered with a warmed blanket. Ineither scenario, the stability of the newborn dictates thelocation of aftercare. The nurse can also assist with thefirst breastfeeding.
Assessment of the newborn begins at the momentof birth and continues until the newborn is discharged.
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 363
Leftmediolateral
Rightmediolateral
B
l Figure 14-17 Location of an episiotomy. (A) Midline episiotomy. (B) Right and leftmediolateral episiotomies.
A

Admit date
/ /
/ /
Admit time
Current date
Temperature
IntactBulging
MembranesBlood typeand Rh
Deep tendon reflexes Vaginal bleeding Pain Uterine activitymonitor mode
MVUs Montevideo units Fetalmonitor mode
STV short-term variability+ = Present (roughness of tracing line present)∅ = Absent (tracing line is smooth)0 = No response
+1 = Sluggish+2 = Normal+3 = Hyperactive+4 = Brisk + hyperactiveC = Clonus
10 = Highest intensity
5 = Distressing pain
0 = No painP = PalpationE = External
The sum of the peak of eachuterine contraction minus itsresting tone, in a 10-minute period.I = Internal
LTV long-term variabilityA = Auscultation (fetoscope)D = DopplerE = ExternalI = Internal
--------
NS = Normal showABN = Frank vaginal bleeding
∅ = 0– 2 BPM = Absent↓ = 3– 5 BPM = Minimal+ = 6–25 BPM = Absent↑ = greater than 25 BPM = Marked
Pulse
Vit
alsi
gn
sM
ater
nal
Ute
rin
eac
tivi
tyF
etal
asse
ssm
ent
(mL’s
/Hr)
Con
tmed
sIn
terv
enti
on
Abb
revi
atio
ns/
key
Inta
ke/o
utpu
t
Blood pressure
Deep tendon reflexes(L/R)
Respiration /O2 saturation
Urine (protein/sugar)Vaginal bleeding
Pain
/ / / / / / / / / / / / / / / / / // / / / / / / / / / / / / / / / / /
Edema (site, extent)
Monitor mode
Frequency
Duration
Peak IUP
Resting toneIntensity
MVUsMonitor mode (Strip #____)
Time
Age G T Pt A L EDD____/____/___
LMP____/____/___
Ruptured SROM AROM
Date____/____/___ Time___
Baseline (FHR)STVLTV
AccelerationsDecelerationsMembranes/fluid
Scalp pH
IV
POUrine
Emesis
Pitocin mU/minMagnesium sulfate gms/hr
TreatmentsTeaching/support
Touch
Position/activity
Physical care
Initials
Labor Progress ChartMaternal/Newborn Record System
l Figure 14-18 A sample labor flow sheet. (Used with permission. Briggs Corporation, 2001.) (continued)
364 Unit 4 LABOR AND BIRTH

None Latex/ /
Current date
Other_______________________________________________________________________________Allergy/sensitivity
Accelerations Membranes Treatments Teaching/support Touch Physical carePosition/activity
FluidDecelerations
+ = less than 15 BPM ↑+/or less than 15 sec
++ = 15 BPM ↑X 15 sec
0 = None
N = NoneE = EarlyV = Variable
L = LateP = Prolonged
I = IntactB = Bulging
C = ClearM = Meconium stainedB = BloodyF = Foul odor
NF = No foul odor
R = Ruptured
O2 = O2 L/minIVB = IV bolusSC = Straight catheterizationFC = Foley catheterization
ABD = Abdominal hair removal
O = Orient to unit E = Effleurage MC = Mouth careSC = Superficial coldSH = Supericial heatPC = Peri careBP = Bedpan
w = WalkingC = Chair
SQ = SquattingJR = Jet hydrotherapySH = Shower
K = KneelingLS = Left sideRS = Right sideKC = Knee chest
T = Trendelenburg
B = BackrubCP = Counterpressure
M = Massage
SR = Safety reviewLR = Labor review
F = FocusingBRT = Breathing/relaxation techniquesPrO = PreOp.
///// // / / / / / / / / / / / / / / ////// // / / / / / / / / / / / / / / /
Chart___________of________
Labor Progress ChartMaternal/Newborn Record System
l Figure 14-18 (continued)
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 365

Examinedby:
Effacement %and/or position
Effacement %and/or position
Effacement %and/or position
DILATATION
DILATATION
STATION
STATION
DILATATION
STATION
Labor Progress ChartMaternal/Newborn Record System
Date, time
Startdate
Medication/dose Route Site Initials Initials Signature
Signature keyInterval medications
IV Record
Time Site Solution Amount(mL’s)
Medication/doseadded Initials Infused
date Time Amountinfused
Labor progress curves derived from the work of Emanuel A. Friedman, M.D.
COMPOSITE CURVES OF ABNORMAL LABOR PROGRESS—MULTIPAROUSCOMPOSITE NORMAL DILATATION CURVES
1000
0800
0900
1100
1200
1300
1400
1500
1600
1700
1000
0800
0900
1100
1200
1300
1400
1500
1600
1700 TIME
10
9
8
7
6
5
4
3
2+3
+2
+1
–1
–2
–3
–4
0
Mark X
TIME
10
9
8
7
6
5
4
3
2+3
+2
+1
–1
–2
–3
–4
0
Mark X
TIME
10
9
8
7
6
5
4
3
2+3
+2
+1
–1
–2
–3
–4
0
Mark X
Prolongedlatent phase
Prolongeddeceleration curve
Protractedactive phaseNormal
dilatation curve
MULTIPAROUS(composite) NULLIPAROUS
(composite)Secondary arrestof dilatation
l Figure 14-18 (continued)
366 Unit 4 LABOR AND BIRTH

Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 367
Every 15 min
Newborn—completehead-to-toeassessment; vital signsevery 15 min untilstable
Palpating for firmnessand position every 15 min for first hr
None
Assess every 15 min withfundus firmness
Observe every 15 min:usually excited,talkative, awake;needs to holdnewborn, be close,and inspect body
Table 14-4
*The frequency of assessments is dictated by the health status of the woman and fetus andcan be altered if either one of their conditions changes.
EFM, electronic fetal monitoring.
Second Stage of Labor Third Stage of Labor Fourth Stage of LaborAssessments* (Birth of Neonate) (Placenta Expulsion) (Recovery)
Vital signs (BP, pulse,respirations)
Fetal heart rate
Contractions/uterus
Bearing down/pushing
Vaginal discharge
Behavior/psychosocial
Every 5–15 min
Every 5–15 min by Doppleror continuously by EFM
Palpate every one
Assist with every effortObserve for signs of
descent—bulging ofperineum, crowning
Observe every 15 min:cooperative, focus ison work of pushingnewborn out
Every 15 min
Apgar scoring at 1 and 5 min
Observe for placentalseparation
None
Assess bleeding afterexpulsion
Observe every 15 min:often feelings of reliefafter hearing newborncrying; calmer
Table 14-4 Summary of Assessments During the Second, Third, and Fourth Stages of Labor
l Figure 14-19 Crowning.
Drying the newborn and providing warmth to prevent heatloss by evaporation is essential to help support thermo-regulation and provide stimulation. Placing the newbornunder a radiant heat source and putting on a stockinet capwill further reduce heat loss after drying.
The nurse assesses the newborn by assigning anApgar score at 1 and 5 minutes. The Apgar score assessesfive parameters—heart rate (absent, slow, or fast), respi-ratory effort (absent, weak cry, or good strong yell), mus-cle tone (limp, or lively and active), response to irritationstimulus, and color—that evaluate a newborn’s cardio-respiratory adaptation after birth. The parameters arearranged from the most important (heart rate) to the leastimportant (color). The newborn is assigned a score of 0 to2 in each of the five parameters. The purpose of the Apgarassessment is to evaluate the functioning of the centralnervous system; see Chapter 18 for additional informationon Apgar scoring.
Two identification bands are secured on the new-born’s wrist and ankle that match the band on the mother’swrist to ensure the newborn’s identity. This identificationprocess is completed in the birthing suite before anyoneleaves the room. Some health care agencies also take an

early photo of the newborn for identification in the event ofabduction (McKinney et al., 2005).
Other types of newborn security systems can also beused to prevent abduction. Some systems have sensors thatare attached to the newborn’s identification bracelet orcord clamp. An alarm is set off if the bracelet or clamp acti-vates receivers near exits. Others have an alarm that isactivated when the sensor is removed from the newborn(Fig. 14-21). Even with the use of electronic sensors,the parents, nursing staff, and security personnel areresponsible for prevention strategies and ensuring thesafety and protection of all newborns and their families(Shogan, 2002).
Nursing Management During the Third Stage of LaborDuring the third stage of labor, strong uterine contrac-tions continue at regular intervals under the continuinginfluence of oxytocin. The uterine muscle fibers shorten,or retract, with each contraction, leading to a gradualdecrease in the size of the uterus, which helps shear theplacenta away from its attachment site. The third stage iscomplete when the placenta is delivered. Nursing careduring the third stage of labor primarily focuses on imme-diate newborn care and assessment and being available to
assist with the delivery of the placenta and inspecting it forintactness.
Three hormones play important roles in the thirdstage. During this stage the woman experiences peak lev-els of oxytocin and endorphins, while the high adrenalinelevels that occurred during the second stage of labor toaid with pushing begin falling. The hormone oxytocincauses uterine contractions and helps the woman to enactinstinctive mothering behaviors such as holding the new-born close to her body and cuddling the baby.
Skin-to-skin contact immediately after birth and thenewborn’s first attempt at breastfeeding further augmentmaternal oxytocin levels, strengthening the uterine con-tractions that will help the placenta to separate and theuterus to contract to prevent hemorrhage. Endorphins,the body’s natural opiates, produce an altered state ofconsciousness and aid in blocking out pain. In addition,the drop in adrenaline level from the second stage, whichhad kept the mother and baby alert at first contact, causesmost women to experience feelings of cold and shiveringshortly after giving birth.
A crucial role for nurses during this time is to protectthe natural hormonal process by ensuring unhurried anduninterrupted contact between mother and newborn afterbirth, providing warmed blankets to prevent shivering,and allowing skin-to-skin contact and breastfeeding.
AssessmentAssessment during the third stage of labor includes:
• Monitoring placental separation by looking for thefollowing signs:• Firmly contracting uterus• Change in uterine shape from discoid to globular ovoid• Sudden gush of dark blood from vaginal opening• Lengthening of umbilical cord protruding from vagina
368 Unit 4 LABOR AND BIRTH
l Figure 14-20 Suctioning the newborn immediatelyafter birth.
l Figure 14-21 An example of a security sensor appliedto a newborn’s arm.

• Examining placenta and fetal membranes for intactnessthe second time (the health care provider assesses theplacenta for intactness the first time) (Fig. 14-22)
• Assessing for any perineal trauma, such as the follow-ing, before allowing the birth attendant to leave:• Firm fundus with bright-red blood trickling: laceration• Boggy fundus with red blood flowing: uterine atony• Boggy fundus with dark blood and clots: retained
placenta• Inspecting the perineum for condition of episiotomy, if
performed• Assessing for perineal lacerations and ensuring repair
by birth attendant
Nursing InterventionsInterventions during the third stage of labor include:
• Describing the process of placental separation to thecouple
• Instructing the woman to push when signs of separationare apparent
• Administering an oxytocic if ordered and indicatedafter placental expulsion
• Providing support and information about episiotomyand/or laceration
• Cleaning and assisting client into a comfortable posi-tion after birth, making sure to lift both legs out of stir-rups (if used) simultaneously to prevent strain
• Repositioning the birthing bed to serve as a recoverybed if applicable
• Assisting with transfer to the recovery area if applicable• Providing warmth by replacing warmed blankets over
the woman• Applying an ice pack to the perineal area to provide
comfort to episiotomy if indicated• Explaining what assessments will be carried out over the
next hour and offering positive reinforcement for actions• Ascertaining any needs• Monitoring maternal physical status by assessing:
• Vaginal bleeding: amount, consistency, and color
• Vital signs: blood pressure, pulse, and respirationstaken every 15 minutes
• Uterine fundus, which should be firm, in the midline,and at the level of the umbilicus
• Recording all birthing statistics and securing primarycaregiver’s signature
• Documenting birthing event in the birth book (officialrecord of the facility that outlines every birth event),detailing any deviations
Nursing Management During theFourth Stage of LaborThe fourth stage of labor begins after the placenta isexpelled and lasts up to 4 hours after birth, during whichtime recovery takes place. This recovery period may takeplace in the same room where the woman gave birth, in aseparate recovery area, or in her postpartum room.During this stage, the woman’s body is beginning toundergo the many physiologic and psychological changesthat occur after birth. The focus of nursing managementduring the fourth stage of labor involves frequent closeobservation for hemorrhage, provision of comfort mea-sures, and promotion of family attachment.
AssessmentAssessments during the fourth stage center on the woman’svital signs, status of the uterine fundus and perineal area,comfort level, lochia amount, and bladder status. Duringthe first hour after birth, vital signs are taken every 15 min-utes, then every 30 minutes for the next hour if needed.The woman’s blood pressure should remain stable andwithin normal range after giving birth. A decrease mayindicate uterine hemorrhage; an elevation might suggestpreeclampsia.
The pulse usually is typically slower (60 to 70 bpm)than during labor. This may be associated with a decreasein blood volume following placental separation. An ele-vated pulse rate may be an early sign of blood loss. Theblood pressure usually returns to its prepregnancy level
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 369
A B
l Figure 14-22 Placenta. (A) Fetal side. (B) Maternal side.

and therefore is not a reliable early indicator of shock.Fever is indicative of dehydration (<100.4°F or 38°C)or infection (>101°F), which may involve the genitouri-nary tract. Respiratory rate is usually between 16 and24 breaths per minute and regular. Respirations shouldbe unlabored unless there is an underlying preexistingrespiratory condition.
Assess fundal height, position, and firmness every15 minutes during the first hour following birth. The fun-dus needs to remain firm to prevent excessive postpartumbleeding. The fundus should be firm (feels like the sizeand consistency of a grapefruit), located in the midlineand below the umbilicus. If it is not firm (boggy), gentlymassage it until it is firm (see Nursing Procedure 22-1 formore information). Once firmness is obtained, stop mas-sage. If the fundus is displaced to the right of the midline,suspect a full bladder as the cause.
The vagina and perineal areas are quite stretched andedematous following a vaginal birth. Assess the perineum,including the episiotomy if present, for possible hematomaformation. Suspect a hematoma if the woman reportsexcruciating pain or cannot void or if a mass is noted in theperineal area. Also assess for rectal hemorrhoids, whichcan cause discomfort.
Assess the woman’s comfort level frequently to deter-mine the need for analgesia. Ask the woman to rate herpain on a scale of 1 to 10; it should be less than 3. If it ishigher, further evaluation is needed to make sure therearen’t any deviations contributing to her discomfort.
Assess vaginal discharge (lochia) every 15 minutes forthe first hour and every 30 minutes for the next hour.Palpate the fundus at the same time to ascertain its firm-ness and help to estimate the amount of vaginal discharge.In addition, palpate the bladder for fullness, since manywomen receiving an epidural block experience limitedsensation in the bladder region. Voiding should producelarge amounts of urine (diuresis) each time. Palpation ofthe woman’s bladder after each voiding helps to ensurecomplete emptying. A full bladder will displace the uterusto either side of the midline and potentiate uterine hem-orrhage secondary to bogginess.
Nursing InterventionsNursing interventions during the fourth stage mightinclude:
• Providing support and information to the woman regard-ing episiotomy repair and related pain-relief and self-care measures
• Applying an ice pack to the perineum to promotecomfort and reduce swelling
• Assisting with hygiene and perineal care; teaching thewoman how to use the perineal bottle after each padchange and voiding; helping the woman into a new gown
• Monitoring for return of sensation and ability to void (ifregional anesthesia was used)
• Encouraging the woman to void by ambulating to bath-room, listening to running water, or pouring warm waterover the perineal area with the peribottle
• Monitoring vital signs and fundal and lochia statusevery 15 minutes and documenting them
• Promoting comfort by offering analgesia for afterpainsand warm blankets to reduce chilling
• Offering fluids and nourishment if desired• Encouraging parent–infant attachment by providing
privacy for the family• Being knowledgeable and sensitive to typical cultural
practices after birth• Assisting the mother to nurse, if she chooses, during the
recovery period to promote uterine firmness due to therelease of oxytocin from the posterior pituitary gland,which stimulates uterine contractions
• Teaching the woman how to assess her fundus for firm-ness periodically and to massage it if it is boggy
• Describing the lochia flow and normal parameters toobserve for postpartum
• Teaching safety techniques to prevent newbornabduction
• Demonstrating the use of the portable sitz bath as a com-fort measure for her perineum if she had a laceration oran episiotomy repair
• Explain comfort/hygiene measures and when to use them• Assisting with ambulation when getting out of bed for
the first time• Providing information about the routine on the
mother–baby unit or nursery for her stay• Observing for signs of early parent–infant attachment:
fingertip touch to palm touch to enfolding of the infant(Murray et al., 2002)
K E Y C O N C E P T S
l A nurse provides physical and emotional supportduring the labor and birth process to assist a womanto achieve her goals.
l When a woman is admitted to the labor and birtharea, the admitting nurse must assess and evaluate therisk status of this pregnancy and initiate appropriateinterventions to provide optimal care for this client.
l Completing an admission assessment includes tak-ing a maternal health history; performing physicalassessment on the woman and fetus, including heremotional and psychosocial status; and obtaining thenecessary laboratory studies.
l The nurse’s role in fetal assessment for labor andbirth includes determining fetal well-being and inter-preting signs and symptoms of possible compromise.Determining the fetal heart rate (FHR) pattern andassessing amniotic fluid characteristics are key.
l FHR can be assessed intermittently or continuously.Although the intermittent method allows the clientto move about during labor, the information
370 Unit 4 LABOR AND BIRTH

obtained intermittently does not provide a completepicture of fetal well-being from moment to moment.
l Assessment parameters of the FHR are classifiedas baseline rate, baseline variability (long-term andshort-term), and periodic changes in the rate (accelerations and decelerations).
l The nurse monitoring the laboring client needs tobe knowledgeable about which parameters are reassuring, nonreassuring, and ominous so thatappropriate interventions can be instituted.
l For a nonreassuring FHR pattern, the nurse shouldnotify the healthcare provider about the pattern andobtain further orders, making sure to document allinterventions and their effects on the FHR pattern.
l In addition to interpreting assessment findings andinitiating appropriate inventions for the laboringclient, accurate and timely documentation must becarried out continuously.
l Today’s women have many safe nonpharmacologicand pharmacologic choices for the management ofpain during childbirth. They may be used individu-ally or in combination to complement one another.
l Nursing management for the woman during laborand birth includes comfort measures, emotional support, information and instruction, advocacy, andsupport for the partner.
l Nursing care during the first stage of labor includestaking an admission history (reviewing the prenatalrecord), checking the results of routine laboratorywork and special tests done during pregnancy, asking the woman about her childbirth preparation(birth plan, classes taken, coping skills), and completing a physical assessment of the woman toestablish a baseline of values for future comparison.
l Nursing care during the second stage of labor focuseson supporting the woman and her partner in makingdecisions about her care and labor management,implementing strategies to prolong the early pas-sive phase of fetal descent, supporting involuntarybearing-down efforts, providing instruction and assis-tance, and encouraging the use of maternal positionsthat can enhance descent and reduce the pain.
l Nursing care during the third stage of labor primar-ily focuses on immediate newborn care and assess-ment and being available to assist with the deliveryof the placenta and inspecting it for intactness.
l The focus of nursing management during the fourthstage of labor involves frequently observing the motherfor hemorrhage, providing comfort measures, andpromoting family attachment.
References
Albers, L. (2003). Commentary on “Impact of collaborative manage-ment and early admission in labor on method of delivery.”JOGNN, 32(2), 158–160.
American College of Obstetricians and Gynecologists (ACOG). (2005).Fetal heart rate patterns: monitoring, interpretation, and management(Practice Bulletin Number 62). Washington, DC: Author.
American College of Obstetricians and Gynecologists (ACOG).(2002). Obstetric analgesia and anesthesia (Practice BulletinNumber 36). Washington, D.C: Author.
American Hospital Association. (2003). Hospital statistics. Chicago:Author.
Association of Women’s Health, Obstetric and Neonatal Nurses(AWHONN). (2000). Fetal assessment (Clinical PositionStatement). Washington, DC: Author.
Baird, S. M., & Ruth, D. J. (2002). Electronic fetal monitoring of the preterm fetus. Journal of Perinatal and Neonatal Nursing, 16(1),12–24.
Breslin, E. T., & Lucas, V. A. (2003). Women’s health nursing: towardevidence-based practice. St. Louis: Saunders.
Bricker, L., & Lavender, T. (2002). Parenteral opioids for labor painrelief: a systematic review. American Journal of Obstetrics andGynecology, 186(5), S94–S109.
Buckley, S. (2001). A natural approach to the third stage of labor.Midwifery Today, 59, 33–37.
Campbell, G. (2004). Critical incident analysis of water immersion.British Journal of Midwifery, 12(1), 7–11.
Caton, D., Frolich, M. A., & Euliano, T. Y. (2002). Anesthesia forchildbirth: controversy and change. American Journal of Obstetrics& Gynecology, 186(Suppl. 5), S25–30.
Chalk, A. (2004). Pushing in the second stage of labor: Part 1. BritishJournal of Midwifery, 12(8), 502–509.
Cypher, R., Adelsperger, D., & Torgersen, K. L. (2003).Interpretation of the fetal heart rate. In N. Feinstein, K. L.Torgersen, & J. L. Atterbury (Eds.), Fetal heart monitoring princi-ples and practices (3rd ed., pp. 113–154). Dubuque, IA: Kendall-Hunt Publications.
Dillon, P. M. (2003). Nursing health assessment: a critical thinking, casestudies approach. Philadelphia: F. A. Davis Company.
Duddridge, E. (2002). Using complementary therapies during thechildbearing process. British Journal of Midwifery, 10(11), 699–704.
Eappen, S., & Robbins, D. (2002). Nonpharmacological means ofpain relief for labor and delivery. International AnesthesiologyClinics, 40(4), 103–114.
Eltzschig, H., Lieberman, E., & Camann, W. (2003). Regional anes-thesia and analgesia for labor and delivery. New England Journal ofMedicine, 348, 319–332.
Engstrom, J. (2004). Maternal-neonatal nursing made incredibly easy!Philadelphia: Lippincott Williams & Wilkins.
Feinstein, N., Torgersen, K. L., & Atterbury, J. (2003). AWHONN’sfetal heart monitoring principles and practices (3rd ed.). Dubuque,IA: Kendall-Hunt Publishing Company.
Florence, D. J., & Palmer, D. G. (2003). Therapeutic choices for thediscomforts of labor. Journal of Perinatal and Neonatal Nursing,17(4), 238–249.
Fontaine, P., Adam, P., & Svendsen, K. H. (2002). Should intrathe-cal narcotics be used as a sole labor analgesic? A prospective com-parison of spinal opioids and epidural bupivacaine. Journal ofFamily Practice, 51(7), 630–635.
Garite, T. J. (2002). Intrapartum fetal evaluation. In S. G. Gabbe,J. R. Niebyl, & J. L. Simpson (Eds.), Obstetrics: normal and problempregnancies (4th ed., pp. 395–429). New York: ChurchillLivingstone.
Gilbert, E. S., & Harmon, J. S. (2003). Manual of high risk pregnancy& delivery (3rd ed.). St. Louis: Mosby.
Greenwald, L. M., & Mondon, M. (2003). Malpractice and the perinatal nurse. Journal of Perinatal and Neonatal Nursing, 17(2),101–109.
Gupta, J. K., & Nikodem, V. C. (2003). Woman’s position duringsecond stage of labor. The Cochrane Library, Issue 4, Chichester,UK: John Wiley & Sons, Ltd.
Hansen, S., Clark, S., & Foster, J. (2002). Active pushing versuspassive fetal descent in the second stage of labor: a randomizedcontrolled trial. Obstetrics & Gynecology, 99, 29–34.
Hawkins, J., Chestnut, D., & Gibbs, C. (2002). Obstetric anesthesia.In S. Gabbe, J. Niebyl, & J. Simpson (Eds.), Obstetrics: normal andproblem pregnancies (4th ed., pp. 431–472). Philadelphia: ChurchillLivingstone.
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 371

Hodnett, E. D. (2002a). Pain and women’s satisfaction with theexperience of childbirth: a systematic review. American Journal ofObstetrics & Gynecology, 186(5 Pt. 2), 160–172.
Hodnett, E. D. (2002b). Caregiver support for women during child-birth. Cochrane Database System Review 2002; (1): CD000199.
Hunter, L. P. (2002). Being with woman: a guiding concept for thecare of laboring woman. JOGNN, 31(6), 650–657.
Institute for Clinical Systems Improvement (ICSI). (2003). ICSIHealth Care Guidelines (9th ed.). [Online] Available at: www.icsi.org
Iams, J. D., Newman, R. B., Thom, E. A., et al. (2002). Frequency ofuterine contractions and the risk of preterm delivery. New EnglandJournal of Medicine, 346(4), 250–255.
James, D. C., Simpson, K. R., & Knox, G. E. (2003). How do labornurses view their role? Journal of Obstetric, Gynecologic, andNeonatal Nursing, 32, 814–823.
Kane, A. (2001). Focal point on childbirth education: hypnotic anal-gesic suggestion in childbirth. International Journal of ChildbirthEducation, 16(3), 20–22.
King, T. L., & Simpson, K. R. (2001). Fetal assessment duringlabor. In K. R. Simpson and P. Creehan (Eds.), Perinatal nursing(pp. 378–416). Philadelphia: Lippincott.
Landau, R. (2002). Combined spinal-epidural analgesia for labor:breakthrough or unjustified invasion. Seminars in Perinatology, 26,109–121.
Ladewig, P. A., London, M. L., & Davidson, M. R. (2006).Contemporary maternal-newborn nursing care (6th ed.). UpperSaddle River, NJ: Pearson Prentice Hall.
Leeman, L., Fontaine, P., King, V., Klein, M. C., & Ratcliffe, S.(2003a). The nature and management of labor pain: Part I.Nonpharmacologic pain relief. American Family Physician, 68(6),1109–1112.
Leeman, L., Fontaine, P., King, V., Klein, M. C., & Ratcliffe, S.(2003b). The nature and management of labor pain: Part II.Pharmacologic pain relief. American Family Physician, 68(6),1115–1120.
Leonard, P. (2002). Childbirth education: a handbook for nurses.Nursing Spectrum, [Online] Available at: http://nsweb/nursingspectrum.com/ce/m350c.htm
Lieberman, E., & O’Donoghue, C. (2002). Unintended effects ofepidural anesthesia during labor: a systematic review. AmericanJournal of Obstetrics and Gynecology, 186, S31–68.
Littleton, L. Y., & Engebretson, J. C. (2005). Maternity nursing care.Clifton Park, NY: Thomson Delmar Learning.
Lowdermilk, D. L., & Perry, S. E. (2004). Maternity & women’s healthcare (8th ed.). St. Louis: Mosby.
Mahlmeister, L. (2003). Nursing responsibilities in preventing,preparing for, and managing epidural emergencies. Journal ofPerinatal and Neonatal Nursing, 17(1), 19–32.
Mainstone, A. (2004). The use of Doppler in fetal monitoring. BritishJournal of Midwifery, 12(2), 78–84.
Matthews, R., & Callister, L. C. (2004). Childbearing women’s per-ceptions of nursing care that promotes dignity. JOGNN, 33(4),498–507.
Mattson, S., & Smith, J. E. (2004). Core curriculum for maternal-newborn nursing (3rd ed.). St. Louis: Elsevier Saunders.
Mayberry, L., Clemmens, D., & De, A. (2002). Epidural analgesiaside effects, co-interventions, and care of women during child-birth: a systematic review. American Journal of Obstetrics andGynecology, 186(5), S81–S93.
McKinney, E. S., James, S. R., Murray, S. S., & Ashwill, J. W.(2005). Maternal-child nursing (2nd ed.). St. Louis: ElsevierSaunders.
Mitchell, J. (2002). Labor epidurals. Advance for Nurses, 3(23),25–26.
Moore, M. L., & Moos, M. K. (2003). Cultural competence in the careof childbearing families. March of Dimes Nursing Module. WhitePlains, NY: March of Dimes Birth Defects FoundationEducational Services.
Moses, S. (2003). Fetal heart tracing. Family Practice Notebook.[Online] Available at: www.fpnotebook.com/OB45.htm
Murray, M. L. (2004). Maternal or fetal heart rate? Avoiding intrapartum misidentification. JOGNN, 33(1), 93–104.
Murray, S. S., McKinney, E. S., & Gorrie, T. M. (2002). Foundationsof maternal-newborn nursing, 3rd ed. Philadelphia: W. B. Saunders.
Newman, R. B. (2003). Our unrequited love for simple explanation.Journal of Perinatology, 23, 504–506.
Olds, S. B., London, M. L., Ladewig, P. W., & Davidson, M. R.(2004). Maternal-newborn nursing & women’s health. Upper SaddleRiver, NJ: Pearson Prentice Hall.
Paech, M. (2000). Client-controlled epidural analgesia. In D.Birnbach, S. Gatt, & S. Datta (Eds.), Textbook of obstetric anesthe-sia (pp. 189–202). New York: Churchill Livingstone.
Pillitteri, A. (2003). Maternal & child health nursing: care of the child-bearing and childrearing family (4th ed.). Philadelphia: LippincottWilliams & Wilkins.
Pitter, C., & Preston, R. (2001). Modern pharmacologic methods inlabor analgesia. International Journal of Childbirth Education, 16(2),15–20.
Poole, J. H. (2003a). Neuraxial analgesia for labor and birth: implica-tions for mother and fetus. Journal of Perinatal and NeonatalNursing, 17(4), 252–267.
Poole, J. H. (2003b). Analgesia and anesthesia during labor and birth:implications for mother and fetus. JOGNN, 32(6), 780–793.
Priddy, K. D. (2004). Is there logic behind fetal monitoring?JOGNN, 33(5), 550–553.
Primeau, M. R, Lucey, K. A., & Crotty, P. M. (2003). Managing thepain of labor. Advance for Nurses, 4(12), 15–19.
Roberts, J. E. (2003). A new understanding of the second stage oflabor: implications for nursing care. JOGNN, 32(6), 794–801.
Shogan, M. G. (2002). Emergency management plan for newbornabduction. JOGNN, 31(3), 340–346.
Simkin, P. (2002). Supportive care during labor: a guide for busynurses. JOGNN, 31(6), 721–732.
Simkin, P. (2003). Maternal positions and pelves revisited. Birth,30(2), 130–132.
Simkin, P., & Ancheta, R. (2000). The labor progress handbook.Oxford, UK: Blackwell Science.
Simkin, P., & O’Hara, M. (2002). Nonpharmacologic relief of painduring labor: systematic reviews of five methods. American Journalof Obstetrics and Gynecology, 186(5), S131–S159.
Simpson, K. R. (2003). Fetal pulse oximetry update. AWHONNLifelines, 7(5), 411–412.
Simpson, K. R., & Knox, G. E. (2003). Common areas of litigationrelated to care during labor and birth. Journal of Perinatal andNeonatal Nursing, 17(2), 110–125.
Simpson, K. R., & Porter, M. L. (2001). Fetal oxygen saturationmonitoring: using this new technology for fetal assessment duringlabor. AWHONN Lifelines, 5(2), 27–33.
Sisk, B. (2002). Electronic fetal monitoring during labor. [Online]Available at: http://enursesubscribe.com/fetal.htm
Skidmore-Roth, L. (2004). Mosby’s nursing drug reference. St. Louis:Mosby.
Skilnand, E., Fossen, D., & Heiberg, E. (2002). Acupuncture in themanagement of pain in labor. Acta Obstetricia et GynecologicaScandinavica, 81, 943–948.
Sloane, E. (2002). Biology of women (4th ed.). Albany, NY: Delmar.Society of Obstetricians and Gynecologists of Canada (SOGC).
(2002). Fetal health surveillance in labor (SOGC Clinical PracticeGuidelines No. 112). Journal of Obstetrics and Gynecology inCanada, 112(March), 1–13.
Spratto, G. R., & Woods, A. L. (2004). 2004 edition PDR nurse’s drughandbook. Clifton Park, NY: Thomson Delmar Learning.
Stephens, K. C. (2003). An Appalachian perspective. In: M. L.Moore & M. K. Moos (Eds.), Cultural competence in the care ofchildbearing families (pp. 56–59). March of Dimes NursingModule. White Plains, NY: March of Dimes Birth DefectsFoundation Educational Services.
Thacker, S. B., & Stroup, D. F. (2003). Revisiting the use of the elec-tronic fetal monitor. Lancet, 361(9356), 445–447.
Torgersen, K. L. (2004). Intrapartum fetal assessment. In: S.Mattson & J. E. Smith, Core curriculum for maternal-newborn nurs-ing (3rd ed., pp. 303–368). St. Louis: Elsevier Saunders.
Trainor, C. L. (2002). Valuing labor support. AWHONN Lifelines,6(5), 387–389.
Tucker, S. M. (2004). Pocket guide to fetal monitoring and assessment(5th ed.). St. Louis: Mosby.
U.S. Department of Health and Human Services. (2000). Healthypeople 2010: understanding and improving health (2nd ed.). Chapter 16: Maternal, Infant, and Child Health. (DHHSPublication 017-001-00550-9). Washington, D.C.: Author.
372 Unit 4 LABOR AND BIRTH

Youngkin, E. Q., & Davis, M. S. (2004). Women’s health: a primarycare clinical guide (3rd ed.). Upper Saddle River, NJ: Prentice Hall.
Web Resources
Academy for Guided Imagery, Inc.: www.interactiveimagery.comAmerican College of Obstetricians and Gynecologists: www.acog.orgAmerican Public Health Association: www.apha.orgAssociation of Labor Assistants and Childbirth Educators:
www.alace.orgAssociation of Women’s Health, Obstetric and Neonatal Nurses
(AWHONN): www.awhonn.orgBirthworks: www.birthworks.org
BMJ Publication: Evidence-Based Nursing: www.evidencebasednursing.com
Child Find: www.childfind.orgDepartment of Health and Human Services: www.4women.govDiversity Rx: www.diversityrx.orgDoulas of North America (DONA): www.dona.orgEthnomed: http://ethnomed.orgHypnoBirthing Institute: www.hypnobirthing.comInternational Childbirth Education Association: www.icea.orgLamaze International: www.lamaze-childbirth.comNational Center for Missing and Exploited Children:
www.missingkids.comTranscultural Health Links
www.iun.edu/˜libemb/trannurs/trannurs.htm
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 373

374 Unit 4 LABOR AND BIRTH
ChapterWORKSHEETChapter
l M U L T I P L E C H O I C E Q U E S T I O N S1. When a client in labor is fully dilated, which instruc-
tion would be most effective to assist in encouragingeffective pushing?
a. Hold your breath and push through entire con-traction.
b. Use chest-breathing with the contraction.
c. Pant and blow during each contraction.
d. Push for 6 to 7 seconds several times during eachcontraction.
2. During the fourth stage of labor, the nurse palpatesthe uterus on the right side and sees a saturated peri-neal pad. What is the nurse’s first action?
a. Massage the uterus vigorously.
b. Have the client void and reassess her.
c. Notify the primary care provider.
d. Document as a normal finding.
3. When managing a client’s pain during labor, nursesshould:
a. Make sure the agents given don’t prolong labor.
b. Know that all pain-relief measures are similar.
c. Support the client’s decisions and requests.
d. Not recommend nonpharmacologic methods.
4. When caring for a client during the active phase oflabor without continuous electronic fetal monitoring,the nurse would intermittently assess FHR every:
a. 15 minutes
b. 5 minutes
c. 30 minutes
d. 60 minutes
5. The nurse notes the presence of transient fetal accel-erations on the fetal monitoring strip. Which inter-vention would be most appropriate?
a. Reposition the client on the left side.
b. Begin 100% oxygen via face mask.
c. Document this reassuring pattern.
d. Call the healthcare provider immediately.
l C R I T I C A L T H I N K I N G E X E R C I S E S1. Carrie, a 20-year-old primigravida at term, comes to
the birthing center in active labor (dilation 5 cm and80% effaced, −1 station) with ruptured membranes.She states she wants an “all-natural” birth withoutmedication. Her partner is with her and appears anxious but supportive. On the admission assess-ment, Carrie’s prenatal history is unremarkable; vitalsigns are within normal limits; FHR via Dopplerranges between 140 and 144 bpm and is regular.
a. Based on your assessment data and the woman’srequest not to have medication, what nonpharma-cologic interventions could the nurse offer her?
b. What positions might be suggested to help facilitatefetal descent?
2. Several hours later, Carrie complains of nausea andturns to her partner and angrily tells him to not touchher and to go away.
a. What assessment needs to be done to determinewhat is happening?
b. What explanation can you offer Carrie’s partnerregarding her change in behavior?

l S T U D Y A C T I V I T I E S1. Interview a primigravida at a community maternity
clinic in her last trimester of pregnancy about herbirth plan for pain management and specific copingskills she will use for labor. Evaluate them in terms ofeffectiveness according to the literature, and sharethis information with the woman.
2. On the fetal heart monitor, the nurse notices an ele-vation of the fetal baseline with the onset of contrac-tions. This elevation would describe _____________.
3. Compare and contrast a local birthing center to a com-munity hospital’s birthing suite in terms of the painmanagement techniques and fetal monitoring used.
4. Select a childbirth website for expectant parents andcritique the information provided in terms of its educational level and amount of advertising.
Chapter 14 NURSING MANAGEMENT DURING LABOR AND BIRTH 375