Recognizing and Diagnosing Memory Loss
Recognizing and Diagnosing Memory LossBy Dania Phelps NPMental
Health PractitionerBlack Hills Health Care SystemHot Springs VAMCI
am a Psychiatric Nurse Practitioner working in Primary Care in the
Memory Clinic.Focus of this clinic is early recognition of memory
loss, diagnosis, and case management/support of veterans and their
families coping with dementia.
1Credits:Dementia Demonstration ProjectDirected by Dr. Riley
McCartenDirector or the Geriatric Research Education and Clinical
Center at the Minneapolis Veterans Medical Center
Dementia Demonstration ProjectUtilized advanced practice
registered nurses who were trained in screening, evaluating, and
managing cognitive impairment.Embedded into the Primary Care
Clinics at 7 VA centersThe APRNs functioned as Dementia Care
Coordinators.
Dementia Demonstration ProjectAt the end of the 2 year
project:8342 Veterans accepted memory screeningCriteria being 70
years of age or older with no previous diagnosis of dementia were
offered the screening3 word recall and clock draw test was
utilized97% acceptance rate Dementia Demonstration ProjectOut of
8342 Veterans 2081 (or 26%) failed the screen681 ( or 33 %
)Veterans agreed to a comprehensive evaluationOf this group 95% had
cognitive impairment which included 77% having full blown
dementia
Dementia Demonstration ProjectMean cost of medical care in the
year before diagnosis (minus the cost of evaluation) was
$13,378.00
The year after diagnosis mean cost decreased to $11,636.00Course
Objectives:1. Recognize how an undiagnosed memory problem effects
medical outcomes vs. What a recognized memory diagnosis means to
medical outcomesKnow what meets criteria for Dementia Know the
common causes of DementiaKnow Criteria for Mild Cognitive
Impairment (MCI) and Cognitive Disorder NOSKnow the Criteria for a
Memory Work upBe able to put the data together to form a
Diagnosis/and PlanTreatment for Alzheimers Disease and other
Dementias.Statistics According to the 2011 Alzheimers Disease Facts
and FiguresIt is estimated that 5.4 million Americans have
Alzheimers Disease. 200,000 of those are under the age of 65.This
translates to 13% or 1 in 8 Americans over the age of 65 have
Alzheimers Disease.This means: 4% are under the age of 656% are
65-74 years old45% are 74-84 years old45% are 85 or olderStatistics
ContinuedBy the time we reach 85 years of age we have a 50% chance
of having Alzheimers Disease at some stage or another.Women develop
Alzheimers Disease more often then men which is partially explained
by the fact they still tend to live longer.Currently every 69
seconds someone in this country develops Alzheimers Disease. By mid
century one in 33 will develop Alzheimers Disease.DSM IV Dementia
CriteriaEvidence of memory impairmentNeuro/Psych evaluationMMSE ,
SLUMS, MoCA or other reliable testingPlus one of the following
deficitsAphasiaApraxiaAgnosiaExecutive dysfunction
Cognitive deficits cause:Impairment in social or occupational
functioningMust represent a decline in functioningDo not occur
exclusively during deliriumAre not due to other CNS or systemic
disease or substance induced.Are not better accounted for by
another DSM-IV Axis 1 Disorder
Dementia is not a specific disease, but rather a descriptive
term for a collection of symptoms. There are many disorders that
can cause dementia.10Mild Cognitive ImpairmentMild cognitive
impairment is evidenced by neuropsychological testing or clinical
assessment. People with MCI function normally so therefore do not
meet criteria for dementia. 45 50% of those diagnosed with MCI will
develop Alzheimers Disease, the other 55-50% will improve or Stay
the same.Cognitive Disorder NOS294.9 Per DSM-IV-TRThis category is
for disorders that are characterized by cognitive dysfunction
presumed to be due to the direct physiological effect of a general
medical condition that do not meet criteria for any of the specific
deliriums, dementias, or amnestic disorders.Delirium Is NOT
dementiaPeople with dementia are more prone to developing
deliriumOften associated with illnesses, hospitalization, surgery
,and medicationsCharacterized by:Rapid onset of confusion,
disorientation, waxing and waning of attention, waxing and waning
of consciousnessAssociated with higher mortality
Alzheimers Disease Accounts for 50-70% of all dementiasGenerally
appears after the age of 60, but some early onset forms can appear
as early as age 30. Most often we see this in people in their 70s
and 80s.By the time someone is diagnosed the person may have had
the disease 10-20 years.Memory changes occur initially, but as the
disease progresses we start seeing problems with executive
functioning, and eventually problems with movement and changes in
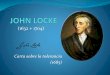
perspective.Alzheimers Disease is a terminal diseaseNeuronHealthy
brain cell and a diseased brain cellAlzheimers Disease: Unraveling
the Mystery National Institute on Aging National Institute on
Health
Brain cells in Alzheimers Disease develop neurofibrillary
tangles and largely made up of the protein tau. Tau is normal in
brain cells, but in AD the tau is changed. The tau is twisted into
pairs of helical filaments that collect into tangles.This causes a
collapse of the neurons transport system then death of the
neuron.15Lewy Body DementiaAccounts for about 15% of all
dementiasProgressiveStarts in the mid brain called the substantia
nigra developing abnormal structures called Lewy Bodies. Lewy
Bodies are made up of the protein call alpha synuclein, also linked
to Parkinsons Disease and other disorders. Symptoms include
hallucinations, Parkinsonism, memory impairment, poor judgment,
confusion, shuffling, day to day fluctuations in attention, REM
sleep disturbance, and autonomic dysfunction e.g. labile BPs.
What Causes Dementia?Alzheimers DiseaseLewy Body DementiaFrontal
Temporal DementiaParkinsons DementiaNormal Pressure
HydrocephalyStrokeHead traumaBrain Mass (benign or
malignant)Alcohol and other drugsTo name the most common.Frontal
Temporal DementiaGenerally a spectrum of disorders that is
sometimes hard to distinguish from Alzheimers Disease, Parkinsons
or Amyotrophic lateral sclerosis (ALS)
Accounts for about 2-10 % of the dementiasSymptoms usually
appear between the ages of 40 and 65Some people with FTD have a
family hx indicating a strong genetic factorPeople live an average
of 5-10 years after diagnosis.Frontal Temporal Disorders
cont.Grouped into 3 types: 1. Progressive behavior/personality
decline Picks Disease, Frontal Temporal variant Characterized by
changes in behavior, personality, poor judgment, and emotional
changes2. Progressive Language decline characterized by changes in
language, speaking, understanding, reading and writing.3.
Progressive motor decline characterized by difficulty in movement,
shaking, difficulties with gate, frequent falls, and poor
coordination.
Parkinsons DementiaBelieved to be part of the Lewy Body Spectrum
of Disorders 60% of people with Parkinsons Disease will
developDementia.
Normal Pressure HydrocephalusAbnormal accumulation of fluid in
the ventricles of the brain.Can be found on CTCan be surgically
correctedMemory loss , changes in executive functioningIncontinence
new onsetShuffling gate/changes in coordinationSlowed
processing
Vascular DementiaAccounts for up to 20% of all the
dementiasCaused by cerebrovascular or cardio vascular problems
Begin suddenly after a major stroke or multiple strokesshowing a
stepwise progression. Those who have had a stroke may improve over
timeKeep in mind cardio vascular problems are a vulnerability for
Alzheimers DiseaseIf you have a sloping progression you may want to
consider a mixed dementia
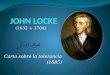
In Alzheimers Disease, Disease starts in the area of the
hippocampus, progresses to the frontal brain and then through out
the cortex.23Unmodifiable Risk Factors for dementiaAge (Number 1
risk factor for dementia)Family hx of Dementia (Genetics)
Scientists have discovered variations that directly cause
Alzheimers disease in the genes coding three proteins: amyloid
precursor protein (APP), presenilin-1 (PS-1) and presenilin-2
(PS-2). APOE status APOE-e4 is one of three common forms of the
APOE gene; the others are APOE-e2 and APOE-e3. Everyone inherits a
copy of some form of APOE from each parent. Those who inherit
APOE-e4 from one parent have an increased risk of Alzheimers. Those
who inherit APOE-e4 from both parents have an even higher risk, but
not a certainty.Female GenderAlzheimer's Association National
Office 225 N. Michigan Ave., Fl. 17, Chicago, IL 60601Alzheimer's
Association is a not-for-profit 501(c)(3) organization
24Modifiable Risk Factors for DementiaHypertensionElevated
cholesterolHigh Homocysteine levels Diabetes-elevated insulin
levelsHeart DiseaseCerebrovascular diseaseHead InjuryEnvironmental
exposureObesityMultiple exposure to anesthesiaPTSDThe Alzheimers
Answer 2008 by Marwin Noel Sabbach, MD Wiley and Sons
PublishingHigh Homocysteine levels may also be related to low
folate, B12, B6 25Recognized vs. Unrecognized
DementiaUNRECOGNIZEDRECOGNIZEDForgets to refill medicationTakes
medications incorrectly e.g. warfarinDoes not remember or
understand medical directions or appointmentsMore falls and
injuriesMore trips to ER/UCHigher cost for medical careUnrecognized
driving concernsHigher risk for wandering
Providing more support for the patient with memory problems e.g.
home care nurse, family involvement, meals on wheels, adult day
care, financial helpAsking family to attend appointments.
Monitoring for caregiver burn outDriving
retirement/monitoringPlanning for the future and help with
transitional support
What is normal aging vs. a memory concern?Normal aging does not
cause dementia.We may not process information as quickly. We may
not multitask as well. Sure we forget to pay a bill once in a
while, perhaps forget to take our medication, and even have
problems with remembering the names of familiar people (not close
family or friends) but we are still able to cognitively manage our
lives.
27What isnt normal agingMemory changes that disrupt daily
lifeChallenges in planning or solving problemsDifficulty completing
familiar tasks Confusion with time or place Trouble understanding
visual images and spatial relationships New problems with words in
speaking or writing Misplacing things and losing the ability to
retrace steps Decreased or poor judgment Withdrawal from work or
social activities Changes in mood or personality2009 Alzheimers
Association
Memory Screening in the Clinical SettingWe routinely screen for
many problems such as colo/rectal cancer, depression, PTSD,
prostate testing etc. Memory needs to be assessed to.Assessing
Mental Status is important to ensure you are receiving a reliable
history and that the patient is able to comply with the recommended
treatment.Dementia is common and age is the #1 risk factor. In the
early stages it is hard to recognize in a 20-30 minute clinic
visit.Pay attention:Are they reordering their medications in a
timely basis according to how you have prescribed them (Have them
bring in their prescriptions and OTC)Be alert to family/friend
concerns of memory or behavior changesAre they reporting a recent
car accident, falls, speech/language problems.Remember the patient
may not notice they have a memory concern.Is there a change in
their general hygiene?Do they seem more disorganized, irritable,
vague in their hx, facts not adding up, confused?
Tools for Screening MemoryMini Mental State Exam: Fairly common,
has a copy write, and takes more than 5 minutes to perform perhaps
not as sensitive to dementiaMoCA (Montreal Cognitive Assessment)
again takes more than 5 minutes to perform and time is limited in
the clinic setting though more sensitive to dementia and can be
used in clinical setting without permission. I like using the MINI
Cog It is a 3 word recall and clock draw test. It doesnt diagnose,
it is a screening tool only but it provides immediate recall,
visual spatial/executive function, and delayed recall information.
Takes about 2 minutes to perform.
Please see sample MINI Cog and MoCA.30MINI COG ScoringScoring is
1 point for each word recalled2 points for a correct clock, must
have a circle, #s 1-12 in fairly accurate axis.Hands pointing to
the correct time. Hands do not have to be of correct
length.Negative score is 4-5 points (In my clinic)Positive score is
3 points or less. At this point you recommend or start a memory
evaluation. Memory EvaluationSee Hand out:Identifying Data:
Name/Age/SSN/Sex/Marital Status and Home Status/Occupation/Dominant
Hand/ and who accompanies them for the evaluation and are they
reliable.Chief Complaint: Patients view of their memory Often they
do not recognize a problem.History of Present Illness Precipitating
factor? Past Medical History (Stroke, exposures (radiation, heavy
metals, chemicals), surgeries, accidents, head trauma etc)
Provide copy of a H&P format and MoCA32Evaluation
cont.AllergiesCurrent Medication and verify against medical chartBe
sure to look at bottles and when they were last filledIs compliance
good? Who sets up and reorders the meds?Are there any medication
that cause cognitive effect?For example: hypnotics,
anticholinergics, pain medications, atypical antipsychotics,
antidepressants, antileptics,
Evaluation Cont.Family History: CNS disorders, Stroke/TIA, MH
issues Dementia, seizure disorders etc. Status of Family members:
Father, Mother, Siblings,childrenSocial History:Alcohol Occupation
SpiritualTobacco Armed forces Service Gambling Hobbies Education
Level Street Drugs Exercise
Evaluation cont.Review of Systems: Neurologic examCognitive
Test: MoCA, MMSE, SLUMS (I use the MoCA. Geriatric 15 question
depression scaleFunctional Assessment Staging (FAST Score)Labs :
CBC, Lytes, BUN/CR, Hepatic Panel, Magnesium, Calcium, RPR, UA,
Glucose/HgA1C, TSH, B12, Folate, Vitamin D, Heavy Metals if
indicated.Brain Imaging: CT of Head without or with/without
Contrast or Brain MRICognitive Performance Test and Driving
ScreenSometimes a Neurology consult, Neuro Psych, Speech Therapy
consult etc.
Rapid Plasma Reagin (RPR) refers to a type of test that looks
for non-specific antibodies in the blood of the patient that may
indicate that the organism (Treponema pallidum) that causes
syphilis is present.
35Making Sense out of the DataMaking a diagnosis is a process of
ruling in and ruling out differential diagnosis.At this time there
is no definitive test to diagnose Alzheimers Disease other than
autopsy.This includes frontal temporal dementiaLewy body
dementiaParkinsons Dementia
MRI and CT of Head can pick up stroke, masses, NPH.Staging
DementiaFAST Copyright 1984 by Barry Reisberg, M.DReproduced by
permission from Barry Reisberg, MD
Professor of Psychiatry Director, Fisher Alzheimers Disease
ProgramClinical Director, Aging & Dementia Clinical Research
CenterDirector, Clinical Core, NYU Alzheimers Disease CenterCenter
of Excellence on Brain Aging New York University Langone Medical
Center
Case Studies1st Case Study 2nd Case Study 3rd Case Study
Read case studies and discuss38
TreatmentMedications: For Alzheimers Disease , Parkinsons
Dementia, Lewy Body dementia, or Mixed Dementia (Vascular and
Alzheimers Disease)Cholinesterase InhibitorsAricept
(donepezil)Razadyne (galantamine)Exelon (Rivastigmine)
Namenda (memantine) N-Methyl D-Aspartate antagonist. Blocks
toxic effects ofGlutamate and regulates Glutamate activation
Co existing Depression Start antidepressant such as SSRI
Behaviors: Behavior management through behavior modification
preferredtypical and atypical antipsychotics (Be very cautious due
to increase risk of death. If so start low and go very slow)
ConclusionDementia is a functional diagnosis.
There are many causes, vulnerabilities, and diagnosis that lead
to dementia.
To determine the cause of dementia allows for proper treatment,
support, and education to your patients and their support
systems/family.Questions?