Embed Size (px)
Citation preview
Burkitt-Like Lymphoma Infiltrating a HyperfunctioningThyroid Adenoma and Presenting as a Hot Nodule
Antonella Camera,1 Flavia Magri,1 Rodolfo Fonte,1 Laura Villani,2 Matteo G. Della Porta,3
Vittorio Fregoni,4 Luigi La Manna,5 and Luca Chiovato1
Background: Most solitary hyperfunctiong regions on thyroid scan consist of benign tissue. Here we report apatient with a Burkitt-like lymphoma that was infilterated into a region containing a hyperfunctioning nodule.Summary: A 56-year-old man was referred to our Endocrine Unit in May 2009 due to the incidental discovery ofa large left thyroid lobe nodule by a computed tomography study. This had been performed to search for aprimitive tumor in a patient with bone metastasis. He was clinically and biochemically thyrotoxic with noevidence of humoral thyroid autoimmunity. The nodule had a dyshomogenous appearance at neck ultraso-nography, with multiple hypoechogenic areas and calcifications. (99m)-Technetium thyroid scintiscan revealed ahot nodule with suppression of the contralateral lobe. Fine-needle aspiration cytology indicated the presence ofneoplastic cells not of thyroid origin. Remission of hyperthyroidism was obtained with methimazole, and thepatient was submitted to left lobe thyroidectomy and istmectomy. Histological analysis of the surgical specimenled to a diagnosis of Burkitt-like large B-cell lymphoma harbored within a thyroid adenoma. After furtherstaging, the final diagnosis was stage IV E Burkitt-like lymphoma with the involvement of the bone and thethyroid. This is the first description of an aggressive Burkitt-like lymphoma that infiltrated an hyperfunctioningthyroid adenoma, thus presenting as a hot nodule at thyroid scintiscan. In our patient there was no humoral orhistological evidence of thyroid autoimmunity, thus suggesting a metastatic seeding of the lymphoma within thehyperfunctioning thyroid nodule.Conclusions: Involvement of the thyroid gland by Burkitt-like lymphoma is extremely rare as is close locali-zation of malignancy and a hyperfunctioning thyroid nodule. As highlighted by the present report, performingfine-needle aspiration cytology should be always considered in the clinical context of a metastatic disease ofunknown origin or when there are ultrasonography signs suggesting malignancy, even when the nodule ishyperfunctioning.
Introduction
Thyroid nodules are one of the most frequent findings inclinical endocrinology. Thyroid ultrasonography (US),
fine-needle aspiration cytology (FNAC), and scintigraphy arerecommended in some patients to evaluate these lesions. Lessthan 5% of all thyroid nodules are malignant. Of these, lym-phomas account for only 1%–5% of all thyroid cancers (1).Most thyroid lymphomas arise in a clinical and histologicalbackground of chronic autoimmune thyroiditis, usuallycharacterized by hypothyroidism, and most frequently pres-ent as cold nodules on thyroid scintiscan. Here we report anunusual thyrotoxic patient with a thyroid lymphoma that washidden in an hyperfunctioning thyroid nodule.
Patient
A 56-year-old man was referred to our Endocrine Unit inMay 2009 for evaluation of a thyroid nodule that was noted oncomputed tomography as part of the workup of a suspectedunderlying neoplasm. In January 2009 he suffered a patho-logical fracture of the right femoral diaphysis due to a lyticlesion of unknown origin. A computed tomography scan ofthe thoracic and abdominal districts revealed two smallnodules in the right kidney, an abnormal mass in the anteriormediastinum corresponding to the thymic area and a largenodule of the left thyroid lobe. In April 2009 the patient un-derwent an osteosynthesis of the right femoral diaphysis.At histology, the resected bone fragment was found to be
Units of 1Internal Medicine and Endocrinology and 2Pathology and Cytology, Fondazione Salvatore Maugeri IRCCS; 3Clinical Oncology,University of Pavia Medical School; 4Medical Oncology, 5Department of General and Mininvasive Surgery, Fondazione Salvatore MaugeriIRCCS; University of Pavia, Pavia, Italy.
THYROIDVolume 20, Number 9, 2010ª Mary Ann Liebert, Inc.DOI: 10.1089/thy.2010.0048
1033

extensively necrotic and to contain a neoplastic cell popula-tion, which was not further defined.
When first seen in our outpatient clinic, the patient ap-peared slightly thyrotoxic with fine tremors and sinus tachy-cardia, but no evidence of inflammatory eye disease. Neckpalpation revealed a firm, 5-cm nodule in the left thyroid lobe.The right thyroid lobe was barely palpable and there was noevidence of lymphoadenopathy. Thyroid function tests indi-cated overt thyrotoxicosis (thyrotropin< 0.004 mU/L, range0.4–4 mU/L; free thyroxine¼ 31.2 pg/mL, range 8.0–19.0 pg/mL; free triiodothyronine¼ 7.8 pg/mL, range 1.8–4.2 pg/mL). Tests for anti-thyroglobulin, anti-thyroid peroxidase,and anti-thyrotropin-receptor antibodies were negative.Serum thyroglobulin was high (434 ng/mL), and serum cal-citonin was undetectable (<2 pg/mL).
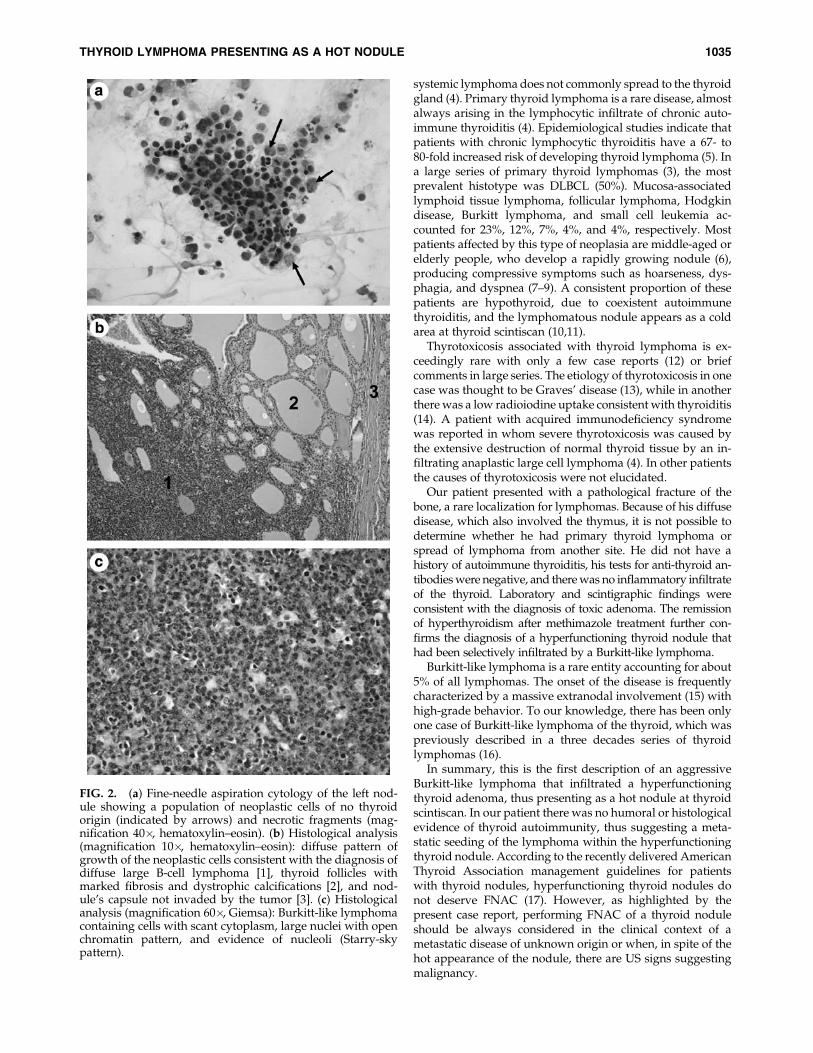
Neck US showed an asymmetrical thyroid with a huge leftlobe (estimated volume¼ 70 mL), which was almost com-pletely occupied by a large nodule measuring 46�49�60 mm.The nodule was not homogenous but contained multiple hypoand anechogenic areas, intralesional vascular spots, and calci-fications (Fig. 1a). A rightward tracheal dislocation was evi-dent. Due to the thyrotoxic state, a (99m)-technetium scintiscanwas ordered, which revealed a large hot nodule of the leftthyroid lobe. No radioisotope uptake was evident in the rightlobe. Thus, the nuclear medicine imaging was consistent with ahyperfunctioning thyroid nodule with suppression of thecontralateral lobe (Fig. 1b). FNAC of the left nodule was per-formed, which yielded a population of neoplastic cells thatwere not considered of thyroid origin (Fig. 2a). The patient wasstarted on methimazole (20 mg/day), with remission of hy-perthyroidism within 3 weeks. In June 2009, an 18-fluorodeoxyglucose positron emission tomography wasperformed, which showed a pathological uptake of the radio-isotope corresponding to the left thyroid nodule, as well as in
the mediastinum and right femur. Considering the malignantcytological findings and the surgical accessibility of the thyroidnodule, a left lobe thyroidectomy and istmectomy were per-formed. The thyroid nodule was easily resectable, with noevidence of adherence to the trachea or to other neck structures.Histological analysis led to the diagnosis of diffuse large B-celllymphoma (DLBCL) (1), with an high proliferation index (Ki-67> 95%) and a CD20/CD79a positivity. Given the high pro-liferation rate, it was classified as a Burkitt-like lymphoma (Fig.2b, c). The surgical specimen of the nodule also containedthyroid tissue with a macrofollicular appearance, markedfibrosis, and dystrophic calcifications. A nuclear magneticresonance of the brain excluded cerebral metastases. Furtherinvestigations involved the assay of serum lactate dehy-drogenase (1585 U/L, range 240–480 U/L) and b2-micro-globulin (2310 mg/L, range 609–2366 mg/L). A bone marrowbiopsy did not show malignant cells. The final diagnosis wasstage IV E Burkitt-like lymphoma according to the WHOclassification. According to the recent revision of the 2008WHO Classification (2), this lymphoma may alternately beincluded in the provisional category termed B-cell lymphoma,unclassifiable, with features intermediate between DLBCL andBurkitt lymphoma. The patient was treated with eight cycles ofintensive chemotherapy (hyperfractionated cyclophospha-mide, vincristine, doxorubicine, and dexamethasone), and haddramatic reduction of all lesions with improvement of symptoms.
Discussion
Lymphoma within the thyroid gland is a rare and hetero-geneous disease, accounting for 1%–5% of all thyroid cancersand occurring in 1%–2.5% of all lymphomas (3). Lymphomasmore commonly spread to lymph nodes, bone marrow, cen-tral nervous system, liver, and gastrointestinal tract. As noted,
FIG. 1. (a) Neck ultrasonography showing the left thyroid lobe almost completely occupied by a large nodule(46�49�60 mm), dyshomogeneous, with multiple hypo-anechogenic areas and calcifications. (b) (99m)-Technetium scintis-can consistent with an hyperfunctioning thyroid nodule in the left thyroid lobe, with suppression of the contralateral lobe.
1034 CAMERA ET AL.
systemic lymphoma does not commonly spread to the thyroidgland (4). Primary thyroid lymphoma is a rare disease, almostalways arising in the lymphocytic infiltrate of chronic auto-immune thyroiditis (4). Epidemiological studies indicate thatpatients with chronic lymphocytic thyroiditis have a 67- to80-fold increased risk of developing thyroid lymphoma (5). Ina large series of primary thyroid lymphomas (3), the mostprevalent histotype was DLBCL (50%). Mucosa-associatedlymphoid tissue lymphoma, follicular lymphoma, Hodgkindisease, Burkitt lymphoma, and small cell leukemia ac-counted for 23%, 12%, 7%, 4%, and 4%, respectively. Mostpatients affected by this type of neoplasia are middle-aged orelderly people, who develop a rapidly growing nodule (6),producing compressive symptoms such as hoarseness, dys-phagia, and dyspnea (7–9). A consistent proportion of thesepatients are hypothyroid, due to coexistent autoimmunethyroiditis, and the lymphomatous nodule appears as a coldarea at thyroid scintiscan (10,11).
Thyrotoxicosis associated with thyroid lymphoma is ex-ceedingly rare with only a few case reports (12) or briefcomments in large series. The etiology of thyrotoxicosis in onecase was thought to be Graves’ disease (13), while in anotherthere was a low radioiodine uptake consistent with thyroiditis(14). A patient with acquired immunodeficiency syndromewas reported in whom severe thyrotoxicosis was caused bythe extensive destruction of normal thyroid tissue by an in-filtrating anaplastic large cell lymphoma (4). In other patientsthe causes of thyrotoxicosis were not elucidated.
Our patient presented with a pathological fracture of thebone, a rare localization for lymphomas. Because of his diffusedisease, which also involved the thymus, it is not possible todetermine whether he had primary thyroid lymphoma orspread of lymphoma from another site. He did not have ahistory of autoimmune thyroiditis, his tests for anti-thyroid an-tibodies were negative, and there was no inflammatory infiltrateof the thyroid. Laboratory and scintigraphic findings wereconsistent with the diagnosis of toxic adenoma. The remissionof hyperthyroidism after methimazole treatment further con-firms the diagnosis of a hyperfunctioning thyroid nodule thathad been selectively infiltrated by a Burkitt-like lymphoma.
Burkitt-like lymphoma is a rare entity accounting for about5% of all lymphomas. The onset of the disease is frequentlycharacterized by a massive extranodal involvement (15) withhigh-grade behavior. To our knowledge, there has been onlyone case of Burkitt-like lymphoma of the thyroid, which waspreviously described in a three decades series of thyroidlymphomas (16).
In summary, this is the first description of an aggressiveBurkitt-like lymphoma that infiltrated a hyperfunctioningthyroid adenoma, thus presenting as a hot nodule at thyroidscintiscan. In our patient there was no humoral or histologicalevidence of thyroid autoimmunity, thus suggesting a meta-static seeding of the lymphoma within the hyperfunctioningthyroid nodule. According to the recently delivered AmericanThyroid Association management guidelines for patientswith thyroid nodules, hyperfunctioning thyroid nodules donot deserve FNAC (17). However, as highlighted by thepresent case report, performing FNAC of a thyroid noduleshould be always considered in the clinical context of ametastatic disease of unknown origin or when, in spite of thehot appearance of the nodule, there are US signs suggestingmalignancy.
FIG. 2. (a) Fine-needle aspiration cytology of the left nod-ule showing a population of neoplastic cells of no thyroidorigin (indicated by arrows) and necrotic fragments (mag-nification 40�, hematoxylin–eosin). (b) Histological analysis(magnification 10�, hematoxylin–eosin): diffuse pattern ofgrowth of the neoplastic cells consistent with the diagnosis ofdiffuse large B-cell lymphoma [1], thyroid follicles withmarked fibrosis and dystrophic calcifications [2], and nod-ule’s capsule not invaded by the tumor [3]. (c) Histologicalanalysis (magnification 60�, Giemsa): Burkitt-like lymphomacontaining cells with scant cytoplasm, large nuclei with openchromatin pattern, and evidence of nucleoli (Starry-skypattern).
THYROID LYMPHOMA PRESENTING AS A HOT NODULE 1035

Disclosure Statement
The authors declare that they have nothing to disclose.
References
1. Delsol G 2008 The 2008 WHO lymphoma classification. AnnPathol 28:S20–S24.
2. Jaffe ES 2009 The 2008 WHO classification of lymphomas:implications for clinical practice and translational research.Hematology Am Soc Hematol Educ Program 523–531.
3. Thieblemont C, Mayer A, Dumontet C, Barbier Y, Callet-Bauchu E, Felman P, Berger F, Ducottet X, Martin C, SallesG, Orgiazzi J, Coiffier B 2002 Primary thyroid lymphoma is aheterogeneous disease. J Clin Endocrinol Metab 87:105–111.
4. Samuels MH, Launder T 1998 Hyperthyroidism due tolymphoma involving the thyroid gland in a patient withacquired immunodeficiency syndrome: case report and re-view of the literature. Thyroid 8:673–677.
5. Holm LE, Blomgren H, Lowhagen T 1985 Cancer risks inpatients with chronic lymphocytic thyroiditis. N Engl J Med312:601–604.
6. Kalinyak JE, Kong CS, McDougall IR 2006 Burkitt’s lym-phoma presenting as a rapidly growing thyroid mass.Thyroid 16:1053–1057.
7. Hamburger JI, Miller JM, Kini SR 1983 Lymphoma of thethyroid. Ann Intern Med 99:685–693.
8. Oertel JE, Heffess CS 1987 Lymphoma of the thyroid andrelated disorders. Semin Oncol 14:333–342.
9. Matsuzuka F, Miyauchi A, Katayama S, Narabayashi I,Ikeda H, Kuma K, Sugawara M 1993 Clinical aspects ofprimary thyroid lymphoma: diagnosis and treatment basedon our experience of 119 cases. Thyroid 3:93–99.
10. Hardoff R, Bar-Shalom R, Dharan M, Luboshitsky R 1995Hodgkin’s disease presenting as a solitary thyroid nodule.Clin Nucl Med 20:37–41.
11. Hervas Benito I, Vera Espallardo F, Saura Quiles A, Gon-zalez Cabezas P, Bello Arques P, Rivas Sanchez A, Alonso
Monfort J, Perez Velasco R, Mateo Navarro A 2001 Thyroidscintigraphy and body scanning with 67 Ga in a caseof primary thyroid lymphoma. Rev Esp Med Nucl 20:
462–465.12. Jennings AS, Saberi M 1984 Thyroid lymphoma in a patient
with hyperthyroidism. Am J Med 76:551–552.13. Zeki K, Eto S, Fujihira T, Masuda M, Oda S, Chiba S, Suzuki
H 1985 Primary malignant lymphoma of the thyroid in apatient with long-standing Graves’ disease. Endocrinol Jpn32:435–440.
14. Shimaoka K, VanHerle AJ, Dindogru A 1976 Thyrotoxicosissecondary to involvement of the thyroid with malignantlymphoma. J Clin Endocrinol Metab 43:64–68.
15. Ferry JA 2006 Burkitt’s lymphoma: clinicopathologic fea-tures and differential diagnosis. Oncologist 11:375–383.
16. Lam KY, Lo CY, Kwong DL, Lee J, Srivastava G 1999 Ma-lignant lymphoma of the thyroid. A 30-year clinicopatho-logic experience and an evaluation of the presence ofEpstein-Barr virus. Am J Clin Pathol 112:263–270.
17. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL,Mandel SJ, Mazzaferri EL, McIver B, Pacini F, SchlumbergerM, Sherman SI, Steward DL, Tuttle RM 2009 RevisedAmerican thyroid association management guidelines forpatients with thyroid nodules and differentiated thyroidcancer. Thyroid 11:1167–1214.
Address correspondence to:Luca Chiovato, M.D., Ph.D.
Unit of Internal Medicine and EndocrinologyFondazione Salvatore Maugeri IRCCS
University of PaviaVia S. Maugeri 10
I-27100 PaviaItaly
E-mail: [email protected]
1036 CAMERA ET AL.