ORIGINALARTICLEsbr_473
274..281StructurevalidityofthePittsburghSleepQualityIndexinrenaltransplantrecipients:AconrmatoryfactoranalysisHannaBURKHALTER,1SusanMSEREIKA,2SandraENGBERG,3AnnaWIRZ-JUSTICE,4JrgSTEIGER5andSabinaDEGEEST11InstituteofNursingScience,UniversityofBasel,4CenterforChronobiology,PsychiatricUniversityClinic,and5DivisionofTransplantImmunologyandNephrology,UniversityHospitalBasel,Basel,Switzerland;and2DepartmentsofHeathandCommunitySystemsandBiostatistics,SchoolofNursingandGraduateSchoolofPublicHealth,and3DepartmentofHealthPromotion&Development,SchoolofNursing,UniversityofPittsburgh,PA,USAAbstractTheprimaryaimof
this studywas tot andtest thehypothesizedthree-factor model of
thePittsburgh Sleep Quality Index (PSQI) reported by Cole (2006) in
renal transplant (RTx) recipients. Weconductedacross-sectional
descriptivestudyusingaconveniencesampleofhome-dwellingRTxrecipients,
transplanted 6 months to 5 years prior to initiation of the study.
Of the 135 RTx patientsmeeting the inclusion criteria, 29% were
women with a mean age of 52 years (SD: 12; range: 21 to76). The
PSQI and a structured demographic questionnaire were mailed to the
patients homes.
Weconductedaconrmatoryfactoranalysistotandtestasingle-factormodelproposedbyBuysse(1989)aswell
astheCole(2006)three-factormodel.Conrmatoryfactoranalysisprovidedweakempirical
support for the three-factor model (c2= 16.555, d.f. = 8, P <
0.0351; RMSEA = 0.089;WRMR = 0.492;CFI =
0.983).Posthocexplorationofthethree-factormodelindicatedtheinclusionofanadditional
pathfromsleep-medicationitemstothefactorofsleepefciency,whichdemon-strated
an improved t (c2= 11.850, d.f. = 8, P = 0.408; RMSEA = 0.060; WRMR
= 0.384; CFI = 0.992).Conrmatory factor analysis suggests that the
three-factor model of the PSQI has a better t than
theoriginalone-factormodel,andtheadditionalpathwaymayimproveitst.Thethree-factormodelwiththeadditionalpathshouldbetestedinanewsamplebeforeuseinRTxrecipients.Keywords:conrmatoryfactoranalysis,daytimedisturbances,renaltransplantation,sleepefciency,sleepquality.INTRODUCTIONRenal
transplant (RTx) recipients are chronically illpatients confronted
with side effects of the immunosup-pressive regimen, which causes
signicant co-morbidity,including cardiovascular complications,1de
novo
malig-nancies,2andinfections.3Ithasalsobecomeclearthatsleepwake
disregulation leads to insomnia and/orexcessive daytime
sleepiness.4The detrimental effects ofsleepwake disregulation have
been well documented inhealthy patients and include metabolic
derangements,5cardiovascular disease,6coronary artery
calcication,7depression,8chronicinammation9andanincreaseinmortality.10In
the chronically ill, for example in heart-failurepatients,
daytimesleepiness is associatedwithpoor self-care11,12andindialysis
patients poor
sleepqualityisassociatedwithincreasedmortality.13InRTxCorrespondence:
Dr Sabina De Geest, Institute of NursingScience, University of
Basel, Bernoullistrasse 28, CH-4056Basel, Switzerland. Email:
[email protected] 12 September 2010.Sleep and
Biological Rhythms 2010; 8: 274281
doi:10.1111/j.1479-8425.2010.00473.x274 2010 The AuthorsSleep and
Biological Rhythms 2010 Japanese Society of Sleep
Researchrecipients sleep impairments are associated with adecreased
emotional state,14increased psychologicalproblems,
co-morbidities,15anddecreasedquality oflife.1517The Pittsburgh
Sleep Quality Index (PSQI) is a widelyused19-itemself-report
questionnaire that measuressleep disturbances. Seven clinically
derived domains ofsleepdifculties are assessedbythe PSQI.
Together,these sleep domains are scored as a single factor
namedSleep Quality (SQ). Psychometric properties of the
PSQIhavebeenexaminedandfoundtobeappropriateinrelationto internal
consistency,18,19concurrent
valid-ity19,20anddiscriminativevalidity19,20inhealthyandillpopulations.Coleet
al.(2006)21examinedthefactorstructureofthe PSQI using a
cross-validation approach. An
explor-atoryfactoranalysisincommunity-dwellingdepressedand
non-depressed older adults was followed by
aconrmatoryfactoranalysistoascertainthereproduc-ibility of the
factor structure. They identied and
con-rmedathree-factorstructureof thePSQI (basedonthe conrmatory
factor analysis, all t indices weregood) andrecommendedthat this
model beusedtodocument disturbances in three separate factors
ofsubjectivesleep: (i) perceivedSQ(ii) daytimedistur-bances
and(iii) sleepefciency. Another study
withNigerianstudents22conrmedColesndings.In previous studies, the
prevalence of poor SQ in RTxrecipients assessedwiththe
PittsburghSleepQualityIndex (PSQI) ranged from 30% to
62%.14,15,23Despite itsuse in this population, the PSQI has not
been validatedin RTx recipients.It is likely that the one-factor
model of Buysse(1989)18will not fully capture the
multidimensionalnature of sleep disturbance in RTx recipients.
Wehypothesizethatathree-factormodelsimilartoColesmodel will better
represent thesleepdisturbances inthis population. Our rationale for
this belief is thereported high prevalence of depression and
anxietyamong RTx recipients. A quarter of RTx recipientshave
depression (prevalence ranging from5%24to25%25) or
anxiety(prevalencerangingfrom15%25to70%26). Fear of losing the
transplanted kidney throughrejection is a common source of anxiety.
While weexpect the factor structure inour populationto besimilar
tothat reportedby Cole et al., the way thatsleep drugs relate to
other items may differ because theutilizationof these agents inthe
RTx populationislikely to differ from their use in the
populationColestudied.
Somesleepdrugsinterferewithimmu-nosuppressants,27so clinicians may
be less likely toprescribe them for these patients than for other
patientgroups.This study aims to assess whether the one-factormodel
proposed conceptually by Buysse18or the three-factor model identied
by Cole21best captures the mul-tidimensional nature of sleep
disturbance in
RTxrecipients.METHODSParticipantsThisstudyusedacross-sectionaldescriptivedesignina
single RTx center. Aconvenience sample of 217community-dwelling
adult RTx recipients who receivedrenal transplants at the
UniversityHospital inBasel,Switzerland were included. The inclusion
criteria were:(i) rst RTx, (ii) between6 months and5 years
posttransplant, (iii) ability to understand and read German,(iv)
more thaneighteenyears of age andwilling toprovide written informed
consent. Patients wereexcluded if they had had a combined
transplant, lackedmental claritybasedontheir clinicians appraisal,
orcould not read the questions.MeasuresDemographic and clinical
dataBasic demographic data (i.e. age [years]
andgender[male/female])wereretrievedfrommedicallesintheUniversityHospital
inBasel, Switzerlandandfromastructuredself-report
questionnairedevelopedfor theSwiss Transplant Cohort Study (STCS).
Sociodemo-graphicvariablesincludedhighest completedlevel
ofeducation (no completed school, mandatory school,apprenticeship,
general qualication for Universityentrance, higher professional
education, higher techni-cal or commercial school, university,
other); currentoccupation or last professional position
(self-employed,working ina relatives rmor business,
apprentice/trainee, director/manager, middle/lower
management,employee, househusband/-wife, student,
other);workingcapacity(percentageof timeworkedforpayduring the past
6 months); marital status (single,married/living together,
widow[er], divorced/separated); and monthly income in Swiss francs
(CHF)(1CHF = 0.90USD):9001).Validity of the PSQI275 2010 The
AuthorsSleep and Biological Rhythms 2010 Japanese Society of Sleep
ResearchPittsburgh Sleep Quality IndexThePSQI consistsof
19self-ratedquestionsandvequestionsratedbythebedpartnerorroommate.
Thelatter vequestions areusedfor clinical
informationonlyandarenotincludedinthescoringofthePSQI.The
19self-ratedquestions assess a wide variety
offactorsandaregroupedintosevencomponentscores,each weighted
equally on a 03 scale. According to thescoring guidelines provided
by Buysse et al. (1989), the19items are
analyzedtoyield7sleepcomponents:subjectivesleepquality,
sleeplatency, sleepduration,habitual sleep efciency, sleep
disturbances, use ofsleeping medications, and daytime dysfunction.
Thesevencomponent
scoresarethensummedtoyieldaglobalPSQIscore,whichrangesfrom0to21.Higherscores
indicate poorer SQ.18The PSQI has shown favorable psychometric
proper-ties in previous research with internal consistency
coef-cients rangingfrom0.8019to0.8318andtestretestcorrelation
coefcients from 0.8518to 0.8720in healthy,depressive, insomnia,
cancer and transplant popula-tions. Convergent validity has
beenestablishedwithother self-report measures of sleep19and sleep
logs.20AtotalPSQIscoreof5ormoreshowedgoodsensitivityand specicity
for the identication of poor versus goodSQwhentestedagainst
polysomnography.20Backhauset al.20reportedaCronbachsaof 0.85,
atestretestreliability coefcient of 0.87, a sensitivity ranging
from80% to 100% and a specicity ranging from 80 to 83%in German
patients with primary insomnia.Data collectionThe studyreceivedthe
approval of the Ethics Com-mittee of Basel. The subjects signed an
informedconsent form prior to participation. Data
werede-identiedandstoredinananonymous electronicdatabase.
Questionnaires were placed in a lockedcabinet for security. Data
collectiontookplace fromSeptember 2008 to November 2008. Addresses
andtelephone numbers of all patients who fullled the eli-gibility
criteria were extracted fromthe UniversityHospital in Basel
database, and eligible patientsreceiveda short letter describingthe
purpose of thestudy. If a patient was willing to participate in
thestudy he/she signed the written informed consent form(two
copies, one for the patient and one for
theresearcher)andlledoutthequestionnaires.Allques-tionnaireshadauniqueidentierthatallowedidenti-cation
of patients by the investigator. Patients sent
thecompletedquestionnairesbackinapre-stamped, pre-addressed
envelope. Patients who had not returnedtheir questionnaires after
30 days received a mailedreminder tocompletethequestionnaires.
Thosewhodidnot respondwithin10 days receiveda remindertelephone
call. If the completedquestionnaires werenot
returnedafterthetelephonecall, thepatient
wasconsideredanon-responder.Data management and analysisData were
entered twice in the data managementpackage SPSS and checked for
inconsistencies betweentheentries. All
discrepancieswerecomparedwiththeoriginal data and
corrected.Exploratoryanddescriptivedataanalyseswereper-formedusingSPSSsoftwareversion14.0(SPSS,
Inc.,Chicago, IL, USA). Exploratory analyses entailed screen-ing
for univariate and multivariate outliers and theevaluation of
missing data in terms of the amount andpattern of missingness.
Missing data analysis examinedthe variables of the education,
profession, work capacity,marital status, socioeconomic status and
PSQI in termsof missingnessandtheobservedvaluesof thesevari-ables.
Littles MCAR test was used to assess whether
themissingnesswascompletelyatrandom(MCAR).28ForLittles MCARtest,
anon-signicant ndingprovidessome support for the
MCARassumptionandthat alistwise deletion approach may be
reasonable. Descrip-tive statistics were calculated as frequencies
(%) for cat-egorical variables, while continuous interval or
ratioscaled variables were summarized using means andstandard
deviations (or medians and inter-quartileranges (IQR),
respectively, if datawerenon-normallydistributed and/or extreme
values were present). Group-comparative statistics (two-sample
t-test for approxi-mately normally distributed interval- or
ratio-scaledsubject descriptors, Mann-WhitneyU-test for
ordinalscaledor non-normallydistributedinterval- or
ratio-scaledvariables, andchi-squaretestsof independencefor
nominally scaled characteristics) were used tocompare the subgroups
of responders and non-responders and subjects and dropouts. All
tests ofhypotheses were two-tailed and the level of signicancewas
set at 0.05.Conrmatoryfactor analysis (CFA) was conductedusing
Mplus (version 5.21, 2007 Muthen & Muthen) onthe seven
component scores, given the different scalingand non-linear
transformation from item responses intocomponent scores. Through
CFA we analyzed
thesingle-factorscoringmodeloriginallyproposedbytheH Burkhalter et
al.276 2010 The AuthorsSleep and Biological Rhythms 2010 Japanese
Society of Sleep Researchdeveloper of
thescale.18Wealsoanalyzedthethree-factormodel
suggestedbyCole.21Multiplet indiceswere used to determine adequate
model t:29compara-tive t index (CFI); weighted root mean square
residual(WRMR); androotmeansquarederrorofapproxima-tion(RMSEA).
Finallythemodels werecomparedtoeach other by delta chi-squared
(Dc2) statistics to deter-mine whichbest t the data. The cutoffs
suggestinggood t are: RMSEA < 0.05 (0.05 < RMSEA < 0.08
indi-cates adequate model t; RMSEA 0.08 suggests poormodel t); CFI
close to 1 (CFI > 0.95 indicates good t);andWRMRvalue less
than0.90. Asignicant
chi-squareindicateslackofsatisfactorymodelt.Thatis,the chi-square
test statistic used in modeling tting is agoodness of t measure in
that a nding of statisticalsignicance means the estimated
covariance/correlationstructurebasedonthemodel
issignicantlydifferentfromthe observed covariance/correlation
matrix.30,31Modication indices are generated by the
softwarepackage; theyaredata-drivenindicatorsofchangestothe model
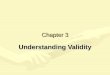
that are likely to improve model t.RESULTSThe sample ow is shown in
Figure 1. Out of the 217eligible patients, 156 (72%) returned the
questionnairepackets. Of these, only 135 (68%) fully completed
thePSQI. Non-respondents (n = 61; 28%) were signi-cantly older than
respondents (t = 2.9, d.f. = 214,P =
0.004).Therewerenosignicantdifferencesinthepatientswho did not
completely ll out the PSQI (n = 21) andthose who did (n = 135).
Therefore we chose a listwisedeletionandhada 13%sample drop-out
rate. TheLittles MCARtest (c2= 42.455, d.f. = 45P =
0.580),demonstratedthat themissingness of datawas com-pletelyat
random, further
supportingthedecisiontoincludeonlythosesubjectswhocompletelylledoutthe
PSQI.Thesample(N = 135)included94men(70%)and41 women (30%) with a
median age of 52 years (IQR:19). Median time since transplantation
was 2 years(IQR: 3). Nineteenpercent of the subjects (N = 14)had
more than one co-morbidity. A third (N = 45)were unemployed, while
two-thirds (N = 89) weremarriedor livingwitha signicant other. The
PSQIglobal score for the 135 subjects ranged from 1 to
19,withamedianof 5(IQR:5). Usingtherecommendedcutoff point of 5,
47.4%(N = 64) of the subjectsreported poor SQ. Table 1 displays the
descriptive sta-tisticsforthesevenPSQI
componentsandthecorre-lations betweenthe components. Eachof the
scoresrangedfrom0to3. Thelowest inter-component cor-relation was
between the use of sleep medication andsleepduration(r =
0.14)andthehighestcorrelationwas between sleep efciency and sleep
duration(r = 0.73).The t statistics for the single-factor model
proposedby Buysse18universally indicated a poor t with the data(c2=
51.850, P < 0.0001; RMSEA = 0.188; WRMR =1.024; CFI = 0.915).
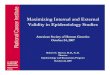
Wealsottedthehypothesizedthree-factor model published by Cole21and
Aloba.22Thethree-factor model, displayed in Figure 2, also
demon-stratedpoort,buttoalesserextentthattheoriginalone-factor
model (c2= 16.555; P < 0.0351; RMSEA =0.089;WRMR = 0.492;CFI =
0.983).Therelationshipof eachPSQI component score toits
correspondingfactor was signicant and large ranging from
standard-izedpathcoefcients of 0.56 (daytime disturbancesto daytime
function factor) to 0.99 (habitual sleepAssessed for eligibility (n
= 236)EnrolmentMailed questionnaires (n = 217)Analysis Excluded (n
= 61) Not responding to letter and questionnaireExcluded (n = 19)
Other reasons (n = 0) Declined to participate (n = 0)Not meeting
inclusion criteria (n = 19)Returned questionnaires (n =
156)Analysed (n = 135)Excluded (n = 21) Listwise deletion Figure
1Flow diagram of thesample.Validity of the PSQI277 2010 The
AuthorsSleep and Biological Rhythms 2010 Japanese Society of Sleep
Researchefciency to sleepefciency factor). The
correlationbetweenthefactors rangedfrom0.52(medium-largeeffect) to
0.81 (large effect).32Model modication indices for the three-factor
modelpointedtosome sources of poor t, specically thepossible
cross-loadingof the sleepdrugs componenton the sleep efciency
factor(Dc2= 6.646 improve-ment). The three-factor model with the
additional pathfrom the sleep efcency factor to sleep drugs
componentshowed very good t based on all t indices(c2= 11.850, P =
0.408; RMSEA = 0.060; WRMR =0.384; CFI = 0.992) (Fig. 3 and Table
2). The relation-ship between each PSQI component score and
itscorrespondingfactorwassignicantandlargerangingfromthe
standardized path coefcients of b = 0.51(sleepefciencyfactor
tosleepdrugs component) to1.088 (perceivedsleepquality factor to
sleepdrugscomponent). The correlation between the
factorsrangedfrom0.53(medium-largeeffect)to0.80(largeeffect).DISCUSSIONThis
study is the rst to assess the PSQI factor scoringstructure in the
RTx population. A three-factor scoringmodel
isfavoredoverasinglescore. Congruent withprevious research, we
showed that the three-factormodel showedgoodt criteria, aside
fromRMSEA,chi-square and a possible cross-loading indicated by
themodication indices. For this reason we continued themodeling and
added a path from sleep drugs to the sleepefcency factor. The model
with the modied pathshowed very good t criteria.The three-factor
scoring model shows that per-ceived sleep quality, daytime
disturbances andTable 1PSQI component correlations and descriptive
statistics1 2 3 4 5 6 71. Subjective sleep quality 12. Sleep
latency 0.55 13. Sleep duration 0.53 0.44 14. Habitual sleep
efciency 0.56 0.44 0.73 15. Sleep disturbances 0.52 0.43 0.19 0.35
16. Use of sleep medications 0.42 0.40 0.14 0.30 0.32 17. Daytime
disturbances 0.36 0.22 0.18 0.28 0.41 0.21 1Mean 0.96 1.16 0.55
0.74 1.26 0.33 1.01Standard deviation 0.72 0.96 0.87 1.01 0.59 0.85
0.86Median 1 1 0 0 1 0 1IQR 01 02 01 01 12 00 01Correlations of the
seven components of the PSQI, provided for descriptive
purposes..810 .991 .632 .681 .944 .840Sleep durationE3Sleep
efficiencySleep efficiencyE4Subjective sleep qualityE1Sleep
latencyE2Sleep drugsE6Sleep disordersE5Daytime
disturbancesE7Daytime function Perceived sleep quality .926 .562
.741 .523 Figure 2Three-factor model on thesamplehavingcompletePSQI
data(n = 135).H Burkhalter et al.278 2010 The AuthorsSleep and
Biological Rhythms 2010 Japanese Society of Sleep Researchsleep
efciency are three correlated concepts thatcover patientssleep
experience. Our ndings are con-sistent withthestudyof Coleet al.
(2006)21andthestudyof Alobaet al. (2007)22inthat
thethree-factormodel wasabettertthanasingle-factormodel. Wedidnot,
however, ndt indices as goodas thosefoundby Cole. This couldbe
relatedtothe use ofdifferent analysisapproachesaswell
asdifferencesinsamples. We hadskeweddata anduseda
statisticalprogramfor the CFAthat can handle ordinal data.Further,
our sample has completelydifferent charac-teristics: they live with
a new organ, take a lot of
medi-cationandcontinuetofearorganrejectionorloss.Theadditionof
apathpredictingsleepmedicationfromthesleepefciencyfactor
signicantlyimprovesthemodel.
Thesleepmedicationcomponentiscorre-latedwiththe factors of
perceivedsleepqualityandsleepefciency.Thecomponentofsleepmedicationisbased
on only one itemasking During the pastmonth, howoften have you
taken medicine (Pre-scribedor over thecounter)
tohelpyousleep(NotduringthePast month/ Lessthanonceaweek/ Onceor
twice a week/ Three or more times a week)?. Whensubjects in our
study took sleep medications more fre-quently, they perceiveda
decrease inthe quality oftheir sleep (b = 1088). In contrast their
perceived sleepefciencyimproved(b = 0.51). Themeaningof
theseresultsisnot clear: it couldbethat
sleepinducedbymedicationisnot thesameasnatural
sleepandthusperceiveddifferently. Wesuggest
clarifyingtheminafurther study. The model modication was post hoc
andmayhavecapitalizedonchance.
Ideallytheseresultsshouldbecross-validatedwithanewsample.This study
has several limitations. First, the data werecollectedanonymously.
Consequentlyit wasnot pos-sible to call the patient to obtain
missing data.
Second,alargersamplesize(>200)wouldhaveincreasedtheprecisionof
theestimators fromtheCFA(e.g. factorloadings, factor correlations,
etc.) and hence ultimatelythe stability of the estimators further
validating thethree-factor model. Third, our sample consisted
ofpatients who were 6 months to 5 years
post-transplant.Intherstyearfollowingtransplantationanumberofpredisposing(e.g.corticosteroiddrugs)andprecipitat-ing
factors (e.g. anxiety, stress) can increase the risk
ofpoorsleep.Aftertherstyeartherearefewerprecipi-tatingfactors, but
thereis theriskthat sleepdistur-bancesduringtherstyearcontinue.
Alargersamplewouldhave permittedus todoa stratiedanalysis.Lastly,
this study was cross-sectional and does not.801 .773 .532 .934
-.513 .985 .924 .677 1.088 .846Sleep durationE3Sleep
efficiencySleep efficiencyE4Subjective sleep qualityE1Sleep
latencyE2Sleep drugsE6Sleep disordersE5Daytime
disturbancesE7Daytime function Perceived sleep quality .557 Figure
3Three-factor model withadditional path, suggested frommodication
indices.Table 2Fit statistics of the three modelsModel d.f.Number
offree parameters c2(P-value) RMSEA WRMR CFI1-Factor 9 28 51.850 (P
< 0.000) 0.188 1.024 0.9153-Factor8 31 16.555 (P = 0.035) 0.089
0.492 0.9833-Factor8 31 11.850 (P = 0.041) 0.060 0.384
0.992Bestmodel,exceptforRMSEA;Modicationindices.CFI,ComparativeFitIndex;RMSEA,RootMeanSquareErrorofApproximation;WRMR,
Weighted Root Mean Square Residual d.f. = Degrees of freedom. c2=
Chi-square goodness-of-t statistic.Validity of the PSQI279 2010 The
AuthorsSleep and Biological Rhythms 2010 Japanese Society of Sleep
Researchprovide any information on the persistence of the
three-factor structure over time.CONCLUSIONConrmatory factor
analysis suggests that the three-factor model of the PSQI
mayholdpromise for thesubjective assessment of SQ in RTx
recipients.
Furtherconrmatoryworkisneededtoinvestigatethethree-factor model
with the additional path.TRANSPARENCY
DECLARATIONTheauthorshavehadnoinvolvement, nancial inter-ests or
arrangements, any other nancial connections, orother situations,
direct or indirect, that might raise thequestion of bias in the
work reported.REFERENCES1Ojo AO. Cardiovascular complications after
renal trans-plantationandtheir prevention. Transplantation2006;82
(5): 60311.2KauffmanHM, CherikhWS, McBride MA, Cheng Y,Hanto DW.
Post-transplant de novo malignancies
inrenaltransplantrecipients:thepastandpresent.Trans-plant. Int.
2006; 19 (8): 60720.3Parasuraman R, Yee J, Karthikeyan V, del Busto
R. Infec-tiouscomplicationsinrenal transplant recipients.
Adv.Chronic. Kidney Dis. 2006; 13 (3): 28094.4American Academy of
Sleep Medicine. The InternationalClassication of Sleep Disorders,
Diagnostic and CodingManual, 2nd edn. American Academy of Sleep
Medicine:Weschester,
ILinassociationwiththeEuropeanSleepResearchSociety, Japanese
Society of SleepResearch,Latin American Sleep Society;
2006.5KnutsonKL, Spiegel K, PenevP, VanCauter E. Themetabolic
consequences of sleep deprivation. Sleep Med.Rev. 2007; 11 (3):
16378.6YndestadA, DamasJK, OieE, UelandT, GullestadL,Aukrust P.
Roleof inammationintheprogressionofheart failure. Curr. Cardiol.
Rep. 2007; 9 (3): 23641.7KingCR, KnutsonKL, Rathouz PJ, SidneyS,
LiuK,Lauderdale DS. Short sleep duration and incident
coro-naryarterycalcication. JAMA2008; 300(24): 285966.8Benedetti F,
Bernasconi A, Blasi Vet al. Neural andgenetic correlates of
antidepressant response tosleepdeprivation: a functional magnetic
resonance imagingstudyof moral
valencedecisioninbipolardepression.Arch. Gen. Psychiatry 2007; 64
(2): 17987.9Frey DJ, Fleshner M, Wright KP Jr. The effects of40
hours of total sleep deprivation on
inammatorymarkersinhealthyyoungadults. BrainBehav. Immun.2007; 21
(8): 10507.10CappuccioFP,DEliaL,StrazzulloP,MillerMA.Sleepduration
and all-cause mortality: a systematic review andmeta-analysis of
prospective studies. Sleep 2010; 33 (5):58592.11Riegel B, Weaver
TE. Poor sleep and impaired self-care:towards acomprehensivemodel
linkingsleep, cogni-tion, and heart failure outcomes. Eur. J.
Cardiovasc. Nurs.2009; 8 (5): 33744.12Riegel B, Vaughan Dickson V,
Goldberg LR, Deatrick JA.Factors associatedwiththe development of
expertiseinheartfailureself-care.Nurs.Res.2007;56(4):23543.13ElderSJ,PisoniRL,AkizawaTet
al.Sleepqualitypre-dictsqualityoflifeandmortalityriskinhaemodialysispatients:
results from the Dialysis Outcomes and PracticePatterns Study
(DOPPS). Nephrol. Dial. Transplant. 2008;23 (3): 9981004.14Kachuee
H, Ameli J, Taheri S et al. Sleep quality and itscorrelatesinrenal
transplant patients. Transplant. Proc.2007; 39 (4):
10957.15Sabbatini M, CrispoA, Pisani Aet al.
Sleepqualityinrenaltransplantpatients:aneverinvestigatedproblem.Nephrol.
Dial. Transplant. 2005; 20 (1): 1948.16Diaz-Atauri MJ, Ausin P,
Sayas J, Torralba FG, Morales J.Conrming high prevalence of
patients with a high riskfor obstructive sleep apnoea syndrome
after kidneytransplantation. Nephrol. Dial. Transplant. 2008; 23
(4):14589; author reply 9.17Molnar MZ, NovakM, Mucsi I.
Sleepdisorders andqualityof lifeinrenal transplant recipients. Int.
Urol.Nephrol. 2009; 41 (2): 37382.18Buysse DJ, Reynolds CF3rd,
MonkTH, BermanSR,KupferDJ. ThePittsburghSleepQualityIndex:
anewinstrument for psychiatric practice and research. Psychia-try
Res. 1989; 28 (2): 193213.19Carpenter JS, Andrykowski MA.
Psychometricevalua-tion of the Pittsburgh Sleep Quality Index. J.
Psychosom.Res. 1998; 45 (1 Spec No): 513.20Backhaus J, Junghanns K,
Broocks A, Riemann D,Hohagen F. Test-retest reliability and
validity of thePittsburghSleepQuality Index inprimary insomnia.J.
Psychosom. Res. 2002; 53 (3): 73740.21Cole JC, Motivala SJ, Buysse
DJ, Oxman MN, Levin MJ,Irwin MR. Validation of a 3-factor scoring
model for thePittsburgh sleep quality index in older adults.
Sleep2006; 29 (1):
11216.22AlobaOO,AdewuyaAO,OlaBA,MapayiBM.Validityof the
PittsburghSleepQuality Index (PSQI)
amongNigerianuniversitystudents. SleepMed. 2007;
8(3):26670.23Eryilmaz MM, Ozdemir C, Yurtman F, Cilli A, KaramanT.
Quality of sleep and quality of life in renal transplan-tation
patients. Transplant. Proc. 2005; 37 (5): 20726.H Burkhalter et
al.280 2010 The AuthorsSleep and Biological Rhythms 2010 Japanese
Society of Sleep Research24Dobbels F, Skeans MA, Snyder JJ, Tuomari
AV, MacleanJR, Kasiske BL. Depressive disorder in renal
transplanta-tion:ananalysisofMedicareclaims.Am.J.KidneyDis.2008; 51
(5): 81928.25Arapaslan B, Soykan A, Soykan C, Kumbasar H.
Cross-sectional assessment of psychiatric disorders
inrenaltransplantation patients in Turkey: a preliminary
study.Transplant. Proc. 2004; 36 (5): 141921.26De Pasquale C,
Pistorio ML, Sorbello M et al. Body imagein kidney transplantation.
Transplant. Proc. 2010; 42 (4):11236.27Sabbatini M, Pisani A,
Crispo A et al. Renal transplanta-tionandsleep:
anewlifeisnotenough. J. nephrology.2008; 21 (Suppl 13):
S97101.28LittleRJA. Atestof
missingcompletelyatrandomformultivariate data with missing values.
J. Am. Stat. Assoc.1988; 83 (404): 1198202.29Schumacker RE, Lomax
RG. A Beginners Guide to Struc-tural Equation Modeling, 2ndedn.
Lawrence ErlbaumAssociates, Inc: Mahwa, NJ, 2004.30Backhaus K,
Erichson B, Plinke W, Weiber R.
Multivari-ateAnalysemethoden,3rdedn.Springer:Berlin,Heidel-berg,
New York, 2006.31TabachnickBG, Fidell LS.
UsingMultivariateStatistics,5th edn. Pearson International
Education: Boston, 2007.32Leonhard R. Lehrbuch Statistik Einstieg
Und Vertiefung.Hans Huber Verlag: Bern, 2009.Validity of the
PSQI281 2010 The AuthorsSleep and Biological Rhythms 2010 Japanese
Society of Sleep Research