Embed Size (px)
Citation preview
2012 Annual Report
Building on 20 Years of CollaborationAccelerating Our Progress to Better Hea th,l Better Care and Lower Costs

MembersAffi liated Community Medical CentersWillmar, MNAllina Health: Allina Medical Clinic Minneapolis, MN Aspen Medical Group St. Paul, MN Quello Clinic Bloomington, MNBaldwin Area Medical CenterBaldwin, WIBrown ClinicWatertown, SDCenter for Diagnostic Imaging/ Medical Scanning ConsultantsSt. Louis Park, MNCentraCare Health SystemsSt. Cloud, MNChippewa County-Montevideo Hospital & ClinicMontevideo, MNCuyuna Regional Medical CenterCrosby, MNEntira Family ClinicsMaplewood, MNEssentia HealthDuluth, MNFairview Health ServicesMinneapolis, MNFairview RangeHibbing, MNFamily Practice Medical CenterWillmar, MNGillette Children’s Specialty HealthcareSt. Paul, MNGrand Itasca Clinic & HospitalGrand Rapids, MNHamm ClinicSt. Paul, MNHealthEast Care SystemSt. Paul, MNHealthPartners Central Minnesota ClinicsSt. Cloud, MNHealthPartners Medical Group & Regions HospitalMinneapolis & St. Paul, MN
Hennepin County Medical CenterMinneapolis, MNHoward Young Medical CenterWoodruff, WIHudson PhysiciansHudson, WIHutchinson HealthHutchinson, MNIntegrity Health NetworkDuluth, MNLake Region Healthcare CorporationFergus Falls, MNLakeview ClinicWaconia, MNMankato ClinicMankato, MNMarshfi eld ClinicMarshfi eld, WIMAPS Medical Pain ClinicsMinneapolis, MNMayo ClinicRochester, MNMercy Hospital & Health Care CenterMoose Lake, MNMidwest Spine InstituteStillwater, MNMinnesota Association of Community Health CentersMinneapolis, MNMinnesota GastroenterologySt. Paul, MNMulticare AssociatesBlaine, MNNew Richmond ClinicNew Richmond, WINorth ClinicRobbinsdale, MNNorth Memorial Health CareRobbinsdale, MNNorthwest Family PhysiciansCrystal, MNOBGYN SpecialistsEdina, MNOlmsted Medical CenterRochester, MNPark Nicollet Health ServicesSt. Louis Park, MN
Planned Parenthood Minnesota, North Dakota, South Dakota St. Paul, MNRice Memorial HospitalWillmar, MNRidgeview Medical CenterWaconia, MNRiver Falls Medical ClinicRiver Falls, WIRiverwood Healthcare CenterAitkin, MNSouth Lake PediatricsMinnetonka, MNSouthside Community Health ServicesMinneapolis, MNStillwater Medical GroupStillwater, MNUniversity of Minnesota PhysiciansSt. Paul, MNWinona HealthWinona, MN
Principal SponsorsBlue Cross and Blue Shield of Minnesota HealthPartnersMedica
Associate SponsorsSecurity Health Plan of Wisconsin UCare
Institute for ClinicalSystems Improvement
1
AboutICSI
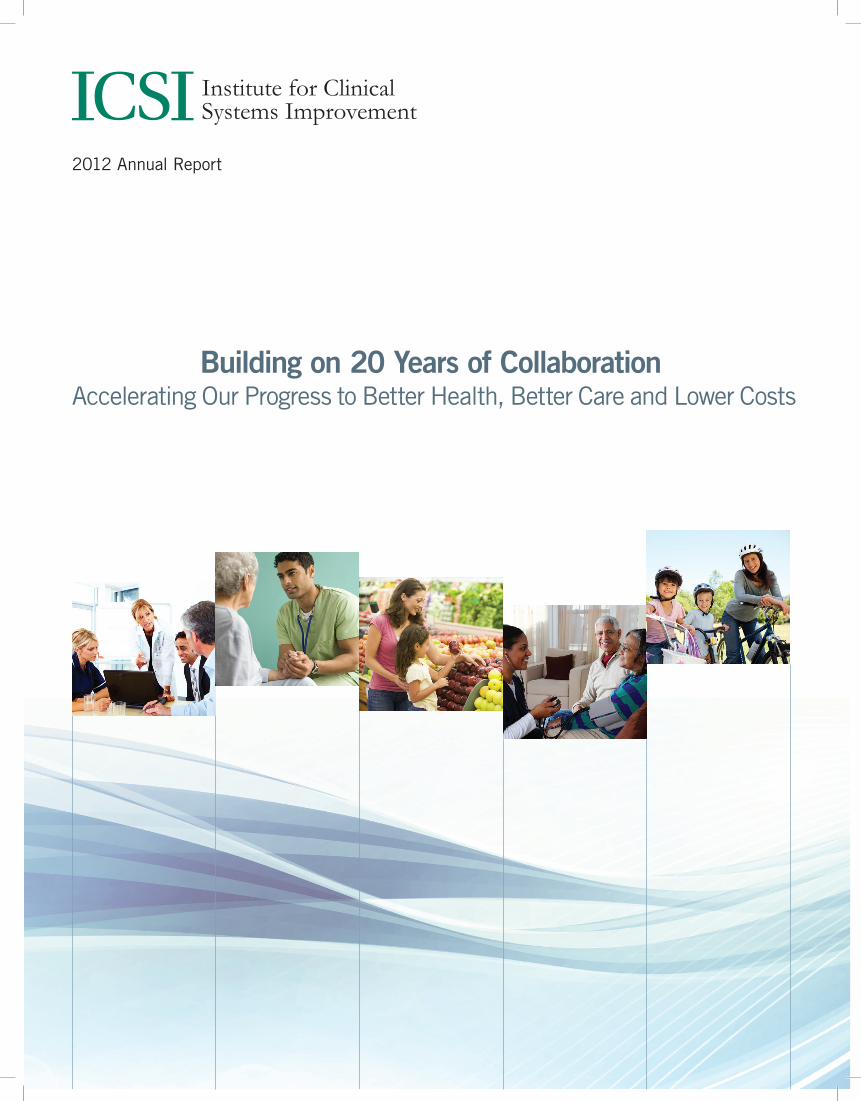
ICSI 1.01993–1997
ICSI 2.01998–2005
ICSI 3.02006–2009
ICSI 4.02010–Present
Expert, Evidence-based Role
Expert, Evidence-based Role
Expert, Evidence-based Role
Expert, Evidence-based Role
Process/QualityImprovement Role
Process/QualityImprovement Role
Process/QualityImprovement Role
Honest Broker Role;Transition to Value
Improvement
Honest Broker Role;Transition to Value
Improvement
Transformational Role:Targeting the
Triple Aim
The Institute for Clinical Systems Improvement (ICSI) is an independent, nonprofi t health care improvement organization that unites clinicians, health plans, employers, policymakers and consumers to bring innovation and urgency to improve population health, optimize the patient experience and make health care more affordable. Celebrating its 20th year, ICSI is comprised of 50+ medical group and hospital members representing 9,000 physicians, and is sponsored by fi ve Minnesota and Wisconsin nonprofi t health plans.
Our mission is to champion the cause of health care quality and to accelerate improvement in the value of the health care we deliver to the populations we serve.
ICSI 1.0
HealthPartners, Mayo Clinic and Park Nicollet Health Services founded the Institute for Clinical Systems Integration in 1993. Under its fi rst president, Gordon Mosser, MD, ICSI brought leading medical experts together to rigorously develop best practice health care guidelines for numerous diseases and health conditions. ICSI continues this foundational work today.
ICSI 2.0In 1997, the organization changed its name to the Institute for Clinical Systems Improvement to refl ect an added focus on accelerating improvement in the value and quality of health care delivered to patients. ICSI achieved this by helping medical groups and hospitals establish cultures of quality and implement system-wide best clinical practices.
ICSI expanded in 2001 when Blue Cross and Blue Shield of Minnesota, Medica, PreferredOne, and UCare became new sponsors, and medical group membership expanded. With statewide reach, ICSI tackled major health issues like diabetes across all member organizations.
ICSI 3.0In its third phase of growth, ICSI brought together providers, health plans, employers, patients and other stakeholders to tackle health care system challenges that no single group could solve on its own. A key improvement springing from this system-focused collaboration was the Depression Improvement Across Minnesota, Offering A New Direction (DIAMOND) program, which changes how care for patients with depression in primary care clinics is delivered and paid for.
ICSI 4.0Heading into its third decade, ICSI is helping the regional health community achieve the Triple Aim1. Today, ICSI collaborates locally and nationally with organizations outside its membership to accelerate transformation across more populations and to launch initiatives that meet SMART (specifi c, measurable, attainable, realistic and timely) goals. It is focusing on health reform as well as health care reform, and is working to co-create solutions that engage community resources and help consumers and patients share ownership in their health and care.
ICSI is further expanding its infl uence nationally through alignment with the Network for Regional Healthcare Improvement, a group of 31 regional health improvement collaboratives.
ICSI’s consulting arm, Professional Partnerships, takes the knowledge and programs ICSI developed for its members and helps other health care organizations implement them locally and nationally.
1. The Triple Aim: Care, Health and Costs. Berwick DM, Nolan TW and Whittington J. Health Affairs, May 2008, Vol. 27, No. 3, 759-769.
Dr. Gordon Mosser
2
Dear Colleagues and Friends
It is a time to celebrate 20 years of collaboration around the ICSI table working to transform health care together. Congratulations to our members, nonprofi t health plan sponsors, purchasers, consumers and other community stakeholders for reaching this signifi cant milestone. It shows your unwavering commitment to remain at the forefront of improving the health care system and the health of our citizens and communities.
This milestone causes us to both refl ect on the mission and values that got us here, and review actions taken in 2012 to launch ICSI into its third decade. Looking back, we note that ICSI has always pushed the health care improvement envelope. In 1993, convincing clinicians to use evidence-based guidelines was a somewhat radical idea. Today, medical personnel in 180 countries use our guidelines to help keep people healthy and to prevent, diagnose, treat and manage diseases.
Integrity, leadership, innovation and collaboration have been the foundation of our success. These values have enabled medical groups and hospitals to establish cultures of quality and improve processes faster by working together. Our region would not enjoy the high-quality health care we have today without this willingness to co-create and share the best of what we do to improve care. Together we’ve worked on common measures for quality improvement, technology assessment, disease management, shared decision-making, advanced access, the culture needed for quality, patient activation, adaptive leadership and many other components of a quality health care system.
With an evidence-based foundation and collaboration came trust that enabled ICSI to tackle complex and sometimes contentious health care system issues with innovative approaches. We launched the DIAMOND program to redesign care and payment for patients with depression in primary care, and we created the high-tech diagnostic imaging (HTDI) initiative to ensure appropriate use of medical imaging. We broadened the groups of collaborators who sat around the table to include more providers, health plans, patients, employers, policymakers and other community stakeholders. We used our DIAMOND experience to address risky substance use through SBIRT (Screening, Brief Intervention and Referral to Treatment) and to work with clinics taking care of people with other serious mental illnesses.
2
3
As innovative as programs like DIAMOND and HTDI are — even as their models expand nationally — ICSI cannot rest. As the tsunami of baby boomers enters a still fragmented health care system, we must embrace new values and approaches to achieve the Triple Aim of better population health, better care experience and more affordable health care.
In 2012, we successfully targeted the Triple Aim on a number of fronts. ICSI is currently:
• Nearing the goal of preventing 4,000 avoidable hospital readmissions through the RARE (Reducing Avoidable Readmissions Effectively) Campaign with our operational and community partners (www.rarereadmissions.org)
• Spreading the collaborative care management model of DIAMOND in Minnesota and across seven other states through the COMPASS (Care of Mental, Physical and Substance-Use Syndromes) initiative funded by a Center for Medicare and Medicaid Innovation award; we are one of 107 such awards in the country
• Providing the evidence-based guidance and tools to help primary and specialty care clinicians work together to provide appropriate and coordinated care for patients with acute back pain, mental illness and those needing complex care coordination
• Sharing ways to increase shared decision-making with tools for Collaborative Conversations™
• Helping medical groups, health plans and other stakeholders address the total cost of care in the context of the Triple Aim
• Working with health care and community leaders, citizens and other stakeholders to co-create a sustainable healthy tomorrow.
Looking at 2013 as our founders looked at 1993, we again have a great opportunity to lead the transformation of health and health care. We will continue to play the key roles that have helped us evolve and grow over the past 20 years — serving as an honest broker and trusted convener for evidence-based expertise, care and process improvement, and health care system transformation. The Triple Aim will remain our guidepost, and addressing health care affordability will be a key focus in the coming years.
Just as we led the movement to evidence-based medicine, ICSI will help lead the movement to value-based medicine, allowing our communities to reinvest in the social determinants of health, such as education, housing, job development, and healthy environments, that arguably are more critical to our well-being and longevity than health care.
So while we celebrate our past, we must strongly embrace our future together. The challenges of today are greater and even more pressing, and we must use our collective wisdom and collaborative spirit for the common good. It is only with the vision, resolve, collaboration, and hard work of all of us that we can co-create a sustainable, healthy tomorrow for our families, our children and our communities.
Sanne Magnan, MD, PhDPresident and CEO
Brian Rank, MDChair, ICSI Board of DirectorsMedical DirectorHealthPartners Medical Group & Regions Hospital
4
Transformational Role:Targeting the
Triple Aim
ICSI believes that the best way for providers and health plans to improve the health of citizens, the quality and experience of care for patients, and the affordability of care is to collaborate on the goals and alignment, and to compete on execution. With apologies to Paul Wellstone, ‘We all meet the Triple Aim when we all meet the Triple Aim’.”
– �Pete Benner, ICSI Board Member
“
ICSI Leads Initiative to Manage Mind-Body Health in Primary Care
The expertise ICSI gleaned from its work with the DIAMOND program for depression, the SBIRT program, and health care home over the past fi ve years helped ICSI, other medical groups and two supporting partners secure an $18 million, three-year cooperative agreement from the Center for Medicare and Medicaid Innovation in 2012.
ICSI is leading a consortium of 10 medical groups in eight states to implement a care management model for patients with diabetes or cardiovascular disease who also suffer from depression and possibly risky substance use. A number of ICSI member organizations were ready to begin offering the COMPASS program in 2013. If COMPASS can provide a sustainable model for treating patients with both mental and physical chronic diseases, it could possibly alter how patients with chronic conditions are treated and how primary care is reimbursed by CMS moving forward.
RARE Campaign Nears Readmission Goals, Improves Patient Care TransitionsThe RARE (Reducing Avoidable Readmissions Effectively) Campaign appeared ready to reach its goal of preventing 4,000 avoidable readmissions by the end of 2012. (Results for 4th quarter of 2012 will be available in May 2013.) The campaign provides support to more than 80 hospitals through education, networking, coaching and sharing of best practices focused on fi ve areas — comprehensive discharge planning, patient/family engagement, medication management, transition care support and transition communication. The campaign has as operating partners ICSI, Minnesota Hospital Association, and Stratis Health, with supporting partners MN Community
Measurement, the Minnesota Medical Association and VHA Upper Midwest, and more than 75 community partners. Some 2012 highlights of the campaign include:
• Developing recommended actions for improved care transitions, including those for patients with mental illnesses and/or substance use disorders
• Providing training for 11 organizations on the Care Transition Intervention with funding provided by Partnership for Patients
• Hosting two action learning days that attracted more than 350 attendees, and providing 10 webinars with more than 1,000 participants.
The RARE Campaign is continuing through 2013 with the goal of maintaining the 20 percent reduction in avoidable readmissions. The operating partners are evaluating the potential of RARE to enable a follow-up initiative to better meet the needs of complex patients and to reduce preventable health care events.
ICSI’s Initiatives Target the Triple Aim, Impact Health Care Regionally and Nationally
Each person represents 250 prevented readmissions, and 1,000 more nights of sleep in their own beds for Minnesotans
Progress Toward RARE Campaign Goals
5
Improving Interaction Between Primary and Specialty Care to Treat Low Back Pain
An ICSI multi-stakeholder advisory committee, plus care model and measurement subgroups, used a revised ICSI guideline as the
foundation to improve the care of patients with low back pain. These groups accomplished the following during the year:
• Reached consensus on key care delivery elements in a model called ACTIVE (Active Care Treating Intense low back pain Very Effec-tively) with the expectation that evidence-based care and best practices will result in better care, less pain, and lower rates of back surgery
• Developed a toolkit to help clinicians implement ACTIVE
• Identifi ed the need for a region-wide, consistent approach to opiate use for low back pain.
ICSI Works to Improve Affordability of Care, Co-creating with CommunitiesStarting with the Reinertsen Lecture and a workshop late in 2011, ICSI has concentrated on the Total Cost of Care (TCOC) within the context of the Triple Aim. A key goal is to bring the same understanding, legitimacy and importance to this topic as ICSI did to improving quality in health care.
Highlights of this affordability work include:
• Educating our members and community on the importance of TCOC as a community measure
• Identifying care transitions and care coordination as high priority elements to decrease waste
• Prioritizing opportunities to address waste in health care using a recent Berwick and Hackbarth paper
• Hosting webinars on cost-related topics, such as “Moving from Fee-for-Service to Value-Based Care” and “Choosing Wisely.®”
“ It’s clear that individuals need to become more engaged in health care and their own wellness. ICSI is again at the forefront with its efforts to engage citizens in establishing accountable health communities.”
– Jim Guyn, MDVP & Senior Medical Offi cer,Health Management, Medica
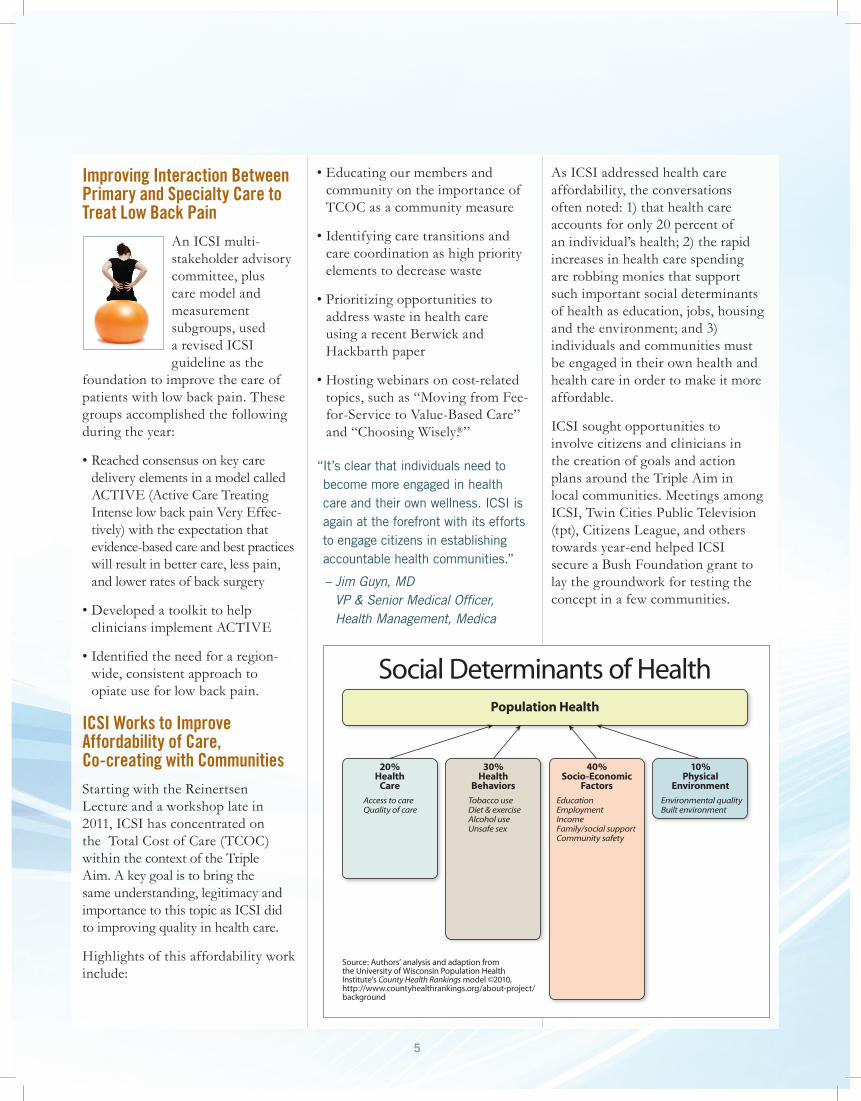
As ICSI addressed health care affordability, the conversations often noted: 1) that health care accounts for only 20 percent of an individual’s health; 2) the rapid increases in health care spending are robbing monies that support such important social determinants of health as education, jobs, housing and the environment; and 3) individuals and communities must be engaged in their own health and health care in order to make it more affordable.
ICSI sought opportunities to involve citizens and clinicians in the creation of goals and action plans around the Triple Aim in local communities. Meetings among ICSI, Twin Cities Public Television (tpt), Citizens League, and others towards year-end helped ICSI secure a Bush Foundation grant to lay the groundwork for testing the concept in a few communities.
Population Health
40%Socio-Economic
Factors
10%Physical
Environment
Environmental qualityBuilt environment
EducationEmploymentIncomeFamily/social supportCommunity safety
30%Health
Behaviors
Tobacco useDiet & exerciseAlcohol useUnsafe sex
20%Health
Care
Access to careQuality of care
Social Determinants of Health
Source: Authors’ analysis and adaption from the University of Wisconsin Population Health Institute’s County Health Rankings model ©2010, http://www.countyhealthrankings.org/about-project/background
6
Other work under this “Co-creating a Sustainable Healthy Tomorrow” theme included publishing “Achieving Accountability for Health and Health Care” in Minnesota Medicine, and engaging 45+ stakeholders in a ReThink Health Dynamics simulation model workshop to possibly leverage this model to prioritize initiatives that may best address the Triple Aim in Minnesota.
Honest Broker Role;Transition to Value
Improvement
The trusted role that ICSI plays as a neutral convener has enabled it to collaborate with other organizations to accelerate change across our region and the entire continuum of health services, as we are now doing through the RARE Campaign.”
– �Jan Malcolm, CEO, Courage Center
“
ICSI Provides Trusted Haven for ACOs to Move Toward Value-Based Health Care ICSI provided a neutral venue for Minnesota-selected Pioneer ACOs to network and discuss challenges. This sharing helped identify key attributes needed for successful ACOs — such as care coordination, care transitions and communications — and how they relate to form an integrated health care system. One of ICSI’s contributions to our community is to provide a trusted, safe harbor with our strong anti-trust policy for competitors to focus on the Triple Aim. We are expanding these conversations through our Affordability Council as more organizations work to create accountable care.
Examples of Triple Aim goals achieved or set for several key ICSI initiatives in 2012.
Initiative Population Health Care Experience Affordability of Care
RARE 82 hospitals, 75 Community Partners involved
Prevent 4,000 avoidable readmissions by end of 2012; at 3,60 through3 September (last data available)
Recaptured 14,41 nights2 of patients/families sleeping in their own beds (based on average length of stay in hospital)
Saved an estimated $25 million to date
COMPASS10 medical groups in eight states involving many clinics participating
Decrease severity of depression (based on PHQ-9 scores) by 5 points or achieve a PHQ-9 score of <10 for 40 percent of patients. Improve diabetes and hypertension control rates by 20 percent
Improve clinical care and decrease un-needed hospitalizations and emergency department visits. Improve patient and clinician satisfaction with care process by 20 percent
Projected to reduce health care costs of Medicare and Medicaid-measured patients by $25 million by June 2015
DIAMOND70 clinics offer; many of them also offer SBIRT
Getting 30 percent of patients into remission by six months
Patients report they prefer more frequent contact enabled by team-based model
Research fi ndings to be released in summer 2013
HTDI78 percent of Minnesota medical groups using decision support
Estimated to have prevented 75 cases of cancer due to unnecessary exposure to radiation
Patient leaves clinic knowing right scan has been ordered; can share in decision-making with provider
Held increases in HTDI claims to 1 percent in Minnesota (2007-2012), down from 8 percent annual increases (2003-2006), saving an estimated $150 million
7
Shared Decision-Making Integrated into Additional ICSI ActivitiesICSI expanded the use of shared decision-making to improve patient engagement and adherence with care plans, improve patients’ experience by involving them as partners in their health care, and reduce or contain costs by minimizing care that patients do not value. Highlights of this work include:
• Completing the Robert Wood Johnson Foundation grant work on engaging patients with life-limiting illnesses in shared decision-making
• Integrating Collaborative Conversations™, an ICSI-developed model to facilitate shared decision-making between a patient and their care team, into a motivational interviewing and coaching program to help medical groups meet requirements for such things as health care home certifi cation and pay for performance
• Assisting the community-wide MN Shared Decision Making Collaborative
• Including shared decision-making language in guideline revisions.
Use of Decision Support to Order Medical Imaging ChangesNuance Communications, ICSI’s vendor providing appropriateness criteria to medical groups for ordering high-tech diagnostic imaging scans, suspended sales of its RadPort software in April. As a result, ICSI discontinued additional implementation of the Nuance tools, and responsibility for decision support changed to medical groups
and/or health plans. ICSI continues to serve as a knowledge expert at the state and federal level for HTDI decision support and is exploring how to help the American College of Radiology develop universal appropriateness criteria so a decision-support option is available nationally for ordering HTDI scans. Guidance regarding HTDI choices is being incorporated into ICSI’s evidence-based guidelines as appropriate.
ICSI Helps Accelerate Integration of Behavioral Health into Primary CareThe DIAMOND program exemplifi es how the collaboration and innovation among ICSI stakeholders can result in foundational changes in care delivery and payment. The success of DIAMOND led to ICSI’s participation in an Agency for Healthcare Research and Quality (AHRQ) grant with two other regional collaboratives to combine DIAMOND for depression and Screening, Brief Intervention and Referral to Treatment (SBIRT) for risky substance use. In year two of this three-year AHRQ grant, ICSI:
• Began collecting data from the six ICSI member medical groups whose clinics are implementing the model to screen for risky substance use
• Worked with Invitation Health Institute to determine one community’s perception and attitudes towards substance use, its readiness to address the issues, and how the community could work with ICSI member Chippewa County-Montevideo Hospital and Clinic to support its DIAMOND/SBIRT program
• Created a community resource guide/toolkit to help SBIRT sites identify appropriate treatment programs and support services.
ICSI’s Professional Partnerships group contracted with the Minnesota Department of Human Services to support the Minnesota 10 x 10 Initiative. The primary goal of this collaborative was to pilot a project with seven Assertive Community Treatment (ACT) teams to improve the physical health of clients with serious mental illness, then spread successful implementation strategies to other ACT teams.
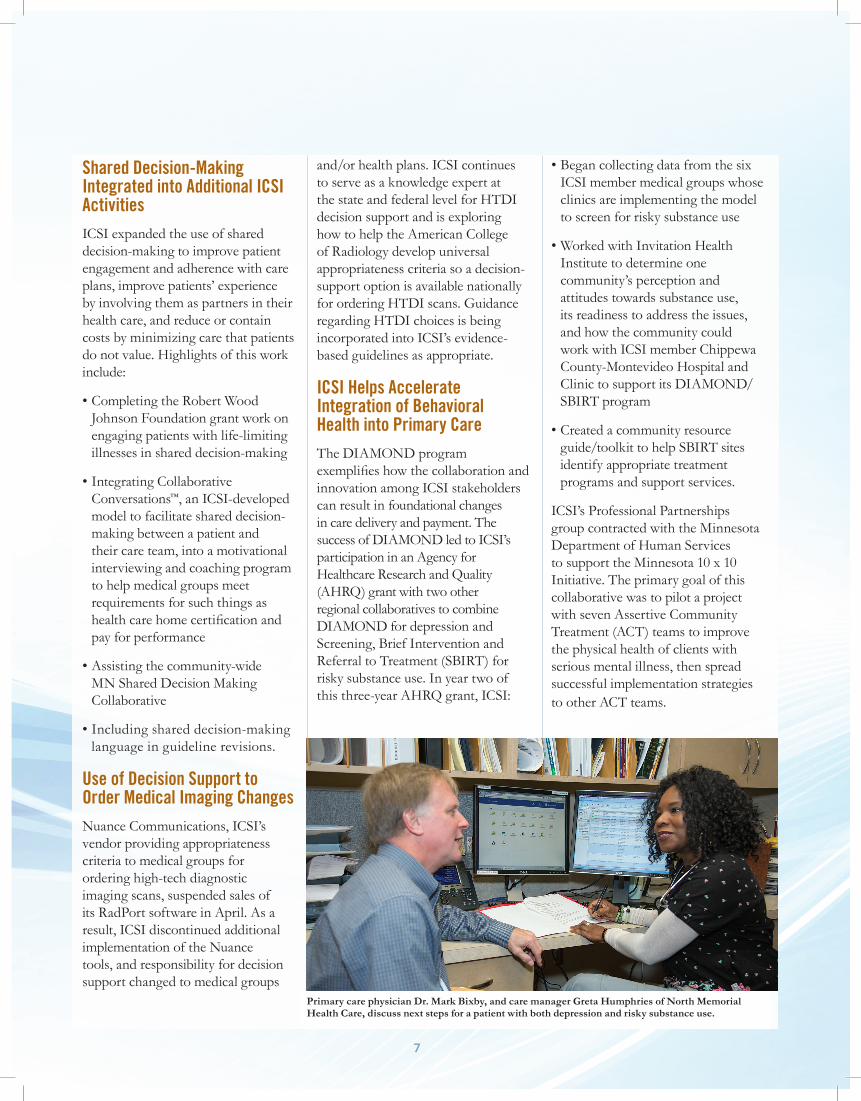
Primary care physician Dr. Mark Bixby, and care manager Greta Humphries of North Memorial Health Care, discuss next steps for a patient with both depression and risky substance use.

8
ICSI Helps 100+ Organizations With Health Care Home Certifi cationIn June, ICSI completed a Minnesota Department of Health contract to design and initiate a learning collaborative model to support ICSI members and other medical organizations preparing to seek or maintain health care home (HCH) certifi cation. More than 100 clinics participated. ICSI also provided an innovative, three-month patient activation and engagement learning collaborative at four regional sites, supporting HCH organizations in co-creating systems that achieve Triple Aim results.
Process/QualityImprovement Role
As a change agent and leader in health care, ICSI helps its members make quantum leaps toward achieving the Triple Aim through a focus on community involvement across our region.”
– �Gary McDowell, MS Administrator/COO Family Practice Medical Center of Willmar
“
Leading Innovation, Providing EducationICSI members again took advantage of numerous opportunities designed to support their efforts to achieve the Triple Aim. The year was highlighted by near-record attendance (500) at the
annual Colloquium on Health Care Transformation, and an engaging Reinertsen Lecture that focused on population health. Other educational activities focused on:
• High-demand topics such as motivational interviewing, patient engagement, patient safety and elective procedures/inductions
• New developments in clinical practice or translation of evidence into practice that have resulted in signifi cant changes to ICSI scientifi c documents
• Foundational quality improvement training (e.g, The Cultivating Quality series for three new members) and “QI Boot Camps” for members seeking a refresher course
• Adaptive leadership training
• Ideagora discussions on new and emerging methods and care practices.
Providing Greater Value to Members; Expanding Member InnovationsICSI acknowledged the rapidly changing demands on member organizations by modifying member requirements and fee structures during the year. The new requirements give members more fl exibility to tailor their involvement in ICSI, provide greater equity among members, and encourage members to participate in activities they deem strategic to align with their individual needs and quality goals.
ICSI continued to seek grants that support its mission and strategic initiatives as well as provide members and non-members with consulting services through its Professional Partnerships consulting business.
Much of the consulting done by ICSI Professional Partnerships involved supporting the COMPASS cooperative agreement, as a key expertise of this consulting group is integrating behavioral and mental health into primary care.
“ MAPS is proud to be a new ICSI member. Our pain experts were delighted to work with other medical experts to revise ICSI’s Low Back Pain Guideline. The group’s discussions on improving patient care and reducing costs by using the latest evidence to guide pain management services will contribute to improved best medical practice.”
– David M. Schultz, MD, Medical Director, MAPS Medical Pain Clinics
The 2012 Reinertsen Lecture “From ACOs to Accountable Health Communities: Delivering on Population Health in the Triple Aim,” was given by Bobby Milstein, PhD, MPH, Director of ReThink Health Dynamics (left), and David Kindig, MD, MPH, Professor Emeritus, Emeritus Vice-Chancellor for Health Sciences, University of Wisconsin.
9
In addition to COMPASS, the group continued to expand the DIAMOND/SBIRT model enabled by the AHRQ grant. It provided ICSI members with training on leadership, motivational interviewing, value-stream mapping and more.
Connecting the DotsICSI enhanced its reputation as a leader in achieving the Triple Aim in numerous venues regionally and nationally. It collaborated with other regional collaboratives through the Network of Regional Healthcare Improvement to enlist support for pilot projects that support ICSI strategic initiatives. ICSI also informed and engaged state and national opinion leaders to champion health care quality and value in order to affect public policy at the state, regional and national levels.
Expert, Evidence-based Role
Health professionals across the country rely on ICSI guidelines. It’s great as an ICSI member to know I contributed to help develop them.”
– �John M. Wilkinson, MD Assistant Professor of Family Medicine Mayo Clinic College of Medicine
“
Translating evidence into practice through health care guidelines and protocols remained a core function of ICSI, with more than 300 members helping to revise 21 scientifi c documents during the year. Key focuses in this segment of ICSI’s work in 2012 include:
• Revising the guideline process to most effectively and effi ciently translate evidence into practice to support ICSI initiatives and the work of its members and sponsors
• Strengthening the confl icts and competing interests policy, and collaborating with MN Community Measurement to create a combined confl ict of interest committee
• Collaborating with other guideline developers such as Kaiser Permanente and the Veterans Administration to use their expertise and resources to enhance ICSI’s evidence work
• Determining content ICSI should add to its scientifi c documents, such as decision support, shared decision-making, comparative effectiveness, translational research, and affordability
• Assessing the value of providing scientifi c documents in an additional, abbreviated form limited to algorithms and clinical recommendations
• Holding bi-monthly Patient Advisory Council meetings to provide patient feedback on ICSI guidelines.
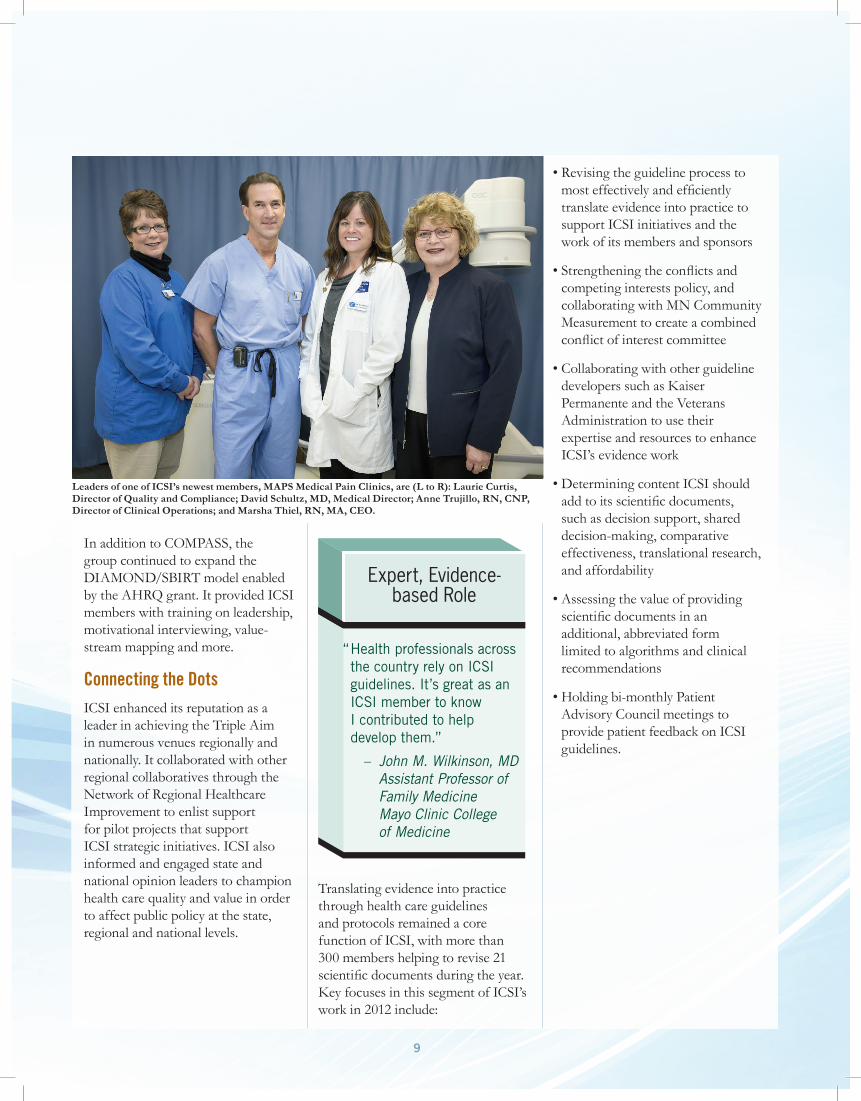
Leaders of one of ICSI’s newest members, MAPS Medical Pain Clinics, are (L to R): Laurie Curtis, Director of Quality and Compliance; David Schultz, MD, Medical Director; Anne Trujillo, RN, CNP, Director of Clinical Operations; and Marsha Thiel, RN, MA, CEO.
Offi cersChairBrian Rank, MDMedical DirectorHealthPartners Medical Group
Vice-ChairPaula Santrach, MDChair, Clinical Practice Quality Oversight CommitteeMayo Clinic
SecretaryGary McDowell (2010-2012)Administrator andChief Operating Offi cerFamily Practice Medical Center
DirectorsDavid Abelson, MDPresidentPark Nicollet Health Services
Beth Averbeck, MDAssociate Medical DirectorPrimary CareHealthPartners Medical Group
Pete BennerAFSCME Council 6AFL-CIORetired
Jim ChasePresidentMN Community Measurement
Patrick Courneya, MDMedical DirectorHealthPartners Health Plan
Mark Eustis (2011-2012)President & CEOFairview Health System
Gregory Gilmet, MD, MPH (2009-2012)Vice President andChief Medical Offi cerMedical AffairsBlue Cross and Blue Shield of Minnesota
Jim Guyn, MDVice President and Senior Medical Offi cerMedica
Robert Karasov, MDPediatricianPark Nicollet Health Services
Scott Ketover, MDPresident & CEOMinnesota Gastroenterology
Larry Lee, MDExecutive Medical Director for Provider Relations and QualityBlue Cross and Blue Shield of Minnesota
Timothy Lineberry, MDVice-Chair, Hospital Practice CommitteeMayo Clinic
Sanne Magnan, MD, PhDPresident & CEOInstitute for Clinical Systems Improvement
Jan MalcolmCEOCourage Center
Joshua Riff, MD (2011-2012)Chief Medical DirectorTarget Corporation
Larry SchultzCEOLake Region Healthcare
Rachelle Schultz (2008-2012)President & CEOWinona Health
Mark Werner (2012)Chief Clinical Integration Offi cerFairview Health Services
AlternatesSteven M. Connelly, MDChief Medical Offi cerPark Nicollet Health Services
Marc Manley, MD, MPH (2005-2012)Vice President & Chief Prevention Offi cerBlue Cross and Blue Shield of Minnesota
Leif I. Solberg, MDAssociate Medical DirectorHealthPartners Medical GroupDirector, Care Improvement ResearchHealthPartners Institute for Education and Research
Robert Stroebel, MDChair, Primary Care Internal MedicineCPC Chair, Employee & Community HealthMayo Clinic
Sidna M. Tulledge-Scheitel, MD, MPHConsultant in Primary CareInternal MedicineAssistant Professor, Mayo Medical CollegeMayo Clinic
2012 Board of Directors
8009 34th Avenue SouthSuite 1200Bloomington, MN 55425Phone: (952) 814-7060Fax: (952) 858-9675Email: [email protected]
© 2013 Institute for Clinical Systems Improvement