Embed Size (px)
Citation preview

ACHIEVING EXCELLENCE: HIRING THE BEST. DEVELOPING THE BEST. KEEPING THE BEST!
Building a Comprehensive Approach to
Wellness in the Residency Liselotte Dyrbye, MD, MHPE, FACP
Mayo Clinic
The afternoon session will target Faculty, Program Directors, Chief Residents, Residency & Fellowship
Coordinators, Medical Education Specialists, and other GME professionals.
The session will be held in the Mystic Ballroom.
Session Objectives:
1. Explain the prevalence of burnout and potential contributors
2. Describe the consequences of burnout
3. Give examples of self-care strategies that mitigate risk of burnout
4. Identify organizational strategies/system approaches to enhance well-being and encourage
appropriate help-seeking behaviors
5. Describe strategies to reduce risk of resident suicide
11:45-12:30 pm Poster Presentations and Buffet Luncheon
12:30-12:35 pm Welcome, Overview & Introductions
12:35 – 1:40 pm Part 1 – Prevalence, Drivers and Consequences of Burnout
1:40 –1:55 pm Q & A
1:55 - 2:15 pm Break – View Poster Presentations
2:15 – 2:45 pm Part 2 - Personal Strategies to Mitigate Risk
2:45 – 3:45 pm Part 3 - Overview of Evidence-Based Organizational Strategies and
Developing System-Level Change
3:45 – 4:15 pm Review, Priority Action Plans, and Final Discussion
4:15 – 4:30 pm Wrap-up & Complete Evaluations

Lotte Dyrbye, MD, MHPE Program on Physician Well-Being Mayo Clinic
1
Building a Comprehensive Approach to Wellness in the Residency
Part 1. Prevalence, Drivers, and Consequences
Epidemiology of Burnout1-6
~54% of physicians have substantial symptoms of burnout, higher than other US workers
even after controlling for work hours
Prevalence of burnout increased 9% from 2011 to 2014
Substantial differences in prevalence of burnout by specialty
Greater burnout: more work hours, younger age, female physicians, pay based entirely on
billing, children <22 years old, dual career relationships
30-70% of residents have burnout, unknown if varies by specialty, lower prevalence among
IMG
27% of residents have depression, higher than age-similar norms, with 11% have suicidal
ideation
At matriculation medical students have better mental health profiles than peers who choose
other careers
Drivers2,3,7-14
• Excessive workload
• Inefficient work environment
• Problems with work-life integration
• Loss of autonomy, flexibility and control
• Poor alignment of values
• Reduction of meaning in work
• Lack of social support at work
• Learning climate, relationships with supervisors, lack of timely feedback
• Educational debt
• Personal life events
Consequences10,15-30
Decreased quality of care, medical errors
Career choice regret, career dissatisfaction
Malpractice litigation
Lower medical knowledge
Turnover and decreased productivity
Poor professionalism, lower empathy
Suicidal ideation
Alcohol abuse/dependence
Motor vehicle incidents

Lotte Dyrbye, MD, MHPE Program on Physician Well-Being Mayo Clinic
2
Part 2. Personal strategies to mitigate risk7,31-35
“These are the duties of a physician: First…to heal his mind and to give help to himself before
giving it to anyone else.” - Epitaph of an Athenian doctor, AD 2
Self-Calibration Exercise Relationships
Work Hours Delayed Gratification Mindfulness
Meaning in Work Work-life Balance Work-Home Conflict
Take Vacation Positive Outlook Focus on Most Important
Lotte Dyrbye, MD, MHPE Program on Physician Well-Being Mayo Clinic
3
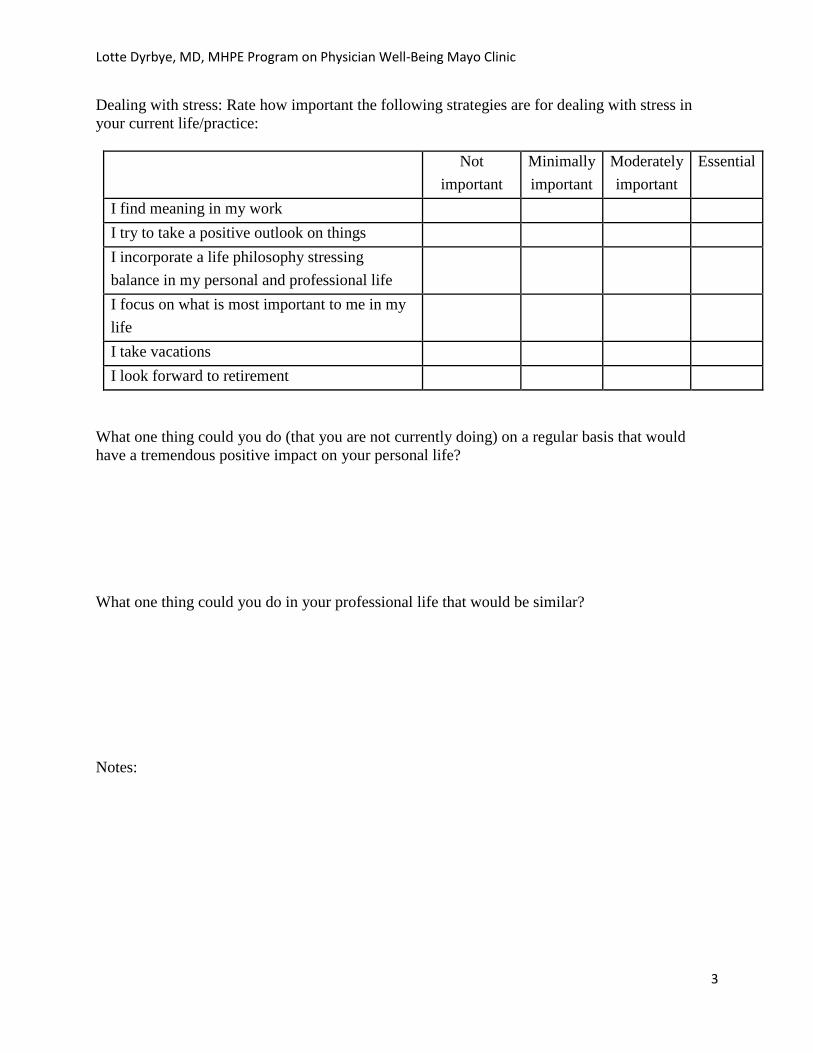
Dealing with stress: Rate how important the following strategies are for dealing with stress in
your current life/practice:
Not
important
Minimally
important
Moderately
important
Essential
I find meaning in my work
I try to take a positive outlook on things
I incorporate a life philosophy stressing
balance in my personal and professional life
I focus on what is most important to me in my
life
I take vacations
I look forward to retirement
What one thing could you do (that you are not currently doing) on a regular basis that would
have a tremendous positive impact on your personal life?
What one thing could you do in your professional life that would be similar?
Notes:
Lotte Dyrbye, MD, MHPE Program on Physician Well-Being Mayo Clinic
4
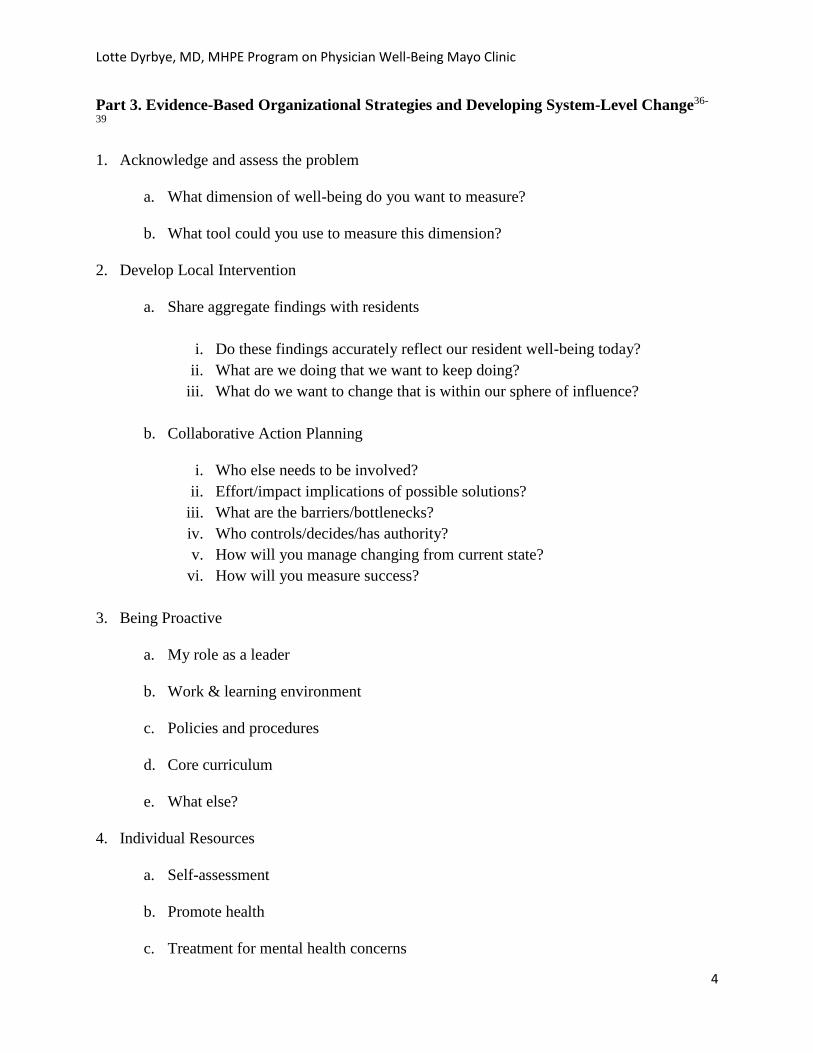
Part 3. Evidence-Based Organizational Strategies and Developing System-Level Change36-
39
1. Acknowledge and assess the problem
a. What dimension of well-being do you want to measure?
b. What tool could you use to measure this dimension?
2. Develop Local Intervention
a. Share aggregate findings with residents
i. Do these findings accurately reflect our resident well-being today?
ii. What are we doing that we want to keep doing?
iii. What do we want to change that is within our sphere of influence?
b. Collaborative Action Planning
i. Who else needs to be involved?
ii. Effort/impact implications of possible solutions?
iii. What are the barriers/bottlenecks?
iv. Who controls/decides/has authority?
v. How will you manage changing from current state?
vi. How will you measure success?
3. Being Proactive
a. My role as a leader
b. Work & learning environment
c. Policies and procedures
d. Core curriculum
e. What else?
4. Individual Resources
a. Self-assessment
b. Promote health
c. Treatment for mental health concerns

Lotte Dyrbye, MD, MHPE Program on Physician Well-Being Mayo Clinic
5
Select References
1. Shanafelt T, Hasan O, Dyrbye L, et al. Changes in burnout and satisfaction with work-life balance
in physicians and the general US working population between 2011 and 2014. Mayo Clin Proc. 2015;90:1600-1613.
2. Dyrbye LN, T.D. Shanafelt, C.A. Sinsky, P.F. Cipriano, J. Bhatt, A. Ommaya, C.P. West, and D. Meyers. Burnout among health care professionals: A call to explore and address this underrecognized threat to safe, high-quality care. . NAM Perspectives. Discussion Paper, National Academy of Medicine, Washington DC. https://nam.edu/burnout-among-health-careprofessionals-a-call-to-explore-and-address-this-underrecognized-threat-to-safe-high-quality-care. 2017.
3. Dyrbye LN, Shanafelt T. A narrative review on burnout experienced by medical students and residents. Med Educ. 2016;50:132-149.
4. Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89:443-451.
5. Mata DA, Ramos MA, Bansal N, et al. Prevalence of Depression and Depressive Symptoms Among Resident Physicians: A Systematic Review and Meta-analysis. JAMA. 2015;314:2373-2383.
6. Brazeau CM, Shanafelt T, Satele D, Sloan J, Dyrbye LN. Distress among matriculating medical students relative to the general population. Acad Med. 2014;89:1520-1525.
7. Shanafelt TD, West CP, Sloan JA, et al. Career fit and burnout among academic faculty. Arch Intern Med. 2009;169:990-995.
8. Dyrbye LN, West CP, Satele D, Sloan J, TD S. Work-home conflict and burnout among academic internal medicine physicians. Arch Intern Med. 2011;171:1207-1209.
9. Dyrbye LN, Sotile W, Boone S, et al. A survey of U.S. physicians and their partners regarding the impact of work-home conflict. Journal of General Internal Medicine. 2014;29:155-161.
10. West C, Shanafelt T, Kolars J. Quality of life, burnout, educational debt, and medical knowledge among internal medicine residents. JAMA. 2011;306:952-960.
11. Dyrbye LN, Thomas MR, Harper W, et al. The learning environment and medical student burnout: a multicentre study. Med Educ. 2009;43:274-282.
12. Dyrbye LN, Thomas MR, Huntington JL, et al. Personal life events and medical student well-being: A multicenter study. Acad Med. 2006;81:374-384.
13. Shanafelt T, Dyrbye LN, Sinsky C, et al. Relationship Between Clerical Burden and Characteristics of the Electronic Environment With Physician Burnout and Professional Satisfaction. Mayo Clin Proc. 2016;91:836-848.
14. Prins JT, Gazendam-Donofrio SM, Dillingh GS, van de Wiel HB, van der Heijden FM, Hoekstra-Weebers JE. The relationship between reciprocity and burnout in Dutch medical residents. Med Educ. 2008;42:721-728.
15. Wallace JE, Lemaire JB, Ghali WA. Physician wellness: a missing quality indicator. Lancet. 2009;374:1714-1721.
16. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Annals of Surgery. 2010;251:995-1000.
17. Shanafelt TD, Balch CM, Bechamps GJ, et al. Burnout and career satisfaction among American surgeons. Annals of Surgery. 2009;250:463-471.
18. Shanafelt T, Bradley K, Wipf J, Back A. Burnout and self-reported patient care in an Internal Medicine residency program. Ann Intern Med. 2002;136:358-367.

Lotte Dyrbye, MD, MHPE Program on Physician Well-Being Mayo Clinic
6
19. Balch CM, Oreskovich MR, Dyrbye LN, et al. Personal consequences of malpractice lawsuits on American surgeons. J Am Coll Surg. 2011;213:657-667.
20. Shanafelt T, L.N. D, West CP, Sinsky C. Potential Impact of Burnout on the US Physician Workforce. Mayo Clin Proc. 2016;91:1667-1668. doi: 1610.1016/j.mayocp.2016.1608.1016.
21. Shanafelt TD, Mungo M, Schmitgen J, et al. Longitudinal Study Evaluating the Association Between Physician Burnout and Changes in Professional Work Effort. Mayo Clinic Proceedings. 2016;91:422-431.
22. Dyrbye LN, Massie FS, Jr., Eacker A, et al. Relationship between burnout and professional conduct and attitudes among US medical students. JAMA. 2010;304:1173-1180.
23. Dyrbye LN, Thomas MR, Massie FS, et al. Burnout and suicidal ideation among US medical students. Ann Intern Med. 2008;149:334.
24. Shanafelt TD, Balch CM, Dyrbye LN, et al. Suicidal ideation among American surgeons. Archives of Surgery. 2011;146:54-62.
25. Oreskovich M, Kaups K, Balch C, et al. The prevalence of alcohol use disorders among american surgeons. Archives of Surgery. 2011;147:168-174.
26. Oreskovich MR, Shanafelt T, Dyrbye LN, et al. The prevalence of substance use disorders in American physicians. Am J Addictions. 2014:1-9.
27. Jackson ER, Shanafelt TD, Hasan O, Satele D, L.N. D. Burnout and Alcohol Abuse/Dependence Among U.S. Medical Students. Acad Med. 2016;91:1251-1256.
28. West CP, Tan AD, Shanafelt TD. Association of resident fatigue and distress with occupational blood and body fluid exposures and motor vehicle incidents. Mayo Clinic Proc. 2012;87:1138-1144.
29. West C, Huschka M, Novotny P, et al. Association of perceived medical errors with resident distress and empathy: A prospective longitudinal study. JAMA. 2006;296:1071-1078.
30. West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD. Association of resident fatigue and distress with perceived medical errors. JAMA. 2009;302:1294-1300.
31. Shanafelt T, Kaups KA, Nelson H, et al. An interactive individualized intervention to promote behavioral change to increase personal well-being in US surgeons. Ann Surg. 2014;259:82-88.
32. Shanafelt TD, Oreskovich MR, Dyrbye LN, et al. Avoiding burnout: the personal health habits and wellness practices of US surgeons. Ann Surg. 2012;255:625-633.
33. Dyrbye LN, Satele D, Shanafelt T. Ability of a 9-Item Well-Being Index to Identify Distress and Stratify Quality of Life in US Workers. J Occup Environ Med. 2016;58:810-817.
34. Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Utility of a brief screening tool to identify physicians in distress. J Gen Intern Med. 2013;28:421-427.
35. Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Ability of the Physician Well-Being Index to identify residents in distress. J Grad Med Educ. 2014;6:78-84.
36. Shanafelt T, Noseworthy JH. Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2016;92:129-146.
37. Shanafelt TD, Gorringe G, Menaker R, et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clinic Proceedings. 2015;90:432-440.
38. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. The Lancet. 2016.
39. West C, Dyrbye L, Rabatin J, et al. Intervention to promote physician well-being, job satisfaction, and professionalism: a randomized clinical trial. JAMA Intern Med. 2014;174:527-533.
1
Physician Well-Being Resources and Playbook
Resident
Well-Being
Resources
and Playbook
Lotte Dyrbye, MD MHPE
Professor of Medicine and Medical Education
Co-Director, Mayo Clinic Program on Physician Well-Being

2
Table of Contents
Introduction
Perspective on how to approach resident well-being p.3
How to use the well-being resource and playbook p. 3
The organization and environment
Over-arching approach to resident well-being p. 4
Monitoring physician well-being and understanding your data p. 4
Responding to your data p. 6
Being proactive p. 7
Individual Resources p. 9
Resources and Bibliography p. 10
ACGME Common Program Requirements VI Well-Being p.13

3
Introduction
Perspective on how to approach resident well-being
The national prevalence of burnout among physicians is > 54%, increasing, and higher than
among other US works even after controlling for work hours and a variety of other factors.
Similar to physicians, residents are more likely to have to burnout than similarly aged individuals
who pursued other careers. Additionally, residents are more likely to experience depression.
This is not because individuals who choose medicine are somehow vulnerable. In fact, a large
national study suggests at matriculation into medical school, medical students have better mental
health (less burnout and depression and better quality of life in multiple domains) than similarly
aged college graduates. A short while later this flips with medical students having more
depression, more burnout, and worse quality of life across multiple domains.
Burnout threatens organizational health, quality and safety of patient care, and physician health.
Studies have found associations between burnout and medical error, medical malpractice
litigation, decreased productivity and professional effort, turnover, lower medical knowledge,
motor vehicle incidents, suicidal ideation, and alcohol abuse/dependence. Total cost attributed to
burnout is greater than $3.4 billion annually to the US health care system.
Burnout, a syndrome characterized by emotional exhaustion and depersonalization (cynicism and
detachment toward patients), is driven by work-related stressors. Most of these stressors stem
from excessive workload, inefficient work environment, problems with work-life integration,
loss of autonomy, control, and flexibility, reduction in meaning in work, lack of social support at
work, and conflict between personal and organizational values. Additional factors associated
with burnout among residents include lack of timely feedback, stressful relationships with
supervisors, feeling uncertain about the future, perception that personal needs are
inconsequential, educational debt, and little emotional support from attendings.
Resident well-being is a shared responsibility of individual residents, the residency program, and
the sponsoring organization. This perspective is reflected in the organization and focus areas of
this book.
How to use the well-being resource and playbook
In this book you will find an over-arching approach to supporting residents and strategies for
how to systematically approach customized, local solutions that leverage organizational
resources. Within the bibliography you will find publications focused on drivers and
consequences of physician well-being and how to mitigate risk.

4
Approach to Resident Well-being
Commitment to residents’ careers and health and personal well-being requires a multi-pronged
organizational approach that includes investing in program director leadership and faculty
development, monitoring and responding to resident well-being scores, having supportive
policies and procedures, cultivating community, and providing resources to promote resilience
and self-care. In addition, sponsoring institutions are encouraged to facilitate and fund
organizational science in physician and resident well-being.
Monitoring Resident Well-being and Understanding Your Data
Well-being should be a routine program and institutional performance metric. It is ideal to use
validated instruments that correlate with outcomes of interest (safety, quality, retention, etc.) and
have national benchmarks.
What tools are available?
A variety of instruments are available that measure burnout, engagement, job satisfaction,
fatigues, stress, and quality of life. Many of these instruments are long, cumbersome to analyze,
and only measure one dimension of distress. As distress can present in a variety of ways using
only one tool would fail to identify many in distress. Instruments that measure dimensions of
burnout are shown in Table 1, along with a composite measure, the Well-Being index, which
evaluates dimensions of burnout, stress, fatigue, mental quality of life, and physical quality of
life in the 7-item version with additional items exploring professional satisfaction and work-life
integration in the 9-item version.
Faculty Development
Monitoring & Responding
•Resident well-being as an organizational performance metric
Promote Health
•Exercise facilities
•Fatigue mitigation strategies
•Nutrition & Prev services
•Education self-care
Program Director Leadership
Institutional Culture
•Policies and procedures
•Professionalism
•Support after medical error
Connect w. Colleagues
•Social events
•Common space/lounge
Self-assessment Academic Support
Services
Treat Mental health
•Integrated behavioral health
•Primary care
•Psychology/psychiatry
•EAP

5
Well-Being Index
Development of the Well-Being index involved a multistep process with expert input, correlation
analysis for previously administered assessments, and validation in separate large samples of
medical students, residents, physicians, nurses, advanced practice providers, and other US health
care workers. The Well-Being index is embedded within the online Well-Being self-assessment
tool that provides individuals a way to anonymously assess their level of well-being and receive
both immediate feedback on how it compares to other like professionals at their place of work
and nationally (residents compared to residents at their own institution and nationally) as well as
resources (locally tailored and national) to help promote wellness. Institutions receive real time
customized reports (e.g., residency program, year in training, sex) with comparative normative
data. Additional information can be found at: https://www.mededwebs.com/well-being-index .
Table 1. Burnout and Composite Well-Being Tools
Scale Notes
Maslach Burnout Inventory
(MBI) - Human Services
Survey (MBI-HSS)
Gold standard. Proprietary (www.mindgarden.com). 22-items.
National benchmarks available for residents and physicians.
Substantial data showing scores correlate with relevant
outcomes.
2-items from MBI Two single questions from the MBI have been validated in
validated in separate samples of medical students, internal
medicine residents, internal medicine faculty, and surgeons. The
2-items correlated strongly with the emotional exhaustion and
depersonalization domains of burnout as measured by the full
MBI with an area under the receiver operator characteristic
curve of 0.94 and 0.93 for emotional exhaustion and
depersonalization, respectively, for these single items relative to
the full MBI. Concurrent validity for the 2-items established
and national benchmarks for physicians and residents available.
Oldenburg Burnout Inventory Developed for use in any occupational group. No national
benchmarks for residents/physicians. Small studies have shown
correlations with relevant outcomes.
Copenhagen Burnout
Inventory
Developed for use in any occupational group. No national
benchmarks for residents/physicians. Small studies have shown
correlations with relevant outcomes.
Physician Work-Life Study
single item (embedded within
“Mini-Z”): “Overall, based on
your definition of burnout,
how would you you’re your
level of burnout?”
Predicts high levels of emotional exhaustion but not low
emotional exhaustion or depersonalization. It is not effective at
capturing individuals who have evidence of burnout in the
depersonalization or personal accomplishment domains. No
national benchmarks and not shown to correlate with relevant
outcomes.
Well-Being Index Specific versions developed for physicians, residents, medical
students, nurses, advance practice providers, and other US
workers. National benchmark data available and scores
correlate with relevant outcomes.

6
Responding to Your Data
After reviewing your data and discussing it with your leadership team it is important to identify
strengths and key areas of opportunity. Scores that are worse than national benchmarks are
concerning, and may suggest a local issue. The next step is to share the findings with the
residents.
Acknowledge the problem
Recognizing the problem and acknowledging the difficulties should be done during gatherings
with residents. Show trends over time and how the results compare to national benchmarks,
when available. Open and candid conversations about the data are useful.
Develop and implement targeted interventions
Although the drivers of burnout are well established (excessive workload, inefficient work
environment, problems with work-life integration, loss of autonomy, control, and flexibility,
reduction in meaning in work, lack of social support at work, and conflict between personal and
organizational values) among physicians how they manifest and which dimension is most
important varies by specialty and work group. In addition, there are unique issues for residents
that likely contribute as well. Engaging residents to develop solutions is vital. The conversation
should focus on understanding the scores, discussing the drivers, and identifying specific
contributing factors. Effort should be made to differentiate between factors that are within the
control of individual residents, immediate leadership (residency program), higher leadership
(institutional DIO), the sponsoring institution, and national factors (e.g., Medicare regulations).
While factors beyond the control of the immediate leadership can be communicated upwards, the
group should prioritize drivers within their control and brainstorm to identify best possible
solutions.
Ways to obtain input from residents include using crowd sourcing activities such as 25/10,
“What I Need From You,” and 1-2-4-All. These approaches stem from liberating structures and
are well described on the website http://www.liberatingstructures.com/ .
Action planning and implementation should involve residents as well as the local leadership
team. The action team should follow-up with residents to report on ongoing progress and discuss
unanticipated barriers. Small tests of change can lead to meaningful difference, and PDSA
cycles can provide a useful and familiar framework.
An ideal solution could be one small action that could really have the biggest impact on burnout
and thriving. Questions to consider when engaging in action planning:
Who else needs to be involved?
Effort required and implications of possible solutions?
What are the barriers/bottlenecks?
Who controls/decides/has authority?
How will you manage changing from current state?
How will you measure success?

7
Being Proactive
What is my role as a leader?
Leaders have critical role in well-being of staff. In a 2013 study of >2800 Mayo Clinic
physicians composite leadership scores of immediate physician supervisor strongly correlated
with burnout and satisfaction scores of individual physicians. On multivariate analysis, each 1
point increase in leadership score was associated with 3.3% decrease in burnout and 9% increase
in satisfaction. Reflect on the below leadership qualities. How often and how well do you
display these behaviors with residents?
Leadership Qualities for Program Directors
Holds career development conversations with residents
Inspires residents to do their best
Empowers residents to do their job
Interested in resident’s opinion
Encourages residents to suggest ideas for improvement
Treats residents with respect and dignity
Keeps residents informed about changes taking place at work
Encourages residents to develop their talents and skills
Which aspects of the work and learning environment should be addressed?
Burnout is driven by work-related stressors. Studies of residents and medical students suggest
the work and learning environment are major contributors to their distress. Improving the work
and learning environment is a key part of the shared responsibility. Providing opportunities for
meaningful work (e.g., minimize non-physician obligations, provide administrative support,
promote progressive autonomy & flexibility, etc.), address schedules, work intensity and work
compression, and evaluate and address workplace safety data (including injuries, vehicle
collisions, well-being after adverse events) are good places to start and are also required by the
ACGME Common Program Requirements. As reciprocal relationships, timely feedback, and
emotional support from attendings have also been shown to be important for resident well-being
faculty development should target these areas in addition to fitness for duty, recognizing and
responding to impairment, psychological distress, and substance abuse in themselves and others.
Lastly, efforts should be made to cultivate community and build social support among the
residents and between residents and attendings.

8
What procedures and policies should be considered to support resident well-being?
Several procedures and policies related to resident well-being are now part of the ACGME
Common Program Requirements. These include:
Unprofessional behavior and process for reporting, investigating, and addressing
Policies and programs that encourage resident and faculty well-being
o Time away for family, personal needs, and own health
o Adequate rest, healthy diet, regular exercise
Time away for medical/psychological/dental care
Policy to ensure coverage of patient care if resident cannot perform their usual duties
(fatigue, illness, family emergencies, etc.)
What should we consider adding to our curriculum to support resident well-being?
There are a variety of individual strategies that lower the risk of burnout and may facilitate high
quality of life (Table 2). Mindfulness has also been shown to reduce burnout, but only with
volunteer participants. A behavior change framework can be used to provide residents with
experience with the process of behavioral change and help translate new knowledge into action.
Table 2. Individual Strategies
• Adequate sleep
• Build relationships & social support
• Maintain personal health
• Manage stress
• Find meaning in work
• Engage in recreation/hobbies
• Exercise
• Maintain positive outlook
• Avoid mentality of delayed
gratification
• Seek advice about debt reduction
• Maximize work-life balance
• Compliant with national exercise
guidelines
• Up-to-date with prev. health care
screening
Additionally, the core curriculum provides an opportunity to educate residents about:
their personal responsibility to be fit for duty
how to recognize impairment from illness, fatigue, substance use in themselves and
others
how to recognize fatigue and sleep deprivation and depression, burnout, and substance
abuse in themselves and others
how to assist those who experience such conditions and seek care.
These topics are required as part of the Common Program Requirements. Residency programs
may also want to show the American Foundation of Suicide Prevention and Mayo Clinic video
“Make the Difference: Preventing Medical Trainee Suicide.” The video can be used as an
educational tool to educate residents on signs to watch for in colleagues and provide them with
words to use when they are concerned about the wellness of a colleague. Effectiveness of
wellness curriculum should be subject to rigorous evaluation to ensure optimal resource
allocation. Residencies should consider adding well-being as a core competency. Doing so
would facilitate development of curricula and thoughtful assessment strategies.

9
What else should be considered?
Sponsoring institutions and residencies should have procedures in place in case of a resident
death by suicide. Doing so is important to helping a grieving community heal and to prevent
contagion. The document “After a Suicide: A Toolkit for Physician Residency/Fellowship
Programs” developed by the American Foundation of Suicide Prevention and the Mayo Clinic
provides a framework for how to develop a suicide response plan, and how to respond should
such an event occur.
Individual Resources
Self-assessment
Self-assessment of one’s level of distress is difficult, even for physicians. In a study involving
over 1100 US surgeons the surgeon’s subjective self-assessment of their well-being relative to
colleagues was poor with 89% believing their well-being was at or above average. Residency
programs must offer self-assessment tools to residents according to Common Program
Requirements. Self-assessment should rely on well-validated instruments assessing important
dimensions of well-being relevant to residents and provide immediate or near immediate
individualized feedback.
Well-Being Index
The online Resident Well-Being Index is a web-based self-assessment tool that relies on the
well-validated resident well-being index. Residents who choose to set up an account can
anonymously assess their level of well-being and receive both immediate feedback on how it
compares to residents at their institution as well as nationally and access to resources to help
promote wellness. Use of an electronic version of the Physician Well-Being Index has been
shown to improve self-calibration and promote behavioral change to improve personal well-
being. Additional information can be found at: https://www.mededwebs.com/well-being-index.
The tool is free for individual physicians, residents, and medical students to self-assess and track
their well-being over time. For locally tailored resources or access to institution/residency
specific reports (aggregate, de-identified data) a subscription is needed. An institutional license
is available that provide access to the physician, resident, medical student, nurse, advance
practice provider, and other health care worker version of the tool. The tool has been used by
more than 35,000 individuals and takes less than 1 minute to use.
American Foundation for Suicide Prevention Interactive Screening Program
Another option for organizations is the American Foundation for Suicide Prevention Interactive
Screening Program. With this program institutional counseling service provider or Employee
Assistance Program obtains a license for a customized website where employees can take a brief
questionnaire for stress and depression. The questionnaire is then reviewed by institutional EAP
or counseling service provider and a personalize message is left for the employee. The employee
logs back in to the website to obtain their message and can exchange messages with the
counselor, get feedback and encouragement, and request an appointment or referral.

10
Promote Health
Promoting health by providing no or low cost access to fitness facilities, healthy food options
while at work, relaxation or quiet rooms, and access to preventative care should be offered to
residents.
Treatment for mental health concerns
24/7 access to confidential, affordable mental health assessment, counseling, and treatment is
required as part of the common program requirements. Care for mental health concerns can be
provided in a variety of ways, including, Employee Assistance Program, primary care physician,
integrated behavioral health, and psychiatry/psychology. Care should be taken to reduce barriers
to access care, including attention to stigma of mental health issues.
Resources
Make the Difference: Preventing Medical Trainee Suicide
https://www.youtube.com/watch?v=I9GRxF9qEBA
After a Suicide: A Toolkit for Physician Residency/Fellowship Programs
http://www.acgme.org/Portals/0/PDFs/13287_AFSP_After_Suicide_Clinician_Toolkit_Final_2.
Nagy C, Schwabe D, Jones W, et al. “Time to Talk About It: Physician Depression and Suicide”
video/discussion session for interns, residents, and fellows. MedEdPORTAL Publications.
2016;12:10508. https://doi.org/10.15766/mep_2374-8265.10508
Well-Being Index https://www.mededwebs.com/well-being-index or text EZWBI to 797979
American Foundation for Suicide Prevention Interactive Screening Program https://afsp.org/our-
work/interactive-screening-program/
Bibliography
Overview Dyrbye LN, T.D. Shanafelt, C.A. Sinsky, P.F. Cipriano, J. Bhatt, A. Ommaya, C.P. West, and D. Meyers.
Burnout among health care professionals: A call to explore and address this underrecognized threat to
safe, high-quality care. NAM Perspectives. Discussion Paper, National Academy of Medicine,
Washington DC. https://nam.edu/burnout-among-health-careprofessionals-a-call-to-explore-and-
address-this-underrecognized-threat-to-safe-high-quality-care. 2017.
Dyrbye LN, Shanafelt T. A narrative review on burnout experienced by medical students and residents.
Med Educ. 2016;50:132-149.
West CP. Physician Well-Being: Expanding the Triple Aim. Journal of General Internal Medicine.
31(5):458-9, 2016 May.
Shanafelt TD; Dyrbye LN; West CP. Addressing Physician Burnout: The Way Forward. JAMA.
317(9):901-902, 2017 03 07.
Dyrbye LN; Shanafelt TD. Physician burnout: a potential threat to successful health care reform. JAMA.
305(19):2009-10, 2011 May 18.

11
Prevalence Shanafelt T, Hasan O, Dyrbye L, et al. Changes in burnout and satisfaction with work-life balance in
physicians and the general US working population between 2011 and 2014. Mayo Clin Proc.
2015;90:1600-1613.
Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career
physicians relative to the general U.S. population. Acad Med. 2014;89:443-451.
Mata DA, Ramos MA, Bansal N, et al. Prevalence of Depression and Depressive Symptoms Among
Resident Physicians: A Systematic Review and Meta-analysis. JAMA. 2015;314:2373-2383.
Brazeau CM, Shanafelt T, Satele D, Sloan J, Dyrbye LN. Distress among matriculating medical students
relative to the general population. Acad Med. 2014;89:1520-1525.
Drivers of Burnout
West C, Shanafelt T, Kolars J. Quality of life, burnout, educational debt, and medical knowledge among
internal medicine residents. JAMA. 2011;306:952-960.
Dyrbye LN, Thomas MR, Harper W, et al. The learning environment and medical student burnout: a
multicentre study. Med Educ. 2009;43:274-282.
Dyrbye LN, Thomas MR, Huntington JL, et al. Personal life events and medical student well-being: A
multicenter study. Acad Med. 2006;81:374-384.
Shanafelt TD, West CP, Sloan JA, et al. Career fit and burnout among academic faculty. Arch Intern Med.
2009;169:990-995.
Dyrbye LN, West CP, Satele D, Sloan J, TD S. Work-home conflict and burnout among academic
internal medicine physicians. Arch Intern Med. 2011;171:1207-1209.
Shanafelt T, Dyrbye LN, Sinsky C, et al. Relationship Between Clerical Burden and Characteristics of
the Electronic Environment With Physician Burnout and Professional Satisfaction. Mayo Clin Proc.
2016;91:836-848
Consequences
West C, Huschka M, Novotny P, et al. Association of perceived medical errors with resident distress and
empathy: A prospective longitudinal study. JAMA. 2006;296:1071-1078.
West CP, Tan AD, Habermann TM, Sloan JA, Shanafelt TD. Association of resident fatigue and distress
with perceived medical errors. JAMA. 2009;302:1294-1300.
West CP, Tan AD, Shanafelt TD. Association of resident fatigue and distress with occupational blood and
body fluid exposures and motor vehicle incidents. Mayo Clinic Proc. 2012;87:1138-1144.
Shanafelt T, Bradley K, Wipf J, Back A. Burnout and self-reported patient care in an Internal Medicine
residency program. Ann Intern Med. 2002;136:358-367.
Dyrbye LN, Massie FS, Jr., Eacker A, et al. Relationship between burnout and professional conduct and
attitudes among US medical students. JAMA. 2010;304:1173-1180.
Dyrbye LN, Thomas MR, Massie FS, et al. Burnout and suicidal ideation among US medical students.
Ann Intern Med. 2008;149:334.
Shanafelt TD, Balch CM, Dyrbye LN, et al. Suicidal ideation among American surgeons. Archives of
Surgery. 2011;146:54-62.
Wallace JE, Lemaire JB, Ghali WA. Physician wellness: a missing quality indicator. Lancet.
2009;374:1714-1721.
Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons.
Annals of Surgery. 2010;251:995-1000.
Shanafelt TD, Balch CM, Bechamps GJ, et al. Burnout and career satisfaction among American surgeons.
Annals of Surgery. 2009;250:463-471.
Balch CM, Oreskovich MR, Dyrbye LN, et al. Personal consequences of malpractice lawsuits on
American surgeons. J Am Coll Surg. 2011;213:657-667.
Shanafelt T, L.N. D, West CP, Sinsky C. Potential Impact of Burnout on the US Physician
Workforce.Mayo Clin Proc. 2016;91:1667-1668. doi: 1610.1016/j.mayocp.2016.1608.1016.

12
Shanafelt TD, Mungo M, Schmitgen J, et al. Longitudinal Study Evaluating the Association Between
Physician Burnout and Changes in Professional Work Effort. Mayo Clinic Proceedings. 2016;91:422-
431.
Jackson ER, Shanafelt TD, Hasan O, Satele D, L.N. D. Burnout and Alcohol Abuse/Dependence Among
U.S. Medical Students. Acad Med. 2016;91:1251-1256
Oreskovich MR, Shanafelt T, Dyrbye LN, et al. The prevalence of substance use disorders in American
physicians. Am J Addictions. 2014:1-9.
Interventions, Organizational and Individual Strategies
West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a
systematic review and meta-analysis. The Lancet. 2016.
Shanafelt T, Noseworthy JH. Executive leadership and physician well-being: Nine organizational
strategies to promote engagement and reduce burnout. Mayo Clin Proc. 2016;92:129-146.
Shanafelt TD, Gorringe G, Menaker R, et al. Impact of organizational leadership on physician burnout
and satisfaction. Mayo Clinic Proceedings. 2015;90:432-440.
Shanafelt TD, Oreskovich MR, Dyrbye LN, et al. Avoiding burnout: the personal health habits and
wellness practices of US surgeons. Ann Surg. 2012;255:625-633.
West C, Dyrbye L, Rabatin J, et al. Intervention to promote physician well-being, job satisfaction, and
professionalism: a randomized clinical trial. JAMA Intern Med. 2014;174:527-533.
Krasner MS, Epstein RM, Beckman H, et al. Association of an educational program in mindful
communication with burnout, empathy, and attitudes among primary care physicians. JAMA.
2009;302:1284-1293.
Kushner RF, Kessler S, McGaghie WC. Using behavior change plans to improve medical student self-
care. Acad Med. 2011;86:901-906
Moutier C, Norcross W, Jong P, et al. The suicide prevention and depression awareness program at the
University of California, San Diego School of Medicine. Acad Med. 2012;87:320-326
Measurement tools
Shanafelt T, Kaups KA, Nelson H, et al. An interactive individualized intervention to promote behavioral
change to increase personal well-being in US surgeons. Ann Surg. 2014;259:82-88.
Dyrbye LN, Satele D, Shanafelt T. Ability of a 9-Item Well-Being Index to Identify Distress and Stratify
Quality of Life in US Workers. J Occup Environ Med. 2016;58:810-817.
Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Utility of a brief screening tool to identify physicians in
distress. J Gen Intern Med. 2013;28:421-427.
Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Ability of the Physician Well-Being Index to identify
residents in distress. J Grad Med Educ. 2014;6:78-84.
West CP, Dyrbye LN, Sloan JA, Shanafelt TD. Single item measures of emotional exhaustion and
depersonalization are useful for assessing burnout in medical professionals. Journal of General Internal
Medicine. 2009;24:1318-1321.
West CP, Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Concurrent validity of single-item measures of
emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. 2012;27:1445-
1452.
Dolan ED, Mohr D, Lempa M, et al. Using a single item to measure burnout in primary care staff: a
psychometric evaluation. Journal of General Internal Medicine. 2015;30:582-587.
Rohland BM, Kruse GR, Rohrer JE. Validation of a single-item measure of burnout against the Maslach
Burnout Inventory among Physicians. Stress and Health. 2004;20:75-79.
Waddimba AC, Scribani M, Nieves MA, Krupa N, May JJ. Validation of single-item screening measures
for provider burnout in a rural health care network. Eval Health Prof. 2015;39:215-225

13
ACGME Common Program Requirements VI Well-Being
Section
Common Program Requirements Checklist
Professionalism
VI.B.4.c).(2)
(educate)
Residents and faculty members must demonstrate an
understanding of their personal role in the: assurance of fitness
for work, including recognition of impairment, including from
illness, fatigue, and substance use, in themselves, their peers,
and other members of the health care team
Well-being
VI.C.1.a)
(work
environt.)
Efforts to enhance meaning in work (minimize non physician
obligations, provide administrative support, promote
progressive autonomy and flexibility, and enhance professional
relationships)
VI.C.1.b)
(work
environt.)
Attention to scheduling, work intensity, and work compression
VI.C.1.c)
(work
environt.)
Evaluate workplace safety data and address safety of residents
and faculty
VI.C.1.d)
(Policies and
procedures)
Policies and programs that encourage optimal resident and
faculty well-being
VI.C.1.d)(1)
(Policies and
procedures)
Residents must be given opportunity to attend medical, mental
health, and dental care appointments, including during
scheduled work hours
VI.C.1.e)
(educate)
Attention to resident and faculty burnout, depression, and
substance abuse. Must educate faculty and residents in
identification of symptoms of burnout, depression, substance
abuse, including means to assist those who experience these
conditions. Residents and faculty must also be educated to
recognize these symptoms in themselves and how to seek
appropriate care
VI.C.1.e)(1)
(educate)
Encourage residents and faculty to alert PD or other personnel
or programs when they are concerned that another resident,
fellow, or faculty may be displaying signs of burnout,
depression, substance abuse, suicidal ideation, or potential for
violence
VI.C.1.e)(2)
(resource)
Provide access to appropriate tools for self-screening
VI.C.1.e)(3)
(resource)
Provide access to confidential, affordable mental health
assessment, counseling, and treatment, including access to
urgent and emergent care 24/7
VI.C.2
(Policies and
procedures)
Policies and procedures to ensure coverage of patient care in
event that a resident may be unable to perform patient care
responsibilities. Implementation of policies without fear of
negative consequences for the resident who is unable to work

14
Notes:

2017-2018 SEMCME FACULTY DEVELOPMENT SERIES: Achieving Excellence: Hiring the Best. Developing the Best. Keeping the Best.
∙∙∙
Building a Comprehensive Approach to Wellness in the Residency
September 15, 2017
Lisolotte Dyrbye, MD, MHPE, FACP is
Professor of Medicine, Professor of Medical Education, and Consultant in the Division of Primary Care Internal Medicine at Mayo Clinic, Rochester, Minnesota. She is also Associate Chair for Faculty Development, Staff Satisfaction, and Diversity for the Department of Medicine, Mayo Clinic, Director of Faculty Development for Mayo Clinic School of Graduate Medical Education, and Associate Director of the Department of Medicine Program on Physician Well-being. She is the Primary Investigator on Mayo Medical School’s grant “Accelerating Change in Medical Education,” awarded by the AMA.
Dr. Dyrbye is a graduate of the University of Wisconsin Medical School where she was selected AOA and she subsequently completed an internship and residency in Internal Medicine at the University of Washington. She also holds a Masters in Health Profession Education from University of Illinois completed in 2009. She holds numerous national education leadership positions including National Board of Medical Examiners USMLE Ambulatory Medicine Test Material Development Committee, Association of American Medical Colleges Research in Medical Education (RIME) Conference Planning Committee Past Chair, and Association for Medical Educators of Europe (AMEE) Research Committee. She is a past councilor for Clerkship Directors of Internal Medicine. She has published 74 peer-reviewed publications many in elite journals. In 2008, she received the Clerkship Directors of Internal Medicine Charles H Griffith Educational research award – awarded to the single Clerkship Directors of Internal Medicine member who has made the greatest impact on medical education over the preceding year. In 2012, she received the only ABIM Professionalism Article Prize in the field of medical education and training for her article “A Multi-Institutional Study Exploring the Impact of Positive Mental Health on Medical Students’ Professionalism in an Era of High Burnout,” published in Academic Medicine. In 2014, she was award the Deans recognition award for her contributions to Mayo Medical School. Her research interests are focused on medical student competency, professionalism, and well-being and she has received 11 competitive research grants to support this work. Dr. Dyrbye is currently recognized as the world expert on medical student, resident, and physician well-being.

Faculty Development Wellness Workshop 9/15/17
Participant Ideas for Reducing Resident Stress (notecard exercise)
I would have regular scheduled social events each month sponsored by the department
Laid back journal club with residents and attendings once a month
Make mindfulness part of monthly meeting
Therapy dogs
Coloring
Develop a mentorship; and get the suicide prevention video
Teach resilience techniques
Have a mentor/wellness program for my residents
Set up a mentoring program and set aside time to meet with each other weekly or bi-weekly to discuss personal
or professional problems
Hire someone to do coding and order entry
Provide quality and affordable onsite child care with extended hours without penalty
Incorporate more open dialogue with faculty about other aspects of residents lives not just medicine
Allow time in residents days to reflect
Promote a sense of community by developing a group that plans activities directly in the city of the hospital
Bring daycare facility to hospital
Provide more ability for social time with co-workers and family
Have more regular sessions that identify conditions that contribute to burnout and methods to address it
Distinguish between burnout and perceived burnout by residents
Quarterly get together sessions (residents and faculty and their families)
Restructure administrative times to build regular work time to finish administrative duties
More outings outside of work
Increase admin support for residents
Encourage more out of work activities that the residents can do together
I would improve the mentoring the trainees receive
Implement an exercise program
Make the attendings write them thank you/appreciation cards
Organize out of work social activities (golf outing, bowling, BBQ, bake Christmas cookies)
Have them rate themselves on their own well-being to obtain a starting point for intervention
Create a wellness evening or event geared towards the resident group
Develop social activities to improve relationships/get ideas from residents and physicians then schedule the
activities
Team building/wellness activities throughout the year
Reduce burnout by: partner faculty into mentorship with residents
Provide increased clinical and administrative support including a culture shift among faculty to support and
value resident education and contributions
Personal assistants/concierge service to help with errands and personal tasks that would be housed at the
hospital
Schedule fun/active wellness activities
Keep a friendly environment where residents can bring up their concerns
Make duty hours less per week
Allow flexibility when possible
Frequent burnout assessments
Reduce workload when possible

Reduce paper/unnecessary work
Increase physical exercise and socialization
Provide 1-2x/week exercise group for residents and faculty
Would also increase resident/faculty interaction outside work situation
Have a counselor/social worker as a safe designated person who is readily available, that residents can go to
when feeling overwhelmed or need to access resources
Set aside administrative time for them to get their clerical/computer work done
Tag onto ½ day academics
Pull them all off all service one time each month to go somewhere fun for the entire day, including their families
Wellness/stress reduce strategies on a continuum
Monthly program sessions to foster community (dinner, discussion of stressors or a wellness type topic or case)
Develop relationships to prevent doctors in isolation –Mentor/Mentee develop program that is interdisciplinary
Bring in teaching/social worker to help develop individual coping mechanism
More free time to do activities
Encourage use of vacation time and shared holiday coverage
Improve communication with program and faculty
Assist in planning clear and reasonable rotation and PGY expectations and discuss them at rotation onset,
midpoint and end
Discuss results of survey with residents that was completed and discuss/solicit their ideas for focus on an action
plan
Respond to our problems/concerns and work together to bring change
Try to increase autonomy with practical work flow solutions
Create emotional support groups including 1 resident from each class supporting each other/knowing their not
alone
Set up a wellness program with 1 hour a 1 month of interaction
Talk about expectation and feedback
Identify how many residents feel burnout and why, send out a survey or self-assessment
All-hour childcare at base hospital
Scheduled time for wellness activities/regular breaks from patient care
Encourage honest, proactive discussions
Bring them coffee and donuts
Hold regular meetings to get feedback, see what is going well and what needs to be changed
Teach residents to be more efficient
Give them a ½ day off each week in the afternoon
No 24 hour calls
Cut back their hours
Program needs to be more organized
Vacation time
More positive feedback from faculty
Give more vacation time
Get rid of all 24 hour calls
Maximum shift 16 hours
Place a time cap on admissions at night
Provide support for non-medical tasks that are now done by residents
I want to give them option to provide solutions to clinic issues or schedules so they have some control
I will set up meetings with fellows with agenda and to get their feedback in problems
Give residents one ½ day off the work week, during daytime hours to get normal life/health activities done

Put together a schedule and determine how clinical needs would get met during those times
Implement monthly/quarterly social activities
Hire scribes to assist with note writing
Nutrition and exercise
Engage their family into the hospital atmosphere
Increase the feeling of community
Identify residents who are not engaged with colleagues at work
Have planned recreational time or time for group get-togethers
Change the hours of certain rotations (8 hour work day)
Integrate resident wellness curriculum into didactics
Start resident wellness committee to integrate into each program
Create small groups for hanging out so to increase community support
Train faculty to provide effective supervision 1 on 1 to residents weekly
Lessen the amount of modules
Enhance outside social activities
Mandatory counseling for all residents
Recognize compliancy at all levels
Due to a day off during the week
Conduct a survey to measure burnout in medical students/residents
Create and mind communication tool so students/residents can reach out for help
Find a way to make the EMR process less time consuming
Engaging in the program (their work and opinions matter in the process)
When you’re starting to feel the pressures of residency, they have a safe place to go and talk
Increase faculty to increase supervision
Decrease ICU load
Have them keep a sleep journal
Limit moonlighting
Reducing duty hours and patient loads
Determine how to incorporate teachings within a reasonable time to decrease fatigue and malpractice
Social support – have them meet with faculty outside of work
We need to decide what is the most important thing they have to learn and focus on it
Give them lunch for noon conference to cut back on time stress
Improve social support between residents – more team rotations
Improve the learning climate
More wellness among all programs
Quarterly wellness events put on by GME
Wellness days 5 to 6 times a year
Standard hospital rounds
One or two times per month outside fun event
Give rid of lazy attendings, identify who they are
Increase administration support for residents
To reduce burnout, I would establish time each month for residents to bring their family to work and have
designated space to meet with them
Make them feel needed, not feel like they are not important
Give them food, something for them to look forward to coming into work for the day
Help evaluate Work-Life balance and give support
Decrease the patient volume they see

Decrease the number of shifts
Increase residency size
Remove patient volume number criteria from program requirements/reduce load to increase time to learn
Remove some attendings from resident teaching and conferences
Send them all on a vacation with the PD and PC
Work less hours
Teach resilience
I would create an anonymous grievance system, totally confidential





























