Embed Size (px)
Citation preview

Inhibition of C3 with APL-2 Results in Normalisation of Markers of Intravascular and Extravascular Haemolysis in Patients with Paroxysmal Nocturnal Haemoglobinuria
Update From the PADDOCK Clinical Trial (Apellis)
BSH2019-328

BSH2019-328
Paroxysmal Nocturnal Haemoglobinuria (PNH)
2
MAC-associated IVH
C3b-mediated opsonization (EVH)
1.Anemia, hemolytic, acquired autoimmune. National Organization for Rare Disorders Web site. https://rarediseases.org/rare-diseases/anemia-hemolytic-acquired-autoimmune/. Accessed March 1, 2018.
• PNH is characterized by bone marrow failure and complement mediated haemolysis resulting in anemia and an increased risk of thrombosis1 :
o Intravascular haemolysis (IVH) mediated by the membrane attack complex (MAC), and
o Extravascular haemolysis (EVH) resulting from C3b opsonization on the surface of defective RBCs

BSH2019-328
Complement C3 is Central in the Disease Pathology of PNH
3
• C3 centrally controls the complement cascade and all subsequent immune responses mediated by complement1,2
o RBC opsonization, which is responsible for C3b-mediated extravascular hemolysis
o C3b activation of C5 convertase, and the subsequent formation of the Membrane Attack Complex (MAC)
o C3b re-uptake resulting in activation of the amplification loop via the alternative complement pathway
1. Rosse WF, Ware RE. The molecular basis of paroxysmal nocturnal hemoglobinuria. Blood. 1995;86(9):3277-3286. 2. Rother RP, Bell L, Hillmen P, Gladwin MT. The clinical sequelae of intravascular hemolysis and extracellular plasma hemoglobin: a novel mechanism of human disease. JAMA. 2005;293(13):1653-1662.

BSH2019-3284
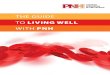
Haemoglobin Levels in Patients Receiving Eculizumab
Source: Peter Hillmen, Professor of Experimental Haematology, University of Leeds
0
2
4
6
8
8 10 12 14 16 18
Num
ber o
f pat
ient
s
Normal individualsPNH patients on eculizumab
>4 g/dL
Hemoglobin (gm/dl)

BSH2019-3285
Haemoglobin Levels & Transfusions in Patients on Eculizumab
~30% of Patients• Transfusion -• Hb >12
~40% of Patients• Transfusion -• Hb <12
~20% of Patients• Transfusion ++• Hb <10
~10% of Patients• Breakthrough ++• Hb = any
v v
1. Risitano AM, Notaro R, Marando L, et al. Complement fraction 3 binding on erythrocytes as additional mechanism of disease in paroxysmal nocturnal hemoglobinuria patients treated by [a C5 inhibitor]. Blood. 2009;113(17):4094-4100.

BSH2019-328
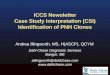
APL-2 Inhibits Complement Protein C3
Lectin Pathway
C5aC3b
C5b MAC
Inflammation
Cell removal, Antigen uptake
by APCs
C5
C3a Inflammation
Classical Pathway
Alternative Pathway
APL-2
C3
6
Cell death, secretion, lysis, or proliferation

Update From the PADDOCK Clinical Trial
7
BSH2019-328

BSH2019-328
Eligibility & Study Design
8
PADDOCK Study Design: APL-2 Monotherapy in Eculizumab-naïve PNH*
* Data is presented from the ongoing study

BSH2019-328
Study Disposition
9
Characteristic Cohort 1 Cohort 2 Overall
Screened Subjects, n 30
Randomized Subjects, n 3 20 23
No. Withdrawn, n 1 4 5
No. Ongoing, n 0 16 16
Completed Study, n 2 0 2
Primary Reason for Withdrawal
Adverse Event, n (%) 0 2 (10.0) 2 (8.7)
Other, n (%) 1 (33.3) 2 (10.0) 3 (13.0)

BSH2019-328
Demographics
10
Baseline Characteristics Cohort 1(180 mg, n=3)
Cohort 2(270 mg, n=20)
Overall(n=23)
Age, years, mean (SD) 42 (16.6) 41.9 (13.3) 42 (13.3)Sex, n (%)Male 2 (66.7) 11 (55.0) 13 (56.5)Female 1 (33.3) 9 (45.0) 10 (43.5)
Ethnicity, n (%)Non-Hispanic or Latino 3 (100) 19 (95.0) 22 (95.7)Unknown 0 1 (5.0) 1 (4.3)
Race, n (%)White 3 (100) 1 (5.0) 4 (17.4)Non-white 0 19 (95.0) 19 (82.6)Native Hawaiian/Pacific Islander 0 1 (5.0) 1 (5.0)Asian 0 15 (75.0) 15 (75.0)Other 0 3 (15.0) 3 (15.0)
Weight, kg, mean (SD) 76.67 (17.9) 67.43 (15.5) 68.63 (15.7)Height, cm, mean (SD) 169.3 (6.0) 165.2 (10.9) 165.7 (10.4)BMI, kg/m2, mean (SD) 26.50 (4.4) 24.58 (4.5) 24.84 (4.4)Number of units pRBCs transfused per patient (prior year pre-screening) 8.7a
Hemoglobin (g/dL) 8.0 (0.6)LDH (IU/L) 2416 (237)Bilirubin (µmol/L) 41.6 (6.3)

BSH2019-328
Study Disposition
11
Baseline (Day 1) Day 29 Day 85
Haemoglobin (g/dL) 8.0 ± 0.6 10.8 ± 0.7 12.2 ± 0.5
Lactate dehydrogenase (LDH)a2416 ± 237(9.7 x ULN)
184 ± 18(0.7 x ULN)
271 ± 13(0.9 x ULN)
ARC (x109/L)b198.6 ± 14.1(2.0 x ULN)
81.4 ± 13.3(0.8 x ULN)
101.8 ± 7.6(1.0 x ULN)
Bilirubin (µmol/L)41.6 ± 6.3
(2.0 x ULN)10.3 ± 1.5
(0.5 x ULN)14.0 ± 1.4
(0.7 x ULN)
a ULN = 250 IU/Lb ULN = 100 x 109/L

BSH2019-328
Results: Haemoglobin
12
Rapid, Sustained and Durable Increase in Haemoglobin (Hb) in Response to APL-2

BSH2019-328
Results: Haemoglobin and Transfusions
13
Increase in Haemoglobin (Hb) Transfusions1 Year Before
Screening During Studya
Mean Number of pRBC Units8.7
(range: 9 to 28)1.9b
(range: 2 to 26)
Number of Subjects Receiving Transfusions 17 4c

BSH2019-328
Results: Lactate Dehydrogenase
14
Rapid, Sustained and Durable Decrease in LDH in Response to APL-2

BSH2019-328
Results: Reticulocyte Count
15
Rapid and Sustained Decrease in Absolute Reticulocyte Count (ARC) in Response to APL-2

BSH2019-328
Results: Total Bilirubin
16
Rapid, Sustained and Durable Decrease in Total Bilirubin in Response to APL-2

BSH2019-328
Results: Flow Cytometry
17
Rapid, Sustained and Durable Increases in Clonal Distribution of PNH Type III RBCs

BSH2019-328
Results: Quality of Life Assessment (FACIT-Fatigue)
18
Rapid, Sustained and Durable Improvement in FACIT Fatigue Score

BSH2019-328
Safety of APL-2
19
Category Cohort 1 (N=3)
Cohort 2(N=20)
Overall(N=23)
n (%) m n (%) m n (%) m
Any TEAE 2 (66.7) 8 15 (75.0) 86 17 (73.9) 94
Serious TEAE 1 (33.3) 2 4 (20.0) 14 5 (21.7) 16
TEAEs Related to Investigational Product 2 (66.7) 7 11 (55.0) 31 13 (56.5) 38
TEAEs Leading to Dose Discontinuation 1 (33.3) 1 1 (5.0) 1 2 (8.7) 2
Severe TEAE 0 7 (35.0) 17 7 (30.4) 17
a As of November 2018. n = number of subjects that experienced the event, m = number of events

BSH2019-328
Conclusion• Treatment with APL-2 in complement inhibitor-naïve PNH patients resulted
in rapid and durable normalisation of Hb, LDH, ARC and Total Bilirubin
• Previously transfusion-dependent patients did not require any transfusions during maintenance treatment with APL-2a
• Clinically-relevant improvement in FACIT-Fatigue score was observed
• APL-2 was well-tolerated
• Inhibition of C3 with APL-2 addressed both the intravascular and extravascular haemolysis in subjects with PNH
20