-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
1/39
GUIDES:- Sh. S.K. Sharma(Lecturer)
Sh.A.P. Chauhan(Tutor)
PRESENTED BY:- Keshav Raj Poudel
DEPARTMENT OFHAEMATOLOGY
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
2/39
PAROXYMAL NOCTURNAL HAEMOGLOBINURIA (PNH)PNH is the chronic
disorder in which I/V
haemolysis occurs due to acquired defects in Redcells which
renders the membrane highlysusceptible to lysis by complement. It
is a clonaldisorder due to somatic mutation in multipotent
haemopoietic stem cells. White cells and plateletsare also
affected by mutation and thrombosis is adangerous complication. In
many cases theemergence of PNH clone is closely linked to
underlying defect of marrow function, particularlyaplastic
anemia, myelosclerosis and leukemia.Symptom is ordinarily dominated
by chronichaemolysis and occasionally terminates as acute
myelogenous leukemia.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
3/39
Etiology and Pathogenesis:
PNH is due to the somatic mutation of a geneon x- chromosome
which enclose a protein- phosphatidyl
glycan protein A(PGPA). Protein A which is essential for
theformation ofglycerol phosphotidyl inositol (GPI) . It acts as
ananchor protein by which no of proteins are attached to
RBCmembrane
S.N
Proteins Examples Designation
1. Compliment
regulatoryproteins
*decay accelerating factor
*membrane inhibition of reactivelysis*C8 binding proteins
(HRF)
*DAF,CD55,
MIRL, CD59C8BP, HRF
2. ENZYMES Erythrocyte acetyl colin esteraseNeutrophil alkaline
phosphatase
NAP
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
4/39
3. Immunefunctionproteins
Lymphocytes function antigen 3-Neutrophil Fcy iii
receptor-Monocyte endotoxin binding
protein receptor- Campath binding protein
LFA 3CD16 aCD14
CD52
4. Otherproteins
Monocyte urokinase receptorJMH antigen binding protein
Four granulocyte surface proteinFolate receptor
Among these different proteins two proteins normally protect
the cell from lysis by activated complement . They are :1. Decay
accelerating factor (CD55)2.Membrane inhibitor of reactive
lysis(MIRL or CD59)
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
5/39
CD55 accelerates the conversion of C3b to inactivate C3d .
CD59 protects the cell from lysis by the membrane attackcomplex
, the final product of complement activation
GPI anchored proteins are also missing from white cells
andplatelets results thrombotic tendency in PNH patient .
There are three population of PNH red cells according to
thedeficiency of CD59.
a) Very sensitive PNH (type III) red cell: 10 -15 times
moresensitive than normal. PNH type III red cell have
completedeficiency of CD59 and lysed by cobra venom factor.
b) Cells of medium sensitivity(type II) : 3-5 times more
sensitive
than normal cells. They have only partial deficiency of CD
59,dont lysed by cobra venom factor.
c) Cells of normal sensitive(type I) : They are equally
sensitive asnormal cells and lack enzyme Erythrocyte
acetylcolinestarase.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
6/39
In vivo the proportion of type III cells parallel the severity
ofpatient haemolysis.
78% of PNH patients blood contains a simple mixture of
PNHI and PNH III cells.- Haemolysis is mild when the proportion
of PNH III cells is
50%
Decay accelerating factor CD55 :
It is a 70,000 molecular weight glycoprotein that binds to C3b
and C4b fragments deposit in the cell membranes, blocksassembly of
the convertase complex ( C4b2b of classicalpathway and C3bBb
complex of the alternative pathway
)and hasten their decay.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
7/39
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
8/39
Complements and its activation Pathways
Complement constitutes of the series of protein, mainly
enzymes
present in the fresh plasma as inactive precursor, which
reactsequentially with each other to form product that are
importantin the destruction of the cells, bacteria etc.
There are total 9 complements denoted by C1-C9. They are
activated in two stages.Stages of complement activation
1. Optionization phase
2. Lytic stage
Optionization phase:
This phase is completed in two pathways
1. Classical pathway
2. Alternative pathway
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
9/39
Classical pathway It can be activated by antigen antibody
complex
,enzymes(tripsin, plasmin , lysosomal enzyme) , Endotoxin,low
ionic strength media etc. Only one molecule of IgM or atleast two
molecules of IgG on the red cell membrane isnecessary to activate
the complement system because IgM Abcarries several C1q binding
sites whereas one mol. of IgG carry
only one. First component of the complement activation is
formation of
complex of three protein molecules C1q, C1r and C1s
After Abs bound to their Ag, C1 binding sites are exposedon the
Fc fragment , C1q sub units binds to it andactivates C1r which in
turns cleaves the third moleculeC1s, yielding a active enzyme form
of C1 complex which isheld together by calcium. In the presence of
EDTA orother chelating agent the complex falls apart and whole
process of complement fixation will not occur.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
10/39
This complex activates sequentially C4 ad C2 inthe presence of
Mg++, generates secondenzyme, C4b2b called C3 convertase.
The cell bounded C3 convertase optimallyactivates several
thousand mol. Since, largeamount of C3 is present in the cell.
C3b attach red cell will adhere to the Monocyteand macrophages
though their C3b receptors
and may be phagocytes or it is rapidlydegraded by an enzyme (C3b
inactivator,factor I ) to C3d remain in the red cell surface.
By occupying the binding C3 sites by C3d , canprevent the
further binding of C3b. C3d,unlike C3b is not capable of adhering
to thereceptor on macrophages and monocyte sothat the cell coated
with C3d may return tothe circulation and will be resistant to
thefurther lysis.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
11/39
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
12/39
Alternative pathway Does not necessary involves Ag Ab reaction
and represents
non specific innate immunity . The alternative pathway can
be activated by IgA , zymosen, bacterial cell
orLipopolysaccharides.
It is two step process.
1. Binding of C3b to the activator and interaction of bound
C3b with neighboring surface structure initiallyspontaneously
generate fluid phase C3b interact with thefactor B to form a
complex .
2. Factor B is activated through a cleavage by the
proteasefactor D releasing a fragment Ba into the plasma and
yielding a transient alternative C3 convertase ( C3bBb)3. C3
convertase ( C3bBb) can be stabilized by properdin.
Although, properdin is no longer implicated ininitiating the
alternating pathway, it is essential for
preventing the dissociation of C3bBb by factor H.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
13/39
Alternative C3 convertase splits serum C3 into C3a and C3b .
The amount of C3b deposited by alternative pathway is low
due to the small amount of the convertase generated and tothe
insufficient deposition of C3b from plasma. Thiscontrasts with the
vast no. of C3b molecules generated bythe classical pathway.
The classical and alternative pathway cannot beseparated from
each other in vivo, the alternative pathwayamplified the classical
pathway because, when C3b isgenerated, factor B and D may be
activated and complex
with it to generate further C3b.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
14/39
The Lytic Phase of complement sequence
It start with the activation of C5 by C3b, yielding
membranebounded C5b and fluid phase C5a. This step is followed
by
the non enzymatic interaction of C5b with C6, C7, C8 andC9.
These molecule adhere to each other to form membraneattack
complex (MAC) and insert themselves to the lipidbilayer of the red
cell membrane. C8 catalyzed by C9produced lesion in the membrane
.These lesions appears asprotein linked cylinders in the red cell
membrane. and areabout 10 nm in diameter. They form pores through
whichions and water cam enter. The osmotic pressure by Hb draw
water into the cell until it swells and burst.Optimum
temperature and pH for complement lysis:
Optimum pH 6.8
Optimum temperature 32-37oC, below 15 red cell cant behaemolysed
by complement
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
15/39
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
16/39
Clinical Features
1. Nocturnal I/v Haemolysis with negative DAT(
occasionallypositive)
2. Nocturnal Haemolysis with low platelets, low WBC counts.
3. Symptoms of anemia and Nocturnal Hemoglobinuria with
darkurine.
4. Recurrent abdominal pain with or without blood in stool.5.
Hepatic vein thrombosis.(Budd-chairi syndrome)
6. Pancytopenia and marrow failure, particularly if there is a
reactivereticulocytosis.
7. Abdominal pain, headache.
8. Thrombophlebitis and thromboembolism
9. Mild jaundice.
10. Mild spleenomegaly.
11. Mild hepatomegaly, marked hepatomegaly in hepatic vein
thrombosis.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
17/39
Laboratory DiagnosisHaemogram :
HB decreased
PCV decreasedRBC count decreasedWBC count mild decreased
Platelets count mild decreasedMCV normal
MCH normalMCHC normal
MCV,MCH,MCHC decrease in chronic caseReticulocyte count
increased but lesser than expected for
degree of anaemia because retics are more
susceptible to compliment lysis thanmature PNH red cell.DLC Mild
neutropeniaPBF N/N , mild macrocytic and mild microcytic
hypochromic RBCs, Neuropenia and Thrombocytopenia
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
18/39
Signs of I/V Haemolysis
Plasma Hb High
Urine Hb Present
Haemosidenuria PositiveHeptoglobin Decreased or Absent
Haemopexin Decreased
Methemealbumin Increased
LDH IncreasedBilirubin Increased
Urine urobilinogen Increased
Othre tests
Methemoglobin IncreasedSerum iron Decreased
Serum ferritin Decreased
DAT Negative , occasionally positive
OFT Normal
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
19/39
NAP (Neutrophil Alkaline Phosphate): Reduced
PNH patient usually possess a sub population of granulocyte
thatexhibit impaired phagocytosis and chemotaxis when exposed
to
activated complement. Mutant granulocyte in PNH are asdeficient
in leukocyte alkaline phosphatase as the granulocyteof CML. Only
those PNH granulocytes that are deficient in LAPare unresponsive to
chemoattractants . Lack of LAP in CMLgranulocyte is associated with
absence of L AP mRNA, whereasin PNH LAP mRNA is normal.
Bone Marrow:
Normoblastic Erythroid Hyperplasia, rarely Megaloblastic
,Megakaryocytes are diminished, in pancytopenia , BM
ishypoplastic.
.
Specific test for PNH :
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
20/39
Specific test for PNH :
Definitive diag. of PNH in vitro is done by variety of
tests-
1. By the activation of alternative pathway. Eg
a)HAMS test
2. By the activation of classical pathways Eg.
a) Sucrose lysis test
3.Flowcytometric analysis
HAMS test:
The standard Hams test significantly underestimates proportional
PNHred cells. The standard Hams test can be negative when there are
less
than 5% PNH type III cells or less than 20% PNH type II cells.
Whenthe Hems test is supplemented with Mg , to optimize the
activation ofcompliment, the percentage lysis gives the more
accurate estimation ofproportion of PNH cells.
Methods: 1) Hams test 2) Modified Hams test
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
21/39
principlePatient red cells undergo haemolysis when incubated
with
compatible acidified serum (PH-6.5-7.0) at 37oC.The serum
may
be of the patient serum or from another normal subject.The
sensitivity of Hams test can be improved by the addition of
Magnesium to the test to enhance the activation of
compliment.
Sample collection:
Every effort must be made to prevent haemolysis during
collectionand manipulation of sample.
Defibrinated blood collection:
5-6 ml of patients or normal controls blood is collected in
a
disposable syringe having wide bore needle with clean
venipuncture. Blood is poured into the flask of 20 ml
capacitycontaining 5-10 glass beads. The flask is gently rotated
until theblood is clotted(10- 15 mins). Place the flask inside
incubator for
5mins. Then the fluid portion is taken out in a clean test
tubeand serum is separated after centrifugation at low speed.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
22/39
Preparation of Fresh normal serum:ABO group compatible normal
serumThere is variability between the sera of individual in there
capacity to
lyse PNH Red cells . The activity of a single individual s serum
also
varies from time to time. Therefore those normal controls are
takenwhose serum sufficiently lyse PNH RBCs.Required for test:a)
Normal fresh serumb) Patients serum
c) 50% normal cells suspensiond) 50% patients cells
suspensionpreparation of heat inactivated serum:Serum is placed in
tube and tubes are placed in water bath at 56oC for
30.
5)Positive control:It is always important to include in any test
, as a positive control , a
sample of known PNH cells or artificially created PNH
likecells(sulphydryl compounds, can act on normal red cells in
vitro so asto increase there compliment sensitivity)
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
23/39
Requirements:
Apparatus:
1) Flasks(20ml) with some piece of glass beads.
2.) Centrifuge 3) Test tube & test tube rack4) Water bath 5)
Pipettes
6) Spectrophotometer
Reagents:
1) 0.2 mole/ l HCL 2) Normal saline
3) 250 m mol/l MgCl2 ( 23.7 g/l)Procedure
S.N REASENT CONTROL CELL
1.
/CONTROLSERU
M2. 3.
TESTcells
4.
/CONTROLSERUM
5. 6.
TESTSERUM
7.
/TESTCELLS
8. 9.
1. Fresh normalserum(ml)
0.5 0.5 0.5 0.5 0.5 0.5 - - -
2. Patients
serum(ml)
- - - - - - 0.5 0.5 0.5
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
24/39
Heat inactivate the serum of Tube no 3,6 and 9.
3 0.2mol/l HCL(ml)
- 0.05 .05 - 0.05 0.05 - 0.05 .05
4 50% patientRBCs (ml)
- - - 0.05 0.05 0.05 0.05 0.05 .05
5 50% normalRBCs (ml)
0.05 0.05 .05 - - - - - -
6 250mol/l MgCl2(ml)
0.01 0.01 .01 0.01 0.01 0.01 0.01 0.01 .01
Mix the content and leave for 1hr at 37C.Centrifuge and look for
haemolysis on tube no. 5 and 8.
Calculation of % of lysis.Blank- normal serum 0.5ml100% lysis(
standard) - 50% washed red cells
0.05 ml in o.55ml water.Test - Supernatant of tube no.5 or 8
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
25/39
Take 0.3ml of each blank, 100% lysis RBCS and supernatant oftest
tube to be tested for haemolysis in 5ml of 0.4ml/l amonia
ordrabkins reagent.
Measure the lysis in the photoelectric colorimeter using the
yellow green filter or in spectrometer at a wavelength of 540
nm. Calculation: % lysis = (Test Blank ) 100
(Std Blank)
False Positive Result:HEMPAS gives positive Hams test withnormal
serum but not withpatients serum. In HEMPAS lysis is due to the
presence ofunusual Ag on red cell surface which react with
complementfixing IgM Ab (anti HEMPAS) present in many but not in
all
sera.Markedly spherocytic red cells may lyse in acidify serum
probablydue to lowered pH and such cells may lyse too in
acidifiedinactive serum.
If acidify serum test is Positive . It is recommended to carry
out
direct AGT . If it is positive the lysis could be due to lytic
Ab.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
26/39
Sucrose lysis test
It is useful screening test for PNH. It is more sensitive than
Hams
test but lack the specificity.Principle:
Red cell absorbed the compliment from serum at low
ionicstrength. PNH cells is greater sensitive to complement
undergoeslysis but not normal cells.
More than 10% lysis implies a positive test. 5-10% lysis is
boarderline . The red cells of some cases of Leukemia or
myelosclerosisgives less than 10% lysis. The sucrose lysis test is
typically neg. inHEMPAS(hereditary erythroid multinuclearity
associated with apositive acidified serum)
Reagent :
a) Iso osmotic solution of sucrose(92.4 g/l)
Procedure:
Take 2 tubes 12*75 mm and proceed as
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
27/39
Incubation at 37 0C for 30 , centrifuge the tubes and examine
for lysis .Calculation of % of lysis.Blank- Supernatant of tube no.
2
100% lysis( standard) - 50% washed red cells0.1ml in 0.9 ml of
ammonia 0.4 ml/l .Test - Supernatant of tube no.1Measure the lysis
in the photoelectric colorimeter using the yellow green filter or
inspectrometer at a wavelength of 540 nm as above.Calculation: %
lysis = (Test Blank ) 100
(Std Blank)
Reagents Tube No 1.(test)
Tube No2.(negative control)
Tube No3.(normal control)
sucrose solution 0.85 ml - 0.85 ml
saline - 0.85 ml -Normal compatible serum 0.05 ml 0.05 ml 0.05
ml
50% patients cells 0.1 ml 0.1 ml -
50% Normal cells - - 0.1 ml
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
28/39
Flowcytometry
Principle:
Various immunoflurescent dyes coated with Ab can beattached to
the Ag present in the cells or particles. As thesample enters the
flow channels and the cells are passedthrough a focused laser beam
one cell at a time. As the cellsor particles intercept the light
source they scatter light andflurochrome are excited to higher
energy state. This energyis released as a photon of light with
specific spectralproperties unique to different fluorochromes.
These lightare captured and converted to electrical signals.
One
unique feature of fluorocytometry is that it measure
thefluoroscent per cell or particle. This contrast with
thespectrophotometry in which the percent abs. andtransmission of
specific wavelength of light for a bulk
volume of sample.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
29/39
FCM
lymphoma Chronic
lymphoid
leukemia
Plasma
celldisorder
s
Acuteleukemi
a
PNH
Mast cell
disease
MDS
CMPD
HEMATOLOGY TESTFORFLOWCYTROMETRY
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
30/39
FLOCYTOMETRY ANALYSIS OF PNH CELLSprinciple:
Patient red cells are stained with a fluorescein labelled
antibodythat is specific for one of several GPI-linked proteins
egCD55,CD59 etc. which are deficence in PNH red cells. Thestained
cells are then analyzed with a flow cytometer.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
31/39
Procedure
Steps for RBCs
1. Three control tubes and three test tubes are taken andlabeled
as T- Negative , T- CD55, TCD59, C-Negative, C-CD55, C-CD59 .
2. The 50 ul of suspension(50ul of whole blood + 500 ul ofPBS)
and 5ul of Ab are mixed in each tube.
3. Incubate in dark for 30 mins
4. Add 1 ml of PBS and then centrifuge for 5 min at 1000
rpm.5. Discard the supernatant.
6. Wash cell again as step 4 and 5.
7. Resuspend the deposit in 500 ul of PBS.
8. Cap the tube and keep at 4oC
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
32/39
Procedure for WBC
1. Four control tubes and four test tubes are taken and labeled
asT- Negative , T- CD55, TCD59, TCD16, C-Negative, C- CD55, C-CD59,
C-CD16.
2. The 50ul of whole blood and 5ul of Ab are mixed in each
tube.
3. Incubate in dark for 30 mins at RT.4. Add 1 ml of FACS lysing
solution and mix in vortex mixture andkeep it for ten mins.
5. Centrifuge for 5 min at 2000 rpm.
6. Discard the supernatant and tip off on the tissue paper.
7. Add 1 ml of PBS and then centrifuge for 5 min at 2000 rpm.8.
Discard the supernatant.
9. Wash the cell again as in step 7 and 8.
10. Resuspend the deposit in 500 ul of PBS.
11. Cap the tube and keep at 4oC .
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
33/39
Above prepared suspension is taken for
flowcytometricanalysis.
Normal Range:
Less than 5% of CD59 cells are considered as normal.
Precaution:
1. PBS is freshly filtered and then be used.
2. Speed of centrifuge should be maintained up to 1200
rpmotherwise high speed breaks the cells.
3. Storage the kit at 2-8 0C
4. Once started , the test must be performed
withoutinterruption.
5. Avoid carry over contamination.
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
34/39
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
35/39
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
36/39
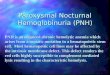
Side Scatter
FSCDetector
CollectionLens
SSCDetector
Laser Beam
Cellgranularity
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
37/39
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
38/39
Treatment
1.Folic acid should be given prophylactically .2. Blood
transfusion:
a) washed red cell
b) saline adenine , glucose, mannitol , preserved blood.
3. Treatment of thrombosis:a)Oral Anticoagulants ( maintain the
INR between 2-3.5)
b)Full Heparinization
c)Fibrinolytic therapy (Tissue type plasmin activator)
4.Bone marrow transplantation
-
7/30/2019 Proxymal Nocturnal Haemoglobinuria (Pnh)
39/39