Embed Size (px)
Citation preview

Fall 2013Volume 84, Number 4
Inside:New Jersey’s Own Maxine Feinberg to Head American Dental Association
Facial Pain of Non-Odontogenic Origin
New Jersey Dental Establishments in 2011: After the Last Recession

The Crowd Pleaser.Nearly one-third of patients with dental benefits are covered by Delta Dental.Over 54 million Americans rely on the dentists in the national Delta Dental system. If you’re already participating in Delta Dental Premier®, why not join another network to have more exposure to newpatients? If you do not participate with Delta Dental, why not join the crowd? We think you’ll be pleased.
Delta Dental. There’s safety in our numbers. To participate with Delta Dental of New Jersey, call 1-888-396-6641 or visit www.deltadentalnj.com.
DDI-1045 NJDA Crowd 7x10_DDI-1045 NJDA Crowd 7x10 9/14/11 12:35 PM Page 1

American Practice Consultants, a full service Dental Practice Broker
& Appraiser, was founded in 1985 by Philip A. Cooper, D.M.D.,
M.B.A. to provide a range of transition services to dentists who are
selling or buying a practice.
Let Us ExpertlyGuide You Through:• VALUATION • MARKETING
• NEGOTIATION • CONTRACT REVIEW
• FINANCING • MINIMIZING TAXES
• TRANSITION PLANNING WITH PATIENTS & STAFF
• AND SO MUCH MORE!
Philip A. Cooper, D.M.D., M.B.A.
Ask About Our
FREE GUIDESFor Sellers & Buyers!
DENTALPRACTICESALESWant to Know More? We Can Guide You.
www.ameriprac.com
704 East Main Street, Suite D • Moorestown, New Jersey 08057856-234-3536 • 800-400-8550 • [email protected]
New Jersey Dental Association and Mid-Atlantic Insurance Resources proudly endorse Meadowbrook Insurance Group for your Workers’ Compensation Insurance needs.
Choosing the right Workers’ Compensation insurance provider makes all the difference. We can assist you with the steps needed to protect you and your employees.
Insurance. Protection. Save. Smile.
For more information about this program, please contact us at:P: 877.476.4588 F: 717.234.4163www.midatlanticir.com
7% workers’ compensation dividend paid in 2011 to NJDA members that met eligibility requirements.
Endorsed Provider of

EditorHarvey S. Nisselson, DDS, FACD, FICD17 Alpine DriveDenville, NJ [email protected]
Managing EditorLorraine [email protected]
Business ManagerArthur Meisel, [email protected]
Publication ManagerMastergraphx
NJDA 2013–2014 OfficersPresident, Robert A. Giantomas, DMDPresident-Elect, Bryon E. Roshong, DMDVice President, Gregory LaMorte, DDSTreasurer, Giorgio DiVincenzo, DMDSecretary, Mark A. Vitale, DMDSpeaker, House of Delegates, Walter I. Chinoy, DMDEditor, Harvey S. Nisselson, DDSImmediate Past President, Michael M. Messana, DMDExecutive Director, Arthur Meisel, Esq.
NJDA 2013–2014 Board Of Trustees Atlantic-Cape May, OPENBergen, Priya Gupta, DDSCentral, Joseph R. Krulewicz, DMDEssex, Thomas A. Rossi, DMDHudson, Luciano A. Ghisalberti, DMDMercer, Fred P. Babinowich, DMDMiddlesex, Mitchell L. Weiner, DMDMonmouth-Ocean, Dipika T. Shah, DDSNJ Student Dental, Meha ShethPassaic, Teresa Michaud, DDSSouthern, Paul J. Lawyer, DMDTri-County, Alan Rothstein, DMDUnion, Barry R. Wolinksy, DDS
Professional StaffPatricia DeCotiis, Esq.Assistant Executive Director/Director of Membership
Mary B. MoskalDirector of Dental Care Programs
James J. Schulz, Jr.Director of Governmental Affairs
Maureen BarlowDirector of Meetings & Events
Stanley OrensteinBusiness Manager
Nicole FredricksonMarketing Communications Manager
The New Jersey Dental Associationis proud to partner with
Mastergraphxto provide the community with a journal printed
on environmentally-friendly paper. By using products with the FSC label you are supporting the growth of responsible forest management worldwide.
Volume 84, Number 4
Member PublicationAmerican Association of Dental EditorsJournal of the New Jersey Dental Association (ISSN 0093-7347, USPS No. 104-650) is published quarterly by the New Jersey Dental Association. Periodical postage paid at North Brunswick, NJ and additional mailing offices. All views expressed herein are published on the authority of the writer under whose name they appear and are not regarded as the views of the Association. We reserve the right to reduce, revise, or reject any manuscript submitted for publication. Copy for publication should be addressed to: Dr. Nisselson. Business communications and address changes should be addressed to: One Dental Plaza, P.O. Box 6020, North Brunswick, NJ 08902-6020, (732-821-9400). Materials may be reproduced without written permission. Subscription rate for members is $20 which is included in the dues; $60 per year for non-members and $100 for foreign subscribers. Single copies are $5 per issue. Periodicals postage paid at New Brunswick, NJ. The Association, in its sole discretion, has the absolute right to accept, reject, and /or cancel any advertisement for any reason whatsoever. POSTMASTER—send address changes to: Journal of the New Jersey Dental Association, One Dental Plaza, PO Box 6020, North Brunswick, NJ 08902-6020.
AdvertisersAFTCO 7American Academy of Facial Esthetics 24American Practice Consultants 1Anesthesia for Dentistry 8B.C. Szerlip Insurance Agency Inc. 38Botwinick & Co. 4The Bronx County Dental Society 18The Clemens Group 31Delta Dental Plan of New Jersey, Inc. IFCDental Dreams 17The Dentists Insurance Company OBCEastern Dental Society IBCEastern Dentists Insurance Company 5Great Expressions™ Dental Centers 20The Insurance Agency for Dentists, LLC 32Meadowbrook® Insurance Group 2Mid-Atlantic® Insurance Resources 35NJ School of Dental Assisting 23Paragon Dental Practice Transitions 39PNC Bank 19RMN Consultants 13Rutgers School of Dental Medicine 40The Snyder Group 15Temple University® Kornberg School of Dentistry 37Mastergraphx 11Valley Forge Dental Conference 33
CoverDelaware Water Gap National Recreation Area
“The New Jersey Dental Association serves and supports its members and fosters the advancement of quality, ethical oral healthcare for the public.”
Mission Statement:
Departments4 From Your President6 Reflections6 In Memoriam8 Executive Director’s Desk10 Members in the News20 Oral Pathology Quiz #8124 Oral Pathology Quiz Answers #8137 Classifieds
Articles9 New Jersey’s Own Maxine Feinberg to Head American Dental Association12 3 Major Obstacles to Going Chartless; and How to Get Around Them!14 Effects of Smoking on Implant Failure—A Review16 Facial Pain of Non-Odontogenic Origin22 NJDA Annual Golf Outing Recap23 Opinion: The Economics of Healthcare and its Implication for Dentistry26 Five Things to Know About Bruxism27 Preprocedural Rinsing in the Dental Office: A Consideration for Improved Infection Control Among the Dental Team and Patients32 New Jersey Dental Establishments in 2011: After the Last Recession36 Opinion: New Kid on the Block
3Volume 84, Number 4

From Your President
Robert A. Giantomas, DMD
We all know about our tripartite membership, but there is a fourth part that is often overlooked—the New Jersey Dental Political Action Committee (NJDPAC).
NJDPAC is a committee run by dentists that raises money to support candidates that support our position—not a party, but our profession. This is a call to action; I am writing this because we need you to join. Less than one in three NJDA members belong to NJDPAC. It has been the number one health PAC in the state for five years but our numbers are dropping.
NJDPAC lets us forge relationships with legislators that drive our agenda forward, be it stopping mid-level providers, or advancing the assignment
of benefits law. All legislators are important, regardless of whether you like them personally. NJDPAC affords you the opportunity to avoid partisan politics, and make it all about the politics of your profession.
Campaigns are expensive, and legislators need to communicate a message to get reelected. NJDPAC allows us to demonstrate value to politicians in their time of need. The strength of our PAC distinguishes NJDA as a leader and a friend against the insurers, attorneys, environmentalists, and others who seek to change how dentistry is practiced in New Jersey. It allows us to change our own destiny.
For more information or to join, contact me at [email protected].
Botwinick & Company, LLCCertified Public AccountantsServing NJ Dentists Since 1968
Sherbrooke Office Center II 201 West Passaic St., Rochelle Park, NJ 07662 T (201) 909.0090 F (201) 909.8533 www.botwinick.com
Isn’t it about time YOU had something to smile about?
When it comes to selecting an accounting firm for your practice, why not follow the lead from your peers. Botwinick & Company, LLC has been serving the accounting needs of New Jersey dentists since 1968. With a firm wide concentration in dental practice accounting, practice management, and acquisition consulting, we are the most trusted dental accounting firm in the Metropolitian Area.
What sets us apart from other firms is the partners’ handson approach to your accounting, tax and managementconsulting needs. One on one attention from youraccountant is guaranteed.
We encourage you to set up a complimentary meeting with one of our partners. Let us show you how you should betreated by your most trusted advisor.
Volume 84, Number 44
ENDORSED BY ENDORSED BY
RHODE ISLANDDENTAL ASSOCIATION
ENDORSED BY
NORTH CAROLINADENTAL SOCIETY 1-800-898-3342 • www.edic.com
EASTERN DENTISTS INSURANCE COMPANYMalpractice Insurance | By Dentists, For Dentists®
YOUR COLLEAGUES! EDIC’s Board of Directors iscomprised of dentists and dental educators. We have a network of national expertsand the best defense counsel at your disposal at any given time. We will go to the wallto defend you, your reputation, and stand by your side when you need us the most.At EDIC, we only insure our colleagues which means you and your claim is ourtop priority.
For over 20 years, EDIC has been committed to dentistry and it’s colleagues. As amutual-owned company we give back to our colleagues, our dental societies, andour dental schools. Our 99% customer retention rate proves we are committed to ourdental community indefinitely.
Join the “By Dentists, For Dentists”® company for all your dental malpractice insuranceneeds, and you can be sure EDIC will always stand by your side.
WHEN YOU GET A CLAIM,WHO WILL DEFEND YOU THE BEST?
EDIC BOARD OF DIRECTORS 2013 - 2014
“Power tends to corrupt,” said Lord Acton, the 19th century historian. “Absolute power corrupts absolutely.” This maxim has been vividly illustrated
in psychological studies, notably the 1971 Stanford Prison Experiment, which was halted when one group of students arbitrarily assigned as “prison guards” over another group began to abuse their wards.
But new scholarship is bringing fresh subtlety to psychologists’ understanding of when power leads people to take ethical shortcuts —and when it doesn’t. Indeed, for some people, power seems to bring out their best. After all, good people do win elective office, says Katherine DeCelles, a professor of management at the University of Toronto, and no few business executives want to do good while doing well. “When you give good people power,” DeCelles says she wondered, are they more able than others “to enact that moral identity, to do what’s right?”
In a study recently published in the Journal of Applied Psychology, DeCelles and her co-authors found that the answer is yes. People’s sense of “moral identity”—the degree to which they thought it was important to their sense of self to be “caring,” “compassionate,” “fair,” “generous” and so on—shaped their responses to feelings of power.
DeCelles and her colleagues developed moral identity scores for two groups, 173 working adults and 102 undergraduates, by asking the participants to rate how important those ethically-related attributes were to them. The researchers had some participants write an essay recalling an incident in which they felt powerful, while others wrote about an ordinary day. Then the participants took part in lab experiments to probe how they balanced self-interest against the common good.
The undergraduates were told they shared a pool of 500 points with other people, and they could take between zero and ten points for themselves. The more points they took, the better their odds of winning a $100 lottery. But if they took too many—there was no way of knowing what that tipping point was—the pot would empty and the lottery would be called off.
The participants who had just written about an ordinary day each took roughly 6.5 points, regardless of their moral identity score. But among those who had been primed to think of themselves as powerful, the people with low moral identity scores grabbed 7.5 points—and those with high moral identity scores took only about 5.5.
In surveys, the last group showed a greater understanding of how their actions would affect other people, which is the crucial mechanism, DeCelles says. Power led them to take a broader, more communally centered perspective.
The experiment involving the adults found a similar relationship between moral identity, ethical behavior and innate aggressiveness. Assertive people who scored low on the moral identity score were more likely to say they’d cheated their employer in the past week than more passive types with similar moral identity scores. But among those with high moral identity scores, the assertive people were less likely to have cheated.
In sum, the study found power doesn’t corrupt; it heightens pre-existing ethical tendencies. Which brings to mind another maxim, from Abraham Lincoln: “Nearly all men can stand adversity, but if you want to test a man’s character, give him power.”
Reflections
PowerHarvey S. Nisselson, DDS, FACD, FICD
InMemoriamMonmouth-Ocean
Gerald S. Gildenberg September 15, 2013Lloyd L. Vaccarelli August 14, 2013
SouthernNorman F. Sengin August 24, 2013
We note with sadness the passing of the following members:
Volume 84, Number 46

Call 1-800-232-3826 today for afree practice appraisal,
a $2,500 value!
AFTCO is the oldest and largest dental practice transition
consulting firm in the United States. AFTCO assists dentists
with associateships, purchasing and selling of practices, and
retirement plans. We are there to serve you through all
stages of your career.
Helping dentists buy & sell practices for over 40 years.
WWW.AFTCO.NET
Paul M. Goodman, D.M.D., Jeffrey M. Goodman, D.M.D., &
David H. Goodman, D.D.S. have acquired the practice of
Richard M. Friedman, D.D.S. - Lawrenceville, New Jersey
Richard Goldberg, D.M.D. has acquired the practice from the estate of
Michael I. Verona, D.D.S. - Monroe Township, New Jersey
Madalina-Elena Iorgulescu, D.M.D. has acquired the practice of
Jane Giordano, D.M.D. - Morristown, New Jersey
AFTCO is pleased to have representedall parties in these transactions.

I f you receive a complaint from the New Jersey State Board of Dentistry, don’t panic. Typically, between five hundred and eight hundred complaints are received by the State Board
each year.
Under the review procedure established by the State Board, most complaints from patients are forwarded to the affected dentists together with a request to produce records and to submit a responsive narrative statement. While the correspondence has the appearance of being personally written,
actually it is a form letter. In some instances, the State Board will initiate an “investigative inquiry,” which is analogous to a deposition.
Upon receiving either a complaint or a notice of an investigative inquiry, NJDA members are encouraged to contact the Association. As a service to members only, at no charge, lawyers with State Board experience will assist members in assessing the seriousness of the complaint and in fashioning a written response.
The tone, content and length of a responsive narrative statement are always important. Depending upon how a narrative statement is written, it can create unnecessary problems or it can hasten a favorable outcome. In more serious matters, where it appears that individual representation is necessary, like when a dentist is summoned for an investigative inquiry or when a formal suspension or revocation proceeding is initiated, lawyers who have experience in appearing before the State Board and who are viewed as being knowledgeable and effective will be recommended.
Among other responsibilities, the State Board has the obligation to protect the public. While at one time the State Board had the reputation of being particularly antagonistic to dentists, that generally is no longer the case. In fulfilling its important public responsibility, the members of the State Board do try to do the right thing in a fair-minded manner without being punitive.
The overwhelming majority of complaints made by patients to the State Board are predicated on disputes over money. When such disputes arise, members are encouraged to promptly contact the NJDA. In many instances, resolutions can be achieved and complaints can be avoided. Patients who feel that they have been treated fairly usually do not file complaints.
The NJDA stands ready and anxious to assist its members by making available legal consultation at a critical time in their professional lives. This is a truly valuable benefit that should not be overlooked or forgotten.
Executive Director’s Desk
Arthur Meisel, Esq.
Anesthesia for DentistryAdministered in your office
There is no fee to become a participating dentist
Glen Atlas, M.D.Board Certified Anesthesiologist
Phone: 973-758-0758Call for availability
www.glenatlasmd.com
Project5_Layout 1 11/13/09 12:44 PM Page 1
Volume 84, Number 48

A t the American Dental Association’s House of Delegates meeting on November 4 in New Orleans, Maxine Feinberg, DDS, was elected president-elect of the American Dental
Association. She will begin her one-year term as president in October, 2014, succeeding Dr. Charles Norman, when the ADA house reconvenes in San Antonio, TX.
Dr. Feinberg, a periodontist, practices in Cranford. A strong proponent of organized dentistry, she has been an ADA member for 32 years. During that time, Dr. Feinberg served locally, at the state level and nationally. She is a member of the Union County Dental Society and is a past president and current member of the New Jersey State Board of Dentistry.
Dr. Feinberg is the first woman to hold the office of president of the NJDA (2002–2003), where she also was treasurer and chair of the Finance Committee. During her term in office at NJDA, Dr. Feinberg is credited with bringing the Give Kids a Smile campaign to the state.
Keeping the Dentist in DentistryIn her message to the delegates of the ADA, Maxine Feinberg noted that her goal would be to “keep the dentist in dentistry.” In her comments, she emphasized three critical issues facing the profession: an uncertain economic future, a volatile regulatory environment, and evolving dental education. As ADA president, Dr. Feinberg plans to expand the ADA’s role in public education and advocacy, noting “We must help states understand the Affordable Care Act while increasing efforts to educate employers and patients on the benefits of good oral health.”
In an interview she gave to the Journal of NJDA in 2002 when she became NJDA president, Dr. Feinberg said, “…because there were few women practitioners, especially specialists, when I started in private practice, it allowed me the freedom to define my own success.” She did say she had great role models, both men and women, whose own commitment to the profession and dedication to organized dentistry fueled her early involvement. She went on to say, “I hope that I can bring about the same feelings in the young practitioners I will meet in the years to come,” an expectation she echoes today at the national level. In her statement to the ADA delegates she said, “My involvement today is to ensure the next generation will be able to afford to go to dental school and continue our proud tradition of improving lives.” From 2011–2013, Dr. Feinberg was the ADA Trustee Liaison to the Task Force on Student Debt and chaired the task force in 2012–2013.
Dr. Feinberg was ADA 4th District trustee at the time of the election. The 4th district is comprised of New Jersey, and Delaware, the District of Columbia, Federal Dental Services, Maryland, Puerto Rico and the Virgin Islands. As an ADA trustee since 2009, Dr. Feinberg served on numerous committees and chaired the Audit Committee in 2012–13. She also has been a delegate to the FDI World Dental Federation since 2009.
Dr. Feinberg is especially committed to strengthening the dentist “as the head of the dental team in all practice models.” After the election results were announced Dr. Feinberg pledged to “move this Association forward as we want to move it, not as others want to.”
A 1980 graduate of New York University College of Dentistry, Dr. Feinberg is a fellow in the American College of Dentists (2000), the International College of Dentists (2002) and the Pierre Fauchard Society (1998). She also maintains memberships in the American Academy of Periodontology and the Academy of General Dentistry. In addition to serving on the NJ State Board of Dentistry, Dr. Feinberg has been a member of the NJ State Dental Medicaid Advisory Committee since 2004, and a member of the North East Regional Board of Dental Examiners. She has been a volunteer with Donated Dental Services since 1998 and was presented with the NJDA Give Kids a Smile Pioneer award in 2012.
Dr. Feinberg is married to John Wynne. They have two daughters, Haley and Rebecca. The family resides in Westfield, NJ.
New Jersey’s Own Feinberg to Head American Dental Association
Former NJDA President andADA 4th District Trustee
9Volume 84, Number 4

Welcome to the 2013–2014 NJDA Component Society Presidents:Boris Kalika, DMD, Atlantic-Cape MayIlya Lipkin, DDS, Bergen CountyMichelle Weddle, DDS, CentralCarol E. Mann, DMD, Essex CountyP. David Gleaner, DMD, Hudson CountyJanhavi S. Rane, DDS, Mercer CountyDavid M. Stein, DMD, Middlesex CountyMiriam T. Furlong, DMD, Monmouth-OceanLeslie Elfenbein, DMD, PassaicFrank R. Batastini, DMD, SouthernEdward M. Tirpack, DMD, Tri-CountyJay L. Greenfield, DMD, UnionMeha Sheth, New Jersey Student Dental
Montclair Orthodontist Edward Gold, DDS, has merged his passion for running with his passion for reading. In 2012, Dr. Gold was ready to run in the New York City marathon for the first time. Unfortunately, Hurricane Sandy put a damper on that effort, but not before he received pledges of nearly $10,000 in
support of the Montclair Public Library. Dr. Gold did make good on his promise, running instead in the Philadelphia marathon on November 18, 2012. This year, proceeds will go to the library’s children’s programs. Dr. Gold explained, “I knew that if I were ever to run a marathon, that I would want to and needed to support a cause...The Montclair Public Library, along with all public libraries can assist in laying the foundation for learning for children that will help our generation and future generations make contributions in all areas of science and humanities…” He noted that the large sum of money raised was realized in increments of “26.2” pennies, dimes and dollars, contributed by Montclair’s children and their parents. When not working, running or reading, Dr. Gold represents the specialty of orthodontics on the NJDA Peer Review Committee.
Give Kids a Smile! Save the Date.Friday, February 7, 2014 is Give Kids a Smile Day! Have you or your office signed up? It’s not too late! February is National Children’s Dental Health Month. On February 7 you and
your staff can make a big difference in a child’s life by accepting patients ages 12 and younger for free screenings, sealants and/or restorative treatment. Register at http://www.ada.org/givekidsasmile.aspx or call the NJDA at 732-821-9400 for information. If you’d like, you can opt to volunteer at another location, such as one of the state’s hygiene schools or another facility. If you are unable to participate but would like to help, please consider making a monetary donation to GKAS-NJ. Donations to GKAS-NJ will be used to offset the cost of student transportation or to provide restorative materials and disposables to locations as needed. Call the number above or email: [email protected].
Irving Horowitz, DMD, an NJDA member practicing in Rocky Hill since 1979, was recently honored with the NYU Faculty of the Year award. A Rutgers College undergrad and Tufts Dental alum, Dr. Horowitz received a certificate in Periodontics from the University of California. He has
been an assistant professor at both the University of Illinois and the University of Pennsylvania dental programs. Currently, Dr. Horowitz is an assistant professor of periodontology and implantology in the NYU residency program, where he has taught for 13 years.
The Southern Dental Society of NJ gathered on April 17th to celebrate the career of long-time business manager, Elaine O’Brien. Elaine began working for the Southern in 1977 and has worked hand in hand with 37 presidents, facilitating the work of the dental society. Over 75 people gathered to honor her many years of dedicated service; among them twenty former Southern presidents. Elaine received many good wishes along with a diamond initial pendant and a framed photograph of her with the former presidents. She will be missed. Elaine is seen in the first row on the right.
Future Members in the NewsThe 91 members of the Rutgers School of Dental Medicine’s (RSDM) inaugural class—the Class of 2017—were welcomed into dentistry and pledged to uphold the integrity of the profession at the 2013 White Coat ceremony. Joining them were 25 students from RSDM’s Internationally Trained Dentist (ITD) program and members of the Class of 2015. The ITD program is for qualified dentists educated outside of the US or Canada, who become part of the third-year class after completing a rigorous three-month program. The ceremony was held on August 28 on the Newark campus of the Rutgers Biomedical Health Sciences unit, part of Rutgers, The State University of New Jersey.
After being cloaked by the presidents of each of the RSDM current classes, the students signed the Rutgers School of Dental Medicine Code of Professional Conduct and Ethics. The ceremony ended with the recitation of the dental oath, led by Dr. Robert Giantomas, president of the New Jersey Dental Association.
Members In The News
Volume 84, Number 410

Members In The News
Photo of Chanan Lerer. (Photo credit: Nick Romanenko)
The first White Coat ceremony took place at Columbia University College of Physicians and Surgeons in 1993. Since then it has become a
tradition at medical and dental schools around the world. The School of Dental Medicine held its first ceremony in 2005. It was one of the first dental schools in the country to do so.
To Contact the NJDA JOURNALTell us about honors and awards that you have received, special things that you wish to share with your colleagues in a Journal article and traditional letters to the editor. Your Journal wants to hear from and about you. Journal of NJDA welcomes submissions of photographs or artwork for consideration as cover art. Submissions should have a vertical orientation and be sent in JPEG, EPS or TIFF format with a minimum resolution of 300 DPI at full size (8.5 x 11). Please include the title, your name and location/date of photo. The Journal reserves the right to reject any submission and to crop images as necessary. The JNJDA also invites members to submit lifestyle and feature stories, in addition to clinical articles. Send inquiries to: Lorraine Sedor, managing editor, at [email protected] or phone 732-821-9400. Harvey S. Nisselson, DDS, Editor.
45 Stouts Lane | P.O. Box 567 | Monmouth Junction, NJ 08852732.329.0088800.675.9819
Mastergraphx Printing
Your one stop source for:
• offset printing
• digital printing
• posters
• banners
• color copies
• pad printing
• graphic design
• CD/DVD duplication
11Volume 84, Number 4

Well, it’s no secret. Chartless dentistry is coming, fast and furious! It’s not a requirement in dentistry yet (unless 30% of your practice is treating Medicaid or Medicare patients),
but at some time in the future, it’s going to be. Let’s look at your practice. Have you started the process of eliminating paper from your chart yet? If not, it is highly recommended to begin. For eliminating a chart in an existing practice with hundreds and even thousands of charts, the process is best done over a longer period of time. Most of the chartless practices today are new ones, that have been built from the ground-up to practice electronically. As for the 25-year old practice that has been pulling, stuffing, and filing charts since its inception, it’s going to take some time, and certainly lots of planning.
This is not going to be a “how-to” article on how to go chartless. There are just too many variables. A strategy should be developed with someone that has the proper expertise, like a dental technology integrator, software trainer, or a practice management consultant. As for any financial investment that would need to be made, there are only three “main ingredients”: an adequate practice management system, a digital X-ray system, and a computer in the operatories. Most practices today have all three of these already, making the transition fairly painless in terms of a monetary investment.
This article, however, is about the obstacles that the typical doctor has created for himself, in his efforts to move forward, or at least begin the process. But here is a secret...most dentists don’t even realize that they have already started the process. There are quite a few technologies that have already been adopted into the practice that have set the ball rolling, eliminating pieces of the paper chart and turning them into bits and bytes and ones and zeros. Take for instance, electronic claims. There was a time when we used to manually fill out a dental claim form, and then make a copy for the chart. Then there is the innovation of digital x-ray technology. Almost 75% of practices have already eliminated x-ray film mounts from their charts. So let’s keep it going.
As a dental IT consultant, my daily conversations with clients and prospects will always lead to a discussion about going chartless. At this point in the evolution of dental technology it certainly should be a goal of your practice. If it’s not, you will do one of two things after reading this article. You will either call your IT support professional and start turning the wheels (even at a slow pace), moving your practice more and more towards “chartlessness.” Or, you will create one of the three most popular obstacles for yourself in order to not move forward; stopping the movement towards eliminating a chart in your practice entirely.
These three obstacles are real, and I hear at least one of them in any given day. Chances are that you are using one, two, or all three of these reasons to keep your practice from moving forward. These are
obstacles that you probably have not received good answers to, or you never asked yourself the question. So, let’s address them now, very simply and adequately.
Obstacle 1: Nervous about losing data or patient records to a crash!
This is a very real concern. Every healthcare provider with a computer should take this one very seriously. In the industry, we call this a data breach. And data breaches in the healthcare community are now subject to huge fines and serious consequences for losing someone’s patient record; but that’s a different article, for a later date. Getting past this obstacle though, is very easy. BACK IT UP!
Please take the time out of your busy practice to meet with a skilled computer professional to design an adequate, full-proof backup strategy. Your strategy should include at least two backup systems, with at least one of them having an offsite option. Also, as a chartless office, it is not only recommended to have a regular backup system, but you should really make the investment in a Backup/Disaster Recovery (BDR) system. A BDR will not only backup your data, but it will include technology that allows you to deploy a backup server if ever needed. As long as you take this strategy very seriously, and do the research to learn what your technology support company actually recommends and supports, you may never have to worry about this obstacle again.
Here are two very important hints for success to make note of: First, test your backup system, including manually restoring data on a monthly basis. Second, have the backup system monitored. Most IT firms offer backup and server monitoring these days.
Obstacle 2: Doctor’s or staff ’s computer skills are not adequate.
This is tough one, even tougher than data security. There is a real human element to this obstacle, which may lead to some tough
3 Major Obstacles to Going Chartless; and How to Get Around Them!
Jeffrey Weiss
Volume 84, Number 412

decisions about the practice’s personnel. Computer skills are skills that are pretty much a standard necessity these days, not only in dentistry and healthcare, but in any profession. Computers are here and are not going away. If anything, they are becoming more involved in our lives. I hear of this obstacle pretty often, and it’s not just from the older generation of doctors. We have seen some young doctors who admit that they have very weak computer skills.
Make no mistake about it, if you’re going to have a chartless office, you are going to either need very good computer skills yourself, or have staff with very strong computer skills. I have seen many offices get by with a doctor that did not have the skills to work the computer in the operatory himself. The routine with his assistant had to be redefined and adjusted to compensate for the doctor’s lacking these skills.
Here are two very important hints for success to make note of:First, get training…and second, get MORE training. Training has been such an important factor in successfully transitioning to chartless dentistry. If you think you know everything that your charting program can do, wait until you realize what it can do that you aren’t even aware of! Furthermore, there are many customizable features in your software that HAVE to be set up and personalized for you before you even begin.
Obstacle 3: The computers or computer network are slow, unreliable or not stable.
This one is certainly a deal breaker. If your computers or computer network are not running smoothly and efficiently, then going chartless is going to be the most frustrating event of your career. Think about how frustrating it will be for you, your staff, and your patients if the digital x-ray system does not fire during an x-ray, or worse yet, the internet has not been working all week so the office manager has not been able to send out electronic claims. These events can not only be annoying, but costly as well, resulting in lost patients or business.
The computers in your office need the same attention, importance, and relevance to your practice that your other dental equipment has. Your dental chairs, your compressor, your handpieces, and the x-ray generators, must all be in tip-top shape to have your operations running smoothly.
So, why not maintain your computers? Computers are machines; and machines need service on a regular basis in order to not break down and to keep running smoothly.
To overcome this obstacle it might be time to get some professional advice from a qualified IT service firm. Many practices do not have a trusted service firm for their computer networks, but instead have a part-time, go-to person who is a patient or a friend. We even come across the ‘Do-It-Yourself ’ computer technician/dentist at times.
For a chartless dental office, here are a few reasons to engage a full-time, IT professional to maintain your office from here on out:• Reliable response time when a question or issue arises. A typical
response time should be under one hour.• Regular maintenance and updates, as recommended by
the software and hardware manufacturers. It is proven that computers run better and smoother when manufacturer updates, patches, and firmware are installed.
• Monitoring services, in order to be proactive in catching issues with hardware as early as possible. Most issues that develop in a computer or server, if caught early enough, will not result in a crash or freeze-up.
• Help Desk support available during regular hours and the proper off-hours protocols.
• A professional who is aware of and familiar with HIPAA laws, Hi Tech Act, and now the final Omnibus Rule for healthcare.
So, those are the three most common obstacles that dentists create in keeping their practices from moving forward with “chartless dentistry.” I’m sure there are others, however, this would be a good time to schedule a consultation with your IT support firm or software vendor to see where your practice is at with your charts. Then, take that knowledge one step further by putting a plan in place to slowly start eliminating the paper inside of it. So when being chartless is required, you will be there already.
About the AuthorJeffrey Weiss is President and partner of High Tech Innovations, LLC, the largest dental integrator in the tri-state area; currently supporting 500+ dental practices. High Tech Innovations prides itself on not only knowing IT and technology, but also understanding the field of dentistry. They are certified as installers by most of the largest dental technology companies in the profession and have recently become an Endorsed Partner of the New Jersey Dental Association. Weiss can be contacted at (973)889-0030 or at [email protected].
13Volume 84, Number 4
IntroductionImplant therapy is highly predictable and successful. However, certain risk factors can predispose individuals to lower rates of success. Cigarette smoking has long been known to be associated with a variety of oral conditions including periodontal disease, bone loss, tissue loss, tooth loss, edentulism, peri-implantitis and dental implant failure. Nicotine in tobacco has been shown to reduce the blood flow in the mouth. Pipe smoking can be worse than cigarettes due to the higher temperatures generated in the upper jaw. Not only is smoking detrimental to implants, it is also bad for conventional bridgework. Smoking affects healing and tissue health in many ways, including impaired neutrophils, altered blood flow to tissues and diminshed oxygen perfusion.
Oral Conditions:1. Periodontal Disease—Periodontitis is an inflammatory
condition of the periodontium in response to bacterial pathogens that promote the release of numerous cytokines and leads to periodontal attachment and bone loss. Twenty years of research show that cigarette smoking is probably a true risk factor for periodontitis. A smoker is 2 to 3 times as likely to develop clinically detectable periodontitis. In addition to increased prevalence, smokers also experience more severe periodontal disease. It appears that a history of treated periodontitis does not adversely affect implant outcome.3,5,10,11
2. Bone and Tissue loss—A study examining the effect of oral burn syndrome on dental implants indicated that there is a direct link between oral tissue loss and smoking.1 In addition, smoking had a significant impact on bone loss.7 The most significant differences regarding implant survival between smokers and nonsmokers were found in studies that identified and evaluated implants placed in the maxilla and those placed in grafted sites. It appears that smoking is a significant risk factor with an adverse effect on implant survival and success in areas of loose trabecular bone.11
3. Tooth loss and Edentulism—Tooth loss and edentulism are more common in smokers than in nonsmokers.4 Tooth loss in older adults occurs because of increased exposure to pathogenic bacteria. Smoking also predisposes patients to develop more severe periodontal disease.2,6
4. Peri-Implantitis—The formation of deep mucosal pockets with inflammation of the peri-implant mucosa around dental implants is called peri-implantitis. Smokers treated with dental implants have a greater risk of developing peri-implantitis. This condition can lead to increased resorption of peri-implant bone. If left untreated, peri-implantitis can lead to implant failure. In a retrospective study conducted at the University of Vienna, the peri-implant tissue of smokers and nonsmokers was compared. The smokers showed a higher score in bleeding index with greater peri-implant pocket depth and radiographically discernible bone resorption around the implant, particularly in the maxilla.8 Implant surface characteristics can influence bone-implant contact and may improve implant outcomes. HA-coated implants can improve the survival or success of implants in smokers compared with nonsmokers.11
Smoke Cessation Former smokers have a lower risk for periodontitis than current smokers. Smoking cessation will result in improved periodontal health and improve a patient’s chance for successful implant osseointegration.4,9
Conclusion The review of this literature demonstrated that smoking has an adverse affect on implant survival and success. Implant success rates tend to be lower than survival rates and vary greatly depending on the criteria used to measure success. Despite these high implant survival and success rates, there is a general appreciation that risk factors predispose individuals to more complications and implant
Effects of Smoking on Implant Failure— A Review
Haritha Mikkilineni, MDSDeepika M. Reddy, DDSNarendra Jayanth, BDS
Volume 84, Number 414
failures, and may result in lower implant survival and success rates. The effect of smoking on implant survival appeared to be more pronounced in areas of loose trabecular bone. A history of treated periodontitis does not appear to adversely affect implant survival rates but it may have a negative influence on implant success rates, particularly over longer periods. Whichever course of treatment patients decide to pursue, they can expect slower healing and a greater possibility of failure if they continue to smoke during or following the treatment healing period. If patients stop smoking three to four weeks prior to implant placement and remain smoke-free during the healing period, results may improve. Many of our smoking patients have used implant treatment as an opportunity to quit smoking altogether. The dentists can prescribe smoke cessation medications and products to assist in the quitting process.
References1. The oral burn syndrome and its effects on dental implants . R.Cullen. J
Oral Implantol 1998;24(4):219–21.
2. Periodontal diseases and dental implants in older adults. Wilson,Higginbottom. J Esthet Dent 1998;10(5):265:71.
3. Surgical determinants of clinical success of osseointegrated oral implants: a review of the literature. Sennerby, Roos. Int J. Prosthodont 1998 sept–oct; 11(5):408–20.
4. Cigarette smoking and periodontal diseases: etiology and management of disease. Tonetti. Ann periodontal 1998 Jul;3(1):88–101.
5. Biological factors contributing to failures of osseointegrated oral implants. (II) Etiopathogenesis. Esposito, Hirsch, Lekholm. Thomsen. Eur J Oral sci 1998 Jun;106(3):721–64.
6. Influences of smoking on the periodontium and dental implants. Dent Update 1997 oct;24(8)328–30.
7. A prospective 15 year follow up study of mandibular fixed prostheses supported by osseointegrated implants. Clinical results and marginal bone loss. Clin Oral Implants Res 1996 Dec;7(4):329–36.
8. The relationship of smoking on peri implant tissue: a retrospective syudy. Haas R; Haimbock W; Mailath G; Watzek G. J Prosthet Dent 1996 Dec;76(6):592–6.
9. Smoking and implant failure—benefits of a smoking cessation protocol. Int J Oral Mxillofac Implants 1996 Nov–Dec; 11(6):756–9.
10. The effect of smoking on early implant failure. DeBruyn, Collaert. Clin Oral Implants Res 1994 Dec;5(4):260–4.
11. INT J Oral Maxillofac Implants 2007;22(suppl):173–202.
About the AuthorsHaritha Mikkilineni, MDS, is a prosthodontist in Hyderabad, India. Deepika M. Reddy, DDS, is a member of the NJDA and an associate dentist at Signature Smiles in Atlantic City, New Jersey. Narendra Jayanth, BDS, is a general dentist in Anantapur, India.
Personalizedfor YourIndividual Needs…Buying or selling a dental practice is one of the most
important business decisions you will ever make.
That’s why Professional Practice Transitions (PPT)
is the best choice to make when you are trying to find
opportunities that match your needs and goals.
With PPT, you are ensured that your life-long
dedication to building and sustaining a successful
business will be respected and leveraged to bring
the results you look forward to.
Call 1-800-988-5674 today to learn more aboutimproving your opportunities for success.
Professional Practice Transitions—we’ll get you there
www.henryschein.com/pptwww.snydergroup.net
12PT6814_PPT_3.5x10bw 10/31/12 3:55 PM Page 3
15Volume 84, Number 4
Dentists encounter patients with facial pain every day in their practices. The most common source of any facial pain involves that of an odontogenic origin. This would include:
• Teeth: caries, periapical pathology, root hypersensitivity,
fractured roots and tooth structure, failed restorations, periodontal, non-carious lesions, occlusal traumatism
• Oral Mucosal Lesions: aphthous, lichen planus, vitral, trauma, mucous membrane disease
• Burning Mouth Syndrome: hormonal influence, medications, xerostomia
When the dentist or endodontist definitively rules out an odontogenic source of facial pain, it is prudent to eliminate all other possible considerations. Too often a TMJ/TMD origin is considered without thoroughly investigating other possible non-odontogenic sources of facial pain.
Facial Pain of Non-odontogenic Source:Myogenous: Muscle spasm or edema; ligamentous or tendinous strain Cervicogenic: Upper cervical spine misalignment involving Atlas bone
Neural and Vascular Compression—Cervico-Trigeminal nerve convergence pain into face
Neurogenous: Associated with Trigeminal, facial & sympathetic nervous system dysregulations—Neurological (conditions of the brain), Multiple sclerosis
Vascular/Glandular: Temporal arteritis, Vascular compression, Glandular disease (Parotid and Submaxillary) Arthrogenous (Structural Displacement TMJ): TMJ with disc displacement, Condylar bone changes
Neoplastic (Obstructive): NeoplasmReferred Source: Otologic, Paranasal Sinuses, Cardiac
We can consider a TMJ source if the patient presents with:• Temporal and frontal headaches• Preauricular and masseteric region pain• TMJ clicking and popping• Ear ringing and clogging• Sensitive teeth.
It is often thought that patients develop facial pain from bruxism. However, grinding of the teeth can be a manifestation of an existing structural problem. It may also develop from sources other than a TMJ dysfunction.
The upper cervical spine is very typically misaligned in patients that have a TMJ dysfunction. Often the same trauma that causes a TMJ disc displacement can cause atlas misalignment. Atlas misalignment contributes to subluxation and compression of the upper cervical
nerves. There is a convergence of the upper cervical nerves and trigeminal nerve in the trigeminal nucleus caudalis. Therefore, facial pain from an upper cervical spine source is very common due to this convergence pattern.
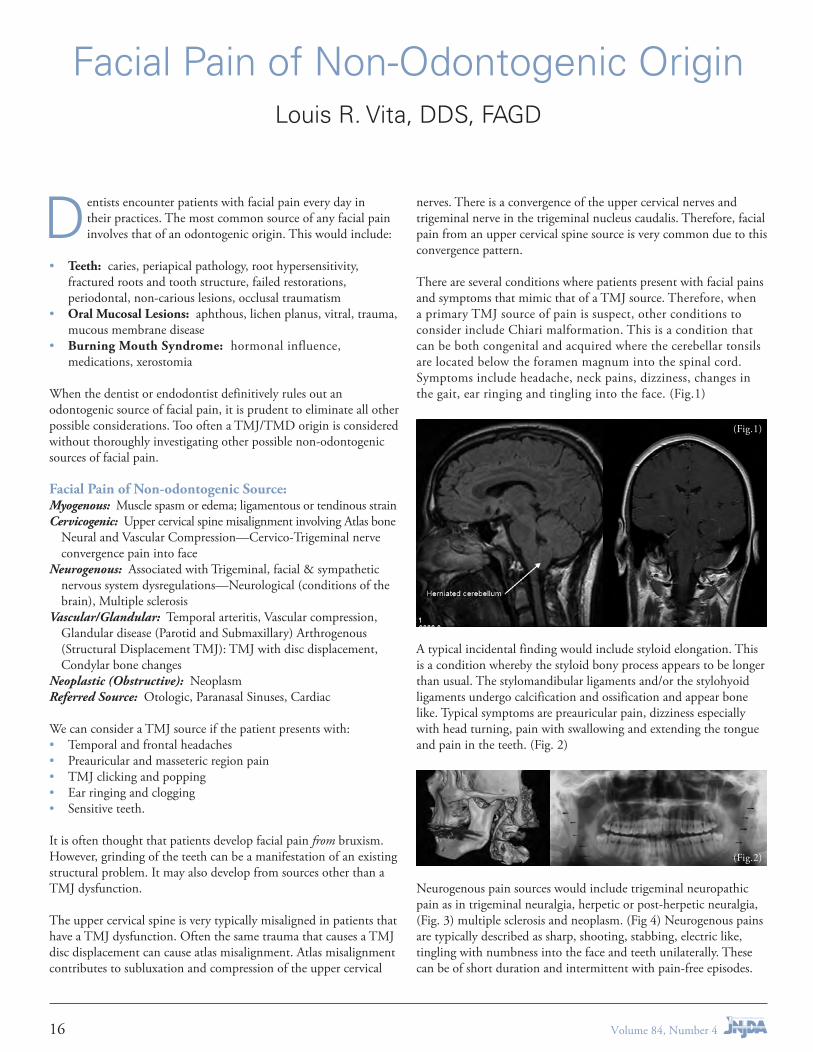
There are several conditions where patients present with facial pains and symptoms that mimic that of a TMJ source. Therefore, when a primary TMJ source of pain is suspect, other conditions to consider include Chiari malformation. This is a condition that can be both congenital and acquired where the cerebellar tonsils are located below the foramen magnum into the spinal cord. Symptoms include headache, neck pains, dizziness, changes in the gait, ear ringing and tingling into the face. (Fig.1)
A typical incidental finding would include styloid elongation. This is a condition whereby the styloid bony process appears to be longer than usual. The stylomandibular ligaments and/or the stylohyoid ligaments undergo calcification and ossification and appear bone like. Typical symptoms are preauricular pain, dizziness especially with head turning, pain with swallowing and extending the tongue and pain in the teeth. (Fig. 2)
Neurogenous pain sources would include trigeminal neuropathic pain as in trigeminal neuralgia, herpetic or post-herpetic neuralgia, (Fig. 3) multiple sclerosis and neoplasm. (Fig 4) Neurogenous pains are typically described as sharp, shooting, stabbing, electric like, tingling with numbness into the face and teeth unilaterally. These can be of short duration and intermittent with pain-free episodes.
Facial Pain of Non-Odontogenic OriginLouis R. Vita, DDS, FAGD
(Fig.1)
(Fig.2)
Volume 84, Number 416

An infectious source can be that of otalgic, mastoid (Fig. 5) or sinus pathology. It is common for sinus disease, ear infections and cardiac conditions to refer pain into the face.
Another common complaint of facial pain involves a dysregulation of the sympathetic nervous system. Commonly thought of as Reflex Sympathetic Dystrophy, this condition is now referred to as Facial Complex Regional Pain Syndrome, i.e., Facial CRPS. When there is a disturbance in the sympathetic nervous system, patients can present with constant burning pain in multiple areas of the head, face and neck. Dental implications of Facial CRPS include hypersensitivity of the teeth especially to cold, pulpal edema and pain even without obvious dental causes as caries or large fillings, painful dental injections from an exaggerated reaction to the stimuli, swelling and pain in the gingiva, cheeks and nasal cavities (congestion). There can be oral and tropic skin changes with tooth discoloration. Facial CRPS would typically contribute to a reduced mandibular range of motion, tremors, dystonia and parafunction as with bruxism and nebulous occlusion in which maximum intercuspation position is not reproducible.
Therefore, when a patient presents with facial pain, the potential odontogenic source must be initially eliminated. Once the health of the oral cavity is determined, all other systems and conditions can be investigated.
References1. Mayo Foundation for Medical Education and Research (MFMER);
1998–2013
2. Zohar et al. 1986, Krennmair et al. 1994 “Symptoms of Styloid Elongation.”
3. Janetta, Peter: Trigeminal Neuralgia, Oxford University Press, Inc. 2011. Diagnostic Criteria for Trigeminal Neuralgia; Table 7.1 Page 75
4. Melis, M et al. Complex Regional Pain Syndrome in the head and neck: a review of the literature. J Orofac Pain 2002 Spring; 16(2): 93–104
About the AuthorLouis Vita, DDS, FAGD, has a general, family practice in Clifton, NJ. He established and directs the Vita Head, Neck & Facial Pain Relief Center and is a recognized authority on the subject. Dr. Vita serves as an attending dentist and lecturer at Hackensack University Medical Center’s Dental Department where he instructs the residents in dentistry and TMJ disorders.
(Fig.3)
(Fig.4)
(Fig.5)
17Volume 84, Number 4
Big Apple
2014
Dental Meeting
Sponsored byThe Bronx County Dental Society
Wednesday, March 19, 2014 Thursday, March 20, 2014
The sheraTon MahWah. MahWah, neW Jersey• Two full days of education• Morning, afternoon and evening seminars• commercial exhibits• $25/$10 discount coupons for Purchases at the Meeting• Free Parking: Indoors and outdoors• Free Breakfast and Free Buffet Lunch For Full day seminars• exhIBIT hours: 9:30 a.m. to 7:00 p.m.
Continuing eduCation Credits will be giv-en to all attendees. these Credits will be appliCable for dentist and dental hygienist re-quirements as allowed by state law.
★ Special BonuS For ★ attending our SeminarS
A $25 exhibitor’s coupon will be given to each dentist for attend-ing a full-day seminar and a $10 coupon to each dentist attending a half-day or evening seminar. When presenting your $25 or $10 coupon for full day, half day and evening paid seminars — any purchase made at the exhibitor’s booth will be discounted at the $25 or $10 rate. You will receive a coupon for every paid course that you attend and no minimum purchase is required!
28th AnnualBIg aPPLedenTaL MeeTIngsponsored byThe Bronx county dental society
1. MATERIALS AND ESTHETICS Dr. George Bambara Dr. David Clark Dr. Howard Glazer Dr. Richard Trushkowsky Dr. Arthur Volker Dr. Carlos Alfonso
2. ENDODONTICS Dr. Douglas Lambert Dr. Jeffrey Linden
3. PROSTHETICS Dr. Michael DiTolla
4. PRACTICE MANAGEMENT Dr. Matthew Krieger Linda Lakin, RDH, MS Christine Taxin 5. TECHNOLOGy Dr. Paul Feuerstein Dr. Gary Severance
6. INFECTION CONTROL Dr. Harold Edelman
2014 partial list of Speakers
7. RISK MANAGEMENT Dr. Robert Peskin Amy Kulb, Esq.
8. PATHOLOGy Dr. Alvin Heller Olga Ibsen, RDH, MS, FAADH
9. MEDICAL EMERGENCIES Dr. Stanley Malamed
10. OPERATIvE Dr. Joel Berg
11. DENTAL ASSISTING Shannon Pace Brinker, CDA, CDD
12. FINANCE Mr. W. Michael Prendergast
For further information, contact: The Bronx county dental society
718-733-2031 • 718-733-0186 (fax)email: [email protected]: www.bigappledentalmeeting.us
secure online registration
on our website.

Big Apple
2014
Dental Meeting
Sponsored byThe Bronx County Dental Society
Wednesday, March 19, 2014 Thursday, March 20, 2014
The sheraTon MahWah. MahWah, neW Jersey• Two full days of education• Morning, afternoon and evening seminars• commercial exhibits• $25/$10 discount coupons for Purchases at the Meeting• Free Parking: Indoors and outdoors• Free Breakfast and Free Buffet Lunch For Full day seminars• exhIBIT hours: 9:30 a.m. to 7:00 p.m.
Continuing eduCation Credits will be giv-en to all attendees. these Credits will be appliCable for dentist and dental hygienist re-quirements as allowed by state law.
★ Special BonuS For ★ attending our SeminarS
A $25 exhibitor’s coupon will be given to each dentist for attend-ing a full-day seminar and a $10 coupon to each dentist attending a half-day or evening seminar. When presenting your $25 or $10 coupon for full day, half day and evening paid seminars — any purchase made at the exhibitor’s booth will be discounted at the $25 or $10 rate. You will receive a coupon for every paid course that you attend and no minimum purchase is required!
28th AnnualBIg aPPLedenTaL MeeTIngsponsored byThe Bronx county dental society
1. MATERIALS AND ESTHETICS Dr. George Bambara Dr. David Clark Dr. Howard Glazer Dr. Richard Trushkowsky Dr. Arthur Volker Dr. Carlos Alfonso
2. ENDODONTICS Dr. Douglas Lambert Dr. Jeffrey Linden
3. PROSTHETICS Dr. Michael DiTolla
4. PRACTICE MANAGEMENT Dr. Matthew Krieger Linda Lakin, RDH, MS Christine Taxin 5. TECHNOLOGy Dr. Paul Feuerstein Dr. Gary Severance
6. INFECTION CONTROL Dr. Harold Edelman
2014 partial list of Speakers
7. RISK MANAGEMENT Dr. Robert Peskin Amy Kulb, Esq.
8. PATHOLOGy Dr. Alvin Heller Olga Ibsen, RDH, MS, FAADH
9. MEDICAL EMERGENCIES Dr. Stanley Malamed
10. OPERATIvE Dr. Joel Berg
11. DENTAL ASSISTING Shannon Pace Brinker, CDA, CDD
12. FINANCE Mr. W. Michael Prendergast
For further information, contact: The Bronx county dental society
718-733-2031 • 718-733-0186 (fax)email: [email protected]: www.bigappledentalmeeting.us
secure online registration
on our website.

Oral Pathology Quiz #81Presented by Rutgers School of Dental Medicine Biopsy Service
The NJDS oral pathology faculty are showing the clinical presentation of some relatively common lesions for readers to self-evaluate their skills in clinical differential diagnosis. You are expected to choose the most likely clinical diagnosis on the basis of history and clinical or radiographic appearance with the appreciation that definitive diagnosis requires microscopic examination of the specimen.
Case Number 1 Figures 1 and 2: Courtesy Drs. Daynet Fraga and Maano Milles, Rutgers University
A 32-year-old man complained of a painless swelling in his mouth, which he said had been present for about a month. The dome-shaped lesion appeared to arise from the left maxillary ridge, in the area of the premolars that had been extracted 3 months previously. The enlargement was relatively soft in consistency, red, and measured approximately 2 cm by 1.5 cm. Clinical and radiographic examination revealed numerous carious teeth and an edentulous left posterior maxillary ridge. There was a small defect in the floor of the left maxillary sinus at the site of the extracted first premolar. The shadow of the soft tissue enlargement is also visible on the radiograph. Which of the following is the most likely diagnosis?
A. Maxillary sinus pseudocyst
B. Postoperative maxillary cyst
C. Herniated maxillary sinus
D. Epulis granulomatosum
Volume 84, Number 420

Answers on page 24
Case Number 4 Figure 5: Courtesy Dr. Roberta Grill Deutsch, New York, NY
Clinical examination of a healthy 63-year-old African-American male detected a compressible area in the mucobuccal fold adjacent to his left maxillary lateral incisor and canine. The canine was an abutment for a bridge. A periapical radiograph revealed a moderately well-defined, unilocular radiolucency above the apices of the two teeth. It measured approximately one cm in diameter. Root canal therapy had been performed on the canine 2 years earlier, with no change in the size of the radiolucency. The lateral incisor was vital. Which of the following is the most likely diagnosis?
A. Radicular (periapical) cyst
B. Dental (periapical) granuloma
C. Ameloblastoma
D. Globulomaxillary cyst
Case Number 2 Figure 3: Courtesy Dr. Daniel Barabas, Ridgewood
A 27-year-old healthy male presented with a solitary, painless, firm, pink, sessile, smooth-surfaced papule on his lower labial mucosa, immediately to the right of the midline. It was 3 mm in maximum dimension. He reported that he had been aware of the lesion for 10 years, but now wanted it removed and diagnosed as soon as possible because he was leaving the United States. The most likely diagnosis is:
A. Pyogenic granuloma
B. Peripheral giant cell lesion
C. Traumatic neuroma
D. Verruca vulgaris
Case Number 3 Figure 4: Courtesy Dr. Andrew Yampolsky, Rutgers University
A 27-year-old female complained of slight buccal expansion in the left body of her mandible. There was no pain or tenderness. She reported that she had “cyst surgery” and extractions in her left lower jaw some time ago but did not know what the diagnosis had been. The only teeth remaining in her left mandible were the incisors and second molar. A panoramic radiograph revealed a multilocular, radiolucent lesion in the edentulous canine-premolar region of her left mandible. It measured approximately 2.5 cm mesiodistally by 1.5 cm vertically. The honeycomb lesion expanded the superior alveolar border and extended inferiorly two-thirds of the way into the jaw. The patient was otherwise healthy and there were no other significant lesions. Which of the following is the most likely diagnosis?
A. Ameloblastoma B. Residual cyst C. Dentigerous cyst D. Lateral periodontal cyst
21Volume 84, Number 4

NJDA Annual Golf Outing RecapGolf is a game in which you yell ‘fore’, shoot six and write down five.
— Paul Harvey
l–r: Giancarlo Ghisalberti, and Drs. Luciano Ghisalberti, Thomas Rossi and Gregory LaMorte.
l–r: Drew Nagle, Sharon and Dr. Richard Riva, Scott Elias.
O ld York Country Club in Chesterfield was the site of the Association’s annual golf outing in August. Eighteen holes of golf, interspersed with occasional rain drops and bright
sunshine, brought out some of the Association’s best golfers, friends and business associates.
Here are this year’s winners: 1st place net, Cristos Gikas, 72; 2nd place net, Drew Nagle, 72; and, 3rd place net, Giancarlo Ghisalberti, 72. First place gross went to Jimmy Arbef, 71; 2nd place gross, Ross Selby, 77; and 3rd place gross to Dr. Luciano Ghisaberti, 81.
Dr. Ghisalberti’s son, Giancarlo, also won the longest drive, on hole #14. Dr. Ralph Baines won closest to the pin, on
hole #2, missing a hole-in-one by only 4’ 6”. Winners of Dr. Charlie Perle’s Putting Challenge, sponsored by Delta Dental of NJ, were Dr. Rocco DiAntonio and Dr. Paul Kaplan.
The annual event is sponsored by the Association’s partners and other corporate supporters, including: New Providence Financial, Delta Dental, NJCAR, Medical Design Build, The Dental Laboratory Group, CareCredit, PNC Bank, AFTCO, Bank of America, Colgate, The Glove Club, Henry Schein Dental, TD Bank, TDIC, Meadowbrook Insurance, High Tech Innovations, FSI, Kuwata Pan Dent, and Demandforce.
Volume 84, Number 422
Recently a patient of mine, who is a physician, told me he sold his practice to Atlantic Health System. Atlantic Health System owns a number of hospitals and also private, or
formerly private, medical practices. There is a trend for the same companies that own hospitals to acquire private practices. The more hospitals and doctors owned by the company, the stronger the power to negotiate with insurers for higher reimbursement rates. The insurer, in turn, raises premiums to cover any increases and additional profit.
As a believer in quality healthcare, I become concerned when decisions are taken away from doctors and other health professionals, and their patients. While consolidation to a point can lower costs and increase efficiency, the number one goal of any corporation is to increase profits. So I question whether the long-term effect of this arrangement offers any benefit to patients.
In the early days of medical insurance, doctors were happy receiving a guaranteed payment of 80% or more of the now obsolete terminology UCR (usual, customary and reasonable) fees, so they were less concerned about collecting the remaining copayment. Insurance companies realized this and started to set their own prices through PPOs and HMOs.
Initially, dental insurance was a totally different entity. We also had UCR fees, but insurance companies, along with our State Board, ensured that copayments were collected. The true difference was, and still is, the overall economics of dentistry vs. medicine. Dental insurance has a maximum per year, where medical insurance did not. In fact, I would propose that dental insurance shares more similarities to auto insurance, with both deductibles and maximums, than medical insurance. Also, the overall cost of dental care is 100 times less than medical care.
I have been a dentist long enough to have seen the HIV scare resulting in necessary improvements in infection control, OSHA, HIPAA, and the effects of a recession on dentistry. So, in the past where patient’s questions may have been about sterilization of instruments, they are now much more concerned about cost of treatment than any other issue. Since the average dental student graduates these days with about $200,000 of student loan debt, coupled with the substantial cost of buying or opening a practice, I am concerned about my profession’s future.
There has to be a reasonable return on investment for students to want to invest a minimum of 8 years of college and postgraduate education and the associated cost of acquiring a dental practice, or we risk becoming an employee profession of corporate health systems. I do believe the current and primary form of solo dental practice is an endangered species due to cost issues.
About the AuthorJeffrey A. Mermelstein, DMD, is a general practitioner with offices in Livingston. A member of the Essex County Dental Society, Dr. Mermelstein also is a member of the NJDA Council on Annual Session.
Opinion:The Economics of Healthcare and
its Implication for DentistryJeffrey A. Mermelstein, DMD
X-Ray TRaining foR nJ License
NJ School of Dental Assisting has a Sunday only 10 week program which
fulfills state license training requirements. We have small classes with experienced instructors. Classes are available at our
New Brunswick and Forked River locations.
Dental Assistants Available
We have trained assistants looking for employment, please e-mail your job
requirements and graduates will contact you directly. This is a free service.
NJ School of Dental Assistingwww.njdentalassist.com
The dental radiology course for dental assistants is accredited by the New Jersey Radiologic Technology Board of Examiners
23Volume 84, Number 4

Oral Pathology Quiz #81Answers
Case Number 1 C. Herniated maxillary sinus
There is considerable individual variation in the thickness and density of bone between the apices of posterior maxillary teeth and the soft tissue lining of the maxillary sinus. Oro-antral communication is most likely to occur as a consequence of extraction of posterior maxillary teeth when the maxillary sinus floor extends beyond one quarter of the length of the roots of the teeth, or between the roots of adjacent teeth. It has been suggested that a sudden increase in pressure within the sinus, such as post-extraction sneezing, may contribute to this complication. Some small oro-antral communications will heal without the formation of a fistula or chronic sinusitis. Numerous factors may interfere with spontaneous resolution, including the presence or absence of pre-existing infection and quality of post-operative care. It is not clear why herniated maxillary sinus mucosa (C) developed in this case.
A biopsy of the soft tissue mass revealed mucosa that lines the sinus, but is not normally found in the oral cavity. The biopsy specimen also revealed typical oral epithelium overlying inflamed connective tissue. That is consistent with epulis granulomatosum (D), which is also known as post-extraction inflammatory mucosal hyperplasia. Hyperplastic tissue growing in an extraction socket is a relatively common event.
In this case, the entire soft tissue mass was removed and the oro-antral defect was surgically repaired.
Maxillary sinus pseudocyst (A) is a relatively common, asymptomatic, non-expansile lesion that presents radiologically as a smooth, non-corticated, dome-shaped, slightly opaque hemisphere above sinus floor. Postoperative maxillary cyst (B) is also known as surgical ciliated cyst. This rare entity is caused by displacement of part of the sinus epithelial lining, usually during surgery. The implanted epithelium then generates a true, expansile cyst that appears radiologically as a well-defined, spherical, radiolucent lesion, within bone but separate from the maxillary sinus.
The Oral Pathology Quiz is presented by faculty of the Rutgers University —Rutgers School of Dental Medicine, Division of Oral Pathology, Drs. Deborah B. Cleveland, Joseph Rinaggio, and Lawrence C. Schneider. Clinicians who have clinical pictures and/or radiographs of cases suitable for future quizzes should call Dr. Schneider at (973) 972-4375. E-mail: [email protected].
Biopsy kits may be obtained without charge by calling (973) 972-1646. Faculty are available to answer questions Monday through Friday, from 8:00 AM to 4:00 PM.
Answers from page 20
Botox® & Dermal Filler Training for Every Dental Practice
THE BEST LIVE PATIENT TRAINING AVAILABLE
December 13-14 ............................New York (Levels I, II)
January 30 - Febuary 1 ................................. New Jersey
CALL 800.952.0521 : : WWW.FACIALESTHETICS.ORG
[SCAN FOR DETAILS]
Register by December 15th and Save! > SIGN UP NOW AND SAVE UP TO $1000
> AGD & AACD MEMBERS SAVE MORE
> CHECK THE AAFE WEBSITE FOR MORE UPCOMING COURSES
Frontline TMJ, Headache and Facial Pain Therapy for Every Dental Practice
LIVE PATIENT 2-DAY COURSE
December 12-13 ................................................ New York
January 30-31 ................................................ New Jersey
Earn up to 24 CE Credits!
Botox® & Dermal Filler Training for Every Dental Practice
THE BEST LIVE PATIENT TRAINING AVAILABLE
December 13-14 ............................New York (Levels I, II)
January 30 - Febuary 1 ................................. New Jersey
CALL 800.952.0521 : : WWW.FACIALESTHETICS.ORG
[SCAN FOR DETAILS]
Register by December 15th and Save! > SIGN UP NOW AND SAVE UP TO $1000
> AGD & AACD MEMBERS SAVE MORE
> CHECK THE AAFE WEBSITE FOR MORE UPCOMING COURSES
Frontline TMJ, Headache and Facial Pain Therapy for Every Dental Practice
LIVE PATIENT 2-DAY COURSE
December 12-13 ................................................ New York
January 30-31 ................................................ New Jersey
Earn up to 24 CE Credits!
AAFE-DJ-NewJersey-7.5x3.25-2clr.indd 1 9/23/13 1:50 PM
Volume 84, Number 424
Case Number 2 C. Traumatic neuroma
Traumatic (amputation) neuroma (C) is linked to injury. Damage to a peripheral nerve fiber bundle sometimes produces a disorganized proliferation of neural tissue and scar tissue. Clinically, it presents as a normal-colored, firm, smooth-surfaced, well-defined nodule or papule that is attached to surrounding mucosa. These lesions may be tender or even painful.
Pyogenic granuloma (A) is excluded because it is soft and red. Peripheral giant cell lesion (B) is excluded because it occurs only on the gingivae or alveolar ridge. Verruca vulgaris (D) is excluded because it has a papillary surface contour.
The differential diagnosis for a solitary, dome-shaped, normal-colored, firm, well-defined nodule or papule on the oral mucosa includes reactive lesions (irritation fibroma, traumatic neuroma, peripheral ossifying fibroma, peripheral giant cell lesion) and benign neoplasms (pleomorphic adenoma, canalicular adenoma, neurilemoma, solitary neurofibroma, and leiomyoma). Peripheral ossifying fibroma and peripheral giant cell lesion occur only on the gingivae or alveolar ridge.
Case Number 3 A. Ameloblastoma
Ameloblastoma (A) is the most common odontogenic neoplasm. The majority of these benign tumors are the classical, infiltrative, aggressive subtype. Most of such lesions are asymptomatic and are recognized during routine clinical or radiographic examination or because they have caused expansion of the jaw. If untreated, they may eventually cause serious deformity. Although they arise anywhere in the jaws, the posterior mandible is the most common location and the mean age at diagnosis is about 35 years. Radiologically, they appear as well-defined radiolucencies, which are more often multilocular than unilocular. Recurrence rates are lowest when tumors are excised at least one cm beyond their radiographic margins.
Residual cyst (B) is excluded because it almost always presents as a unilocular radiolucency. Dentigerous cyst (C) is excluded because it appears as a unilocular radiolucent lesion enveloping all or part of the crown of an impacted tooth. Lateral periodontal cyst (D) is excluded because it is a unilocular radiolucent lesion. (The botryoid odontogenic cyst is the polycystic and multilocular variant of the lateral periodontal cyst.)
The differential diagnosis of well-defined, multilocular radiolucencies of the jaw also includes other odontogenic tumors (odontogenic myxoma and ameloblastic fibroma), odontogenic cysts (odontogenic keratocyst and calcifying odontogenic cyst), non-odontogenic tumors (solitary central giant lesion, central hemangioma, and central mucoepidermoid carcinoma), brown tumor of hyperparathyroidism, and aneurysmal bone cyst.
Case Number 4 B. Dental (periapical) granuloma
Dental (periapical) granulomas (B) are by far the most common inflammatory periapical lesions that are the consequence of pulp necrosis. They are approximately three times more common than radicular (perapical) cysts (A), although that differential is much less significant in cases that have failed to respond to conservative endodontic measures. Clinically and radiologically the two conditions are inseparable.
Ameloblastoma (C) occasionally presents as a periapical radiolucent lesion but all variants of ameloblastoma combined are much less common than dental granulomas.
Historically, the term “globulomaxillary cyst” (D) was applied to cysts between the roots of maxillary lateral incisors and canines that were believed to be “fissural” in origin. It was assumed that they arose from epithelium trapped in line of fusion between median nasal and maxillary processes. Research revealed that they are odontogenic cysts (radicular, lateral periodontal, calcifying odontogenic or odontogenic keratocysts). Currently, the term indicates the location of a “cystic” radiolucency.
The differential diagnosis of a well-defined periapical unilocular radiolucency includes inflammatory lesions (dental granuloma, radicular cyst, apical abscess, and apical scar), other odontogenic cysts (odontogenic keratocyst and calcifying odontogenic cyst), odontogenic tumors (ameloblastoma) , and Langerhans cell disease (histiocytosis X).
25Volume 84, Number 4

1. Bruxism is a repetitive jaw-muscle activity characterized by clenching or grinding of the teeth
Bruxism has been recently defined by an international consensus as ‘a repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible. Bruxism has two distinct circadian manifestations: it can occur during sleep (indicated as sleep bruxism) or during wakefulness (indicated as awake bruxism).’1
2. Bruxism is a centrally-mediated phenomenon
Systematic literature reviews reported that the etiological role of peripheral (i.e., anatomy of dental occlusion and other morphological features) has been progressively dismantled in favor of central origin theories (i.e., psychological, social, neurobiological factors). Importantly, bruxism must not be considered a disorder per se, so that the etiology and clinical meaning of the different forms (i.e., clenching-type vs. grinding-type; sleep vs. awake bruxism) should be better discriminated.2,3
3. Epidemiology of bruxism is characterized by a decrease with age and no gender differences
In recent systematic reviews, bruxism prevalence in adults was between 8% and 31.4%.4 Bruxism was found to be unrelated to gender, and a decrease with age was common to all of the reviewed studies. Very little information is available on the epidemiology of different bruxism activities.
4. Bruxism might be a threat for dental implant treatments
Conclusions from a systematic review suggest that bruxism may be a risk factor for mechanical complications on implant-supported rehabilitations. However, bruxism is less likely to be a risk factor for biological complications around dental implants.6
5. Management of bruxism requires a multidisciplinary approach as well as occlusal appliances, behavioral and pharmacological therapy
Bruxism should be assessed by a multidisciplinary team that includes dentists, neurologists, sleep-medicine specialists, and psychologists. Bruxism can best be managed by adopting a ‘multiple-P’ approach: Plates (i.e., oral appliances), Pep talk (i.e., counseling), Pills (i.e., pharmacological treatments with centrally-acting drugs), and Psychology (i.e., supporting psychological techniques).7
References1. Lobbezoo F, Ahlberg J, Glaros AG, et al. Bruxism defined
and graded: an international consensus. J Oral Rehabil 2013;40(1):2–4.
2. Lobbezoo F, Ahlberg J, Manfredini D, Winocur E. Are bruxism and the bite causally related? J Oral Rehabil 2012;39(7):489–501.
3. Manfredini D, Lobbezoo F. Role of psychosocial factors in the etiology of bruxism. J Orofac Pain 2009;23(2):153–66.
4. Manfredini D, Winocur E, Guarda-Nardini L, Lobbezoo F. Epidemiology of bruxism in adults: a systematic review of the literature. J Orofac Pain 2013;27(2):99–110.
5. Manfredini D, Restrepo C, Diaz-Serrano K, Winocur E, Lobbezoo F. Prevalence of sleep bruxism in children: a systematic review of the literature. J Oral Rehabil 2013;40(8):631–42.
6. Manfredini D, Poggio CE, Lobbezoo F. Is Bruxism a Risk Factor for Dental Implants? A Systematic Review of the Literature. Clin Implant Dent Relat Res 2012.
7. Lobbezoo F, van der Zaag J, van Selms MK, Hamburger HL, Naeije M. Principles for the management of bruxism. J Oral Rehabil 2008;35(7):509–23.
About the AuthorsDr. Kelvin I. Afrashtehfar is a member of the faculty in the department of Restorative Dentistry, at McGill University in Montreal, Canada. Dr. Daniele Manfredini is a member of the department of Maxillofacial Surgery at the University of Padova in Italy.
Five Things to Know About Bruxism
Kelvin I. Afrashtehfar, DDS, FADIDaniele Manfredini, DDS, PhD
Volume 84, Number 426
IntroductionIn the practice of dentistry, the dentist and the dental team are utilizing ultrasonic and sonic scalers, prophylactic polishing angles, low- and high-speed handpieces, air polishers and air abrasion devices to conduct both preventive and restorative procedures on their patients. When conducting these procedures in the dental operatory, small particles are generated which combine with oral microbes, food debris, saliva and blood in the patient’s mouth, causing an aerosol or splatter to occur outside of the oral cavity in the operatory environment. In this article, the transmission of bacteria, rationale for preprocedural rinsing, research published on the use of antimicrobial agents such as chlorhexidine gluconate, essential oils and cetylpyridinium chloride will be discussed. The importance of preprocedural rinsing in reducing salivary bacterial load and microorganisms in saliva and aerosols generated during dental procedures should be taken into consideration in the dental office.
Transmission of Microorganisms in the Dental OperatoryCurrent infection control procedures in the dental office include the use of face masks, plastic eye shields/loupes, gloves and wearing lab coats over scrubs or professional attire to assist in providing barriers for transmission of microorganisms. When conducting dental procedures, an aerosol can occur. This is a mist of particles that are less than 50 micrometers in diameter and may stay in the operatory air or evaporate into smaller invisible particles. Splatter can also occur, which consists of larger droplets that may be more than 50 micrometers in diameter and can spread to the dental practitioner’s lab coat/uniform, eyewear, mask, skin or operatory surfaces. Aerosol and splatter contain airborne or bloodborne pathogens.1–4 The greatest airborne infection threat in dentistry is from aerosols, due to their ability to stay airborne and their potential to enter respiratory passages.5–7 Microorganisms included in dental aerosols have been associated with respiratory infections, hepatitis, tuberculosis, conjunctivitis, herpes lesions and other skin infections.2,3 The prevalence of Streptococcus and Staphylococcus bacteria in the air after dental surgery has been cited.8,9
The most intensive aerosol and splatter occurs during work with an ultrasonic and power scaler tip, the bur on a high-
speed handpiece and with air polishers.10–14 Another study reported that when ultrasonic scalers are used, even in the absence of coolant water, there is aerosolization of material from the operative site.11,18 Research, utilizing a dye expulsion, has confirmed the potential for retracting oral fluids in the internal compartments of the high-speed handpiece.15–17 In dental aerosols, there are elements of saliva, nasopharyngeal secretions, plaque, blood, tooth components and material used in dental procedures.18–20
Preprocedural Rinsing in DentistryPreprocedural rinsing is defined as using an antimicrobial agent for a period of 30 to 60 seconds as a mouthrinse prior to a dental preventive or restorative procedure. The rationale for incorporating preprocedural rinsing prior to dental and dental hygiene appointments is to decrease salivary bacterial load in the mouth, thereby decreasing bacterial microorganisms incorporated into the dental aerosol or splatter that occurs during these procedures.
Antimicrobial Agents Used in Preprocedural RinsingChlorhexidine Gluconate—Chlorhexidine gluconate (CHX) is a cationic bis-biguanide that has a broad antimicrobial activity against a wide variety of Gram-positive and Gram-negative supragingival and subgingival plaque microorganisms and fungi.21,22 It can reduce plaque, dental caries and gingivitis and binds to sites in the oral cavity and is slowly released over seven hours, restricting bacterial growth.21 CHX will rupture the bacterial cell walls and the loss of the cytoplasm results in cell death.23
In one study, CHX reduced salivary bacterial load by 97% and continued for 60 minutes after scaling and root planning; aerobic bacteria at 30 and 60 minutes were reduced 77% compared to control.24 Eapen cited statistically higher reductions in both aerobic and anaerobic counts for CHX versus cetylpyridinium chloride (CPC) and fluoride and normal saline at 2 minutes, 30 minutes and one hour postrinse, but not statistically significantly different at the 2 minute anaerobic count.25 After a single rinse, salivary bacterial counts remained
Preprocedural Rinsing in the Dental Office: A Consideration for Improved Infection Control Among the Dental
Team and PatientsChristine A. Hovliaras, RDH, BS, MBA, CDE
27Volume 84, Number 4

reduced up to 90 minutes for CPC and 5 hours for CHX.26 In another study, Balbuena et al. studied the efficacy of essential oils (EO) and CHX on salivary counts in healthy adults. Both mouthrinses significantly reduced aerobic and anaerobic bacterial counts 1 hour following their use. At 4 hours, CHX continued to produce an 85% reduction in bacteria and the EO was no more effective than rinsing with a normal saline solution.27
Briner et al. compared CHX to EO on salivary bacterial counts; both rinses were equally effective at 30 minutes. However, CHX was more effective at 3 hours and at 5 hours after rinsing than the EO.28 The use of CHX and EO-containing mouthrinse for one minute before a dental procedure has been shown to significantly reduce the bacterial load and contamination of the operative area and staff.29
Feres et al. reported that a 0.05% CPC mouthrinse, when used as a preprocedural mouthrinse, was equally effective as CHX in reducing the levels of splatter bacteria generated during ultrasonic scaling.30 Suresh et al. showed that one minute of preprocedural rinsing with 0.2% of CHX before dental procedures consistently reduced colony-forming units (CFU) as compared to prerinsing with an EO-containing mouthrinse.31
Essential Oils—include four active compounds derived from essential oils contained in a currently marketed EO mouthrinse: 0.063% thymol, 0.091% eucalyptol, 0.02% menthol with 0.0660% methyl salicylate.21,32 EO have strong evidence to support efficacy in reducing plaque and gingivitis.21,33 These essential oils kill microorganisms by disrupting their cell membranes and inhibiting enzyme activity.21,34 The EOs prevent bacteria from aggregating with Gram-positive pioneer species, slow bacterial multiplication and extract endotoxins from Gram-negative pathogens which reduces bacterial load.21,35
Rinsing with the EO antiseptic mouthrinse produced a 94.1% reduction in recoverable CFU compared with the non-rinse control. The non-rinse control treatment produced a 33.9% reduction in CFU.36 Preprocedural rinsing with an EO mouthrinse resulted in a 93.6% reduction in recoverable counts in aerosols generated 40 minutes after rinsing.37 DePaola et al. reported that an EO mouthrinse produced a 60 to 65% reduction in intraoral salivary bacteria (aerobic, anaerobic, Streptococci, Veillonella sp) from baseline at 2 minutes; the significant decreases were sustained up to 60 minutes. Total EO group aerobic, anaerobic and Streptococcal counts were significantly lower than the placebo group.38
Another study by Fine et al. reported the results of two clinical studies that were conducted to determine the efficacy of a mint flavored EO mouthrinse on the level of viable bacteria recovered from dental aerosols immediately after rinsing and then 40 minutes after rinsing. In the first study, the mint flavored mouthrinse group resulted in a 92.1% reduction in viable bacteria in aerosols immediately after rinsing, as compared to a control rinse.39 In the second study, the mint flavored EO mouthrinse
group produced a 91.3% reduction in viable bacteria in aerosols 40 minutes after rinsing, as compared to a control rinse. These studies suggest that preprocedural rinsing with a mint flavored EO mouthrinse may potentially reduce the risk of cross contamination in the dental operatory.39
Cetylpyridinium Chloride (CPC)—is a quarternary ammonium compound that is a cationic agent that will interact with the cell membrane of bacteria, affecting its permeability and resulting in the loss of cell contents, interference with cellular metabolism, inhibition of cell growth and cell death.21,40,41,42,43 CPC has been shown to inhibit the co-aggregation of bacteria, absorb to pellicle-covered enamel and inhibit co-adhesion of bacteria.44, 45, 46
A mouthrinse containing 0.05% CPC and 0.05% sodium fluoride was compared to a control mouthrinse containing 0.05% sodium fluoride to control supragingival plaque bacterial counts for 12 hours after a single treatment and 12 hours after 14 days’ use. The CPC mouthrinse significantly reduced supragingival plaque bacteria counts by 35.3% and 70.9% compared to the control fluoride mouthrinse 12 hours after a single use and after 14 days of use, respectively.47 Other studies have exhibited significant reductions in salivary aerobic and/or anaerobic bacterial counts for up to seven hours following a single rinse with a CPC-containing product.26,46,48,49
Schaeffer et al. reported that a new mouthrinse formulation containing 0.075% CPC and 0.05% sodium fluoride with and without alcohol statistically significantly reduced bacteria levels (Actinobacillus actinomycetemcomitans and Streptococcus mutans) by greater than 99.9% after a 30 second exposure.50
As mentioned previously, Feres et al. reported that a 0.05% CPC mouthrinse when used as a preprocedural mouthrinse was equally effective as CHX in reducing the levels of splatter bacteria generated during ultrasonic scaling.30
DiscussionThe Centers for Disease Control and Prevention (CDC) have indicated that dental aerosols should be controlled to the greatest extent possible.51,52 The CDC reports there is no scientific evidence that indicates that preprocedural mouth rinsing prevents clinical infections among patients or dental healthcare professionals. However, a possible association between the spread of oral microorganisms in the dental office and the development of infectious diseases such as ophthalmic or acute respiratory infections and tuberculosis can occur.17–19,30
Studies have shown that a preprocedural rinse with a product containing an antimicrobial product (chlorhexidine gluconate, essential oils, povidine iodine) can reduce the level of oral microorganisms generated in aerosols or splatter during routine dental procedures with dental handpieces and ultrasonic scalers.36,37,39,53–58 In 1997, the American Heart Association (AHA) suggested that patients at risk for bacterial endocarditis use an antimicrobial mouthrinse before dental treatment. Now, however, the AHA does not list preprocedural rinsing
Volume 84, Number 428

in their bacterial endocarditis guidelines.59 The CDC reports that preprocedural mouthrinses can be most beneficial before procedures (ultrasonic scaling, rubber cup prophylaxis polishing) where a rubber dam cannot be used to minimize aerosol and splatter.22,60 The use of a high volume evacuator should be used with ultrasonic or power scaling devices to control aerosols and splatter.18
The information discussed on the antimicrobial agents (CHX, EO and CPC) in this article will assist the dentist in choosing the proper mouthrinse to consider for a preprocedural rinsing protocol in practice. The dentist should determine the advantages and disadvantages of these agents to provide the clinical and scientific efficacy to reduce salivary bacterial load and aerosolized bacteria in the dental operatory. Selecting a product that is easy to purchase (prescription vs. over-the-counter), cost effective (using the mouthrinse with every patient), tastes pleasant (flavor is appealing to patients), and does not produce an aftertaste or burning sensation after rinsing will provide the best solution.
ConclusionThe implementation of a preprocedural rinsing program in the dental or specialty practice can assist in reducing bacterial salivary load in patients’ mouths and limit aerosolized bacteria and splatter in the dental operatory for a healthier office environment for the entire dental team.
References1. Micik RE, Miller RI, Mazzarella MA, Ryge G. Studies on dental
aerobiology, I: bacterial aerosols generated during dental procedures. J Dent Res 1969; 48(1): 49–56.
2. Miller RL, Micik RE, Abel C, Ryge G. Studies of dental aerobiology II:microbial splatter discharged from the oral cavity of dental patients. J Dent Res 1971;50:621–5.
3. Micik RE, Miller RL, Leong AC. Studies on dental aerobiology, III: efficacy of surgical masks in protecting dental personnel from airborne bacterial particles. J Dent Res 1971;50:626–30.
4. Abel LC, Miller RL, Micik RE, Ryge G. Studies on dental aerobiology, IV: bacterial contamination of water delivered by dental units. J Dent Res 1971;50:1567–9.
5. Hinds WC. Aerosol technology: Properties, behavior, and measurement of airborne particles. New York: Wiley;1982:6–8.
6. Cottone IA, Terezhalmy GT, Molinari JA. Practical infection control in dentistry. Baltimore: Williams & Wilkins;1996:139–40.
7. Crawford JJ, Broderius C. Control of cross-infection risks in the dental operatory: preventon of water retraction by bur cooling spray systems. J Am Dent Assoc 1988;116:685–7.
8. Osorio R, Toledano M, Liebana J, Rosales JI, Lozano JA. Environmental microbial contamination. Pilot study in a dental surgery. Int Dent J 1995, 45: 352–357.
9. Szymanska J. Dental bioaerosol as an occupational hazard in a dentist’s workplace. Am Agric Environ Med 2007;14:203–207.
10. Bennett AM, Fulford MR, Walker JT, Bradshaw DJ, Martin MV, Marsh PD. Microbial aerosols in general dental practice. Br Dent J 2000, 189: 664–667.
11. Harrel SK, Barnes JB, Rivera-Hidalgo F. Aerosol and splatter contamination from the operative site during ultrasonic scaling. J Am Dent Assoc 1998;129:1241–1249.
12. Leggat PA, Kedjarune U. Bacterial aerosols in dental clinic: review. Int Dent J 2001;51:39–44.
13. Mills SE, Kuehne JC, Bradley DV Jr. Bacteriological analysis of high-speed handpiece turbines. J Am Dent Assoc 1993;124:59–62.
14. Perry DA, Bird WF, Armitage GC. Aerosol management policy for powered scalers. CDHA J 2002;18:117–20.
15. Lewis DL, Arens M, Appleton SS, et al. Cross–contamination potential with dental equipment. Lancet 1992;340:1252–4.
16. Lewis DL, Boe RK. Cross–infection risks associated with current procedures for using high-speed dental handpieces. J Clin Microbiol 1992;30:401–6.
17. Checchi L, Montebugnoli L, Samaritani S. Contamination of the turbine air chamber: a risk of cross infection. J Clin Periodontol 1998;25:607–11.
18. Harrel SK, Molinari J. Aerosols and splatter in dentistry: A brief review of the literature and infection control implications. JADA 2004;135(4): 429–437.
19. King TB, Muzzin KB, Berry CW, Anders IM. The effectiveness of an aerosol reduction device for ultrasonic scalers. J Periodontol 1997;68(1): 45–9.
20. Logothetis DD, Gross KB, Eberhart A, Drisko C. Bacterial airborne contamination with an air-polishing device. Gen Dent 1988; 496–9.
21. Hovliaras CA. SAVVY SUCCESS: Achieving professional excellence and career satisfaction in the dental hygiene profession, Volume II: Patient care. Charles C, Santos S, Morris A. Chapter 29: Role of daily use mouthrinses in maintaining oral health. Indiana; Authorhouse; 2012:245–262.
22. Stanley A, Wilson M, Newman H. The in-vitro effect of chlorhexidine on subgingival plaque bacteria. J Clin Periodontol 1989;16(4):254–264.
23. Kaplowitz G, Collins FM. Pre–procedural rinsing: A pre–emptive protocol. Available at: http://www.ineedce.com/courses/1478/PDF/PreProceduralRinsing.pdf. Accessed on September 15, 2013.
24. Veksler AE, Kayrouz GA, Newman MG. Reduction of salivary bacteria by pre-procedural rinses with chlorhexidine 0.12%. J Periodontol 1991;62(11):649–51.
29Volume 84, Number 4
25. Eapen T. Efficacy of two commonly available mouth rinses used as preprocedural rinses in children. J Ind Soc Pedo Prevent Dent 2011;29(2): 113–116.
26. Roberts WR, Addy M. Comparison of the in vivo and in vitro antibacterial properties of antiseptic mouthrinses containing chlorhexidine, alexidine, cetyl pyridinium chloride and hexetidine. Revelance to mode of action. J Clin Periodontol 1981;8(4):295–310.
27. Balbuena I, Stambaugh KI, Ramirez SG, Yeager C. Effects of topical oral antiseptic rinses on bacterial counts of saliva in healthy human adults. Otolaryngol Head Neck Surg 1998;118(5):625–629.
28. Briner WW, Kayrouz GA, Chanak MX. Comparative antimicrobial effectiveness of a substantive (0.12% chlorhexidine) and a nonsubstantive (phenolic) mouthrinse in vivo and vitro. Compendium 1994;15(9):1158, 1160, 1162.
29. Worral SF, Knibbs PJ, Glenwright HD. Methods of reducing bacterial contamination of the atmosphere arising from use of an airpolisher. Br Dent J 1987;163:118–9.
30. Feres, M, Figueiredo LC, Faveri M, Stewart B, DeVizio W. The effectiveness of a preprocedural mouthrinse containing cetylpyridinium chloride in reducing bacteria in the dental office. JADA 2010;141(4): 415–422.
31. Suresh S, Manimegalai M, Sudhakar U, Sopia. Comparison of efficacy of preprocedural rinsing with chlorhexidine and essential oil mouthwash in reducing viable bacteria in dental aerosols—A microbiological study. Int J Contemp Dent 2011;2(6):1–6.
32. Department of Health and Human Services. Oral health care drug products for over-the-counter human use; antigingivits/antiplaque drug products; establishment of a monograph; proposed rules. Part III. Food and Drug Administration. Federal Register 2003;68(103):32241–32243.
33. Van Leeuwen MPC, Slot DE, Van der Weijden GA. Essential oils compared to chlorhexidine with respect to plaque and parameters of gingival inflammation: A systemic review. J Periodontol 2011;82(2):174–194.
34. Fine DH, Furgang D, Lieb R, Korik I, Vincent JW, Barnett ML. Effect s of sublethal exposure to an antiseptic mouthrinse on representative plaque bacteria. J Clin Periodontol 1996;23(5): 444–451.
35. DePaola LG, Overholser CD, Meiller TF, Minah GE, Niehaus C. Chemotherapeutic inhibition of supragingival dental plaque and development. J Clin Periodontol 1985;12:697–704.
36. Fine DH, Mendieta C, Barnett ML, Furgang D, Meyers R, Olshan A, Vincent J. Efficacy of preprocedural rinsing with an antiseptic in reducing viable bacteria in dental aerosols. J Periodontol 1992;63(10)821–4.
37. Fine DH, Yip J, Furgang D, Barnett ML, Olshan AM, Vincent J. Reducing bacteria in dental aerosols: pre-procedural use of an antiseptic mouthrinse. JADA 1993;124(5)L56–8.
38. DePaola LG, Minah GE, Overholser CD, Meiller TF, Charles CH, Harper DS, McAlary M. Effect of an antiseptic mouthrinse on salivary microbiota. Am J Dent 1996;9(3):93–5.
39. Fine DH, Furgang D, Korik I, Olshan A, Barnett ML, Vincent JW. Reduction of viable bacteria in dental aerosols by preprocedural rinsing with an antiseptic mouthrinse. Am J Dent 1993;6(5):219–21.
40. ten Cate JM, Marsh PD. Procedures for establishing efficacy of antimicrobial agents for chemotherapeutic caries prevention. J Dent Res 1994; 73(3):695–703.
41. Scheie A. Modes of action of currently known chemical anti-plaque agents other than chlorhexidine. J Dent Res 1989;68(Spec Iss):1609–16.
42. McDonnell G, Russell AD. Antiseptics and disinfectants: activity, action, and resistance. Clin Microbiol Rev 1999;12:147–79.
43. Gilbert P, Moore LE. Cationic antiseptics: diversity of action under a common epithet. J Applied Micro 2005;99:703–15.
44. Smith RN, Andersen RN, Kolenbrander PE. Inhibition of intergeneric coaggregation among oral bacteria by cetylpyridiunium chloride, chlorhexidine digluconate and octenidine dihydrochloride. J Periodontol Res 1991;26: 422–8.
45. Busscher HJ, White DJ, Atema-Smith J, Geertsem a-Doornbusch G, de Vries J, van der Mei HC. Surfacttive and antibacterial activity of cetylpyridium chloride formulations in vitro and in vivo. J Clin Periodontol 2008;35:547–54.
46. Williams MI. The antibacterial and antiplaque effectiveness of mouthwashes containing cetylpyridinium chloride with and without alcohol in improving gingival health. J Clin Dent 2011;22[Spec Iss]:179–182.
47. Hu D, Li X, Sreenivasan PK, DeVizio W. A randomized, double-blind clinical study to assess the antimicrobial effects of a cetylpyridium chloride mouth rinse on dental plaque bacteria. Clin Ther 2009;31:2540–8.
48. Jenkins S, Addy M, Wade W, Newcombe RG. The magnitude and duration of the effects of some mouthrinse products on salivary bacterial counts. J Clin Periodontol 1994;21:397–401.
49. Elworthy A, Greenman J, Doherty FM, Newcombe RG, Addy M. The substantivity of a number of oral hygiene products determined by the duration of effects on salivary bacteria. J Periodontol 1996;67:572–6.
50. Schaeffer LM, Szewczyk G, Nesta J, Vandeven M, Du-Thumm L, Williams MI, Arvanitidou E. In vitro antibacterial efficacy of cetylpyridinium chloride–containing mouthwashes. J Clin Dent 2011;22[Spec Iss]:183–6.
Volume 84, Number 430

51. Kohn WG, Collins AS, Cleveland JL, et al. Guidelines for infection control in dental health-care settings—2003. MMWR Recomm Rep 2003;52(RR–17):1–61.
52. Centers for Disease Control and Prevention. Infection control in dental settings. Frequently asked questions—preprocedural mouth rinse. Available at: http://www.cdc.gov/oralhealth/infectioncontrol/faq/preprocedural_mouthrinse.htm. Accessed on September 30, 2013.
53. Litsky BY, Mascis JD, Litsky W. Use of an antimicrobial mouthwash to minimize the bacterial aerosol contamination generated by the high-speed drill. Oral Surg Oral Med Oral Pathol 1970;29:25–30.
54. Mohammed CI, Monserrate V. Preoperative oral rinsing as a means of reducing air contamination during use of air turbine handpieces. Oral Surg Oral Med Oral Pathol 1970;29:291–4.
55. Wyler D, Miller RL, Micik RE. Efficacy of self administered preoperative oral hygiene procedures in reducing the concentration of bacteria in aerosols generated during dental procedures. J Dent Res 1971;50:509.
56. Muir KF, Ross PW, MacPhee IT, Holbrook WP, Kowolik MJ. Reduction of microbial contamination from ultrasonic scalers. Br Dent J 1978;145:76–8.
57. Logothetis DD, Martinez-Welles JM. Reducing bacterial aerosol contamination with a chlorhexidine gluconate pre-rinse. JADA 1995;126:1634–9.
58. Klyn SL, Cummings DE, Richardson BW, Davis RD. Reduction of bacteria-containing spray produced during ultrasonic scaling. Gen Dent 2001; 49:648–52.
59. Wilson W, Taubert KA, Gewitz M, Lockhart BP, et al. Prevention of infective endocarditis: guidelines from the American heart association. Circulation 2007;116:1736–1754.
60. Costello MR. Dental dams: the secret tool for infection control. Compend Contin Educ Dent 2006;27(3):196–9.
About the AuthorChristine A. Hovliaras, RDH, BS, MBA, CDE, is president of Professional Savvy, LLC, an oral care consulting, professional marketing and continuing education company in New Jersey. Christine is a dental hygiene professional with over 29 years experience in the dental profession and works for Dr. Marc Appelbaum in Morristown, NJ. The author’s honorarium for production of this article was supported by an unrestricted educational grant from Colgate-Palmolive.
With its unmatched record of successes in dental practice transitions, don’t you owe it to yourself to discover why more than 3,600 dental professionals have turned to The Clemens Group to get them the highest possible valuations for their practices?
Clemens professionals are there to guide and support you every step of the way with the understanding, expertise, and integrity you deserve from the area leader in dental practice sales.
Call today for a confidential, complimentary consultation and see the differ-ence a second opinion can make.
THINKING OF SELLING YOUR PRACTICE? GET A SECOND OPINION FIRST.
Visit us at TheClemensGroup.com or call us toll-free at 1-800-300-2939
Founding member, American Dental Sales All ADS companies are independently owned and operated Listed ADA Dental Practice Appraiser and Valuator Founding member, National Practice Valuation Study Group
31Volume 84, Number 4

“(Just before the last recession) in 2007, the number of dental establishments throughout the state had increased to 4,618 facilities (from 4,380 in 2001) with a continuing decrease in population to 1,880 residents per establishment (compared to 2,385 nationally). The number of employees per ‘average’ establishment increased to 6.2 individuals (comparable to 6.3 nationally).”2
This was the summary statement in an earlier presentation in the JNJDA just before the onset of the last recession. “The Business Cycle Dating Committee of the National Bureau of Economic
Research…determined that…the recession that began in December 2007… (had ended) in June 2009. The recession lasted 18 months, which makes it the longest of any recession since World War II.”3 Reports from the Census Bureau’s annual study of business patterns for each county and state (with specific information on numbers of establishments, employees and salaries) permit a review of these differences. (See the Legend section for the definition of an establishment.)
Evolving Practice ConfigurationsIn 2013, the ADA’s Health Policy Resources Center suggested “…very strongly that the dental economy is in a major transition…
New Jersey Dental Establishments in 2011: After the Last Recession
H. Barry Waldman, DDS, MPH, PhD
30 years experience serving the
dental community!
Providing quality insurance products, at com-petitive prices, with outstanding customer ser-vice; this is our business philosophy. You, our
clients, are our primary concern.
The Insurance Agency for Dentists, LLC
Bob Opperman
609-492-5608/215-990-6709
Fax: 609-492-5609
Email: [email protected]
MY PROFESSION IS
YOUR PROTECTION!
Volume 84, Number 432

Dental spending has not rebounded since the end of the Great Recession and has been stagnant, on a per capita basis, since 2008… the declines in both dental spending and visits predate the economic crisis of 2008.”4 In light of these findings, the changes in business patterns for the delivery of dental services were considered.
Nationally—Between 2007 and 2011 there was an increase of almost five thousand dental establishments, including almost 2,300 small establishments (less than 5 employees) and almost 2,050 establishments with 5–9 employees. (See the Legend section for the definition of employees.) Nevertheless, in this recent period just before the last recession and a couple of years after the end of the recession, as the nation struggled to overcome the impact of the recession:
• The proportion of the dental establishments with less than five employees remained essentially unchanged (at approximately 40%). In the past, between 1990 and 2001, these small establishments decreased from 54.9% to 43.4% of all dental establishments.2 (Table 1).
• The increase of almost five thousand dental establishments between 2007 and 2011 mirrored the general national population increases. As a result, there was only a slight decrease in the population per dental establishment from 2,401 to 2,376 individuals.
New Jersey—Between 2007 and 2011 there was an increase of 102 dental establishments, with the largest increase in the number of 5–9
employee dental establishments. During this period, there was limited change in the proportional representation of small establishments (46%). Similarly, during this period, there were very limited changes in the: 1) number of employees per “average” dental establishment (from 6.1 to 6.2 employees), and 2) population per dental establishment at the overall state level (from 1,880 residents per establishment in 2007 to 1,862 residents per establishment in 2011).5 In 2011, the “average” salary of a dental establishment employee was $43,800. (Table 2) (See Legend section for definition of “average.”)
LegendAn establishment is a single physical location where services are performed. It is not necessarily identical to a company or enterprise, which may consist of one or more establishments. In addition, one or more practitioners may be present in an establishment. Throughout this presentation, (except where specified) the term “dental establishment” refers to those facilities 1) with employees and 2) subject to federal income tax. Government agency programs (hospitals and health department clinics) are not included.
Employees may include dentists, dental hygienists, dental assistants, office staff, etc.
Average dental establishment While there is no such thing as an “average” dental establishment, comparisons between averages (over time and between locales) do provide a picture
• Dr. Gordon Christensen - “Implant Prosthodontics - 2014”
• Dr. Uche Odiatu - “The Miracle of Health”
• AAFE - “Botox Use In Dentistry” - Lecture and Hands On, Part I
• Hiossen - “AIC Basic Implant Course” - Part I
• Dr. Rella Christensen - “What's New in Caries, Restoratives, Laser Perio
and Infection Control”
• Dr. Samuel B. Low - “Successful Management of Periodontal Patient”
• AAFE - “Dermal Fillers In Dentistry” - Hands On, Part II
• Hiossen - “AIC Basic Implant Course” - Part II
• Dr. Harold L. Crossley - “The Real Deal About Street Drugs and Their Effects on You, Your Friends, and Your Dental Practice”
• Dr. John H. Tucker - “Dental Sleep Medicine”
• Dr. Leonard F. Tau - “21st Century Marketing: Using the Power of the Internet and Social Media to Step Up Your Practice”
• Hiossen - “AIC Basic Implant Course” - Part III
Pennsylvania’s Premiere Dental Conference
STEPPING UP
YOUR PRACTICE
with a little help from your friends
28TH ANNUAL
VALLEY FORGE
DENTAL CONFERENCEMark Your Calendar for the...
MARCH 5-6-7, 2014
VALLEY FORGE RADISSON HOTEL
KING OF PRUSSIA, PA
REGISTRATION NOW OPEN AT:
www.vfdc.org800-854-VFDC
• CERP & PDHA Accredited Seminars
• PA CE Requirements
• Cutting Edge Courses for Doctors & Staff
• Exhibit Hall Featuring 52 Companies
WEDNESDAY, MARCH 5, 2014
THURSDAY, MARCH 6, 2014
FRIDAY, MARCH 7, 2014
33Volume 84, Number 4

of the evolving practice of dentistry. The “average” number of employees in New Jersey was determined by dividing the total number of dental employees (29,374) by the number of dental establishments (4,720). The “average” salary was determined by dividing the total annual state payroll figure for dental establishment employees ($1,285,677,000) by the total number of employees (29,374 individuals).
Number of Employees at the County LevelIn 2011, there were 29,374 employees in dental establishments in New Jersey (almost 855,000 nationally). The number of employees in “average” dental establishments in New Jersey counties ranged from a low of 5.0 employees in Bergen County to 10.9 employees in Cumberland County. (Table 2)
Average Salary at the County Level Statewide, the average employee salary was $43,800 (nationally, $45,200). Average employee salaries ranged from $34,800 in Hudson County to $55,700 in Mercer County. (Table 2) (Again, it should be noted, that “employees” may include dentists.) Dental Establishments With No EmployeesIn 2010, there were an additional 1,588 New Jersey dental establishments that were subject to federal income tax but with no employees. These non-employee dental facilities represented one-quarter of the total number of dental establishments in the state in 2010 (i.e., 4,720 dental establishments with employees plus 1,588 establishments with no employees). The New Jersey dental facilities with no employees in 2010 reported a total of $138 million in gross receipts ($86,900 per establishment). Nationally, in 2010 there were 40,897 dental establishments with no employees that reported more than $3.1 billion in gross receipts (an annual average of $75,800 in gross receipts per establishment).
During 2010, in New Jersey, most nonemployee dental establishments were individual proprietorships with average annual gross receipts of $72,400. A smaller number of corporate arrangement facilities had average annual gross receipts of $177,200; a few partnerships had average annual gross receipts of $329,000.8
Given the increasing numbers of employees per dental establishment with employees, how does one account for the great number of facilities with no employees? It was suggested in a previous review that nonemployee establishment arrangements might include:
• Recent graduates just starting practices.• Older practitioners who are decreasing their time commitment
to practice as they prepare for eventual retirement.• An establishment that serves as a secondary activity for an
individual who works full-time for someone else.• Contracts with independent outside firms for auxiliary personnel.• Use of family members as auxiliary personnel and where no
reports are made for Social Security and income tax purposes.• Establishments of independent corporate arrangements for in-
house auxiliaries.• Any number of other alternative practice arrangements
(including practice in private homes and other locations) that do not file required quarterly payroll tax reports.9
Overview: 2007–2011———————————————————————————Between 2007 and 2011:• The number of dental establishments has increased nationally
and in New Jersey (albeit at a slower rate than in previous periods).• The population per dental establishment in New Jersey
decreased to a very limited extent. • The number of employees per average establishment in New
Jersey has remained constant.• Nationally and in New Jersey, the proportional representation of
small dental establishments has remained stable.
Nevertheless, in light of the ADA economic report regarding the stagnation of dental economics, continued monitoring of generalized dental establishment business activities beyond the confines of a single facility is essential, and does provide an appreciation of developments that affect the profession in general and in particular, your establishment. How’s Your Practice Doing?Now that you’ve compared your personal dental establishment numbers to those of the average establishment in your county, remember: there is no such thing as an “average” dental establishment. The particular requisites of your community determine business events in your establishment, including employment patterns, employee salaries and the like. Unfortunately, information from various government agency and professional association reports does not provide data for the numerous particular locales. Table 1. Distribution of dental employees by size of dental establishments. New Jersey and the United States: 2007, 20115
Note: Differences in percentage totals are due to rounding
Volume 84, Number 434
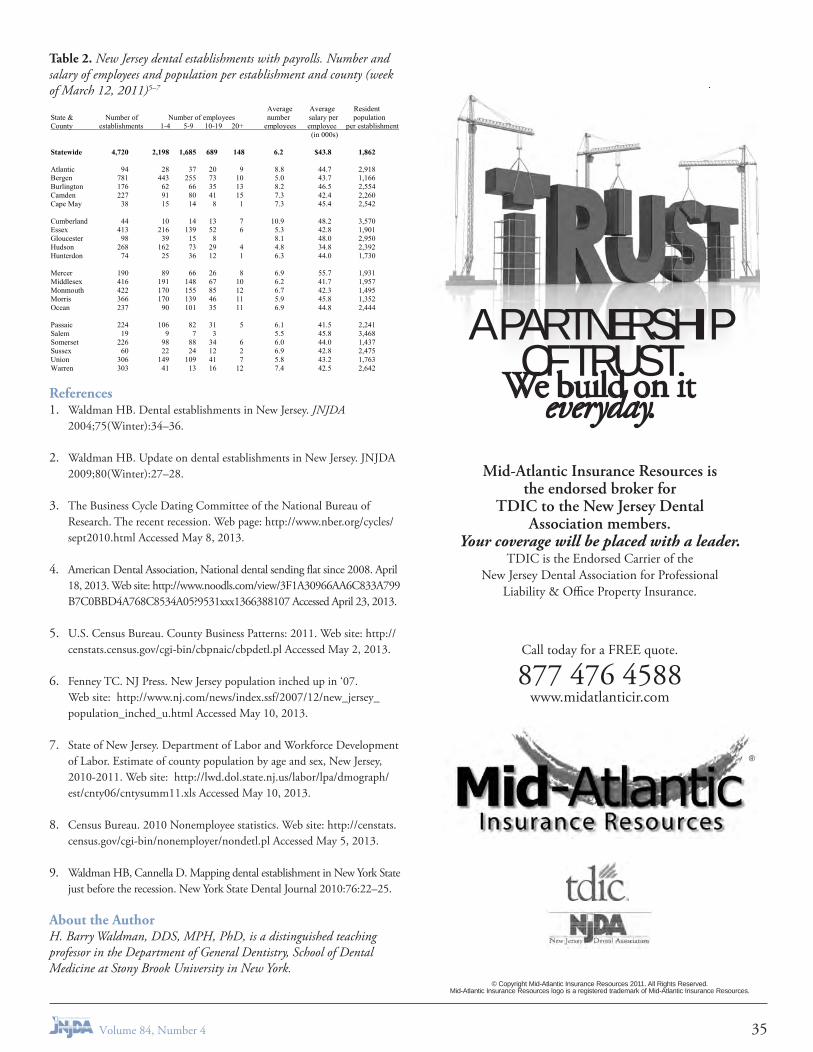
Table 2. New Jersey dental establishments with payrolls. Number and salary of employees and population per establishment and county (week of March 12, 2011)5–7
References1. Waldman HB. Dental establishments in New Jersey. JNJDA
2004;75(Winter):34–36.
2. Waldman HB. Update on dental establishments in New Jersey. JNJDA 2009;80(Winter):27–28.
3. The Business Cycle Dating Committee of the National Bureau of Research. The recent recession. Web page: http://www.nber.org/cycles/sept2010.html Accessed May 8, 2013.
4. American Dental Association, National dental sending flat since 2008. April 18, 2013. Web site: http://www.noodls.com/view/3F1A30966AA6C833A799B7C0BBD4A768C8534A05?9531xxx1366388107 Accessed April 23, 2013.
5. U.S. Census Bureau. County Business Patterns: 2011. Web site: http://censtats.census.gov/cgi-bin/cbpnaic/cbpdetl.pl Accessed May 2, 2013.
6. Fenney TC. NJ Press. New Jersey population inched up in ‘07. Web site: http://www.nj.com/news/index.ssf/2007/12/new_jersey_population_inched_u.html Accessed May 10, 2013.
7. State of New Jersey. Department of Labor and Workforce Development of Labor. Estimate of county population by age and sex, New Jersey, 2010-2011. Web site: http://lwd.dol.state.nj.us/labor/lpa/dmograph/est/cnty06/cntysumm11.xls Accessed May 10, 2013.
8. Census Bureau. 2010 Nonemployee statistics. Web site: http://censtats.census.gov/cgi-bin/nonemployer/nondetl.pl Accessed May 5, 2013.
9. Waldman HB, Cannella D. Mapping dental establishment in New York State just before the recession. New York State Dental Journal 2010:76:22–25.
About the AuthorH. Barry Waldman, DDS, MPH, PhD, is a distinguished teaching professor in the Department of General Dentistry, School of Dental Medicine at Stony Brook University in New York.
Statewide 4,720 2,198 1,685 689 148 6.2 $43.8 1,862
A PARTNERSHIP OF TRUST
We build on it everyday.
Mid-Atlantic Insurance Resources is the endorsed broker for
TDIC to the New Jersey Dental Association members.
Your coverage will be placed with a leader.TDIC is the Endorsed Carrier of the
New Jersey Dental Association for Professional Liability & Office Property Insurance.
© Copyright Mid-Atlantic Insurance Resources 2011. All Rights Reserved. Mid-Atlantic Insurance Resources logo is a registered trademark of Mid-Atlantic Insurance Resources.
Call today for a FREE quote.
877 476 4588 www.midatlanticir.com
®
35Volume 84, Number 4

I t may come as no surprise to anyone, but I am the youngest member of the Passaic County Dental Society. I am also the youngest member on the Board of Trustees and third in line to
be our next society president. You can say that I got an early start to getting involved.
Becoming a dentist never made my top ten list of what I wanted to be when I grew up. Even though I had a father who was a dentist, becoming a ballerina or a baker seemed much more appealing to me. As the years passed, I did some maturing, reached high school and realized medicine was where my future was headed. I studied hard, got good grades, got accepted to Georgetown University and started college as a biology major. Throughout college, various family and friends would hint at the possibility of applying to dental school. I would usually just brush it off until one of my father’s dental school classmates sat me down at a summer barbecue and told me to apply to medical school but to also apply to just one dental school and then make my decision. That conversation ended up changing my life and future career path. I took his advice, took the DATs, applied to dental school on a whim and got accepted to UMDNJ. Hello dentistry! Those four years in dental school were the best and worst years of my life. However, as they say, at the end of every dark tunnel is a white light. Graduation day, May 16, 2010, was the happiest day of my life. I felt lucky to have found a profession that I truly loved and was passionate about. It was also the happiest day of my father’s life, because he finally found his exit strategy.
Even before the ink had dried on my diploma, my father talked to me about joining organized dentistry and the importance of getting involved and giving back to the profession. My first year out of dental school I attended every Passaic County Dental Society meeting and the next year joined the Board of Trustees, alongside my father; the year after that I became an officer. As you can see, it did not take much time or effort to suck me in.
So far, my experience with PCDS has been great. I was warmly welcomed by my fellow colleagues. I have made valuable friendships and been exposed to many different aspects of the dental world. I have formed bonds and mentorships with clinicians thirty years my senior. More importantly, I have found a forum where there is no stupid question, there is no judgment, and members are there to mutually support each other. Not only that, they are there to share
their stories and ideas: What worked for them, and what didn’t work so much.
We, PCDS, are known to have one of the most culturally diverse societies and one of the nicest. We also have many more women than any other society in New Jersey. Our meetings are not cliquish, our members are all approachable and inviting and there is always someone to greet you. There really is the sense of camaraderie and family at every meeting. More often than not, the conversations are centered around family, kids, health and sports.
We also cannot forget what organized dentistry has done and continues to do for us as a profession. We have constant support and resources from a group of people who advocate for our rights and best interests as dentists. As an NJDA member, I can call the NJDA headquarters at any time, pertaining to any issue I may be having in the office. These include legal issues and/or questions, state board, advertising, laws governing hygienists, HIPAA, OSHA, insurance issues, and many, many more. These people have all, for the most part, been involved in dentistry their entire careers and are here to provide us with advice and know-how which, in the long run, saves us time, money, and most importantly, aggravation. All you have to do is call and they actually return the call!
The bottom line is, I honestly do not understand how anyone in this present environment can afford to practice without the backing of organized dentistry. Yes, the economy has changed; yes, practices are slower; and yes, patients have become more demanding. However, these are all the more reasons to stick together as peers, as a profession, and ride out the storm together. There will always be something that could be better, that could be changed, but I am happy to be part of an organization that embraces change and engages conversation for a better tomorrow for you and me.
About the AuthorDena Constandelis, DMD, is a general dentist in practice with her father, Theodore Constandelis, DDS. Their practice, Constandelis Dental Family and Aesthetic Dentistry, has been located in Clifton for more than 30 years. In addition to being involved in organized dentistry, when she finds the time, Dr. Dena enjoys reading, trying new restaurants and running.
This guest editorial originally was published in the PCDS newsletter and is reprinted with permission of the author and the Society.
Opinion:New Kid on the Block
Dena Constandelis, DMD
Volume 84, Number 436

Opportunities AvailableDentist Needed for Space Share in Newly Renovated Office.State-of-the-art, recently remodeled facility equipped with an in-office lab & cone beam technology. Located on a professional suburban street in Bloomfield, New Jersey with easy access rear parking. Well-respected office established for over 50 years. Contact the Office Manager, at: (973) 769-4794 to get details.
Established Multidisciplinary Specialty Dental Practice Seeks a Pediatric Dentist.Located in a suburb of Princeton, Hamilton Dental Associates has been serving central New Jersey for over 50 years. Full-time or part-time associate position leading to equity position for the right individual. Hamiltondental.com. Email: [email protected] or telephone (609) 586- 6603.
Offices For Lease Or PurchaseDental Office.Monmouth County—Ocean Township—NJ—In modern established medical arts building. All dental plumbing, electrical, dental cabinetry and lab in place. Plus 2/3 operatories, furnished waiting room, private bathroom, nurses’ station, private doctor’s office. $1,675 per month, all inclusive. Including all utilities, HVAC, CAM and maintenance. Mr. Mirne (732) 539-6987.
Perfect Office for a Dental Specialist & Support Staff (Medical Practice, or Health Care Professional).Operatory/treatment rooms are plumbed and with electrical power. First floor, parking. Desirable Princeton NJ, high traffic location. Possibly sub-dividable. Contact Michael Mayo, Weichert Realtors, (609) 921-1900 ext 241 cell (713) 449-6498, [email protected] for details.
Linwood Office Condo Lease/Sale.1235 sf., beautiful space, excellent condition, 3 plumbed, networked rooms with cabinetry. Track lights, 4th plumbed, central nitrous. Some equipment for sale separately. Long term lease available. Can sublease. Rent $1999/month includes taxes and condo fees. Purchase option or sale for 250K. (609) 335-4387; [email protected].
Dental Office Space for Rent:Medical office complex in Hunterdon County, presently with 3 chairs/lines, 2 offices, lab, waiting room and bathroom-approximately 1,500 sq. ft. Ideal location for professional, dental or oral surgery office. Office is beautifully decorated/updated in a well cared for medical office building located just off Route 31 with easy access to Route 78 in Annandale, NJ. Available February 2014. Call Judy or Manny (908) 730-6774.
Forked River Ocean County.Office space to share. Orthodontic practice looking to share existing 2,500 sq. ft. office. Ideal for an Endodontist or Periodontist. There are no Perio or Endo practices between Toms River and Barnegat. Space has 2 pvt. treatment rooms and a bay with 4 chairs. Call (732) 995-5297 or email [email protected].
For Sale-Dental Building—Dunellen Middlesex County—$299,900The first floor is a full dental office with 4 operatories. The second floor has a 2 bedroom rental apartment. Separate utilities. Downtown location, walk to train station. Have your dental office downstairs and offset the expenses with the rental income from the apartment. Contact Andrea Lacerda, Prudential NJ Properties (908) 578-1166.
Opportunities SoughtNJ DDS (Semi-Retired) Seeking P/T Position1.) for diagnosis and treatment planning (732) 506-7777. 2.) Seeking satellite office (P/T) Ocean/Monmouth County (732) 644-3000 with/ without staff.
Classifieds
Wednesday, February 26, 2014 Nitrous Oxide Sedation (HANDS-ON)
Dr. Stanton Braid and Dr. Allan Fielding
Wednesday, March 12, 2014 Dental Management of Emergencies and
Medically Compromised Patients Dr. Gary Jones and Dr. Allan Fielding
Friday, March 21, 2014 2nd Annual Engine Driven Instrumentation in
Endodontics – Panel Discussion Moderator: Dr. Cemil Yesilsoy
Speakers: Dr. Chris Glass, Dr. Eric Herbranson and Dr. Martin Trope
Wednesday, April 2, 2014 Updates in Pediatric Dentistry:
Treating Tiny Tots to Teens Dr. Lance Kisby
Friday, April 18, 2014 Feel Good Dentistry –
A Sane Approach to Esthetic Dentistry Dr. Steven Weinberg
Friday, May 16, 2014 Limiting Exposure in the 21st
Century Dental Practice Dr. Michael Ragan
September 12-14, 2014 Bender Seltzer and Grossman
Academic Review of Endodontology Course Director: Dr. Cemil Yesilsoy;
Speakers: Drs. Eleazer, Fouad, Hersh, Holland, Hutter, Keiser, Khan, Pringle and Trope
To advertise please visit:www.mgxprint.com
and click on the JNJDA linkto fill out a classified ad order form
37Volume 84, Number 4

Consultants/ServicesPractice Transitions.We specialize in Practice Sales, Appraisals and Partnership Arrangements. Financing available. Free Guides for Sellers and Buyers. Contact Philip Cooper, DMD, MBA, American Practice Consultants, (800) 400-8550, [email protected].
Let Me Pay for Your Hawaiian Vacation!NJ and PA licensed GP will do quality endo in your office. Also available as an office fill-in for a general dentist. Call (856) 772-2293.
Florida Health Seminar.December 20, 2013. Boca Raton, Fla. AGD, ADA-CERP, C.E. Credits. Endodontics, oral surgery, pediatric dentistry, risk management (HIV update). Contact Linda Golnick, Coordinator: (248) 388-1959 Fax (248) 681-0315.
Sell Your Practice, Realize Your Equity, and Begin Enjoying Your Career!Summit Dental Group is a Dentist-focused organization that allows owner doctors to realize the equity in their practice while continuing to practice in a management free role allowing them to focus on what they enjoy most...patient care.
SDG was created by exceptional dentists, and we want to acquire exceptional practices. We offer win-win-win solutions for you, your staff and your patients that provide you with the greatest value for your practice so you can move forward with your future. You can continue to work without the responsibilities of running a business and we will customize a solution that’s well-suited for you. Our dentists have the clinical control enjoyed in a traditional private practice without the additional financial or administrative burdens associated with practice management. When considering a practice transition with SDG, dentists can expect unlimited production-based earnings, a strong benefits package, a familiar patient base, continuing education opportunities, and long-term clinical or managerial career growth. To learn more please call (201) 875-7522 or visit us on the web at www.SummitDentalGroupNJ.com.
ClassifiedsTHE
Your Business, Lifestyle, and Retirement
PRACTICE INSURANCE INCLUDES
BEST
SINCE INSURANCE IS A NECESSITY WHY NOT GET THE MOST OUT OF IT?Because of our synergistic approach, we provide more dentalpractice insurance than any other New Jersey agency. Why? Wecover every risk aspect from malpractice to property, casualty,workers’ comp, cyber, health and disability coverage. Constantupdating of these plans keeps you safe. Some of our work-sitefeatures also supply your employees with college scholarshipsat no cost to them. Your house and properties, including all vehicles are integrated into these plans to cut costs and provideyou with total peace of mind. Retirement? By using Pension Protection Act 2006 we help you to get more retirement income.
HOW DO YOUR PRESENT PLANS STACK-UP? Now, you can eliminate risk, lower your costs, and gain an enhanced retirement all supported by an unexcelled threedecades of experienced professional service to your profession.
Call us now for an audit of your situation with helpful suggestions at no cost. Because the best practice insurancemust include your business, lifestyle and retirement.
34 Sycamore Avenue • Little Silver, NJ 07739T: 732-842-2020 • F: 732-842-2221 • www.bcszerlip.com
Endorsed By
BCSzerlip_NJDA_BestAd_v8 7/18/13 4:36 PM Page 1
Volume 84, Number 438

Practices For SalePractices for SaleESSEX COUNTY: 2M long-established PPO insurance practice located in a storefront in a high traffic area. The practice is completely digital with 6 equipped operatories and room for expansion. The practice receives 30 new patients per month and has close to 3,000 active patients. The real estate can be purchased or leased at the buyers’ discretion. Asking price for practice is 1.3M.
TRENTON: 800K long-established PPO/FFS practice located in a professional building. Space has 4 equipped operatories in 1,250 square feet. Practice has 4.5 days of hygiene. Office is computerized and has digital x-rays as well as a digital panorex. Real estate can be purchased for 200K or leased. Asking price for practice is 550K.
If interested in either of the above opportunities please call Dr. Ronald Nemeroff at (212) 223-2844 or visit our website at rmndentalbrokers.com for more information.
Classifieds
C
M
Y
CM
MY
CY
CMY
K
NJ-SEP-2013.pdf 1 9/6/13 4:15 PM
MeMbership with NJDAConsidering membership with the NJDA? Here are some highlights of what you get as a member.
MeMbership supports your professioN
Exciting new changes!NJDA announces several new improvements coming soon that will contribute to better serving member dentists as technology and the economy change.
New Dentist conference
Member Day
register, pay for, and keep track of NJDA Ce courses you take on our New website
special Discounts and services from endorsed business Associates (ebA)
NEWjobsearch&classifiedadvertisementfunctionality available to all members automatically
easy-to-access information via our website, the Advocate, the Journal, and your component newsletter
Members-only courses at less than $10/credit
We are constantly learning and growing as an association. If you feel we could better serve you, we’d like to know how! Feel free to reach out at any time. The more dentists involved in our organization, the stronger your practice and your profession.
Serving your practice. Advancing your profession.
Don’t leave decisions that impact you and your profession up to people who aren’t dentists
Organized dentistry is a political force in Trenton. Through a combination of a vibrant New Jersey Dental Political Action Committee (NJDPAC), and an active grassroots membership (including more than 4,600 NJDA members), organized dentistry makes its voice heard in the State House.
Membership and support of NJDPAC guarantee you and other New Jersey dentists that we keep our influential voice in Trenton.
Questions?Call us today: 800-831-6532Or Email: [email protected]
MeMbership with NJDAConsidering membership with the NJDA? Here are some highlights of what you get as a member.
MeMbership supports your professioN
Exciting new changes!NJDA announces several new improvements coming soon that will contribute to better serving member dentists as technology and the economy change.
New Dentist conference
Member Day
register, pay for, and keep track of NJDA Ce courses you take on our New website
special Discounts and services from endorsed business Associates (ebA)
NEWjobsearch&classifiedadvertisementfunctionality available to all members automatically
easy-to-access information via our website, the Advocate, the Journal, and your component newsletter
Members-only courses at less than $10/credit
We are constantly learning and growing as an association. If you feel we could better serve you, we’d like to know how! Feel free to reach out at any time. The more dentists involved in our organization, the stronger your practice and your profession.
Serving your practice. Advancing your profession.
Don’t leave decisions that impact you and your profession up to people who aren’t dentists
Organized dentistry is a political force in Trenton. Through a combination of a vibrant New Jersey Dental Political Action Committee (NJDPAC), and an active grassroots membership (including more than 4,600 NJDA members), organized dentistry makes its voice heard in the State House.
Membership and support of NJDPAC guarantee you and other New Jersey dentists that we keep our influential voice in Trenton.
Questions?Call us today: 800-831-6532Or Email: [email protected]
MeMbership with NJDAConsidering membership with the NJDA? Here are some highlights of what you get as a member.
MeMbership supports your professioN
Exciting new changes!NJDA announces several new improvements coming soon that will contribute to better serving member dentists as technology and the economy change.
New Dentist conference
Member Day
register, pay for, and keep track of NJDA Ce courses you take on our New website
special Discounts and services from endorsed business Associates (ebA)
NEWjobsearch&classifiedadvertisementfunctionality available to all members automatically
easy-to-access information via our website, the Advocate, the Journal, and your component newsletter
Members-only courses at less than $10/credit
We are constantly learning and growing as an association. If you feel we could better serve you, we’d like to know how! Feel free to reach out at any time. The more dentists involved in our organization, the stronger your practice and your profession.
Serving your practice. Advancing your profession.
Don’t leave decisions that impact you and your profession up to people who aren’t dentists
Organized dentistry is a political force in Trenton. Through a combination of a vibrant New Jersey Dental Political Action Committee (NJDPAC), and an active grassroots membership (including more than 4,600 NJDA members), organized dentistry makes its voice heard in the State House.
Membership and support of NJDPAC guarantee you and other New Jersey dentists that we keep our influential voice in Trenton.
Questions?Call us today: 800-831-6532Or Email: [email protected]
39Volume 84, Number 4
Surgical and Restorative
Excellence in Dentistry Symposium
Featured Speakers:
Emil Cappetta, DMD David Garber, DMD Shankar Iyer, DDS, MDS John Kois, DMD, MSD Ernesto Lee, DMD Myron Nevins, DMD Rade Paravina, DDS, PhD Maurice Salama, DMD Michael Sonick, DMD Christian Stappert, DDS, PhD Dennis Tarnow, DMD Arnold Weisgold, DDS
Join us for this one-of-a-kind event where experts
from both specialties will share their wealth of knowledge. The most compelling topics will be discussed and debated by panels of
these dental masters.
Dates: Friday & Saturday, April 4 & 5, 2014 Location: The New York Athletic Club Central Park South, New York City Tuition: $645 – register by February 15, 2014 $695 – register after February 15, 2014
REGISTER ONLINE: cde.sdm.rutgers.edu OR CALL US: 973-972-6561Continuing Dental Education 110 Bergen St, B701 Newark, NJ 07103 email: [email protected]
2013 NJDA Partners
Platinum
Platinum Premier
Gold
Silver
Bronze
Volume 84, Number 440

We continue our 106th year of camaraderie and education asone of the oldest dental societies in the region!
Spring Dine Around: Wednesday, March 12, 2014
"The Many Faces of Facial Pain" Alan Stiles, D.M.D.limited to the management of head, neck, and facial pain. Following his completion of his DMD at Temple University, he completed a residency
CPR: Friday, April 25, 2014The Buck Hotel, Feasterville, PA
Spring All Day Program: Friday, May 9th, 2014The Buck Hotel, Feasterville, PA
“Productivity: It's not by chance”Bruce Baird, D.D.S.: The business of dentistry is changing as rapidly as new technology is changing how we treat patients. To succeed in today’s
change your thinking on the business of dentistry, challenge many of the beliefs that prevent practices from realizing their full potential, and
Dental Center. Dr. Baird specializes in cosmetic makeovers, full mouth rehabilitation, and dental implants.
Annual Golf Outing: June, 2014Philmont Country Club
You are also not a sales goal or a benchmark or a market segment.
You are a dentist. And we are The Dentists Insurance Company,
TDIC. More than 30 years ago, the small group of dentists who
started this company made three promises: to only protect dentists,
to protect them better than any other insurance company out there
and to be there when you need us. Because with TDIC, you’re a
dentist first, last and always.
Protecting dentists. It’s all we do.® 877.476.4588 | thedentists.com
You are not a statistic.
Endorsed by the New Jersey Dental Association
njda_ad_10-13 2.indd 1 10/17/13 9:50 AM





























